Acute Abdominal Pain in Pregnancy
Kelly A. Best
Acute abdominal pain in pregnancy poses a unique challenge for both the clinician and the patient. The physiologic and physical changes associated with pregnancy must be considered when conducting a history, performing a physical examination, and interpreting diagnostic and other laboratory results in the pregnant patient with acute abdominal pain.
Surgical interventions for nonob- stetric reasons during pregnancy are reported to occur in 0.2% to 2.2% of all gestations (1). The most common etiologies for these surgical interventions include adnexal masses, acute appendicitis, and gallstone disease (2). Therefore, it is of critical importance to involve the expertise of the obstetrician, the general surgeon, and the radiologist in the evaluation of the pregnant patient who presents with acute abdominal pain.This chapter reviews common causes of acute abdominal pain in pregnancy and facilitates interpretation of laboratory and diagnostic tests in pregnant women. The diagnostic approach to pregnant as well as nonpregnant patients should be similar. Clinicians should resist the temptation to uniformly attribute the patient’s symptoms to her pregnancy. In addition, clinicians should have a high index of suspicion as classical findings may not be present for certain disease states. Delay in diagnosis resulting in complications associated with the underlying condition may lead to premature labor and delivery (3).
PHYSIOLOGIC CHANGES IN PREGNANCY
Expansion of the plasma volume and an increase in red blood cell mass begin as early as the 4th week of pregnancy, peak at 28 to 34 weeks of gestation, and then plateau until parturition (4,5). Plasma volume expansion is accompanied by a lesser increase in red cell volume (6). As a result, there is a modest reduction in hematocrit, with peak hemodilution occurring at 24 to 26 weeks.
The blood volume in pregnant women at term is about 100mL∕kg (7). The cardiac output rises 30% to 50% (1.8 L per minute) above baseline during normal pregnancy in part from changes in three important factors that determine cardiac output: preload is increased due to the associated rise in blood volume, afterload is reduced due to the decline in systemic vascular resistance, and maternal heart rate rises by 15 to 20 beats per minute (8).During pregnancy, white cell volume increases from 5,000 to 6,000 cells/ mm3 to 16,000 cells∕mm3 in the second and third trimesters and to 20,000 to 30,000 cells∕mm3 in early labor (9). The glomerular filtration rate (GFR) and renal blood flow rise markedly during pregnancy. The increase in GFR can be demonstrated within 1 month of conception and reaches a peak approximately 40% to 50% above baseline levels by the end of the first trimester, resulting in a decrease in blood urea nitrogen and serum creatinine as well as glucosuria despite normal plasma glucose levels (10). Both kidneys increase in size by 1 to 1.5 cm during pregnancy primarily due to an increase in renal vascular and interstitial volumes (10). Ureteral dilatation during pregnancy results from hormonal effects, external compression, and intrinsic changes in the ureteral wall (11). Physiologic hydronephrosis typically occurs and is more common on the right than the left side (90% versus 10%).
In the respiratory system, the diaphragm rises by up to 4 cm, and the chest diameter can increase by 2cm or more (12). Diaphragmatic excursion is not limited by the uterus and actually increases by up to 2 cm. Pregnancy is a state of relative hyperventilation, which may be centrally mediated through progesterone. The respiratory rate does not change while the tidal volume increases, resulting in an approximately 50% increase in minute ventilation. The normal PaO2 in pregnant women ranges from 100 to 110 mm Hg (13-16). In addition, there is a decrease in arterial carbon dioxide levels (PCO2 and PaCO2) from the nonpregnant average of 40 mm Hg to a plateau of 27 to 32 mm Hg during pregnancy (14,15).
This respiratory alkalosis is followed by compensatory renal excretion of bicarbonate, so that the resultant arterial pH is normal to slightly alkalotic (usually 7.40 to 7.45) (16). The decrease in PaCO2 probably helps the fetus to eliminate carbon dioxide across the placenta.Physical examination changes in pregnancy
Pain perceived from the abdomen is caused by peritoneal irritation, mechanical stretching, or ischemia (17). Physical exam findings in pregnancy may be blunted compared with those of nonpregnant patients with the same disease or process. Peritoneal signs may be absent due to the lifting and stretching of the anterior abdominal wall in pregnancy, preventing contact with the parietal peritoneum and eliminating rebound tenderness or guarding (18). In addition, the gravid uterus may distort the clinical picture by obstructing the movement of the omentum to an area of inflammation. Performing an examination with a pregnant patient in the left or right decubitus position, displacing the uterus to one side, may be of some benefit in certain clinical situations.
IMAGING TECHNIQUES
Diagnostic imaging is often necessary during pregnancy. Sonographic examination is a common occurrence in pregnant women, but other types of radiological evaluation may also be required. Although the safety of radiation exposure during pregnancy is a common concern, a missed or delayed diagnosis can pose a greater risk to the woman and her pregnancy than any hazard associated with ionizing radiation (19). In many cases, the perception of fetal risk is higher than the actual risk (20,21). Table 2.1 provides an overview of the total fetal exposure of ionizing radiation in some commonly performed radiologic studies. Ionizing radiation can result in the following three harmful effects: (a) cell death and teratogenic effects, (b) carcinogenesis, and (c) genetic effects or mutations in germ cells (22). The threshold at which an increased risk of congenital malformations is observed in radiation-exposed embryos/fetuses has not been definitively determined.
The best evidence suggests that the risk of malformations is increased at doses above 0.10 Gy, whereas the risk between 0.05 and 0.10 Gy is less clear (23). The American College of Obstetricians and Gynecologists makes the following recommendations for the use of diagnostic imaging techniques in pregnancy (24):Women should be counseled that X-ray exposure from a single diagnostic procedure does not result in harmful fetal effects. Specifically, exposure to less than 5 rad has not been associated with an increase in fetal anomalies or pregnancy loss.
Concern about possible effects of high-dose ionizing radiation exposure should not prevent medically indicated diagnostic X-ray procedures from being performed on a pregnant woman. During pregnancy, other imaging procedures not associated with ionizing radiation (ultrasonography, MRI) should be considered instead of X-rays when appropriate.
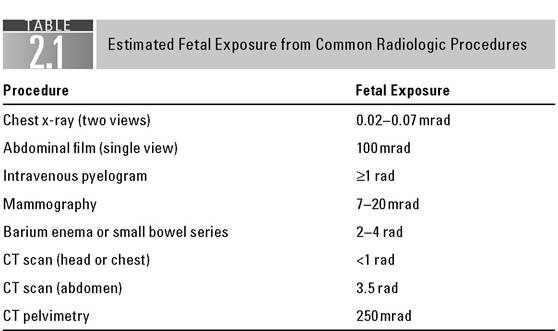
Note: 1 rad = 0.01 gray (Gy).
Source: Adapted from Ref. 24; Data from Cunningham FG, Gant NF, Leveno KJ, Gilstrap LC III, Hauth JC,
Wenstrom KD (eds). General considerations and maternal evaluation. In: Williams Obstetrics. 21st Ed. New York, NY: McGraw-Hill; 2001:1143-1158.
COMMON CAUSES OF ACUTE ABDOMINAL PAIN IN PREGNANCY
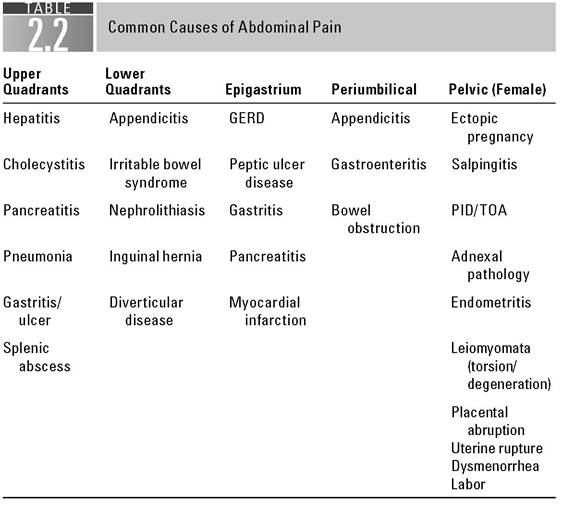
The differential diagnosis of acute abdominal pain in pregnancy includes etiologies similar to those in the nonpregnant patient as well as causes specific to the pregnancy (Table 2.2). The following sections review common causes of acute abdominal pain in pregnancy and detail safe diagnostic strategies for both the mother and the fetus.
Appendicitis
Acute appendicitis is the most common nonobstetric surgical diagnosis during pregnancy (25). The incidence ranges from 0.06% to 0.1%, or 1 in 1,500 deliveries (26-28). Appendicitis is more frequently seen in the second trimester when compared with the first and third trimesters or during the postpartum period (29).
An infected appendix appears to be more likely to rupture during pregnancy, possibly because of delay in diagnosis and intervention (30,31).Right lower quadrant pain is the most common symptom of appendicitis. Although older studies suggested that the location of the appendix migrates upward with the enlarging uterus, this theory has been refuted by subsequent studies which have found that the most common symptom of appendicitis, that is, right lower quadrant pain, occurs within a few centimeters of McBurneys point in the vast majority of pregnant women, regardless of the stage of pregnancy (31,32).
The physiologic changes of pregnancy can confound the diagnosis of appendicitis. Leukocytosis can be a normal finding in pregnant women. Indigestion, bowel irregularity, nausea/vomiting, as well as a sense of not feeling well are also common symptoms of both appendicitis and normal pregnancy. The temporal relationship of these symptoms is essential in differentiating early appendicitis from the nausea and vomiting of pregnancy. In appendicitis, nausea and vomiting, if present, typically follow the onset of pain, whereas nausea and vomiting associated with pregnancy are not usually associated with pain. Microscopic hematuria and pyuria are found in up to one third of patients with acute
appendicitis, and a decrease in the direct contact between the area of inflammation and the parietal peritoneum results in less muscle response or guarding.
The gold standard for diagnostic imaging of the appendix in pregnancy is graded compression ultrasonography. Appendicitis is diagnosed if a noncom- pressible blind-ended tubular structure is visualized in the right lower quadrant with a maximal diameter >6 mm (33,34). Magnetic resonance imaging (MRI) can be useful for the next step in cases with diagnostic uncertainty and provides an attractive alternative to CT because it avoids exposure to ionizing radiation.
Consultation with a general surgeon should be obtained in women whose imaging studies or physical examination suggest appendicitis. The decision to proceed to laparotomy should be based upon the clinical findings, the diagnostic imaging results, and the clinical judgment. Given the diagnostic difficulties and the significant risk of fetal morbidity or mortality with perforation (36% versus 1.5%) (26) or with peritonitis or abscess (fetal loss: 6% versus 2%; early delivery: 11% versus 4%), a higher negative laparotomy rate (20% to 35%) compared with nonpregnant women has generally been considered to be acceptable (35,36).
A transverse incision at McBurneys point, or more commonly over the point of maximal tenderness, can be utilized in pregnancy (37). When the diagnosis is less certain, a lower midline vertical incision can be utilized since it permits adequate exposure of the abdomen for diagnosis and treatment of surgical conditions that mimic appendicitis. A vertical incision can also be used for a cesarean delivery, if subsequently required for obstetric indications. Case reports and small case series regarding laparoscopic appendectomy in pregnancy suggest that such procedures can be performed successfully during all trimesters and with few complications (38-41). The decision to proceed with such an approach should take into consideration the skill and experience of the surgeon, as well as clinical factors such as the size of the gravid uterus. Modifications of the technique during pregnancy should include the following: a slight left lateral positioning of the patient, avoiding the use of any cervical instruments; use of open entry techniques or placement of trocars under direct visualization; and limiting the intra-abdominal pressure to throughout pregnancy, while surgical management of complicated adnexal masses is necessary in approximately 1 in 1,300 pregnancies (51,52).
Adnexal torsion is more common in pregnancy than in the nonpregnant state (26) and has been reported in up to 7% of pregnant patients with adnexal masses (53). Pain associated with torsion is often intermittent, crampy and may radiate to the ipsilateral thigh or flank. Nausea and vomiting may also develop. Examination findings may include a palpable fullness in the pelvis or lower quadrant and, in the presence of rupture, peritoneal signs may be present. While the patient may remain afebrile with a normal or slightly elevated white count, hemoglobin may be decreased when rupture results in hemoperitoneum (and in severe cases, hypovolemic shock). Transvaginal and transabdominal ultrasound examinations are the imaging modalities of choice when evaluating an adnexal mass.
While laparotomy (with a vertical midline incision to facilitate exposure and allow for extension if indicated) should be regarded as the preferred approach for the surgical management of ovarian torsion in pregnancy, several reports have suggested that laparoscopy by a surgeon skilled in this approach may be acceptable (53-55). In some circumstances, adnexal cyst rupture may be treated expectantly if the clinical condition remains stable.
A persistent adnexal cyst larger than 5 cm in a pregnant woman should be removed electively during the early second trimester of pregnancy because torsion, rupture, or hemorrhage often requires emergency surgery and can lead to preterm delivery (51). On occasion, a simple cyst that is 5 to 10 cm in size can be managed expectantly if the patient is asymptomatic and serial ultrasound examinations show no increase in size. If the cyst persists, excision can be performed at cesarean delivery or postpartum. It is important to consider that a large adnexal cyst in the posterior cul-de-sac has the potential to produce obstructed labor and delivery. Surgical intervention is indicated for an adnexal mass of any size suspicious for malignancy or if torsion, rupture, or hemorrhage is suspected. An adnexal mass identified incidentally at the time of cesarean delivery should be removed (56). Complete surgical removal is preferred to aspiration since malignancy could be missed even with simple, smooth-walled cysts (57).
Postoperative progesterone is recommended when the corpus luteum is removed prior to 8 to 10 weeks of gestation.
Pyelonephritis and Nephrolithiasis
Acute pyelonephritis is a common complication of pregnancy as the physiologic changes in pregnancy often predispose women to this condition. Ascending infection from the urinary bladder is the likely etiology in the majority of cases. As the gravid uterus enlarges, increased pressure on the ureters at the pelvic brim, as well as the relaxant effect of circulating progesterone on the ureters, predisposes the pregnant patient to urinary stasis (58).
Patients with acute pyelonephritis often appear acutely ill and may complain of flank pain, dysuria, frequency, fever, and shaking chills. Costovertebral angle tenderness may be present on the affected side while abdominal pain is less common. The white count will likely be elevated with a concomitant left shift. Urinalysis typically reveals both pyuria and bacteriuria. Urine culture with sensitivity will guide treatment; however, initiation of intravenous antibiotics directed at Gram-negative enteric bacteria should be initiated as soon as possible while urinary cultures are pending.
The development of symptomatic nephrolithiasis during pregnancy is a rare event, occurring in about 1 in every 1,500 to 3,000 pregnancies (59). Affected patients usually present in the second or third trimester (—20% in the first trimester) with acute flank pain (90%), which often radiates to the groin or lower abdomen. Nausea, vomiting, urinary frequency, and urgency are also typical. Microscopic hematuria is present in 75% to 95% of patients, one third of whom have gross hematuria (59).
Renal and pelvic ultrasound should be performed when an obstructing calculus is suspected. This modality avoids exposure to radiation and is useful for detecting secondary signs of obstruction, such as hydronephrosis or hydroureter (60). Physiologic hydronephrosis of pregnancy must be distinguished from pathological hydronephrosis from obstruction. When the ultrasound examination is negative and the patient has continued discomfort suggestive of nephrolithiasis, two options are available for diagnosis: a limited intravenous pyelogram (IVP) in which a single abdominal radiograph is taken approximately 5 minutes after intravenous administration of contrast material (60) or, if available, ureteroscopy (61). The single-shot IVP, which delivers about 50 mrad to the fetus, is positive in most pregnant women with a symptomatic stone (60). MRI can also be a useful adjunct in assessing stones during pregnancy. T2-weighted MRI can offer differing urographic appearances in physiologic and calculus obstruction (62).
Most (75% to 85%) stones pass spontaneously, due in part to the normally dilated urinary tract in pregnant women (58,59). Cystoscopy with insertion of a ureteral stent or ureteroscopy to remove or fragment the stone may be required in the patient who is septic, has persistent severe pain, or has obstruction in a solitary functioning kidney (61,63). Ureteral stenting or placement of a nephrostomy tube to relieve obstruction or pain is a valid option for managing pregnant patients. However, pregnancy significantly increases the risk of stent encrustation, necessitating the need for frequent ureteral stent exchange (64). If conservative management fails, ureteroscopy with lithotripsy may be an option. Although shock wave lithotripsy has been inadvertently performed in a few pregnant women, its use during pregnancy is currently contraindicated (65,66).
Bowel Obstruction
Bowel obstruction complicates 1 in 1,500 to 3,500 deliveries (67). Risk factors for bowel obstruction in pregnancy are related to adhesions from pelvic infection and previous surgery, complications of Crohn’s disease, intussusception, and more rarely neoplasm.
Symptoms of intestinal obstruction are similar to those in the nonpregnant population and include abdominal distention, vomiting, abdominal pain, and an inability to pass flatus. Pain is generally periumbilical, paroxysmal, and crampy. On physical examination, the large, gravid abdomen may pose a diagnostic challenge as it may mask the usual findings during auscultation, percussion, and palpation. In general, abdominal tenderness, abnormal bowel sounds (high pitched or hypoactive), tachycardia, and hypotension may be present.
While laboratory studies are not helpful in establishing the diagnosis of bowel obstruction, they may be utilized to monitor the white blood cell count (a sharp rise over a short period of time may indicate strangulation) and to assess the degree of dehydration. The diagnosis of small bowel obstruction can be made by a history and a physical examination in the majority of patients. Plain abdominal radiography is used to confirm the diagnosis of bowel obstruction. Ordering an upright chest film to rule out the presence of free air, as well as supine and upright abdominal films, is appropriate in this setting. Of note, plain films can be equivocal in 20% to 30% of patients and are “normal, nonspecific, or misleading” in 10% to 20% (68,69). Multiple air-fluid levels with distended loops of small bowel are seen in small bowel obstruction, although occasionally they can be seen in the setting of a paralytic ileus. Abdominal ultrasonography can also be useful, especially as a bedside test for the critically ill (70,71).
Treatment of small bowel obstruction in pregnancy is similar to that in nonpregnant individuals. Aggressive intervention is warranted because delay in treatment increases maternal and fetal morbidity and mortality. Fluid and electrolyte replacement, bowel decompression, and prompt surgical intervention in cases resistant to decompression are suggested.
LAPAROSCOPIC SURGERY IN PREGNANCY
Laparotomy has generally been accepted as the approach of choice for surgical exploration in pregnancy. Recent case reports and case series of successful laparoscopy in pregnancy have called into question this long-held belief (55,72,73). Theoretical areas of concern have included the potential decrease in uteroplacental blood flow resulting in fetal hypoxia due to the rise in intra-abdominal pressure during pneumoperitoneum, fetal acidosis from absorption of carbon dioxide, and direct or indirect fetal injury if the uterus is perforated by a trocar or a Veress needle.
Although prospective studies are lacking, multiple case series evaluating the safety of laparoscopy in pregnancy have reported laparoscopic procedures in all trimesters with minimal morbidity to the fetus with regard to fetal weight, gestational duration, intrauterine growth restriction, congenital malformations, stillbirths, or neonatal deaths (73).
The benefits of laparoscopy for pregnant and nonpregnant women include less postoperative pain, less postoperative ileus, reduction in adhesion formation, shorter hospital stay, less narcotic use, improved respiratory efforts, and faster return to usual activities (74). In addition, there may be less uterine manipulation and improved visualization in the gravid population when compared with laparotomy (73-75). The following are considerations when laparoscopy is performed in pregnancy:
1. Laparoscopy can be performed in any trimester; however, the optimal time for nonemergent indications is the early second trimester.
2. Use of an oral or nasogastric tube for gastric decompression.
3. Use of prophylactic pneumatic compression devices (with the need for pharmacologic thromboprophylaxis determined on a case-by-case basis) to prevent thrombosis.
4. Avoidance of uterine/cervical manipulators.
5. Supine or low lithotomy position with a leftward tilt.
6. Establishment of pneumoperitoneum is dependent on the surgeon’s experience and comfort.
7. Intra-abdominal pressure should be maintained between 8 and 12 mm Hg and should not exceed 15 mm Hg.
8. Fetal heart rate should be confirmed and documented before and after the procedure. If fetal monitoring is necessary during the procedure, consideration for transabdominal or transvaginal ultrasound assessment should be made.
9. Fetal heart rate and uterine activity should be monitored in the recovery room by protocols appropriate for gestational age.
10. Nonsteroidal antiinflammatory drugs should be avoided, especially after 32 weeks of gestation, while opioids and antiemetics can be used as needed.
SUMMARY
The presence of the fetus should not delay the decision to perform the indicated diagnostic testing or to initiate treatment, as delays in this setting often result in significant morbidity and mortality for both the mother and the fetus. A multidisciplinary approach with early consultation from obstetric, surgical, laboratory, and radiologic services is warranted. Because obstetric causes for abdominal pain exist in many patients, however, consultation with an obstetric provider will help to define the subset of patients who warrant further investigation into nonobstetric sources for acute abdominal pain.
References
1. Hunt MG, Martin JN Jr, Martin RW, Meeks GR, Wiser WL, Morrison JC. Perinatal aspects of abdominal surgery for nonobstetric disease. Am J Perinatol 1989;6(4):412-417.
2. Semin, GS. Anesthesia for nonobstetric surgery in the pregnant patient. Perinatology. 2002;26(2):136-145.
3. Kilpatrick CC, Orejuela FJ. Management of the acute abdomen in pregnancy: a review. Curr Opin Obstet Gynecol. 2008;20(6):534-539.
4. Assali NS, Brinkman CR III. Pathophysiology of Gestation, Vol 1: Maternal Disorders. New York, NY: Academic Press; 1972:278.
5. Ueland K. Cardiorespiratory physiology of pregnancy. In Vanassa A Barss, MD (ed): Gynecology and Obstetrics. Vol. 3. Baltimore, MD: Harper & Row; 1979.
6. Pritchard JA. Changes in the blood volume during pregnancy and delivery. Anesthesiology. 1965;26:393.
7. Metcalfe J, Ueland K. Maternal cardiovascular adjustments to pregnancy. Prog Cardiovasc Dis. 1974;16:363.
8. Robson SC, Hunter S, Boys RJ, Dunlop W. Serial study of factors influencing changes in cardiac output during human pregnancy. Am J Physiol. 1989;256:H1060.
9. Pritchard JA, Baldwin RM, Dickey JC, et al. Blood volume changes in pregnancy and the puerperium. Am J Obstet Gynecol. 1962;84:1271.
10. Davison JM, Dunlop W. Renal haemodynamics and tubular function in normal human pregnancy. Kidney Int. 1980;18:152.
11. Beydoun SN. Morphologic changes in the renal tract in pregnancy. Clin Obstet Gynecol. 1985;28:249.
12. Weinberger SE, Weiss ST, Cohen WR, et al. Pregnancy and the lung. Am Rev Respir Dis. 1980;121:559.
13. Gilroy RJ, Mangura BT, Lavietes MH. Rib cage and abdominal volume displacements during breathing in pregnancy. Am Rev Respir Dis. 1988;137:668.
14. Liberatore SM, Pistelli R, Patalano F, et al. Respiratory function during pregnancy. Respiration. 1984;46:145.
15. Pernoll ML, Metcalfe J, Kovach PA, et al. Ventilation during rest and exercise in pregnancy and postpartum. Respir Physiol. 1975;25:295.
16. Artal R, Wiswell R, Romem Y, Dorey F. Pulmonary responses to exercise in pregnancy. Am J Obstet Gynecol. 1986;154:378.
17. Mayen IE, Hussain H. Abdominal pain during pregnancy. Gastroenterol Clin North Am. 1998;27:1.
18. Sivanesaratnam V. The acute abdomen and the obstetrician. Clin Obstet Gynaecol. 2000;14(1):89-102.
19. McCollough CH, Schueler BA, Atwell TD, et al. Radiation exposure and pregnancy: when should we be concerned? Radiographics. 2007;27:909.
20. Ratnapalan S, Bona N, Chandra K, Koren G. Physiciansperceptions of teratogenic risk associated with radiography and CT during early pregnancy. Am J Roentgenol. 2004;182:1107.
21. Bentur Y, Horlatsch N, Koren G. Exposure to ionizing radiation during pregnancy: perception of teratogenic risk and outcome. Teratology. 1991;43:109.
22. Hall EJ. Scientific view of low-level radiation risks. Radiographics. 1991;11:509-518.
23. www.icrp.org
24. ACOG Committee Opinion No. 299. Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol. 2004;104:647.
25. Tamir IL, Bongard FS, Klein SR. Acute appendicitis in the pregnant patient. Am J Surg. 1990;160:571.
26. Sharp HT. Gastrointestinal surgical conditions during pregnancy. Clin Obstet Gynecol. 1994;37:306.
27. Andersen B, Nielsen TF. Appendicitis in pregnancy: diagnosis, management and complications. Acta Obstet Gynecol Scand. 1999;78:758.
28. Mourad J, Elliott JP, Erickson L, Lisboa L. Appendicitis in pregnancy: new information that contradicts long-held clinical beliefs. Am J Obstet Gynecol. 2000;182: 1027.
29. Andersson B, Lambe M. Incidence of appendicitis during pregnancy. Int J Epidemiol. 2001;30:1281.
30. Bickell NA, Aufses AH Jr, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. JAm Coll Surg. 2006;202:401.
31. Weingold AB. Appendicitis in pregnancy. Clin Obstet Gynecol. 1983;26:801.
32. Hodjati, H, Kazerooni, T. Location of the appendix in the gravid patient: a re-evaluation of the established concept. Int J Gynaecol Obstet. 2003;81:245.
33. Barloon TJ, Brown BP, Abu-Yousef MM, et al. Sonography of acute appendicitis in pregnancy. Abdom Imaging. 1995;20:149.
34. Lim HK, Bae SH, Seo GS. Diagnosis of acute appendicitis in pregnant women: value of sonography. Am J Roentgenol. 1992;159:539.
35. Babaknia A, Parsa H, Woodruff JD. Appendicitis during pregnancy. Obstet Gynecol. 1977;50:40.
36. McGory ML, Zingmond DS, Tillou A, et al. Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss. J Am Coll Surg. 2007;205:534.
37. Popkin CA, Lopez PP, Cohn SM, et al. The incision of choice for pregnant women with appendicitis is through McBurneys point. Am JSurg. 2002;183:20.
38. Curet MJ, Allen, D, Josloff, RK, Pitcher, DE. Laparoscopy during pregnancy. Arch Surg. 1996;131:546.
39. Gurbuz AT, Peetz ME. The acute abdomen in the pregnant patient. Is there a role for laparoscopy? Surg Endosc. 1997;11:98.
40. Affleck DG, Handrahan DL, Egger MJ, Price RR. The laparoscopic management of appendicitis and cholelithiasis during pregnancy. Am J Surg. 1999;178:523.
41. Wu JM, Chen KH, Lin HF, et al. Laparoscopic appendectomy in pregnancy. J Laparoendosc Adv Surg Tech. 2005;15:447.
42. Al-Fozan H, Tulandi T. Safety and risks of laparoscopy in pregnancy. Curr Opin Obstet Gynecol. 2002;14:375.
43. Landers D, Carmona R, Crombleholme W, Lim R. Acute cholecystitis in pregnancy. Obstet Gynecol. 1987;69:131.
44. Mazze RI, Kallen B. Reproductive outcome after anesthesia and operation during pregnancy: a registry study of 5405 cases. Am J Obstet Gynecol. 1989;161:1178.
45. Stauffer RA, Adams A, Wygal J, Lavery JP. Gallbladder disease in pregnancy. Am J Obstet Gynecol. 1982;144:661.
46. Shea JA, Berlin JA, Escarce JJ, et al. Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Intern Med. 1994;154:2573.
47. Amos JD, Schorr SJ, Norman PF, et al. Laparoscopic surgery during pregnancy. Am J Surg. 1996;171:435.
48. Lanzafame RJ. Laparoscopic cholecystectomy during pregnancy. Surgery. 1995;118:627.
49. Lachman E, Schienfeld A, Voss E, et al. Pregnancy and laparoscopic surgery. JAm Assoc Gynecol Laparosc. 1999;6:347.
50. Hoffman MS, Sayer RA. Adnexal masses in pregnancy. OBG Management. 2007;19:27.
51. Hess LW, Peaceman A, O'Brien WF, Winkel CA. Adnexal mass occurring with intrauterine pregnancy: report of fifty-four patients requiring laparotomy for definitive management. Am J Obstet Gynecol. 1988;158:1029.
52. Whitecar MP, Turner S, Higby MK. Adnexal masses in pregnancy: a review of 130 cases undergoing surgical management. Am J Obstet Gynecol. 1999;181:19.
53. Shalev E, Peleg D. Laparoscopic treatment of adnexal torsion. Surg Gynecol Obstet. 1993;176:448.
54. Cohen SB, Oelsner G, Seidman DS, Admon D, Mashiach S, Goldenberg M. Laparoscopic detorsion allows sparing of the twisted ischemic adnexa. J Am Assoc Gynecol Laparosc. 1999;6:139.
55. Soriano D, Yefet Y, Seidman DS, Goldenberg M, Mashiach S, Oelsner G. Laparoscopy versus laparotomy in the management of adnexal masses during pregnancy. Fertil Steril. 1999;71:955.
56. Koonings PP, Platt LD, Wallace R. Incidental adnexal neoplasms at cesarean section. Obstet Gynecol. 1988;72:767.
57. Rodin A, Coltart TM, Chapman MG. Needle aspiration of simple ovarian cysts in pregnancy. Case reports. Br J Obstet Gynaecol. 1989;96:994.
58. Gilstrap LC, Ramin SM. Urinary tract infections during pregnancy. Obstet Gynecol Clin North Am. 2001;28(3):581-591.
59. Butler EL, Cox SM, Eberts EG, Cunningham FG. Symptomatic nephrolithiasis complicatingpregnancy. Obstet Gynecol. 2000;96:753.
60. Boridy IC, Maklad N, Sandler CM. Suspected urolithiasis in pregnant women: imaging algorithm and literature review. AJRAm J Roentgenol. 1996;167:869.
61. Scarpa RM, De Lisa A, Usai E. Diagnosis and treatment of ureteral calculi during pregnancy with rigid ureteroscopes. J Urol. 1996;155:875.
62. Spencer JA, Chahal R, Kelly A, et al. Evaluation of painful hydronephrosis in pregnancy: magnetic resonance urographic patterns in physiological dilatation versus calculous obstruction. J Urol. 2004;171:256.
63. McAleer SJ, Loughlin KR. Nephrolithiasis and pregnancy. Curr Opin Urol. 2004;14:123.
64. Parulkar BG, Hopkins TB, Wollin MR, et al. Renal colic during pregnancy: a case for conservative treatment. J Urol. 1998;159:365.
65. Asgari MA, Safarinejad MR, Hosseini SY, Dadkhah F. Extracorporeal shock wave lithotripsy of renal calculi during early pregnancy. BJU Int. 1999;84:615.
66. Deliveliotis CH, Argyropoulos B, Chrisofos M, Dimopoulos CA. Shockwave lithotripsy in unrecognized pregnancy: interruption or continuation? J Endourol. 2001;15:787.
67. Coleman MT, Trianfo VA, Rund DA. Nonobstetric emergencies in pregnancy: trauma and surgical conditions. Am J Obstet Gynecol. 1997;177:497.
68. Megibow AJ, Balthazar EJ, Cho KC, et al. Bowel obstruction: evaluation with CT. Radiology. 1991;180:313.
69. Balthazar EJ. George W. Holmes Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol. 1994;162:255.
70. Suri S, Gupta S, Sudhakar PJ, et al. Comparative evaluation of plain films, ultrasound and CT in the diagnosis of intestinal obstruction. Acta Radiol. 1999;40:422.
71. Ogata M, Imai S, Hosotani R, et al. Abdominal ultrasonography for the diagnosis of strangulation in small bowel obstruction. Br J Surg. 1994;81:421.
72. Reedy MB, Kallen B, Kuehl TJ. Laparoscopy during pregnancy: a study of five fetal outcome parameters with use of the Swedish Health Registry. Am J Obstet Gynecol. 1997;177:673.
73. Yumi H. Guidelines for diagnosis, treatment, and use of laparoscopy for surgical problems during pregnancy: this statement was reviewed and approved by the Board of Governors of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), September 2007. Surg Endosc. 2008;22:849.
74. Andreoli M, Servakov M, Meyers P, Mann WJ Jr. Laparoscopic surgery during pregnancy. JAm Assoc GynecolLaparosc. 1999;6:229.
75. Stepp K, Falcone T. Laparoscopy in the second trimester of pregnancy. Obstet Gynecol Clin North Am. 2004;31:485.