23 Postpartum Care and Breast-feeding
Meghan E. Pratts
Shari Lawson
POSTPARTUM CARE
Immediate postpartum care includes monitoring vital signs, managing and relieving pain, and observing for complications. Patients who have had a cesarean section should receive special attention, recognizing that they are postsurgical patients.
As the risk of postpartum complications decreases, attention should be turned to education. Important issues to cover include maternal self-care, appropriate sexual and physical activity, breastfeeding, and infant care and nutrition.Common Postpartum Complications
• Postpartum hemorrhage has various definitions: (a) estimated blood loss of greater than 500 mL for a vaginal delivery or greater than 1,000 mL for a cesarean delivery; (b) a 10% change in hematocrit between admission and the postpartum period; or (c) excessive bleeding that produces symptoms requiring transfusion of packed erythrocytes. Excessive blood loss that occurs within 24 hours of delivery is termed primary or acute postpartum hemorrhage, whereas bleeding that occurs more than 24 hours after delivery (up to 6 weeks) is termed secondary or late postpartum hemorrhage. The incidence of postpartum hemorrhage is approximately 4% with vaginal delivery and 6% with cesarean delivery.
• Postpartum febrile morbidity is defined as a temperature higher than 38.0°C on at least two occasions at least 4 hours apart after the first 24 hours postpartum. Common causes include breast engorgement, atelectasis, urinary tract infection, endomyometritis, drug reaction (especially with misoprostol use), and wound infection. Less common causes of postpartum fever include retained products of conception (especially if bleeding is heavier than normal), pelvic abscess, infected hematoma, pneumonia (particularly if the patient received general anesthesia), ovarian vein thrombosis, and septic pelvic thrombophlebitis.
All maternal fevers should be reported to the newborn nursery.• Urinary tract infection is common in pregnancy and after catheterization; culture should be considered based on clinical examination.
• Endomyometritis complicates 1% to 3% of vaginal deliveries and is up to 10 times more common after cesarean delivery. It presents as fever, uterine fundal tenderness, malaise, or foul-smelling lochia and is usually a polymicrobial infection of Gram-positive aerobes (groups A and B streptococci, enterococci), Gram-negative aerobes (Escherichia coli), and anaerobes (Peptostreptococcus, Peptococcus, Bacteroides) from the genital tract. Bacteremia may be present in 10% to 20% of cases. Endomyometritis should be treated with intravenous antibiotics until the patient is clinically improved and afebrile for 24 to 48 hours. The American College of Obstetricians and Gynecologists (ACOG) recommends treatment with gentamicin (1.5 mg/kg every 8 hours) and clindamycin (900 mg
P.287 every 8 hours), with the addition of ampicillin (2 g every 4 to 6 hours) if fever persists after initial treatment. Some practitioners simply begin initial therapy with the triple antibiotic regimen. Daily dosing of gentamycin (5 mg/kg every 24 hours) has been shown to be as efficacious and more cost-effective than the low-dose regimen. Further treatment with oral antibiotic therapy is unnecessary once the patient has been afebrile for at least 24 hours and her symptoms have improved. Response to antibiotic treatment is usually prompt. Persistent fever after 48 to 72 hours of antibiotic treatment necessitates further evaluation.
• Septic pelvic thrombophlebitis (SPT) is rare and is more frequently associated with cesarean section. It is characterized by high spiking fevers despite appropriate antibiotics. Patients tend to feel well between fevers and have no complaint of pain. Imaging is frequently obtained to look for an abscess, but the pelvic thromboses with SPT are not always seen on computed tomography or magnetic resonance imaging, so the diagnosis is made based on clinical examination and exclusion of other causes.
Continuation of intravenous antibiotics and the potential addition of heparin anticoagulation have been suggested for treatment, although this treatment regimen remains controversial.• Hypertension is defined as blood pressure (BP) of 140/90 mm Hg or higher, taken with the patient in a seated position on two or more occasions at least 6 hours apart. Preeclampsia or eclampsia can present postpartum, even in the absence of antenatal complications. Any pressure reading of 140/90 mm Hg or higher should be evaluated by repeating BP measurement, testing urine for protein, and assessing for other signs and symptoms of preeclampsia. In those women who had antenatal preeclampsia, spontaneous postpartum diuresis and normalization of BP are generally expected. Hypertension from preeclampsia can persist for up to 6 weeks, however, and may require further evaluation and treatment.
Postpartum Immunizations
• ImmunizationsZinjections that may be offered postpartum include hepatitis A and B, rubella, rubeola, pertussis, and varicella, all as indicated.
• Rh D immunoglobulin: An unsensitized Rh-negative woman who delivers an Rh-positive infant should receive 300 μg of Rh D immunoglobulin within 72 hours of delivery even if Rh immunoglobulin was given antepartum. If there is laboratory evidence of excessive maternal-fetal hemorrhage, additional doses may be required. The blood bank should perform a rosette test or the Kleihauer-Betke test to assess the amount of maternal-fetal blood mixing and to calculate the additional amount of Rh D immunoglobulin to administer.
• Rubella vaccine: Mothers who are rubella nonimmune should receive the measles-mumps-rubella (MMR) vaccine prior to discharge after delivery. Use of monovalent rubella vaccine (i.e., Rubivax) is generally not appropriate because MMR is more cost-effective and because many women without immunity to rubella also lack immunity to rubeola (measles). Breast-feeding is neither a contraindication to MMR vaccination nor should breast-feeding be discouraged after MMR injection.
Discharge from Hospital
• When no complications occur, mothers may be discharged 24 to 48 hours after vaginal delivery and 24 to 96 hours after cesarean delivery. The following criteria should be met:
• Vital signs are stable and within normal limits.
• Uterine fundus is firm and involuting (within 24 hours, a postpartum uterus without fibroids should decrease to 20-week size).
P.288
• The amount and color of lochia are appropriate—red, less than a heavy period, and decreasing.
• Urine output is adequate.
• Perineal pain is adequately controlled with sitz baths, ice packs, and analgesics.
• Any surgical incisions or vaginal repair sites are healing well without signs of infection.
• The mother is able to eat, drink, ambulate, and void without difficulty.
• No medical or psychosocial issues are identified that preclude discharge.
• The mother has demonstrated knowledge of appropriate self-care and care of her infant.
• The issue of contraception has been addressed.
• Appropriate immunizations and Rh D immunoglobulin, if appropriate, have been administered.
• Follow-up care has been arranged for mother and infant.
• Infant nutritional needs have been addressed.
Outpatient Postpartum Visit
• The postpartum visit can be scheduled for 4 to 6 weeks postpartum unless a problem that requires closer follow-up is identified. For example, women with hypertensive complications should have a BP check and brief assessment within 1 week of discharge. For women with a history of postpartum depression or a known mood disorder, closer follow-up is warranted. Immunization status should be reviewed and vaccines that were not given immediately postpartum may be offered. The following are other important elements of routine postpartum visits:
Physical Exam
• BP, breast, abdomen, and pelvic examination (including vaginal repair assessment)
• At 2 weeks postpartum, the nonmyomatous uterus is usually not palpable abdominally.
• By 6 weeks postpartum, the uterus should return to 1.5 to 2.0 times its nonpregnant size.
• By 6 weeks postpartum, lochia should be essentially absent.
• If lochia is persistent, it should be reevaluated at 10 to 12 weeks. If still bleeding, evaluation is warranted, including measurement of serum human chorionic gonadotropin.
Sexual Activity and Contraception
• See discussion in “Breast-feeding” section and Chapter 32 for contraception topics.
• When the perineum is healed and bleeding decreased, sexual activity may be safely resumed.
• Any significant dyspareunia should be evaluated.
Depression Screening
• Assess psychosocial well-being; consider depression screening surveys.
• If there is evidence of depression, antidepressant medication should be considered, and the patient should be referred for mental health care. If you elect to start antidepressant medication, the patient should also be screened for a personal history or a family history of bipolar disorder.
• Thyroid-stimulating hormone level may be determined to evaluate postpartum hypothyroidism.
P.289
Antenatal Complications
• Patients with preeclampsia should be followed to ensure resolution of symptoms and exclude underlying
hypertensive or renal disease.
• Women with gestational diabetes should be screened for diabetes at their postpartum visit due to their increased risk of underlying diabetes outside of pregnancy.
BREAST-FEEDING
Recommendations
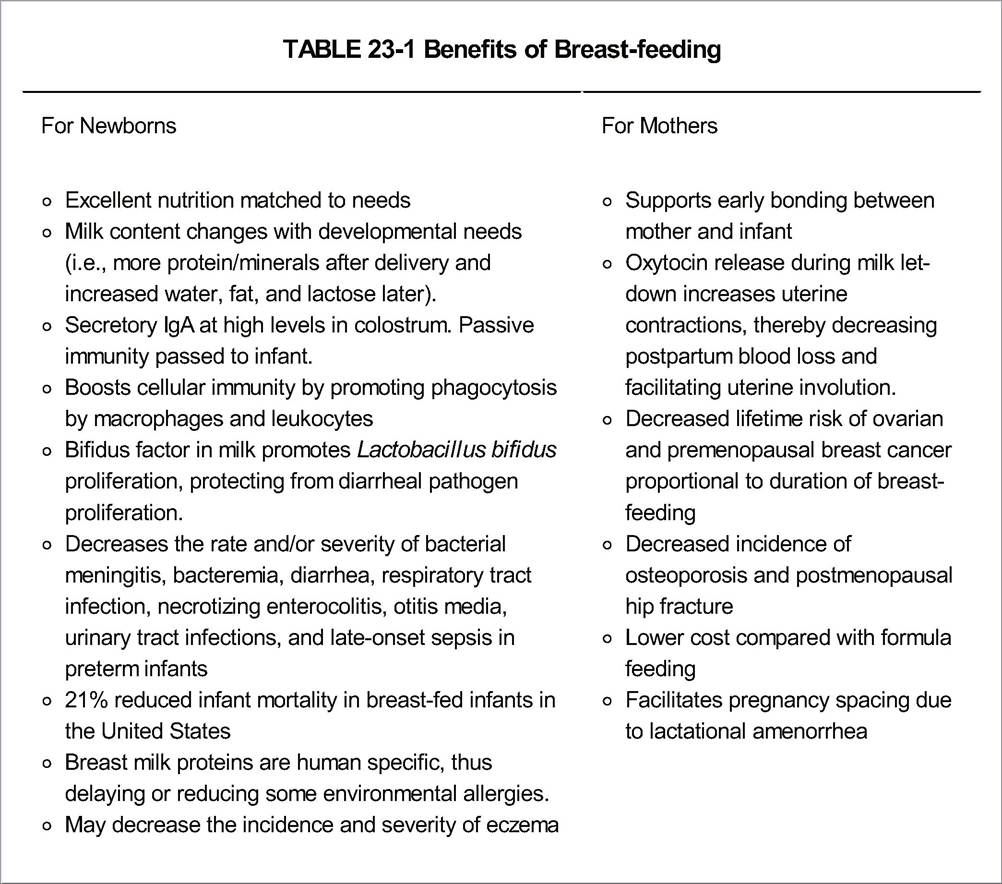
• The American Academy of Pediatrics advises exclusive breast-feeding for the first 6 months of life and partial breast-feeding (plus complementary foods) for at least 12 months (Table 23-1).
P.290
• The World Health Organization recommends continued partial breast-feeding for 2 or more years.
• Breast-feeding should be encouraged as soon as possible after delivery. Infants and mothers who initiate breast-feeding within the first hour after delivery have a higher success rate than those who delay.
• Newborns should be fed every 2 to 3 hours until satiety. Feeding for at least 5 minutes at each breast at each feeding on postpartum day 1 and gradually increasing feeding time over the next few days will allow optimal milk let-down with less nipple soreness.
• Arouse nondemanding infants every 4 hours for feeding. Frequent breast-feeding establishes maternal
milk supply, prevents excessive engorgement, and minimizes neonatal jaundice.
• Breast-feeding may be associated with initial minor discomfort. Painful breasts should be assessed and positioning reevaluated. Nursing on the less sore breast first, rotating stress points on nipples, and breaking suction before removing the infant may help. Nipple tenderness can be treated with lanolin cream or all-purpose nipple ointment.
• Breast-feeding increases maternal caloric requirements by 500 to 1,000 kcal/day and increases the risk of deficiencies in magnesium, vitamin B6, folate, calcium, and zinc. Thus, women should be encouraged to continue taking their prenatal multivitamin supplement. Human milk may not provide adequate iron for premature newborns or for infants older than 6 months. These infants, and babies of mothers with iron deficiency, should receive iron supplements. Infants who are breast-fed should also receive vitamin D supplementation because human milk does not provide an adequate supply.
• Women who are not breast-feeding will experience breast engorgement about 3 days postpartum, which is often uncomfortable. Breast binding, ice packs, and avoiding nipple stimulation are recommended.
• Healthy People 2020 goals are 81.9% of all mothers breast-feeding immediately postpartum, 60.6% at 6 months, and 34.1% at 12 months.
Contraindications to Breast-feeding
• Some structural problems make breast-feeding difficult and sometimes impossible. These include tubular breasts, hypoplastic breast tissue, true inverted nipples (rare), and surgical alterations that sever the milk ducts.
• Contraindications to breast-feeding include the following:
• Mother actively using drugs of abuse, including excessive alcohol
• Infant with galactosemia
• Maternal HIV infection in a developed country. In developing countries, the benefits of breast-feeding may outweigh the small risk of HIV transmission.
• Maternal active, untreated tuberculosis or women with human T-cell lymphotropic virus type I or II. Women can give their infant expressed breast milk and can breast-feed once their treatment regimen is well established.
• Active untreated maternal varicella. Once the infant has been given varicella zoster immunoglobulin, expressed milk is allowed if there are no lesions on the breast. Within 5 days of the appearance of the rash, maternal antibodies are produced, making breast milk beneficial for passive immunity.
• Active herpes simplex lesions on the breast
• Mothers who are receiving diagnostic or therapeutic radioactive isotopes or have had recent exposure to radioactive materials
• Mothers receiving antimetabolites or chemotherapeutic agents
P.291
Noncontraindications
• Healthy term infants with acquired or congenital cytomegalovirus should breast-feed for the benefit of maternal antibodies.
• Babies of mothers with hepatitis A or B may breast-feed as soon as the infant receives appropriate immunoglobulin and the first dose of hepatitis vaccine series. Special attention to avoid broken skin on or around the nipples of mothers with hepatitis B should be advised.
• Mothers with hepatitis C may breast-feed. There is no evidence for hepatitis C transmission via breast milk. Again, advise no breast-feeding if skin on or around nipples is broken.
Breast-feeding and Maternal Medications
• Nearly all antineoplastic, thyrotoxic, and immunosuppressive medications contraindicate breast-feeding (Table
23-2). In general, breast-feeding can continue during maternal antibiotic therapy. Although all major anticonvulsants are secreted in breast milk, they need not be discontinued unless the infant exhibits excessive sedation (Table 23-3). The Web site of the American Academy of Pediatrics (www.pediatrics.org) contains updated information on medication use in breast-feeding.
Breast-feeding and Contraception
• Return of fertility: In the non-breast-feeding woman, the average time to first ovulation is 45 days (range 25 to 72 days). The mean time to ovulation is 190 days in women who are breast-feeding exclusively (Fig. 23-1). The lactational amenorrhea method is 95% to 99% protective against pregnancy in the first 6 months
P.292 postpartum if strict criteria are followed. Feedings must be every 4 hours during the day and every 6 hours at night, and supplemental feedings should not exceed 5% to 10%.
TABLE 23-2 Medications Contraindicated during Breast-feeding
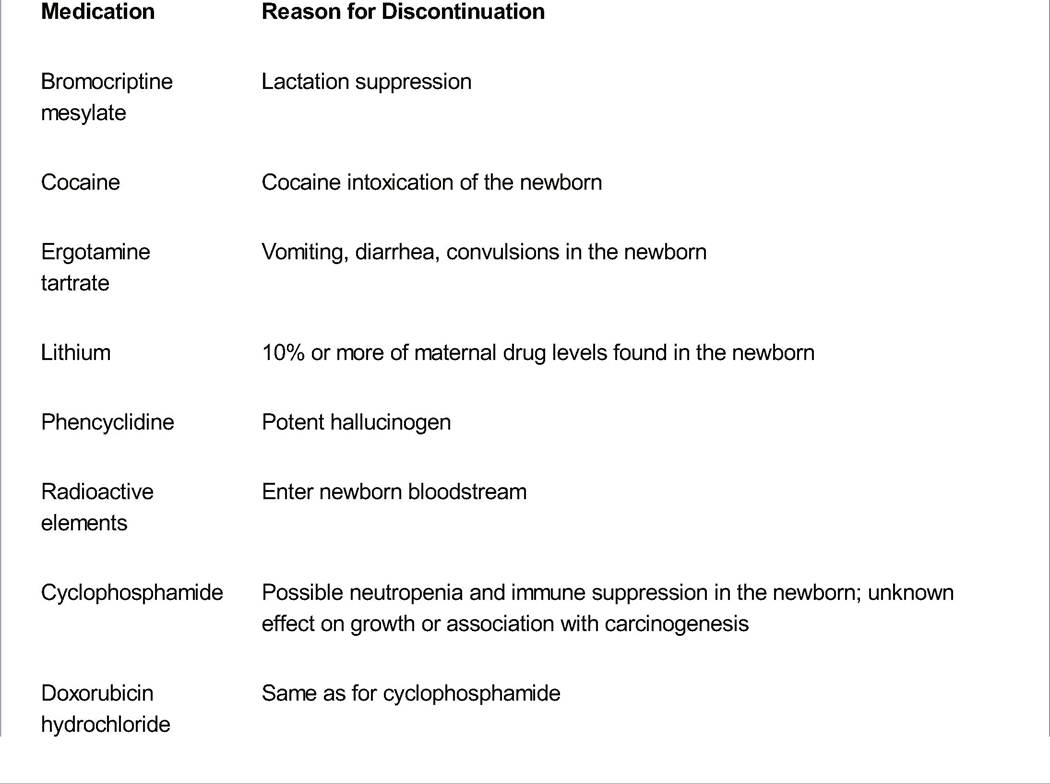
Adapted from Toxicology Network Web site. http://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm. Accessed November 29, 2014; Sachs HC; Committee on Drugs. The transfer of drugs and therapeutics into human breast milk: an update on selected topics. Pediatrics 2013;132(3):e796- e809.
TABLE 23-3 Common Medications Typically Compatible with Breast-feeding (with No Known Observable Changes in the Nursing Infant When Used)
• Captopril • Progestins
• Enalapril • Sumatriptan
• Hydrochlorothiazide • Warfarin
Adapted from Toxicology Network Web site. http://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm. Accessed November 29, 2014; Sachs HC; Committee on Drugs. The transfer of drugs and therapeutics into human breast milk: an update on selected topics. Pediatrics 2013;132(3):e796- e809.
• Contraception during lactation:
• Progestin-only contraceptives (e.g., mini pill, progestin injectables, progestin implants, and the levonorgestrel intrauterine device) do not affect the quality of and may increase the volume of breast milk. These contraceptives are among the preferred methods of hormonal contraception in the immediate postpartum period. Progestins are detectable in breast milk, but no evidence suggests adverse effects on the infant. The levonorgestrel intrauterine device (Mirena) or the etonogestrel implant (Implanon and Nexplanon) are the progestin-only options with the greatest efficacy; either may be inserted immediately postpartum or at the 6-week postpartum visit without affecting the quality and volume of breast milk.
• Nonhormonal methods of contraception (e.g., condoms, copper intrauterine device, sterilization) will have no impact on milk production and are also among the preferred methods of contraception for lactating mothers.
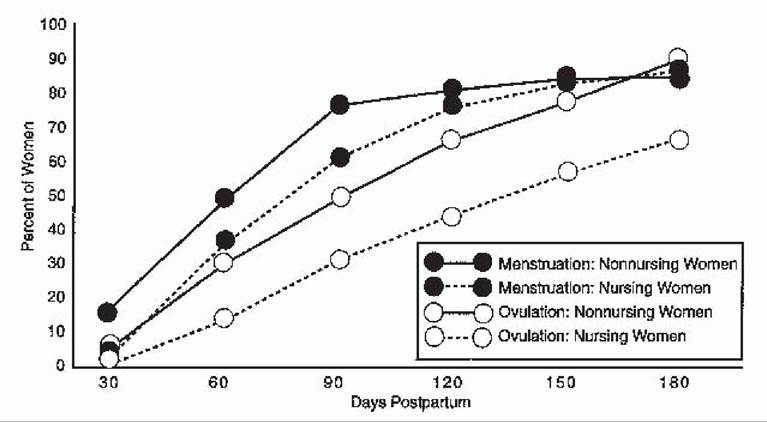
Figure 23-1. Postpartum return of menstruation and ovulation.
P.293
• The estrogen in combination estrogen-progestin oral contraceptive pills (OCPs) can reduce the quantity and duration of breast milk. ACOG recommends that if combination OCPs are preferred, they should not be started before 6 weeks postpartum and should only be started after lactation is well established and the infant's nutritional status is good. Some providers may initiate OCPs earlier if lactation is well established, if the patient declines other forms of contraception, or if the risk of repeat pregnancy is significant. In 2011, the CDC revised its recommendations for combined OCPs postpartum to include that in women without other risk factors for venous thromboembolism, it may be advantageous to begin combined OCPs as early as 21 days postpartum. The WHO recommends waiting at least 6 months before initiating combination OCPs for breastfeeding women worldwide. The U.S. Food and Drug Administration labeling committee recommends not using combination OCPs until the child is completely weaned.
Mastitis
• Mastitis is a breast infection that occurs in 1 % to 2% of breast-feeding women, usually between the first and fifth weeks postpartum. It is characterized by a localized sore and reddened, indurated area on the breast and is often accompanied by fever, chills, and malaise.
• Forty percent of mastitis is due to Staphylococcus aureus infection. Other common organisms include β- hemolytic streptococci, E. coli, and Haemophilus influenzae.
• Treatment includes continued nursing, nonsteroidal anti-inflammatory pain medication, and antibiotics. Initial antibiotic therapy is often started with dicloxacillin 500 mg orally four times daily for 10 days. Clindamycin 300 mg orally four times per day may be used in patients with an allergy to beta-lactams. Women should continue to express milk, starting on the affected side, to encourage complete emptying. If there is no improvement in 48 hours, antibiotic coverage should be changed to cephalexin or ampicillin with clavulanate (Augmentin). Persistent mastitis, particularly if there is evidence of abscess formation, requires evaluation for the possibility of methicillin-resistant S. aureus infection.
• The differential diagnosis for mastitis (Table 23-4) includes the following:
• Clogged milk ducts: a tender lump in the breast not accompanied by systemic symptoms that resolves after application of warm compresses and massage.
P.294
Unrelieved, clogged ducts can lead to galactoceles, cysts filled initially with milk that can become a thick cheesy substance that is difficult to drain. Galactoceles may require ultrasound treatment or needle aspiration if conservative methods fail.
TABLE 23-4 Diagnosis of Postpartum Breast Tenderness
| Finding | Engorgement | Mastitis | Plugged Duct |
| Onset | Gradual | Sudden | bgcolor=white>Gradual|
| Location | Bilateral | Unilateral | Unilateral |
| Swelling | Generalized | Localized | Localized |
| Pain | Generalized | Intense, localized | Localized |
| Systemic symptoms | Feels well | Feels ill | Feels well |
| Fever | No | Yes | No |
From Beckmann CRB, Ling FW, Barzansky BM, et al. Obstetrics and Gynecology, 4th ed. Baltimore, MD: Lippincott Williams and Wilkins, 2002:158, with permission.
• Breast engorgement while breast-feeding: bilateral, generalized tenderness of breasts, often occurring 2 to 4 days postpartum and associated with low-grade fevers. May be treated with application of warm compresses followed by hand or pump expression of milk and continued breast-feeding.
• Inflammatory breast cancer: a rare disease that presents with breast tenderness and breast skin changes.
• Breast abscess: a firm, tender, usually well-circumscribed mass. Breast sonography may be required for diagnosis, and incision and drainage may be necessary for treatment.
Decreased Milk Supply
• The normal volume of milk produced at the end of the first postpartum week is 550 mL/day. By 2 to 3 weeks, milk production is increased to approximately 800 mL/day. Production peaks at 1.5 to 2.0 L/day. Exclusively breast-fed newborns can be expected to lose 5% to 7% of birth weight in the first week. If the loss is >7% or very rapid, the adequacy of feeding should be assessed. Glycogen stores in fullterm infants generally provide sufficient initial nutrition. Therefore, supplemental feeding should be avoided unless medically indicated. Frequent breast-feeding and good maternal nutrition help maintain milk stores. Sheehan syndrome (postpartum pituitary necrosis) can also result in lack of milk production from low prolactin levels. It is characterized by postpartum lethargy, anorexia, weight loss, as well as inability to lactate. See Chapter 13.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG committee opinion no. 361: breastfeeding:
maternal and infant aspects. Obstet Gynecol 2007;109:279-280.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 76: postpartum hemorrhage. Obstet Gynecol 2006; 108:1039-1047.
Centers for Disease Control and Prevention. Update to CDC's U.S. Medical Eligibility Criteria for Contraceptive Use, 2010: revised recommendations for the use of contraceptive methods during the postpartum period. MMWR Morb Mortal Wkly Rep 2011 ;60:878-873.
French L, Smaill FM. Antibiotic regimens for endometritis after delivery. Cochrane Database Syst Rev2012; (8):CD001067.
Schanler RJ, ed. Breastfeeding Handbook for Physicians. Elk Grove Village, IL: American Academy of Pediatrics, 2006.
Truitt ST, Fraser AB, Gallo MF, et al. Combined hormonal versus nonhormonal versus progestin-only contraception in lactation. Cochrane Database Syst Rev2010;(12):CD003988.