41 Hyperandrogenism
Katherine Ikard Stewart
Lisa Kolp
Androgens are necessary for normal ovarian and sexual function. They play an important role in cognition, bone health, muscle mass, body composition, mood, and energy.
The obstetrician-gynecologist must have a strong knowledge base regarding the role androgens play in normal female physiology.• Androgens are precursors for estrogen synthesis.
• Although controversial, it has been proposed that androgens may be necessary for normal sexual desire in women.
• Androgens also affect skeletal homeostasis. They affect bone metabolism directly via androgen receptors expressed by osteocytes and indirectly via conversion of androgens to estrogen. Multiple studies have shown that women with low androgen concentrations have lower bone density and increased fracture risk.
ANDROGENS IN THE FEMALE
Androgens circulate in the body in various forms. Circulating androgens found in the blood of premenopausal women include testosterone, androstenedione, dehydroepiandrosterone (DHEA), DHEA sulfate (DHEA-S), and dihydrotestosterone (DHT). Androgens are produced by the adrenal glands and the ovary and arise from peripheral conversion.
Testosterone
• T estosterone is the most potent androgenic hormone.
• In women, nearly 25% of testosterone is secreted from the ovaries and 25% is from the adrenal glands. The remaining one half is produced from peripheral conversion of androstenedione to testosterone in the kidneys, liver, and adipose tissue.
• Normal circulating concentrations range from 20 to 80 ng/dL.
• Approximately 65% of testosterone in the circulation is bound to sex hormone-binding globulin (SHBG). Nineteen percent to 33% of testosterone is loosely bound to albumin. The remaining 1% of testosterone circulates in the free and active form (Fig. 41-1).
• T estosterone levels decrease by 50% from ages 20 to 40 years.
Less testosterone is secreted from the ovary with menopause, as the ovarian theca cells are less responsive to luteinizing hormone (LH). As menopause is entered, SHBG levels remain constant, yielding an even greater decrease in free testosterone. However, serum hormone concentrations of SHBG fall due to the lack of estrogen, finally resulting in an increase in bioavailable testosterone.Androstenedione
• Is a less potent androgen than testosterone but can produce significant androgenic effects when present in excess amounts
• Is produced in equal amounts by the adrenal glands (50%) and the ovaries (50%)
Majority of androstenedione is converted to testosterone.
P.537
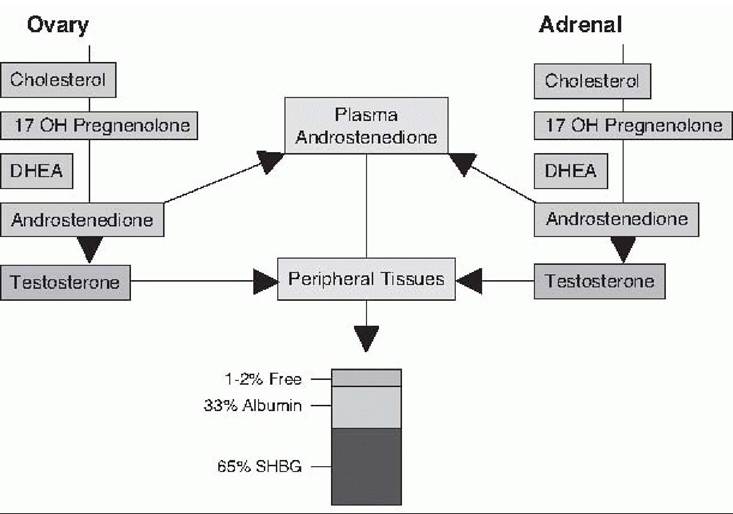
Figure 41-1. Endogenous production and secretion of testosterone in women. DHEA, dehydroepiandrosterone; SHBG, sex hormone-binding globulin.
• Normal serum concentration ranges from 60 to 300 ng/dL, often with a 15% increase at midcycle. Androstenedione circulates in blood, bound to both SHBG and albumin.
Dehydroepiandrosterone and Dehydroepiandrosterone Sulfate
• Androgen precursors, much less potent than testosterone, are produced predominantly by the adrenal glands, with some component of ovarian production and peripheral conversion.
• DHEA is metabolized quickly, thus measurement of its serum concentration does not reflect adrenal gland activity. DHEA-S has a much longer half-life than DHEA, and measurement of its serum level is used to assess adrenal function.
• Serum hormone concentrations of DHEA-S in women vary widely and depend on age (normal range of approximately 35-340 pg/dL depending on the lab).
Dihydrotestosterone
• Testosterone is converted to DHT by 5-alpha reductase, an enzyme found in many androgen-sensitive tissues.
• DHT is a very potent androgen primarily responsible for the androgenic effects on hair follicles.
Sex Hormone-Binding Globulins
• Androgenicity is determined by free hormone concentrations.
Thus, SHBG influences the hormonal state. Testosterone and insulin both decrease SHBG levels, whereas estrogen and thyroid hormone increase its levels.Symptoms of hyperandrogenism may be seen in patients with a normal total testosterone level if the serum hormone concentration of SHBG is reduced to a level that significantly increases the free hormone.
CLINICAL FINDINGS IN HYPERANDROGENISM
Hyperandrogenism is characterized by an abnormally elevated serum concentration of androgens and/or physical findings consistent with androgen excess. Androgenic hormones in the female can stimulate abnormal terminal hair growth, voice and muscle changes, hair loss, clitoral enlargement, and reduction in breast size. Physical characteristics of hyperandrogenism are as follows.
Androgenic Hair Changes
• During gestation, the hair follicles of the developing fetus produce fine, unpigmented hair known as lanugo. The total number of hair follicles is determined late in the second trimester of pregnancy. With time, some of the hair follicles produce thick, darkly pigmented terminal hair in response to androgen exposure. The remaining hair follicles produce vellus hair, which are finer and not as darkly pigmented.
• Normal hair growth cycle follows three stages: anagen (growth phase), catagen (involution phase), and telogen phase (rest phase).
Hirsutism
• Hirsutism is excessive male pattern hair growth in women. It refers to the growth of terminal hair on the face, chest, back, lower abdomen, and upper thighs caused by the overactivity or overexpression of circulating androgens. The abnormal hair growth is predominantly midline. Androgens stimulate hair growth, increase the diameter of the hair shaft, and deepen the pigmentation of the hair. In contrast, estrogens slow hair growth and decrease hair diameter and pigmentation.
• Idiopathic hirsutism is the term used when a hirsute individual has normal levels of circulating androgens and has not been diagnosed with polycystic ovarian syndrome (PCOS) or another disorder.
• The Ferriman-Gallwey score is an objective tool that may be used in the clinical setting to grade hair growth in women. This method evaluates nine different androgen-sensitive hair growth sites on a scale from 0 to 4. Ninety-five percent of women will have a score under 8. Scores >8 suggest an excess of androgenmediated hair growth and this should be confirmed with a more extensive hormone evaluation.
Hypertrichosis
• Hypertrichosis is the generalized, excessive growth of vellus hair. It may be caused by genetic factors, underlying malignancy, or exposure to drugs such as phenytoin, penicillamine, diazoxide, cyclosporine, and minoxidil. It may also be seen with a number of medical conditions, including anorexia nervosa, hypothyroidism, malnutrition, porphyria, dermatomyositis, and paraneoplastic syndromes. Hypertrichosis should not be mistaken for hirsutism.
Hair Loss
• Recession of hair in the frontal and temporal regions of the scalp and the crown of the head (i.e., male pattern baldness) in response to androgens is common with aging. This is the most common pattern of hair loss and affects approximately 30% to 40% of men and women alike. However, hair loss is less evident in women because it is typically more diffuse and rarely complete. The fact that excessive androgen activity stimulates hair growth on some parts of the body while causing hair loss from others remains unexplained.
P.539
• Young men and women with androgenic alopecia have higher levels of 5-alpha reductase, increased androgen receptors, and lower levels of the enzyme cytochrome P-450 aromatase (which converts androgens
such as testosterone and 4-androstenedione to the estrogens estradiol and estrone, respectively).
Virilization
• This is an appearance of masculine features due to extreme excess androgenic activity. It refers to a constellation of symptoms, including deepening of the voice, male body habitus, male pattern baldness, clitoromegaly, and reduction of breast size.
• Virilization is very rare and may be associated with adrenal tumors and hyperplasia or ovarian tumors, such as theca lutein cysts, luteomas, and Sertoli-Leydig cell tumors.
Skin Changes
• Androgens stimulate secretions from pilosebaceous glands, resulting in oily skin. Severe acne is a manifestation of excessive androgenic hormone activity.
Voice Changes
• The vocal cords can undergo irreversible thickening, resulting in a lower tone of the voice.
Male Body Habitus
• Hypertrophy of major muscle groups, such as arm and leg muscles, occurs in response to androgen exposure and may result in the development of a male body habitus.
Clitoromegaly
• Enlargement of the clitoris may occur. This is a dose-dependent event and is irreversible. It is more commonly seen when the excessive androgen exposure occurs in childhood or around the time of puberty.
Acanthosis Nigricans
• Acanthosis nigricans is a gray-brown, velvety discoloration of the skin that is associated with hyperinsulinemia and obesity. Acanthosis nigricans is typically seen in the groin, neck, axillary, and vulvar regions. These patients should undergo testing for diabetes mellitus. Acanthosis nigricans can also be a paraneoplastic syndrome and associated with an underlying malignancy, commonly an adenocarcinoma involving the gastrointestinal (GI) tract.
DIAGNOSIS OF HYPERANDROGENISM
History and Physical Examination
• Hyperandrogenism may be diagnosed if signs of androgen excess are present (see earlier discussion).
• A careful medical history should be taken, including a detailed menstrual history asking about age of menarche, regularity of menstrual cycles, pregnancies, oral contraceptive preparation (OCP) use, and presence of symptoms of ovulation or menstrual molimina. Patients should also be asked about a history of thyroid disease and hyperinsulinemia.
• A complete physical examination should be conducted, including evaluation for galactorrhea and acanthosis nigricans.
• Pay particular attention to medications (see earlier text) and family history.
P.540
Laboratory Evaluation
• Measurement of serum androgen levels may be obtained to diagnose hyperandrogenism (Fig. 41-2). The clinician should check the following:
• Testosterone serum hormone concentrations
• DHEA-S >700 ng/dL, consistent with abnormal adrenal function
• 17-Alpha-hydroxyprogesterone (17-OHP): Normal level is 100 to 300 ng/dL.
• Prolactin (normal range 1 to 20 ng/mL): Hyperprolactinemia can be associated with hyperandrogenism, as it is likely that prolactin receptors are located on the adrenal glands. When prolactin binds to these adrenal receptors, it stimulates the release of DHEA-S.
• Thyroid function tests
• Assessment of hyperinsulinemia:
î Normal fasting glucose 126 mg/dL, hemoglobin A1C >6.5%, 2-hour oral glucose tolerance test (75-g load) >200 mg/dL, or a random plasma glucose >200 mg/dL.
CAUSES AND TREATMENT OF HYPERANDROGENISM
Five major causes of hyperandrogenism have been identified:
• PCOS
• Late-onset adrenal hyperplasia
• T umors of the ovary or adrenal glands
• Cushing syndrome
• Idiopathic or drug-induced processes
Polycystic Ovarian Syndrome
• PCOS is the most common endocrine disorder among reproductive age women. It affects approximately 4% to 12% of this population.
• In 1935, Stein and Leventhal described seven women who were amenorrheic, obese, and hirsute with cystic ovaries. From this initial description, the term Stein-Leventhal syndrome was originally used to identify other similarly affected women.
• Because of the cystic changes found within the ovaries of affected patients, the terms hyperandrogenemic chronic anovulation syndrome, PCOS, and polycystic ovary disease (PCOD) are now used to describe these patients. However, polycystic ovaries alone seen on radiologic imaging are a nonspecific finding and may be seen in normal women.
• Individuals with PCOS do not have orderly follicular development. Most cycles fail to lead to the emergence of a dominant follicle or release of an oocyte. Although follicle development occasionally proceeds to ovulation, development of the follicle to only its initial growth stage is common. The ovarian cortex becomes populated with numerous small follicles or “cysts.” The hyperandrogenemic state is believed to be both a cause and effect of incomplete follicular development.
• PCOS is associated with amenorrhea, hyperandrogenism, hyperinsulinemia, and metabolic syndrome. In patients affected by this disorder, it is important to make the appropriate diagnosis early and to closely monitor these individuals, as they may be at risk for other comorbidities as a consequence of the underlying pathology.
Diagnosis of Polycystic Ovarian Syndrome
• In May 2003, the Rotterdam European Society of Human Reproduction and Embryology/American Society for Reproductive Medicine-sponsored PCOS consensus workshop revised the diagnostic criteria to include any two of the following three manifestations:
• Oligomenorrhea and/or anovulation
• Hyperandrogenism (clinical and/or biochemical signs)
• Polycystic ovaries
• In 2009, the Androgen Excess and PCOS Society also defined less inclusive criteria for PCOS which required ALL of the following criteria be met:
• Hyperandrogenism: hirsutism and/or hyperandrogenemia AND
• Ovarian dysfunction: oligo-anovulation and/or polycystic ovaries AND
• Exclusion of other androgen excess or related disorders
• Of note, PCOS is always a diagnosis of exclusion in all definitions. All other etiologies of hyperandrogenism must be ruled out.
• Patients with PCOS typically present with oligomenorrhea, amenorrhea, hirsutism, obesity, and infertility. All or some of these symptoms may be present.
• Hyperandrogenism can be demonstrated by either hirsutism or elevated levels of androgens.
• Virilization is not consistent with a diagnosis of PCOS and other etiologies should be considered.
• Polycystic ovaries are defined as 12 or more follicles in each ovary measuring 2 to 9 mm and increased ovarian volume >10 mL as judged by transvaginal sonography.
• Insulin resistance and metabolic syndrome are often associated with PCOS and all obese women should be screened for comorbidities. Providers should check a cholesterol panel, blood pressure, fasting glucose, and 2-hour oral glucose tolerance test. Further studies are needed to determine the use of these tests in nonobese women with PCOS.
Pathophysiology of Polycystic Ovarian Syndrome
• The exact cause of PCOS remains unknown. Abnormalities of the hypothalamicpituitary axis and the ovarian or adrenal steroidogenic pathway have been suggested as possible explanations.
• Pituitary and hypothalamus: At the level of the hypothalamic-pituitary axis, increases in the frequency and amplitude of LH pulses have been recorded. A ratio of serum LH to follicle-stimulating hormone of greater than 2 is observed in PCOS patients.
• Ovarian androgen production: Increased secretion of androgens from the ovaries has been observed in patients with PCOS. Elevated LH levels may lead to increased activity of ovarian theca cells, thus producing androgens. Also, elevated insulin may stimulate androgen secretion from both the ovaries and adrenals.
• Adrenal androgen production: Some PCOS patients may have mild elevations of DHEA-S levels.
• Consequences of anovulation: Ovulation for many women with PCOS may occur infrequently, but ovaries in these patients continue to secrete low levels of estrogen. Due to the lack of cyclic estrogen and progesterone withdrawal over time, unopposed estrogen can lead to proliferation of the endometrium that may result in abnormal bleeding and, if untreated, may progress to endometrial hyperplasia and/or endometrial carcinoma.
• Hyperinsulinemia and insulin resistance: Increased resistance to insulin is often observed in patients with PCOS, whether or not they are obese. Insulin may cause or contribute to the hyperandrogenic state by activating insulin receptors within the ovary, augmenting androgen secretion, or by acting on insulin-like growth factor receptors.
Treatment for Hyperandrogenism/Polycystic Ovarian Syndrome
• Treatment of the patient with hirsutism, hyperandrogenism, or hyperandrogenic chronic anovulation depends on the underlying etiology and the desire for pregnancy. Hirsutism is slow to respond to hormone suppression. Results may not be seen for up to 6 months. Unfortunately, androgen suppression will not alter previous hair growth patterns. Mechanical methods of hair removal, such as shaving, waxing, depilatories, laser, and electrolysis, should also be considered.
• Lifestyle modifications should be first line in the management of hyperandrogenism. For those individuals who suffer from hirsutism and obesity, weight loss of even 5% of original body weight can often improve symptoms related to
P.543 PCOS. Weight loss may result in an elevation of SHBG, a decrease in bioavailable testosterone, and an improvement in insulin sensitivity.
• OCPs reduce circulating gonadotropin levels and increase SHBG levels; both work to decrease circulating androgens. OCPs are the first line of treatment of oligomenorrhea caused by PCOS. Progestins decrease total androgen level by reducing the activity of 5-alpha reductase. OCP usage results in an overall decrease in the formation of new androgen-dependent hair growth and androgenstimulated acne. All low-dose OCP preparations are believed to have similar results. If therapy with OCPs is suboptimal, addition of an antiandrogen, such as spironolactone or finasteride, is recommended.
• If combination OCPs are contraindicated or not desired, medroxyprogesterone acetate may be administered (5 to 10 mg for 10 to 12 days) every month or every other month to produce regular withdrawal bleeding. Patients should be cautioned that, unless contraception is used, pregnancy is possible with cyclic progestin therapy.
• Metformin hydrochloride is a biguanide antihyperglycemic drug, U.S. Food and Drug Administration (FDA) approved for the management of type 2 diabetes mellitus. Metformin decreases hepatic gluconeogenesis, thus reducing the need for insulin secretion. It also decreases the intestinal absorption of glucose and improves insulin sensitivity in the peripheral system, including skeletal muscle, liver, and adipose tissue. In some studies, metformin has been shown to restore menses in approximately 50% of women with PCOS. Another trial showed that metformin, compared to placebo, can improve plasma insulin and insulin sensitivity, reduce serum free testosterone, and increase serum high-density lipoprotein cholesterol.
î Dosing: The optimum dose of metformin for restoration of menses in women with PCOS ranges from 500 mg by mouth three times daily to 850 mg by mouth twice daily. Patients should be titrated up to the appropriate dose of this medication, starting at the lowest dose once daily, due to the GI side effects.
î Metformin has a limited role in the treatment of hirsutism. Other agents may be added to metformin to improve these symptoms.
î Metformin appears to be unique among insulin-sensitizing agents in that it can improve weight loss (particularly a greater reduction in abdominal fat), hyperandrogenism, and menstrual cycles in individuals with PCOS.
• Spironolactone therapy is often initiated if OCP use is not an option for the treatment of hirsutism or if results from OCP therapy are not optimal. An aldosterone antagonist, spironolactone, is an antihypertensive agent that was originally found to cause gynecomastia in men. Spironolactone directly inhibits 5-alpha reductase and decreases androgen synthesis. The usual dose is 25 to 100 mg by mouth twice daily. After 6 months of therapy at 100 to 200 mg/day, there is a reduction in the diameter of terminal hair and cessation of new terminal hair growth. Doses are then tapered to a maintenance dose of 25 to 50 mg per day. Because of potential adverse effects on genitalia of male fetuses, spironolactone should be used with contraception in sexually active women. Other side effects include diuresis, orthostatic hypotension, fatigue, dysfunctional uterine bleeding, hyperkalemia, and breast enlargement.
• Flutamide is a nonsteroidal antiandrogen used for prostate cancer that blocks the binding of androgen to its receptor. When administered in a dosage of 250 mg/day, inhibition of new hair growth is observed. Side effects include dry skin and, rarely, hepatotoxicity. Liver function should be monitored during treatment. Due to adverse fetal effects, effective contraceptive therapy is mandatory.
• Finasteride: An inhibitor of mostly type II 5-alpha reductase, finasteride was developed initially as a treatment for prostate hypertrophy and cancer. By inhibiting
P.544 5-alpha reductase, the drug decreases DHT activity at the level of the hair follicle. Finasteride treatment prevents new hair growth and decreases the terminal hair shaft diameter. Finasteride is orally dosed at 5 mg daily. No major side effects have been associated with this drug. Again, due to adverse fetal effects, reliable contraception should be used.
• Minoxidil is the only drug approved by the FDA for treatment of androgenic alopecia in women. It promotes hair growth by increasing the duration of the anagen phase and enlarging miniaturized and suboptimal follicles. It is available over the counter as a 2% and 5% topical solution.
• Corticosteroid therapy is another alternative for the treatment of hirsutism and hyperandrogenism and is the primary mode of therapy for those individuals suffering from congenital adrenal hyperplasia (CAH). The steroids suppress the hypothalamicpituitary-adrenal axis and can result in improved hirsutism and ovulatory function. Corticosteroid therapy should not be used for the long term in patients with PCOS, as it may result in debilitating osteoporosis and worsening glucose intolerance.
• Eflornithine hydrochloride is a cream that reduces unwanted facial hair. Eflornithine is a potent antagonist of ornithine decarboxylase, the enzyme necessary for the production of polyamines, organic compounds that stimulate and regulate the growth of hair follicles and other organs. Women who apply eflornithine hydrochloride (13.9% cream) to their faces twice daily have shown improvement after 24 weeks in some clinical trials. The benefit is usually first seen at 8 weeks.
• Surgery: Older women who have no desire for fertility and who do not desire continued hormonal therapy may consider bilateral oophorectomy, with or without hysterectomy.
Fertility Treatment for Polycystic Ovarian Syndrome
• In PCOS patients, assistance with ovulation induction frequently is required.
• Clomiphene citrate is usually administered orally in dosages of 50 to 100 mg/day for 5 days on a monthly basis to induce ovulation in infertile women. It is not used for cycle regulation or as a primary treatment for hirsutism. Monitoring with a basal body temperature chart, LH levels, pelvic ultrasonography, or serum progesterone 14 days after the last clomiphene citrate dose may be used to confirm ovulation. For the patient resistant to clomiphene citrate, the addition of metformin hydrochloride (500 mg three times daily) may result in ovulation.
• Direct stimulation of the ovary may be used to induce ovulation through the intramuscular or subcuticular administration of gonadotropins in the treatment of anovulatory infertility. See Chapter 32.
Late-Onset or “Nonclassical” Adrenal Hyperplasia
• Excess androgen production is a common feature shared by most forms of CAH. Unlike typical CAH, symptoms of late-onset CAH are not evident until late childhood or adolescence.
• The most common adrenal enzyme defect is 21-hydroxylase (21-OH) deficiency, which is an autosomal recessive disorder.
• Enzyme deficiencies of 11-beta-hydroxylase and 3-beta-hydroxysteroid dehydrogenase are far less common.
• 21-OH converts progesterone to 11-deoxycorticosterone or 17-OHP to 11-deoxycortisol (Table 41-1). A decrease in the activity of this enzyme causes diminished cortisol production by the adrenal gland, resulting in increased pituitary secretion of adrenocorticotropic hormone (ACTH). ACTH stimulates the adrenal gland to
P.545 produce increased precursor 17-OHP. Higher 17-OHP levels lead to secretion of androstenedione, which is then converted to testosterone.
TABLE 41-1 Enzymes and Their Characteristics
| Deficient Enzyme | Androgen Levels | Mineralocorticoid Levels | Female Virilization at Birth |
| 21-Hydroxylase | Excess | Deficiency | Yes |
| 11-β-Hydroxylase | Excess | Excess | Yes |
| 17-α-Hydroxylase | Deficiency | Excess | No |
Diagnosis
• Measure the basal levels of 17-OHP in the morning. Levels of 17-OHP should be 1,000 mg/dL are concerning for the presence of an ovarian or adrenal androgen-producing tumor.
• Surgical removal with or without adjuvant therapy is the treatment of choice.
P.546
Cushing Syndrome
• Patients with Cushing syndrome often exhibit specific physical findings. See Chapter 13.
Idiopathic and Drug-Induced Hirsutism
• Idiopathic hirsutism is diagnosed in hirsute individuals who have a negative workup for other causes of hirsutism. Studies show that 5% to 15% of hirsute patients may have idiopathic hirsutism. An alternative explanation is based on the hypothesis that patients with idiopathic hirsutism demonstrate increased skin sensitivity to androgens. One theory is that patients with idiopathic hirsutism convert testosterone to DHT in greater quantities than normal due to increased activity of 5-alpha reductase.
• Occasionally, drugs may be causative. Danazol and methyltestosterone are two drugs that may cause iatrogenic hirsutism.
• The same medications used to treat hirsute PCOS patients may be used to treat patients with idiopathic hirsutism.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 108: polycystic ovary syndrome. Obstet Gynecol 2009;114:936-949.
Brodell LA, Mercurio MG. Hirsutism: diagnosis and management. Gend Med 2010;7(2):79-87.
Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab 1961;21:1440-1447.
Hock DL, Seifer DB. New treatments of hyperandrogenism and hirsutism. Obstet Gynecol Clin North Am 2000;27(3):567-581, vi-vii.