19 Neurologic Diseases in Pregnancy
Sarahn M. Wheeler
Irina Burd
A wide range of neurologic disorders can complicate pregnancy. The obstetric care provider is often challenged with managing these symptoms with a limited spectrum of medications known to be safe in pregnancy and a desire to minimize radiographic studies during parturition.
Additionally, women with complex preexisting neurologic conditions often achieve pregnancy, necessitating the obstetric provider to be well versed in the treatment of these conditions and the unique implications of these diseases in the setting of pregnancy. This section will review common neurologic complaints and preexisting neurologic conditions and their management during pregnancy.HEADACHE
• Headache is a common complaint in pregnancy.
• Although most of these headaches are due to benign causes, it is imperative that obstetric providers perform a thorough history and physical examination to identify those headaches that warrant further workup (Table 191).
• In the presence of concerning signs or symptoms, neurologic consultation and diagnostic workup should be performed.
P.242
TABLE 19-1 History and Physical Exam Findings that Should Prompt Further Headache Workup
| History | Physical Exam |
| • Sudden or rapid onset • Prior or coexisting infection • Onset during exertion • Immunosuppression • Environmental exposure • No relief from pain medication | • Toxic appearance • Fever • Decreased mental status • Papilledema • Any localizing or lateralizing signs • Meningismus |
Adapted from Contag SA, Bushnell C. Contemporary management of migrainous disorders in pregnancy. Curr Opin Obstet Gynecol 2010;22:437.
ImagingZDiagnosis
• Lumbar puncture (LP), magnetic resonance imaging (MRI), and head computed tomography (CT) can be considered for headache with concerning features.
• MRI poses no radiation exposure risks to the fetus and is the imaging of choice for pregnant patients.
However, MRI is expensive and often not readily available.
• Head CT is the imaging of choice for nonpregnant patients, as it is less expensive and more readily available in most settings. Although head CT does expose the fetus to some radiation, it is approximately 0.05 rad. A fetus must be exposed to 5 rad prior to significantly increased fetal risks, including fetal anomalies or pregnancy loss (Fig. 19-1). As such, the diagnostic benefit of a head CT, as with any clinical test, should be weighed against its risks.
• LP is not contraindicated in pregnancy and should be used if clinically indicated.
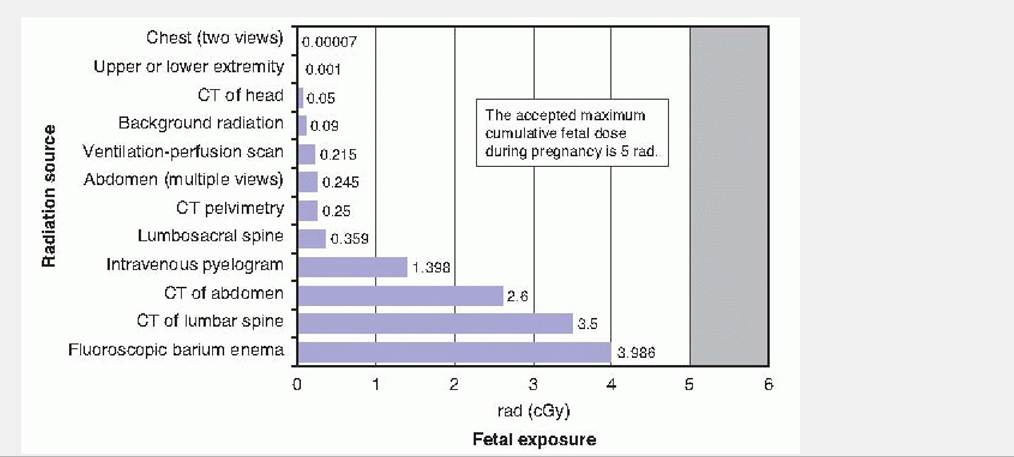
Figure 19-1. Fetal exposure to radiation with varying imaging studies. (From Toppenburg KS, Hill DA, Miller
DP. Safety of radiographic imaging during pregnancy. Am Fam Physician 1999;59:1813-1818, 1820.)
P.243
Common Obstetric Causes of Headache
• Any headache beyond 20 weeks' gestation and up to 12 weeks' postpartum should be included on the differential diagnosis preeclampsia, and the patient should have a blood pressure check and evaluation for proteinuria. If suspicion for preeclampsia is high, further workup including 24-hour urine collection and laboratory evaluation may be indicated (see Chapter 14).
• Post-epidural headache should be considered in postpartum patients particularly in postural headaches. Although acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), and caffeine are often sufficient treatment, anesthesia consultation for blood patching should be considered in patients who are refractory to conservative treatments.
Migraine
• Although many chronic migraine sufferers report improved symptoms during pregnancy, it remains a common cause of headache in pregnancy.
• Approximately 2% of women have their first migraine while pregnant.
• Typical migraine symptoms include unilateral headache with a throbbing quality, nausea, vomiting, and sensitivity to light and sound. Some patients also describe precipitating symptoms such as visual changes or weakness, known as an aura.
• Treatment of migraines in pregnancy: Many of the same pharmacologic and nonpharmacologic treatments
that are useful outside of pregnancy are also used intrapartum.
• Acute symptom management: T reatment of acute migraines can involve a variety of medications (T able 19-2).
• Chronic symptom management: Preventive therapy for frequent migraines with beta-blockade and calcium channel blockers can be used in pregnancy. Patients should be aware that prolonged use of betablockers may be associated with mild intrauterine growth restriction, transient bradycardia of the neonate, or hyperbilirubinemia.
• Refractory symptom management: Selective serotonin reuptake inhibitors (SSRI), serotonin norepinephrine reuptake inhibitors (SNRI), and tricyclic antidepressants may be useful, particularly for patients with comorbid depression.
• Although most of the medications used for migraine treatment are safe in pregnancy, there are some notable exceptions. Ergotamine is contraindicated in pregnancy due to its association with hypertonic uterine contractions. Isometheptene is generally avoided due to concern for compromising uterine blood flow.
Tension Headaches
• These are the most common type of headache.
• Patients describe tightness or tension in their head often with radiation to the neck.
• The frequency of tension headaches typically not altered by pregnancy
• T reatment: Nonpharmacologic treatments such as heat, massage, rest, and stress management are often helpful. Acetaminophen is the first-line pharmacologic therapy. NSAIDs can be used in the second trimester. Muscle relaxants can often be a useful adjunct. Opioids should be reserved for rare circumstances and for a limited course.
Cluster Headaches
• These are recurrent, unilateral headaches that are accompanied by autonomic symptoms such as nasal stuffiness, tearing, facial swelling, or eyelid edema.
P.244
• Recurrent headaches are more common in males.
• Treatment: Oxygen therapy is first line for both pregnant and nonpregnant patients. Intranasal lidocaine and triptans can also be useful adjunct therapies.
TABLE 19-2 Treatment Options for Acute Migraine Headache in Pregnancy
First-Line Therapies
Acetaminophen a Extensive evidence of its safety in pregnancy
• Inexpensive
• May be used in combination with other drugs
• Maximum of 4 g daily to avoid liver toxicity
Caffeine a Up to 200 mg daily considered safe in pregnancy
• Can be used in combination with acetaminophen
Metoclopramide ∙ Often helpful with headache reduction and alleviates associated nausea
• Can cause dystonic reaction
Second-Line Therapies
NSAIDs∕aspirin ∙ Not used in first trimester due to possible teratogenicity
• Safe in second trimester
• Use in third trimester should be limited to 48 hr or less due to possible premature ductal closure, platelet dysfunction, and oligohydramnios
Third-Line Therapies
Opioids ∙ Should be used for short duration, as dependence can develop in the mother or
fetus with high doses over long duration
• Can cause constipation and worsen nausea/vomiting associated with migraines
• No teratogenic effects associated with opioids
Severe Symptoms
Triptans a Studies show no association with triptans and birth defects
• Use in third trimester associated with slight increased risk of uterine atony and increased blood loss at delivery
NSAIDs, nonsteroidal anti-inflammatory drugs.
CARPAL TUNNEL SYNDROME
• Diagnosed clinically. Symptoms include pain and numbness in the median nerve distribution.
P.245
• Pregnant patients at increased risk due to swelling of carpal tunnels leading to compression of median nerves.
• Symptoms most often present in the third trimester and can remain for up to a year after delivery.
• T reatment with conservative measures such as a wrist brace is usually effective. In rare cases, corticosteroid injections or surgery is indicated.
CHRONIC NEUROLOGIC DISEASES
Multiple Sclerosis
• Multiple sclerosis (MS) is an autoimmune demyelinating disease characterized by relapsing and remitting neurologic deficits.
• Common symptoms during a flare include optic neuritis, asymmetric numbness, weakness, or ataxia.
• There are no current recommendations regarding whether women should become pregnant in the setting of
MS.
• MS can have a variable course in pregnancy.
• The intrapartum period is associated with decreased MS flare risk, whereas postpartum patients have an increased risk.
• Taken together, pregnancy overall has not been shown to alter the long-term disease course.
• Many of the common treatment options for MS are teratogenic. Patients are often advised to discontinue disease-modifying drugs due to teratogenic concerns and decreased risk of flare intrapartum.
• Acute flares in pregnancy are typically managed with glucocorticoids.
• Classically, MS was considered a contraindication for spinal anesthesia. More recently, data has supported individualizing the plan of anesthetic care and spinal anesthesia.
Epilepsy
• Many of the drugs used to control epilepsy are teratogenic; therefore, patients should be weaned to the lowest dose possible prior to pregnancy or weaned off of the medications entirely.
• Valproate, carbamazepine, phenobarbital, and lamotrigine are commonly used antiepileptics and are all associated with an increased risk of neural tube defects. Recent data suggests that when used as single agents, these medications cause less frequent severe congenital defects than previously thought (Fig. 19-2).
• Women with epilepsy who are pregnant or planning a pregnancy should be supplemented with 4 mg of folic acid daily to help prevent neural tube defects.
• Pregnancy does not typically affect the frequency of seizures.
However, a confounding factor is that pregnant mothers are often noncompliant with medications for fear of teratogenicity.• Seizure during pregnancy can cause fetal hypoxia. Fetal monitoring may reflect fetal hypoxia for up to 30 minutes after the seizure. Emergent delivery is not indicated based on this tracing alone.
• Preeclampsia must be considered in the differential in the setting of seizures, particularly in the third trimester (see Chapter 14).
P.246
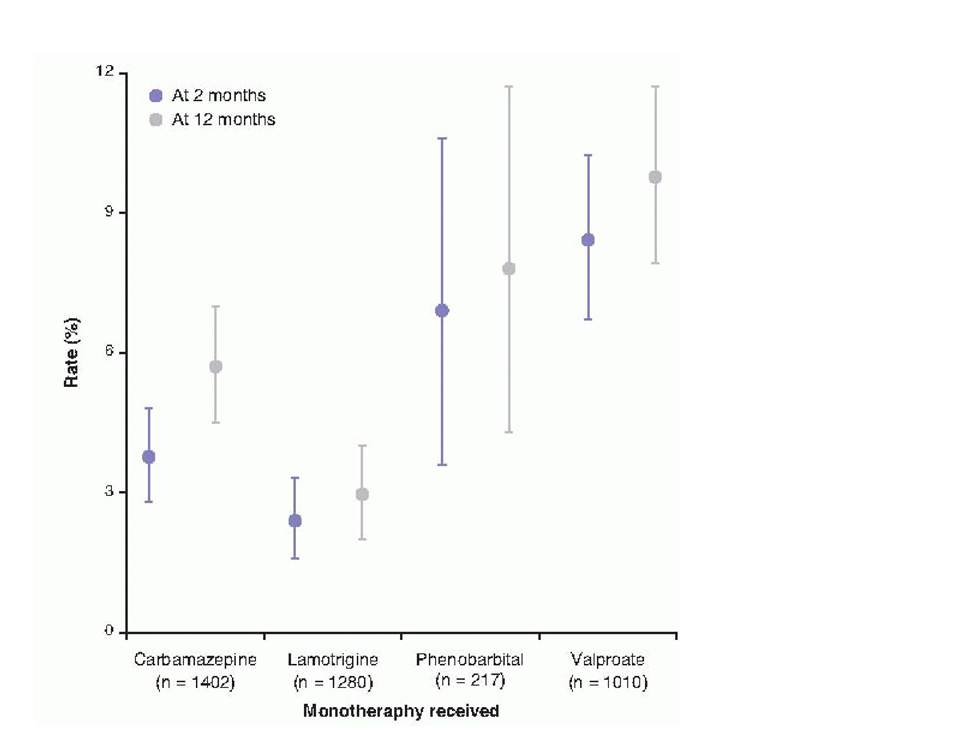
Figure 19-2. The rates of major anomalies associated with in utero exposure to various antiepileptic medications and 2 and 12 months of life. (From Tomson T, Battino D. Teratogenic effects of antiepileptic drugs. Lancet Neurol 2012;11[9]:803-813.)
Spinal Cord Injury
Complications of pregnancy in patients with prior spinal cord injuries are often related to the level of the spinal cord lesion.
• Patients with lower lesions (T 11 and below) will likely perceive labor pain. Most complications in their pregnancies are related to recurrent urinary tract infections and decubitus ulcers.
• Patients with mid lesions (T5 to T10) often have painless deliveries. These patients must be counseled carefully and monitored closely to avoid undetected labor and delivery. Patients can use home uterine monitors or be taught uterine palpation. Weekly cervical examinations should be considered near term.
• Higher lesions (above T5 to T6) are associated with autonomic dysreflexia leading to potentially lifethreatening sympathetic hyperactivity. This is manifested by severe hypertension, loss of consciousness, headache, nasal congestion, facial erythema, sweating, piloerection, bradycardia, tachycardia, or arrhythmia. It can be very challenging to distinguish this condition from preeclampsia. Epidural anesthesia up to T10 is critical in patients with high spinal cord lesions to prevent this complication. In the setting of acute autonomic dysreflexia, labetalol or nifedipine can be used to control blood pressure. Magnesium sulfate has been
P.247 shown to have some benefit in the setting of autonomic dysreflexia (although it is not first line) and should be considered if preeclampsia cannot be definitively excluded.
Myasthenia Gravis
• Myasthenia gravis (MG) is an autoimmune disease marked by muscle fatigue due to antibodies against acetylcholine receptors.
• There are two types of MG:
• Ocular MG involves only the eyelids and extraocular muscles
• Generalized MG involves ocular, bulbar, limb, and respiratory muscles affected
• Exacerbation in pregnancy noted in approximately 40% of patients. Flares are particularly likely in the first trimester and immediately postpartum.
• Treatment:
• Acetylcholinesterase inhibitors are first-line therapy for pregnant and nonpregnant patients.
• Glucocorticoids, azathioprine, and cyclosporine are second-line options and are safe in pregnancy.
• Medication interactions:
• Patients with MG are often challenging to manage because a wide variety of medications can exacerbate symptoms. These medications range from anesthetics to antibiotics, even oxytocin and magnesium sulfate.
• Magnesium sulfate is contraindicated for these patients. In the setting of preeclampsia, levetiracetam or valproic acid can be used for seizure prophylaxis.
• Concerns during labor:
• First stage of labor is not affected by MG, as this stage is mediated by smooth muscles. MG only affects skeletal muscle.
• Second stage of labor can be affected and patients can become fatigued with pushing. “Laboring down” or operative delivery can be used to minimize fatigue.
• Fetal concerns:
• Immunoglobulin G anti—acetylcholine receptor antibodies can cross the placenta leading to fetal manifestations of MG.
• Polyhydramnios due to impaired swallowing, decreased fetal movement, and decreased fetal breathing can be observed in fetuses of MG patients.
• Nonstress test is often not reliable because fetal movement and therefore accelerations can be impaired by MG. Contraction stress testing can be useful.
• Up to 20% of neonates develop transient MG postpartum, lasting for up to 3 months.
• Most studies do not show an increased long-term risk of MG in fetuses born to MG patients, although data are limited.
POSTPARTUM COMPRESSION NERVE INJURIES
• Risk factors include fetal macrosomia, epidural anesthesia, prolonged second stage, and poor positioning in stirrups.
• Prolonged pushing and “over”-aggressive McRoberts during second stage of labor can be associated with postpartum neuropathies. This is particularly true in patients who have an epidural during the second stage of labor.
• See Table 19-3 for common nerve palsies and the associated mechanism of injury.
• Most patients make a complete recovery. Physical therapy can be helpful.
P.248
| TABLE 19-3 Common Postpartum Nerve Palsies and Mechanisms of Injury | ||
| Nerve Damaged | Common Mechanism of Injury | Deficit |
| Peroneal nerve | • Prolonged knee flexion during labor • Pressure of fibular head from stirrups • Palmar pressure during pushing | • Inability to dorsiflex the foot, i.e., foot drop |
| Femoral nerve | • Prolonged hip flexion with McRoberts | • Weak quadriceps leading to inability to flex hip • Sensory loss over anterior and medial thigh |
| Lateral femoral cutaneous | • Prolonged compression | • Purely sensory defect, often paresthesias on outer thigh |
SUGGESTED READINGS
Boonmak P, Boonmak S. Epidural blood patching for preventing and treating post-dural puncture headache. Cochrane Database Syst Rev2010;(1 ):CD001791.
Contag SA, Bushnell C. Contemporary management of migrainous disorders in pregnancy. Curr Opin Obstet Gynecol 2010;22:437.
Coyle, PK. Pregnancy and multiple sclerosis. Neurol Clin 2012;30(3):877-888.
Estresvag JM, Zwart JA, Helde G, et al. Headache and transient focal neurologic symptoms during pregnancy, a prospective cohort. Acta Neurol Scand 2005;111:233.
Ferrero S, Esposito F, Biamonti M, et al. Myasthenia gravis during pregnancy. Expert Rev Neurother 2008;8(6):979-988.
Osterman M, Ilyas AM, Matzon JL. Carpel tunnel syndrome in pregnancy. Othop Clin North Am 2012;43(4):515-520.
Pasto L, Portaccio E, Ghezzi A, et al. Epidural analgesia and cesarean delivery in multiple sclerosis postpartum relapses: the Italian cohort study. BMC Neurol 2012; 12:165.
Pearce CF, Hansen WF. Headache and neurological diseases in pregnancy. Clin Obstet Gynecol 2012;55(3):810-828.
Signore C, Spong CY, Krotoski D, et al. Pregnancy in women with physical disabilities. Obstet Gynecol 2011;117(4):935-947.
Tomson T, Battino D. Teratogenic effects of antiepileptic drugs. Lancet Neurol 2012;11(9): 803-813.
Toppenburg KS, Hill DA, Miller DP, et al. Safety of radiographic imaging during pregnancy. Am Fam Physician 1999;59:1813-1818.
Wong CA, Scavone BM, Dugan S, et al. Incidence of postpartum lumbosacral spine and lower extremity nerve injuries. Obstet Gynecol 2003;101:279.