Medical Emergencies in the Pregnant Patient
Saju D. Joy and Stephen A. Contag
This chapter highlights five serious medical complications during pregnancy. These conditions affect two patients, the pregnant woman and her fetus.
The clinician’s goal is to treat the acute condition and concurrently address the possibility of pregnancy in women of childbearing age. Determining the gestational age and viability of the pregnancy is extremely important. The clinician must expeditiously evaluate and treat each of the following medical complications: pulmonary embolism (PE), asthma, diabetic ketoacidosis, thyroid storm, and seizures.PULMONARY EMBOLISM
Venous thromboembolism is five times more likely in the pregnant patient than in the nonpregnant patient due to the increase in venous stasis, changes in coagulation factors, and tissue trauma (1). Symptomatic venous thromboembolism has been shown to complicate 0.5 to 3 in 1,000 pregnancies (1,2), while PE complicates 1.3 per 10,000 pregnancies (3) and has been the leading cause of pregnancy-related deaths. During the period between 1991 and 1999, it was responsible for nearly 20% of all pregnancy-related maternal deaths in the United States (4). Recent data suggest that the frequency has decreased to approximately 10% of all pregnancy-related deaths (5). Deep venous thrombosis (DVT) occurs with equal frequency in all three trimesters; however, PE is more common during the postpartum period (1,2). The likelihood of developing a pulmonary embolus is greatly affected by the adequate treatment of DVT. If left untreated, 24% of patients with a DVT will suffer a pulmonary embolus, with a mortality rate of 15%. In patients who receive adequate therapy with anticoagulants, the risk for PE declines to approximately 5% and the mortality rate decreases to 85 mm Hg. Chest radiography and electrocardiography may also be helpful. A chest radiograph may reveal an infiltrate suggestive of pneumonia or atelectasis.
These findings, however, do not rule out the possibility of PE, and the diagnosis should be pursued whenever one has a high suspicion of embolism (8,9). The most common ECG abnormality during a pulmonary embolus is tachycardia; however, findings suggestive of acute right-heart failure may be seen including S1, Q3, T3 patterns, right bundle-branch block, P-wave pulmonale, or right axis deviation. These are more common with massive embolism than with smaller emboli, but these findings are also nonspecific (10,11).D-dimer test measures plasma levels of cross-linked fibrin formed after fibrin lysis by plasmin. This test is a nonspecific indicator of venous thrombosis, and PE is a possible diagnosis. It may be positive in patients with pregnancy, surgery, infection, cancer, trauma, and other inflammatory states and cannot guide decisions about treatment (11,12). Highly sensitive enzyme-linked immunosorbent assay (ELISA)-based D-dimer tests have sensitivity for the diagnosis of PE and DVT of 96% to 98% and a negative likelihood ratio of 0.12 that yield a high certainty for excluding DVT or PE. The sensitivity and positive likelihood values that are between 1.5 and 2.5 do not greatly increase the certainty of diagnosis because of the high frequency of false-positive results. These highly sensitive D-dimer tests can be used to rule out pulmonary embolus. The negative predictive value for these tests when used alone is not high enough to rule out PE, but they may be useful when used in conjunction with another test for PE (13,14). Troponin and brain natriuretic peptide have also been used as indirect markers of PE secondary to the development of myocardial ischemia or right ventricular overload (7).
Evidence of DVT can be used as a surrogate method for diagnosis of PE. In patients who present with acute PE, bilateral venography and compression ultrasonography detect DVT in approximately 75% and 50% of patients, respectively. Additional methods include CT venography and magnetic resonance imaging (MRI) of the lower extremities (7).
When there is a high clinical suspicion of PE, and a DVT has been detected, anticoagulation therapy should be started. A negative imaging study for DVT reduces the likelihood of PE; however, the diagnosis cannot be excluded (14).Ventilation-perfusion (V/Q) lung scanning can be used to evaluate for PE. A normal scan rules out PE but is obtained in only 25% of patients in whom the diagnosis is suspected (15). A high-probability V/Q scan is associated with a prevalence of PE of >80%, but only 45% of patients with suspected pulmonary embolus will have a high-probability scan. Patients with intermediate- or low-probability scans will require further evaluation (14).
Spiral computed tomography (CT) is becoming more widely used for detection of PE. Intraluminal filling defects in lobar or main pulmonary arteries have a positive predictive value for PE of 85%. The sensitivity for subsegmental emboli is only 30%; therefore, intraluminal defects in segmental or subsegmental pulmonary vessels require further evaluation. The combination of CT venography with CT of the pulmonary arteries increases the sensitivity for the diagnosis of PE from 85% to 90% (7). A normal spiral CT significantly reduces the likelihood of PE but does not exclude the diagnosis. Contrast-enhanced CT arteriography has advantages over V/Q scanning, including speed, characterization of nonvas- cular structures, and detection of venous thrombosis (7).
Pulmonary angiography is the gold standard for diagnosis of PE. Maternal morbidity is associated with catheterization and injection of the contrast solution at a rate of 4% to 5%. The procedure-related maternal mortality rate is 0.2% to 0.3%. Pulmonary angiography is used only when a high suspicion of PE is present, but the other less invasive diagnostic tests are inconclusive (9,10).
The fetal radiation dose with chest radiography (with asthma found no association of the disease with preterm delivery. The only significant association found was an increased risk for cesarean delivery (32).
Most studies suggest that patients receiving chronic medications for asthma, especially oral corticosteroids, have the highest risk for preterm delivery and small-for-gestational-age infants (31,33). An increased risk for preeclampsia has been noted among patients with daily symptoms or requiring theophylline (34). A lower forced expiratory volume at 1 second (FEV1) has been associated with an increased risk for low birth weight and prematurity (35). It remains unclear whether the pregnancy complications are due to the chronic medications, the severity of the disease, or both factors combined.Pharmacologic Agents
The treatment goal for the pregnant asthmatic is to obtain optimal therapy by maintaining control of her asthma thus ensuring improved maternal health and normal fetal maturation (36). The components of caring for a patient with asthma include assessment and monitoring of asthma, including objective measures of pulmonary function; control of factors contributing to asthma severity; patient education; and pharmacologic therapy using a stepwise approach (36).
Most asthma medications are safe and better than the alternative of asthma symptoms and exacerbations that may impair fetal oxygenation during pregnancy (36). Prevention of inflammation, airway hyperresponsiveness, and symptoms is the cornerstone of therapy. Stepwise therapy requires additional medications and dosages adjusted to the symptom severity. A patient not responding to any given treatment should be stepped up to the next level of therapy. Medications are categorized in two general classes: (a) long-term control medications to achieve and maintain control of persistent asthma—especially important is daily medication to suppress the inflammation that is considered an early and persistent component in the pathogenesis of asthma—and (b) quick-relief medications that are taken as needed to treat symptoms and exacerbations (36).
Inhaled Ä-agonists are recommended for the acute asthma exacerbation by relieving acute bronchospasm of any severity.
They are also the first-line medication for mild intermittent and exercise-induced asthma. They are not very effective in preventing airway hyperresponsiveness among patients with persistent asthma (37). To date, no congenital anomalies have been associated with these medications in animals or humans (38). Subcutaneous injection of selective Ä-agonists, such as terbutaline, may be used in patients with severe exacerbation who are unconscious, cannot use an inhaler, or is moving air very poorly (39). Exclusive use of short-acting Ä-agonists for management of persistent asthma is associated with an increased mortality (40). Long-acting Ä-agonists have been shown to significantly decrease the number and severity of exacerbations when used in combination with inhaled corticosteroids; however, their safety in pregnancy has not been proven (30,38).Inhaled corticosteroids are the mainstay of long-term control of persistent asthma of any severity. These medications decrease airway inflammation, thereby decreasing the number and severity of exacerbations as well as the need for additional inhaled Ä-agonist therapy. The majority of inhaled corticosteroids are pregnancy category C, with the exception of budesonide, which is now pregnancy category B. Several large studies have shown no increased risk for congenital anomalies when budesonide was used during pregnancy (36,41,42). Oral corticosteroids have been associated with orofacial clefting and intrauterine growth restriction in some trials; however, poor asthma control may lead to worse maternal and fetal complications (28,38,42,43). The main indication for oral steroids is patients not responsive to short-acting bronchodilators and inhaled corticosteroids regardless of the severity of the disease. Quick-relief medication Ä-agonists should be available to all patients with persistent asthma being treated with inhaled corticosteroids or other long-term anti-inflammatory medications (36).
Theophylline is rarely used for asthma management during pregnancy because of its side effects.
Drug levels may change dramatically during the course of pregnancy due to pregnancy-related changes in pharmacokinetics and interactions with other drugs. Serum levels must be checked regularly since theophylline has a narrow therapeutic window, and supratherapeutic drug levels can cause death (38,42). The recommended serum concentration is 5 to 12 ^g/mL. It is used as an alternative treatment for mild persistent asthma or adjunctive treatment to be used with inhaled corticosteroids in moderate to severe persistent asthma (36).Cromolyn and nedocromil are mast cell stabilizers dispensed as inhalers. They are used as an alternative to inhaled corticosteroids for therapy in mild persistent asthma. Leukotriene receptor antagonists, including zafirlukast and montelukast, may also be considered as an alternative for mild persistent asthma and as an adjunctive therapy for long-term control in moderate persistent asthma (36).
Ipratropium bromide is an inhaled anticholinergic agent and is pregnancy category B. A recent metaanalysis revealed significantly improved pulmonary function following administration of anticholinergic inhalers in combination with inhaled Ä-agonists for patients with a severe exacerbation (44).
Emergency Therapy
Treatment of an acute asthma exacerbation during pregnancy is very similar to treatment for nonpregnant patients (Fig. 1.1). Treatment of an acute exacerbation begins at home. Patients should have individualized treatment plans. Treatment begins with inhaled albuterol 2 to 4 puffs every 20 minutes for up to 1 hour (36). This is followed by inhaled or oral corticosteroids for long-term management and suppression of inflammation and hyperreactivity. For the patient that has a severe exacerbation not responsive to home therapy, rapid evaluation upon presentation is critical. Initially, airway patency should be established. The physical examination should include auscultation, heart rate and respiratory rate evaluation, and, in addition, observing if the patient is using accessory muscles. Pulse oximetry should be obtained. In the pregnant patient, supplemental oxygen should be administered to maintain the pulse oximetry value at ≥95% to assure adequate fetal oxygenation. In patients at ≥24 weeks of gestation, external fetal heart rate (FHR) monitoring should be continued until significant maternal improvement. Pulmonary function should be determined using both spirometry and FEV1 or a peak expiratory flow meter (45). Peak expiratory flow rate (PEFR) appears to be equivalent to FEV1 for determining airway constriction. Arterial blood gas testing should be considered for any patient with pulse oximetry values 50% of that predicted, an inhaled Ä-agonist should be administered every 20 minutes for 1 hour. Oral systemic corticosteroids should be added if there is no response or if the patient recently took inhaled corticosteroids. If the initial PEFR is should continue with dual inhaled therapy and intravenous systemic corticosteroids.
After 1 hour, the patient must be reassessed. A PEFR of 50% to 70% of the predicted value suggests a moderate exacerbation, and the patient should receive a short-acting inhaled Ä-agonist every 60 minutes. Systemic steroids should be initiated in all patients with a suboptimal response. The patient may continue this regimen for up to 3 hours as long as there is continued clinical improvement. A PEFR of shock may occur.
Central nervous system dysfunction is seen in up to 90% of patients with thyroid storm (56). Manifestations vary from change in mental status, restlessness, anxiety, confusion, and agitation to the extremes of delirium, disorientation, and psychosis. Tremor and proximal muscle weakness are common. Without expedient treatment, severe consequences of thyroid storm include emotional lability, seizures, obtundation, and coma (52). Gastrointestinal manifestations may result in the patient experiencing weight loss, despite an increased appetite (54). Other symptoms include diarrhea, anorexia, nausea, vomiting, and crampy abdominal pain, a constellation that mimics an acute abdomen. Occasionally, jaundice and/or tender hepatomegaly are noted.
Differential Diagnosis
Thyroid storm may be confused with other hyperkinetic states but should be suspected in any thyrotoxic patient with fever (54). A careful medication history should be obtained. The review of systems should be focused to include the above-mentioned cardiac, central nervous system, and gastrointestinal manifestations. During the physical examination, the clinician should examine the patient for a palpable goiter or eye signs suggestive of Graves’ ophthalmopathy. The differential diagnosis includes anxiety states, psychosis, drug abuse (cocaine toxicity), pheochromocytoma, heat stroke, malignant neuroleptic syndrome, acute abdomen, alcoholic complications, and sepsis.
Laboratory Evaluation
Thyroid function tests do not distinguish storm from uncomplicated thyrotoxicosis, because the values overlap (57). However, serum-free thyroxine (FT4), free triiodothyronine (FT3), and thyroid-stimulating hormone levels need to be

Management of Thyroid Storm
I. Inhibit thyroid hormone synthesis
a. Thionamide
• Propylthiouracil(PTU):—first-line agent: 600-800 mg PO, then 150-200 mg q 4-6 hr
• Methimazole: 40 mg rectally t.i.d or 15-25 mg PO q 6 hr
II. Inhibit thyroid hormone release
a. Thionamide
b. Sodium iodide: 1-2 hr post thionamide administration
• Saturated solution of potassium iodide (SSKI): 2-5 drops PO q 8 hr
• Sodium iodide: 0.5-1 g IV q 8 hr
• Lugol's solution (5% KI, 10% KI2): 8 drops q 6 hr
c. Iodide allergy: 1-2 hr post thionamide administration
• Lithium carbonate: 300 mg PO q 6 hr
III. Block peripheral effects/conversion to active hormone
a. Thionamide
b. Dexamethasone: 2 mg IV or IM q 6 hr for four doses
IV. Identify and treat precipitating factor(s)
Treat underlying hypertension, infection, or bleeding
V. General supportive/symptomatic care
a. Tachycardia
• β-Blocker: Propranolol—20-80 mg PO q 4-6 hr or 1-2 mg IV q 5 min to total of 6 mg, then 1-10 mg IV q 4 hr
• Bronchospasm history: Diltiazem—60 mg PO q 6-8 hr
b. Hyperthermia: Acetaminophen ± cooling blanket
c. Dehydration: Fluid replacement; caution for heart failure; consider central hemodynamic monitoring
d. Restlessness: Phenobarbital—30-60 mg PO q 6-8 hr as needed
• Electrolyte replacement
• Consider plasma exchange
obtained. If thyroid storm is suspected, the clinician should not await the results of these laboratory tests but proceed with empiric management.
Management
Ihr' key to successful management of thyroid storm requires supportive care, prompt identification of etiology, and quadruple therapy (thionamide, iodide, glucocorticoids, and β-blockers). These efforts to resuscitate and treat should occur in an intensive care unit. Quadruple therapy is used in (a) preventing the synthesis and the release of T4, (b) preventing the conversion of T4 → T3, and (c) blocking the actions of thyroid hormone on the cardiovascular system (24). A management protocol for thyroid storm with suggested medications is outlined in Table 1.3 (52,55).
Supportive care includes hydration with intravenous fluids andelectrolytes to replace gastrointestinal and insensible losses. Supplemental oxygen with continuous cardiac monitoring should be employed. Congestive heart failure should be treated the same as in the nonpregnant individual, but patients may be refractory to digoxin and require higher doses (57). Control of tachycardia with β-blockade may pose problems in the face of recalcitrant congestive heart failure. Alternatives to β-blockade include IM reserpine, guanethidine, and dil- tiazem. Fever should be controlled with antipyretics (acetaminophen) and, if necessary, a cooling blanket. Phenobarbital is used to reduce extreme agitation and can increase the catabolism of thyroid hormone. Aspirin is contraindicated in thyrotoxic crisis because it displaces T3 and T4 from binding proteins.
Identifying and treating precipitating factors are critical in the management of thyroid storm. A thorough search as to the cause, such as infection, trauma, labor, or pulmonary embolus, should be conducted. Broad-spectrum antibiotic coverage should be initiated early and continued until final cultures are negative, unless another precipitating cause is identified.
In pregnancy, the drug of choice for medical treatment of hyperthyroidism is propylthiouracil (PTU), rather than methimazole. PTU will block thyroid hormone synthesis by inhibiting both the organification of tyrosine residues and the peripheral conversion of T4 to T3 (58). A loading dose of 600 to 800 mg orally should be given, followed by ł5î to 200 mg orally every 4 to 6 hours (52). PTU is only available orally but can be administered via nasogastric tube. Although PTU begins to act in the 1st hour after administration, the full therapeutic effect is not achieved for 3 to 6 weeks (56). Newborns of treated mothers generally have small goiters, if one is present at all, and mild hypothyroidism, which resolves shortly after birth. Although the evidence linking methimazole to aplasia cutis in the newborn is debated, practitioners in the United States still hesitate to use the drug unless the patient cannot tolerate PTU (54) or oral administration is not possible. Methimazole does not inhibit the peripheral conversion of T4 to T3. Methimazole is administered 40 mg rectally three times a day.
Iodide treatment blocks the release of thyroid hormone and thus it is included as part of the quadruple therapy. Options include (a) a saturated solution of potassium iodide, 2 to 5 drops orally or by nasogastric tube every 8 hours;
(b) sodium iodide, 0.5 to 1.0 g every 8 hours by slow intravenous infusion;
(c) Lugol’s solution, 8 drops every 6 hours; and (d) lithium carbonate, 300mg orally every 6 hours (especially for patients allergic to iodine) (52). Iodide administration should not be initiated until 1 to 2 hours after PTU or methimazole therapy has begun, so that there is no further buildup of hormone stores (57).
Glucocorticoids decrease thyroid hormone release and inhibit peripheral tissue conversion of T4 to T3, decreasing the peripheral manifestations of thyrotoxicosis. Dexamethasone can be used at 2mg intravenously or intramuscularly every 6 hours for four doses.
Propranolol can be used to control tachycardia, tremor, and restlessness. The intravenous protocol recommends 1 to 2 mg intravenously per 5 minutes for a total of 6mg, then 1 to 10mg intravenously every 4 hours, versus the oral protocol of 20 to 80 mg orally every 4 to 6 hours. If the patient has a history of severe bronchospasm, reserpine (1 to 5mg intramuscularly every 4 to 6 hours), guanethidine (1mg∕kg orally every 12 hours), or diltiazem (60mg orally every 6 to 8 hours) may be administered (52). Plasmapheresis and peritoneal dialysis are reserved for patients for whom conservative therapy fails.
After initial clinical improvement, iodine and glucocorticoid therapy can be discontinued. Antithyroid medications should be continued until the patient is euthyroid. In general, the therapeutic goal is to maintain high to normal maternal thyroid hormone levels to minimize the potential for suppression of the fetal gland. If storm occurs early in pregnancy, a subtotal thyroidectomy can be performed in the second trimester. Use of the preceding management protocol has resulted in a decrease in mortality to the range of 10% to 20% (57). Death, however, is usually the result of cardiac failure or intercurrent infection (56).
DIABETIC KETOACIDOSIS
Diabetic ketoacidosis (DKA) complicates about 1% to 3% of all diabetic pregnancies (58-62). In one study, 30% of cases of DKA occurred in women who did not have known diabetes (63). Despite improved supportive care, DKA is still a significant cause of mortality. Although maternal mortality in DKA has been reduced from 50% in the pre-insulin era to mL of half-normal saline per hour should be given until approximately 75% of the deficit is corrected. When the serum glucose falls below 250 mg/dL, the intravenous fluids can be changed to a 5% dextrose solution (62). Six to eight liters of fluids should be replaced over the first 24 hours of treatment to compensate for approximately 75% of the estimated fluid loss. Solutions containing lactate should be avoided. Urine output must be monitored closely, continuously checking for glucose and ketones.
After initial blood studies have been done and hydration begun, insulin therapy should be started. There are many regimens for insulin replacement; one option is as follows: initially, 0.1 U/kg body weight should be given as an intravenous push; then, an intravenous drip of regular insulin is given, at 0.1 U/kg body weight per hour (equivalent to 8 to 10 units per hour). Serum glucose should be checked every 1 to 2 hours, and if a decrease of 25% or more (50 to 75 mg) is not achieved within the first 2 hours, the insulin infusion rate should be doubled (62). As mentioned previously, when the serum glucose falls below 250 mg/dL, the intravenous solution should include 5% dextrose with half-normal saline, and the insulin infusion rate should be decreased by half. When the blood glucose drops below 150 mg/dL, a basal rate of 1 to 2 U of insulin per hour should be adequate to maintain homeostasis, with the patient able to eat and return to split-dosing of subcutaneous insulin (62). The insulin drip may then be tapered over 4 to 6 hours and discontinued.
Potassium loss due to vomiting and massive osmotic diuresis is usually in the range of 5 to 10 mEq/kg body weight. Acidosis causes displacement of intracellular potassium to the extracellular space, giving the clinician spurious reassurance that potassium stores are adequate. Correcting the acidosis drives potassium back into the cell, rapidly decreasing the serum potassium level. Potassium can also be bound by ketones that are being removed by increasing diuresis. The calculated potassium deficit is 5 to 10 mEq/kg of body weight. Potassium repletion does not need to be initiated until serum concentrations are below 5.3 mEq/L. Potassium chloride, up to 40 mEq/L, should be added to the intravenous solution (half-normal saline), and the serum electrolytes should be checked every 2 to 4 hours (68). If phosphorus is low, 10 to 20mEq/L of potassium phosphate can replace 10 to 20 mEq/L of potassium chloride as long as renal function is adequate (62).
Bicarbonate replacement is somewhat controversial and should be considered only if the pH is 20 weeks’ gestation) and postpartum eclampsia are noted to be more frequent occurrences.
Essential in the diagnosis of eclampsia is the presence of a seizure concurrent with the diagnosis of preeclampsia (hypertension and proteinuria). The progression of preeclampsia leads to end-organ damage. Associated laboratory abnormalities include an elevation of the serum uric acid level, serum creatinine >1 mg/dL, blood urea nitrogen >10 mg/dL, and sometimes an elevation of the serum transaminases or depression of the platelet count. The serum alkaline phosphatase level cannot be used to assess liver function, as the placenta produces alkaline phosphatase, and this will give a misleading, elevated result. It is important to note, however, that these blood tests are not always uniformly abnormal in the eclamptic patient and that an elevated blood pressure may be the only objective sign seen in these patients. Prodromal complaints indicating severe preeclampsia include excessive weight gain in the preceding few weeks, right upper quadrant pain, visual disturbances consisting of scotomata or blurry vision, and a headache unresponsive to acetaminophen.
Idiopathic epilepsy affects 0.5% to 1.0% of the population of North America. It complicates approximately 0.3% to 0.6% of pregnancies (77). These seizures can be categorized as generalized tonic-clonic seizures, partial complex seizures that may or may not generalize, and absence seizures. While 17% to 33% of epileptic women report an increase in seizure frequency (78) during pregnancy, up to 25% report a decrease and up to 50% report no change in frequency (79). In part, the increased seizure risk is due to the pharmacokinetic changes during pregnancy (decreased protein binding, increased volume of distribution, increased renal clearance, with impaired intestinal absorption, and increased hepatic metabolism), which combine to lower the free circulatory levels of antiepileptic drugs (AED). However, patient noncompliance with anticonvulsant therapy is a more frequent reason for low circulatory levels of AED. Often, as soon as the pregnancy test is positive, gravidas stop taking their anticonvulsant medications, because of the perceived teratogenicity. Although one would expect an increase in seizure activity during the first trimester, there persists an increased risk throughout gestation with the highest incidence in the peripartum period because of the combination of noncompliance and pharmacokinetic changes (80).
Pregnancy Effects on Epilepsy
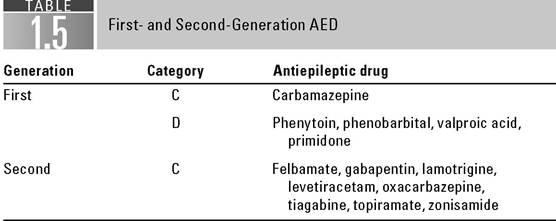
As mentioned previously, low serum concentrations of AED can accompany the increased seizure frequency seen in some pregnancies. This finding may be because of our present ability to measure levels of anticonvulsant drugs in epileptic patients. Table 1.5 lists the first- and second-generation antiepileptic medications. Pregnancy is known to change the disposition of anticonvulsant medications (81). The increase in plasma volume, the presence of fetal and placental compartments, and the increase in extracellular fluid all increase the volume of distribution of anticonvulsant medications and can lower the total serum concentration of these medicines. Free serum drug levels best represent the drug available to the central nervous system for anticonvulsant activity, therefore, only the free, unbound drug that is pharmacologically active is measured. Bardy et al. (82) measured serum phenytoin levels during pregnancy in 111 patients and concluded that they are lowest at the time of delivery. During the late third trimester and in labor, free levels of carbamazepine have been noted to fall 11%, phenytoin 31%, and phenobarbital 50% (78). Furthermore, many patients experience nausea and vomiting in the first trimester of pregnancy, which reduces the absorption of anticonvulsant drugs from the gastrointestinal tract (83). Barbiturates and phenytoin induce hepatic microsomal enzymes, which hasten their own metabolism. In addition, pregnancy increases the liver’s ability to hydroxylate these medications (81). This
is only a brief example of the many ways in which serum anticonvulsant levels can change during a normal pregnancy and why it is important to measure these drug levels in epileptic patients who are seen after a seizure. Some authors recommend checking levels each trimester and after delivery (76).
Fetal Effects of Anticonvulsant Medications
Many pregnant women become noncompliant because they are concerned about the teratogenicity associated with AED. Major malformations occur in 2% to 4% of the general population. Whereas the incidence is approximately twice as high among women with epilepsy not using any AEDs, among epileptics on monotherapy, it is 4% to 6% (84). Major congenital malformations associated with AEDs include heart defects, neural tube defects including anencephaly, and cleft lip and palate. Certain abnormalities have been associated with the specific medications. Barbiturate use is associated with facial clefts and congenital heart disease. Carbamazepine and valproic acid use in the first trimester is associated with neural tube defects of 20 weeks’ gestation. In this situation, the clinician should have a high suspicion of eclampsia in the presence of hypertension and proteinuria. These patients should be treated as if they are eclamptic until further studies and history can be obtained.
There are several steps in managing a pregnant patient with a seizure. The ABCs for resuscitation should be followed. First, an adequate airway must be maintained to allow oxygenation after the patient’s respirations resume, following the convulsion. Breathing and circulation need to be assessed after the convulsion ceases. During the seizure, it is necessary to prevent self-injury and uterine (fetal) trauma. After the seizure, the airway should be cleared and the patient should be suctioned to reduce the risk of aspiration of secretions or vomitus. She should also be watched carefully to prevent bodily injury, lacerations, and fractures (85,88). If seizures persist, the airway must be protected, possibly requiring intubation.
If an eclamptic seizure is the working diagnosis, the patient should be treated with intravenous magnesium sulfate, if possible. The usual initial dose is 6g, administered intravenously and slowly, over 1 to 2 minutes. If intravenous access is not available, 10 g may be administered intramuscularly. Overdoses of magnesium can lead to respiratory depression, and inadequate doses can result in continued seizures. If seizures continue, another 2 g of magnesium sulfate may be given intravenously. After controlling the eclamptic seizure, a maintenance dose of 2 g per hour should be administered. Renal function should be evaluated (magnesium is cleared renally) and a Foley catheter placed. Magnesium toxicity progresses from loss of deep tendon reflexes to ECG variations to apnea and cardiac arrest, because of electrical-mechanical disassociation. Calcium gluconate 1 g IV (1 ampule) may be administered to reverse magnesium toxicity.
If the patient has a history of epilepsy, she should be treated with the parenteral form of the medication she has been taking. If the etiology of the seizures is uncertain, phenytoin may be used for acute treatment. The usual loading dose is 10 to 15 mg/kg prepregnancy weight, given intravenously over an hour. The infusion is started at a rate of up to 50 mg per minute to a total dose of 20 mg/kg. Phospheny- toin may also be administered, in place of phenytoin, at a rate of 150 mg per minute in cases of status epilepticus. The patient should be placed on a cardiac monitor while phenytoin or phosphenytoin is being administered. Subsequently, the patient should be given 200 mg either orally or intravenously, beginning 12 hours after the bolus. This dosage regimen also has been used successfully to treat eclampsia (88).
Diazepam and the other benzodiazepines are considered first-line treatments for status epilepticus. They can be used to treat seizures acutely until the patient can be transported to a labor floor and treated appropriately for eclampsia. Lorazepam at a dose of 4 mg IV can be given slowly over 2 to 5 minutes, which may be repeated in 10 to 15 minutes; usual maximum dose is 8 mg. Alternatively, diazepam can be administered at 0.1 to 0.3 mg/kg intravenously, with termination of seizures within 20 seconds of administration. However, because of subsequent redistribution of the drug into adipose tissue, the duration of diazepam’s acute anticonvulsant effect is typically Dombrowski MP. Asthma and pregnancy. Obstet Gynecol. 2006;108(3, pt 1):667-681.
29. Schatz M, Dombrowski MP, Wise R, et al. Asthma morbidity during pregnancy can be predicted by severity classification. JAllergy Clin Immunol. 2003;112(2):283-288.
30. National Asthma Education and Prevention Program. Expert panel report: guidelines for the diagnosis and management of asthma update on selected topics. JAllergy Clin Immunol. 2002;110(5 Suppl.):13-29.
31. Bracken MB, Triche EW, Belanger K, et al. Asthma symptoms, severity, and drug therapy: a prospective study of effects on 2205 pregnancies. Obstet Gynecol 2003;102(4):739-752.
32. Dombrowski MP, Schatz M, Wise R, et al. Asthma during pregnancy. Obstet Gynecol. 2004;103(1):5-12.
33. Schatz M, Dombrowski MP, Wise R, et al. The relationship of asthma medication use to perinatal outcomes. JAllergy Clin Immunol. 2004;113:1040-1045.
34. Triche EW, Saftlas AF, Belanger K, Leaderer BP, Bracken MB. Association of asthma diagnosis, severity, symptoms, and treatment with risk of preeclampsia. Obstet Gynecol. 2004;104: 585-593.
35. Schatz M, Dombrowski MP, Wise R, et al. Spirometry is related to perinatal outcomes in pregnant women with asthma. Am J Obstet Gynecol. 2006;194:120-126.
36. U.S. Department of Health and Human Services. National Institutes of Health National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Working Group Report on Managing Asthma during Pregnancy: Recommendations for Pharmacologic Treatment, Update 2004. NIH Publication No. 05-5236, March 2005. Available at: http://www.nhlbi.nih.gov/ health/prof/lung/ asthma/astpreg.htm. Retrieved November 20, 2008.
37. Cockcroft DW, Murdock KY. Comparative effects of inhaled salbutamol, sodium cromoglycate, and beclomethasone dipropionate on allergen-induced early asthmatic responses, late asthmatic responses, and increased bronchial responsiveness to histamine. JAllergy Clin Immunol 1987;79:734-740.
38. Demoly P, Piette V, Daures J-P. Asthma therapy during pregnancy. Expert Opin Pharmacother. 2003;4(7):1019-1023.
39. Papiris S, Kotanidou A, Katerina M, Rousos C. Clinical review: severe asthma. Crit Care. 2002;6(1):30-44.
40. Spitzer WO, Suissa S, Ernst P, et al. The use of beta-agonists and the risk of death and near death from asthma. N EnglJMed. 1992;326:501-506.
41. Kallen B, Rydhstroem H, Aberg A. Congenital malformations after the use of inhaled budesonide in early pregnancy. Obstet Gynecol. 1999;93:392-395.
42. Liccardi G, Cazzola M, Canonica GW, et al. General strategy for the management of bronchial asthma in pregnancy. Respir Med. 2003;97(7):778-789.
43. Park-Wyllie L, Mazzotta P, Pastuszak A, et al. Birth defects after maternal exposure to corticosteroids: prospective cohort study and meta-analysis of epidemiological studies. Teratology. 2000;62:385-392.
44. Rodrigo G, Rodrigo C, Burschtin O. A meta-analysis of the effects of ipratropium bromide in adults with acute asthma. Am JMed. 1999;107(4):363-370.
45. National Asthma Education and Prevention Program. Practical Guide for the Diagnosis andManagement of Asthma. Publication 97-4053. Bethesda, MD: National Heart, Lung, and Blood Institute of the National Institutes of Health; 1997.
46. Adams BK, Cydulka RK. Asthma evaluation and management. Emerg Med Clin North Am. 2003;21(2):315-330.
47. Allan WC, HaddowJE, Palomaki GE, et al. Maternal thyroid deficiency and pregnancy complications: implications for population screening. JMed Screen. 2000;7:127-130.
48. Fernandez-Soto ML, Jovanovic LG, Gonzalez-Jimenez A, et al. Thyroid function during pregnancy and the postpartum period: iodine metabolism and disease states. Endocr Pract. 1998;4(2):97-105.
49. Ecker JL, Musci TJ. Treatment of thyroid disease in pregnancy. Obstet Gynecol Clin North Am. 1997;24(3):575-589.
50. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicatingpregnancy. Am J Obstet Gynecol. 1989;160(1):63-70.
51. Tietgens ST, Leinung MC. Thyroid storm. Med Clin North Am. 1995;79(1):169-184.
52. ACOG. Thyroid Disease in Pregnancy. ACOG Technical Bulletin 37. Washington, DC: American College of Obstetricians and Gynecologists, 2002.
53. Hershman JM. Human chorionic gonadotropin and the thyroid: hyperemesis gravidarum and trophoblastic tumors. Thyroid. 1999;9(7):653-657.
54. Mestman JH. Diagnosis and management of maternal and fetal thyroid disorders. Curr Opin Obstet Gynecol. 1999;11:167-175.
55. Calhoun BC, Brost B. Emergency management of sudden puerperal fever. Obstet Gynecol Clin North Am. 1995;22:357-367.
56. Mestman JH. Hyperthyroidism in pregnancy. Clin Obstet Gynecol. 1997;40:45-64.
57. Mestman J. Severe hyperthyroidism in pregnancy. In: Clark SL, Phelan JP, Cotton DB, eds. Critical Care Obstetrics. Oradell, NJ: Medical Economics Books; 1987:262.
58. Gittoes NJ, Franklyn JA. Hyperthyroidism: current treatment guidelines. Drugs. 1998;55:543-553.
59. Kilvert J, Nicholson HO, Wright AD. Ketoacidosis in diabetic pregnancy. Diabet Med. 1993;10:278-281.
60. Cullen MT, Reece EA, Homko CJ, et al. The changing presentations of diabetic ketoacidosis during pregnancy. Am J Perinatol. 1996;13:449-451.
61. Schneider M, Umpierrez GE, Ramsey RD, et al. Pregnancy complicated by diabetic ketoacidosis: maternal and fetal outcomes. Diabetes Care. 2003;26:958-959.
62. Ramin KD. Diabetic ketoacidosis in pregnancy. Obstet Gynecol Clin North Am. 1999;26:481-488.
63. Montoro MN, Myers VP, Mestman JH, et al. Outcome of pregnancy in diabetic ketoacidosis. Am J Perinatol. 1993;10:17-20.
64. Gabbe SG, Mestman JH, Hibbard LT. Maternal mortality in diabetes mellitus: a 1-year survey. Obstet Gynecol. 1976;48(5):549-551.
65. Schneider MB, Umpierrez GE, Ramsey RD, Mabie WC, Bennett KA. Pregnancy complicated by diabetic ketoacidosis. Diabetes Care. 2003;26(3):958-959.
66. Kent LA, Gill GV, Williams G. Mortality and outcome of patients with brittle diabetes and recurrent acidosis. Lancet. 1994;344:778-781.
67. Parker JA, Conway DL. Diabetic ketoacidosis in pregnancy. Obstet Gynecol Clin North Am. 2007;34(3):533-543.
68. Brumfield CG, HuddlestonJF. The management of diabetic ketoacidosis in pregnancy. Clin Obstet Gynecol. 1984;27:50-59.
69. Pitteloud N, Binz K, Caulfield A, et al. Ketoacidosis during gestational diabetes: case report. Diabetes Care. 1998;21:1031-1032.
70. Metzgar BE, Coustan DR. Summary and recommendations of the Fourth International Workshop-Conference on Gestational Diabetes. Diabetes Care. 1998;21:B161- B167.
71. Tibaldi JM, Lorber DL, Nerenberger A. Diabetic ketoacidosis and insulin resistance with subcutaneous terbutaline infusion: a case report. Am J Obstet Gynecol. 1990;163:509-510.
72. Bernstein IM, Catalano PM. Ketoacidosis in pregnancy associated with the parenteral administration of terbutaline and betamethasone: a case report. J Reprod Med. 1990;35:818-820.
73. Hollingsworth DR. Medical and obstetric complications of diabetic pregnancies: IDDM, NIDDM, and GDM. In: Brown C-L, Mitchell C, eds. Pregnancy, Diabetes and Birth: A Management Guide. 2nd Ed. Baltimore, MD: Williams & Wilkins; 1992.
74. Cullen MT, Reece EA, Homko CJ, Sivan E. The changing presentations of diabetic ketoacidosis during pregnancy. Am JPerinatol. 1996;13:449-451.
75. Stecker MM. Management of status epilepticus. UpToDate (electronic journal), October 24, 2002.
76. Beach RL, Kaplan PW. Seizures in pregnancy: diagnosis and management. Int Rev Neurobiol. 2008;83:259-271.
77. ACOG. Seizure Disorders in Pregnancy. ACOG Educational Bulletin 231. Washington, DC: American College of Obstetricians and Gynecologists; 1996.
78. Shuster EA. Seizures in pregnancy. EmergMed Clin North Am. 1994;12(4):1013-1025.
79. Treiman DM. Current treatment strategies in selected situations in epilepsy. Epilepsia. 1993;34(Suppl. 5):s17-s23.
80. EURAP Study Group. Seizure control and treatment in pregnancy: observations from the EURAP epilepsy pregnancy registry. Neurology. 2006;66(3):354-360.
81. Nulman I, Laslo D, Koren G. Treatment of epilepsy in pregnancy. Drugs. 1999;57: 535-544.
82. Bardy AH, Hiilesmaa VlI, Teramo KA. Serum phenytoin during pregnancy, labor and puerperium. Acta Neurol Scand. 1987;75:374-375.
83. Ramsay RE, Strauss RG, Wilder J, Wilmore U. Status epilepticus in pregnancy: effect of phenytoin malabsorption on seizure control. Neurology. 1978;28:85-89.
84. McAuleyJW, Anderson GD. Treatment of epilepsy in women of reproductive age. Clin Pharmacokinet. 2002;41(8):559-579.
85. Gedekoh RH, Hayashi TF, McDonald HM. Eclampsia at Magee-Womens Hospital, 1970-1980. Am J Obstet Gynecol. 1981;140(8):860-866.
86. Harden CL. Antiepileptic drug teratogenesis: what are the risks for congenital malformations and adverse cognitive outcomes? IntRevNeurobiol. 2008;83:205-213.
87. Pennell PB. Antiepileptic drug pharmacokinetics during pregnancy and lactation. Neurology. 2003;61(6 Suppl. 2):S35-S42.
88. Morrell MJ. Guidelines for the care of women with epilepsy. Neurology. 1998;51(Suppl. 4): S21-S27.