42 Female Sexual Response and Sexual Dysfunction
Nina Resetkova
Linda Rogers
EPIDEMIOLOGY
• In the 1999 National Health and Social Life Survey, 1,410 men and 1,749 women aged 18 to 59 years were surveyed and 43% of these women reported sexual concerns.
A British national survey found that 54% of women reported at least one sexual problem lasting at least 1 month but only 21% sought help.• The most common female sexual problem in both studies was a lack of interest. Difficulty with orgasm was reported by 24%, difficulty with arousal by 19%, and pain
P.547 with sex by 14%. Accurate assessments of female sexual dysfunction are hampered by the fact that many patients have more than one type of dysfunction. Additionally, many patients complaining of lack of interest actually have a problem with another phase of the sexual response cycle, in part because they lack familiarity with the terms.
• Multiple studies have found that female sexual dysfunction is associated with a decreased sense of physical and emotional satisfaction and a decreased sense of overall well-being.
DIAGNOSIS OF SEXUAL DISORDERS
Screening
• Many physicians infrequently discuss sexual dysfunction due to limited time and training, embarrassment, or the perceived notion that there is an absence of effective treatment options. A few simple questions can initiate the discussion:
• Are you currently involved in a sexual relationship?
• Do you have sex with men, women, or both?
• Do you have any concerns about or pain with sex?
• Do you have any concerns you would like to discuss?
• Once a dialogue has been initiated, a complete history can be obtained. This should include the nature and frequency of the problem, the degree of distress, whether the problem is lifelong versus newly acquired, situational, or generalized. Additionally, the partner's sexual problems or concerns, partner reaction, and history of prior treatment or intervention should be discussed.
• It is important to elicit the patient's thoughts concerning the cause of the problems and their expectations from treatment. The physician must also get a medical history, a psychological/psychiatric history (e.g., mood disorders, body image disorders), sexual history including sexual abuse or violence, and a psychosocial history (e.g., relationship difficulties, cultural and religious beliefs that may affect function, work/finance/children, and other life stressors). It is also important to inquire about the use of medications that may cause sexual side effects and about the use of personal hygiene products such as soaps, laundry products, douches, or other possible skin irritants.
Physical Exam
• A thorough physical exam can help identify causes, address concerns, and educate the patient about her anatomy.
• During visual inspection of the external female genitalia and perineum, it is important to note any atrophy, lack of estrogenization, loss of architecture, scarring, hypopigmentation or hyperpigmentation, or possible infection. The exam should include the urethral meatus and anus. Wet prep and pH should be performed to evaluate signs of infection. Fungal cultures or polymerase chain reaction (PCR) testing should be sent if there is any doubt about the presence of yeast, as wet prep has a sensitivity of only 50%. Suspicious skin changes on the vulva warrant biopsy.
• A moistened cotton swab is used to systematically examine the vulva and map any areas of pain. If present, tenderness is most commonly found adjacent to the hymenal ring, but it is important to check the rest of the vulva for more generalized tenderness.
• A speculum exam and gentle digital exam are then performed. Attention should be paid to tenderness, adnexal masses or nodularity, pelvic floor muscle tone, prolapse, and the anal reflex.
• Laboratory tests are rarely useful, as they are poorly predictive of function and perception of function.
P.548
PHYSIOLOGY OF FEMALE SEXUAL FUNCTION
Female sexual function is a complex interplay of the central nervous system (CNS), peripheral nervous system, and end organs.
• The medial preoptic, anterior hypothalamic, and limbohippocampal areas are involved in sexual arousal.
• Estrogens, androgens, oxytocin, and dopamine are believed to promote female sexual response. In contrast, progesterone, prolactin, and serotonin are inhibitory.
• The vasculature and musculature changes involved in arousal are mediated by dopaminergic stimulation of the peripheral nervous system. Autonomic nerves release nitric oxide and vasointestinal polypeptide that modulate vasodilatation.
• Increased blood flow causes labial engorgement, increased vaginal lubrication, vaginal lengthening and dilation, and increased clitoral size.
• The pelvic floor muscles and the smooth muscle of the vagina spasm during orgasm. Contraction of the pelvic floor muscles involves adrenergic and cholinergic mechanisms from the efferent pudendal nerve.
• Estrogen primarily maintains the integrity of the tissues. Androgen levels are associated with libido and arousal.
• The arousal response in women involves increased heart rate, muscle tension, changes in breast sensations, and a subjective state of arousal.
THEORIES OF SEXUAL FUNCTION
For many years, female sexual function was described with a model more characteristic of men than of women. In 1966, Masters and Johnson defined the human sexual response as a sequential model including excitement (desire and arousal), plateau, orgasm, and resolution (Table 42-1). Recent research has found that the female sexual response is much more complex and is usually not linear.
• The Study of Women's Health Across the Nation (SWAN) surveyed 2,400 women of various ethnicities
(Hispanic, White non-Hispanic, African American, Chinese, and Japanese) in six US cities. The study found that 40% of these women never or infrequently felt desire, although the majority reported being capable of arousal. Only 13% expressed discontent.
• In 2011, Rosemary Basson developed a model of sexual arousal that incorporated psychological and social aspects of women's lives.
In her model, desire does not always precede sexual arousal. Instead, women often begin at a state of “sexual neutrality” and respond to or seek sexual stimuli based on many possible psychological motivations. The response to this stimulus is usually arousal, which leads to desire and improved arousal. This model can be explained to patients concerned about lack of desire and can normalize what women commonly experience (a lack of spontaneous desire but the presence of reactive desire) (Figure 42-1).• The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V), recently published in 2013, made some significant changes compared to the prior edition. Importantly, the diagnosis of sexual dysfunction requires a minimum duration of 6 months. The new edition combines female sexual desire disorder and female sexual arousal disorder into female sexual interest/arousal disorder, reflecting the research showing that most women experience both of these disorders and have difficulty distinguishing between them. A new diagnosis, genitopelvic pain/penetration disorder, merged vaginismus and dyspareunia, reflecting the difficulty women have in distinguishing the cause of penetration pain and the inadequacy of vaginal muscle spasm.
P.549
TABLE 42-1 Physiologic Female Sexual Response
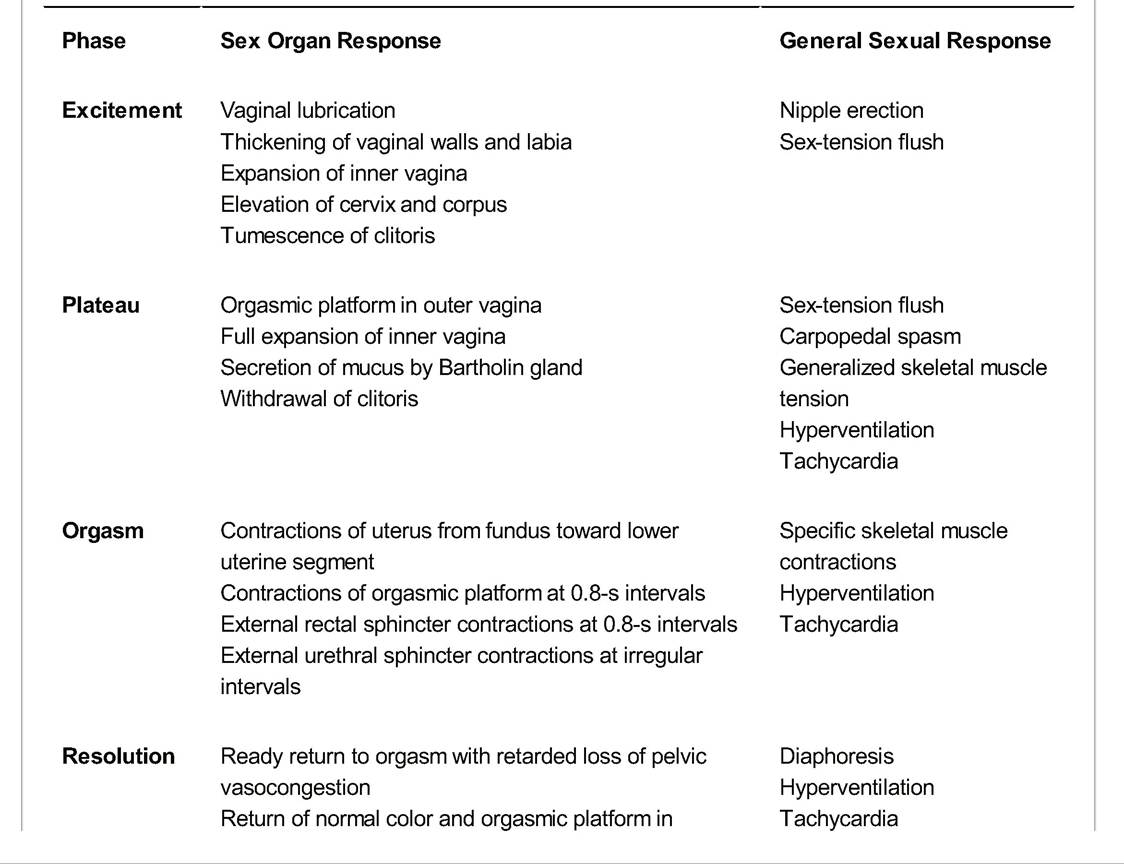
primary (rapid) stage
Loss of clitoral tumescence and return to position
From Beckman CR, Ling F, Barzansky BM, et al. Obstetrics and Gynecology, 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2002:610, with permission.
SEXUAL DYSFUNCTION DISORDERS
• Hypoactive sexual desire disorder—persistent or recurrent deficient or absent sexual fantasies or desire for sexual activity that causes marked distress or interpersonal difficulty
• Sexual aversion disorder—persistent or recurrent aversive response to any genital contact with a sexual partner, emphasizing the role of avoidance
• Female sexual interest/arousal disorder in DSM-V is a combination of the DSM-IV female sexual arousal disorder and female orgasmic disorder—persistent or recurrent deficient or absent sexual fantasies or desire for sexual activity and/or inability to attain or to maintain until completion of sexual activity an adequate genital lubrication-swelling response of sexual excitement and/or delay in or absence of orgasm following a normal sexual excitement phase that causes marked distress or interpersonal difficulty.
P.550
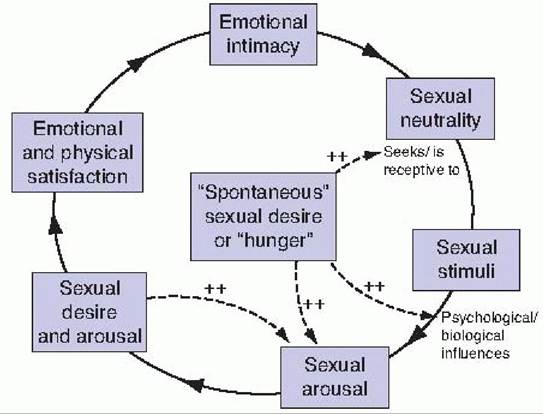
Figure 42-1. Basson's model of female sexual response. (From Basson R. Female sexual response: the role of drugs in the management of sexual dysfunction. Obstet Gynecol 2001 ;98:350-353, with permission.)
• Sexual pain disorders
• Genitopelvic pain/penetration disorder combines vaginismus and dyspareunia. Vaginismus was defined as persistent or recurrent involuntary spasm of the outer third of the vagina that interferes with sexual intercourse. Although this has been eliminated in the DSM-V, many providers continue to use this terminology. Dyspareunia was defined as genital pain associated with sexual activity that causes distress or interpersonal difficulty.
• Vulvodynia and vaginismus—these disorders typically present with introital dyspareunia. The International Society for the Study of Vulvovaginal Disease (ISSVD) defines vulvodynia as “vulvar discomfort, most often described as burning pain, occurring in the absence of relevant visible findings or a specific clinically identifiable, neurologic disorder.” Vulvodynia is then further divided into generalized and localized.
î Generalized
î Provoked (sexual, nonsexual, or both)
î Unprovoked
î Mixed (provoked and unprovoked)
î Localized (vestibulodynia—previously known as vulvar vestibulitis, clitorodynia, hemivulvodynia, etc.)
î Provoked (sexual, nonsexual, or both)
î Unprovoked
î Mixed (provoked and unprovoked)
î Although there may be no visible physical findings or microbiologic abnormalities, vulvodynia is now understood to involve changes in the nervous system, including an increase in nerve density and sensitivity in the vulva (peripheral sensitization), and changes in the CNS, which amplify the pain rather than diminish it (central sensitization).
P.551 î Localized vulvodynia in the vestibule is the most common subset of vulvodynia. According to a 2003 population-based study, the lifetime incidence of localized vulvodynia in women is about 12%, compared to 3% for generalized vulvodynia.
Assessment of Vulvodynia and Vaginismus
• The highest incidence of vulvodynia is in women ages 18 to 32 years. When perimenopausal or menopausal women present with these symptoms, it is important to first evaluate for and treat vaginal atrophy if indicated. Breast-feeding mothers and oral contraceptive pill users can also present with atrophic vaginitis and pain. This may be in part because of their progestogenic effect, which can block estrogenic effects. Additionally, there may be estrogen-related elevation in sex hormone-binding globulin, which binds preferentially to androgens, preventing their binding to androgen receptors in vaginal and vulvar tissue.
• Patients with vulvodynia are more likely to have other pain disorders such as migraine headaches, fibromyalgia, irritable bowel syndrome (IBS), and interstitial cystitis. Allergies and endometriosis may also be more prevalent. Reed et al. demonstrated that the presence of vulvodynia was associated with the presence of fibromyalgia, interstitial cystitis, and IBS with 27% of patients surveyed screening positive for multiple conditions.
• Many patients with vaginismus have a significant phobia regarding penetration and have never experienced penetration. Their physical exam may be indistinguishable from the vulvodynia patient. Introital hypersensitivity and muscle hypertonicity are commonly identified.
• Question carefully about hygiene practices. Patients may attribute their symptoms to uncleanliness and overwash with harsh soaps or use over-the-counter products with potential irritants, such as benzocaine (Vagisil).
T reatment for Vulvodynia and Vaginismus
• Nearly all patients with these disorders benefit from pelvic floor physical therapy performed by a physical therapist with specialized training.
• Mental health counseling is helpful for patients or couples to cope with the disorder.
• Vaginal dilator therapy can be initiated for those patients who are willing and exhibit identifiable Introital muscle tightness. Begin by teaching Kegel exercises and relaxation, then helping patient to insert the smallest dilator while in the office. Patients may use a mirror. Daily use is preferable.
• Dilators can be purchased online, or other cylindrically shaped objects can be used, including culturette tubes, syringes (with the Luer-lock tips removed), and candles.
• Patients can be encouraged to use their own fingers and later their partner's fingers as dilators.
Medical Treatments
• Many of the same oral medications that are used for other types of neuropathic pain are used. These patients tend to be anxious, hypervigilant, and sensitive to side effects, so start with a low dose and increase gradually.
• Tricyclic antidepressants (e.g., amitriptyline, desipramine): 25 to 150 mg/day
• Gabapentin 900 to 3,600 mg/day
• Topiramate 25 to 200 mg/day
• Venlafaxine 37.5 to 150 mg/day
• Duloxetine 60 mg/day
P.552
• Topical medications are often preferred by patients. No randomized controlled trials exist, and medications must usually be compounded in a specialized pharmacy. The vehicle is important because many patients are prone to irritant reactions. In general, gels and ointments are tolerated better than creams. Cellulose gel, acidmantle cream, and stearin-lanolin are examples of vehicles that tend to be well tolerated. Patients should be shown where to apply the product, as they may lack knowledge of their own anatomy.
• Lidocaine 2% to 5%, applied three times daily. This may cause stinging in some patients.
• Gabapentin 6%, applied three times daily
• Amitriptyline 2%/baclofen 2%
• Estradiol 0.01 % is often tolerated better in a noncream base such as cellulose gel
• T opical steroids are generally not recommended, especially for long-term therapy, because of the potential for tissue thinning and steroid rebound dermatitis.
Surgical Treatment
• Surgical management with vestibulectomy has an approximately 85% success rate.
• Success rates are lower for women with vulvodynia or vaginismus who decline sexual counseling, those who have untreated hypertonicity, and those with a longer duration of symptoms.
Follow-Up for VaginismusZVulvodynia Patients
• Patients should be reevaluated periodically during treatment (e.g., every 4 to 8 weeks) to track their response to treatment and to check for emergence of other disorders, such as vulvovaginal candidiasis or other infections, dermatologic problems, worsening pelvic floor muscle function, or relationship issues. Compliance with and tolerance of medications need to be reassessed periodically.
Vulvovaginal Atrophy
• Atrophy has become an increasingly common cause of sexual pain in the years since the Women's Health Initiative Study was published due to the decrease in use of systemic estrogen. Very tiny amounts of topical estrogen (a low-dose vaginal ring, 10-μg pills, or 0.5 g of estrogen cream twice weekly) are extremely effective and have little systemic absorption. When there is introital discomfort, it is critical that estrogen also be applied topically to the introitus; vaginal application will not affect this area. Topical estrogen is thought to be superior to systemic estrogen for the treatment of vulvovaginal atrophy and has shown benefit for overactive bladder symptoms and recurrent urinary tract infections. Symptom relief may occur within 3 to 4 weeks but may last up to 6 to 12 weeks. Women who do not wish to use topical estrogen can be counseled that regular sexual activity can be very effective at maintaining tissue integrity and elasticity.
• Ospemifene was approved by the U.S. Food and Drug Administration (FDA) in February of 2013 for the treatment of moderate to severe dyspareunia when the symptoms are related to vulvar and vaginal atrophy. This is a once-daily oral selective estrogen receptor modulator. It has a positive effect on the vaginal epithelium with lower rates of adverse effects of estrogen, such as stimulation of the endometrium and thrombosis.
Treatments for Sexual Interest and Arousal Disorder in Women
• Given that there is so much overlap among these disorders and that the female sexual response is a complex interaction, treatment must often be multifaceted.
P.553
• Pharmacology
î Androgens—there are currently no FDA-approved androgen treatments available for women, although there are several under development. Of women who have undergone oophorectomy and hysterectomy, those with a 300-mg transdermal testosterone patch had significantly increased numbers of sexual fantasies, amount of masturbation, and number of episodes of sexual intercourse. The feeling of positive well-being increased and depressed mood decreased at 300 mg versus 150 mg or placebo. There are concerns about the lack of safety data and the risks of clitoromegaly, hirsutism, acne, hepatotoxicity, and worsening lipid profile with prolonged use. Androgens can masculinize a female fetus. The risk of breast cancer with androgen use is unknown, and results from studies are contradictory.
î Estrogen—improves vaginal atrophy. The Women's Health Initiative trial did not show a significant difference in satisfaction with estrogen use.
î Sildenafil—a randomized trial of 781 women with arousal disorder showed no conclusive impact of sildenafil. It does appear to be beneficial for patients taking selective serotonin reuptake inhibitors (SSRIs) or those with spinal cord injury. The phosphodiesterase inhibitor tadalafil (Cialis) is longer acting.
• Counseling
î Cognitive behavioral therapy—identifies and modifies factors such as maladaptive thoughts, unreasonable expectations, behaviors that reduce trust, and insufficient stimuli and works to increase communication among partners. Orgasmic function can be treated as a learned skill, and cognitive behavioral treatments (e.g. directed masturbation) are highly effective.
î Sex therapy—includes sensate therapy that initially starts with nonsexual intimacy and focuses on feedback on what is pleasurable. This technique is effective in reducing sexual anxiety and helps both
partners avoid “spectating” or monitoring their own response during the encounter.
î Bupropion—as a non-SSRI antidepressant with dopaminergic activity, it may help with mood disorders, and can be used instead of SSRIs, or may be used to counteract SSRIs' effects on sexual function. There is some evidence that bupropion has prosexual effects in nondepressed women.
• Other treatments
î The suction vacuum device—the clitoral suction vacuum increases clitoral engorgement when the vacuum is applied and may lead to improved vascularization and sensation.
î Several over-the-counter, topically applied, arousal-enhancing products are available in the form of personal lubricants. There is limited research showing improvement in arousal or orgasm. These products can cause irritation of mucous membranes and should be applied to the labia majora or clitoris. Some herbal products also have limited research showing improvement in desire and satisfaction.
î Self-treatment books such as For Yourself by Lonnie Barbach, or Becoming Orgasmic by Julia Heiman and Ray Lopiccolo, are useful.
Persistent Genital Arousal Disorder
• First described in 2001, this disorder is characterized by persistent sensations of genital arousal even without sexual or emotional stimuli, causing the patient at least moderate distress. There are many proposed etiologies of PGAD, which may involve a range of psychological, pharmacologic, neurologic, and vascular causes. It
P.554 has been associated with other conditions including overactive bladder and restless leg syndrome and may often indicate a pudendal neuropathy. Treatment requires a multidisciplinary approach as well as cognitive therapy. Physical therapy, topical lidocaine, pudendal nerve blocks, transcutaneous electrical nerve stimulation units, or medications for chronic pain such as gabapentin may be helpful.
SEXUAL FUNCTION AND SPECIAL POPULATIONS
• Postpartum—sexual activity postpartum is affected by many things including fatigue, breast-feeding, adjustment to the new baby, hormonal changes, pain, and healing. In one study of 796 women, 32% resumed intercourse within 6 months and 89% after 6 months. Additionally, fewer women with anal sphincter tears reported sexual activity compared to those without these lacerations.
• Menopause and premature ovarian failure—postmenopausal women or those with premature ovarian failure are significantly affected by dysfunction and dyspareunia. One contributing factor in this population is vulvovaginal atrophy.
• Nonheterosexual relationships—regardless of a patient's sexual orientation, providers should address sexual concerns such as pain, risk for sexually transmitted diseases, and screening for domestic violence.
• Medical disorders and medications can affect sexual arousal and function. For example, diabetes and peripheral vascular disease may affect vasocongestion. Depression, substance abuse, and tobacco use can affect sexual function. Medications such as SSRIs, antipsychotics, antihypertensives, oral contraceptive pills, and medroxyprogesterone acetate are also known to affect sexual function.
• Pelvic floor disorders are associated with decreased arousal, infrequent orgasm, and increased dyspareunia. Patients may have loss of self-esteem, embarrassment, and decreased desire. Urinary or fecal incontinence may additionally cause fear of odor. Surgical management for pelvic floor disorders may increase sexual function, although patients should be counseled about operative risks such as dyspareunia or damage to nerves such as the dorsal nerve of the clitoris.
• Posthysterectomy—there are theoretical concerns that total or supracervical hysterectomy can disrupt the complex neurologic and vascular anatomy involved in sexual response. However, sexual function has not been shown to be compromised for most women and may actually be improved once issues such as menorrhagia are resolved. Additionally, studies have shown no difference for patients who preserved their cervix or not.
• Breast cancer and gynecologic oncology patients—disease and treatment can cause decreased desire, arousal, opinion of self, and overall decreased quality of life. Patients may have pain or bleeding. Radiotherapy, in particular, has sexual side effects. Symptoms such as vaginal atrophy or dyspareunia can be specifically addressed. Women can be encouraged to use vaginal moisturizers (applied two or three times weekly) and engage in regular sexual activity or masturbation to maintain blood flow to the genitals. The use of topical estrogens may be contraindicated or at least controversial in some patients, for instance those on aromatase inhibitors or with a history of estrogen receptor-positive breast cancer. However, it is sometimes done after consultation of the patient's oncologist. Estradiol levels can be followed to reassure the patient of minimal absorption. Options in the future may include ospemifene, topical testosterone, topical estriol, or topical oxytocin.
• Infertility—many infertile couples think of sexual intercourse as goal-oriented and may have trouble finding pleasure in sexual activity.
P.555
SUGGESTED READINGS
American College of Obstetricians and Gynecologists Committee on Practice Bulletins— Gynecology. ACOG practice bulletin no. 119: female sexual dysfunction. 2011;117(4): 996-1007.
Basson R. Sexual desire and arousal disorders in women. N Engl J Med 2006;354(14):1497-1506.
Carey JC. Pharmacological effects on sexual function. Obstet Gynecol Clin North Am 2006;33: 599-620.
Facelle TM, Sadeghi-Nejad H, Goldmeier D. Persistent genital arousal disorder: characterization, etiology, and management. J Sex Med 2012;10(2):439-450.
Haefner HK, Collins ME, Davis GD, et al. The vulvodynia guideline. J Low Genit Tract Dis 2005;9(1):40-51.
Kammerer-Doak D, Rogers R. Female sexual function and dysfunction. Obstet Gynecol Clin North Am 2008;35:169-183.
Reed BD, Harlow SD, Sen A, et al. Relationship between vulvodynia and chronic comorbid pain conditions. Obstet Gynecol 2012;120(1 ):145-151.
Rosen RC, Barsky JL. Normal sexual response in women. Obstet Gynecol Clin North Am 2006;33: 515-526.
Shifren JL, Braunstein GD, Simon JA, et al. Transdermal testosterone treatment in women with impaired sexual function after oophorectomy. N Engl J Med 2000;343(10):682-688.
Srivastava R, Thakar R, Sultan A. Female sexual dysfunction in obstetrics and gynecology. Obstet Gynecol Surv 2008;63(8):527-537.