Anatomy of the Female Pelvis
Lauren Owens
Isabel Green
ABDOMINAL WALL
The anterior abdominal wall lies ventrally and is outlined superiorly by the lower edge of the rib cage; caudally by the iliac crests, inguinal ligaments, and pubic bone; and dorsolaterally by the lumbar spine and adjacent muscles.
Layers of the Anterior Abdominal Wall
• Skin
• Subcutaneous layer: This consists of fat globules in a meshwork of fibrous septa. Camper fascia is the more superficial aspect of the subcutaneous layer.
P.327 Scarpa fascia is the deeper portion and has a more organized consistency than Camper fascia secondary to more fibrous tissue.
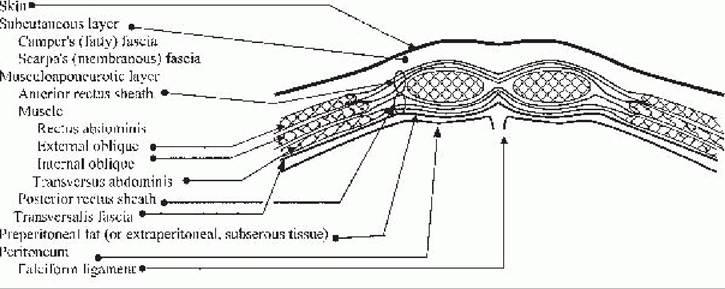
Figure 26-1. Layers of the anterior abdominal wall cephalad to the arcuate line.
• Musculoaponeurotic layer: Located immediately below the subcutaneum, the musculoaponeurotic layer consists of layers of fibrous tissue and muscles that hold the abdominal viscera in place.
• Rectus sheath: The aponeuroses of the external oblique, internal oblique, and transversus abdominis muscles comprise the rectus sheath.
• The anterior rectus sheath is anatomically different above and below the arcuate line. The arcuate line (linea semicircularis, semilunar fold of Douglas) is located midway between the umbilicus and symphysis pubis. It marks the lower edge of the posterior rectus sheath.
î Above the arcuate line, the anterior rectus sheath is composed of the aponeuroses of the external oblique and ventral half of the internal oblique muscles. The posterior rectus sheath is composed of the aponeuroses of the dorsal half of the internal oblique and transversus abdominis muscles (Fig. 26-1).
î Below the arcuate line, the anterior rectus sheath is composed of the aponeuroses of all the muscles previously mentioned (Fig. 26-2).
î The linea alba is the midline between the rectus abdominis muscles.
Above the arcuate line, the lineaalba marks the fusion of the anterior and posterior rectus sheaths.
• Abdominal wall muscles
• Oblique flank muscles lie lateral to the rectus abdominis muscles.
î The external oblique muscle originates from the lower eight ribs and iliac crest and runs obliquely, anteriorly, and inferiorly.
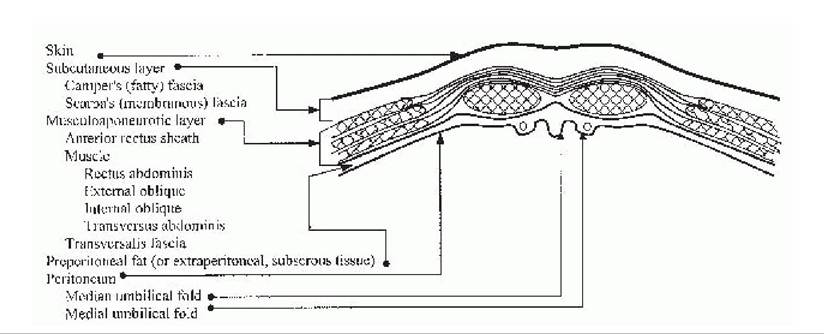
Figure 26-2. Layers of the anterior abdominal wall caudal to the arcuate line.
P.328 î The internal oblique muscle originates from the anterior two thirds of the iliac crest, the lateral part of the inguinal ligament, and the thoracolumbar fascia in the lower posterior flank. It runs obliquely, anteriorly, and superiorly.
î The transversus abdominis muscle runs transversely, originating from the lower six costal cartilages, the thoracolumbar fascia, the anterior three fourths of the iliac crest, and the lateral inguinal ligament. The nerves and vasculature of the flank are found between the internal oblique and transversus abdominis muscles and, therefore, are susceptible to injury in transverse incisions.
• Longitudinal muscles
î The rectus abdominis muscle is a paired muscle, found on either side of the midline, originating from the sternum and cartilage of ribs 5 through 7 and inserting into the anterior surface of the pubic bone.
î The pyramidalis muscle is a vestigial muscle with a variable presence among individuals. It arises from the pubic bone and inserts into the linea alba several centimeters cephalad to the symphysis ventral to the rectus abdominis muscle.
• The transversalis fascia is a layer of fibrous tissue, located underneath the abdominal wall muscles and outside the peritoneum. The transversalis is separated from the peritoneum by a variable layer of adipose tissue.
• Peritoneum: A single layer of serosa lines the posterior aspect of the anterior abdominal wall. Five vertical folds converge toward the umbilicus.
• The median umbilical fold is a single fold created by the median umbilical ligament or obliterated urachus.
î The apex of the bladder blends into the median umbilical ligament and is highest in the midline. This relationship should be considered when entering the peritoneal cavity.
• The medial umbilical folds are paired folds lateral to the median umbilical fold, remnants of the obliterated
umbilical arteries; they converge at the umbilicus.
• The lateral umbilical folds are paired folds caused by the inferior epigastric vessels.
Vasculature of the Abdominal Wall
• Subcutaneous vascular supply (Fig. 26-3)
• The superficial epigastric artery branches from the femoral artery after it descends through the femoral canal. It runs superomedially, approximately 5 cm lateral to the midline.
• The superficial circumflex iliac artery branches from the femoral artery and runs laterally toward the flank.
• Musculofascial blood supply parallels the subcutaneous supply (see Fig. 26-3).
• The inferior epigastric artery branches from the external iliac artery, proximal to the inguinal ligament. It runs cephalad, deep to the transversalis fascia and lateral to the rectus muscle. Midway between the pubis and umbilicus, the vessels intersect the lateral border of the rectus muscle and course between the dorsal aspect of the rectus and the posterior rectus sheath. These vessels run between 4 and 8 cm lateral to the midline. After entering the posterior rectus sheath, numerous branches supply all layers of the abdominal wall and anastomose with the superior epigastric vessels.
• The superior epigastric artery branches from the internal thoracic artery and runs caudally to form anastomoses with the inferior epigastric artery.
• The deep circumflex iliac artery also branches from the external iliac artery and runs laterally between the internal oblique and transversus abdominis muscles.
P.329
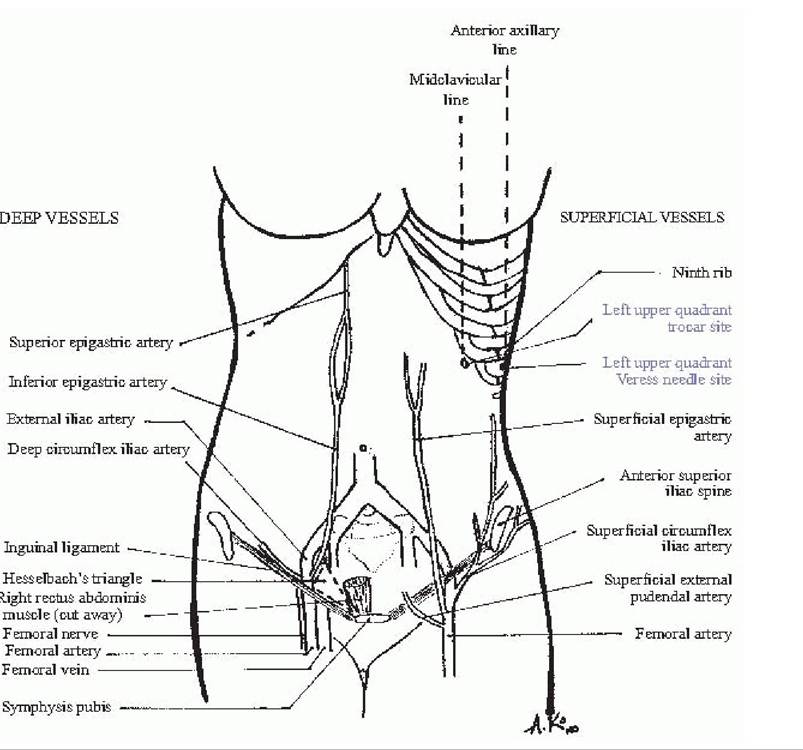
Figure 26-3.
Vasculature and laparoscopic landmarks of the anterior abdominal wall. (Original drawing by Alice W. Ko from Bankowski BJ, Hearne AE, Lambrou NC, eds. The Johns Hopkins Manual of Gynecology and Obstetrics, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002.)Abdominal Wall Incisions
• Vertical: A midline incision provides optimal exposure to the abdomen. The incision is made from the symphysis to below the umbilicus, depending on how much space is needed. A small incision or “mini-lap” may offer excellent visualization and improved cosmesis. The incision can always be extended more cephalad and then circumferentially around the umbilicus to the left to avoid the ligamentum teres. The anterior rectus sheath is incised longitudinally. The peritoneum is entered taking care to avoid the superior aspect of the bladder.
• Pfannenstiel incision: This is one of the most common incisions in obstetrics and gynecology. A transverse incision is made approximately two fingerbreadths (3 to 4 cm) above the pubic symphysis. Transverse incisions are generally less painful and more cosmetic than longitudinal incisions as they run along Langer lines. The incision is continued through the rectus sheath, and then the rectus muscles are dissected cephalad and caudad off the posterior aspect of the rectus sheath. Then, the rectus muscles are separated in the midline to gain entry to the peritoneum through a midline longitudinal incision. The degree of separation of the rectus
P.330 fascia from the underlying rectus muscles determines the amount of exposure provided by the Pfannenstiel incision. If more space is needed, the rectus fascia can be separated from the rectus muscle up to the umbilicus. Lateral extension of the skin incision runs a greater risk of injury to the ilioinguinal and iliohypogastric nerves either by direct incision or more often by entrapment during fascial closure.
• Cherney incision: A modification of the Pfannenstiel incision, the Cherney incision provides better exposure to the pelvis than the Pfannenstiel.
After the rectus muscle is dissected off the fascia, as in a Pfannenstiel, the tendinous insertion of the rectus muscle is cut approximately 0.5 cm above the insertion site at the posterior aspect of the pubic bones. The rectus bellies are then moved cephalad, providing excellent exposure to the pelvis. Note the importance of leaving enough tendons on the pubic bone so that the caudal aspect of the rectus muscles can be reapproximated to the tendon with a delayed absorbable suture in a horizontal mattress fashion during closure.• Maylard incision: The Maylard incision provides the best pelvic exposure of all the incision types. This incision is transverse, like the Pfannenstiel, with two main differences. The Maylard incision is made slightly more cephalad (at the level of the anterior superior iliac spine), and the rectus muscles are not dissected off the fascia. Rather, they are left attached to the rectus sheath and the muscles are transected. The inferior epigastric vessels are identified and ligated before the rectus muscles are transected completely. This helps to prevent blood loss from inadvertent inferior epigastric injury and also serves to preserve blood supply. This type of incision has the potential for greater blood loss but also for better pelvic exposure.
Abdominal Landmarks for Laparoscopy
• Primary laparoscopic trocars are placed for initial access. In gynecology, these are most often placed at the umbilicus or in the left upper quadrant. Accessory trocars may be placed suprapubically or laterally (see Fig. 26-3).
• Umbilical trocar: The umbilical trocar should be placed at a 45-degree angle in thin women in order to avoid hitting the aorta or common iliacs. In an obese patient, the trocar can be placed at a more perpendicular angle due to the amount of adipose tissue that must be traversed.
• Left upper quadrant trocar: A trocar may be placed at Palmer point, 3 cm below the left costal margin in the midclavicular line. Prior to trocar insertion, the stomach should be emptied with a nasogastric tube.
This location is preferred in patients with prior midline surgery to avoid potential visceral adhesions.• Suprapubic trocar: The suprapubic trocar is placed two fingerbreadths above the pubic symphysis. It is placed under direct visualization and after Foley insertion in order to assure that the bladder is not in line of the trocar path.
• Lateral trocars: The lateral trocars are placed at least 5 cm cephalad to the pubic symphysis and 8 cm lateral to the midline in order to avoid the inferior epigastric vessels. The trocar is placed under direct visualization lateral to the lateral umbilical folds to avoid injury to the inferior epigastric vessels.
PELVIC VISCERA
Vagina
• The vagina is shaped like a flattened tube, starting at the distal hymenal ring and ending at the fornices surrounding the proximal cervix. Its average length is 8 cm; this varies greatly with age, parity, and surgical history.
P.331
• The vaginal epithelium is nonkeratinized, stratified squamous epithelium lacking mucous glands and hair follicles.
• Deep to the epithelium is the vaginal muscularis or endopelvic fascia. The term fascia is misleading because this is actually fibromuscular tissue that includes fibroblasts, smooth muscle cells, and elastin, in addition to type I and III collagen, all loosely arrayed to create an elastic supportive layer. At the vaginal apex, this fibromuscular layer coalesces to create the cardinal and uterosacral ligaments. The fanshaped cardinal ligament creates a sheath that envelops the uterine artery and vein, fusing medially with the paracervical ring. The uterosacral portion inserts into the posterior and lateral aspect of the paracervical ring and then curves laterally along the pelvic sidewall to attach to the presacral fascia that overlies the second, third, and fourth sacral vertebrae. Together, the cardinal and uterosacral ligaments pull the vagina proximally toward the sacrum, suspending it over the muscular levator plate.
• The endopelvic fascias of the anterior and posterior vaginal wall are known as the pubocervical fascia and rectovaginal fascia, respectively. Again, these layers are not true fasciae but composed of fibromuscular sheets. Superiorly, the pubocervical fascia attaches to the cervix and the cardinal/uterosacral support of the vaginal apex. Laterally, it coalesces with the fascia of the obturator internus muscle to create the arcus tendineus fascia pelvis (ATFP) or “white line.” Inferiorly, it attaches to the pubic symphysis. The rectovaginal fascia in the upper vagina coalesces with the lateral support of the anterior vaginal wall and fuses with the ATFP. The lower half of the rectovaginal fascia fuses with the aponeurosis of the levator ani muscles along a line referred to as the arcus tendineus fascia rectovaginalis. At its most inferior point, the rectovaginal septum fuses with the perineal body (Fig. 26-4).
Uterus
• The uterus is a fibromuscular organ composed of the corpus and the cervix.
• Corpus: The endometrium is the innermost lining of the uterus made up of columnar epithelium and specialized stroma. The superficial layer of the endometrium contains hormonally sensitive spiral arterioles, which shed with each cycle. The myometrium contains interlacing smooth muscle fibers, and the serosal surface of the uterus is formed by peritoneal mesothelium. The fundus is the portion of the uterus cephalad to the endometrial cavity. The cornua are located where the fallopian tubes insert into the uterine cavity, lateral to the fundus.
• Cervix: The cervix is generally 2 to 4 cm in length and has two parts: the portio vaginalis (protruding into the vagina) and the portio supravaginalis (lying
P.332 above the vagina). The cervix is made up of dense fibrous connective tissue and is surrounded in a circular fashion by a small amount of smooth muscle into which the cardinal and uterosacral ligaments and pubocervical and rectovaginal fascia insert. The cervix contains a central longitudinal canal connecting the endometrial cavity with the vagina, called the endocervical canal. The internal os of the cervix is at the junction of the endocervical canal and the endometrial cavity. The external os is the distal opening of the cervical canal to the vagina. The squamocolumnar junction is located at the external os. It marks the transition from the squamous epithelium of the ectocervix to the columnar epithelium of the endocervical canal at the external os. The squamocolumnar junction is sampled with Pap smears and is a common site for cervical dysplasia and cancer. The ectocervix is the outer portion of the cervix.
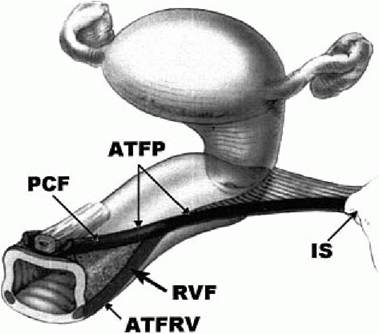
Figure 26-4. Illustration of attachment of rectovaginal fascia (RVF) and arcus tendineus fascia pelvis (ATFP) to the pelvic sidewall. RVF represents the ideal line of suture placement during lateral defect repair. PCF, pubocervical fascia; ATFRV, arcus tendineus fascia rectovaginalis; IS, ischial spine. (From Leffler KS, Thompson JR, Cundiff GW, et al. Attachment of the rectovaginal septum to the pelvic sidewall. Am J Obstet Gynecol 2001;185:43, with permission.)
Ligaments of the Uterus
• These ligaments are formed by thickening of the endopelvic fascia or folds of peritoneum.
• The round ligament courses from the anterolateral aspect of the uterine corpus through the inguinal canal to insert into the labia majora. It has a fibromuscular element and can give rise to leiomyomas. It contains the artery of Sampson. This ligament provides no support for the uterus.
• The utero-ovarian ligament contains the anastomotic vasculature of the uterine and ovarian vessels and connects the uterus and ovaries.
• The cardinal ligaments (Mackenrodt ligaments) extend from the lateral pelvic walls and insert into the lateral portion of the vagina, uterine cervix, and isthmus. These contain both the uterine artery and vein and play an important role in support of the pelvic organs.
• The infundibulopelvic ligament (IP ligament, suspensory ligament of the ovary) contains the ovarian vessels. The ovarian arteries branch directly off the aorta. The right ovarian vein feeds into the inferior vena cava, whereas the left vein drains into the left renal vein.
• The uterosacral ligaments extend from the sacral fascia and insert into the posterior portion of the uterine isthmus and endopelvic fascia. They are composed of connective tissue and smooth muscle and contain the autonomic sympathetic and parasympathetic nerves of the pelvic organs. Together, the cardinal and uterosacral ligaments form the parametrium and play an important role in pelvic organ support.
• The broad ligament is the peritoneum that covers the uterus and fallopian tubes. It forms a mesentery around the uterine structures: The mesoteres surrounds the round ligament, the mesosalpinx contains the fallopian tube, and the mesovarium contains the utero-ovarian ligament.
Adnexa
• The fallopian tubes are bilateral tubular structures that connect the endometrial cavity to the peritoneal cavity. They are, on average, 10 cm in length. Distally, the tubes have a fimbriated end that receives each ovum after ovulation. The lumen is lined by ciliated columnar epithelium. The fallopian tube has four regions (from proximal to distal): interstitial, isthmic, ampullary, and infundibular.
• The ovaries are bilateral, white, flattened oval structures that store ova. The ovary is suspended laterally from the pelvic sidewall by the IP ligament and medially from the uterus by the utero-ovarian ligament. Each ovary rests in the ovarian fossa (fossa of Waldeyer), which is bordered dorsomedially by the hypogastric artery and ventrolaterally by the external iliac artery. The ureter runs at the base of this fossa. The ovary has a fibromuscular and vascular medulla and an outer cortex that contains
P.333 specialized stroma with follicles, corpora lutea, and corpora albicantia. The ovary is covered by cuboidal epithelium.
Ureter
• The ureter courses from the kidneys retroperitoneally, crosses the pelvic brim at the level of the bifurcation of the common iliac artery, and continues in the medial leaf of the broad ligament. It enters the tunnel of Wertheim as it passes under the uterine artery 1.5 cm lateral to the cervix at the level of the internal cervical os and enters the trigone of the bladder. The three most common areas of ureteral injury during gynecologic surgery are at the pelvic brim during clamping of the IP ligaments, during clamping of the uterine artery at time of hysterectomy, and near the trigone when mobilizing the bladder off the lower uterine segment.
SURGICAL SPACES OF THE PELVIS
The reproductive, urinary, and gastrointestinal organs found in the pelvis have the ability to change their size and shape independently of each other, which is made possible by their loose attachments via connective tissue planes composed of fat and areolar tissue. These planes are potential spaces that can be entered with surgical dissection. The neurolymphovascular supply to the organs remains in the connective tissue septae, permitting blunt and bloodless dissection of the surgical spaces. Eight avascular spaces are described: prevesical, vesicovaginal, paravesical (2), pararectal (2), rectovaginal, and retrorectal (Fig. 26-5).
• The prevesical space, also known as the space of Retzius or retropubic space, is separated ventrally from the rectus abdominis by the transversalis fascia. Laterally, the muscles of the pelvic wall, cardinal ligament, and attachment of the pubocervical fascia to the ATFP border the prevesical space. Important structures within the space of Retzius include the dorsal clitoral vessels, obturator nerves and vessels, nerves of the lower urinary tract, iliopectineal line, ATFP, and the arcus tendineus levator ani. Burch urethropexies are performed in this space.
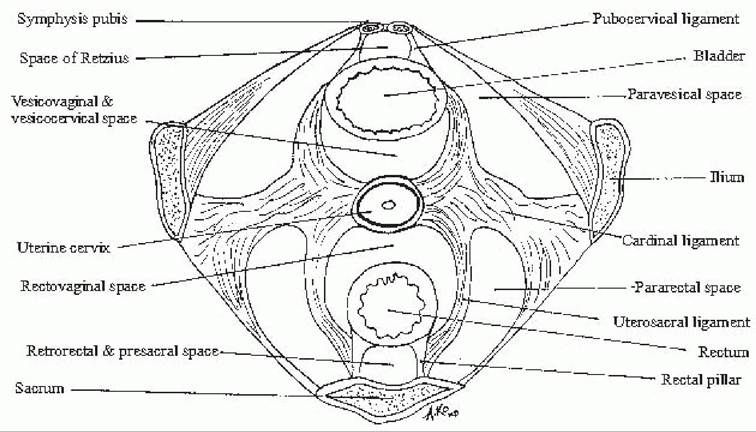
Figure 26-5. Surgical spaces of the pelvis. (Original drawing by Alice W. Ko from Bankowski BJ, Hearne AE,
Lambrou NC, eds. The Johns Hopkins Manual of Gynecology and Obstetrics, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002.)
P.334
• The vesicovaginal spaces (also called vesicocervical) are separated by a thin supravaginal septum. The spaces are bound caudally by the fusion of the junction of the proximal one third and distal two thirds of the urethra with the vagina, ventrally by the urethra and bladder, cephalad by the peritoneum, forming the vesicocervical reflection. This is the space entered when developing a “bladder flap” during cesarean delivery or hysterectomy.
• The paravesical spaces are paired spaces adjacent to the bladder. They are bordered medially by the bladder and obliterated umbilical artery, laterally by the obturator internus, dorsally by the cardinal ligament, ventrally by the pubic symphysis, and caudally by the levator ani. The ureter can be found in the tissue between the paravesical and vesicovaginal spaces. Parametrial tissue obtained in a radical hysterectomy is located between the paravesical and pararectal spaces.
• The pararectal spaces are paired spaces adjacent to the rectum. The space is bordered medially by the ureter, uterosacral ligament, and rectum; laterally by the hypogastric vessels and pelvic wall; ventrolaterally by the cardinal ligament; and dorsally by the sacrum. The coccygeus forms the floor of this space. Bleeding can be encountered from the lateral sacral and hemorrhoidal vessels if dissection is carried to the pelvic floor. These spaces allow access to the sacrospinous ligaments, as well as identification of the ureter for ureterolysis when indicated.
• The rectovaginal space is bordered caudally by the apex of the perineal body; laterally by the uterosacral ligament, ureter, and rectal pillars; ventrally by the vagina; and dorsally by the rectum. The pouch of Douglas or posterior cul-de-sac is the space between the uterus and rectum bounded inferiorly by the peritoneum. The rectovaginal space is below this peritoneum and cul-de-sac and is developed by incising the peritoneal fold between the uterus and rectum.
• The retrorectal space is caudal to the presacral space and bordered ventrally by the rectum, posteriorly by the sacrum, and laterally by the uterosacral ligaments. The presacral space is bordered laterally by the internal iliac arteries, cephalad by the bifurcation of the aorta, dorsally by the sacrum, and ventrally by the colon. It contains the presacral nerve (superior hypogastric plexus), the middle sacral artery and vein (originating from the dorsal aspect of the aorta and vena cava), and the lateral sacral vessels. This space is entered for sacrocolpopexy for pelvic organ prolapse, presacral neurectomy for pelvic pain, and para-aortic lymph node dissection.
VASCULATURE OF THE ABDOMEN AND PELVIS
• Aorta: From cephalad to caudad, the arteries that stem from the aorta below the diaphragm are inferior phrenic, celiac trunk, suprarenal, superior mesenteric, renal, lumbar, ovarian, inferior mesenteric, and median sacral. The aorta then bifurcates into the common iliac arteries at the level of the fourth lumbar vertebra.
• Celiac trunk: The celiac trunk has three main branches: the left gastric, the splenic, and the common hepatic arteries. The left gastric artery divides into the esophageal branches and branches that supply the lesser curvature of the stomach. The splenic artery divides into pancreatic branches: short gastric arteries, which supply the fundus of the stomach, and the left gastroepiploic artery, which supplies the greater omentum and the greater curvature of the stomach. The left gastroepiploic artery anastomoses with the right gastroepiploic, which is a terminal branch of the common hepatic. The common hepatic artery has two main divisions: the proper hepatic artery and the gastroduodenal artery. The proper hepatic artery divides into the right gastric artery and enters the lesser omentum to anastomose with the left gastric artery and
terminates into the right and left hepatic arteries. The cystic
P.335 artery often branches from the right hepatic artery and supplies the gallbladder. The gastroduodenal artery branches into the supraduodenal artery, the right gastroepiploic artery, and the superior pancreatoduodenal artery. The right gastroepiploic artery enters the greater omentum and anastomoses with the left gastroepiploic artery along the greater curvature of the stomach. The superior pancreatoduodenal artery supplies the second part of the duodenum and the head of the pancreas.
• The superior mesenteric artery branches into the jejunal and ileal artery branches, the ileocolic artery, the right colic artery, and the middle colic artery.
• The inferior mesenteric artery branches into the left colic artery, the sigmoid branches, and the superior rectal artery.
• Ovarian vessels: The ovarian arteries originate from the anterior aspect of the aorta and course toward the pelvis, crossing laterally over the ureters at the level of the pelvic brim and passing branches to the ureters and fallopian tubes. They then cross medially over the proximal external iliac vessels and run medially in the infundibulopelvic ligaments. The left ovarian vein drains into the left renal vein, whereas the right ovarian vein drains directly into the inferior vena cava.
• The aorta bifurcates into the common iliac arteries at the level of the fourth lumbar vertebra. The common iliac then bifurcates into the external and internal (hypogastric) arteries. The hypogastric artery divides into an anterior and posterior division 3 to 4 cm after the branching off of the common iliac artery. The ureter courses anteriorly to the division of the hypogastric and external iliac arteries.
• Anterior division of the hypogastric artery: Some variance exists in the branching pattern. The branches include the obturator, uterine, vaginal, inferior, and superior vesicals; middle rectal; internal pudendal; and inferior gluteal arteries. The ureter passes laterally under the uterine artery at the level of the internal cervical os. During hypogastric artery ligation, the anterior division of the hypogastric artery should be doubly ligated with 1-0 silk (do not divide) 2.5 to 3.0 cm distal to the bifurcation of the common iliac. The dissection is done laterally to medially to avoid damaging the hypogastric vein.
• Posterior division of the hypogastric artery: The branches include the iliolumbar, lateral sacral, and superior gluteal arteries, all of which have anastomosing channels in the pelvis.
• External iliac artery: The deep epigastric and deep circumflex iliac arteries branch from the external iliac artery before it travels under the inguinal ligament and into the femoral canal, where it becomes the femoral artery.
• Anastomoses: The superior rectal artery branches off the inferior mesenteric artery, the middle rectal artery branches off the anterior division of the hypogastric artery, and the inferior rectal artery branches off the pudendal artery (a branch of the hypogastric). This allows for redundant blood flow to the pelvis.
VULVA AND PERINEUM
External Anatomy
• The bony pelvic outlet is bordered anteriorly by the ischiopubic rami and posteriorly by the coccyx and sacrotuberous ligaments. The outlet can be divided into anterior and posterior triangles sharing a common base along a line between the ischial tuberosities.
• Skin and subcutaneous layer (Fig. 26-6). The subcutaneous tissue has two nondiscrete layers: Camper fascia and Colles fascia.
• Camper fascia includes the continuation of this layer from the anterior abdominal wall.
• Colles fascia is similar to Scarpa fascia of the anterior abdominal wall. It fuses posteriorly with the perineal membrane and laterally with the ischiopubic rami.
P.336
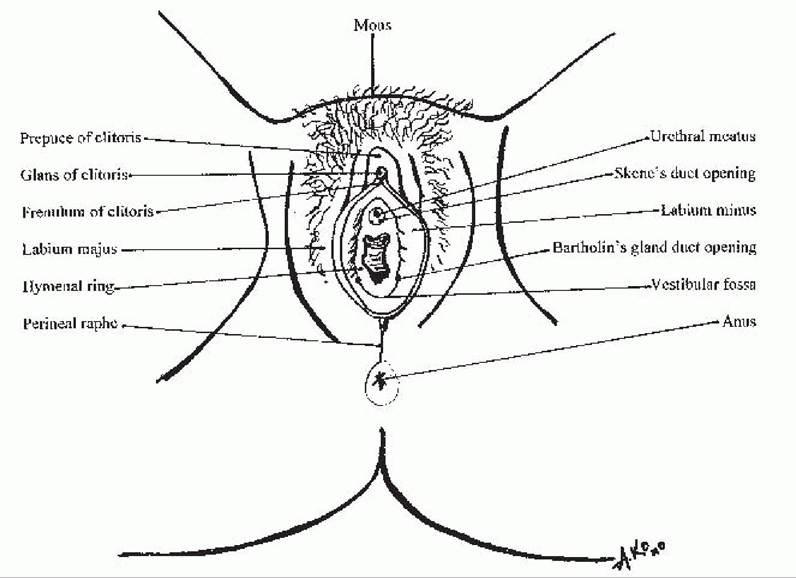
Figure 26-6. Vulva and perineum. (Original drawing by Alice W. Ko from Bankowski BJ, Hearne AE, Lambrou NC, eds. The Johns Hopkins Manual of Gynecology and Obstetrics, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002.)
• The mons (mons pubis, mons veneris) is hair-bearing skin overlying adipose tissue that lies on the pubic bones.
• The labia majora extend posteriorly from the mons and contain similar hairbearing skin. The labia majora contain the insertion of the round ligaments.
• The labia minora are hairless skin folds that split anteriorly to form the prepuce and frenulum of the clitoris. They overlie loosely organized connective tissue rather than adipose tissue.
• Gland duct openings
• The greater vestibular (Bartholin) gland duct opening is seen on the posterolateral aspect of the vestibule 3 to 4 mm lateral to the hymenal ring.
• The minor vestibular gland duct opening is seen in a line above the greater vestibular gland duct opening toward the urethra.
• The Skene ducts are located inferolateral to the urethral meatus at approximately 5 and 7 o'clock.
• Specialized glands
Holocrine sebaceous glands are located in the labia majora and are associated with hair shafts.
Apocrine sweat glands are located lateral to the introitus and anus. Hidradenitis suppurativa can occur if these glands become chronically infected. Hidradenomas are neoplastic enlargements of these glands.
Eccrine sweat glands are also located laterally to the Introitus and anus. They can enlarge and form a syringoma.
P.337
Superficial Compartment of the Vulva
• This compartment lies between the subcutaneous layer and the perineal membrane (Fig. 26-7).
• The clitoris consists of the glans, a shaft that is attached to the pubis by a subcutaneous suspensory ligament, and paired crura that stem from the shaft and attach to the inferior aspect of the pubic rami.
• Ischiocavernosus muscles overlie the crura of the clitoris. They originate at the ischial tuberosities and free surfaces of the crura and insert into the upper crura and clitoral shaft.
• Bulbospongiosus muscles originate in the perineal body and insert into the clitoral shaft. They overlie the centrolateral aspects of the vestibular bulbs and Bartholin gland.
• Superficial transverse perineal muscles originate from the ischial tuberosities and insert into the perineal body.
• The perineal body (central tendon of the perineum) is connected anterolaterally with the bulbocavernosus muscle and anteriorly with the perineal membrane, which attaches the perineal body to the inferior pubic rami. The perineal body is attached laterally to the superficial transverse perineal muscles, posteriorly to the external anal sphincter, and superiorly to the distal rectovaginal fascia.
• The vestibular bulbs are paired erectile tissues that lie immediately under the skin of the vestibule and under the bulbocavernosus muscles.
• Bartholin glands lie between the bulbocavernosus muscles and the perineal membrane at the tail end of the vestibular bulb. Their ducts empty into the vestibular mucosa.
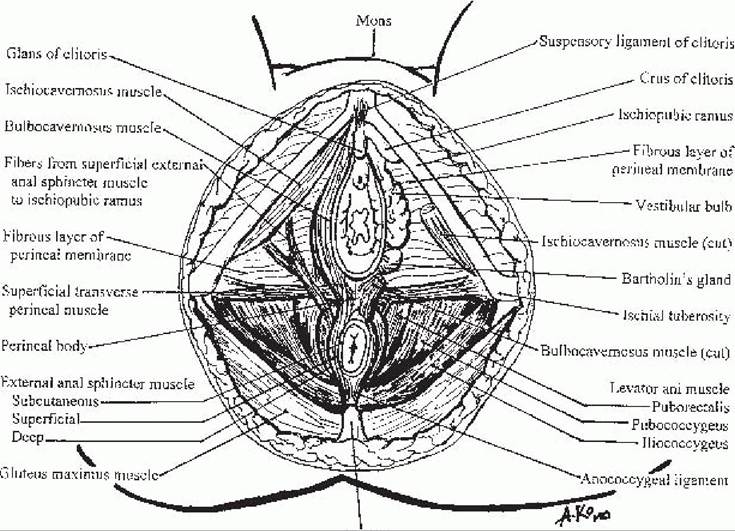
Figure 26-7. Superficial compartment of the vulva. (Original drawing by Alice W. Ko from Bankowski BJ, Hearne AE, Lambrou NC, eds. The Johns Hopkins Manual of Gynecology and Obstetrics,, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002.)

Pelvic Floor
• The pelvic floor comprises the perineal membrane and the muscles of the pelvic diaphragm. It helps support the pelvic contents above the pelvic outlet.
• The perineal membrane is a triangular sheet of dense fibromuscular tissue that spans the anterior triangle. It provides support by attaching the urethra, vagina, and perineal body to the ischiopubic rami. The perineal membrane contains the dorsal and deep nerves and vessels to the clitoris.
• The muscles of the pelvic diaphragm comprise the levator ani and coccygeal muscles. These are covered by the superior and inferior fascias (Fig. 26-8).
• Levator ani muscles
• The puborectalis arises from the inner surface of the pubic bones and inserts into the rectum. Some fibers form a sling around the posterior aspect of the rectum.
• The pubococcygeus arises from the pubic bones and inserts into the anococcygeal raphe and superior aspect of the coccyx.
• The iliococcygeus arises from the arcus tendineus levator ani and inserts into the anococcygeal raphe and coccyx.
• The coccygeus muscle arises from the ischial spine and inserts into the coccyx and lowest area of the sacrum. It lies cephalad to the sacrospinous ligament.
Posterior T riangle
• This area is bounded bilaterally by the ischial tuberosities and posteriorly by the coccyx.
• External anal sphincter
• The superficial portion is attached anteriorly to the perineal body and posteriorly to the coccyx.
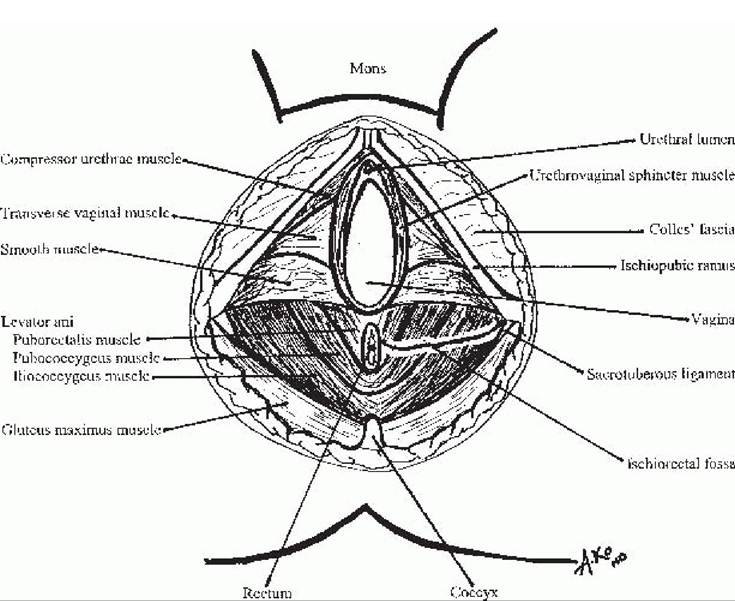
Figure 26-8. Pelvic diaphragm. (Original drawing by Alice W. Ko, from The Johns Hopkins Manual of Gynecology and Obstetrics, 2nd Ed. Philadelphia, PA: Lippincott Williams and Wilkins, 2002.)
P.339
• The deep portion encircles the rectum and blends in with the puborectalis muscle.
• Internal anal sphincter: This sphincter is a smooth muscle that is separated from the external sphincter by the intersphincteric groove as well as fibers from the longitudinal layer of the bowel.
• The ischioanal fossa contains the pudendal neurovascular trunk; it is bordered medially by the levator ani muscles and laterally by the obturator internus muscles. It has an anterior recess that lies above the perineal membrane and a posterior portion that lies above the gluteus maximus. This space allows for physiologic expansion of the rectum.
Levels of Pelvic Support
• The pelvic muscles and connective tissue are the primary support for the pelvic organs. The pelvic muscles consist of the levator ani plate (i.e., puborectalis, pubococcygeus, and ileococcygeus) and the coccygeus muscle. The connective tissue attachments (uterosacral/cardinal ligament complex and the endopelvic fascia) stabilize the pelvic organs in the correct position to receive support from the pelvic muscles. With pelvic muscle weakness or damage secondary to obstetric injury, the endopelvic fascia becomes the primary mechanism of support. This stress can attenuate, stretch, or break the endopelvic fascia resulting in failure of support of the pelvic organs and pelvic organ prolapse.
• There are three levels of support, as described by DeLancey:
• Level I is the upper vertical axis or uterosacral/cardinal ligament complex. The uterosacral/cardinal ligament complex supports the cervix and upper vagina to maintain vaginal length and to keep the upper vaginal axis nearly horizontal so that it rests on the rectum and can be supported by the levator plate.
• Level II is the horizontal axis or paravaginal supports. The pubocervical fascia and rectovaginal fascia spread over the vagina and condense into the ATFP to support the midvagina and create the anterior lateral vaginal sulci.
• Level III is the lower vertical axis or perineal body, perineal membrane, and the superficial muscles (bulbocavernosus, ischiocavernosus, superficial and deep transverse perineal muscles). This supports and maintains the normal position of the distal one third of the vagina and introitus, which is nearly vertical in a standing female.
• Levels I, II, and III are connected through continuation of the endopelvic fascia.
NERVES OF THE PELVIS AND PERINEUM
Pelvic Diaphragm
• The pudendal nerve supplies the external anal sphincter and the urethral sphincter.
• The anterior branch of the ventral ramus of S3 and S4 innervates the levator ani and coccygeal muscles.
Perineum
• The pudendal nerve is the sensory and motor nerve of the perineum.
• The pudendal nerve originates from the sacral plexus (S2 to S4), exits the pelvis through the greater sciatic notch, hooks around the ischial spine and sacrospinous ligament, and enters the pudendal canal (canal of
Alcock) in the lesser sciatic notch. The pudendal nerve has several terminal branches:
î The clitoral nerve runs along the superficial aspect of the perineal membrane to supply the clitoris.
î The perineal nerve runs along the deep aspect of the perineal membrane. Its branches supply the muscles of the superficial compartment; subcutaneum; and skin of the vestibule, labia minora, and medial aspect of the labia majora.
P.340 î The inferior hemorrhoidal nerve (inferior rectal) innervates the external anal sphincter and the perianal skin.
• A pudendal block is performed by injecting anesthetic just inferior to the ischial spine; this provides local analgesia for vaginal deliveries. This block may also be performed in cases of nerve injury or compression and resulting pudendal neuralgia.
Nerve Injuries in Gynecologic Surgery
• Nerve injuries are encountered from positioning, incisions, use of retractors, and dissection (Table 26-1).
TABLE 26-1 Nerve Injuries in Gynecologic Surgery
| Nerve | Injury | Motor Loss | Sensory Loss |
| Femoral L2-L4 | Deep retraction on psoas muscle, excessive hip flexion | Hip flexion, knee extension, knee DTR, leg adduction | Anteromedial thigh, anteromedial leg and foot |
| Lateral femoral cutaneous L2- L3 | Deep retraction on psoas muscle, excessive hip flexion | None | Anterolateral and posterolateral thigh |
| Genitofemoral branch L1-L2 | Pelvic sidewall dissection | None | Mons, labia majora, anterior superior thigh |
| Obturator L2-L4 | Retroperitoneal surgery, lymph node dissection, paravaginal defect repair | Leg abduction | Anteromedial thigh |
| Sciatic L4-S3 Common peroneal L4-S2 | Extensive endopelvic resection Compression from stirrups on lateral calf | Hip extension, knee flexion Foot dorsiflexion and eversion | Lateral calf, dorsomedial foot Lateral calf, dorsomedial foot |
| Tibial L4-S3 | Compression from stirrups on lateral calf | Foot plantar flexion and inversion | Toes, plantar foot |
| Transverse abdominal incision | None | Mons, labia, inner |
T12
thigh
Ilioinguinal L1 Transverse abdominal incision None Groin, symphysis
pubis
DTR, deep tendon reflex.
Adapted from Irvin W, Anderson W, Rice L. Minimizing the risk of nerve injury in gynecologic surgery. Obstet Gynecol 2004;103:374-382.
P.341
LYMPHATIC DRAINAGE OF THE PELVIS
• The vulva and lower vagina drain to the inguinofemoral lymph nodes and then to the external iliac nodes. See Chapter 44.
• The cervix drains through the cardinal ligaments to the pelvic nodes (hypogastric, obturator, and external iliac) and then to the common iliac and para-aortic lymph nodes.
• The uterus drains through the broad ligament and intraperitoneal ligament to the pelvic and para-aortic lymph nodes.
• The ovaries drain to the pelvic and para-aortic lymph nodes.
SUGGESTED READINGS
Ashton-Miller JA, DeLancey JO. Functional anatomy of the female pelvic floor. Ann NYAcad Sci 2007;1101:266-296.
DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol 1992;166:1717-1728.
DeLancey JO. Structural anatomy of the posterior pelvic compartment as it relates to rectocele. Am J Obstet Gynecol 1999;180:815-823.
Law YM, Fielding JR. MRI of pelvic floor dysfunction: review. Am J Roentgenol 2008;191: S45-S53.
Weber AM, Walters MD. Anterior vaginal prolapse: review of anatomy and techniques of surgical repair. Obstet Gynecol 1997;89:311-318.
27