21 Alloimmunization
Berendena I. M. Vander Tuig
Karin J. Blakemore
Alloimmunization in pregnancy refers to maternal antibody formation against fetal red blood cell (RBC) or platelet antigens. Antibody-coated erythrocytes or platelets are destroyed by the fetal immune system, leading to fetal anemia or thrombocytopenia.
Antibodies are formed after uncrossmatched transfusion or fetomaternal hemorrhage (FMH), when foreign or fetal blood components enter the maternal circulation. Untreated alloimmunization can cause significant fetal and newborn morbidity and mortality from hemolytic anemia (hydrops fetalis) or neonatal alloimmune thrombocytopenia.RED CELL ALLOIMMUNIZATION
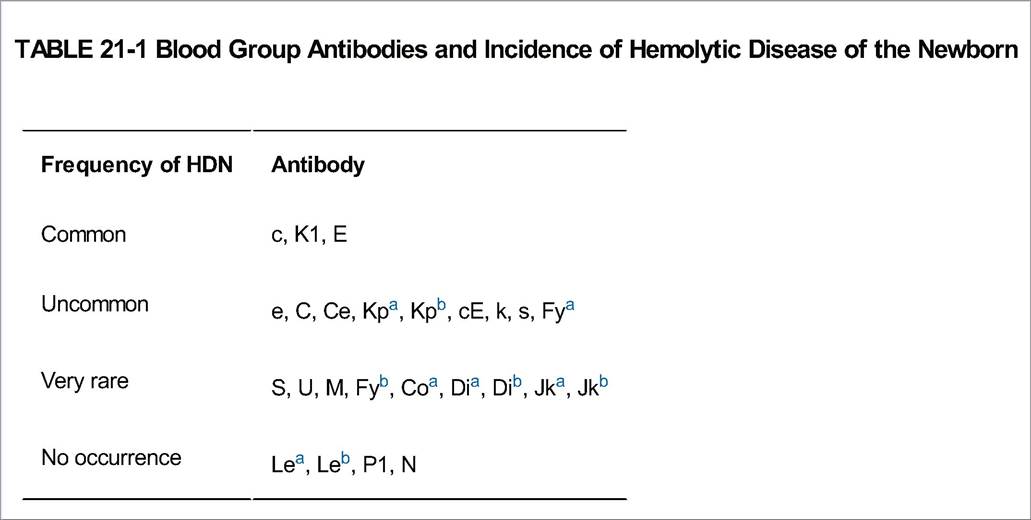
Red cell alloimmunization to clinically significant antigens occurs in approximately 25 of 10,000 births. The most common of these antigens is the Rhesus “D” (or Rh D) antigen. Maternal blood type is usually described as ABO+ or ABO-, signifying the presence (+) or absence (—) of the Rh D antigen. The Rhesus system also includes the antigens C, c, E, and e. Other important red cell antigens are the ABO blood group antigens and more than 50 other minor antigens. Only some of these are associated with red cell alloimmunization (Table 211).
P.268
Rh D Alloimmunization
Pathophysiology
• Prevalence of Rh D blood type varies by ethnicity. Fifteen percent of Caucasians and 8% of African Americans and Hispanic Americans are Rh-. The populations with the highest and lowest Rh- prevalence respectively are Spanish Basque (30%) and Native Americans (1%).
• Exposing an Rh- woman to Rh D antigen initiates an immune response that produces anti-D immunoglobulin (Ig) M and IgG and results in memory B cells that produce IgG upon reexposure to the antigen.
This process is termed Rh sensitization.• During pregnancy, the RBCs of an Rh+ fetus are targeted by maternal IgG, which can cross the placenta. Fetal anemia develops as Rh+ fetal RBCs are sequestered and hemolyzed.
• The fetal response to anemia includes increased erythropoietin production and hematopoiesis. As hemolysis outpaces production, more immature RBCs appear in the fetal circulation, a condition known as erythroblastosis fetalis. Extramedullary hematopoiesis may occur.
• If the anemia is left untreated, hydrops fetalis develops. The pathophysiology is not completely understood but is thought to involve heart failure due to anemia, portal hypertension from extramedullary hematopoiesis in the liver, and reduced hepatic protein synthesis leading to hypoalbuminemia.
• FMH with transplacental passage of Rh+ fetal erythrocytes into the maternal circulation is the main cause of Rh sensitization. See Table 21-1 for causes of FMH.
• An immune response can be generated with as little as 20 μL of blood or possibly even less.
• FMH is most likely to occur at delivery. Cesarean delivery, multifetal delivery, abruption, bleeding previa, or manual placental delivery may increase the quantity of FMH.
• Fetal RBC antigens are present by 38 days of gestation, so even first-trimester events such as ectopic pregnancy, spontaneous or elective abortion, or threatened abortion can theoretically cause alloimmunization.
• Invasive prenatal diagnostic procedures such as chorionic villus sampling, amniocentesis, or fetal blood sampling and external cephalic version can lead to FMH and alloimmunization.
• Maternal trauma can also cause FMH and alloimmunization.
P.269
Prevention
• Injectable anti-D Ig (RhoGAM) was developed in the 1960s as a means to prevent Rh D alloimmunization.
It is made from pooled sterile human IgG antibodies to the Rh D antigen.
• Before RhoGAM's development, 17% of all Rh- women carrying an Rh+ fetus developed antibodies during their first incompatible pregnancy.
• Now, with routine screening and use of RhoGAM, only 0.1% to 0.2% of pregnancies in Rh- mothers are complicated by anti-Rh D antibody production.
• RhoGAM prevents alloimmunization by binding to any fetal RBCs that enter the maternal circulation. The fetal cells are then cleared by the mother's immune system. Maternal B-cell immune response is not initiated, so no memory response develops.
• In the United States, RhoGAM is routinely administered to Rh- women at 28 weeks' estimated gestational age (EGA) and again postpartum if neonatal Rh+ status is confirmed.
• The standard RhoGAM dose for routine prophylaxis is 300 μg intramuscularly (IM).
• “Mini-dose” RhoGAM (50 μg) IM is sufficient in the first trimester as the fetus' circulating volume is smaller.
• Ten micrograms of RhoGAM IgG “neutralizes” 1 mL of fetal blood. Therefore, the standard dose protects against up to 30 mL of fetal blood entering the maternal system. After an event likely to cause FMH, quantification of FMH with a Kleihauer-Betke (KB) test guides additional RhoGAM dosing.
• The half-life of RhoGAM is 24 days but it can be detected on maternal antibody screens for up to 12 weeks.
Management of Rh-Unsensitized Patients
• Pregnant patients are screened for antibodies by indirect Coombs test, in which maternal serum is exposed to Rh+ red cells.
• Lack of agglutination signifies the absence of circulating antibody in maternal serum and suggests unsensitized status (Table 21-2).
P.270
• If the indirect Coombs test is positive (i.e., agglutination occurs), the laboratory must distinguish between sensitization and RhoGAM administration earlier in pregnancy.
• Rh- pregnant patients should be screened at the first prenatal visit. If unsensitized, no intervention is required at that time. If sensitized, see “Management of Rh-Sensitized Patients.”
• The antibody screen may be repeated at 28 weeks of EGA.
If the screen is negative, the standard dose of 300 μg of RhoGAM is administered. If the patient is sensitized, see “Management of Rh-Sensitized Patients.”• At the time of delivery, both the patient and infant are screened.
• If the neonate is Rh-, no RhoGAM is necessary.
• If the neonate is Rh+ and the mother is antibody negative, the standard dose of RhoGAM is given and a KB test is performed to evaluate the need for additional RhoGAM.
• If the neonate is Rh+ and the mother is antibody positive, no RhoGAM is given and the mother's next pregnancy is managed as Rh sensitized.
• When in question, RhoGAM is given. The risk of giving RhoGAM to a sensitized person is negligible compared with the consequences of permanent sensitization.
TABLE 21-2 Indications for RhoGAM Administration in Rh-, Unsensitized Women with Negative Antibody Screen
First-trimester spontaneous or elective abortion
Threatened abortiona
Ectopic pregnancy
Amniocentesis, fetal blood sampling, or chorionic villus sampling
Second-trimester or third-trimester bleeding (e.g., placenta previa or abruption)
Abdominal trauma
Intrauterine fetal demise
Routine prophylaxis at approximately 28 weeks' EGA
External cephalic version
Birth of an Rh+ infant
aUse is recommended in the United States, but evidence is limited. RhoGAM is not given to Rh+ or sensitized Rh- women.
EGA, estimated gestational age.
Management of Rh-Sensitized Patients
• An Rh- patient with anti-D titer > 1:4 should be considered sensitized.
• Accurate gestational dating is critical for the interpretation of other tests and the timing of interventions.
• If paternity is absolutely certain, paternal blood typing is performed to determine whether the fetus can inherit the Rh D antigen. Paternal zygosity for RHD was previously determined by testing the father for products of the closely linked RHC/E gene and calculating the probability of heterozygosity from population data.
Although this is still used, now quantitative polymerase chain reaction (PCR) techniques are available.î If the father is heterozygous for Rh D, the fetus has a 50% chance of being Rh+.
î If the father is homozygous for Rh D, the fetus will be Rh+ and is at risk.
î If the father is Rh-, no further testing is indicated.
î If paternity is unknown or testing is not possible, the fetus is assumed to be Rh+.
• Follow serial maternal D antibody titers monthly until 24 weeks, then every 2 to 4 weeks.
î Most Rh-sensitized patients have a chronic low D antibody titer. The fetus is not at risk of anemia until a critical titer is reached.
î The critical titer varies by laboratory but is usually between 1:8 and 1:16. An increase of more than one titer dilution (e.g., 1:2 to 1:8) is also considered concerning. The tests should be performed in the same laboratory.
î The titer represents the maximum dilution that produces a positive Coombs result. A titer of 1:8 would represent 1 part serum to 8 parts diluent. Note that some labs report titers as the denominator only (i.e., titer of 1:2 is reported as “2”).
î Once maternal antibodies exceed the critical titer, the fetus is at risk for the remainder of the pregnancy regardless of subsequent titer values.
î In the first affected pregnancy, titers correlate well with fetal status. In subsequent pregnancies, the titer may be less predictive.
P.271
• If the critical titer is reached and the paternal genotype is unknown or heterozygous, fetal antigen status is determined by amniocentesis or free fetal DNA testing.
î Amniocentesis
î Fetal blood genotype is determined from amniocyte by PCR. The falsenegative rate is up to 1.5%.
î Both maternal and paternal blood samples should be sent along with the amniotic fluid.
î Transplacental amniocentesis should be avoided whenever possible to avoid FMH that can worsen the alloimmunization.
î If the results suggest that the fetus is Rh+, the maternal sample is checked for the Rh pseudogene.
Some people, particularly of African descent, are phenotypically Rh- but have some portions of the RHD gene. If these sequences are passed on to the fetus, amniocyte analysis may falsely identify the fetus as Rh+.î If the results suggest that the fetus is Rh-, the paternal sample should be analyzed by PCR. Occasionally, spontaneous gene rearrangement results in a fetus mistakenly labeled as Rh-, when in fact, it did inherit the paternal D antigen.
î If the results suggest that the fetus is Rh- and a paternal sample is unavailable, the maternal titer is repeated in 4 to 6 weeks. If it remains stable, the fetus is likely Rh-. A rise in the titer should raise suspicion that the fetus is actually Rh+ and the pregnancy should be managed accordingly.
î Cell-free fetal DNA
î Fetal DNA can be found in the maternal circulation as early as 38 days of gestation.
î Cell-free fetal DNA has already been employed as a diagnostic tool for fetal red cell typing, mostly in Europe.
î A maternal blood sample is obtained and reverse transcriptase PCR is used to amplify RHD exons. These exons would not be found in the blood of an Rh- mother.
• If the results suggest that the fetus is Rh D+, the result is considered conclusive.
• If the exons are not found, the presence of fetal DNA must be confirmed.
• If gene products of the Y chromosome are found, it is an indicator that the fetus is male and the Rh- result is conclusive.
• If Y chromosome products are not found, then single nucleotide polymorphism (SNP) analysis must be performed. If >6 of the 92 analyzed SNPs are found to differ between maternal and presumed fetal DNA, then it is assumed that the fetus is female and the Rh- result is conclusive.
• If six or fewer of the analyzed SNPs differ, the result is inconclusive. The test may be repeated in 4 to 6 weeks or amniocentesis may be used to determine fetal antigen status.
• Follow middle cerebral artery (MCA) Doppler as a noninvasive alternative to amniocentesis to track fetal anemia. Most centers follow Doppler every 1 to 2 weeks to detect evolving anemia. Doppler testing may begin as early as 16 to 18 weeks' EGA.
î Blood viscosity is decreased in severe anemia, so the peak systolic velocity of blood in the MCA is increased. Additionally, the anemic fetus preferentially shunts blood to the brain, a phenomenon known as “brain sparing,” which may also contribute to increased velocity.
P.272 î A peak systolic velocity >1.5 multiples of the median (MoM) suggests clinically significant anemia.
î MCA Doppler testing is 88% sensitive and 87% specific. The positive predictive value is 53%, and the negative predictive value is 98%.
î MCA Doppler must be performed in centers with trained, experienced personnel.
î Reliability of MCA Doppler decreases after 35 weeks and after fetal blood transfusion.
• Amniocentesis may also be used to follow fetal anemia. In 1961, Liley demonstrated that amniotic fluid bilirubin levels due to fetal hemolysis are directly proportional to the spectrophotometric absorbance at 450 nm (ΔOD450). This measure correlates well with fetal status. Most centers begin serial amniocentesis at 24 to 26 weeks. ΔOD450 trends are more reliable than a single value, so serial amniocenteses should be plotted.
î The Liley curve has three prognostic zones (Fig. 21-1):
î Zone 1: The fetus is unaffected or only mildly affected; repeat amniocentesis may be performed, usually in 10 to 14 days.
î Zone 2: The fetus has mild-to-moderate hemolysis. A value in upper zone 2 (>80%) is an indication for fetal blood sampling. A value in the lower zone (fetal alloimmune thrombocytopenia (FAIT) or fetomaternal alloimmune thrombocytopenia (FMAIT). The overall incidence of NAIT is 1 to 2:1,000 deliveries, although this varies by ethnicity. Over 15 platelet antigens have been identified to date, with varying severity of disease. Antibodies to platelet antigen HPA-1a (PLA-1) are implicated in 80% of all NAIT cases and 90% of severe cases.
Pathophysiology
• The sensitizing process is similar to RBC alloimmunization.
• Antibody-mediated destruction of fetal platelets in the most severe cases can result in fetal intracranial hemorrhage (ICH) or visceral hemorrhage.
• The same alloantigens are found as endothelial cell surface antigens; it is possible that hemorrhage may be exacerbated by immune-mediated damage to the lining of fetal capillaries.
• Maternal antibody transfer can occur as early as the first trimester.
• The fetus of the primary sensitizing pregnancy can develop serious NAIT sequelae.
• Ten percent to 20% of fetuses with NAIT have ICH. Twenty-five percent to 50% of those can be detected in utero by ultrasound. Fetal death in utero occurs in approximately 14% of cases.
Diagnosis of Neonatal Alloimmune Thrombocytopenia
• Diagnostic workup is prompted by clinical suspicion. There is currently no routine screening test for NAIT.
• NAIT evaluation may be initiated for any the following: sonographic detection of in utero fetal hemorrhage, neonatal thrombocytopenia after delivery, or a prior pregnancy affected by NAIT or by fetal hemorrhage. Workup should also be initiated if the mother has a sister whose pregnancy was complicated by NAIT and who is HPA-1a negative.
• The NAIT workup begins with maternal antiplatelet antibody testing. If antigenspecific antibodies are present in maternal blood, then both maternal and paternal platelet genotyping are performed to assess for discordant antigens. Even if antigenspecific antiplatelet antibodies are not present in maternal blood, however, paternal platelet genotype discordance helps to confirm the NAIT diagnosis. Antiplatelet antibodies are not always present or may be only intermittently present.
• If the paternal genotype is heterozygous for a platelet-specific antigen that the maternal genotype lacks, there is a 50% probability (for each discordant antigen) that the fetus is at risk for NAIT. Platelet genotyping from fetal blood or amniotic fluid should be performed.
• If the paternal genotype is homozygous for a platelet-specific antigen that the maternal genotype lacks, then all pregnancies are at risk.
If the maternal and paternal genotypes are the same, the risk of an affected pregnancy is very low.
P.275
• The differential diagnosis for fetal/neonatal thrombocytopenia includes idiopathic thrombocytopenic purpura (ITP). In ITP, maternal platelets are also affected and mothers are thrombocytopenic.
Management of Neonatal Alloimmune Thrombocytopenia
• Management of pregnancies at risk for NAIT varies among centers. There is no consensus on optimal treatment.
• Maternal antibody titers are not useful and do not guide treatment.
• IVIG with or without corticosteroids is currently the best noninvasive therapy. Corticosteroids are usually reserved for persistent fetal thrombocytopenia despite IVIG treatment. In cases with a history of severe neonatal thrombocytopenia in a previous child, whether or not the child had suffered an ICH, weekly maternal IVIG may be initiated at 12 weeks' EGA and continued throughout the pregnancy.
• Fetal blood sampling is the only way to determine fetal platelet count in pregnancies at risk for NAIT. If a patient had a prior pregnancy that was severely affected by NAIT, she can be offered fetal blood sampling at 22 and 28 weeks or later. Antigen-screened platelets can be transfused for severe fetal thrombocytopenia. Cordocentesis or intrahepatic vein (IHV) blood sampling may be used. The IHV site is preferred, as there is a decreased risk of continued bleeding from the sampling site. Furthermore, IHV sampling may avoid the placenta and cause less FMH than cordocentesis, thereby reducing the risk of further sensitization.
î For possible coincident anemia or acute procedure-related hemorrhage, RBC product is also made available during fetal blood sampling.
î If fetal thrombocytopenia is severe, weekly transfusions may be required until delivery due to the short half-life of transfused platelets.
î Fetal sonographic assessment for growth and for any evidence of intrafetal hemorrhage is generally performed.
• Vaginal delivery is recommended unless otherwise contraindicated. There is no benefit to cesarean delivery except for the usual obstetric indications. The timing is individualized and is related to fetal status. In severe cases, many centers confirm fetal platelet count before delivery and transfuse as needed prior to induction. At the time of delivery, a complete blood count is obtained on the cord blood.
• After delivery, neonatal platelet counts reach a nadir within the first few days after birth and gradually improve over weeks as maternal antiplatelet antibodies resolve.
• Term infants with platelets Accessed March 26, 2012.
Peterson JA, McFarland JG, Curtis BR, et al. Neonatal alloimmune thrombocytopenia: pathogenesis, diagnosis and management. Brit J Haematol 2013; 161(1):3-14
Risson DC, Davies MW, Williams BA. Review of neonatal alloimmune thrombocytopenia. J Paediatr Child Health 2012;48(9):816-822.