Obstetric Anesthesia
Abigail D. Winder
Jamie Murphy
Labor and delivery is a time of intense pain, often influenced by the psychological, emotional, social, cultural, and physical state of the parturient.
Multiple techniques and procedures for pain relief during the birthing process are available. With appropriate counseling of risks and benefits, patients can choose their preferred analgesic treatments.PAIN PATHWAYS
• In the first stage of labor (cervical dilation), the pain is visceral, produced by the distention of the lower uterus and cervix and ischemia of the uterine and cervical tissues. Visceral pain signals traverse T10 to L1 white rami communicantes and enter the spinal cord.
• The second stage involves both visceral and somatic pain. The parturient experiences more somatic pain in the late first stage of labor (7 to 10 cm cervical dilation), entering into the second stage from distention of the vagina, perineum, and pelvic floor. Somatic pain signals traverse the pudendal nerve (S2 to S4) and enter into the anterior spinal cord. The parturient also experiences rectal pressure. See Chapter 30 for more on biologic basis of pain perception.
OVERVIEW OF OBSTETRIC ANALGESIA/ANESTHESIA
• Local, regional, and systemic methods of analgesia and anesthesia are used in obstetrics. Local and regional methods include local injection, peripheral nerve
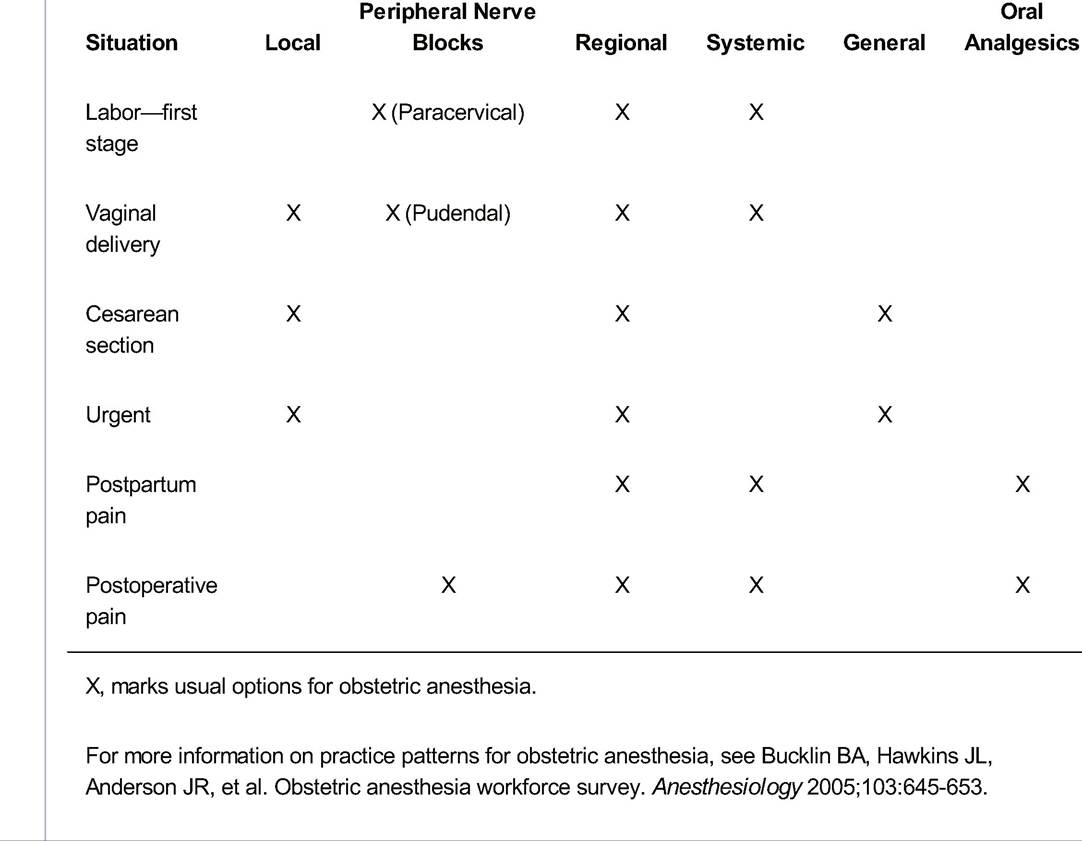
P.319 block, and regional block. Systemic methods can be administered intramuscularly, intravenously, or by inhalation. General anesthesia is often used in cases where total motor and sensory loss is necessary (Table 25-1) or when contraindications to neuraxial anesthesia are present.
• During the first stage of labor, visceral pain is mollified by the preferred use of regional anesthesia, such as an epidural, spinal, or a combination of both.
• In vaginal deliveries, the goal is to block nociceptive pathways while preserving motor function so that the parturient is comfortable but can participate actively with second stage expulsive effort.
Local anesthesia or peripheral nerve block with pudendal injection or more systemic analgesia with intravenous (IV) pain medication or spinal/epidural block can be used during the second stage of labor.• In cesarean delivery, anesthetic selection is often determined by the condition of the mother and fetus, the urgency of the procedure, and physician preference. Operative anesthesia requires a denser motor and sensory block than that used for a vaginal delivery. Neuraxial anesthesia is often the preferred method used because it provides adequate pain control while minimizing the maternal risk of aspiration or unanticipated difficult airway. In addition, neuraxial anesthesia decreases systemic catecholamine release and systemic response to surgery, avoids the side effects of postoperative IV narcotics, and allows the mother to interact with the newborn soon after delivery. Effective neuraxial anesthesia can be achieved by epidural, spinal, or combined spinal epidural approaches. General anesthesia is appropriate when the patient presents with contraindications to neuraxial anesthesia, medical indications, or in emergency cases where neuraxial anesthesia cannot be administered in a timely manner. Supplemental local anesthesia can be used by the obstetrician on the operative field as well.
TABLE 25-1 Use of Anesthesia in Obstetric Situations
P.320
TYPES OF OBSTETRIC ANALGESiAZANESTHESiA
Local Injection (Field Block)
Indications
• Used before cutting or repairing episiotomies or lacerations during and after the delivery
• Common agents include lidocaine (1% to 2%) or 2-chloroprocaine (1% to 3%), which provide anesthesia for 20 to 40 minutes. The maximum allowed dose of injected lidocaine is 4.5 mg/kg.
Advantages
• Can provide pain relief without special equipment or personnel
• Local block can relieve most of the pain of simple laceration repair.
• Minimal systemic effect if administered correctly
Limitations
• May not cover entire field well or may not entirely block pain perception.
Risks/Complications
• Inadvertent IV injection can lead to serious systemic complications.
• Hypotension, arrhythmias, and seizures are rare complications.
Peripheral Nerve Block (Pudendal, Paracervical)
Indications
• Paracervical block may be considered for the first stage of labor in patients for whom an epidural or spinal is contraindicated, unavailable, or undesired.
• Pudendal block may be used as analgesia during the second stage of labor or before operative vaginal deliveries if neuraxial anesthesia has not been provided or in supplement if there is inadequate pain relief.
Technique
• Paracervical: Five to 10 mL of local anesthetic (e.g., 2% chloroprocaine) is injected in the lateral vaginal fornices at the 4 and 8 o'clock positions to a depth of 3 to 4 mm.
• Pudendal: Five to 10 mL of local anesthetic (e.g., 1% lidocaine) is injected transvaginally about 1 cm medial and posterior to the ischial spine along the sacrospinous ligament at a depth of about 1 cm bilaterally. Care must be taken to avoid injecting directly into the pudendal vessels.
Advantages
• Peripheral nerve block is highly effective and may offer relief in up to 75% of cases.
Limitations
• Total anesthetic injection limits apply, as mentioned earlier.
• In some cases, relief may be inadequate. Twenty to 30 minutes are required before full effect. Pudendal block may be ineffective in up to 50% of patients and is frequently unilateral.
Risks/Complications
• Intravascular injection can result in systemic effects including medication toxicity, hematoma formation, and pelvic infection; these are recognized complications.
P.321
• Fetal bradycardia is a known side effect of paracervical block, occurring in approximately 15% of cases. Direct fetal injection is also a risk with paracervical block, resulting in fetal cardiac toxicity.
Except in select cases in which other analgesia is not available, paracervical block is usually avoided.Regional Anesthesia (Epidural, Spinal)
• Epidural and spinal anesthesia are the preferred methods for obstetric pain control in the United States. They may be administered separately or as a combined spinal-epidural (CSE). Analgesia occurs at or below the T8 to T10 dermatomes, with varying degrees of motor blockade.
Indications
• Neuraxial anesthesia is the preferred method of pain control because of its effectiveness and safety. General anesthesia is associated with increased maternal morbidity associated with increased risk of maternal aspiration and unanticipated difficult intubation.
• May be used when there is anticipated difficulty with intubation, a history of malignant hyperthermia, cardiovascular or respiratory disorders, or a need to prevent autonomic hyperreflexia in women with high spinal cord lesions.
• Regional anesthesia is preferred in women with preeclampsia because it may increase intravillous blood flow and reduce the need for general anesthesia if cesarean delivery is indicated.
• Maternal request alone is sufficient reason to give regional anesthesia.
Technique
• Table 25-2 lists agents commonly used for obstetric regional anesthesia.
• Epidural (Fig. 25-1): A catheter is introduced into the lumbar epidural space through an epidural needle. The catheter is secured to the patient's back with adhesive tape. Medication is administered via continuous infusion pump (preferred) or intermittent bolus to provide consistent pain relief. Local anesthetic, neuraxial opioid, or a combination of both is used. A test dose (typically 3 mL of
P.322
1.5% lidocaine with 1:200,000 epinephrine in bolus) should be given to rule out intrathecal or intravascular catheter placement and avoid complications. Patientcontrolled epidural anesthesia allows the patient to selfadminister small bolus doses by pressing a dose-demand button.
Pain relief may be further improved by a combination of continuous plus patient-controlled dosing. Breakthrough pain is addressed by increasing the continuous infusion rate or giving a second bolus dose.TABLE 25-2 EpiduralZSpinal Anesthetics
| Class | Action | Examples |
| Local anesthetics | Block conductance through sodium channels in axons. Reversible effect | Amides: lidocaine, bupivacaine, ropivacaine Ester: chloroprocaine |
| Opioids | Act on opioid receptors in dorsal horn of spinal cord | Morphine, fentanyl, sufentanil, alfentanil, meperidine |
| Adrenergic agonists | Bind to alpha-2 receptors in the spinal cord | Epinephrine, clonidine, dexmedetomidine |
Cholinergic Increase cholinergic effect via muscarinic agonists receptors in the dorsal horn of spinal cord
Neostigmine
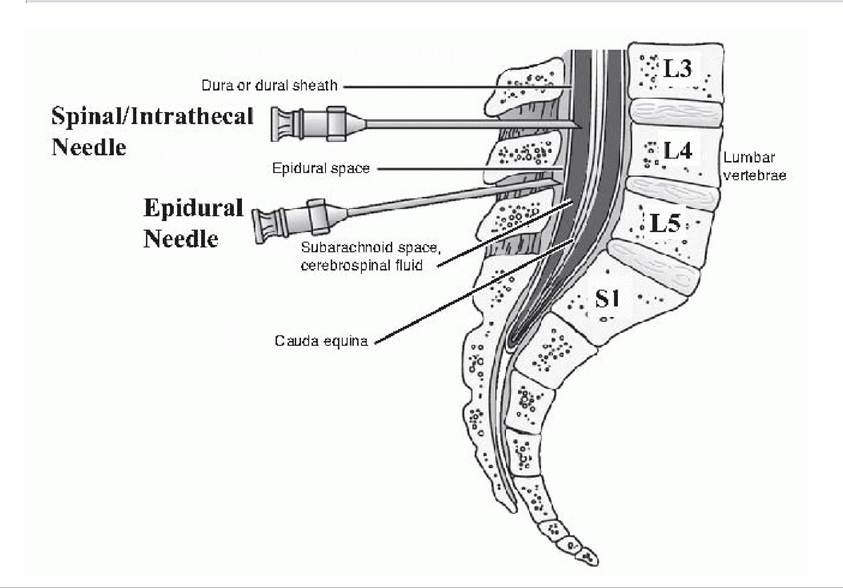
Figure 25-1. Placement of spinal and epidural anesthesia. The spinal cord ends at the conus medullaris near lumbar vertebral bodies L1/L2 in adults, with the cauda equina nerves extending below. Spinal anesthesia is injected directly into the cerebrospinal fluid of the subarachnoid space, whereas epidural anesthesia is deposited in the epidural space (near L3/L4). Combined spinal-epidural analgesia can be administered with a single needle that allows intrathecal injection followed by epidural catheter placement. L, lumbar; S, sacral. (Adapted from Taylor C, Lillis CA, LeMone P. Fundamentals of Nursing, 2nd ed. Philadelphia, PA JB Lippincott, 1993, with permission.)
• Spinal: A local anesthetic, often in combination with an opioid, is injected into the subarachnoid space.
The onset of action is rapid. Continuous spinal anesthesia can be given via an intrathecal catheter, although there is a risk for transient neurologic syndrome especially with infusions of high-dose lidocaine anesthetics.• CSE: This is the needle-through-needle approach in which a smaller bore spinal needle (i.e., — 24G to 27G) is placed inside the epidural needle. The spinal medication is injected, then the small needle is withdrawn and an epidural catheter threaded into the epidural space as mentioned earlier. A single spinal bolus of opioid, sometimes with local anesthetic, is injected into the subarachnoid space. This method combines the rapid onset of spinal anesthesia with the longer lasting relief of an epidural.
Advantages
• Regional analgesia provides excellent pain control but allows the patient to participate actively in the labor and delivery process.
P.323
• Increased use of neuraxial anesthesia and the reduction in general anesthesia during delivery has led to significant decreases in anesthesia-associated maternal morbidity and mortality related to aspiration pneumonia and inability to intubate.
Limitations
• Regional anesthesia cannot be placed in every case due to time limitations, anatomic considerations, comorbidities, or contraindications.
• Twenty to 30 minutes are required for full effect of an epidural.
• Spinal anesthesia lasts only 30 to 250 minutes depending on the drug injected.
• CSE is associated with a higher incidence of fetal bradycardia, with emergency cesarean delivery occurring in 1 % to 2% of cases.
• Failure of the spinal component may occur in 4% of cases in which CSE is used.
Contraindications
• Patient refusal
• Coagulopathy
• Thrombocytopenia
• Infection at injection site
• Sepsis
• Hemodynamic instability or refractory hypotension
• Increased intracranial pressure caused by a mass lesion
Risks/Complications
• Infection: meningitis, epidural abscess, reactivation of latent herpes simplex virus (HSV) (associated with neuraxial morphine use), and maternal fever
• Neurologic complications: epidural hematoma, neural injury, spinal headache, catheter- and needle- related complications, back pain, and nerve palsies
• Spinal headache: If the subarachnoid space is entered by the epidural needle, a spinal headache may result in up to 70% of patients. Management includes analgesics, supine positioning, hydration, caffeine, and abdominal binding. A blood patch can be offered if conservative management fails and the patient desires it.
• Back pain: There is no evidence implicating epidural anesthesia as a cause of chronic back pain.
• Nerve palsies: Injuries to the lumbosacral trunk, lateral femoral cutaneous, femoral, and common peroneal nerves have been reported.
• Adverse drug reactions: Local anesthetic toxicity, high spinal block/respiratory distress, allergic reaction, and transient neurologic impairment are possible complications.
• Local anesthetic toxicity: Symptoms include tinnitus, disorientation, and seizures; cardiovascular symptoms include hypotension, dysrhythmias, and cardiac arrest.
• High spinal: Respiratory compromise may result if the block progresses above the C6 dermatome level.
• Motor block: Motor impairment can reduce maternal expulsive efforts and alter the birthing process and parturient experience.
• Intrathecal opioids can cause maternal respiratory depression and hypoxemia.
• Hypotension: Low blood pressure can result with regional anesthesia from sympathetic blockade- induced vasodilation or position-dependent decreased venous return. Hypotension is significant when symptoms develop, such as maternal light-headedness or fetal bradycardia. Episodes can be treated with bolus IV fluids or low-dose ephedrine (5 mg) or phenylephrine (100 μg). Adequate IV hydration must occur before epidural or spinal access is placed.
P.324
• Fetal complications
• Nonreassuring fetal monitoring: Bradycardia and transient heart rate decelerations may occur. Hydration is usually adequate treatment, although pressor support (as mentioned earlier) may be indicated. Repositioning should also be attempted.
• Instrumentation: There is mixed evidence for increased rates of forceps or vacuum delivery with regional anesthesia, with challenges in demonstrating causation versus association.
• When compared to IV systemic opioid analgesia, early neuraxial anesthesia does not increase the risk of cesarean delivery.
Systemic Analgesia
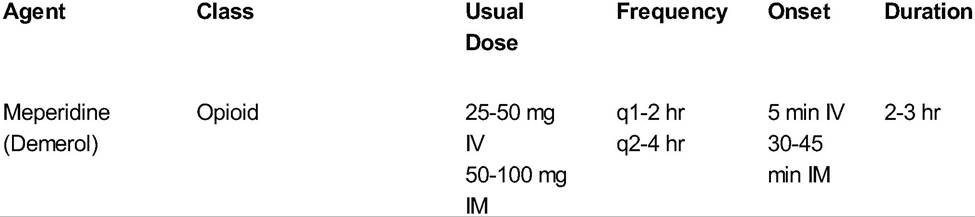
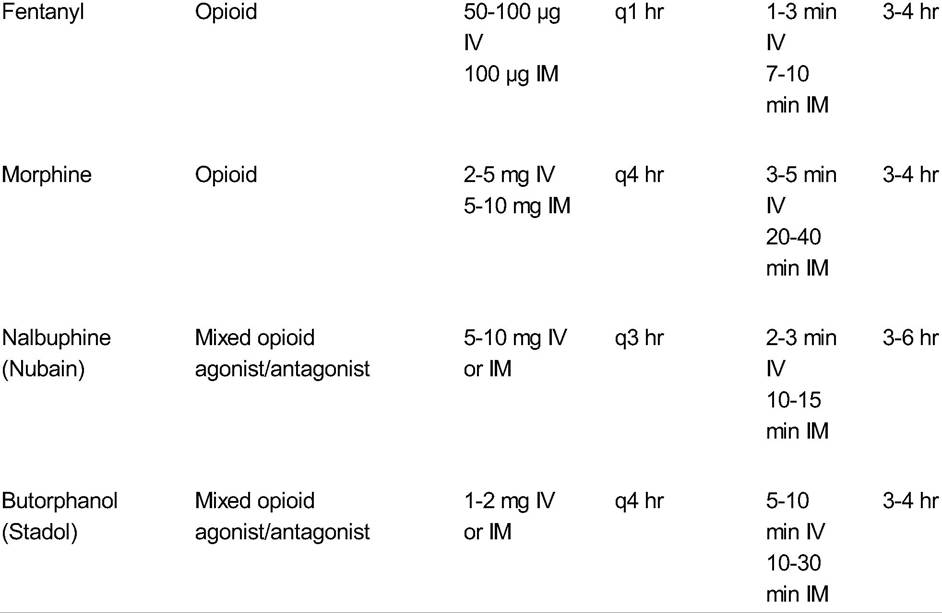
Opioids (morphine, fentanyl, meperidine) or mixed opioid agonist-antagonists (butorphanol, nalbuphine) are used for systemic pain relief (Table 25-3). They can be administered by intramuscular or IV injection depending on the onset and duration of relief desired.
Indications
• Maternal request
Advantages
• Rapid onset and ease of administration
• Can be administered via IV patient-controlled anesthesia
Limitations
• Randomized controlled trials demonstrated higher pain scores during labor for parenteral compared with regional anesthesia.
TABLE 25-3 Parenteral Agents for Labor Pain
IV, intravenous; IM, intramuscular.
Adapted from Althaus J, Wax J. Analgesia and anesthesia in labor. Obstet Gynecol Clin N Am 2005;32:231-244.
P.325
• It is difficult to obtain adequate pain control throughout labor with only narcotic analgesia.
Risks/Complications
• Maternal respiratory depression requires close monitoring.
• Sedative effects may increase aspiration risk.
• All opiates cross the placenta, affecting both fetal and newborn status. Fetal tracings may show decreased variability with maternal narcotic analgesia. Newborns may require extra assistance after delivery including supplemental oxygen and ventilatory support.
General Anesthesia
Indications
• General anesthesia is useful in urgent situations in which epidural/spinal is not available, in cases where regional anesthesia is contraindicated, and in parturients with medical problems that require general anesthesia.
Technique
• Before intubation, the patient receives a nonparticulate antacid, such as sodium citrate, to neutralize gastric pH and decrease aspiration risk. One hundred percent oxygen is administered for 3 to 5 minutes before induction and intubation to fortify oxygen reserve.
• IV agents are used in a rapid sequence induction to minimize aspiration from the abdominal distention/pressure of the gravid uterus.
• The trachea is intubated quickly with a cuffed endotracheal tube as cricoid pressure is applied to reduce aspiration risk.
Advantages
• Intubation can be performed rapidly in emergent cases.
• Inhaled fluorinated anesthetics cause rapid uterine relaxation which may be used to correct uterine inversion or to facilitate internal/external version or release fetal head entrapment.
• The patient remains still throughout the procedure and does not remember an extensive or prolonged procedure.
Limitations
• The parturient is unable to witness the birth of her child.
• All inhalational agents cross the placenta and can affect the fetus, leading to brief neonatal respiratory depression after delivery; the time from intubation to delivery should be as brief as feasible and safe.
Risks/Complications
• Given the decreased functional residual capacity and increased oxygen requirements of pregnancy, in addition to increased airway edema and friability, there is an increased maternal morbidity associated with general anesthesia/intubation.
• Aspiration and hypoxemia can lead to postoperative medical complications.
• Neonatal respiratory depression occurs as a result of fetal perfusion of the anesthetics
• Uterine relaxation can increase surgical blood loss. Pitocin, Methergine, and misoprostol should all be on hand at the time of obstetric general anesthesia.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 36: obstetric analgesia and anesthesia. Obstet Gynecol 2002;100:177-191.
P.326
Gaiser R. Chapter 2: physiologic changes of pregnancy. In Chesnut DH, Polley LS, Tsen LC, et al, eds. Chestnut’s Obstetric Anesthesia: Principles and Practice, 4th ed. Philadelphia, PA: Mosby Elsevier, 2009.
Kopp SL, Horlocker TT. Anticoagulation in pregnancy and neuraxial blocks. Anesthesiol Clin 2008;26:1-22.
Santos AC, Bucklin BA. Chapter 13: local anesthetics and opioids. In Chestnut DH, Polley LS, Tsen LC, et al, eds. Chestnut’s Obstetric Anesthesia: Principles and Practice, 4th ed. Philadelphia, PA: Mosby Elsevier,
2009.
Wong CA, Nathan N, Brown DL. Chapter 12: spinal, epidural, and caudal anesthesia. In Chesnut DH, Polley LS, Tsen LC, et al, eds. Chestnut’s Obstetric Anesthesia: Principles and Practice, 4th ed. Philadelphia, PA Mosby Elsevier, 2009.
26