43 Menopause
Chantel Washington
Howard A. Zacur
DEFINITIONS AND EPIDEMIOLOGY OF MENOPAUSE
Menopause is the permanent cessation of menses, dated by the last menstrual period followed by 12 months of amenorrhea.
• The average age of menopause is 51 years, with a normal range of 43 to 57 years.
• Can also be induced by oophorectomy or iatrogenic ablation of ovarian function.
• In 2001, the Stages of Reproductive Aging Workshop divided normal female reproductive aging into stages, with the goal of clarifying terminology relating to menopause (Fig. 43-1).
• The transition from reproductive to postreproductive life is divided into several stages, with the final menstrual period (FMP) serving as an anchor.
î Five stages (-5 to -1) precede the FMP and two stages follow (+1 and +2).
• Menopausal transition, traditionally termed perimenopause or the climacteric, is the transition period from regular menstruation until menopause.
î May last for 5 years or more, highly variable in duration
î Characterized by menstrual cycle changes that include variable cycle length, with skipped periods and increasingly longer intervals of amenorrhea
P.556
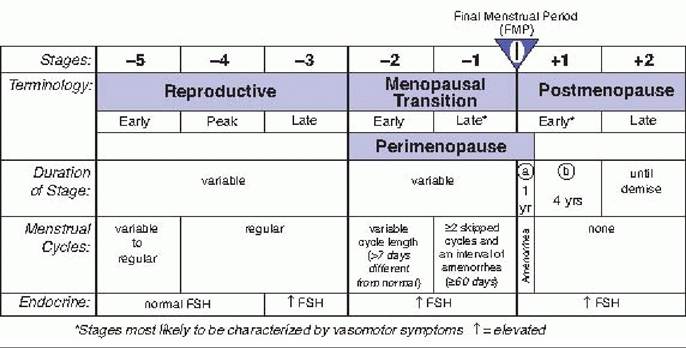
Figure 43-1. Stages/nomenclature of normal reproductive aging in women. (From Soules MR, Sherman S, Parrott E, et al. Executive summary: stages of reproductive aging workshop [STRAW]. Fertil Steril 2001;76:874, with permission.)
î Associated with the cessation of ovulation, a marked decline in estradiol production, and a modest decline in androgen production
î Early menopausal transition (-2) is depicted by variable cycle length (>7 days different from the norm) and increased follicle-stimulating hormone (FSH).
î Late menopausal transition (-1) is characterized by two skipped cycles and an interval of amenorrhea >60 days.
• Diagnosis of menopause is clinical, without reliance on hormonal measurements.
• When any doubt exists about menopause, other causes of secondary amenorrhea must be ruled out. See Chapter 39.
PHYSIOLOGY OF MENOPAUSE
• Oocytes undergo atresia throughout a woman's life, with follicular quantity and quality undergoing a critical decline approximately 20 to 25 years after menarche. This follicular decline results in loss of ovarian sensitivity to gonadotropin stimulation.
• During perimenopause, follicular dysfunction can lead to variable menstrual cycle length. The follicular phase of the cycle is usually shortened due to the decreased number of functional follicles.
• The early menopause transition is typified by increased levels of FSH leading to overall higher estrogen levels.
• As follicular depletion continues, decreased inhibin produced by follicles leads to continued increased FSH. Follicular depletion also leads to recurrent anovulation and subsequent increase in FSH and luteinizing hormone levels.
MENOPAUSAL SYMPTOMS AND TREATMENT
Vasomotor Symptoms
• Seventy-five percent of menopausal women experience vasomotor symptoms such as hot flashes and night sweats.
• Symptoms begin an average of 2 years before the FMP.
• Eighty percent of women who have hot flashes endure them for longer than 1 year and 50% for longer than 5 years.
P.557
• Pathophysiology: due to vasomotor instability thought to be secondary to dysfunction of the thermoregulatory nucleus which is responsible for maintaining body temperature within a set range known as the thermoregulatory zone
• Characterized by a sudden reddening of the skin over the head, neck, and chest, accompanied by a feeling of intense body heat, palpitations and anxiety, sleep disturbance, and irritability. Concludes with profuse perspiration.
• Risk factors: surgical menopause (up to 90% of women will have vasomotor symptoms), early menopause, low circulating levels of estradiol, smoking, and possibly low body mass index (BMI)
• Treatment: Hormone therapy (HT) is first-line treatment.
Current recommendations are that HT use should be limited to the lowest effective dose for the shortest treatment duration and that ongoing use should be reevaluated periodically.• Estrogen administration: the most effective treatment for hot flashes, given orally, transdermally, or vaginally (T able 43-1)
î Oral dosing: results in plasma level fluctuations and an estradiol to estrone ratio of modification:
• The North American Menopause Society recommends maintaining a low core body temperature by using a fan and drinking cool beverages to manage mild hot flashes.
• Relaxation techniques, such as slow breathing and yoga, can reduce the frequency of menopausal symptoms and alleviate hot flashes.
• Exercise may increase the severity of symptoms by raising core body temperature.
Urogenital Atrophy
• Pathophysiology: The vagina, urethra, and bladder trigone have high estrogen receptor concentrations. Loss of estrogen that accompanies menopause thus leads to urogenital atrophy.
• Atrophic vulva loses most of its collagen, adipose tissue, and water-retaining ability and becomes flattened and thin. Sebaceous glands remain intact, but secretions decrease, leading to vaginal dryness.
• Vaginal shortening and narrowing occur, and the vaginal walls become thin, lose elasticity, and become pale in color.
P.560
• Dyspareunia is the most common complaint related to vaginal atrophy.
• Estrogen deficiency within the urethra and bladder is associated with urethral syndrome, which is characterized by recurrent episodes of urinary frequency and urgency with dysuria.
• Treatment:
• Moisturizers and lubricants are used to relieve symptoms related to vaginal dryness and dyspareunia.
• Astroglide and K-Y jelly are used at the time of coitus to alleviate dyspareunia, whereas Replens is used on a sustained basis.
• Local estrogen therapy improves vaginal atrophy and associated symptoms.
î Can also relieve dysuria and may protect against recurrent lower urinary tract infections
î Estrogen therapy does not improve urinary stress or urge incontinence.
î Different forms of estrogen therapy are available.
î Low-dose estrogen creams are applied intravaginally from daily to two times a week at doses of 0.3 mg of conjugated estrogens or 0.5 g of estradiol per application.
î Estring is a silicone ring embedded with estrogen that releases 6 to 9 mg of estradiol daily and is kept in place for 3 months. It has minimal systemic absorption.
î Vagifem tablets are given vaginally as one per day for 14 days followed by twice per week. They have also been shown to estrogenize the vaginal mucosa without resulting in significant systemic absorption.
Menstrual Cycle Disturbances
• Because of the changing hormonal milieu, complaints of irregular bleeding are very common during the menopausal transition.
• If episodes of bleeding occur more often than every 21 days, last longer than 8 days, are very heavy, or occur after a 6-month interval of amenorrhea, evaluation of the endometrium must be undertaken to rule out neoplasm. This includes pelvic ultrasound, endometrial biopsy, and possible dilation and curettage with hysteroscopy.
• Oral contraceptive pills can be used during the menopausal transition until the onset of menopause.
• Benefits of this therapy, in addition to relief of vasomotor symptoms, include contraception, decreased
risk of endometrial and ovarian cancers, establishment of regular menses, and increased bone density.
SPECIAL CONCERNS FOR MENOPAUSAL WOMEN
Osteoporosis
• Osteoporosis is the condition of decreased bone mass and bone microarchitectural deterioration with resulting increased risk of skeletal fractures.
• In the United States, 4 to 6 million women (13% to 18% of those older than 50 years old) have osteoporosis, resulting in 1.5 million fractures per year.
• Ninety percent of all hip and spine fractures in Caucasian women aged 65 to 84 years are secondary to osteoporosis.
• Pathophysiology
• Estrogen deficiency causes an imbalance of skeletal remodeling, with an increase in resorption that is greater than bone formation.
• Results from a dominance of osteoclasts, which break down bone, and a decrease in osteoblastic activity. Estrogen binds to receptors on osteoclasts and inhibits their activity.
P.561
• Decreased serum calcium levels lead to an increase in parathyroid hormone (PTH), which stimulates osteoclastic activity. Estrogen deficiency also leads to increased bone sensitivity to PTH.
• Bone resorption matches bone formation until approximately age 25 to 35 years old. Bone mass decreases after that at a rate of 0.4% per year.
• After menopause, bone mass decreases 2% to 5% annually for 10 years and then the rate stabilizes to 1 % per year.
• Most common fracture sites include the lumbar vertebrae, wrist (distal radius), and hip (femoral neck).
• Known risk factors account for 30% of osteoporosis incidence (T able 43-2).
• Prevention and treatment guidelines are in Table 43-3.
• Diagnosis is determined by bone mineral density (BMD) with dual-energy x-ray absorptiometry (DEXA) being the preferred technique.
• BMD is best measured at the hip and is predictive of hip fracture and fracture at other sites.
î 7-scores are standard deviations above or below the comparison mean BMD of young women aged 20 to 29 years.
î Z-scores correspond to the same measurements using women of the same age as the reference.
î Normal bone 7-scores are above -1.0.
î Osteopenia 7-scores are between -1.0 and -2.5.
TABLE 43-2 Risk Factors for Osteoporosis
Family history of osteoporosis
Current cigarette smoking
Low body weight: fracture based on 7-score and other variables.
î Can help in determining when a patient should be screened for osteoporosis and when treatment should be initiated
î The U.S. Preventive Services Task Force (USPSTF) uses the FRAX algorithm to determine who should be screened. The USPSTF recommends screening before age 65 years for women who have risk for fracture that is equal to or greater than that of a 65-year-old Caucasian woman.
î The strongest risks for osteoporosis identified were low body weight, older age, weight under 57.7 kg (127 pounds) or BMI outcomes and specific aspects of memory function.
Cardiovascular Health
• Coronary artery disease (CAD) is the leading cause of death among postmenopausal women.
• Women lag 10 years behind men in terms of CAD risk prior to menopause.
• By age 70 years, a woman has the same risk of CAD as a male of the same age.
• Estrogen has a protective effect on reducing cardiovascular disease (CVD) risk in premenopausal women.
• Estrogen aids in vascular smooth muscle relaxation, decreases inflammation, decreases low-density lipoprotein levels, and increases high-density lipoprotein levels.
• The Framingham study showed a two- to sixfold increased incidence of CAD in postmenopausal women compared to premenopausal women in the same age group.
Hormone Replacement Therapy
Hormone Therapy and Coronary Heart Disease
• This is an area that is currently undergoing extensive review and debate.
• Observational studies
• Nurses' Health Study was the largest cohort study of US women, following 121,700 premenopausal women aged 30 to 55 years. A 10-year follow-up study found a reduced risk of major coronary disease and mortality from CVD for women taking estrogen compared to women who never used estrogen.
P.566 (The primary indication for HT in users was for primary prevention or treatment of vasomotor symptoms.)
• Prospective randomized clinical trials
• The Postmenopausal EstrogenZProgestin Interventions or PEPI trial found that women on HT had greater high-density lipoprotein cholesterol levels than women taking placebo. However, the Heart and EstrogenZprogestin Replacement Study (HERS) concluded that the use of estrogen plus progestin did not prevent further heart attacks or death from CHD. There were significantly more thromboembolic events in the HT users.
• The Women's Health Initiative (WHI) enrolled postmenopausal women aged 50 to 79 years (mean age 63 years; however, approximately one fourth of women were older than 70 years). In the estrogen plus progestin arm, approximately one third of women were receiving treatment for hypertension and 13% had high cholesterol. Women with severe menopausal symptoms were discouraged from participating.
î Participants received either estrogen plus progestin, estrogen alone if they had a hysterectomy, or placebo.
î The primary outcome was CHD, with fractures being a secondary outcome.
î Adverse events monitored were breast cancer and venous thromboembolism.
î After 5 years, the estrogen plus progestin arm of the study was stopped early because the number of
cases of breast cancer in the treatment group exceeded the predetermined threshold for increased risk.
î In 1 year, of 10,000 postmenopausal women who took estrogen plus progestin, 38 were diagnosed with breast cancer compared to 30 of 10,000 women who took placebo.
î Women in the estrogen alone group have not shown increased rates of breast cancer.
î Regarding CHD and other vascular events, results showed that per 10,000 women annually, the number of heart attacks, strokes, and blood clots were 37, 29, and 34 in the estrogen plus progestin arm compared to 30, 21, and 16 per 10,000 women taking placebo.
î Women taking estrogen alone also showed increased risk of these events relative to placebo.
î There were fewer bone fractures and diagnoses of colon cancer in both hormone groups.
î A secondary analysis showed that women who initiated HT closer to menopause (within 10 years) had reduced CHD risk compared to women more distant from menopause.
î Lower risk was found for young women and higher risk for older patients.
• The “timing hypothesis”: Given the findings of the Nurses Health Study and the secondary analyses of the WHI, it has been theorized that there could be a “window of opportunity” in the early postmenopause stage, when HT can have a protective effect on CVD risk. Further prospective, randomized controlled trials are necessary to evaluate this theory.
Hormone Therapy Conclusions
• HT remains the most effective treatment for menopausal signs and symptoms. It should not be used for the prevention of chronic diseases.
• Further study is required to determine the role and cardiovascular effects of estrogen in women less than 10 years post menopause.
P.567
SUGGESTED READINGS
American College of Obstetrics and Gynecologists Committee on Practice Bulletins— Gynecology. ACOG practice bulletin no. 129: osteoporosis. Obstet Gynecol 2012;120(3): 718-734.
American College of Obstetricians and Gynecologists Women's Health Care Physicians. Executive summary. Hormone therapy. Obstet Gynecol 2004;104(4)(suppl):1S-4S.
American College of Obstetricians and Gynecologists Women's Health Care Physicians. Vasomotor symptoms. Obstet Gynecol 2004;104(4)(suppl):106S-117S.
Anderson GL, Limacher M, Assag AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized control trial. JAMA 2004;291:1701.
Archer DF, Sturdee DW, Barber R, et al. Menopausal hot flushes and night sweats: where are we now?
Climacteric 2011;14:515-528.
Barrett-Connor E, Grady D, Sashegyi A, et al. Raloxifene and cardiovascular events in osteoporotic postmenopausal women: four-year results from the MORE (Multiple Outcomes of Raloxifene Evaluation) randomized trial. JAMA 2002;287:847.
Bone HG, Hosking D, Devogelaer JP, et al. Ten years' experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med 2004;350:1189.
Grady D. Management of menopausal symptoms. N Engl J Med 2006;355:2338.
Grady D, Herrington D, Bittner V, et al. Cardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA 2002;288:49.
Gourlay ML, Fine JP, Preisser JS, et al. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med 2012; 366(3):225-233.
Harlow SD, Gass M, Hall JE, et al. Executive summary: stages of reproductive aging workshop +10: addressing the unfinished agenda of staging reproductive aging. Menopause 2012;4:387-395.
Management of osteoporosis in postmenopausal women: 2010 position statement of the North American Menopause Society. Menopause 2010;17(1):25-54; quiz 55-56.
Nelson HD. Commonly used types of postmenopausal estrogen for treatment of hot flashes: scientific review. JAMA 2004;291:1610.
Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321.
Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007;297:1465.
The Writing Group for the PEPI T rial. Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women: the Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 1995;273:199.