46 Cervical Cancer
Amy H. Gueye
T eresa P. Diaz-Montes
Cervical cancer is the most common gynecologic malignancy in the world and the second most frequently diagnosed cancer in women worldwide after breast cancer.
Eighty percent of cases occur in developing countries. In the United States, cervical cancer is the third most common gynecologic malignancy and the second most common cause of gynecologic cancer death. Mortality and incidence rates for cervical cancer have declined in most developed countries due to the introduction of national standardized screening protocols using routine Papanicolaou smear (Pap test) and, more recently, human papillomavirus (HPV) screening.EPIDEMIOLOGY OF CERVICAL CANCER
Approximately 60% of women diagnosed with cervical cancer in developed countries have either never been screened or have not been screened in the preceding 5 years. The mean age for cervical cancer is 52.2 years, and the distribution of cases is bimodal, with peaks at 35 to 39 years and 60 to 64 years.
RISK FACTORS FOR CERVICAL CANCER
• The main risk factors for cervical cancer include exposure to HPV, smoking, parity, and immunosuppression; other factors that have been linked with cervical cancer are race/socioeconomic status and sexually transmitted infections.
• HPV infection is present in 99.7% of all cervical cancers. HPV is a nonenveloped, double-stranded DNA virus. The DNA is enclosed in a capsid shell with
P.593 major L1 and minor L2 structural proteins. The virus is spread through sexual contact. Thus, traditional risk factors for cervical cancer include early age at first coitus, multiple sexual partners, multiparity, lack of barrier contraception, and history of sexually transmitted infections.
î High-risk HPV types 16, 18, 31,33, 35, 45, 52, and 58 are associated with 95% of squamous cell carcinomas of the cervix. HPV 16 is most commonly linked with squamous cell cervical cancer.
HPV 18 is most commonly present in adenocarcinoma.î Most HPV infections are transient, resulting in either no change in the cervical epithelium or low-grade intraepithelial lesions that are often spontaneously cleared. The progression from high-grade lesion to invasive cancer takes approximately 8 to 12 years, yielding a long preinvasive state with multiple opportunities for detection through screening.
• Cigarette smoking is an independent risk factor in the development of cervical disease. Smokers have a 4.5-fold increased risk of carcinoma in situ (CIS) compared with matched controls. Additionally, an increased risk of cervical cancer has been noted in women exposed passively to tobacco smoke. The potential effect of smoking appears to be limited to squamous cell carcinoma of the cervix.
• Immunosuppression may increase the risk of developing cervical cancer, with more rapid progression from preinvasive to invasive lesions. Patients with HIV infection present earlier and with more advanced disease than noninfected patients. The Centers for Disease Control and Prevention has described cervical cancer as an AIDS-defining illness.
Race and socioeconomic status
î The incidence per 100,000 women per year of cervical cancer in the United States varies by ethnicity/race.
î African Americans, 11; Caucasians, 8; Native Americans, 12; Hispanics, 6; and Asians, 7
î These differences are partially accounted for by the increased risk of cervical cancer among women of low socioeconomic status. When access to care is made equal, the excessive risk of cervical cancer precursor lesions among African American women decreases.
î Racial differences are also apparent in survival; 58% of all African Americans with cervical cancer survive 5 years, compared with 72% of all whites.
SCREENING, PRESENTATION, AND DIAGNOSIS
Cervical neoplasia is presumed to be a continuum from dysplasia to CIS to invasive carcinoma. Screening for cervical cancer with the use of an exfoliative cytologic study (i.e., Pap smear) has significant effects on the incidence, morbidity, and mortality of invasive disease by facilitating the discovery and early treatment of precursor lesions.
See Chapter 45.Clinical Presentation
• Early symptoms:
• Abnormal vaginal bleeding may take the form of postcoital, intermenstrual, or postmenopausal bleeding.
• Serosanguineous or yellowish vaginal discharge, at times foul-smelling
• Dyspareunia
P.594
• Late symptoms:
• Hematometra due to occlusion of the endocervical canal
• Symptomatic anemia
• Pelvic pain
• Sciatic and back pain can be related to sidewall extension, hydronephrosis, or metastasis.
• Bladder or rectal invasion by advanced-stage disease may produce urinary or rectal symptoms (e.g., vaginal passage of stool or urine, hematuria, urinary frequency, hematochezia).
• Lower extremity swelling from occlusion of pelvic lymphatics or thrombosis of the external iliac vein.
Diagnosis of Cervical Cancer
• Most women with cervical cancer have a visible cervical lesion.
• On speculum examination, cervical cancer may appear as an exophytic cervical mass (Fig. 46-1) that characteristically bleeds on contact. Endophytic tumors develop entirely within the endocervical canal, and the external cervix may appear normal. In these cases, bimanual examination may reveal a firm, indurated, and often barrel-shaped cervix. The vagina should be inspected for extension of disease. Rectal exam provides information regarding the nodularity of the uterosacral ligaments and helps determine extension of disease into the parametrium.
• On general physical examination, advanced cervical cancer may present with pleural effusions, ascites, and/or lower extremity edema. Unilateral lower extremity edema may indicate involvement of the pelvic sidewall. Groin and supraclavicular lymph nodes may be indurated or enlarged, indicating spread of disease.
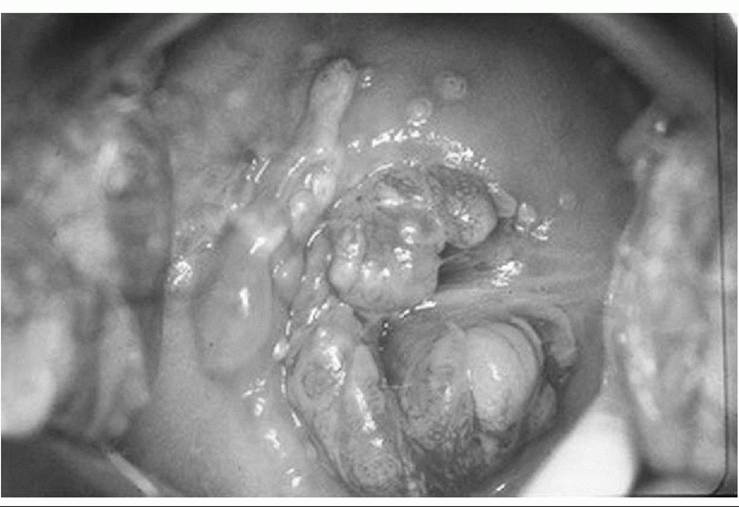
Figure 46-1. Photograph of the cervix demonstrating an exophytic cervical carcinoma. (Courtesy of Dr. Robert Giuntoli, The Johns Hopkins Hospital, Department of Gynecology and Obstetrics, Division of Gynecologic Oncology.)
P.595
• With obvious exophytic lesions, cervical biopsy is usually all that is needed for histologic confirmation.
• In patients with a grossly normal cervix and abnormal cytology on Pap smear, colposcopic examination with directed biopsies and endocervical curettage (ECC) is necessary. See Chapter 45.
• If a definite diagnosis of cervical cancer cannot be made on the basis of office biopsies, diagnostic cervical conization may be necessary.
DISEASE PROGRESSION, STAGING, AND PROGNOSIS
Routes of Cervical Cancer Spread
• Cervical cancer usually spreads by direct extension.
• Parametrial extension: The lateral spread of cervical cancer occurs through the cardinal ligament lymphatics and vessels, and significant involvement of the medial portion of this ligament may result in ureteral obstruction.
• Vaginal extension: The upper vagina is frequently involved (50% of cases) when the primary tumor has extended beyond the confines of the cervix.
• Bladder and rectal involvement: Anterior and posterior spread of cervical cancer to the bladder and rectum is uncommon in the absence of lateral parametrial disease.
Cervical cancer may also progress via lymphatic spread (Fig. 46-2). The cervix is drained by preureteral, postureteral, and uterosacral lymphatic channels.
• The following are considered first station nodes: obturator, external iliac, hypogastric, parametrial, presacral, and common iliac.
• Para-aortic nodes are second station, are rarely involved in the absence of primary nodal disease, and are considered metastases.
• The percentage of involved lymph nodes increases directly with primary tumor volume and stage of disease.
• Hematologic spread metastases from cervical carcinomas occur but are less frequent and are usually seen late in the course of the disease.
Staging of Cervical Cancer
• Staging of cervical cancer is based on clinical rather than surgical evaluation (Tables 46-1 and 46-2).
• Routine laboratory studies should include a complete blood count, complete metabolic profile, and urinalysis. No tumor marker has achieved widespread acceptance.
• Inspection and palpation should begin with the cervix, vagina, and pelvis and continue with examination of extrapelvic areas, including the abdomen and supraclavicular lymph nodes.
• Lymphangiograms, arteriograms, computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography, laparoscopy, or laparotomy findings are not used for clinical staging, but their results may be valuable for planning treatment. Imaging studies beyond chest x-ray should be obtained only when the findings will have an impact on treatment.
• Cervical cancer is staged according to the International Federation of Gynecology and Obstetrics (FIGO) system (see Table 46-1; Fig. 46-3). Lymph—vascular involvement does not alter the classification.
• When doubt exists concerning the stage to which a tumor should be assigned, the earlier stage is chosen. Once a clinical stage has been determined and treatment
P.596 has begun, subsequent findings do not alter the assigned stage. Overstaging and understaging of the parametria are problematic and may affect therapeutic decisions. FIGO stage correlates with prognosis, and strict adherence to the rules of clinical staging is necessary for comparison of results between institutions.
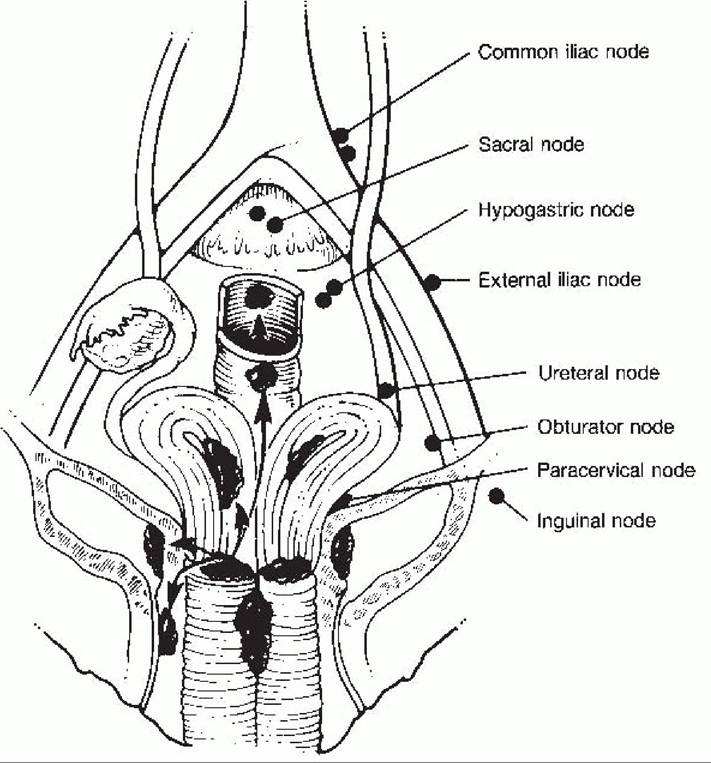
Figure 46-2. Possible sites of direct extension of cervical cancer to adjoining organs or metastases to regional lymph nodes. The uterus, cervix, and vagina are depicted bisected and opened to reveal the possible sites of tumor implantation. (From Scott JR, DiSaia PJ, Hammond CB, et al. Danforth’s Obstetrics and Gynecology, 7th ed. Philadelphia: Lippincott-Raven Publishers, 1997:909, with permission.)
• The distribution of patients by clinical stage is as follows: 38% stage I, 32% stage II, 25% stage III, 4% stage IV. Clinical stage of disease at the time of presentation is the most important determinant of survival regardless of treatment modality.
• Five-year survival declines as FIGO stage at diagnosis increases from stage IA (95%) to stage IV (14%).
• Only the subclassifications of stage I (IA1, IA2) require pathologic assessment.
• Vast discrepancies can exist between clinical staging and surgicopathologic findings, such that clinical staging fails to identify extension of disease to the para-aortic
P.597
P.598
P.599 nodes in 7% of patients with stage IB disease, 18% with stage IIB, and 28% with stage III. Thus, some clinicians emphasize surgical staging in women with locally advanced cervical carcinoma to identify occult tumor spread and allow treatment of metastatic disease beyond the traditional pelvic radiation field.
TABLE 46-1 International Federation of Gynecology and Obstetrics Staging System for Carcinoma of the Cervix (2009)
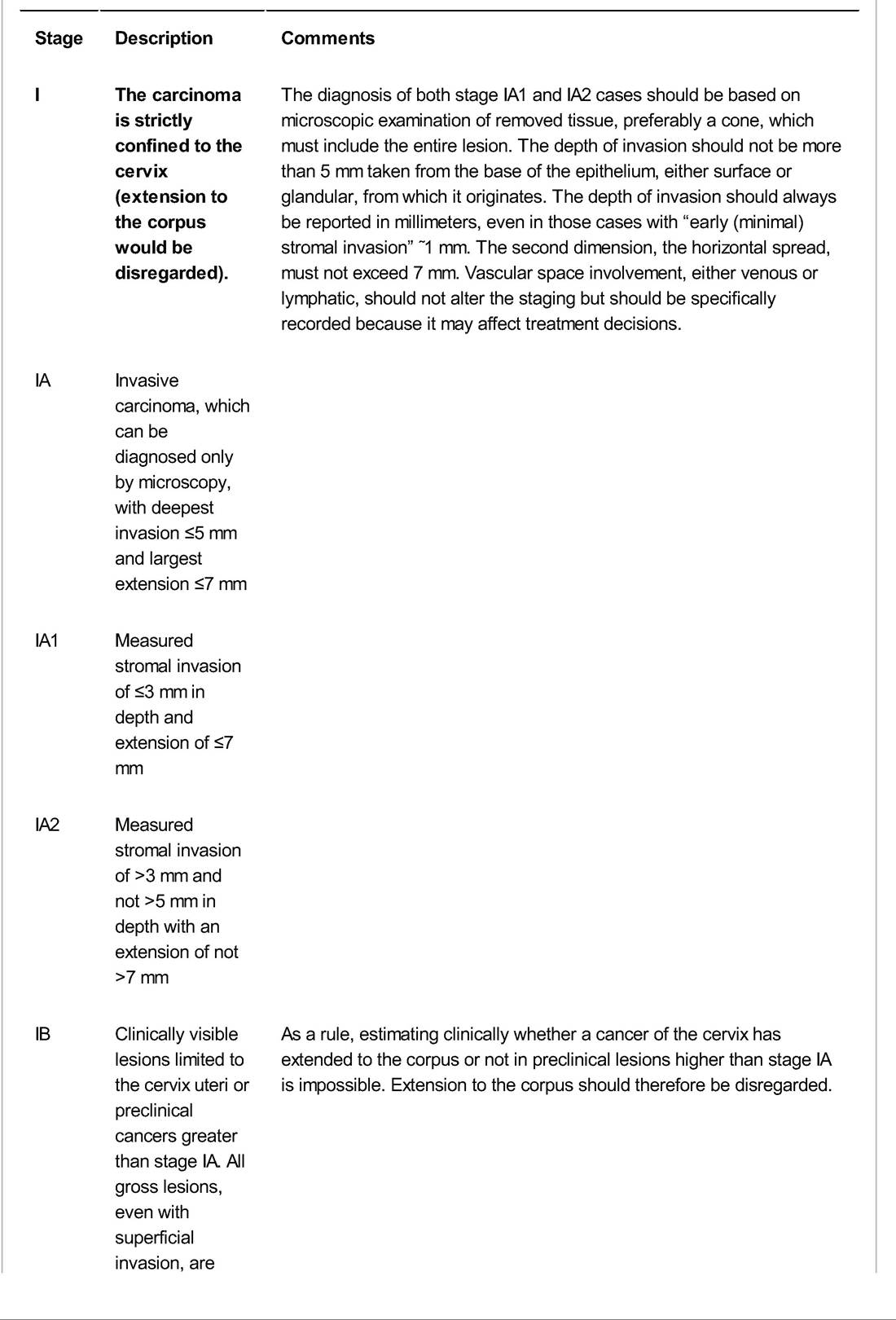
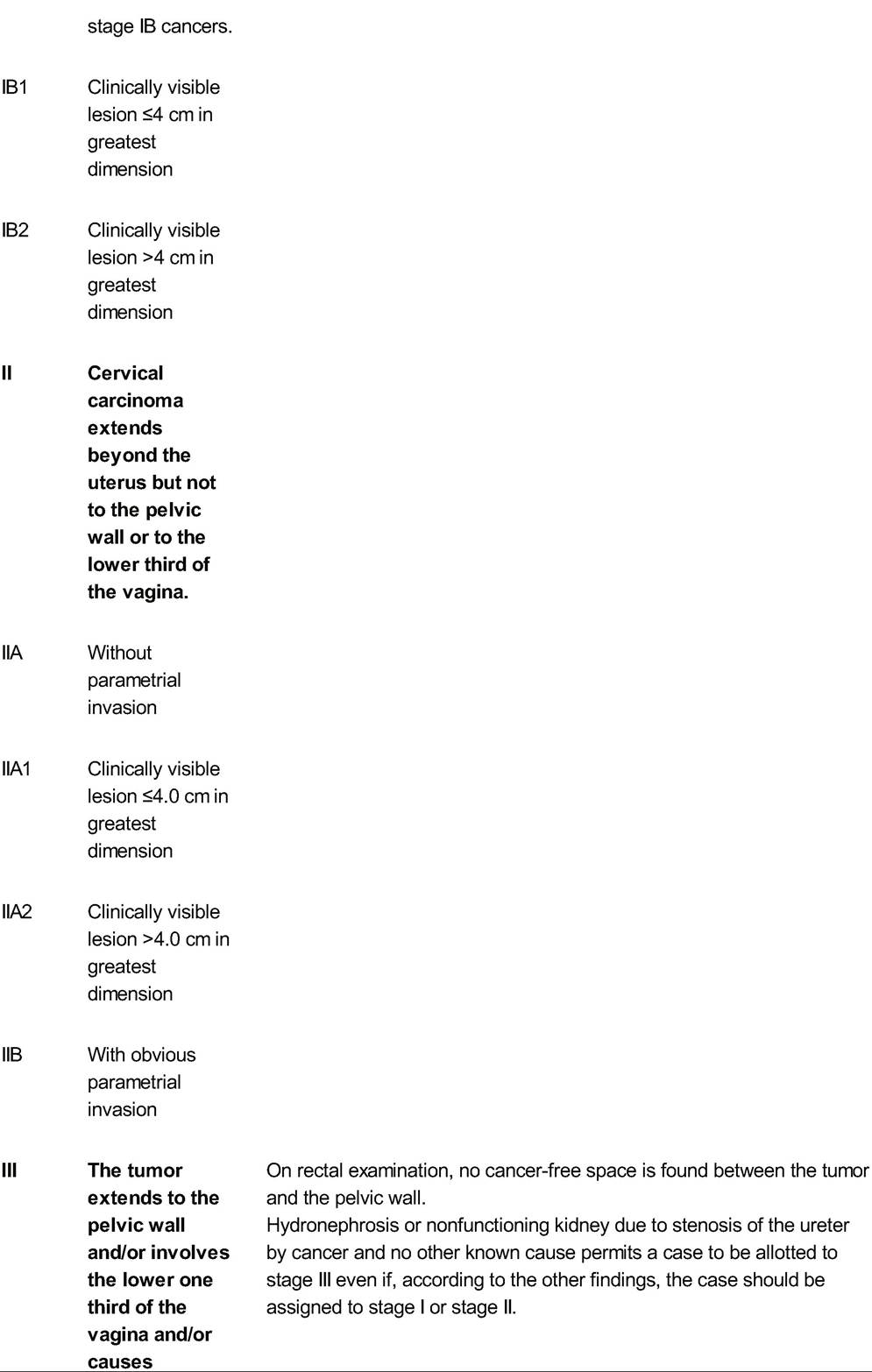
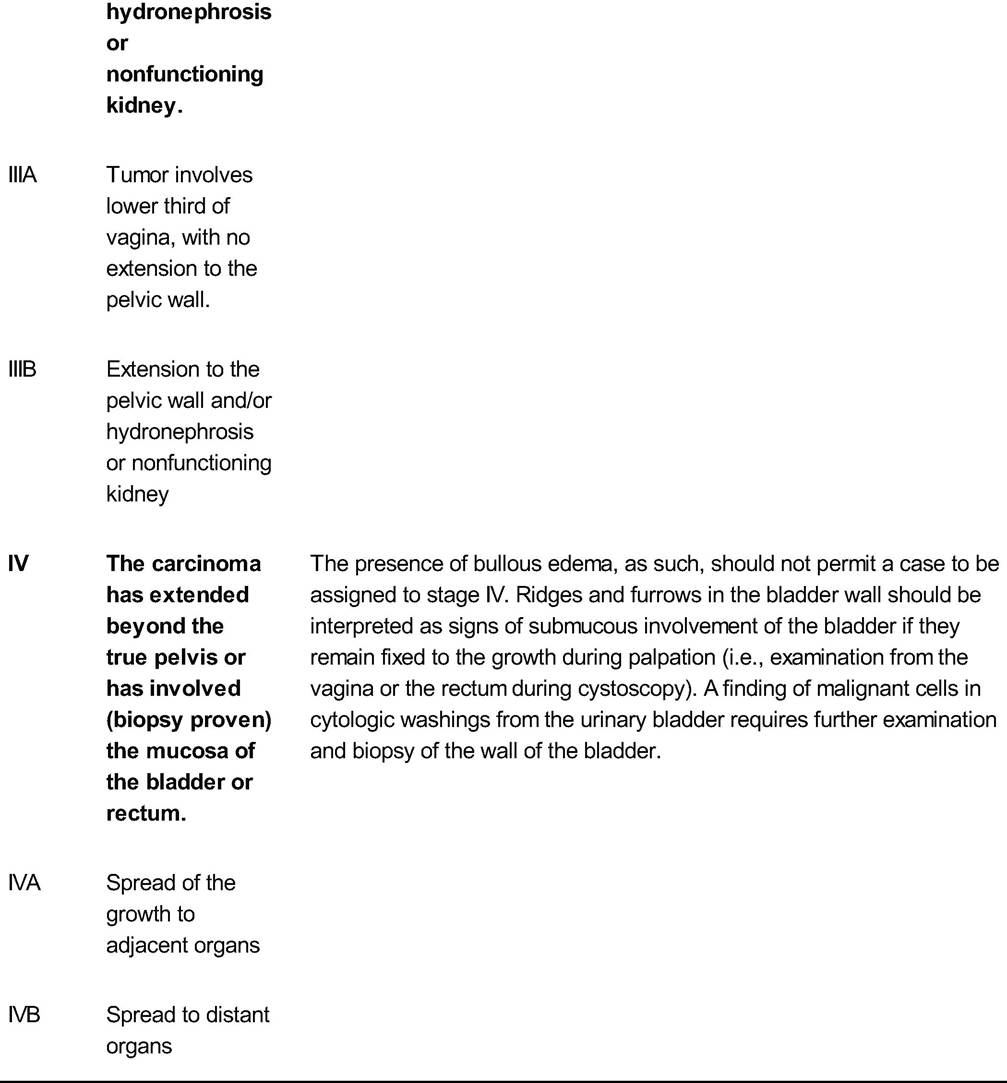
Adapted from Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet 2009; 105:103-104.
TABLE 46-2 Staging Procedures for Cervical Cancer
Physical examination13 Palpation of lymph nodes
Examination of vagina
Bimanual rectovaginal examination (under anesthesia recommended)
Radiologic studiesa lntravenous pyelogram (|vp)
Barium enema
Chest radiograph
Skeletal radiograph
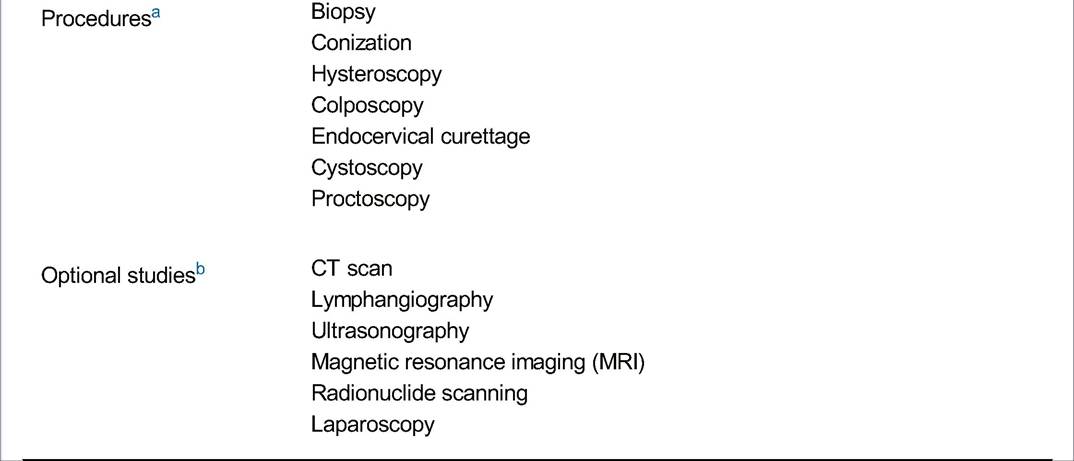
aAllowed for cervical cancer staging by International Federation of Gynecology and Obstetrics (FIGO). bInformation that is not allowed by FIGO to change the clinical stage but may be useful for treatment and planning.
Adapted from Berek JS, Hacker NF, eds. Practical Gynecologic Oncology, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2004.
Prognostic Factors for Cervical Cancer
• Prognosis is directly related to tumor characteristics including histologic subtype, histologic grade, FIGO stage, lymph node status, tumor volume, depth of invasion, and lymph—vascular space involvement (Table 46-3). Other prognostic variables include age, race, socioeconomic status, and immune status.
Histologic Subtype
• Conflicting data exist on the influence of histologic subtype on tumor behavior, prognosis, and survival.
• Invasive squamous cell carcinoma is the most common histologic type of cervical cancer, comprising about 80% of cases. Squamous cell carcinomas are also subclassified according to cell type: large cell keratinizing, large cell nonkeratinizing, and small cell types. Rarer types include verrucous carcinoma and papillary squamous cell carcinoma.
P.600
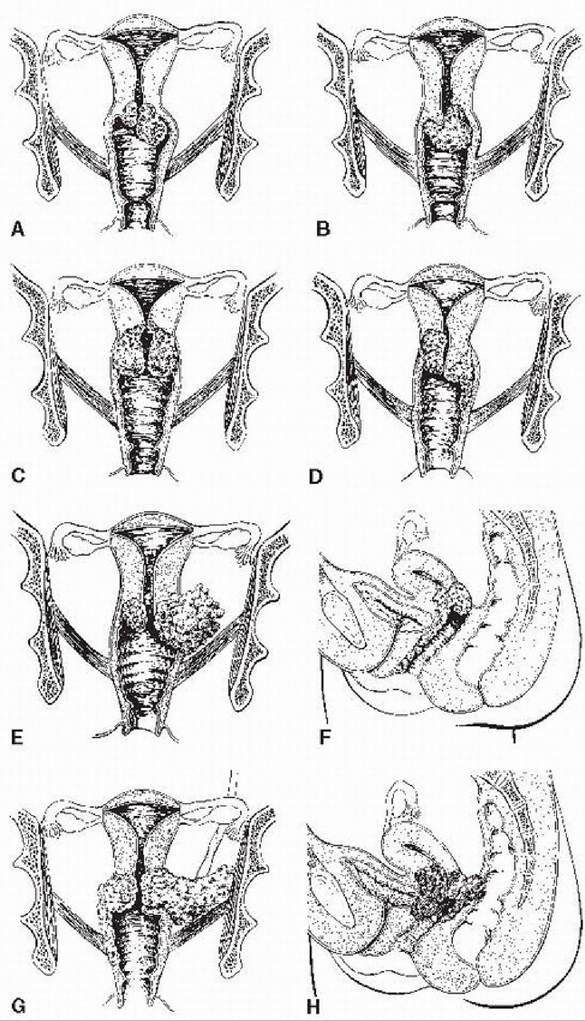
Figure 46-3. FIGO classification of carcinoma of the cervix. In stage I (A,B), only the cervix is involved. In stage II (C,D,E), the parametrium or upper two thirds of the vagina is involved. In stage III (F,G), the tumor involves the lower one third of the vagina or extends to the pelvic sidewall. In stage IV (H), areas beyond the true pelvis are involved or the bladder or rectal mucosa. (Adapted from Chi DS, Abu-Rustum NR, Hoskins WJ. Cancer of the cervix. In Rock JA, Jones HW III, eds. TeLindeS Operative Gynecology, 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:1378-1379, with permission.)
P.601
TABLE 46-3 Cervical Cancer Survival by International Federation of Gynecology and Obstetrics Stagea

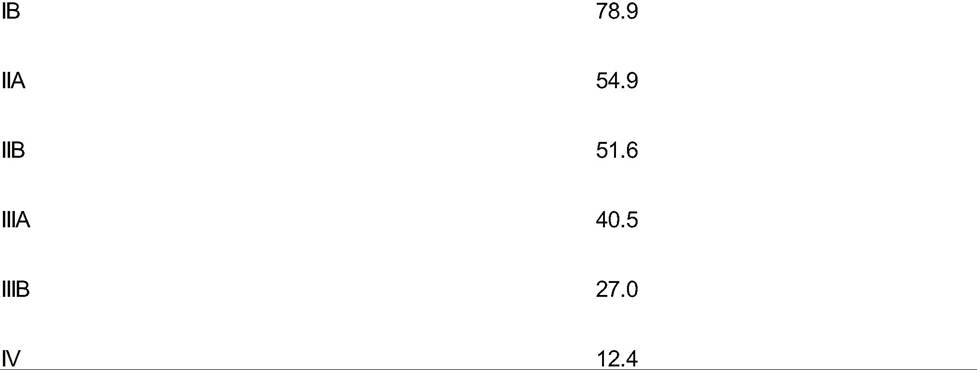
aBased on 1994 FIGO staging of carcinoma of the cervix uteri.
From Kosary CL. FIGO stage, histology, histologic grade, age and race as prognostic factors in determining survival for cancers of the female gynecological system: an analysis of 1973-87 SEER cases of cancers of the endometrium, cervix, ovary, vulva, and vagina. Semin Surg Oncol 1994;10:31-46.
• Adenocarcinomas comprise 15% of invasive cervical carcinomas. Grossly, cervical adenocarcinoma may appear as a polypoid or papillary exophytic mass. However, in nearly 15% of adenocarcinomas, the lesion is located entirely within the endocervical canal and escapes visual inspection.
î Mucinous adenocarcinoma is the most common type and is well differentiated with plentiful mucin production.
î Endometrioid carcinoma, 30% of cervical adenocarcinomas, resembles those typical of the uterine corpus.
î Clear cell carcinomas, approximately 4% of adenocarcinomas, are nodular, reddish lesions with punctate ulcers and cells with abundant, clear cytoplasm. Diethylstilbestrol exposure is a risk factor.
î Minimal deviation adenocarcinoma, or adenoma malignum, is reported to represent 1% of cervical adenocarcinomas.
• Primary cervical carcinoma with both malignant-appearing glandular and squamous elements is referred to as adenosquamous carcinoma. The clinical behavior of these tumors is controversial, with some studies suggesting lower survival rates and others higher survival rates than with the more common squamous tumors.
• Small cell carcinomas of the uterine cervix are similar to small cell neuroendocrine tumors of the lung and other anatomic locations. These tumors are clinically aggressive, with a marked propensity to metastasize. At diagnosis, disease is often disseminated, with bone, brain, and liver being the most common sites. Because of high metastatic potential, local therapy alone (surgery, radiation, or both) rarely results in longterm survival. Multiagent chemotherapy, in combination with external beam and intracavitary radiation therapy, is the standard therapeutic approach.
Histologic Grade
• Histologic differentiation of cervical carcinomas includes three grades.
• Grade 1 tumors are well differentiated with mature squamous cells, often forming keratinized pearls of epithelial cells. Mitotic activity is low.
P.602
• Grade 2 tumors are moderately well-differentiated carcinomas having higher mitotic activity and less cellular maturation accompanied by more nuclear pleomorphism.
• Grade 3 tumors are composed of poorly differentiated smaller cells with less cytoplasm and often bizarre nuclei. Mitotic activity is high. Poorly differentiated tumors have lower 5-year survival rates.
Other Prognostic Factors
• The most important factor in the prognosis for cervical cancer is clinical stage.
• Node status: Among surgically treated patients, survival is related to the number and location of involved lymph nodes.
• When pelvic nodes alone are involved, the 5-year survival rate is about 65%. Fiveyear survival drops to 25% when common iliac lymph nodes are positive, and involvement of para-aortic nodes further lowers survival. Bilateral pelvic lymph node involvement has a worse prognosis than unilateral disease.
• Tumor volume: Lesion size is an important predictor of survival, independent of other factors. Five-year survival rates for lesions 4 cm are approximately 90%, 60%, and 40%, respectively.
• Depth of invasion: Survival rates are inversely correlated with depth of stromal invasion.
• Lymph—vascular space invasion: No clear relationship exists between lymph—vascular space involvement and survival.
MANAGEMENT OF CERVICAL CANCER
Surgery and radiation therapy are the two modalities most commonly used to treat invasive cervical carcinoma.
Surgical Management
• In general, primary surgical management is limited to stages I through IIA.
• Advantages of surgical therapy:
• Allows for thorough pelvic and abdominal exploration, which can identify patients with a disparity between the clinical and surgicopathologic stages. These patients can be offered an individualized treatment plan based on their disease status.
• Permits conservation of the ovaries with their transposition out of radiation treatment fields
• Avoids the use of radiation therapy and its complications
• Disadvantages to surgical therapy:
• Risks of surgery, including bleeding; infection; and damage to organs, vessels, and nerves
• Radical hysterectomy results in vaginal shortening; however, with sexual activity, gradual lengthening may occur.
• Fistula formation (urinary or bowel) and incisional complications related to surgical treatment. These tend to occur early in the postoperative period and are usually amenable to surgical repair.
• Other indications for the selection of radical surgery over radiation:
• Concomitant inflammatory bowel disease
• Previous radiation for other disease
• Presence of a simultaneous adnexal neoplasm
P.603
• The abdomen is opened through either a low transverse incision using the Maylard or Cherney method or through a vertical midline incision. Once inside the peritoneal cavity, a thorough abdominal exploration should be performed to evaluate for visual or palpable metastases. Particular attention should be paid to the vesicouterine peritoneum for signs of tumor extension or implantation and palpation of the cardinal ligaments and the cervix. The para-aortic nodes should be palpated transperitoneally.
• Five distinct classes of hysterectomy are used in the treatment of cervical cancer (Table 46-4 and Fig. 46-4 for a brief comparison).
• Class I hysterectomy refers to the standard extrafascial total abdominal hysterectomy. This procedure ensures complete removal of the cervix with minimal disruption to surrounding structures (e.g., bladder, ureters). This procedure may be performed in patients with stage IA1 cervical cancer.
• Class II hysterectomy is also referred to as a modified radical hysterectomy or Wertheim hysterectomy and is well suited for patients with stage IA2 and small lesions that do not distort the anatomy.
• Class III hysterectomy, also known as radical abdominal or Meigs hysterectomy, is recommended for stages IB and IIA.
• Class IV or extended radical hysterectomy includes removal of the superior vesical artery, periureteral tissue, and up to three fourths of the vagina.
• In a class V or partial exenteration operation, the distal ureters and a portion of the bladder are resected. Class IV and class V procedures are rarely performed today because patients with disease extensive enough to require these operations can be more adequately treated using primary radiation therapy.
• In the past 15 years, surgeons have begun to investigate minimally invasive methods of treating early cervical cancers. These include laparoscopic procedures and, more recently, robotic-assisted laparoscopic procedures. Several small studies have compared laparoscopic and robotic radical hysterectomy with the open laparotomy approach. Findings include no significant differences in postoperative complications among the three groups, with longer mean operating times, shorter length of hospital stay, and smaller estimated blood loss for laparoscopic procedures compared with laparotomy.
Fertility-Preserving Surgical Options
• Fertility-preserving surgeries are used for younger women who have not completed childbearing and require treatment for early-stage cervical cancer. These methods include cervical conization and radical trachelectomy (i.e., Dargent operation) and appear to have similar recurrence rates to radical hysterectomy if candidates are selected appropriately.
• Cervical conization is generally reserved for stage IA cervical cancers but has also been performed with lymphadenectomy for IB1 cancers. Of the few published studies, no recurrences were noted with a minimum of 14 months follow-up.
• Radical trachelectomy can be performed for up to stage IB1 cancer with negative nodes in patients with tumors 46-4. Diagram of pelvic anatomy and types of hysterectomy. (From Berek JS, Hacker NF. Practical Gynecologic Oncology, 4th ed. Philadelphia, PA Lippincott Williams & Wilkins, 2005:356, with permission.)
• External photon beam radiation is usually delivered from a linear accelerator. Microscopic or occult tumor deposits from epithelial cancers require 4,000 to 5,000 cGy for local control. A clinically obvious tumor requires in excess of 6,000 cGy.
• Once external therapy has been completed, brachytherapy can be delivered using various intracavitary techniques, including intrauterine tandem and vaginal colpostats, vaginal cylinders, or interstitial needle implants. The tandem is placed through the cervix into the uterus, and the ovoids are placed in the lateral vaginal fornices (Fig. 46-5). Brachytherapy can be delivered as low-dose rates (LDR) or high-dose treatments. LDR treatments are inpatient over 3 to 4 days and receive 40 to 70 cGy/hr. High-dose rate treatments may be delivered on an outpatient basis over five visits.
î Two reference points are commonly used to describe the dose prescription for cervical cancer:
î Point A is 2 cm lateral and 2 cm superior to the external cervical os and theoretically represents the area where the uterine artery crosses the ureter.
î Point B is 3 cm lateral to point A and corresponds to the pelvic sidewall and to the location of the
obturator lymph nodes.
î The cumulative dose to point A, regardless of method, adequate for central control is usually between 7,500 and 8,500 cGy. The prescribed dose to point B is 4,500 to 6,500 cGy, depending on the bulk of parametrial and sidewall disease.
Chemotherapy
• Single-agent chemotherapy is used to treat patients with extrapelvic metastases as well as those with recurrent tumor who have been previously treated with surgery or radiation and are not candidates for exenteration procedures.
P.606
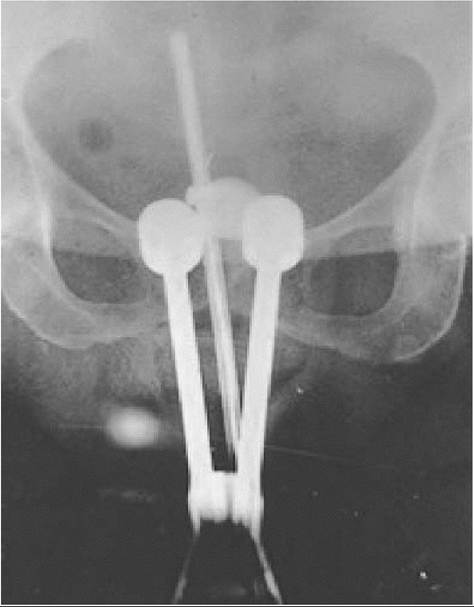
Figure 46-5. Brachytherapy: pelvic radiograph showing tandems and ovoids. (Image courtesy of Dr. Robert Giuntoli, The Johns Hopkins Hospital, Department of Gynecology and Obstetrics, Division of Gynecologic Oncology.)
• The best candidates for chemotherapy are those with an excellent performance status and disease that is both outside of the field of radiation and not amenable to surgical resection.
î Cisplatin has been the most extensively studied agent and has demonstrated the most consistent clinical response rates (20% to 25%).
• The most active combination chemotherapy regimens for cervical cancer contain cisplatin.
• The agents most commonly used in combination with cisplatin are bleomycin, 5-fluorouracil, mitomycin C, methotrexate, cyclophosphamide, and doxorubicin.
• A limited number of randomized trials comparing dual-agent regimens with either triple-agent regimens or single-agent regimens have demonstrated that combination therapy leads to a slightly higher response rate and a longer progression-free survival; however, no difference was found among the regimens in terms of
overall survival.
Combined Modalities
• Postoperative adjuvant radiation therapy has been advocated for patients with microscopic parametrial invasion, pelvic lymph node metastases, deep cervical invasion, and positive or close surgical margins. Postoperative radiation therapy reduces the rate of pelvic recurrence after radical hysterectomy in high-risk patients.
P.607
• Neoadjuvant chemotherapy: T rials testing the efficacy of preoperative chemotherapy suggest improved outcomes, but results have not been consistent.
• Chemoradiation confers significant survival benefit over radiation alone in the treatment of cervical cancer. When combined with radiation, weekly cisplatin administration reduces the risk of progression for stage IIB through stage IVA cervical cancer.
• Cisplatin acts as a radiosensitizer, yielding a large reduction in the rate of local recurrence and a more modest reduction in the rate of distant metastases.
Management by Stage of Disease
• Stage IA1 without lymph—vascular invasion is managed with conservative surgery, such as excisional conization or extrafascial hysterectomy. Conization may be used selectively if preservation of fertility is desired, provided that the surgical margins are free of disease. Patients treated with conization should be followed closely with Pap smear, colposcopy, and ECC every 3 months for the first year. For medically inoperable patients, stage IA carcinoma can be effectively treated with chemoradiation.
• Stage IA2 is associated with positive pelvic lymph nodes in 5% of cases. The preferred treatment of these lesions is modified radical (class II) hysterectomy with pelvic lymphadenectomy. In patients who desire preservation of fertility, radical trachelectomy with laparoscopic or extraperitoneal lymphadenectomy may be performed.
• In a radical trachelectomy, cervical and vaginal branches of the uterine artery are ligated, whereas the main trunk of the uterine artery is preserved. Once the blood supply has been controlled, the cervix is amputated at a point approximately 5 mm caudal to the uterine isthmus. The uterus is then suspended from the lateral stumps of the transected paracervical ligaments. Once the uterus has been suspended, isthmic cerclage is performed, using a technique similar to that used as prophylaxis against miscarriage. Subsequently, the vaginal and isthmic mucosa are reapproximated.
• Stages IB1, IB2, and IIA: Radical hysterectomy (class III hysterectomy) and radiation are equally effective in treating stages IB and IIA carcinoma of the cervix (studies based on 1994 FIGO staging).
• Management of patients with bulky stage I disease (IB2) is controversial. The two options are a class III hysterectomy or radiation. Often, surgery is first performed with postoperative radiation. Alternatively, a gynecologic oncology group study showed that weekly cisplatin 40 mg/m2 (six doses) with external radiation and a single implant to give 55 Gy at point B, followed by extrafascial hysterectomy, gave the best outcome.
• Stages IIB, III, IVA, and IVB: Radiation therapy is the treatment of choice for patients with stage IIB and more advanced disease. Long-term survival rates with radiation therapy alone are approximately 70% for stage I disease, 60% for stage II disease, 45% for stage III disease, and 18% for stage IV disease. With the routine use of chemoradiation, long-term survival and disease-free progression are expected to increase for all stages of disease. Patients with stage IVB disease are usually treated with chemotherapy alone or chemotherapy in combination with local radiation. These patients have a uniformly poor prognosis regardless of treatment modality.
Treatment-Related Complications
• Modern surgical techniques and anesthesia have reduced the operative mortality rate.
P.608
• Febrile morbidity is common after radical hysterectomy due to typical postoperative reasons.
• Major causes of morbidity include lower extremity venous thrombosis, vesicovaginal fistulas (6 months for an additional 2 years and every 6 months to 1 year thereafter.
• More frequent examinations are warranted if abnormal signs or symptoms develop.
• Pap smears should be obtained at every visit, with consideration for annual chest x-ray and intravenous pyelogram or abdominal pelvic CT.
• Cervical cancer detected within the first 6 months after therapy is termed persistent cancer. Disease diagnosed > 6 months later is referred to as recurrent disease.
• T reatment of recurrent cervical cancer is dictated by the site of recurrence and by the mode of initial therapy.
î Only patients with central recurrence and no evidence of disease outside the pelvis are candidates for pelvic exenteration.
Special Management Issues
Cervical Cancer in Pregnancy
• Cervical cancer is the most common malignancy in pregnancy, ranging from 1 in 1,200 to 1 in 2,200 pregnancies. Cervical cancer coincident with pregnancy requires complex diagnostic and therapeutic decisions that may jeopardize both mother and fetus.
• The symptoms of cervical cancer are the same in pregnant patients and nonpregnant patients. Pregnant women are at risk of delay of diagnosis of cervical cancer.
• Directed cervical punch biopsies can be performed safely during pregnancy when high-grade intraepithelial lesions or microinvasion is suspected.
• ECC should be avoided due to the risk of rupturing the amniotic membranes.
• Cervical conization should be performed only if it is strictly indicated and between 12 and 20 weeks of gestation.
• Pregnant women with cervical cancer should undergo the same evaluation as nonpregnant women.
• Because the bimanual examination may be difficult in pregnancy, MRI may be useful to identify extracervical disease.
• In patients with intraepithelial lesions or microinvasive disease stages IA1 and IA2, there appears to be no harm in delaying definitive therapy until after fetal lung maturity has been attained.
P.609
• Patients with less than 3 mm of invasion and no lymph—vascular space involvement may be followed to term and delivered vaginally.
• The major risk during delivery is hemorrhage due to tearing of the tumor.
• Recurrences of cervical cancer have been reported at the episiotomy site in women who deliver vaginally.
• Following vaginal delivery, these women should be reevaluated and treated at 6 weeks postpartum.
• If delivery is by cesarean section, extrafascial hysterectomy can be performed at the time of delivery or after a delay of 4 to 6 weeks if further childbearing is not desired.
• Patients with 3 to 5 mm of invasion or lymph—vascular invasion can also be safely followed until term.
• In these cases, however, surgical treatment should include a modified radical hysterectomy with pelvic lymph node dissection, performed either at the time of cesarean delivery or at 4 to 6 weeks postpartum.
• Radiation therapy is associated with survival rates comparable to those after surgical treatment.
• In patients with stages IB1, IB2, and IIA (studies based on 1994 FIGO staging), a delay in therapy in excess of 6 weeks may impact survival. If the diagnosis is made after 20 weeks of gestation, consideration may be given to postponing therapy until fetal viability.
• Standard treatment consists of classical cesarean delivery followed by radical hysterectomy with pelvic and para-aortic lymph node dissection; however, this procedure is associated with longer operative time and greater blood loss than in nonpregnant patients.
• Lower segment transverse cesarean section is not recommended because of the increased risk of cervical extension with this procedure that may increase intraoperative bleeding.
• Radiation therapy results in equivalent survival rates and may be preferable for patients who are poor surgical candidates.
Cervical Hemorrhage
• Profuse vaginal bleeding from cervical malignancies is a challenging therapeutic situation. Generally, conservative measures to control cervical hemorrhage are preferable to emergency laparotomy and vascular (i.e., hypogastric artery) ligation. Attention must first be directed toward the stabilization of the patient with appropriate intravenous fluid and blood product replacement.
• Immediate control of cervical hemorrhage can usually be accomplished with a vaginal pack soaked in Monsel solution (ferric subsulfate). Topical acetone (dimethyl ketone) applied with a vaginal pack placed firmly against the bleeding tumor bed has also been used successfully to control vaginal hemorrhage from
cervical malignancy.
• Definitive control of cervical hemorrhage can be accomplished with external radiation therapy of 180 to 200 cGy/day if the patient has not previously received tolerance doses of pelvic irradiation.
• Alternatively, arteriography can be used to identify the bleeding vessel(s), and Gelfoam or steel coil embolization can then be performed.
î Vascular embolization has the disadvantage of producing a hypoxic local tumor environment and potentially compromising the efficacy of subsequent radiation therapy.
P.610
CERVICAL CANCER AND GLOBAL HEALTH
• Cervical cancer is the leading cause of cancer death in women of developing countries where over 85% of worldwide deaths from cervical cancer are clustered in low-income countries.
• The World Health Organization estimates that over half a million women will be newly diagnosed with cervical cancer every year, and the majority of these women are between the ages of 15 and 45 years, living in developing nations. Regions at highest risk include East and West Africa, South Africa, Central Asia, and Middle Africa. It is estimated that by 2030, the majority (98%) of cervical cancer deaths will occur in developing countries.
• The disparity can be explained by the lack of widespread screening for cervical cancer. The Papanicolaou screening tool is neither feasible nor practical in most low-resource settings, as cytology requires infrastructure, expertise, and resources.
• Much research has been conducted on the “see and treat” method that makes use of the visual inspection with acetic acid (VIA) test as an alternative to the Pap smear in low-resource settings. This tool uses application of acetic acid directly to the cervix followed by visualization and immediate treatment of acetowhite lesions with cryotherapy or cervical conization. Women thus do not need to make several trips for screening and treatment.
î A large screening study performed in Bangladesh showed that among the 100,000 women screened with VIA, only half of the 5% who were screened positive returned for a colposcopy, and of those, only half returned for treatment.
î Across several large studies, VIA has shown varying sensitivities and specificities; one meta-analysis showed a sensitivity of 82% and a specificity of 60%.
• More recently, HPV screening has emerged as a good alternative or addition to VIA in low-resource settings. Minimal training is required for sample collection or may even be performed by the patient.
• A cost analysis in South Africa found that HPV DNA testing followed by treatment could decrease cervical cancer incidence by 27% for only $39 of years of life saved (YLS) compared to 26% for VIA followed by treatment. Cytology would decrease incidence by 19% in low-resource settings and would be more costly per YLS.
• Finally, an important debate in the global fight against cervical cancer will be the introduction of vaccines in low-income settings.
• Studies have shown that for the vaccine to be cost-effective, the three shots must cost between US $10 and $25. Although it will take several decades to see an impact on mortality, this will be an important milestone in overcoming the global cervical cancer burden.
SUGGESTED READINGS
Amant F, Van Calsteren K, Halaska MJ, et al. Gynecologic cancers in pregnancy: guidelines of an international consensus meeting. Int J Gynecol Cancer 2009;19(suppl 1):S1-S12.
Green JA, Kirwan JM, Tierney JF, et al. Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: a systematic review and meta-analysis. Lancet 2001 ;358:781- 786.
Hacker NF, Friedlander ML. Cervical cancer. In Berek JS, Hacker NF, eds. Practical Gynecologic Oncology, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2005.
Schiffman M, Castle PE, Jeronimo J, et al. Human papillomavirus and cervical cancer. Lancet 2007;370:890- 907.