I ENDOMETRIOSIS ^595
Endometriosis, defined as the presence of endometrial tissue outside the uterine cavity, is a gynecologic condition that affects 6-10% of women of reproductive age, 50-60% of women and adolescent girls with pelvic pain, and up to 50% of women with infertility.
A familial predisposition toward endometriosis via a proposed polygenic and multifactorial mechanism has been documented. A female patient who has an affected first-degree relative has a 7-10-fold increased risk of also developing the condition. The retrograde menstruation theory has gained widespread acceptance as an explanation for the dissemination of endometrial cells outside of the uterus. The exact factor or factors that lead to the survival and subsequent implantation of the displaced endometrium remain unknown but may include immune dysfunction, gene mutations, or both. Defects with obstructed outflow, such as cervical or vaginal atresia and incomplete mullerian fusion, commonly are associated with pelvic endometriosis, although regression usually occurs after surgical correction of the anomaly.Endometriosis differs in presentation, findings on physical examination, and visibility at the time of laparoscopy between adolescents and adults (see also “Endometriosis in Adolescents” later in this section). Many experts have attempted to develop a classification system for endometriosis. The classification system developed by the American Society for Reproductive Medicine is commonly used (see Fig. 4-2). This system classifies endometriosis by the extent and location of disease.
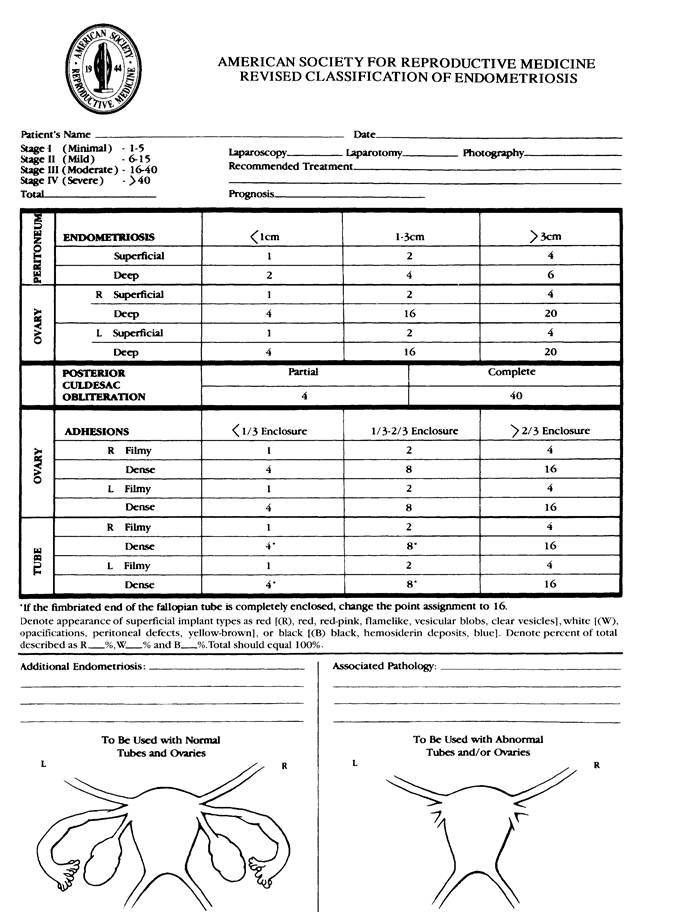
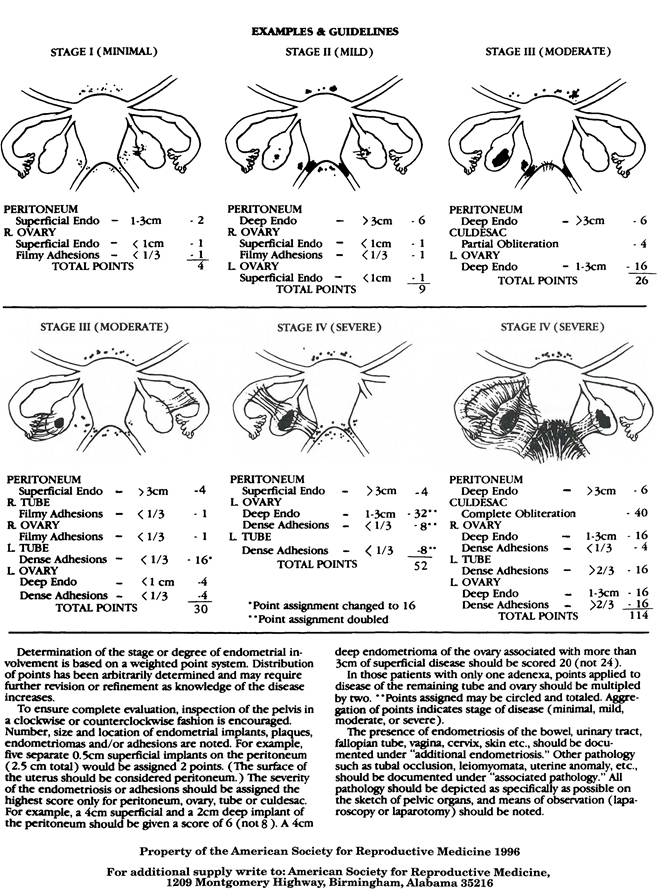
Fig. 4-2. Classification of endometriosis. (Reprinted from Fertility and Sterility Vol 67, American Society for Reproductive Medicine.
Revised classification of endometriosis, p. 817-21. Copyright 1997, with permission from American Society for Reproductive Medicine.) ^Symptoms
Symptoms and sequelae of endometriosis vary widely but include the following:
• Dysmenorrhea
• Adnexal mass (symptomatic or asymptomatic)
• Abnormal uterine bleeding
• Chronic pelvic pain
• Dyspareunia
• Infertility
• Uterosacral ligament nodularity
The most common symptom noted in published reviews is acquired or progressive dysmenorrhea. Pain often starts before the onset of menses. Other symptoms may include gastrointestinal symptoms, and a blackbrown discharge before menses.
Evaluation and Diagnosis
The differential diagnosis for endometriosis includes primary dysmenorrhea, adenomyosis, irritable bowel syndrome, obstructive mullerian anomalies, pelvic inflammatory disease, interstitial cystitis, musculoskeletal disorders, and other problems associated with pelvic pain, such as sexual abuse. Clinicians should carefully evaluate women for these other causes of pelvic pain before initiating aggressive treatment for endometriosis and reconsider these etiologies in women who do not respond to standard endometriosis therapies.
A significant number of women with endometriosis remain asymptomatic. For example, endometriosis is found in women undergoing tubal ligation and hysterectomy who have no history of endometriosis or pelvic pain. Thus, clinicians should consider the possibility that patients with proven endometriosis also may have other conditions that cause pelvic pain (see also the “Acute and Chronic Pain Management” section later in Part 4).
Direct visualization of endometriosis lesions remains the preferred method for diagnosing endometriosis. Nonetheless, the need for a surgical procedure to determine a diagnosis of endometriosis as the cause of pelvic pain continues to be debated. Arguments against the requirement to perform surgery to definitively diagnose endometriosis include the imprecision of surgical diagnosis as well as the inherent risks of surgery.
Management
Medical and surgical modalities have been used for management. For pain management, evidence exists to support short-term benefits with either modality. No definitive data indicate the superiority of either modality for long-term management of pain, and a substantial proportion of women managed with either method experience a recurrence of symptoms. Medical suppressive therapies, such as oral contraceptives or gonadotropinreleasing hormone (GnRH) agonists for endometriosis-associated infertility, are ineffective according to a 2007 Cochrane review (see Bibliography).
Clinicians should recognize that endometriosis is a chronic disorder. In discussing treatment options with the patient, clinicians should plan longterm therapy based on the patient’s age, presenting symptoms, severity of disease, and reproductive plans.
Nonsurgical Interventions
First-line therapy for women with presumed endometriosis who wish to preserve fertility includes combined oral contraceptives and nonsteroidal antiinflammatory drugs (NSAIDs). After failure of initial treatment, second-line therapies include empiric therapy with a 3-month course of a GnRH agonist, depot medroxyprogesterone acetate, the levonorgestrel intrauterine system (levonorgestrel intrauterine device [IUD]), and dan- azol. The role of aromatase inhibitors in the treatment of endometriosis is under investigation. Gonadotropin-releasing hormone agonists are highly effective in reducing the pain syndromes associated with endometriosis but are not superior to other methods, such as combined oral contraceptives as first-line therapy, and may have significant adverse effects, including hot flushes, vaginal dryness, and osteopenia. When a GnRH agonist is used for therapy, the administration of add-back therapy (using either sex-steroid hormones or other specific bone-sparing agents) may reduce or eliminate bothersome adverse effects and drug-induced bone mineral loss without reducing the efficacy of pain relief.
Add-back regimens have been advocated for use in women undergoing long-term GnRH therapy (more than 6 months), but can be started immediately. In patients with laparoscopy- confirmed endometriosis and dysmenorrhea, combined oral contraceptives and oral norethindrone, depot medroxyprogesterone acetate or the levonorgestrel IUD are effective compared with placebo and are equivalent to more costly regimens, such as GnRH agonists. Nonpharmacologic therapeutic options to manage pain associated with endometriosis include pelvic biofeedback, physical therapy, hypnotherapy, cognitive and relaxation techniques, massage, and acupuncture (see also the “Complementary and Alternative Medicine” section in Part 3).Surgical Interventions
The efficacy of surgical therapy depends heavily on the experience and expertise of the surgeon. Excision of an endometrioma is superior to simple drainage and ablation of the cyst wall. Long-term (at least 24 months) oral contraceptive use is effective in reducing endometrioma recurrence as well as in reducing the frequency and severity of dysmenorrhea. As discussed previously, medical suppressive therapies appear ineffective in the treatment of endometriosis-related infertility. Although surgical management of endometriosis-related infertility does improve pregnancy rates, the magnitude of improvement is unclear.
When surgery is elected, operative laparoscopy has numerous advantages compared with laparotomy. However, no conservative surgical method has been shown to be superior in the treatment of endometriosis. A substantial number of women (44%) will experience recurrence of symptoms within 1 year postoperatively.
Surgical methods in use include the following:
• Ablation of lesions
• Excision
• Endocoagulation
• Electrocautery
• Laser vaporization
Hysterectomy, with or without bilateral oophorectomy, often is regarded as definitive therapy for pain control; however, symptoms may recur even after hysterectomy and oophorectomy.
Ovarian conservation is associated with increased likelihood of recurrence of symptoms and additional surgery. Menopausal estrogen therapy is not contraindicated after bilateral salpingo-oophorectomy, but data on the recurrence of lesions and symptoms are limited.Consultation or Referral
Generalists should consider consultation or referral to a specialist if their level of expertise has been exceeded. The following referrals or support services may be needed:
• Reproductive endocrinologist
• Gynecologic surgeon
• Pain management unit
• Radiographic imaging
• Physical therapist
• Alternative therapies
— Hypnotherapy
— Relaxation techniques
— Massage
— Acupuncture
Endometriosis in Adolescents ^583
Endometriosis can be a debilitating disease in adolescent females, and prompt evaluation and consideration of the adverse effects of endometriosis is essential in this age group. Gynecologists, pediatricians, and other adolescent health care providers should recognize that thelarche and the presence of endogenous estrogen can be considered a developmental milestone and benchmark for inclusion of endometriosis in the differential diagnosis of adolescent females with chronic pelvic pain or dysmenorrhea. A multidisciplinary team approach to the adolescent who has endometriosis may be the most rewarding for the adolescent, her family, and the clinician.
Evaluation and Diagnosis
Adolescent patients typically present with progressive and severe dysmenorrhea, but also may present with noncyclic pelvic pain. A thorough review of a patient’s history and physical examination are necessary to assess for the differential diagnoses of pelvic pain, such as appendicitis, pelvic inflammatory disease, mullerian anomalies or outflow obstruction, bowel disease, hernias, musculoskeletal disorders, and psychosocial complaints. It is important to evaluate the vagina and uterus for a possible obstructive anomaly and the ovaries for a possible ovarian mass.
Findings of the physical examination of adolescents may vary from the adult population because uterosacral nodularity and endometriomas are found in more advanced disease and, thus, are uncommon in adolescents.Management
Treatment should focus on conservative, fertility-sparing measures with medical and surgical interventions. The first line of therapy for an adolescent with presumed endometriosis should include combined oral contraceptive and NSAIDs. After a comprehensive evaluation and adequate trial of combined oral contraceptives and NSAIDs without improvement in pain, laparoscopy can be offered for diagnosing and treating presumed endometriosis in an adolescent. Laparoscopy can be safely performed in adolescents, but the benefits always should be considered relative to the risks of surgery. Gynecologic surgeons who perform laparoscopy in adolescents with pelvic pain should be familiar with the typical lesions of endometriosis in adolescents, which tend to be red, clear, or white, as opposed to the “powder-burn” lesions seen commonly in adults who have endometriosis.
All adolescents should be offered medical therapy after surgery until they have completed child-bearing to suppress pain and progression of disease. Treatment after surgery should involve the use of NSAIDs and menstrual suppression with continuous combined oral contraceptives, depot medroxyprogesterone acetate, or the levonorgestrel IUD. Gonadotropinreleasing hormone agonists are effective in the treatment of endometriosis- related pain in adolescents, but their use alone (without add-back therapy) is limited to 6 months because of adverse effects on bone mineral density. Because there are limited data on the long-term effects of GnRH agonists with add-back therapy, their use may be reserved for adolescents refractory to continuous combination hormonal therapy menstrual suppression. Long-term treatment should continue until desired family size is reached or fertility no longer needs to be preserved. For more information, please see the American College of Obstetricians and Gynecologists’ resource Guidelines for Adolescent Health Care.
Bibliography
American College of Obstetricians and Gynecologists. Endometriosis in adolescents. Guidelines for adolescent health care [CD-ROM]. 2nd ed. Washington, DC: American College of Obstetricians and Gynecologists; 2011. p. 164-71.
Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril 2012;98:511-9. [PubMed] [Full Text]
Davis L, Kennedy SS, Moore J, Prentice A. Oral contraceptives for pain associated with endometriosis. Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD001019. DOI: 10.1002∕14651858.CD001019.pub2. [PubMed] [Full Text] Elective and risk-reducing salpingo-oophorectomy. ACOG Practice Bulletin No. 89. American College of Obstetricians and Gynecologists. Obstet Gynecol 2008;111: 231-41. [PubMed] [Obstetrics & Gynecology]
Endometriosis and infertility: a committee opinion. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril 2012;98:591-8. [PubMed] [Full Text]
Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am 1997;24:235-58. [PubMed]
Goldstein DP, deCholnoky C, Emans SJ, Leventhal JM. Laparoscopy in the diagnosis and management of pelvic pain in adolescents. J Reprod Med 1980;24:251-6. [PubMed]
Hughes E, Brown J, Collins JJ, Farquhar C, Fedorkow DM, Vanderkerchove P. Ovulation suppression for endometriosis for women with subfertility. Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD000155. DOI: 10.1002/ 14651858.CD000155.pub2. [PubMed] [Full Text]
Malinak LR, Buttram VC, Jr, Elias S, Simpson JL. Heritage aspects of endometriosis. II. Clinical characteristics of familial endometriosis. Am J Obstet Gynecol 1980;137:332-7. [PubMed]
Management of endometriosis. Practice bulletin No. 114. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010;116:223-36. [PubMed] [Obstetrics & Gynecology]
Matalliotakis IM, Arici A, Cakmak H, Goumenou AG, Koumantakis G, Mahutte NG. Familial aggregation of endometriosis in the Yale Series. Arch Gynecol Obstet 2008;278:507-11. [PubMed]
Noncontraceptive uses of hormonal contraceptives. Practice Bulletin No. 110. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010;115: 206-18. [PubMed] [Obstetrics & Gynecology]
Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril 1997;67:817-21. [PubMed]
Treatment of pelvic pain associated with endometriosis. Practice Committee of American Society for Reproductive Medicine. Fertil Steril 2008;90:S260-9. [PubMed] [Full Text]
Resources
American College of Obstetricians and Gynecologists. Abnormal uterine bleeding. Patient Education Pamphlet AP095. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Chronic pelvic pain. Patient Education Pamphlet AP099. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
American College of Obstetricians and Gynecologists. Dysmenorrhea. Patient Education Pamphlet AP046. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Endometriosis. Patient Education Pamphlet AP013. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Evaluating infertility. Patient Education Pamphlet AP136. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Treating infertility. Patient Education Pamphlet AP137. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. When sex is painful. Patient Education Pamphlet AP020. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
American Society for Reproductive Medicine. Endometriosis. Available at: http:// www.asrm.org/topics/detail.aspx?id=440. Retrieved July 31, 2013.
American Society for Reproductive Medicine. Endometriosis: a guide for patients. Birmingham (AL): ASRM; 2012. Available at: http://www.asrm.org/uploadedFiles/ ASRM_Content/Resources/Patient_Resources/Fact_Sheets_and_Info_Booklets/ endometriosis.pdf. Retrieved July 31, 2013.
Cochrane Collaboration. Cochrane reviews. Available at: http://www.cochrane.org/ cochrane-reviews. Retrieved July 31, 2013.