44 Diseases of the Vulva and Vagina
Amelia M. Jernigan
Robert L. Giuntoli II
Vulvar and vaginal disease should be understood by its presentation, etiology, location, and associated systemic and laboratory findings.
Clinicians should have a low threshold to biopsy any suspicious vulvar abnormalities because the appearance of malignant lesions is often similar to that of benign processes. The majority of patients with vulvar cancer experience symptoms for at least months prior to diagnosis. Early biopsy of suspicious lesions is preferable in order to make a diagnosis of vulvar and vaginal malignancies, if present, and to potentially avoid progression to advanced disease.ANATOMY OF THE VULVA AND VAGINA
• The vulva is that area of skin encompassing the labia majora to the hymen. See Chapter 26.
• The vulva is bordered laterally by the genitocrural folds, anteriorly by the mons pubis, and posteriorly by the perineal body. The medial side of the labia minora to the hymen is known as the vulvar vestibule or introitus.
• Hart line is the thin zone of color and texture change between the labia minora and the vestibule, marking the transition from the skin of the external genitalia to the mucosa of the vestibule.
• Within the vestibule lie the urethral meatus, vaginal introitus, ostia of Bartholin glands (major vestibular glands), minor vestibular glands, and Skene ducts.
• Branches of the external and internal pudendal arteries provide the vascular supply to the vulva (Fig. 44-1).
• Sensory innervation of the anterior vulva is via the genitofemoral nerve and the cutaneous branch of the ilioinguinal nerve, whereas the posterior vulva and the clitoris are innervated by the pudendal nerve.
• The medial group of superficial inguinal nodes collects the lymphatic drainage of the vulva (Fig. 44-2).
P.569
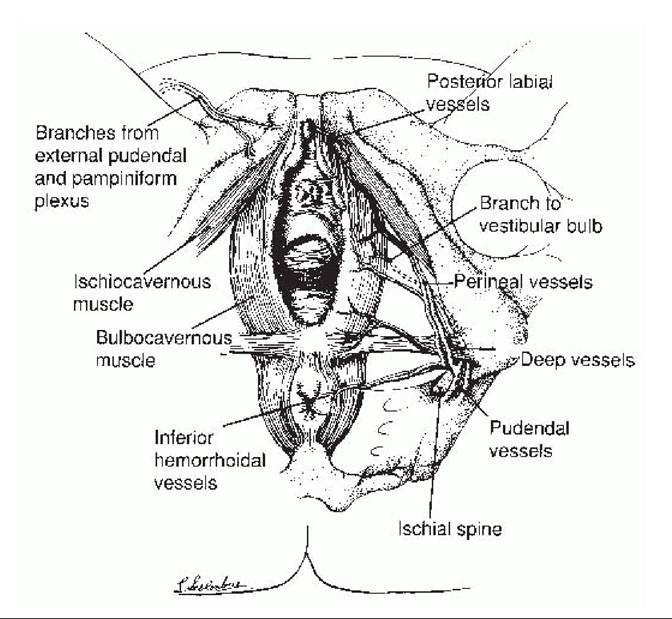
Figure 44-1.
Superficial vulvar musculature and vascular supply of the vulva. (From Rock JA, Jones HW, TeLinde RW. Te Linde’s Operative Gynecology, 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008:505, with permission.)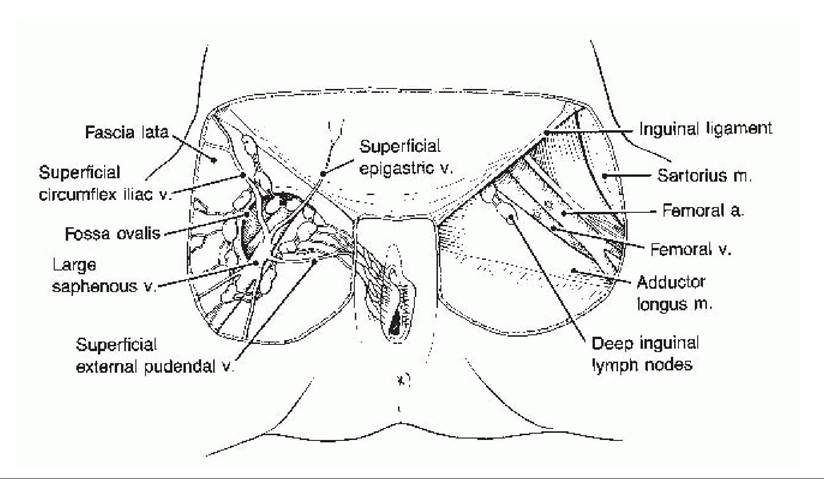
Figure 44-2. Superficial and deep lymphatic drainage of the vulva and femoral triangle. (From Rock JA, Jones HW, TeLinde RW. Te Linde’s Operative Gynecology, 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008:85.)
P.570
• The vagina is a hollow viscus extending from the hymenal ring to the vaginal fornices surrounding the proximal cervix; it is lined by hormone-responsive nonkeratinized stratified squamous epithelium.
• The vascular supply of the vagina is provided by the vaginal branch of the internal iliac artery and extensions of the uterine artery that form an anastomotic plexus along the lateral vaginal sulci.
• The distal vagina also receives blood from pudendal vessels, and the posterior wall receives contributions from the middle rectal artery.
• The vagina is innervated by fibers from the pudendal nerves and the vaginal plexus, which arises from the hypogastric plexus (sacral rami S2 to S4).
• The primary sites of lymphatic drainage for the vagina are the hypogastric, obturator, and external iliac lymph nodes via the lateral perivaginal plexus.
• The distal third of the vagina may also drain to the inguinofemoral nodes, and the posterior vagina may drain to the inferior gluteal, presacral, or perirectal lymph nodes.
INFECTIOUS DISEASES OF THE VULVA
• Sexually transmitted, viral, and fungal infections and parasite infestations of the vulva and vagina are discussed separately in Chapter 28.
• Bacterial skin infections of the vulva include folliculitis and furunculosis, most frequently caused by Staphylococcus, and cellulitis secondary to infection with Staphylococcus or Streptococcus.
• T reatment of initial infection: warm compresses three times a day (tid) and cephalexin 500 mg orally (PO) four times a day (qid) or dicloxacillin 500 mg PO qid or clindamycin 300 to 450 mg PO tid
• For recurrent infections: Add to previous regimen Hibiclens washes + 2% mupirocin ointment tid ? 10 days.
DERMATOSES AND INFLAMMATORY CONDITIONS
Behςet Syndrome
• Behpet syndrome is a rare chronic disease characterized by a triad of relapsing oral ulcers, genital ulcers, and ocular inflammation. The disease is most common in Japan and the Middle East.
• Other findings include acne, cutaneous nodules, thrombophlebitis, and colitis.
• Genital ulcers are small, painful, and deep and may result in fenestration of the labia. Ulcers generally heal in 7 to 10 days.
• Treatment options include topical (betamethasone valerate ointment 0.1%), intralesional (triamcinolone, 3 to 10 mg/mL, injected into ulcer base), or systemic corticosteroids (prednisone 1 mg/kg for severe involvement, especially central nervous system).
Hidradenitis Suppurativa
• Hidradenitis suppurativa is a chronic, painful apocrine gland disorder resulting from chronic occlusions of follicles that causes deep, suppurated subcutaneous nodules that form sinus tracts and confluent masses. The axillae and anogenital region are most frequently involved. The lesions wax and wane; flares are common with menstruation. The lesions ulcerate, resulting in draining sinuses and extensive scarring.
P.571
• The severity of this disease varies, and it can be graded by the Hurley clinical staging system:
• Stage I: single or multiple abscesses but no sinus tracts or scarring
• Stage II: recurrent abscesses, tract formation and scarring, widely separated lesions
• Stage III: diffuse or near diffuse involvement or multiple interconnected sinus tracts and abscesses across the entire area
• Superinfection of hidradenitis suppurativa is polymicrobial and cultures help guide treatment. The effectiveness of medical therapy wanes as deeper tissues become involved.
• Treatment options are extensive and are approached in stepwise fashion.
• Advise patients to wear loose, light clothing; avoid manipulation of lesions or trauma to the area (e.g., with loofah sponges); keep the area dry; and use gentle, nonirritating cleansers.
• Stage I disease: T opical therapy with clindamycin 1 % twice a day (bid) with or without intralesional corticosteroids may be a useful initial approach to stage I (mild) disease. After this, 7 to 10 days of doxycycline, minocycline, clindamycin, or amoxicillin clavulanate are sometimes recommended.
• Stage II disease: Oral tetracyclines (tetracycline, doxycycline, or minocycline) for several weeks are often used for 8 to 12 weeks or until lesions resolve. If disease persists, clindamycin (300 mg PO bid) with rifampin (600 mg PO daily) has shown promising results. For its antiandrogenic properties, some suggest that an oral contraceptive containing drospirenone or norgestimate with spironolactone may be helpful. Surgery is reserved for cases resistant to medical management.
• Stage III or refractory disease of any stage sometimes requires surgical debridement. This must be extensive; simple incision and drainage is not adequate. Postoperative recurrences at previously affected and new sites can occur and close surveillance is indicated. Medical therapies that are potentially helpful in severe or refractory disease include tumor necrosis factor-α inhibitors, interleukin-12/23 inhibitors, oral retinoid, or systemic immunosuppressants or glucocorticoids.
Fox-Fordyce Disease
• Fox-Fordyce disease is a rare disease characterized by papular eruption caused by the occlusion of apocrine sweat glands in the axilla and anogenital region. Patients present with flesh-colored or dark domeshaped papules in clusters that are intensely pruritic, often leading to lichenification. It predominantly affects African Americans. Exacerbations tend to occur before and during menses. Symptoms regress during pregnancy.
• Treatment is with oral contraceptives (high estrogen content), topical estrogen ointment (1 mg estrone in peanut oil [Theelin] per ounce of petrolatum), or antiacne topical agents.
Atrophic Vulvovaginitis
• The hypoestrogenic state of menopause produces atrophy of the vulvar and vaginal epithelium leading to dryness, pain, burning, pruritus, dyspareunia, and dysuria.
The mucosa becomes friable and easily irritated and is more prone to infection. The diagnosis is clinical.• On physical examination, the labia majora appear lax, whereas the labia minora are significantly atrophied. The mucosa is thin, pale, and smooth with loss of the normal rugae of the vagina. Fissures may be present.
• Avoid use of harsh soaps and hygiene products. T reatment with estrogen replacement therapy, either topical or oral, helps relieve symptoms.
P.572
Contact Dermatitis
• Soaps, detergents, hygiene products, vaginal creams, and clothing can all produce a local reaction on the vulva, which may last days to weeks.
• On physical examination, symmetric eczematous lesions are seen at the area of contact.
• Identify and remove the offending agent. Oatmeal soaks and sitz baths can be used to help control symptoms, and for severe reactions, a mild steroid ointment may be used sparingly.
Psoriasis
• Psoriasis typically appears as erythematous plaques with silvery, thick scales. However, the scales are often more difficult to identify on the vulva.
Lichen Simplex Chronicus
• Lichen Simplex Chronicus is characterized by intense and persistent pruritus. The rash often involves the perineum.
• Continual scratching of the vulva leads to lichenification, producing a thickened, leathery appearance with prominent skin markings and scaling (hyperkeratosis).
• Foci of atypical hyperplasia or cancer can develop, with a 3% chance of developing invasive squamous cell carcinoma.
• Evaluation should include colposcopy and full-thickness biopsy.
• Initial treatment with topical tricyclic/antipruritic ointments (doxepin 5% ointment), antihistamines (hydroxyzine
25 to 50 mg nightly), or an anxiolytic/sedative may relieve pruritus. For more difficult cases, topical corticosteroid preparations covered by continuous dry occlusive gauze dressings (betamethasone valerate ointment 0.1%) or intralesional corticosteroids (triamcinolone 3 mg/mL) are effective.
Lichen Planus
• Lichen planus is an uncommon, papulosquamous eruption that can affect the genitalia and oral mucosa. The pathophysiology is thought to involve T-cell autoimmunity to basal keratinocytes.
• Patients present with complaints of itching, pain, and burning of the vulva.
• White papules in a linear or reticular pattern are often seen on the vulva (Wickham striae).
• A wide range of morphologies are seen, the most common and most difficult to treat is the erosive form. When the erosive disease progresses, the vulva and vagina become denuded and scarred with loss of the clitoris and labia minora. Introital stenosis is present in severe disease.
• Lichen planus is a chronic recurrent disease; hence, complete control is not typical and spontaneous remission is unlikely. The use of ultrapotent topical steroids is first-line treatment. Surgery is not curative and is reserved for treatment of postinflammatory sequelae, such as labial adhesions and introital stenosis.
Lichen Sclerosus
• Lichen sclerosus is of unknown etiology and is characterized by white, wrinkled, atrophic lesions associated with severe vulvar pruritus, atrophy, and scarring, with gradual loss of the labia minora and prepuce of the clitoris. The perirectal area is often involved.
• This chronic disease occurs at any age but most commonly affects postmenopausal white women.
• Women with lichen sclerosus have a 20% risk of having other autoimmune disease, most frequently alopecia areata, vitiligo, or thyroid disease.
P.573
Patients have a 5% chance of developing vulvar squamous cell carcinoma, although lichen sclerosus is
usually not considered a premalignant lesion.
• Vulvar punch biopsies should be performed to confirm the diagnosis.
• Treatment includes chronic use of ultrapotent topical corticosteroid (0.05% clobetasol propionate ointment). Topical estrogen (0.01% estradiol cream) is indicated for atrophic symptoms. Periodic clinical examinations should be performed and patients should return for biopsy if ulcerations persist or new lesions appear. Surgery is reserved for management of malignancy and postinflammatory sequelae, such as labial adhesions and introital stenosis.
VULVAR PAIN SYNDROMES
• See also Chapters 30 and 42.
Vulvodynia
• Vulvodynia is defined as chronic vulvar discomfort, occurring in the absence of relevant visible findings or a specific identifiable neurologic disorder. The pain is often described as burning, stinging, or throbbing. These symptoms interfere with the ability of women to have vaginal intercourse, wear tight clothing, exercise, or even sit down. Vulvodynia affects roughly 15% of the female population.
• Symptoms may be generalized, localized, provoked, unprovoked, or mixed.
• The cotton swab test has been described to systematically map affected areas of the vestibule, perineum, and inner thigh for initial evaluation, to differentiate localized from generalized vulvodynia, and to gauge treatment success.
• Vulvodynia is a diagnosis of exclusion and thorough evaluation is needed to rule out other pathologies.
• Often, a combination of multiple treatments may be required to improve symptoms of vulvodynia.
• These include general vulvar care, topical local anesthetics and estrogen creams, oral medications (e.g., tricyclic antidepressants, gabapentin, carbamazepine), trigger point injections with combined steroids and local anesthetics, dietary changes, cognitive behavioral therapy, biofeedback and physical therapy, and surgery for resistant localized pain.
Vulvar Vestibulitis Syndrome
• Vulvar vestibulitis syndrome (VVS) is chronic inflammation of the vestibular glands and is characterized by erythema and severe pain elicited by touch only. The main presenting symptoms are dyspareunia and terminal dysuria.
• Patients with VVS usually benefit from pelvic rest, anti-inflammatory/antiallergenic therapy (e.g., Burow soak baths/sitz baths, antihistamine therapy, stearin-lanolin cream application), and pelvic relaxation exercises. Infectious etiologies, if present, should be treated. Medical therapies as described earlier for vulvodynia may be appropriate.
• Surgical repair of the vulva and perineum is usually performed for patients who fail to respond to conservative therapy or those who suffer from scars or recurrent perineal tears.
Levator Ani Myalgia
• Pelvic floor myalgia is often the result of trauma or inflammation of the perineal branch of the pudendal nerve causing painful spasms of the affected muscles and fascia.
• Treatment of pelvic muscle myalgia may require pudendal block (triamcinolone + local anesthetic) and pelvic physiotherapy/biofeedback.
Vulvar Neuropathy
• The pudendal, genitofemoral, and ilioinguinal nerves are the main nerves serving the vulvovaginal area. Trauma to these nerves may result in continuous dull, aching, or burning neuropathic pain.
• Gabapentin 300 to 1,200 mg PO tid or amitriptyline 0.5 to 2 mg/kg PO every night at bedtime have been shown to be effective treatments.
BENIGN VULVAR LESIONS
Urethral Caruncle
• Urethral caruncle is a benign, generally asymptomatic exophytic papule at the urethral meatus that may cause bleeding. It must be differentiated from malignancy. No treatment is required unless symptomatic, in which case topical estrogen therapy (0.01 % Estrace cream, 2 to 4 g daily for 1 to 2 weeks), cryosurgery, or laser vaporization will control bleeding.
Acrochordon
• Acrochordons (i.e., skin tags) are common, frequently pedunculated fibroepithelial polyps that have a rubbery consistency. They often arise in areas of chronic irritation. Acrochordons do not need to be removed unless they are symptomatic.
Seborrheic Keratoses
• Seborrheic keratoses are flat to slightly raised pigmented lesions that have a characteristic waxy, “stuck-on” appearance. Although benign, providers should have a low threshold to perform excisional biopsy to rule out carcinoma.
Lipoma
• Lipomas are benign tumors composed of adipose tissue. They are soft and sometimes pedunculated. They commonly appear on the mons pubis and labia majora. No treatment is necessary unless the lipoma is bothersome, in which case it can be excised.
Ectopic (Extramammary) Breast
• Supernumerary ectopic breast tissue may be found anywhere along the milk line, which extends from the groin to the axillae. The tissue may undergo cyclical changes with the menstrual cycle like normal breast tissue and is subject to similar pathologies. Evaluation for associated renal system anomalies should be considered.
BENIGN VULVAR CYSTS
Bartholin Cyst
• Bartholin glands (greater vestibular glands) produce a clear, mucoid secretion that provides continuous lubrication for the vestibular surface. They are lined by transitional epithelium and are prone to obstruction, which results in Bartholin cyst formation. Superinfection results in an abscess. Usually polymicrobial, approximately 10% of Bartholin abscesses may be caused by Neisseria gonorrhoeae.
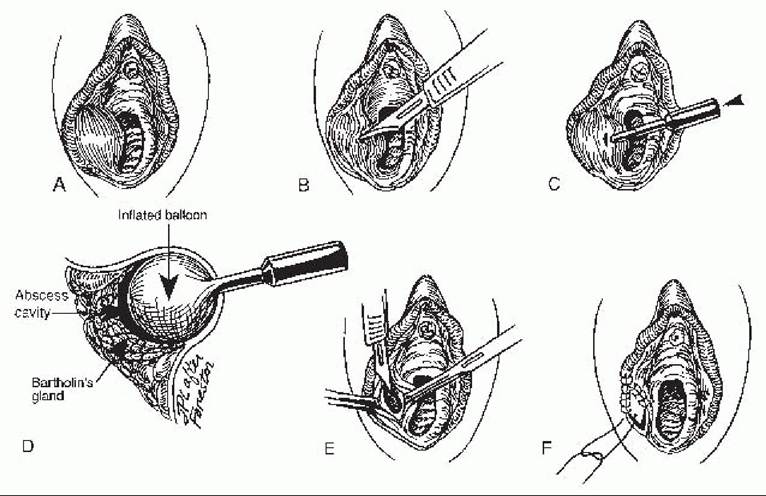
Figure 44-3. Surgical management of Bartholin abscess. (A) Typical presentation of a Bartholin cyst or abscess; (B) small stab incision of the cyst near the hymenal ring; (C) insertion of a Word catheter which is inflated in (D) to allow fistula drainage tract formation; (E) opening of the cyst wall for marsupialization seen in (F). (From Beckmann CR, Ling F, Barzansky BM, et al. Obstetrics and Gynecology, 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002:372.)
• Treatment of Bartholin gland abscesses may include incision and drainage, marsupialization, or in case of recurrence, resection of the gland (Fig. 44-3). Attempts at incision and drainage are therapeutic only when the lesion becomes fluctuant. The incision is made near the hymenal ring (i.e., at the vaginal introitus near the duct orifice), and a Word catheter is inserted.
• In women aged 40 years or older, biopsy is recommended because of the risk of Bartholin adenocarcinoma.
• Antibiotic therapy, even after incision and drainage, is not usually necessary unless cellulitis is also present. Simple Bartholin cysts that are not infected and not causing symptoms may not need treatment.
Epidermal Cysts
• Epidermal inclusion cysts are seen frequently on the labia majora, containing a white or yellow material made up of keratin and lipid-rich debris. They arise from blockage of pilosebaceous ducts. If traumatized, they can become erythematous and tender. If symptomatic, cysts can be surgically excised.
Mucus Cysts
• Mucus cysts are found within the vestibule and develop from vestigial embryonic structures or from obstruction of the minor vestibular glands. They are lined by mucus-secreting simple columnar epithelium without myoepithelial cells.
Gartner Cysts
• Gartner duct cysts arise from remnants of the mesonephric ducts. They most often appear as multiple small cysts along the lateral vagina and hymenal ring. These cysts
P.576 are usually asymptomatic and are discovered incidentally. Treatment is not necessary unless cysts are very
large, in which case they can be excised.
Cysts of the Canal of Nuck (Processus Vaginalis Peritonei)
• These peritoneal-lined cysts are found in the superior aspect of the labia majora. They arise from inclusions of the peritoneum at the insertion of the round ligament to the labia majora. These cysts must be distinguished from an inguinal hernia.
Premalignant neoplastic diseases of the vulva and vagina
Vulvar Intraepithelial Neoplasia
• Histologic criteria for vulvar intraepithelial neoplasia (VIN) include disordered maturation and nuclear abnormalities, loss of polarity, pleomorphism, mitotic figures, and coarsened nuclear chromatin. Cytologic atypia is present throughout the epithelium. Historically, the degree of maturation present in the surface epithelium defined the grade of dysplasia.
• VIN 1 (mild dysplasia) demonstrates loss of squamous maturation in the lower one third of the epithelium. This usually reflects self-limited disease.
• VIN 2 (moderate dysplasia) shows loss of maturation in the lower two thirds of the epithelium. Surface maturation is present.
• VIN 3 (severe dysplasia, carcinoma in situ) presents with full-thickness loss of squamous maturation. Stromal invasion does not occur. Cytologic atypia may be severe.
• In a newer system of classification, VIN 1 is eliminated and only high-grade disease (VIN 2 or 3) is categorized. There are three subcategories that reflect the malignant potential of the lesion:
• VIN usual type (basaloid, warty, or mixed variants): associated with human papillomavirus (HPV) infection (especially 16 and 18), seen in younger women, tends to be multifocal lesions, 5% to 6% progress to invasive cancer
• VIN differentiated: not associated with HPV and generally seen in older women, associated with atrophy and dermatoses (lichen sclerosus, lichen simplex chronicus, etc.), often unifocal, aggressive with one third progressing to invasive cancer
• VIN unclassified: rare cases that cannot be classified as discussed earlier
• One third of VIN cases will recur, regardless of how they are treated.
Vaginal Intraepithelial Neoplasia
• This rare condition affects 0.2 to 2 per 100,000 women.
• Vaginal intraepithelial neoplasia (VaIN) is usually asymptomatic, although patients can present with postcoital spotting or vaginal discharge. It is diagnosed by persistently abnormal Pap smears with no evidence of cervical neoplasia. After VaIN is diagnosed, invasive disease must be excluded by colposcopy and biopsy, especially before undertaking nonexcisional therapy. VaIN progresses to invasive cancer in 3% to 7% of patients.
• Risk factors include HPV infection, current or prior lower genital preinvasive or invasive lesions, immunosuppression, history of radiation exposure, pessary use, and prolapse.
• VaIN is a preinvasive lesion defined by the presence of squamous cell atypia without invasion. Lesions are classified according to the depth of epithelial involvement.
P.577
• VaIN 1: Cytologic atypia is present throughout the lower one third of the epithelium.
• VaIN 2: Cytologic atypia is present throughout the lower two thirds of epithelium.
• VaIN 3: Cytologic atypia involves more than two thirds of the epithelium.
Treatment of Vulvar Intraepithelial Neoplasia and Vaginal Intraepithelial Neoplasia
• Surgical resection is the mainstay of treatment and should be performed if invasion cannot be excluded.
• Wide local incision: 5-mm margin, ideal for localized lesions
• Skinning vulvectomy: large, extensive, or multifocal lesions
• T otal vulvectomy or vaginectomy
• Topical agents (5% imiquimod and 5-fluorouracil cream): useful for persistent low-grade, multifocal lesions or women who are poor surgical candidates
• Intracavitary radiation therapy: effective for VAIN; associated with morbidity; and should be reserved for women who are poor surgical candidates, have multifocal disease, and/or have failed other treatments
• CO2 laser ablation: Must rule out invasion with pretreatment biopsies; useful with multifocal disease, minimal scarring, and sexual dysfunction. VIN lesions should be ablated to 3 mm in hair-bearing areas and 1 mm on nonhairy surfaces.
MALIGNANT NEOPLASTIC DISEASES OF THE VULVA
Vulvar neoplasms are relatively rare and represent 3% to 5% of all primary malignancies of the female genital tract. The American Cancer Society estimates that 4,850 women will be diagnosed with and 1,030 women will die from cancer of the vulva in 2014. Squamous cell carcinoma is the most common histopathology found in vulvar cancer, followed by melanoma, basal cell carcinoma, and sarcoma. These lesions most commonly present as pruritus and are often misdiagnosed by health care providers.
Squamous Cell Vulvar Neoplasia
• Squamous cell lesions account for 85% to 90% of vulvar malignancies.
• As with VIN, two subtypes of invasive squamous cell carcinomas exist.
• The classic, warty, or Bowenoid type is identified in younger patients and is related to HPV. These lesions may be multifocal.
• The keratinizing, differentiated, or simplex types occur in older women and is not associated with HPV. These lesions tend to be unifocal, and a significant number are associated with atrophic lesions, such as lichen sclerosus.
• Accurate surgical staging predicts prognosis, as nodal status has the most prognostic significance, and directs treatment for squamous cell carcinoma of the vulva. The International Federation of Gynecology and Obstetrics (FIGO) staging system was recently revised to reflect the risk of nodal metastases on survival (Table 44-1).
• Treatment. Vulvar carcinomas, especially early-stage lesions, are treated surgically. Good margins and reliable assessment of lymph nodes are essential, as recurrences are often fatal.
• Stage IA (microinvasive) vulvar cancer: Radical local excision with a 1-cm margin at the time of resection.
Inguinofemoral Iymphadenectomy is not recommended because the risk of metastasis to the lymph nodes is extremely low.
TABLE 44-1 International Federation of Gynecology and Obstetrics Staging for Carcinoma of the Vulva (2009) and 5-Year Survival
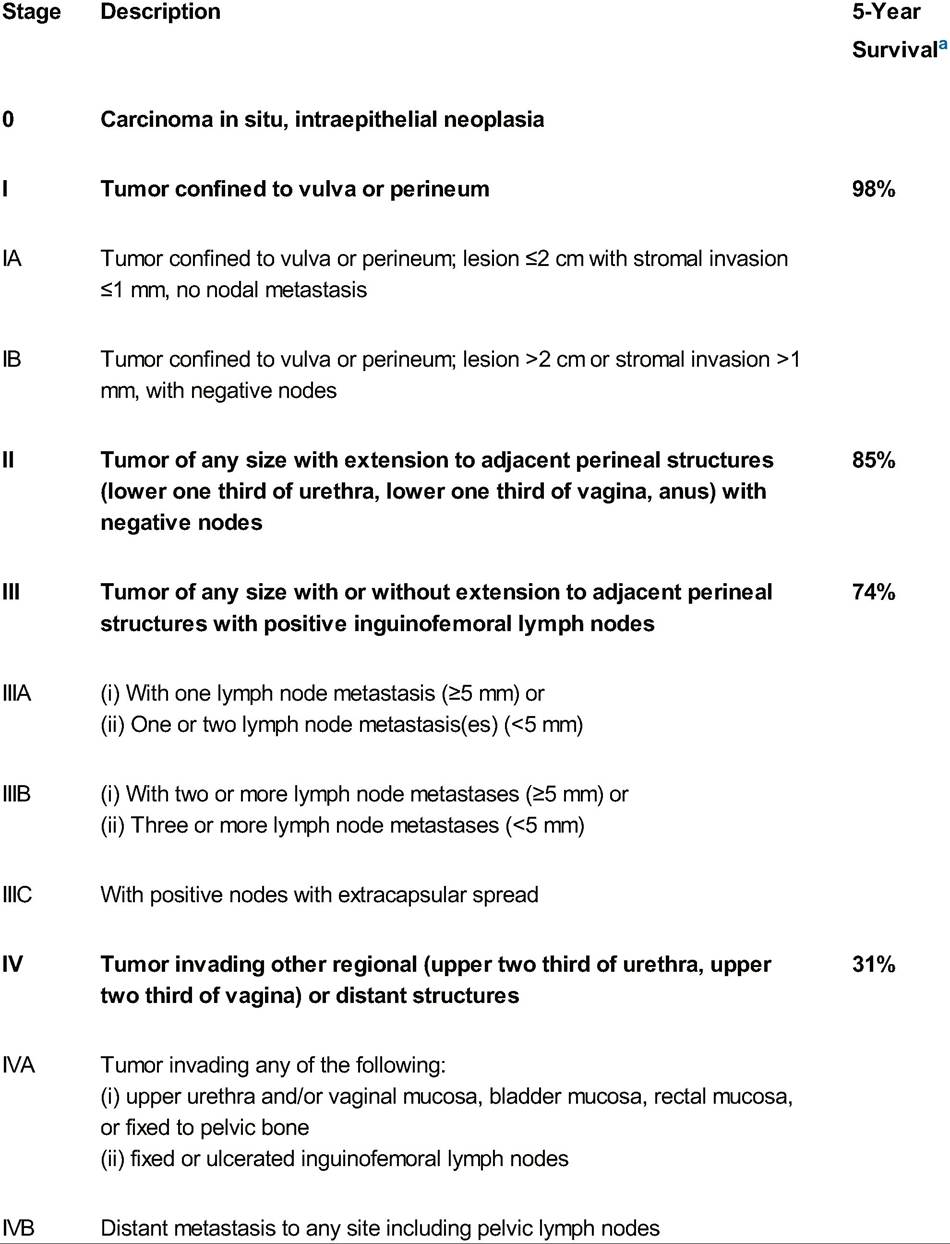
aFive-year survival data according to previous FIGO staging system.
Adapted from Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynecol Obstet 2009;105:103-104.
• Early-stage disease: Treat surgically with a radical procedure and lymph node assessment. More aggressive traditional surgeries are making way for less invasive approaches.
î Historically, this was accomplished with a butterfly-shaped en block excision of the vulva, inguinal and femoral lymph nodes, and the skin and lymphatics in between. A modified three-incision technique has fewer complications and similar survival.
P.579 î A radical excisional procedure (total radical vulvectomy, partial radical vulvectomy, radical local excision) obtains 1- to 2-cm clinical margins and dissects down to the perineal membrane.
• Inguinofemoral lymphadenectomy: removal of nodal tissue from the lateral border of the adductor longus to medial border of the sartorius muscle, the mons pubis and pubic tubercle medially and cephalad, and the external oblique laterally.
î This inguinofemoral lymphadenectomy may be ipsilateral only if the tumor is >2 cm lateral to the midline and vaginal cancer is very rare, accounting for of visually abnormal cervical epithelial cells. Both techniques are equally sensitive and specific. Oncogenic HPV infection can be detected with the Digene hybrid capture test, which can be performed either on cytology specimens or using the Digene sampling brush.
• Annually, 4.8 million women have an abnormal Pap smear in the United States. Cytologic abnormalities are categorized using the Bethesda system (see the following text).
• Histologic abnormalities are classified in a two-tiered system of low-grade and high-grade squamous intraepithelial lesions. Low-grade squamous intraepithelial lesions (LSILs) include mild dysplasia and cervical intraepithelial neoplasia (CIN 1). High-grade squamous intraepithelial lesions (HSILs) include moderate and severe dysplasia, carcinoma in situ, and CIN 2/3.
• CIN 1 is associated with a high rate of spontaneous regression, whereas untreated CIN 3 has a reported cumulative incidence of invasive cancer of 30.1% at 30 years.
PRIMARY PREVENTION
• Smoking cessation: Women who smoke have an increased risk of developing cervical cancer compared to nonsmokers. This is thought to be related to the fact that smoking triples the likelihood of persistent HPV infection and doubles the risk of progression to CIN 3.
• All women with abnormal Pap smears should be offered testing for HIV and other sexually transmitted infections.
• A quadrivalent HPV vaccine directed against HPV types 6, 11, 16, and 18 (Gardasil, Merck, Whitehouse Station, NJ) was approved for use in 9- to 26-year-old females by the U.S. Food and Drug Administration (FDA) in 2006. The vaccine is very effective in HPV 16/18 naive women, preventing essentially 100% of HSILs. However, the preventive vaccine does not have therapeutic effect against existing infection. Both the Advisory Committee on Immunization Practices (ACIP) and American College of Obstetricians and Gynecologists (ACOG) recommend administration of the vaccine to females aged 9 to 26 years.
• The vaccine is administered in three doses at 0, 2, and 6 months. See Chapter 1. Currently, HPV vaccination does not change screening recommendations. However, looking forward, HPV vaccination is likely to influence positive and negative predictive values of the Pap smear by decreasing cervical abnormalities in the population.
SCREENING
• Cytologic changes associated with HPV infection and neoplasia can be identified using Pap smears, which are the basis of cervical cancer screening programs. Abnormal Pap smears are followed by colposcopic evaluation of the cervix, as indicated in the flow diagrams later.
• Screening guidelines are formulated by the American Society for Colposcopy and Cervical Pathology (ASCCP) and used in the 2013 ACOG practice bulletin. The guidelines were issued in 2001,2006, and 2012, adapting new scientific insights and epidemiologic changes.
P.585
• HPV vaccination may change the HPV genotype distribution as well as the positive and negative predictive value of Pap smears. Furthermore, vaccination may influence adherence to screening. Therefore, new guidelines will be needed to accommodate to those changes.
• Based on the ASCCP guidelines from 2012:
• Regular screening should begin at 21 years of age, regardless of the age of first sexual intercourse. Women aged 21 to 29 years should be screened every 3 years with cytology only. In this age cohort, HPV infections are likely to be transient.
• In women aged 30 to 65 years, screening can be performed every 3 years with cytology alone. However, preferably, screening can be performed every 5 years with HPV cotesting (cytology and high-risk HPV testing).
• Screening can be stopped at age 65 years if a woman does not have risk factors and has 10 years of negative screening that includes at least three negative test results. Screening should not be reinstituted, even in the case of a new sexual partner after the age of 65 years. Annual well-woman exams are still recommended for all adult women.
• Women who have had a total hysterectomy for benign indications and who do not have a history of highgrade lesion do not require further screening.
• Women with a history of CIN 2/3 should undergo screening every 3 years for at least 20 years after an initial adequate posttreatment surveillance period, regardless of their age. The same period of vaginal screening is advised for those who underwent a hysterectomy as part of treatment for recurrent CIN 2/3.
• HIV-positive women should be screened at 6-month intervals for 1 year after the diagnosis of HIV and then may resume an annual screening schedule. Immunocompromised and women who were exposed to diethylstilbestrol (DES) in utero should also be screened annually.
• Visual inspection with acetic acid and direct treatment with cryotherapy is currently the most effective cervical cancer prevention in low-resource settings where pathology laboratories and personnel are scarce and monetary and/or logistical constraints prohibit follow-up.
PAP SMEAR
• Pap smear reports include specimen type, specimen adequacy, results, and any ancillary testing performed (i.e., high-risk HPV probe).
• Specimen type indicates whether the test is a vaginal or cervical sample.
• Adequacy is reported as satisfactory, unsatisfactory, or endocervical cells not present/lack of transformation zone.
• Unsatisfactory Pap smears should be repeated in 2 to 4 months.
• Pap smears that lack an endocervical component can be repeated in 1 year or postpartum unless any of the following risk factors are present, all of which necessitate repeat screening in 6 months:
î History of atypical squamous cells of undetermined significance or greater abnormalities in the past, without three-interval normal Pap smears
î High-risk HPV positivity in the previous 12 months
î Previous glandular abnormality
î Immunosuppression
î Inability to visualize the endocervical canal
• Patient noncompliance
• The results section relays any cytologic abnormality.
P.586
DIAGNOSTIC CATEGORIES: CYTOLOGY
The 2001 revision of the Bethesda system is used to describe abnormal cervical cytology employing the following categories:
• Atypical squamous cells (ASC)
• Of undetermined significance (ASC-US)
• Cannot exclude high grade (ASC-H)
• Low-grade squamous intraepithelial lesion
• High-grade squamous intraepithelial lesion
• Atypical glandular cells (AGC) (endocervical or endometrial)
• Not otherwise specified (AGC-NOS)
• Favor neoplasia (AGC-favor neoplasia)
• Adenocarcinoma in situ (AIS)
Atypical Squamous Cells
• Approximately 2 million ASC Pap smears a year are recorded in the United States.
• ASC-US is present in 4.7% of samples and is associated with a 7% to 12% prevalence of CIN 2/3.
• ASC-H is present in 0.4% of samples and CIN 2/3 is present in 26% to 68% of women with this result.
• The risk of invasive cancer associated with an ASC Pap is 0.1% to 0.2%.
Atypical Glandular Cells
• AGC are found in 0.4% of Pap smears.
• AGC are associated with significant neoplasia in 9% to 38% (CIN 2/3, AIS) and in 3% to 17% associated with cancer.
• One study found that the malignancies of the women with AGC were found in women older than 35 years, are mainly of endometrial origin, and therefore suggested endometrial biopsy for every woman with AGC after the age of 35 years.
• AGC-favor neoplasia has a higher risk of neoplasia (27% to 96%) than AGC-NOS (9% to 41 %).
Low-Grade Squamous Intraepithelial Lesions
• LSIL is reported in 2.1% of Pap smears and is strongly correlated with HPV infection.
• High-grade dysplasia or neoplasia is found in 12% to 17% of women who undergo colposcopy for LSIL.
High-Grade Squamous Intraepithelial Lesions
• HSIL is reported in 0.7% of Pap smears.
• CIN 2/3 is found in 53% to 97% of women with HSIL cytology. Invasive cancer is identified in 2.0% of women with HSIL cytology.
TREATMENT OPTIONS
• T reatment options can be classified as ablative or excisional.
• Ablative procedures do not obtain a sample for pathologic examination.
• Excisional procedures should be performed when invasive cancer cannot be ruled out, microinvasive cancer is suspected on a biopsy, a two-level discrepancy between cytology and histology exists, and whenever concern is raised for endocervical disease.
P.587
Ablative Methods
• Cryotherapy is performed with a supercooled probe applied directly to the lesion. Not appropriate for endocervical disease.
• Carbon dioxide laser is used to vaporize the tissue to 7-mm depth. Special equipment is necessary, but more irregular areas can be treated.
• Ablative methods are not acceptable for AIS or for unsatisfactory colposcopy.
Excisional Methods
• Excisional procedures may increase a woman's risk of future preterm delivery or premature rupture of the membranes.
• Loop electrosurgical excision procedure (LEEP) is an excisional procedure employing a wire with an electrical current. The shape and size of the loop can be altered, and a second “hat” can be done to obtain further endocervical tissue.
• Cautery artifact can make interpretation of margins difficult.
• Cold knife cone (CKC) employs a scalpel to excise a cone-shaped wedge of the cervix. The size and shape of the cone can be tailored to the lesion, and this method allows for pathologic determination of margin status.
• CKC should be considered over LEEP for cases with AIS, suspected microinvasion, unsatisfactory colposcopy, or a lesion extending into the endocervical canal.
MANAGEMENT STRATEGIES: CYTOLOGIC ABNORMALITIES
Atypical Squamous Cells of Undetermined Significance
• Reflex testing for high-risk HPV: A positive result should be followed by colposcopy. A negative result allows for resumption of standard screening. With this strategy, the sensitivity for detection of CIN 2/3 is 92% (Fig. 45-1).
Special Populations
• Adolescents (between 13 and 20 years old) have a higher prevalence of HPV but are likely to clear the infection. Therefore, they should not be tested for HPV.
• Delaying first testing until age 21 years is designed to reduce unnecessary diagnostic procedures or interventions and potential iatrogenic morbidity in young women.
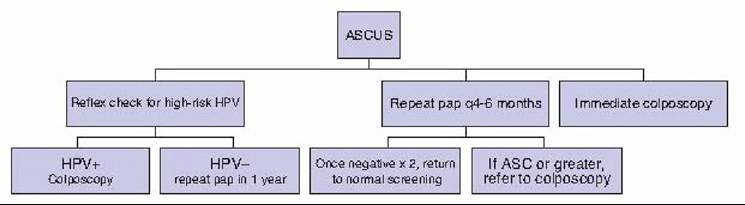
Figure 45-1. Triage strategy for ASC-US. ASC-US, atypical squamous cell of undetermined significance; HPV, human papillomavirus; ASC, atypical squamous cell. (Adapted from Massad LS, Einstein MH, Huh WK, et al. 2012 consensus guidelines for the management of women with abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis 2013; 17:S1-S27.)
P.588
• Pregnant women are tested according to their age group, with the exception that colposcopy can be deferred to 6 weeks postpartum. Endocervical curettage is never acceptable in pregnancy.
• Immunosuppressed and postmenopausal women are managed in a manner identical to the general population.
Atypical Squamous Cells, Cannot Exclude High Grade
• These patients require colposcopic examination. Negative colposcopy should be followed by cytology in 6 and 12 months or cotesting at 12 months.
Atypical Glandular Cells
• All women with AGC should undergo colposcopy with endocervical biopsy; HPV DNA testing is preferred.
• Endometrial sampling should be performed routinely for the finding of atypical endometrial cells.
• Endometrial sampling should be performed in women aged 35 years and older and in those with risk factors
for endometrial cancer.
• Follow-up for AGC-NOS after negative findings is repeat cytology/HPV DNA testing at 6 months if they are initially HPV DNA positive and 12 months if negative.
• Follow-up for AGC-favor neoplasia after a negative evaluation is a diagnostic excisional procedure, preferably CKC.
• AIS is managed by a diagnostic excisional procedure, preferably CKC.
Special Populations
• Pregnant women should be managed in an identical fashion to the general population with the exception that endometrial and endocervical biopsies are unacceptable.
• Benign-appearing endometrial cells on a Pap smear in postmenopausal women should be evaluated with endometrial biopsy.
Low-Grade Squamous Intraepithelial Lesion
• LSIL carries the same risk of high-grade dysplasia as ASC-US + HPV and is therefore managed identically (colposcopy).
• Endocervical curettage is preferred in those with an unsatisfactory or negative colposcopic examination.
• A finding of less than CIN 2/3 can be followed by cytology at 6 and 12 months or HPV DNA testing at 12 months.
Special Populations
• Adolescents with LSIL should be followed by repeat cytology at 12 months and 24 months. A finding of HSIL or greater at 12 months or ASC-US or greater at 24 months merits colposcopy. Only immunosuppressed adolescents are now screened.
• Postmenopausal women can be managed by reflex HPV DNA testing, colposcopy, or repeat cytology at 6 and 12 months.
• Pregnant women with LSIL should have a colposcopic examination. Postpartum follow-up is also acceptable.
High-Grade Squamous Intraepithelial Lesion
• Due to the high risk of significant cervical disease, one approach is to “see and treat” with immediate LEEP.
P.589
• Colposcopy with endocervical curettage is also acceptable. An unsatisfactory colposcopy should be managed by a diagnostic excisional procedure.
• A satisfactory colposcopy that results in a diagnosis of less than CIN 2/3 can be followed by colposcopy/cytology at 6 and 12 months, excisional diagnostic procedure, or review of the original pathologic material to verify the diagnosis.
Special Populations
• A satisfactory colposcopy detecting less than CIN 2/3 should be followed by colposcopy/cytology every 6 months for up to 2 years.
• Persistent HSIL for 24 months should be evaluated with an excisional diagnostic procedure.
• Two consecutive negative Pap smears and no high-grade lesions on colposcopy allow for resumption of a normal screening schedule.
• Pregnant women with HSIL should be evaluated by colposcopy. Lesions suspicious for CIN 2/3 or cancer should be biopsied; it is unacceptable to biopsy other lesions.
• Evaluation no sooner than 6 weeks postpartum should be performed for women with a diagnosis of less than CIN 2/3.
DIAGNOSTIC CATEGORIES VIA COLPOSCOPY: HISTOLOGY
• Colposcopy is used for the evaluation of abnormal cervical cytology. The average sensitivity of cytology is only 48%. Therefore, colposcopic examination should include a biopsy of a visible lesion, with the exception of pregnant women, or those who will undergo a diagnostic excision.
• A colposcope is used to examine the cervix after the application of a dilute, 3% acetic acid wash. The dilute acid dehydrates epithelial cells with a high nuclear-tocytoplasmic ratio, resulting in acetowhite changes.
• Colposcopy is considered satisfactory if the entire squamocolumnar junction is visualized circumferentially and if all lesions are completely visualized.
Cervical Intraepithelial Neoplasia 1
• CIN 1 is the histologic diagnosis applied to low-grade lesions. However, it is not equivalent to LSIL.
• An estimated 1 million women are diagnosed with CIN 1 annually in the United States, and the annual incidence of CIN 1 is estimated to be 1.2 per 1,000 women.
• CIN 1 progresses in approximately 11% to CIN 2/3 (Table 45-1).
Cervical Intraepithelial Neoplasia 2/3
• CIN 2/3 is the histologic diagnosis applied to high-grade lesions; it is not equivalent to HSIL.
• An estimated 500,000 women are diagnosed with CIN 2/3 annually in the United States, and the annual incidence of CIN 2/3 is estimated to be 1.5 per 1,000 women.
Adenocarcinoma In Situ
• Unlike squamous lesions, AIS lesions are often multifocal. Therefore, negative margins do not reliably predict excision of all disease.
P.590
TABLE 45-1 Natural History of Untreated Cervical Intraepithelial Neoplasia
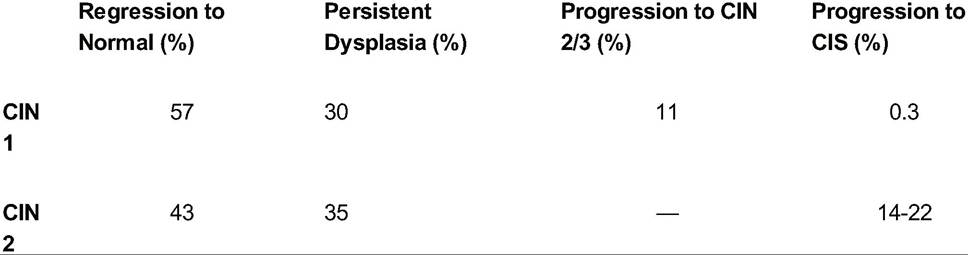

CIN, cervical intraepithelial neoplasia; CIS, carcinoma in situ.
Adapted from Mitchell MF, Tortolero-Luna G, Wright T, et al. Cervical human papillomavirus infection and intraepithelial neoplasia: a review. J Natl Cancer Inst Monogr 1996;(21):17-25.
MANAGEMENT STRATEGIES: HISTOLOGIC ABNORMALITIES
Cervical Intraepithelial Neoplasia 1
• The management of CIN 1 depends on the cytology, as the risk of an occult highgrade lesion is greater when the referral cytology is HSIL or AGC (Fig. 45-2).
• CIN 1 preceded by ASC-US, ASC-H, or LSIL
• Follow-up with repeat cytology at 6 and 12 months or HPV DNA testing at 12 months. A positive HPV DNA or cytology equal to or greater than ASC-US necessitates repeat colposcopy.
• Two negative Pap smears or a single negative HPV DNA allows for resumption of standard screening.
• Persistent (>2 years) CIN 1 can be followed as mentioned earlier or treated. Ablative and excisional procedures are acceptable given a satisfactory colposcopy. Ablation is unacceptable after unsatisfactory colposcopy.
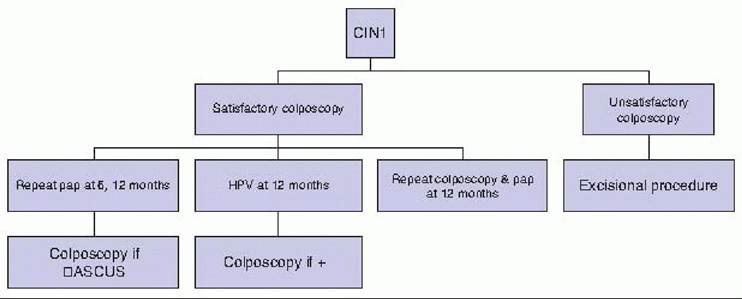
Figure 45-2. Triage strategy for CIN 1. CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; ASC-US, atypical squamous cell of undetermined significance. (Adapted from Massad LS, Einstein MH, Huh WK, et al. 2012 consensus guidelines for the management of women with abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis 2013;17:S1-S27.)
P.591
• CIN 1 preceded by HSIL or AGC-NOS
• Diagnostic excisional procedure or colposcopy/cytology at 6-month intervals is acceptable. Endocervical curettage should be performed if colposcopy is selected.
• Unsatisfactory colposcopy or persistence of HSIL or AGC-NOS cytology requires a diagnostic excisional procedure.
Negative cytology/colposcopy for 1 year allows for resumption of routine screening.
Special Populations
• Adolescents with CIN 1 should be followed with yearly cytology. HSIL or greater at 1 year should be evaluated with colposcopy, as should ASC-US or greater after 24 months.
• Pregnant women with CIN 1 should be followed without treatment.
Cervical Intraepithelial Neoplasia 2 and 3
• CIN 2/3 requires excision or ablation after a satisfactory colposcopy.
• Recurrent CIN 2/3 should be excised. Ablation is unacceptable for CIN 2/3 and an unsatisfactory colposcopy.
• Hysterectomy is not an acceptable management for CIN 2/3.
• After treatment, CIN 2/3 can be followed by HPV DNA testing at 6 to 12 months, cytology every 6 months, or cytology/colposcopy at 6-month intervals.
• Either HPV DNA positivity or ASC-US or greater on cytology require colposcopy with endocervical sampling.
• If testing is negative after posttreatment evaluation for 1 year, routine screening should be employed for at least 20 years.
• Hysterectomy is acceptable for persistent or recurrent CIN 2/3.
• Positive margins can be followed with Pap smear, colposcopy, and endocervical curettage every 4 to 6 months, or a further excisional procedure can be performed.
Special Populations
• In younger women, future fertility should be taken into account; because CIN 2/3 can regress spontaneously, colposcopy evaluation with endocervical assessment is therefore an appropriate initial evaluation.
• The main goal for pregnant women is to exclude invasive cancer. Biopsy is important if the colposcopy impression is high grade and a biopsy during pregnancy is not jeopardizing the pregnancy. Reassessment not earlier than 6 weeks postpartum is warranted for follow-up and further management.
Adenocarcinoma In Situ
• Cold knife conization is the first-line treatment for AIS.
• Diagnostic excisional procedure can be considered for women who want to maintain fertility. An endocervical curettage should be performed at the time of the resection.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 99: management of abnormal cervical cytology and histology. Obstet Gynecol 2008;112(6):1419-1444.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 140: management of abnormal cervical cancer screening test results and cervical cancer precursors. Obstet Gynecol 2013;122(6):1338-1367.
P.592
American College of Obstetricians and Gynecologists Committee on Practice Bulletins— Gynecology. ACOG practice bulletin no. 131: screening for cervical cancer. Obstet Gynecol 2012;120(5):1222-1238.
Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. Am J Clin Pathol 2012;137(4):516-542.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012;62:10-29.
World Health Organization. Cervical Cancer, Human Papillomavirus (HPV), and HPV vaccines: Key Points for Policy-Makers and Health Professionals. Geneva, Switzerland: World Health Organization, 2008.
World Health Organization. Prevention of Cervical Cancer through Screening Using VIA and Treatment with Cryotherapy. Geneva, Switzerland: World Health Organization, 2012. http:ZZapps.who.int/irisZbitstreamZ10665/75250/1Z9789241503860_eng.pdf. Accessed February 2, 2013.