24 HIV in Pregnancy
Sangini Sheth
Jenell Coleman
The Centers for Disease Control and Prevention (CDC) first reported unusual opportunistic infections in previously healthy gay men in 1981. By 1982, the CDC reported the first case of AIDS transmitted from mother to infant.
T oday, approximately 34 million people are living with HIV infection/AIDS worldwide. One half of the infected are women. Over two thirds of infected persons live in sub-Saharan Africa. In 2011, there were an estimated 49,273 new HIV infections in the United States with an incidence of 15.8 per 100,000 people. The number of new HIV diagnoses in women is growing fastest among women of childbearing age. In 2007, the CDC reported HIV as the third leading cause of death in black women from 25 to 44 years of age. Women account for approximately 21% of new HIV infections in the United States annually, and over two thirds are of reproductive age.
With the widespread use of highly active antiretroviral therapy (HAART) in the developed world, people infected with HIV live longer and lead healthier lives. Improved treatment has reduced morbidity, increased survival, and markedly decreased perinatal transmission. Recent data reported a 150% increase in births to HIV-positive women since widespread use of HAART in pregnancy. This chapter summarizes recommendations regarding the care of HIV-infected women during pregnancy; readers are advised that this is a rapidly evolving field and the most current guidelines should be consulted.
PATHOPHYSIOLOGY OF HIV/AIDS
• HIV is an RNA virus that belongs to the retrovirus (Retroviridae) family and Lentivirus subfamily.
• The most common cause of HIV disease in the United States is HIV-1.
• HIV-2, a related strain, is endemic to Western Africa. It is less virulent than HIV-1 and less transmissible. It has a longer incubation period, is associated with lower viral loads, and progresses to AIDS less often than HIV-1.
HIV-2 is primarily seen in the United States in immigrants from West Africa.• Currently, it is estimated that two thirds to three fourths of new cases of HIV in women in the United States result from heterosexual transmission.
• Without any intervention, maternal-to-child transmission (MTCT) of HIV occurs in 14% to 42% of live births, depending on the setting.
• HIV infection results in progressive depletion of helper T cells.
• The subset of T lymphocytes affected is defined phenotypically by the presence of the CD4 receptor, which is the primary docking protein for HIV.
• Fusion and entry of the virus into the cell are facilitated by coreceptors, including CXCR4 and CCR5.
• Infection results in functional impairment and gradual depletion of CD4 cells, leading to immunodeficiency and subsequent opportunistic infection.
P.296
• HIV-RNA level (viral load) reflects active viral replication, and this can be used to track disease progression and therapeutic response. Higher viral loads predict more rapid disease progression.
COUNSELING AND TESTING
• The American College of Obstetricians and Gynecologists (ACOG) and CDC recommend offering HIV testing to all pregnant women:
• as a routine part of antenatal care, unless the woman declines (opt-out approach).
• with repeat testing in the third trimester to those in areas with high HIV prevalence, to those known to be at risk, and to those who declined earlier testing.
• as a rapid screen on presentation to labor and delivery for any pregnant woman of unknown HIV status or any pregnant woman who tested negative in early pregnancy but is at high risk of infection (sexually transmitted infection [STI] diagnosis, illicit drug use, trade of sex for money or drugs, multiple partners, HIV-positive partner, signs/symptoms of HIV, or living in an area with high HIV incidence/prevalence) and was not tested in the third trimester.
• It is important to know individual state law concerning HIV testing in pregnancy, as rules vary widely.
• Studies have shown that the rate of acceptance of HIV testing varies with the approach.
• When extensive pretest counseling is required and patients must specifically consent to testing (the opt-in approach), testing occurs less frequently. The opt-out approach includes counseling for basic information about HIV, the rationale for testing, the availability of therapeutic and preventive interventions, and recognition of ability to refuse testing.
• Most patients test positive within 1 month of primary infection, however, seroconversion may take up to 6 months.
• The most commonly used HIV screening test is a laboratory serum enzyme-linked immunosorbent assay (ELISA). A positive or indeterminate test is followed by a Western blot for confirmation.
• Rapid HIV antibody assays are available and require about 5 to 20 minutes, depending on the test, to obtain a result. Rapid tests use a variety of specimens including blood, plasma, serum or saliva. Many of the simple bedside or office rapid tests are clinical laboratory improvement amendments (CLIA) waived. The sensitivity and specificity of these tests are comparable to the ELISA HIV test. Because the positive predictive value declines with decreasing seroprevalence, a positive result with a rapid HIV test must be confirmed by the Western blot test.
• Appropriate posttest counseling is required. Important issues include:
• The role of safe sex practices in preventing HIV transmission and limiting other STIs, including superinfection with resistant strains of HIV-1
• HIV screening of older children who may have been perinatally infected
• Encouraging substance abuse rehabilitation, if appropriate
• Encouraging disclosure to sexual partners and health care providers; offer assistance with disclosure and consider issues related to possible domestic violence
MANAGEMENT OF HIV INFECTION IN PREGNANCY
Preconception
• Pregnancy intentions and information on effective contraception should be discussed on a routine basis with women of childbearing age.
Current data suggest thatP.297
over 50% of pregnancies in HIV-positive women are unintended. In HIV-positive adolescents, the rate of
unintended pregnancy is as high as 83%.
• In pregnancies complicated by HIV disease, the major goals are to optimize maternal health and to reduce the risk of perinatal transmission. Ideally, a treatment plan will be made during preconception counseling that excludes drugs with teratogenic potential. HIV status should be assessed by viral load and CD4 count. Women on antiretroviral therapy should be encouraged to achieve an undetectable HIV-1 RNA viral load prior to conception to decrease the risk of MTCT.
• Women who meet criteria to initiate HAART for maternal viral status should do so prior to pregnancy. Women who do not yet meet HAART criteria are generally not started until after the first trimester. Efavirenz should not be initiated in women who may become pregnant or during the first trimester of pregnancy.
• Appropriate vaccinations to be administered (ideally before conception) include influenza, pneumococcus, hepatitis A, hepatitis B, tetanus. Rubella and varicella vaccine is given prepregnancy if the CD4 count is >200.
• Women should be counseled on the importance of eliminating tobacco, alcohol, and illicit drug use prior to conception.
• Serodiscordant couples that wish to conceive should be referred for expert consultation. Appropriate screening and counseling on safe conception options depending on the gender of the infected partner should be addressed.
Antepartum
• In the United States, approximately 19% of HIV/AIDS cases are due to injection drug use. Noninjection drug use (e.g., crack cocaine) also contributes to HIV transmission, and illicit drug use has been associated with higher vertical transmission rates. Rehabilitation resources should be provided.
• Screening for domestic violence is important. Approximately two thirds of HIVpositive women have a lifetime or recent history of violence.
• Addressing mental health concerns is paramount. Up to 50% of HIV-positive women experience depression— more than twice as often as HIV-positive men or the general population. HIV-positive women should be screened for depression in pregnancy and managed appropriately. Mental health status can affect medication adherence.
• Variables associated with increased vertical transmission include the following:
• High plasma or genital tract HIV viral load
• Primary HIV infection or advanced AIDS
• Low CD4 count
• Sexually transmitted/genital tract coinfection
• Placental disruption/abruption, chorioamnionitis
• Active substance abuse
• Invasive fetal monitoring or assessment (e.g., fetal scalp sampling, chorionic villus sampling, amniocentesis)
• Prolonged rupture of membranes
• Preterm delivery
• Episiotomy
• Instrumental delivery
• Breast-feeding
Antiretroviral Therapy during Pregnancy
• All pregnant women should be offered treatment regardless of CD4 T-cell count or viral load to reduce MTCT (Table 24-1); women should be counseled on the
P.298 benefits and possible risks of HAART. A combined antiretroviral drug regimen is recommended and adherence must be stressed.
TABLE 24-1 Antiretroviral Therapy and Rates of Perinatal HIV Transmission
Treatment Category Vertical Transmission Rate (%)
Untreated 20-30
Zidovudine monotherapy 10
Dual therapy 4
HAART 1-2
HAART, highly active antiretroviral therapy.
• Initial evaluation should include:
• History of HIV-related conditions and trend of prior CD4 T-cell counts and HIV viral loads
• Current CD4 T-cell count and HIV viral load
• Baseline complete blood cell count and liver function testing
• Screening for hepatitis C virus and tuberculosis infection
• Antiretroviral drug resistance studies in all women with HIV-1 RNA viral load levels above the threshold of resistance testing before initiating or changing HAART regimen
• Appropriate prophylaxis in women at risk for opportunistic infections, as outlined in Table 24-2
• For women who are not on antiretroviral therapy at the beginning of pregnancy, it may be delayed until after the first trimester in women with high CD4 cell count and low HIV viral load.
Some evidence has shown that earlier initiation of antiretroviral (ARV) medications may lead to more effective viral suppression and reduce the risk of vertical transmission of HIV.• Decisions regarding an appropriate regimen should consider:
• Previous and current ARV treatment and viral resistance. Women who are receiving ARVs for their own health should not discontinue during pregnancy. The current HAART regimen should be continued as long as it is tolerated and effectively leading to viral suppression.
Safety and toxicity profiles for specific drugs during pregnancy (considering both mother and fetus)
Medical comorbidities that may contraindicate certain medications
• Patient compliance/adherence to treatment
• Specific drug regimens should be selected in consultation with an HIV specialist.
• To optimally suppress viral replication, minimize the risk of vertical transmission, and minimize the risk of new resistance mutations; strict adherence to the treatment regimen is crucial.
• The use of zidovudine (AZT) alone in the antenatal period is now generally discouraged except in select circumstances including high CD4 count with very low viral load (< 1,000), patient refusal of HAART, or patient nonadherence to HAART. Combination therapy should be considered for all pregnant women, regardless of CD4 or HIV viral load.
P.299
TABLE 24-2 Opportunistic Infection Primary Prophylaxis
Opportunistic
| Infection | Indication | Recommendation |
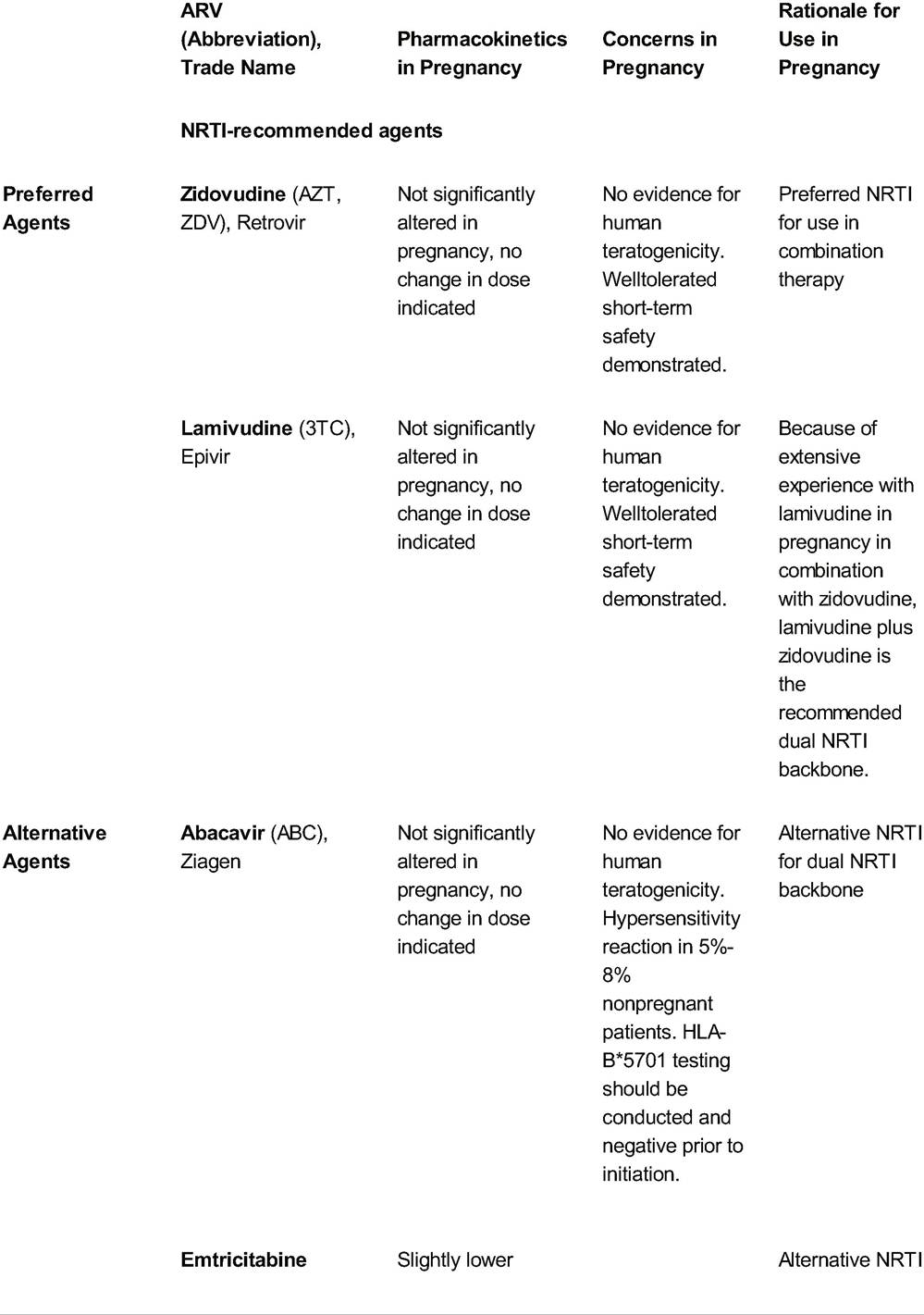
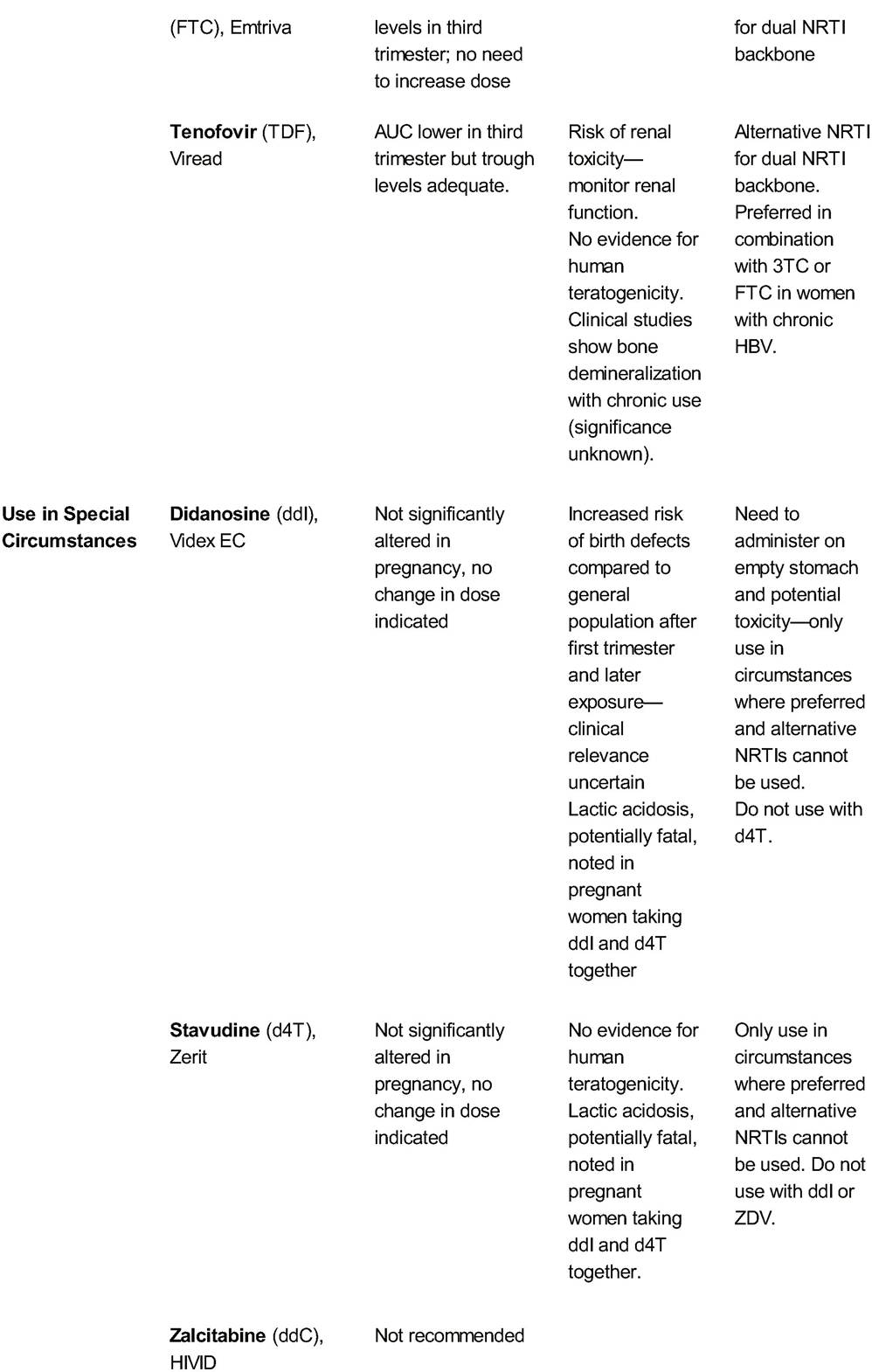
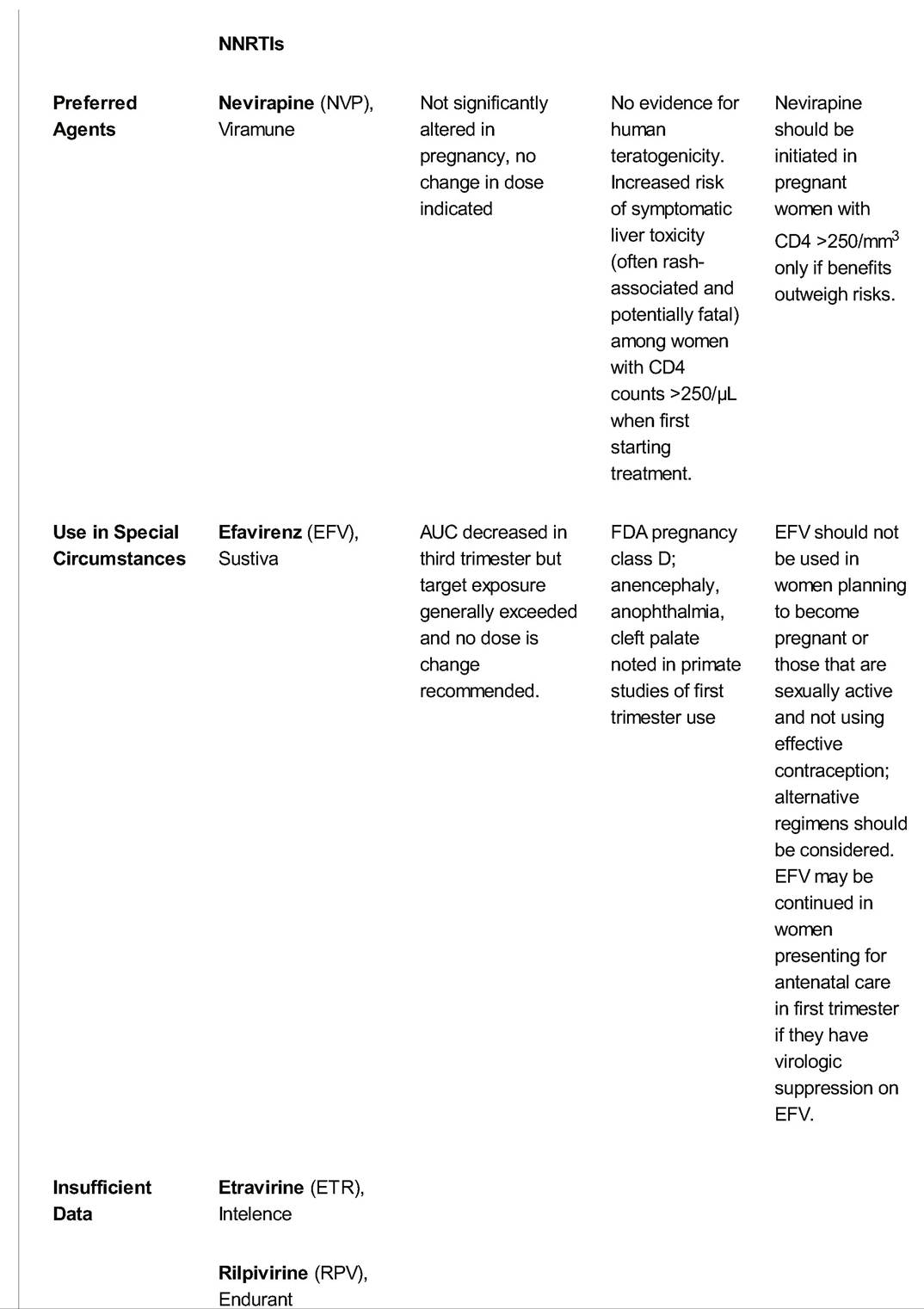
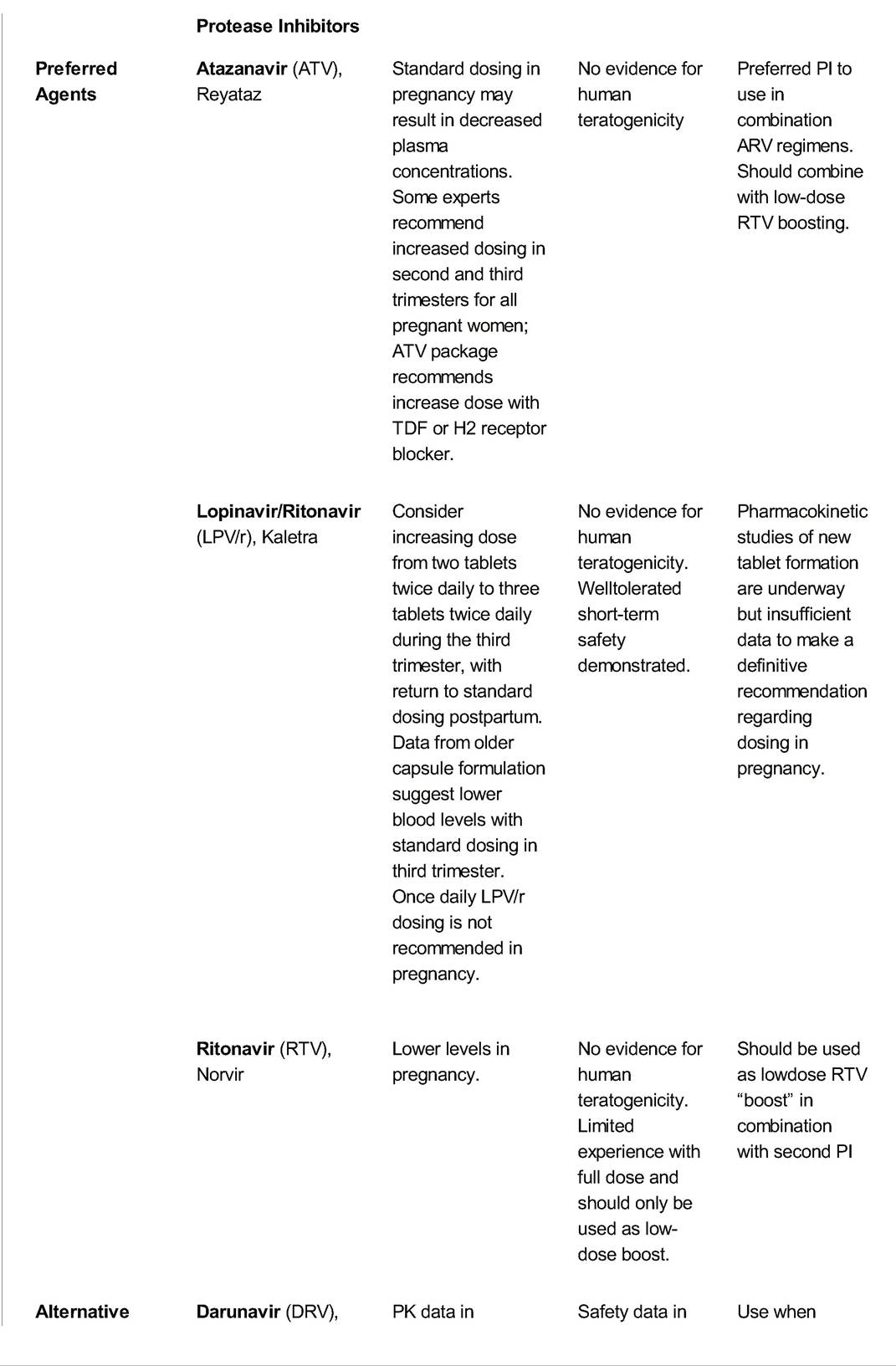
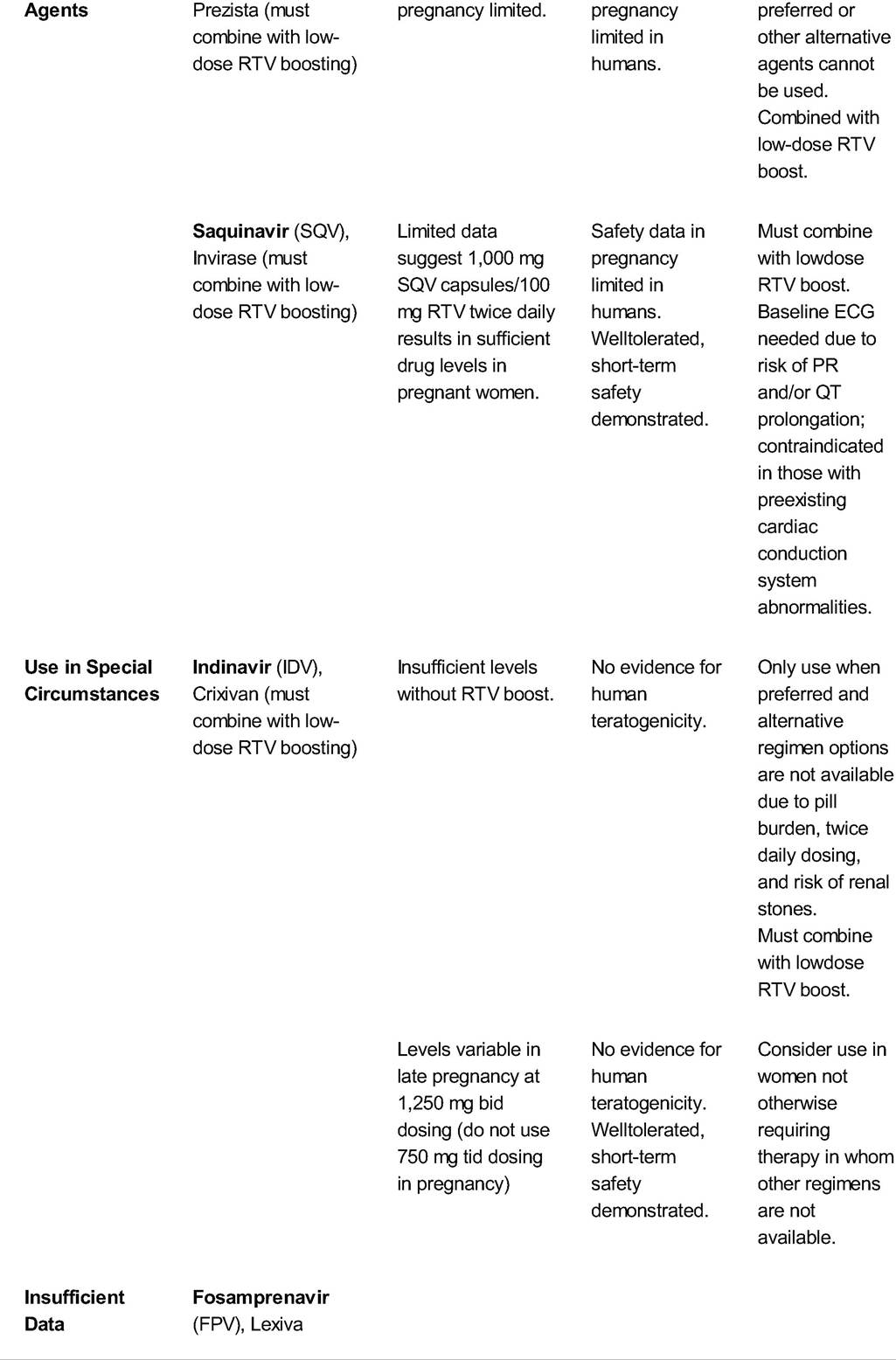
| Pneumocystis jiroveci (formerly called Pneumocystis carinii) pneumonia | CD4 avium complex | CD4 250∕μL. • Death from fulminant hepatic failure has been reported. î Most cases occur within the first 18 weeks of therapy; onset can be abrupt. Women who become pregnant while on NVP-containing regimens and have immune reconstitution with higher CD4 counts are at lower risk. NVP naive women with CD4 counts >250∕μL should not be started on NVP as part of combination therapy unless benefit clearly outweighs risk. î When NVP multidrug therapy is initiated, close clinical and laboratory monitoring is advised. î Hepatotoxicity has not been reported with single-dose NVP for peripartum prophylaxis. • NVP carries risk for drug rash as high as 17%. Severe hypersensitivity and Stevens-Johnson syndrome have been reported. Two-week introduction dosing of 200 mg NVP daily, increasing to 200 mg twice daily may be helpful. • EFV (Sustiva) is pregnancy category D. • Serious teratogenic effects in primates and neural tube defects in humans with early in utero exposure are reported. • EFV should be avoided in sexually active HIV-positive women who are not using effective consistent contraception. • EFV should also be avoided in pregnancy, particularly in the first trimester. • However, if a woman is on EFV when she conceives, she does not need to discontinue it during the first trimester, as long as EFV is part of a regimen providing effective virologic suppression. Entry Inhibitors, Integrase Inhibitors • There is little data on the use of these newer drugs in pregnancy. Intrapartum • Combination HAART regimen should be continued intrapartum. • Intravenous (IV) zidovudine should be administered to women with an HIV viral load >400 copies/mL or unknown viral load near delivery regardless of antepartum regimen or mode of delivery. For women on an antepartum regimen that includes oral zidovudine, the oral zidovudine should be stopped while they receive the IV infusion. • Women on HAART and with HIV viral load delivery. • A scheduled cesarean section at 38 weeks is recommended for women with an HIV viral load >1,000 copies/mL near delivery. When C-section is planned, IV zidovudine should be administered for at least 3 hours prior to C- section to ensure therapeutic blood levels (1-hour IV loading dose followed by continuous IV dose for 2 hours) to minimize risk of vertical transmission. • IV zidovudine should be started immediately in women presenting in labor with a positive rapid HIV test; CD4 T lymphocyte and HIV-1 RNA viral load should accompany confirmatory HIV antibody testing in the postpartum period. • Single-dose NVP has not been shown to decrease transmission further in women on combination antiretroviral therapy. P.305 P.306 P.307 P.308 P.309 P.310 TABLE 24-4 Pharmacokinetics and Toxicity of Antiretroviral Drugs and Recommendations for Use in Pregnancy
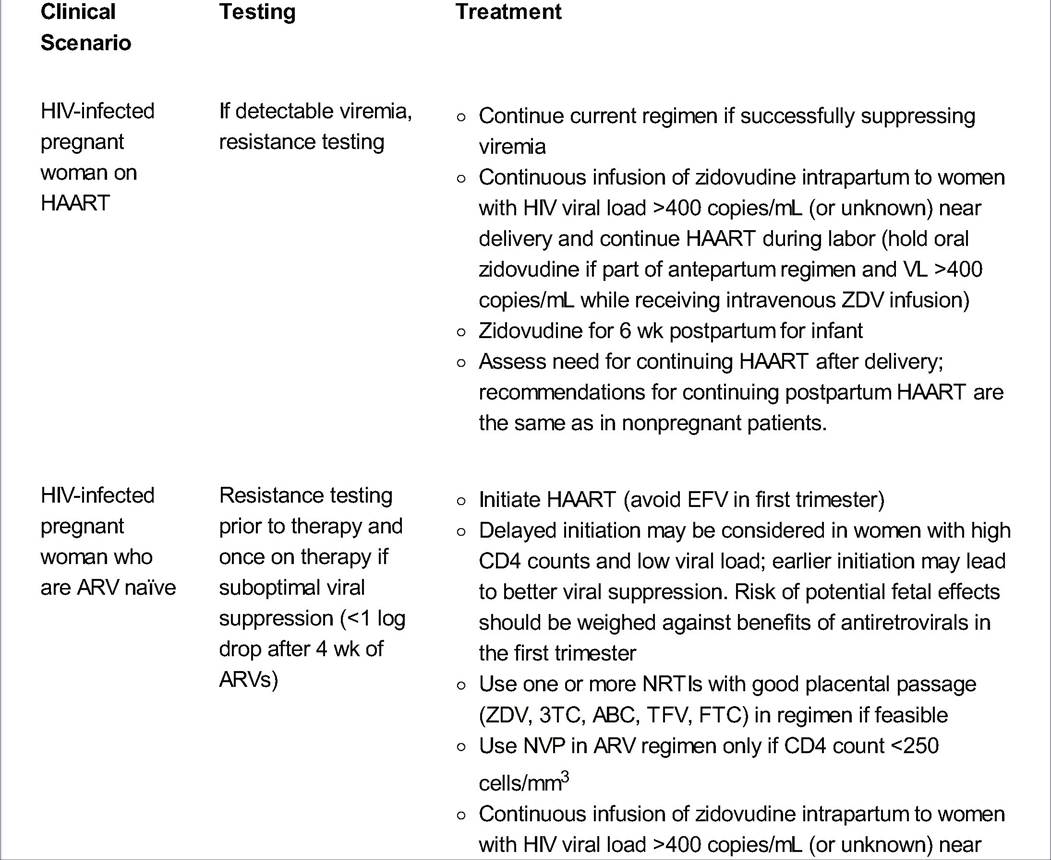
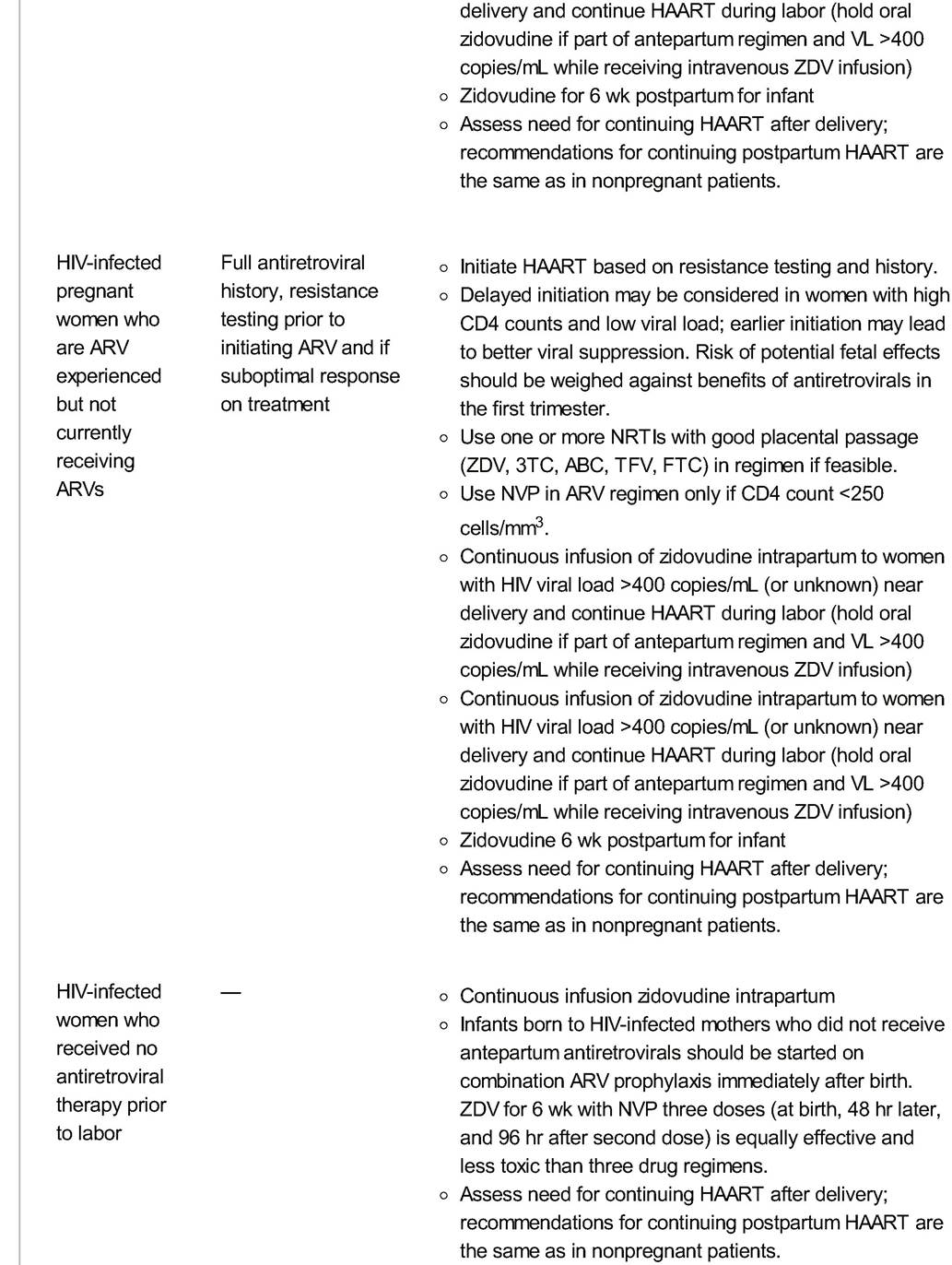
Tipranavir (TPV), Aptivus Insufficient data to recommend entry inhibitors and integrase inhibitors ARV, antiretroviral; NRTI, nucleotide reverse transcriptase inhibitor; AUC, area under the curve; HBV, hepatitis B virus; NNRTI, nonnucleoside reverse transcriptase inhibitor; FDA, U.S. Food and Drug Administration; PI, protease inhibitor; PK, pharmacokinetics; ECG, electrocardiogram; bid, twice a day; tid, three times a day. Adapted from Panel on T reatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States, Table 5 (pp. 14-29). http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf. Accessed April 6, 2013. P.312 Postpartum • Continuation of ARV treatment in the postpartum period is dependent on a number of factors as listed below and is a decision that should involve the patient and her primary HIV care provider. • CD4 count: Randomized control data demonstrates a benefit in treatment for those women with a CD4 count 500 cells/mm3. A multicenter trial (PROMISE study) investigating the risks and benefits of discontinuing combination ARV regimens in postpartum women with high CD4 cell count is underway. • Patient preference • Partner HIV status • Compliance and risk of viral resistance with suboptimal adherence • Drug toxicity • Cost • Infants should receive zidovudine starting 6 to 12 hours after birth and continuing for 6 weeks. Infants born to women who did not receive antepartum ARV medication (and with or without intrapartum maternal prophylaxis) should receive zidovudine for 6 weeks plus three doses of NVP in the first week of life—at birth, 48 hours later, 96 hours after the second dose. No studies are available to determine whether additional ARVs are beneficial for those infants delivered by cesarean section to mothers who received antenatal ARV treatment but had high viral loads (HIV RNA >1,000 copies/mL) near delivery. Among infants of women with high viral loads near delivery who deliver vaginally, zidovudine combined with NVP should be administered. If the mother's HIV status is unknown at the time of delivery, immediate rapid HIV antibody testing of mother or baby is recommended and the infant should receive zidovudine and NVP prophylaxis if the rapid test is positive. Perinatal HIV Transmission: Mode of Delivery • Evidence does NOT support cesarean delivery for patients on combination therapy with viral load 1,000 copies/mL who present in labor or with ruptured membranes. Mode of delivery should be selected based on duration of rupture, labor progress, HIV viral load, current antiretroviral therapy, and other clinical factors. Augmentation to shorten the time to vaginal delivery may be considered for some patients. • HIV-infected women have higher complication rates (mostly infectious) from scheduled cesarean deliveries than from vaginal deliveries but less than those associated with urgent or emergent C-sections. They also have more complications than uninfected women after cesarean delivery, particularly with lower CD4 counts. The complications with cesarean section are not of sufficient frequency or severity to outweigh the potential benefit for women with increased risk of vertical transmission. More studies are needed to determine the optimal management of preterm premature rupture of membrane with HIV infection and for patients with newly diagnosed HIV in labor (T able 24-5). Early data indicated that transmission risk increased with low maternal CD4 counts and rupture of membrane for longer than 4 hours. However, more recent data have found that duration of membrane rupture does not increase MTCT if the patient is taking HAART, has a low viral load, and receives zidovudine intrapartum. P.313 P.314 P.315 TABLE 24-5 Treatment Recommendations Based on Clinical Scenario in the United States
HAART, highly active antiretroviral therapy; VL, viral load; ZDV, zidovudine; ARV, antiretroviral; EFV, efavirenz; NRTI, nucleotide reverse transcriptase inhibitor; 3TC, lamivudine; ABC, abacavir; TFV, tenofovir; FTC, emtricitabine; NVP, nevirapine; IV, intravenous. Adapted from Panel on T reatment of HIV-Infected Pregnant Women and Prevention of Perinatal T ransmission. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States, Table 6 (pp. 30-33). http://aidsinfo.nih.gov /contentfiles/lvguidelines/PerinatalGL.pdf. Accessed April 7, 2013. P.316 • In general, amniotomy, fetal scalp electrodes for fetal monitoring, and operative vaginal delivery or episiotomy should be avoided. • Uterotonic medications typically used in the management of postpartum hemorrhage due to uterine atony may interact with a patient's ARV regimen: • Protease inhibitors are cytochrome P (CYP) 3A4 enzyme inhibitors, and therefore, Methergine should be used only if benefit from use outweighs risks and there are no alternative options available. The lowest effective dose should be administered when use is necessitated. • CYP3A4 enzyme inducers such as NVP, EFV, or etravirine may make Methergine less effective, requiring additional uterotonic medications. Management in Resource-Limited Areas • Management of HIV-positive pregnancies in resource poor countries can be very different from the recommendations presented here. With limited medications, poor health infrastructure, reduced bottle feeding options, and less laboratory testing availability, these recommendations cannot always apply. POSTPARTUM CONTRACEPTION The postpartum period is an important time to discuss safe sex practices and provide comprehensive family planning services. Contraception counseling, when initiated during prenatal care, is associated with more effective contraception use postpartum. • A dual protection strategy using barrier protection such as condoms and another effective contraception method should be considered in HIV-infected women. • Long-term reversible contraception (LARC) methods such as injectables, implants, and intrauterine devices may serve as options. • Drug interactions between oral contraceptive pills and ARV medications have been observed in pharmacokinetic studies. Studies are ongoing to investigate clinical implications and alternative contraception methods are recommended in cases of known drug interactions. • Although conflicting results have been published regarding possible increased risk of HIV transmission in women using hormonal contraception (HC), the World Health Organization and CDC recommend HC may be used in women with HIV who do not have other contraindications. COINFECTION WITH VIRAL HEPATITIS Some women with HIV are coinfected with hepatitis B (HBV) or hepatitis C (HCV) virus. Antepartum screening is recommended. The hepatitis B vaccine series should be initiated for those women screening negative. Women with chronic HBV should be screened for hepatitis A antibodies and receive the hepatitis A virus vaccine series if they screen negative. Hepatitis B/HIV Coinfection • Consultation with an expert is recommended for management of pregnant women with HIV/HBV coinfection. • T reatment with interferon alpha or pegylated interferon alpha is not recommended during pregnancy. • Women with chronic HBV who require HAART or HBV treatment should receive a three-drug regimen including a dual NRTI/nucleotide analogue reverse transcriptase P.317 inhibitor (NtRTI) backbone of tenofovir plus lamivudine or emtricitabine. These drugs show activity against HBV. T riple therapy is indicated to prevent HBV drug resistance. • An elevation of hepatic enzymes may occur following antiretroviral therapy initiation due to an immune-mediated flare in HBV disease from immune reconstitution syndrome, particularly in women with a low CD4 cell count. • HBV may increase the hepatotoxicity of certain agents, specifically PIs and NVP. Women with HIV/HBV coinfection should be counseled about signs and symptoms of liver toxicity. • Liver function tests should be obtained 1 month after starting treatment and then at least every 3 months. • Discontinuation of ARVs postpartum may result in exacerbation of HBV infection; liver function tests should be monitored and treatment reinitiated for HIV and HBV if a flare is suspected. • Infants should receive hepatitis B immunoglobulin and the first dose of the HBV vaccine series within 12 hours of birth. The second dose of the HBV series should be administered at 1 month; the third dose at 6 months. Hepatitis C/HIV Coinfection • The seroprevalence of HCV in HIV-positive pregnant women is 17% to 54%. • Pegylated interferon alpha is not recommended, and ribavirin is contraindicated during pregnancy. • Coinfection significantly increases perinatal HCV transmission. Maternal HCV/HIV coinfection may also increase risk for perinatal HIV transmission. • Effective combination therapy with three drugs should be considered for all HCV/HIV-infected women regardless of CD4 count and viral load. • These women can also experience a transient worsening in symptoms due to immune-mediated flare in HCV disease. • HCV may increase the hepatotoxicity of certain agents, specifically PIs and NVP. See recommendations for HBV for testing protocol (as mentioned earlier). • Intrapartum management of HIV/HCV-coinfected women is no different from management of HIV infection alone. Decisions concerning mode of delivery in HCV/HIV-coinfected pregnant women should be based on HIV considerations alone. • Infants should receive HCV antibody testing after 18 months of age. If earlier testing is indicated or desired, HCV RNA testing can be performed between 3 and 6 months of age. SUGGESTED READINGS American College of Obstetricians and Gynecologists. ACOG committee opinion no. 234: scheduled cesarean delivery and the prevention of vertical transmission of HIV infection. Int J Gynecol Obstet 2001 ;73:279-281. American College of Obstetricians and Gynecologists. ACOG committee opinion no. 313: the importance of preconception care in the continuum of women's health care. Obstet Gynecol 2005;106(3):665-666. http://www.ncbi.nlm.nih.gov/pubmed/16135611. Accessed April 5, 2013. Apetrei C, Marx PA, Smith SM. The evolution of HIV and its consequences. Infect Dis Clin North Am 2004;18(2):369-394. Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep 2006;55(RR-14):1-17; quiz CE1-CE4. http://www.ncbi.nlm.nih.gov/pubmed/16988643. Accessed April 5, 2013. P.318 Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med 2011 ;365(6):493-505. Cooper ER, Charuat M, Mofenson L, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr 2002;29(5):484-494. Dao H, Mofenson LM, Ekpini R, et al. International recommendations on antiretroviral drugs for treatment of HIV-infected women and prevention of mother-to-child HIV transmission in resource limited settings: 2006 update. Am J Obstet Gynecol 2007;197(3)(suppl): S42-S55. Hammer SM. Clinical practice. Management of newly diagnosed HIV infection. N Engl J Med 2005;353(16):1702-1710. Panel on Treatment of HIV-Infected Pregnant Women and Prevention of Perinatal Transmission. Recommendations for use of antiretroviral drugs in pregnant HIV-1-infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf. Accessed April 5, 2013. 25
More medical literature on Medic.Studio
More on the topic 24 HIV in Pregnancy:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|