Amenorrhoea (absence of menstruation) and dysmenorrhoea (menstrually related pelvic pain)
Introduction to amenorrhoea and dysmenorrhoea
Amenorrhoea and dysmenorrhoea are two common symptom groupings presenting at opposite ends of the menstrual cycle symptom spectrum.
Amenorrhoea is generally understood to be the complete absence of menstrual bleeding at a time when it would be expected. Hence, the common perimenstrual symptoms which frequently accompany AUB rarely occur in these women. Dysmenorrhoea means pelvic pain accompanying menstruation. Both of these symptoms are common in women within the reproductive ages between menarche and menopause, but the two cannot, by definition, occur in the same patient at the same time! Management of both requires a sound knowledge of the anatomy, physiology, and potential pathophysiology of the reproductive tract.Amenorrhoea
Amenorrhoea is a very specific type of menstrual disturbance where menstruation does not occur at the specific times when it is expected. The term literally means absence or cessation of bleeding, and the duration of this absence needs to be specified. Amenorrhoea can be divided into two separate categories:
• Primary amenorrhoea: failure of natural menstruation to spontaneously begin at the normal age of puberty. If absent at age 15, it should be investigated. However, this symptom needs to be looked at in two ways:
■ The young woman who has had normal onset of other pubertal symptoms and signs, such as breast and pubic hair development, at normal age, but has not menstruated by age 15. She needs to be investigated for ‘menstrual delay.
■ The young woman who has not yet developed the expected symptoms and signs of puberty. She needs to be investigated for ‘delay of onset of normal puberty, and this investigation should usually begin earlier than age 15.
• Secondary amenorrhoea: this is the absence of menstruation for at least 6 months in a woman, who has previously menstruated.
Three other terms are relevant here:
• Infrequent menstruation: this category used to be called ‘oligomenorrhoea, but that term has now been abandoned. This term is usually applied to women with long gaps between periods. The upper limit of the normal regular cycle is taken at 38 days. Above this is mild (>38 days), moderate (>50 days), or severely (>90 days) infrequent bleeding. This symptom merges into secondary amenorrhoea, and should be investigated in a similar manner.
• Physiological amenorrhoea: this covers those situations where absence of menstruation is expected: prepuberty, postmenopause, pregnancy, and breastfeeding (lactation).
• Pharmacological amenorrhoea: occurs when menstruation ceases as a consequence of the administration of specific drugs or of a specific surgical procedure (Box 41.13).
Causes of primary amenorrhoea
Primary amenorrhoea typically results from constitutional delay, genetic factors, or from an outflow tract obstruction, such as in the case of imperforate hymen, transverse vaginal septum, or cervical blockage (Box 41.14). Constitutional delay is characterized by delayed skeletal growth and is one of the common causes for delayed puberty and menstruation. Chronic illnesses such as diabetes, renal insufficiency, and thyroid disease can further lead to menstrual dysfunction, as can malignancy and its therapies.
History and examination for primary amenorrhoea
A detailed history and examination for the presence, timing, or absence of secondary sexual characteristics is essential. Information regarding past and current medical illness, such as thyroid disease, renal disease, diabetes, malignancy, and therapies should be ascertained. Social history, life stressors, excessive exercise, weight change, potential for anorexia or bulimia, and detailed family history should be explored.
Examination of women with primary amenorrhoea involves recording growth, body mass index (BMI), and pubertal stage. The Tanner system of staging breast and pubic hair development is commonly utilized to compare development of secondary sexual characteristics against normal.
In addition to these checks it may be appropriate to perform a pelvic exam (usually only in those who have been sexually active).Investigations for primary amenorrhoea
After a thorough history and examination, the patients can be grouped into two categories—those with delayed puberty (in whom
Box 41.13 Pharmacological amenorrhoea
Drugs
• Combined oral contraceptive pills taken continuously
• Levonorgestrel intrauterine systems
• Progestogen subdermal implants and injectables
• Some antidepressants/antipsychotics
• Some antihypertensives
• Many chemotherapeutic agents
Surgical interventions
• Endometrial destructive techniques such as ablation or resection
• Hysterectomy
Box 41.14 Well-recognized causes of amenorrhoea
• Hypothalamic dysfunction:
— Excessive exercise
— Excessive weight loss, anorexia nervosa
— Rare hypothalamic diseases
• Pituitary dysfunction:
— Hyperprolactinaemia
— Pituitary adenoma
— Medications:
• Oral contraceptive pill
• Antidepressants
• Antihypertensives
• Ovarian dysfunction:
— Polycystic ovary syndrome
— Menopause/menopause transition
— Premature ovarian insufficiency:
• Autoimmune
• Endocrine
• Chemotherapy, radiotherapy
• Infection
• Genetic
• Outflow tract (uterus, cervix, and vagina) dysfunction:
— Mullerian agenesis
— Intrauterine scarring
— Intrauterine infections
— Transverse vaginal septum
— Cervical stenosis
• Physiological:
— Prepubertal
— Pregnancy
— Lactation
— Postmenopausal
• Other:
— Thyroid disease
— Chronic systemic illness secondary sexual development has not yet occurred or is minimal) and those with normal puberty (Figure 41.1 and Box 41.15).
Delayed puberty-investigations and differential diagnosis
In patients in whom secondary sexual characteristics have not developed or are minimal, the key investigation is to measure serum follicle-stimulating hormone (FSH). However, we usually choose to measure other relevant hormones at the same time at the initial visit.
These include serum luteinizing hormone (LH), oestradiol, prolactin, thyroid-stimulating hormone (TSH), free triiodothyronine (FT3), and free thyroxine (FT4).If FSH is low then the differential diagnosis includes constitutional delay in ‘switching on' of hypothalamic mechanisms resulting in the initiation of pulsatile GnRH secretion and any hypothalamic cause, including anorexia, bulimia, and a range of chronic and systemic illnesses, often called hypogonadotropic hypogonadism. A number of genetic mutations have been identified in patients with congenital GnRH deficiency including mutations in genes such as KAL1, FGFR1, and GNRHR (11) and patients in whom these defects are present may among other things present with amenorrhoea. Kallmann syndrome is a rare but well-recognized condition, which is due to failure of the GnRH-secreting neurons to migrate from their early embryonic origins in the frontal cortex to the adult site in the hypothalamus. This condition is also linked with congenital anosmia and failure of the neurons for sense of smell to develop within the frontal cortex.
If, however, serum FSH and LH levels are high (hypergonadotropic hypogonadism), and oestradiol levels are very low, indicating premature ovarian insufficiency (POI), it is appropriate to investigate further and perform genetic testing. Differential diagnoses include Turner syndrome (45XO), fragile X syndrome (defective gene on X chromosome), XY female, and primary ovarian failure. Turner syndrome is characterized by a 45XO karyotype, and is a condition
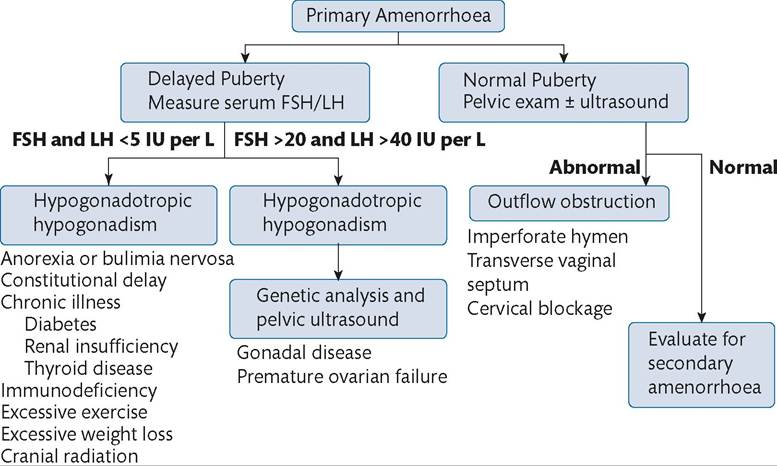
Figure 41.1 Evaluation of primary amenorrhoea.
Source data from Master-Hunter T, Heiman DL. Amenorrhea: evaluation and treatment. Am Fam Physician 2006;15:1374-82 and Slap GB. Menstrual disorders in adolescence. Best Pract Res Clin Obstet Gynaeco12003;17:75-92.
Box 41.15 The two key questions needed in assessing primary amenorrhoea
1 Does she have no signs of normal puberty? (She has ‘delayed puberty'.)
2 Does she have normal pubertal changes in body shape and normal breast and pubic hair development? (She has ‘delayed onset of menstruation'.)
Box 41.16 Principles of management of primary amenorrhoea
• Counselling
• Medical management
• Surgical management
• Actively treating infertility factors
• Prevention of associated side effects
caused by the absence of one complete or partial copy of the X chromosome in some or all of the cells.
Primary ovarian failure commonly results from radiation or chemotherapy exposure in childhood. It may also result from exposure to previous infection (e.g. mumps).
Girls of 15 years or more with normal pubertal changes in body habitus, breasts and public hair but no periods- investigations and differential diagnosis
It is wise to objectively assess pubertal changes in breasts and pubic hair using the Tanner Sexual Maturity Rating scales against a background of body shape and general maturity to ensure that puberty has been normal. Also check whether she has been treated with ‘hormones’ such as the contraceptive pill.
It is then useful to perform a pelvic ultrasound scan (transvaginal or abdominal, depending on previous sexual activity), which will aid in identifying outflow tract obstruction, or Mullerian agenesis. Outflow tract obstruction can occur at the level of the hymen or within the vagina or cervix. On vaginal examination, obstruction by an imperforate hymen is characterized by a bulging, blue introital membrane through which menstrual effluent can be visualized. Obstruction within the vagina, by a transverse vaginal septum, can occur at any level. Ultrasound scanning may also reveal Mullerian agenesis, characterized by the congenital absence of the uterus, upper (occasionally upper and lower) vagina and cervix, and portions of the fallopian tubes. The ovaries usually appear normal and are normally sited. Ovulation appears to continue in a fairly regular manner.
In the presence of normal ultrasound findings, further investigation should proceed as outlined in the ‘Secondary amenorrhoea’ section.
Management of primary amenorrhoea
Treatment of primary amenorrhoea often involves, where possible, correcting underlying pathology, improving fertility (or actively treating infertility) and preventing associated adverse side effects that may result from long-term low oestrogen levels (Box 41.16).
In the first instance, patients and family members should be thoroughly counselled.
This is especially important for patients with Mullerian agenesis and/or in whom a Y chromosome is present. These patients require careful explanation of the causes and possible management options, as well as discussion regarding gender issues and their future fertility outlook. Surgical management may be appropriate, particularly where there is a need to correct vaginal tract outflow obstruction. Management of outflow tract obstruction at the level of the hymen is through a cruciate incision in the hymen with limited trimming of the redundant membrane tissue, which allows release of the menstrual flow. Management of a transverse septum often requires more complex surgical intervention with some vaginal reconstructive surgery.Generally for patients with hypo- oestrogenism, hormone replacement therapy or the combined oral contraceptive pill (COCP) is suggested to reduce future cardiovascular or osteoporosis risks. For patients considering pregnancy, referral for assisted reproductive technologies and consultation with an experienced infertility specialist is appropriate. For patients with hypothalamic or pituitary dysfunction, exogenous gonadotrophins or pulsatile GnRH can be administered in a precise manner, and can be combined with other modern in vitro fertility technologies. For others, discussion around oocyte donation or surrogacy may be appropriate fertility considerations.
Secondary amenorrhoea
Pregnancy and lactation (planned or unplanned) are the commonest causes of secondary amenorrhoea. However, non-physiological causes of secondary amenorrhoea can be grouped according to the following subgroups in terms of an anatomically based approach (Box 41.17).
Hypothalamic dysfunction
Hypothalamic dysfunction is characterized by suppressed pulsatile GnRH secretion, absence of FSH and LH secretion, absence of ovarian follicle development, and very low serum oestradiol. This dysfunction can be attributed to excessive exercise or major weight reduction, eating disorders, and ‘stress’. There is great variability in the degree of weight loss, eating disorders, excessive exercise, and physical and emotional stressors required to induce amenorrhoea. Familial polycystic ovary tendency may contribute. Pathways by which these act are poorly understood.
Other GnRH suppressors include systemic chronic illnesses and rare hypothalamic tumours and infiltrative lesions. Type 1 diabetes mellitus and coeliac disease may also interfere with GnRH secretion (12, 13).
Pituitary dysfunction
A common cause of secondary amenorrhoea is excessive pituitary secretion of prolactin, often from a benign prolactin-s ecreting adenoma—a ‘prolactinoma’. Raised prolactin levels induce amenorrhoea by suppressing hypothalamic GnRH secretion. Other rare pituitary lesions (‘non-functional’ or other pituitary adenomas), can also suppress GnRH secretion, with or without hyperprolactinaemia.
Box 41.17 Anatomical causes of secondary amenorrhoea
H: hypothalamic dysfunction, 35%
P: pituitary dysfunction, 17%
O: ovarian dysfunction, 40%
U: uterine dysfunction, 7%
Other, 1%
Ovarian dysfunction
Polycystic ovary syndrome (PCOS) accounts for approximately 20% of cases of secondary amenorrhoea. The pathophysiology of PCOS is complex and variable; however, it is usually associated with ovulatory dysfunction, androgen excess, and with increased ovarian antral follicles on ultrasound. Classical signs of hyperandrogenism include oily skin, hirsutism, and acne, and women with PCOS are commonly overweight and have insulin resistance and metabolic syndrome. Women with PCOS typically present with infrequent and irregular periods or secondary amenorrhoea (AUB-O). PCOS is addressed in much more detail in Chapter 42).
Some PCOS patients may develop endometrial hyperplasia (and rarely low-grade endometrial adenocarcinoma at an early age) due to anovulation with excessive ovarian follicular secretion of oestradiol and absence of progesterone secretion. Endometrial hyperplasia may be accompanied by irregular and sometimes very heavy uterine bleeding (AUB-M).
Premature ovarian failure (often nowadays called POI), is characterized by excessive premature depletion of follicles and oocytes prior to the age of 40 years. This can occur at any age, including before puberty. Lack of ovarian endocrine function leads to very low circulating levels of oestradiol and endometrial atrophy. POI may result from a range of rare and poorly known causes of follicular destruction (e.g. the range of blepharophimosis-ptosis-epicanthus inversus syndromes, and carriers of the fragile X premutation) are often combined with POI and amenorrhoea).
Small numbers of women with POI will have moderate numbers of histologically normal follicles and oocytes still present in the ovaries, albeit unresponsive to FSH. Rarely, one or more of these follicles and oocytes may become spontaneously sensitive to FSH and LH and even ovulate.
Genetic and hereditary ovarian causes are likely to present as primary amenorrhoea; however, secondary amenorrhea can occur on a background of autoimmune diseases affecting ovaries (such as in Addison's disease, diabetes mellitus, rheumatoid arthritis, Sjogren syndrome, and systemic lupus erythematosus) or as a result of ovarian toxicity induced by radiation or chemotherapy exposure. Other ovarian causes of amenorrhoea are rare and include rare ovarian tumours, such as fibrothecomas.
Uterine dysfunction
The most common, but still rare, cause of amenorrhoea attributable to uterine dysfunction is the development of intrauterine adhesions following major damage to the endometrium. This is usually referred to as Asherman syndrome (or intrauterine synechiae). These adhesions prevent normal endometrial proliferation, decidualization, and shedding. This scarring is typically secondary to curettage carried out to remove retained placental products postpartum or postabortion in the presence of low-grade endometrial infection and secondary postpartum haemorrhage. This is one of only two situations when amenorrhoea occurs in the presence of regular ovulation, the other being absence of the uterus (either Mullerian agenesis or hysterectomy).
Other causes
A range of other uncommon causes can be implicated in amenor- rhoea. Both hyper- and hypothyroidism can cause amenorrhoea, which may be primary or secondary. Appropriate investigation will often pick up thyroid dysfunction and for these patients referral and management by a specialist endocrinologist is indicated. Treatment of underlying thyroid dysfunction will lead to restoration of a normal menstrual cycle.
Evaluation of secondary amenorrhoea
Evaluation of secondary amenorrhoea begins with exclusion of pregnancy, which can occur ‘out of the blue' even following a prolonged period of amenorrhoea. This is easily done with urinary and/or serum beta-human chorionic gonadotropin measurement. Detailed history and examination should follow a negative test.
Detailed history to assess secondary amenorrhoea
A thorough history will usually form the basis of the underlying diagnosis. Duration of amenorrhoea and potential recent exacerbating factors (changes in weight, diet, exercise, stressors) are important. Detailed medical, surgical, gynaecological, and family histories are critical. Information should be sought regarding specific signs and symptoms, such as hirsutism, acne and infrequent bleeding (PCOS), neurological symptoms and visual disturbances (hypothalamic-pituitary disease), symptoms of oestrogen deficiency (POI), uterine surgery (Asherman syndrome), or galactor- rhoea (hyperprolactinaemia).
Examination for secondary amenorrhoea
Physical examination should include weight and BMI measurements. The patient should be specifically examined for signs of PCOS, oestrogen deficiency, galactorrhoea, thyroid disease, and for signs of other systemic diseases.
Physical examination and investigations for secondary amenorrhoea
Principles of investigations for secondary amenorrhoea are listed in Box 41.18.
Laboratory investigations
Initial laboratory investigations for secondary amenorrhoea are listed in Box 41.19.
Patients in whom prolactin and TSH are normal, and in whom FSH levels are normal or low, are likely to have amenorrhoea attributed to hypothalamic-pituitary dysfunction or PCOS. However, endocrine findings in PCOS can sometimes be complicated and some PCOS patients may have mildly or moderately elevated serum prolactin. In patients with functional hypothalamic amenorrhoea, the ‘low' FSH levels are commonly higher than the LH levels, while in PCOS, FSH levels tend to be lower.
Box 41.18 Principles of investigations for secondary amenorrhoea
• Physical examination (weight and BMI); hirsutism, acne, galactorrhoea, thyroid signs
• Laboratory investigations (see Box 41.19)
• Imaging (e.g. transvaginal ultrasound, pituitary MRI)
• Genetic testing
• Hysteroscopy (for Asherman syndrome)
Box 41.19 Laboratory investigations for secondary amenorrhoea
Serum levels of the following:
• Beta-human chorionic gonadotropin
• FSH
• LH
• Prolactin
• TSH, FT3, and FT4
• Oestradiol
• Dehydroepiandrosterone sulphate (DHEAS) and 17-hydroxy- progesterone
• Total or free testosterone (if PCOS is suspected)
• Other (HbA1c, fasting blood sugar levels), full blood count, Multi Biochemical Analysis 20 (MBA-20)
Highly elevated FSH levels with low oestrogen levels in conjunction with the presence of hot flushes/symptoms of vaginal atrophy are indicative of POI.
Raised prolactin levels may result on a background of stress or other systemic illness, and therefore initially raised prolactin levels should be repeated. Generally, levels greater than 50 mcg/L (or 500 IU/L) warrant further investigation with imaging. Measuring TSH levels is often all that is needed to elucidate thyroid dysfunction (especially hypothyroidism) and ensure appropriate endocrine referral and treatment.
Greatly raised testosterone levels may be suggestive of PCOS or raise suspicion of a rare androgen-secreting tumour. In the presence of clinical features of hyperandrogenism (hirsutism, acne), serum testosterone levels and transvaginal ultrasound imaging may be diagnostic of PCOS.
Imaging of the pelvic organs and the pituitary gland
Ultrasonography is an extremely useful imagining modality in modern gynaecology and particularly may aid in detection of features suggestive of PCOS (with many follicles) or ovarian failure (with few or no small follicles). It may also be invaluable in assessing the presence, size, and shape of the uterus and the presence of adhesions within the endometrial cavity. For young women who have never been sexually active, it may not be appropriate to attempt a transvaginal scan. An abdominal scan will often reveal all that is necessary, but is less clear and more difficult to interpret.
In patients in whom prolactin levels are raised, imaging of the hypothalamus and pituitary with MRI is indicated to assess the possible presence of a pituitary adenoma. MRI or computed tomography imaging may also be indicated in patients who exhibit neurological signs or symptoms and where there is suspicion of other pituitary or hypothalamic lesions causing local pressure symptoms or tissue damage.
Hysteroscopy
Hysteroscopy may be indicated in evaluation and active management of intrauterine adhesions, through direct visualization of the endometrial cavity and division of the adhesions themselves, following careful ultrasound assessment.
Management of secondary amenorrhoea
The principles of management of secondary amenorrhoea are listed in Box 41.20.
Restoration of menses
For patients with hypothalamic amenorrhoea, restoration of menstruation is often achieved through lifestyle modification and behavioural changes. This may include increased (or decreased) caloric intake, limitation (or increase) of energy expenditure, and nutritional counselling, In addition, appropriate detection, specialist referral, and treatment of underlying systemic diseases is crucial and will aid in restoration of menstruation.
Improving fertility
Various specialized regimens can be used to help induce ovulation, including treatment with the antioestrogenic drugs clomiphene and tamoxifen, and the aromatase inhibitor, letrozole, or more complex fertility regimens utilizing more modern technologies. Therapy for intrauterine adhesions may usually be carried out with hysteroscopic adhesiolysis under direct vision followed by cyclical oestrogen stimulation, aimed to promote regeneration of the endometrial lining.
Prevention of side effects
It is recommended that patients with POI be treated with combined oestrogen-progestogen therapy to prevent bone density loss, through either an oral contraceptive pill or hormone replacement therapy.
Treatment of hyperandrogenism is directed towards treating troublesome signs and symptoms (hirsutism and acne) and preventing long-term sequelae of PCOS (endometrial hyperplasia— or cancer, metabolic dysfunction, or obesity). Antiandrogen therapy can be given using the antiandrogenic steroids spironolactone or cyproterone acetate with the COCP, generally under specialist supervision.
Society concerns, mythology, and changing society perceptions
Amenorrhoea (except in the presence of breastfeeding) has generally been regarded with fear and disfavour in most communities— reflecting influence of ‘evil spirits' and effects on fertility. In some
Genetic testing
In cases of POI and where an obvious underlying cause is uncertain, genetic testing for Turner syndrome and fragile X is suggested. In the very near future, genetic testing will become a much more important aspect of management of patients with primary or secondary amenorrhoea, in order to identify uncommon or rare genetic syndromes with significant familial implications.
Box 41.20 Principles of management of secondary amenorrhoea
• Restoration of menses
• Treatment of underlying disease
• Improvement of fertility (preservation or treatment)
• Prevention of adverse effects of untreated pathology cultures, there are beliefs that menstruation is not only necessary for internal ‘cleansing’, but also for confirming fertility potential.
Emerging evidence supports the safety and efficacy of menstrual suppression with COCP and other hormones and is leading to change in society expectations among women, who often favour a ‘bleed-free’ existence until pregnancy is desired. For many women, menstrual suppression has substantial advantages in terms of managing a range of benign gynaecological conditions, improving quality of life, reducing menstrual symptoms, and has further benefits in terms of improved contraception compliance.
Dysmenorrhoea: definitions
‘Dysmenorrhoea’, a term derived from Greek (Dys, difficult; meno, monthly; rhoea, flow), clinically refers to the symptom of menstrually related pelvic pain. It often occurs in association with other symptoms including headache, AUB, nausea, vomiting, and lethargy. Primary and secondary dysmenorrhoea differ in that primary is defined as menstrual pain that occurs in absence of identifiable ‘structural’ pelvic pathology, while secondary dysmenorrhoea is related to pelvic pathologies which can be ‘imaged’.
Primary dysmenorrhoea and secondary dysmenorrhoea are both highly variable symptom complexes, with different types of pain experience for ‘primary’ or ‘secondary’ sufferers. Primary dysmenor- rhoea is one of the commonest gynaecological complaints among adolescent girls, typically beginning 1-3 years after the onset of menstruation, coinciding with the onset of ovulation, and reaching a peak at around 17-18 years of age. It then has a tendency to spontaneously improve in the 20s and after the first pregnancy.
The secondary type of dysmenorrhoea is usually attributable to a recognizable underlying pelvic ‘structural’ lesion, which can be ‘imaged’ and identified in a defined way. Onset of secondary dysmenorrhoea tends to occur in mid to later reproductive years; however, it is now being recognized that the symptoms of pelvic pain with a condition such as endometriosis often have their onset in the adolescent years. Hence, a well-structured history is useful in distinguishing primary and secondary types of menstrual pain, and an important starting point in determining the most appropriate management.
Presentation and symptoms of dysmenorrhoea
Primary and secondary dysmenorrhoea are symptoms or symptom complexes, which may present in different ways in different types of patients (Box 41.21). Optimum management therefore depends on symptom characteristics and understanding of likely underlying causes. Young women with ‘primary dysmenorrhoea’ may experience a spectrum of associated symptoms as well as varying types of pain symptom, ranging from a dull ache and ‘tightenings’, through obvious contractions to deep colicky-type pain. These pains may range in severity from mild ‘cramps’ through to some of the most severe pains that a woman can imagine. The pains may radiate to the back, inguinal region, or legs, and can be associated with nausea, vomiting, diarrhoea, fatigue, fever, irritability, myalgia, and headaches.
The pain of primary dysmenorrhoea tends to be ‘spasmodic’ in nature, and commonly begins just prior to or at the onset of menstruation. The intensity of pain can be very severe and is sometimes associated with the amount of menstrual flow.
Conversely, secondary dysmenorrhoea is associated with a type of pelvic pain often described as ‘dragging’ or ‘congestive’ in nature, and
Box 41.21 Common characteristics of the symptoms of primary and secondary dysmenorrhoea
Primary
• Intense spasms
• Onset around beginning of menstruation
• Radiating pain (to back/legs)
• Associated symptoms (nausea, headaches)
Secondary
• Dragging-type pain, often prolonged
• May begin several days before menstruation
• Can occur variably throughout menstrual cycle
• Associated symptoms: HMB and deep dyspareunia
this may well be a component of more chronic pelvic pain, which tends to be more prolonged or erratic and can occur throughout the menstrual cycle. Chronic pelvic pain is dealt with in more detail in Chapter 44. Typically, this pain begins several days prior to menstruation, peaking with onset of bleeding. Associated symptoms can include HMB and deep dyspareunia associated with uterine tenderness.
Underlying causes, mechanisms, and contributing factors of dysmenorrhoea
Early pathophysiological studies in the 1950s and 1960s investigated the relationship between an intense rise in intrauterine pressure and spasms of pain perception in women with primary dysmenorrhoea.
This lead to the demonstration that a rise in intrauterine pressure on a background of markedly increased myometrial contractile activity caused a reduction in endometrial blood flow, in turn causing uterine ischaemia and release of pain-stimulating metabolites (13). The intrauterine pressures generated by these intense contractions can sometimes exceed 200 mm Hg, substantially higher than is experienced in obstetric labour.
Prostaglandins
Disturbances of endometrial prostaglandin metabolism are also implicated in primary dysmenorrhoea. Endometrial prostaglandins F2α and E2 can directly sensitize afferent (sensory) nerve fibres in the uterus leading to generation of pain (14).
Vasopressin and other peptides
Experimental evidence further suggests that raised endometrial and circulatory vasopressin, as well as peptides such as oxytocin, endothelins, and related prostanoid metabolites such as leukotrienes, contribute to increasing myometrial contractility, promote vasoconstriction, and contribute to uterine ischaemia (15).
Imbalance of ovarian hormones
Ovarian hormones can modulate the synthesis and release of prostaglandins and vasopressin and increase myometrial sensitivity. Increased endometrial and circulating oestradiol in the adolescent pelvis appears to stimulate vasopressin release (16).
Figure 41.2 provides a schematic diagram of factors involved in the generation of pain in women with primary dysmenorrhoea. Exacerbating factors can include cigarette smoking, obesity, and local chlamydia infection (17) and there can be a clear familial link (18).
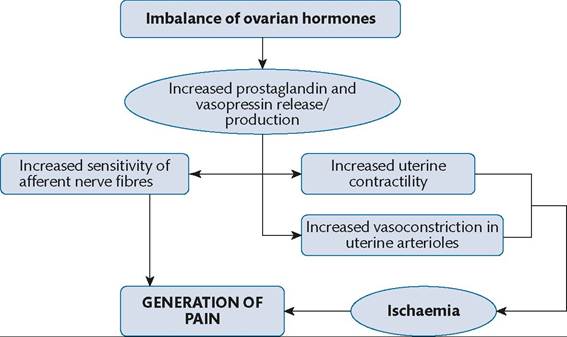
Figure 41.2 Proposed scheme of generation of uterine pain in primary dysmenorrhea.
Secondary dysmenorrhoea
Secondary dysmenorrhoea refers to the painful menstruation that is attributed to certain structurally identifiable, and usually ‘inflammatory’, pelvic pathologies. These structural lesions can contribute to generation of pain directly by distorting the pelvic anatomy (including nerves) or indirectly via production of inflammatory and other molecules that stimulate the triggering or persistence of pain signals. These lesions are also generally tender to palpation.
Some common causes of secondary dysmenorrhoea are listed and described in Box 41.22.
Most ovarian cysts may cause pelvic pain by intermittent torsion, but probably not dysmenorrhoea, except in the case of endometriotic ovarian cysts.
Endometriosis
Endometriosis is a common condition characterized by presence of endometrial-like glands and stroma that develop into lesions at sites outside the uterus, especially on the pelvic peritoneum, in the deeper pelvis, or in the ovaries in the form of local endometriotic cystic lesions, commonly causing intense menstrually related pain. Similar endometriosis pains can also occur at other times of the cycle as erratic, chronic pelvic pain. This disease is a complex and variable condition, which is comprehensively addressed in Chapter 45.
Adenomyosis
Adenomyosis is characterized by the presence of endometrial glands and stroma within the myometrium, and the severity of
Box 41.22 Common causes of secondary dysmenorrhoea
• Structural lesions usually with an inflammatory component:
- Endometriosis
- Adenomyosis
- Leiomyomas
- Chronic pelvic inflammatory disease
- Endometrial polyps
• Other causes:
- Congenital (imperforate hymen, non-communicating uterine horn, transverse vaginal septum)
- Psychological factors dysmenorrhoea is often associated with the depth and extent of myometrial ‘invasion’. This condition is now recognized to be common in older women in the reproductive age-groups, and it can be well imaged by the latest ultrasound equipment with experienced gynaecological operators, and by modern MRI. It is typically associated with HMB, secondary dysmenorrhoea, and deep dyspareunia; however, many cases of adenomyosis are not associated with obvious symptoms. Many cases of this disease coexist with other benign gynaecological diseases, such as endometriosis, endometrial polyps, leiomyomas, and endometrial hyperplasia, with each or sometimes even none of these diseases contributing to symptoms. These conditions need much more attention with research into their associations and varied symptoms.
Uterine leiomyomas (myomas, fibroids)
Commonly referred to as ‘fibroids’, uterine leiomyomas (benign, smooth-muscle tumours within the myometrium) can be associated with HMB, and chronic, dragging, and sometimes colicky pain. While many women suffering from myomas can remain asymptomatic, the submucous myomas, which protrude into the uterine cavity are more likely to be associated with dysmenorrhoea and particularly heavy HMB. These tumours are described in detail in Chapter 49.
Chronic pelvic inflammatory disease
Chronic pelvic inflammatory disease usually follows a delayed or inadequately treated acute pelvic infection or, less frequently, spontaneous, induced abortion or normal delivery with retained intrauterine products of conception (Chapter 43). Infection may be caused by specific local bacterial (gonorrhoea), rickettsial (chlamydia) or viral (human papilloma virus, HPV) organisms acting in the sensitized or damaged pelvic tissues. Pelvic inflammatory disease is usually associated with local tenderness, dyspareunia, and chronic, dragging pain, and is often maximal prior to onset of menstruation.
Endometrial polyps
Endometrial and cervical polyps are a common cause of irregular uterine bleeding and sometimes HMB, and dysmenorrhoea is an occasional, accompanying symptom.
Ovarian cysts can be associated with ovarian torsion, with intracyst haemorrhage, or with local infection. These pathologies can cause various types of acute or semi-acute pelvic pain, but rarely pain that is labelled as ‘dysmenorrhoea’. The only type of ovarian cyst which is frequently associated with ‘secondary dysmenorrhoea’ is endometriosis.
It should not be forgotten that pain from other organs, such as the bowel or the renal tract, may sometimes mimic dysmenorrhoea.
Mechanisms of pain generation with secondary dysmenorrhoea
Pain associated with endometriosis has been given much more research attention than adenomyosis, leiomyomas, or polyps, and it is clear that the mechanisms of secondary dysmenorrhoea and chronic pelvic pain with endometriosis are complex.
Experimental evidence shows that the endometrium of women with endometriosis is innervated with sensory and sympathetic nerve fibres, which are not usually present in women without the disease. These nerve fibres are also present within the endometriotic lesions and adhesions, along with the expression of multiple inflammatory and neural mediators, contributing to the generation of pain signals. Nociceptors in the sensory nerve fibres, tissue distortion, and ischaemia also contribute to the origin of pain signals.
There are multiple neural pathways through pelvic nerve tracts and neural ganglia leading to the dorsal root ganglia and afferent spinothalamic tracts within the spinal cord. These modulated signals are finally processed in centres within the thalamus and basal brain centres prior to onward referral to the cerebral cortex where they are finally ‘perceived’. Other factors, such as psychological factors, influence this interpretation and ultimately perception of pain differs greatly between individuals.
History, examination, and investigations for dysmenorrhoea
History
Initial assessment of dysmenorrhoea begins with a structured history (Box 41.23). This is important in order to characterize pain and to determine the likely origin.
Examination
Examination is not usually indicated when history is suggestive of classical primary dysmenorrhoea and in patients who have not previously been sexually active. However, full examination including
Box 41.23 History-taking for dysmenorrhoea
Box 41.24 Exam characteristics for dysmenorrhoea
• General appearance, abdominal exam
• Pelvic exam—inspection of external genitalia
• Assess for lesions, discharge, point tenderness
• Bimanual exam—cervical motion tenderness, uterine size, mobility, adnexal masses/tenderness, uterosacral nodularity
• Speculum exam
• With or without per rectal exam
bimanual and speculum examination may be particularly useful in assessing secondary dysmenorrhoea (Box 41.24).
Investigations
Initial investigations including routine Pap smear and vaginal swabs for infection are an integral part of the pelvic exam. This is often followed by a good-quality transvaginal ultrasound, which may highlight need for further hysteroscopic or laparoscopic intervention (Box 41.25). Hysteroscopy can reveal the appearance of polyps (endometrial and cervical), myomas, adenomyosis, hyperplasia, cancer (although these do not usually present with pelvic pain at an early stage), and infection
Management of primary dysmenorrhoea
A good structured history is often sufficient in identification of primary dysmenorrhoea. These patients should be managed with a trial of suitable analgesics (with strict instructions on how these analgesics should be taken) and this can usually be managed at the level of the general practitioner. Specialist advice may be sought when initial management has failed or in those in whom compliance may be a problem. Optimum medical management depends on precise definition of symptoms and exclusion of structural lesions as possible underlying causes.
Medical management
Mild analgesics
Paracetamol and a wide range of marketed combinations with codeine phosphate, doxylamine, or dextropropoxyphene can be effective in mild dysmenorrhoea.
Prostaglandin inhibitors (NSAIDs)
A range of prostaglandin inhibitors can produce good clinical effect in up to 90% of sufferers. Commonly used NSAIDs include ibuprofen, naproxen sodium, mefenamic acid, and diclofenac sodium. A double dose is usually recommended as the starting dosage to gain initial pain control. Ongoing dosage is usually tailored to response of the primary dysmenorrhoea, but is recommended to be one or two tablets/capsules every 6-8 hours while the pain is severe. Pain relief is not usually needed for more than 2-3 days for primary dysmenorrhoea. Some users experience side effects which are dose related, mainly nausea and gastrointestinal.
• Nature of pain:
— Site
— Onset and duration
— Character
— Severity
— Exacerbating/relieving factors
• General medical history
• Menstrual and sexual history
• Family history (endometriosis, bowel disease, interstitial cystitis, inflammatory conditions and malignancy)
• Effect on quality of life
Box 41.25 Potential investigations for dysmenorrhoea
• Pap smear (at time of speculum examination)
• High vaginal swab/chlamydia and gonorrhoea polymerase chain reaction
• Pelvic/transvaginal ultrasound (becoming routine)
• MRI (rarely needed)
• Hysteroscopy with or without excision
• Diagnostic laparoscopy with or without excision
Combined oestrogen-progestogen oral contraceptive pills
These agents can be very effective in suppressing moderate to severe primary dysmenorrhoea. Combined oral contraceptives have been shown to reduce prostaglandin and vasopressin receptor activity and thus reduce uterine contractility and sensitivity. Monophasic pills with a strong progestogenic balance tend to be most effective, likely attributed to more effective suppression of endometrial proliferation, development, and prostaglandin production.
Levonorgestrel-releasing intrauterine system
The LNG-IUS is highly effective in suppressing endometrial proliferation and local prostaglandin production. In many patients it induces complete amenorrhoea and markedly reduces any complaint of primary dysmenorrhoea.
Other agents
Other agents, which have been utilized in the past for treatment of primary dysmenorrhoea, include danazol, GnRH agonists, and common antihypertensive agents such as calcium channel blockers and beta-blockers. These agents can induce endometrial atrophy, reduce uterine contractility, and promote relaxation of uterine muscle, reducing the symptoms of dysmenorrhoea. However, these agents are rarely used in modern management and their use is limited by their side effects.
Surgical management
Various surgical methods can be used to aid in diagnosis and management of dysmenorrhoea.
• Diagnostic laparoscopy, lesion biopsy, and endometrial biopsy.
• Presacral neurectomy: is rarely used nowadays, has limited levels of benefit and can have permanent adverse effects on bowel function.
• Laparoscopic laser uterine nerve ablation: has also lost popularity and is now recognized to have limited benefits.
• Hysteroscopic endometrial ablation or hysterectomy: these relatively major surgical procedures are regarded as unnecessarily extensive for primary dysmenorrhoea.
• Cervical dilatation has limited symptomatic benefits, and can cause cervical damage through tearing of the cervical muscular and fibrous structure.
Adjuvant therapy
Numerous other therapies for alleviation of dysmenorrhoea have been tried, and these may include dietary changes, smoking cessation, exercise, heat compresses, acupuncture, and transcutaneous nerve stimulation. Limited benefit occurs in some users.
Management of secondary dysmenorrhoea
Management of secondary dysmenorrhoea usually relies on effective management of underlying pathology. This may require a combination of medical and surgical approaches. Simple analgesics and prostaglandin inhibitors (NSAIDs) generally work less well with the pain symptoms of secondary as opposed to primary dys- menorrhoea, and patients may respond more effectively to a higher NSAID dosage, a combination of agents, or stronger analgesic agents (such as tramadol or oxycodone) to achieve optimum pain control. Nowadays, it is wise to refer to up-to-date pharmacological recommendations on dosage (using a current ‘App’ such as ‘iMIMS’).
Management is further challenged by the erratic nature of chronic pelvic pain, which may be exacerbated at menstruation, but may also be present at other times of the cycle. Surgical excision of underlying conditions such as endometriosis, adenomyosis, uterine fibroids, and even endometrial polyps usually requires a highly specialized, skilled, and planned laparoscopic, hysteroscopic, or laparotomy approach.
Society impact
Primary dysmenorrhoea tends to affect women during their early reproductive years (typically during adolescence), while secondary dysmenorrhoea is more commonly seen in the later reproductive years. Both of these two symptoms can have a major impact on quality of life for the woman, and those around her. It may impact self-esteem, time with family, and quality of both social and sexual life. Many women need to take time off from school and from work. In modern Western society, especially among younger, professional women, there is a steadily increasing desire for a ‘bleed-free’ and ‘pain-free’ existence, as far as menstruation is concerned. This scenario and these expectations are becoming much more widespread through the impact of modern social media.
The discussed hormonal and other therapies have additional powerful social benefits in that they reduce the amount of monthly bleeding, the associated menstrual pain, other menstrual symptoms, and the associated social impacts for the woman, her quality of life, her family, and her workplace.
Prognosis
Primary dysmenorrhoea tends to spontaneously improve with time as a woman moves into her 20s, and after a first full-term pregnancy, but may continue for many years. Secondary dysmenorrhoea, on the other hand, tends to progress and become worse with time for many women, unless effectively treated. Both types of symptoms can have a severe impact on the quality of life for sufferers.
Summary
This section has presented practical clinical information on two of the commonest symptoms encountered in gynaecology, and has highlighted the important and common underlying causes in a context of the important investigations. These two symptoms can play havoc with the daily lives of women who experience moderate or severe variations.
Understanding of the symptom presentations and the differential diagnoses are critical in determining the most relevant medical or surgical managements for individual women.
Many modern young women (in most cultures) are demonstrating an increasing societal change within health lifestyles in seeking an existence where menstruation is ‘switched off’ until ovulation is required when seeking a pregnancy. The convenience of pharmacological amenorrhoea is being increasingly recognized as a component of modern business and social lifestyles. This social change is
likely to continue and health professionals will need to understand the clinical importance of different causes of amenorrhoea.
Dysmenorrhoea is very common in all societies and can be a major contributor to a significant level of incapacity during menstruation. HMB is often accompanied by menstrual pain, and women with combined HMB and pain are significantly more likely to present with the symptoms to a doctor than women with HMB alone.
These two symptoms are so common and so intrusive into the modern lifestyle that a sound understanding of their impact is essential for the modern doctor. Indeed, these symptoms have an impact, as an important comorbidity, on most medical conditions in women. Further, these are symptoms which rely on a carefully taken case history in order to understand their main impacts on the woman and possible interactions with other medical conditions.