20 Hematologic Disorders of Pregnancy
Nina Resetkova
Linda M. Szymanski
ANEMIA
• The Centers for Disease Control and Prevention’s definition of anemia in pregnancy is hemoglobin (Hgb) or hematocrit (Hct) value less than the fifth percentile in a healthy reference population at the same stage of pregnancy.
• Typical values include Hgb < 11.0 g/dL in the first and third trimesters and can be associated with severe pain, fever, organ dysfunction, and tissue necrosis. Vaso-occlusive crises may be triggered by infection, hypoxia, acidosis, dehydration, or psychological stress. A serious complication is acute chest syndrome, one of the leading causes of hospitalization and death in patients with SCD. Acute chest syndrome is characterized by a combination of respiratory symptoms, new lung infiltrates, and fever.
• Diagnosis: The anemia is normocytic, normochromic with an Hgb concentration of 6 to 10 g/dL and Hct of 18% to 30%. The reticulocyte count is increased to 3% to 15%. Lactate dehydrogenase is elevated, and haptoglobin is decreased. The peripheral blood smear may show sickle cells, target cells, and Howell-Jolly bodies. Diagnosis is confirmed by Hgb electrophoresis, which typically shows 85% to 100% HbS, absent HbA, normal HbA2, and moderately elevated HbF (usually < 15%). Jaundice may result from red blood cell
destruction, leading to unconjugated hyperbilirubinemia.
• Treatment: Hydroxyurea may be used to reduce intracellular sickling but is not recommended in pregnancy because it is teratogenic in animal studies. Infections are treated aggressively with antibiotics. Severe anemia is treated with blood transfusion. Pain crises are managed with oxygen, hydration, and analgesia. Controversy surrounds prophylactic exchange transfusion and is reserved for the most severe cases. Additionally,
P.252 the risks involved with transfusions must be taken into account.
Advantages of transfusion are an increase in HbA level, which improves oxygen-carrying capacity and a decrease in HbS-carrying erythrocytes. If a transfusion is given, leukocyte-depleted packed red cells, phenotyped for major and minor antigens, should be used.• Pregnancy considerations: Patients with SCD are at increased risk for sickling during pregnancy because of increased metabolic requirements, vascular stasis, and a relative hypercoagulable state. Complications during pregnancy in women with SCD include an increased risk of spontaneous abortion, intrauterine growth restriction (IUGR), fetal death in utero, low birth weight, preeclampsia, and premature birth. Women with SCD also experience greater risk of urinary tract infection (UTI), bacteriuria, pulmonary infections and infarction, and, possibly, more painful crises. Due to elevated risk of UTI, a urine culture should be evaluated at minimum in every trimester and treated correspondingly. Women with SCD should receive the pneumococcal vaccine before pregnancy and folate supplementation of 1 to 4 mg/day. Iron supplements should be prescribed only if iron is deficient. The intensity of fetal surveillance varies according to the clinical severity of the disease. In severe cases, twice weekly assessment of fetal wellbeing should begin at 32 weeks' gestation, and monthly sonography should be performed to evaluate fetal growth. All African American patients should undergo an Hgb electrophoresis to assess carrier status. If both the patient and the father of the baby are found to be hemoglobinopathy carriers, genetic counseling is indicated. Amniocentesis or chorionic villus sampling (CVS) may be offered for prenatal diagnosis. After delivery, patients should practice early ambulation and wear thromboembolic deterrent stockings to prevent thromboembolism.
• Regarding contraception, the levonorgestrel-containing intrauterine device (IUD) and progestin-only implants are considered excellent contraceptive options for patients with SCD.
No well-controlled studies have evaluated oral contraceptives in SCD; however, low-dose combined contraceptives appear to be a good choice in some women with SCD. The benefits of copper-containing IUDs are debated due to a potential for increased blood loss but copper-containing IUDs are generally considered a safe and effective method of contraception for women with SCD. Progestin-only pills, depot medroxyprogesterone, and barrier devices are also safe for contraception. Medroxyprogesterone acetate (Depo Provera) injections may decrease the number of pain crises.Sickle Trait
• Sickle cell trait (HbAS) is common in African Americans (1 in 12, or 8%) and is also prevalent in persons of Mediterranean, Middle Eastern, Indian, Caribbean, and Central and South American descents. Women with sickle cell trait have approximately twice the frequency of UTIs compared to the general population, especially during pregnancy, and should be screened each trimester. No direct fetal compromise exists from maternal sickle cell trait. Partners should be screened because the risk of having a child with SCD becomes one in four if the father is also a carrier.
Thalassemias
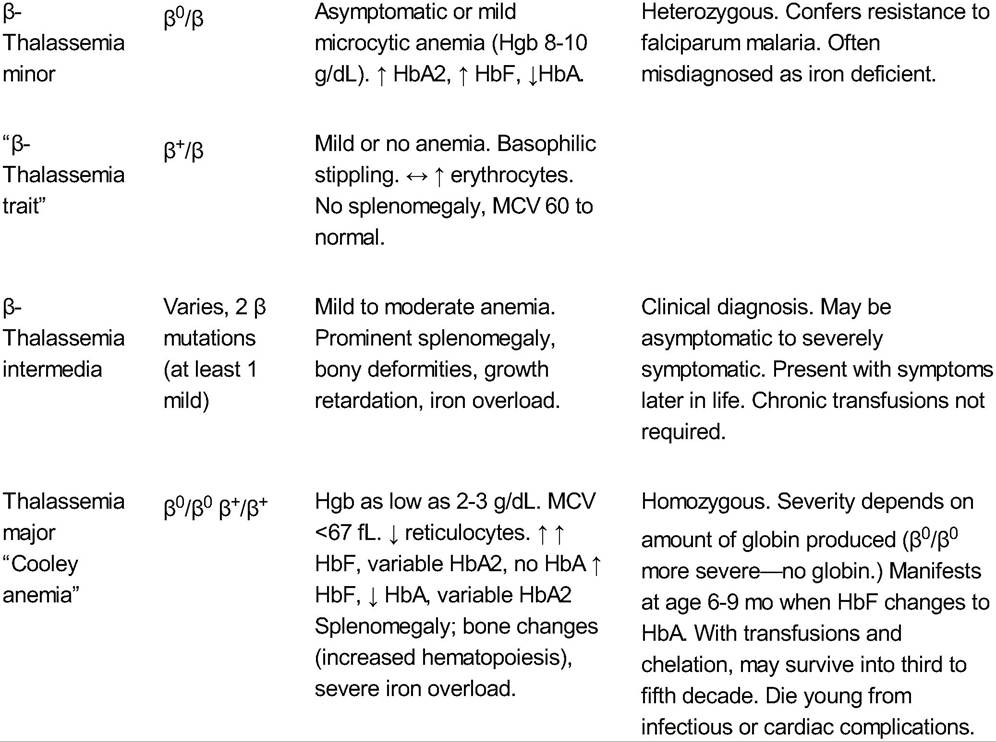
• The term thalassemia encompasses a group of inherited blood disorders that can cause severe microcytic hypochromic anemia. Alpha (α)-thalassemia and beta (β)-thalassemia result from absent or decreased production of structurally normal α- and β-globulin chains, respectively, generating an abnormal ratio of α to non-α chains (see Table 20-3). The excess chains form aggregates that lead to ineffective erythropoiesis and/or hemolysis. A broad spectrum of syndromes is possible, ranging from no symptoms to transfusiondependent anemia and death. Both diseases are transmitted as autosomal recessive traits.
P.253 P.254 P.255
• Alpha-thalassemia is associated with Southeast Asian, African, Caribbean, and Mediterranean origin and results from a deletion of one to all α genes, located on chromosome 16.
Excess β globins then form β-globin tetramers called HbH. A fetus would be affected because fetal Hgb also requires α chains.• Beta-thalassemia is associated with Mediterranean, Asian, Middle Eastern, Caribbean, and Hispanic origin. More than 200 alterations (mostly point mutations) in β-globin genes, located on chromosome 11, have been reported. The two consequences of these gene defects are the following: β0, which is the complete absence of the β chain, and β+, which is decreased synthesis of the β chain.
• Diagnosis: Thalassemia is usually microcytic and hypochromic with an MCV of 3.5%).
• Pregnancy and thalassemia
• Women with trait status for either thalassemia require no special care.
• Women diagnosed with or at high risk for thalassemia should be offered preconception counseling and information about the availability of prenatal diagnosis. First-trimester, DNA-based prenatal testing (CVS) is available if both members of the couple are carriers. Preimplantation genetic diagnosis may also be an option for affected parents.
• Women with HbH may have successful pregnancies, with maternal outcome related to the severity of anemia.
• Pregnancy may exacerbate the anemia, necessitating transfusions, and place women at an increased risk for preeclampsia, congestive heart failure, and premature delivery.
• Information on pregnancy in women with β-thalassemia major or intermedia is more limited, although successful pregnancies have been reported. These women require close medical evaluation and follow-up.
• If asplenic, vaccinations for pneumococcus, Haemophilus influenzae, and meningococcus need to be up-to- date.
• Thalassemia may confer an increased risk of neural tube defects secondary to folic acid deficiency, so up to 4 mg/day periconceptional folic acid supplementation is recommended. Iron supplements should be prescribed only if iron deficiency is present; otherwise, iron overload can result.
• Antepartum fetal testing should be undertaken in anemic thalassemia patients.
• Periodic fetal sonography to assess fetal growth as well as nonstress testing to evaluate fetal well-being is recommended.
• Ultrasonography is also useful to detect hydrops fetalis but usually at a later gestational age. Options for affected fetuses include intrauterine blood transfusions, which have shown good success in fetuses with hydrops fetalis.
TABLE 20-3 Findings in Thalassemia
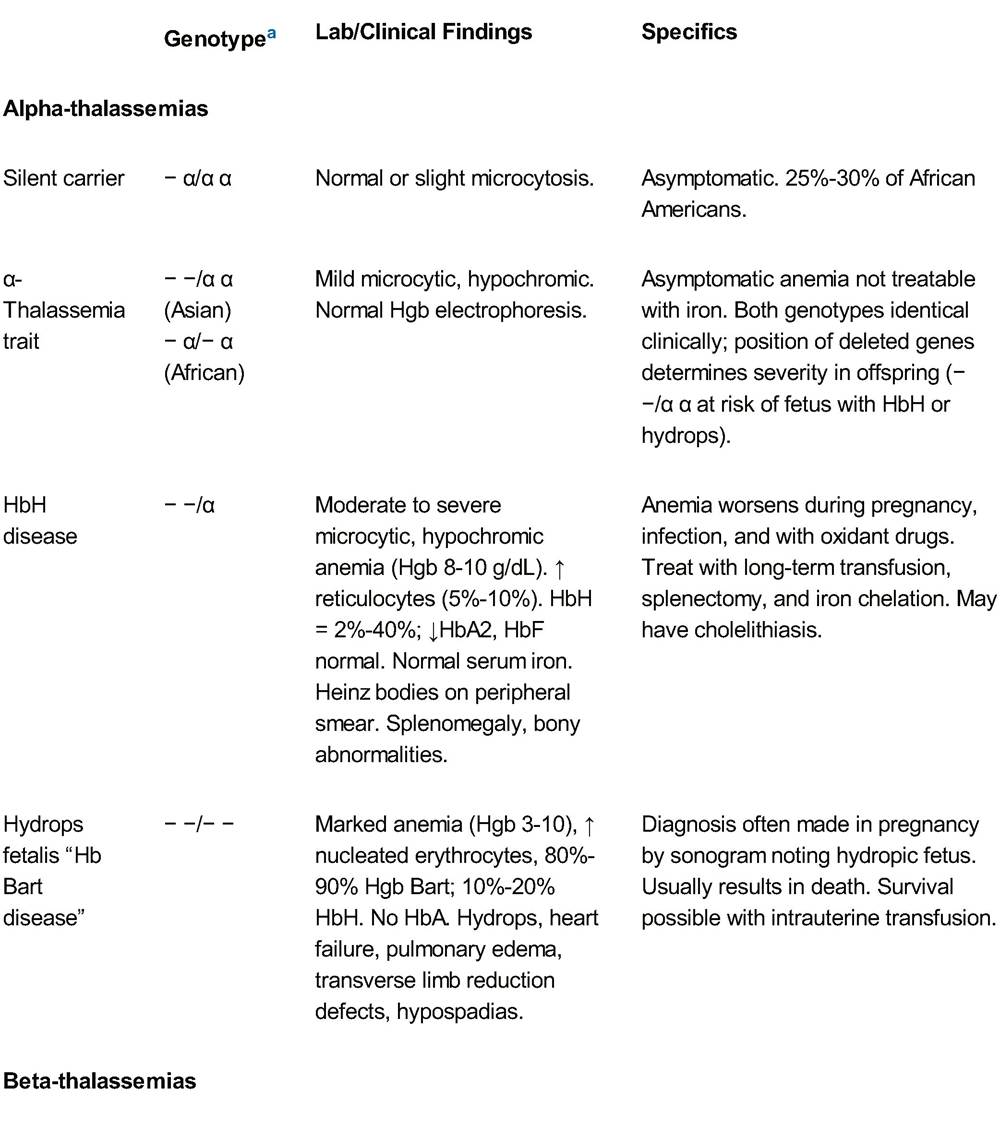
aGenotype: β and δ—single gene per chromosome. α Gene is duplicated producing two genes per haploid and four per diploid.
Hgb, hemoglobin; HbH, hemoglobin H; HbA, hemoglobin A; HbA2, hemoglobin alpha 2; HbF, feta hemoglobin; MCV, mean corpuscular volume.
Adapted from American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 78: hemoglobinopathies in pregnancy. Obstet Gynecol 2007;109:229-237.
P.256
Megaloblastic Anemia
• Megaloblastic anemia is the result of impaired DNA synthesis, leading to ineffective erythropoiesis.
• Megaloblastic anemia is a much greater problem in underdeveloped countries and is primarily the result of dietary folic acid deficiency. Folic acid requirements increase from 50 pg/day in the nonpregnant state to up to 800 pg/day during pregnancy. Phenytoin, nitrofurantoin, trimethoprim, and alcohol decrease absorption of folic acid.
• A less common cause of megaloblastic anemia is vitamin B12 deficiency, often from a long-term vegan diet or decreased intestinal absorption due to tropical sprue, regional enteritis, gastrointestinal resection for bariatric surgery, or chronic giardiasis.
• Megaloblastic anemia in pregnancy may lead to poor outcomes. Animal studies suggest that it may be related to abruptio placentae, preeclampsia, IUGR, and prematurity.
Folic acid deficiency is also linked toopen neural tube defects.
• Diagnosis: Megaloblastic anemia is often slowly progressive and tends to occur in the third trimester. Weight loss and anorexia may occur in addition to the usual symptoms of anemia, roughness of the skin, and glossitis. It can also manifest as bleeding due to thrombocytopenia or as an infection resulting from leukopenia.
• Laboratory findings:
î Macrocytic, normochromic anemia involving erythrocytes, leukocytes, and platelets
î Peripheral blood smear shows hypersegmented neutrophils, oval macrocytes, and Howell-Jolly bodies.
î To diagnose folate deficiency, consider the erythrocyte folate level, as it is a better indicator of whole body stores than the serum level, which can vary widely.
• Treatment: Determining which deficiency exists is important before commencing treatment.
î Folate deficiency is generally treated with daily folic acid supplementation of 1 mg/day. Within 7 to 10 days, the white blood cell and platelet counts should normalize. Hgb gradually increases to normal levels after several weeks of therapy.
î If the anemia is due to vitamin B12 deficiency, folate supplementation may ameliorate the anemia, masking the B12 deficiency; it may also precipitate neurologic deficits. Vitamin B12 deficiency is treated with intramuscular cobalamin. Affected patients may require monthly (1 mg) injections for life.
THROMBOCYTOPENIA
Thrombocytopenia is defined as a platelet count < 150,000∕μL and occurs in about 10% of pregnancies. Clinical signs, such as petechiae, easy bruising, epistaxis, gingival bleeding, and hematuria, are usually not seen until platelets are leading to increased destruction of platelets by the reticuloendothelial system (primarily the spleen) that exceeds the rate of platelet synthesis by the bone marrow. The course of ITP is not typically affected by pregnancy.
• Diagnosis: Diagnosis is based on the history, physical exam, complete blood count, and peripheral smear. Women with ITP may report symptoms of easy bruising, petechiae, epistaxis, or gingival bleeding predating pregnancy. ITP is a diagnosis of exclusion, and there is no diagnostic test. If thrombocytopenia is mild, it is difficult to distinguish ITP from gestational thrombocytopenia. Detection of platelet-associated antibodies is consistent with, but not diagnostic of, ITP because they may also be present in women with gestational thrombocytopenia and preeclampsia. Platelet antibody testing has a fairly low sensitivity (49% to 66%). However, the absence of platelet-associated IgG makes the diagnosis of ITP less likely. ITP is more likely if the platelet count is imparts a three to five times greater risk than a vaginal delivery.
Risk Factors for Venous Thromboembolism
• Pregnancy is considered a hypercoagulable state. Fibrinogen, coagulation factors, and plasminogen activator inhibitor-1 (PAI-1) levels are increased; free protein S levels are decreased, and fibrinolytic activity is decreased. Additionally, VTE risk is increased by anatomic changes in pregnancy including increased venous stasis and compression of the inferior vena cava and pelvic veins by the enlarging uterus.
• One of the most significant risk factors is a personal history of VTE. Maternal medical conditions including heart disease, SCD, lupus, obesity, diabetes, and hypertension increase risk. Other risk factors include recent surgery, family history of VTE, bed rest or prolonged immobilization, smoking, age older than 35 years, multiple gestations, preeclampsia, and postpartum infection.
• Thrombophilias may be inherited or acquired.
• Pregnancy may trigger an event in women with an underlying thrombophilia.
• Fetal death in utero, severe IUGR, abruption, and severe early-onset preeclampsia have been correlated with underlying thrombophilias that affect uteroplacental circulation; however, this is controversial and recent studies fail to reliably establish causal links between thrombophilias and these adverse pregnancy outcomes.
• Inherited thrombophilias (Table 20-4):
î Increase the risk of a maternal thromboembolic event approximately eightfold
î Are present in over half of all maternal thrombotic events.
î Antithrombin deficiency and homozygosity for factor V Leiden mutation are the most potent of the inherited thrombophilias. Double or compound heterozygotes (for both factor V Leiden and prothrombin G20219A) are also at greater risk of VTE.
• Acquired thrombophilias:
î Include persistent antiphospholipid antibody syndromes (APS) (lupus anticoagulants or anticardiolipin antibodies). APS is present in 15% to 17% of women with recurrent pregnancy loss.
• Routine screening for thrombophilias is not recommended in all pregnant women and screening indications are controversial. ACOG no longer recommends thrombophilia testing in women with recurrent fetal loss, placental abruption, IUGR, or preeclampsia. A thrombophilia workup (Table 20-5) should be considered for the following:
î VTE during pregnancy (workup after delivery) or VTE associated with a nonrecurrent risk factor such as prolonged immobilization.
P.261 î Personal or family history of VTE (first-degree relative with VTE before age 50 years in absence of other risk factors).
î APS screening may be appropriate for women with repeated fetal losses (three losses indicated for PE workup are minimal compared with the consequences of a missed PE.
• Pulmonary angiography is the gold standard for PE diagnosis, but it is expensive and invasive.
• Computed tomographic (pulmonary) angiography (CTA) is becoming the recommended imaging test in pregnant women with suspected PE. CTA is easier to perform, more readily available, more cost-effective, and provides a lower dose of radiation to the fetus than a V/Q scan. CTA is also useful in detecting other abnormalities that may be contributing to the patient's symptoms (e.g., pneumonia, aortic dissection). Newer technology, multidetector computed tomography pulmonary angiography, allows visualization of finer pulmonary vascular detail and provides greater diagnostic accuracy.
• Historically, the V/Q scan has been the primary diagnostic test for PE. It is interpreted as low, intermediate, or high probability for PE. High-probability scans (i.e., segmental perfusion defect with normal ventilation) confirm PE, with a positive predictive value over 90% when pretest likelihood is high. V/Q scans are limited in their usefulness because of the large proportion of indeterminate results. Most fetal radiation exposure occurs when radioactive tracers are excreted in the maternal bladder. Therefore, exposure can be limited by prompt and frequent voiding after the procedure. If patient is postpartum and breast-feeding, breast milk should not be used for 2 days after a V/Q scan.
• If a pregnant woman has a nondiagnostic lung scan, bilateral venous duplex imaging of the lower extremities is recommended to evaluate for DVT. If DVT is found, PE can be diagnosed. If no DVT is seen, arteriography may be performed for further evaluation before a commitment to long-term anticoagulation is made, or venous duplex imaging may be repeated in 1 week.
• According to the Centers for Disease Control and Prevention, in all stages of gestation, a dose of 5,000 U SC q 24 hr
Tinzaparin 4,500 U SC q 24 hr
UFH
UFH 5,000 U SC q 12 hr
Alternativeb
UFH 5,000-7,500 U SC q 12 hr in first trimester
UFH 7,500-10,000 U SC q 12 hr in second trimester
UFH 10,000 U SC q 12 hr in third trimester (unless aPTT elevated)
Intermediate dose
LMWH
Enoxaparin 40 mg SC q 12 hr
Dalteparin 5,000 U SC q 12 hr
UFH
UFH SC q 12 hr; doses adjusted to target peak antifactor Xa levels (4 hr after injection) of 0.1 to 0.3 U/mL
Treatment (weight-adjusted) dose
LMWH
Enoxaparin 1 mg/kg SC q 12 hr (or enoxaparin 1.5 mg/kg SC q 24 hrc)
Dalteparin 200 U/kg SC q 24 hr or 100 U/kg SC q 12 hr
Tinzaparin 175 U/kg SC q 24 hr
UFH
UFH SC q 12 hr; doses adjusted to obtain midinterval (6 hr postinjection) therapeutic aPTT (often a ratio of 1.5-2.5)
Postpartum anticoagulation (for 4-6 wk)
Warfarin with a target INR of 2.0-3.0 with initial UFH or LMWH overlap until INR >2.0 for 2 d
Prophylactic LMWH or UFH
aSome experts recommend twice daily dosing of enoxaparin secondary to pharmacokinetic properties of LMWH in pregnancy; however, comparison data are lacking. Additionally, women at the extremes of weight may require different dosing.bFrom James AH, Brancazio LR, Ortel TL, et al. Thrombosis, thrombophilia, and thromboprophylaxis in pregnancy. Clin Adv Hem Oncol 2005;3:187-197.cFrom Chunilal SD, Bates SM. Venous thromboembolism in pregnancy: diagnosis, management and prevention. Thromb Haemost 2009; 101:428-438.
LMWH, low-molecular-weight heparin; SC, subcutaneous; UFH, unfractionated heparin; aPTT, activated partial thromboplastin time; INR, international normalized ratio.
Adapted from Bates SM, Greer IA, Pabinger I, et al. Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 8th ed. Chest 2008;133:844S-886S.
Prophylaxis for Venous Thromboembolism in Pregnancy
Antepartum
• Limited data exist regarding the use of prophylactic anticoagulation for VTE during pregnancy. Women need to be stratified by risk and clinical judgment applied when making recommendations for prophylaxis. Although recommendations vary, women at very high risk for VTE probably benefit from UFH or LMWH throughout pregnancy and postpartum. At a minimum, postpartum prophylaxis is usually recommended in women at elevated risk for VTE.
At Delivery
• The risk of maternal hemorrhage may be minimized with carefully planned delivery. If possible, induction of labor or scheduled cesarean section should be considered in women on therapeutic anticoagulation dosing regimens, so therapy may be discontinued at an appropriate time. When used in therapeutic doses, LMWH should be discontinued 24 hours before elective induction of labor or cesarean delivery. Epidural or spinal anesthesia should not be administered within 24 hours of the last therapeutic dose of LMWH. A common approach is to transition from LMWH to UFH at 36 to 38 weeks' gestation. If the patient goes into spontaneous labor and is receiving SC UFH, she should be able to receive regional analgesia if the aPTT is normal. If significantly prolonged, protamine sulfate may be administered at 1 mg/100 U of UFH. If the patient is at very high risk for VTE, IV UFH can be started and then discontinued 4 to 6 hours before expected delivery. When receiving LMWH once daily for prophylaxis, regional anesthesia can be administered 12 hours after the last dose. LMWH should be withheld for at least 2 to 4 hours after the removal of an epidural catheter.
Postpartum
• Postpartum anticoagulation may be resumed within 12 hours of cesarean delivery and 4 to 6 hours after vaginal delivery. If at high risk of bleeding postpartum, IV UFH may be chosen initially because its effect dissipates more rapidly and may be reversed with protamine sulfate. Once adequate hemostasis is assured, warfarin can be started by initial overlap with UFH or LMWH until international normalized ratio (INR) is 2.0 for 2 consecutive days, with a target INR of 2.0 to 3.0. Anticoagulation should be administered for at least 6 weeks postpartum for DVT and 4 to 6 months for PE.
• Birth control options for women with a history of VTE or those with high-risk thrombophilias:
• Due to the thrombogenic potential of estrogen-containing contraceptives, progestin-only or nonhormonal contraceptive methods are recommended. Natural family planning, condoms, progestin-only pills, Levonorgestrel-releasing IUD, copper IUD, or tubal ligation/occlusion are methods that can be discussed with patients at high risk for VTE.
P.267
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 6: clinical management guidelines for obstetrician-gynecologists: thrombocytopenia in pregnancy. Int J Gynaecol Obstet 1999;67(2):117-128.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 124: inherited thrombophilias in pregnancy. Obstet Gynecol 2013;122(3):706-717.
James A; American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Obstetrics.
ACOG practice bulletin no. 123: thromboembolism in pregnancy. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118(3): 718-729.
James AH. Thromboembolism in pregnancy: recurrence risks, prevention and management. Curr Opin Obstet Gynecol 2008;20:550-556.
Marik PE, Plante LA. Venous thromboembolic disease and pregnancy. N Engl J Med 2008;359: 2025-2033.
Rogers DT, Molokie R. Sickle cell disease in pregnancy. Obstet Gynecol Clin North Am 2010; 37(2): 223237.
Rosenberg VA, Lockwood CJ. Thromboembolism in pregnancy. Obstet Gynecol Clin N Am 2007;34:481- 500.
Sukenik-Halevy R, Ellis MH, Fejgin MD. Management of immune thrombocytopenic purpura in pregnancy. Obstet Gynecol Surv 2008;63(3):182-188.