Changes in the renal system
In pregnancy the renal parenchymal volume increases by 70% by the third trimester. Both the vascular volume and the interstitial space increases with the most dramatic anatomical changes in dilatation of the calyces, renal pelvis and ureter (50).
These changes occur in the first trimester due to the hormonal changes in pregnancy. The changes are more prominent on the right side due to anatomical distribution. As pregnancy progresses the uterus may cause partial ureteric obstruction as it compresses the ureters at the pelvic brim. There is hypertrophy of the ureteric smooth muscle and hyperplasia of the connective tissue, ureteral peristalsis is unchanged.Renal blood flow and GFR are both increased during a normal ovulatory menstrual cycle. If conception occurs these changes are maintained, thus renal blood flow increases by 50-80% in the first trimester (51, 52). This is maintained in the second trimester and decreases by 15% during the third trimester. GFR also increases in the first trimester and then is maintained until delivery although the extent of increase is less than that of renal blood flow. These changes are shown in Figure 8.3. Changes in the 24-hour creatinine clearance are a convenient method of assessing probable change in the GFR. By 4 weeks of gestation, the 24-hour creatinine clearance has increased by 25% and by 9 weeks, by 45% (51). During the third trimester there is a steady decrease towards non-pregnant values (53). A small increase in the GFR and creatinine clearance is seen in the initial few days following delivery (53).
The increase in plasma volume in pregnancy is secondary to water retention. Very early in pregnancy the plasma osmolality decreases to about 10 mOsm/kg less than prepregnancy (54). In the
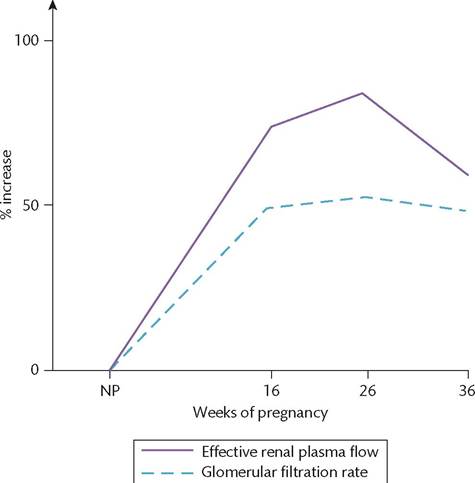
Figure 8.3 The changes in renal function during pregnancy are largely complete by the end of the first trimester and are thus proactive not reactive to the demands of pregnancy.
The filtration fraction falls during the first trimester but begins to return to non-pregnant (NP) levels during the third trimester.Reproduced from Chamberlain G & Broughton Pipkin F (eds); Clinical Physiology in Obstetrics; 3rd edn: Blackwell Science; 1998 with permission from Blackwell.
non-pregnant state, this reduction in plasma sodium and anions would inhibit antidiuretic hormone arginine vasopressin (AVP) release, therefore causing diuresis. However, in pregnancy the osmotic thresholds are reduced by 4-6 weeks of pregnancy, stimulating water intake and diluting bodily fluids (54). These changes are thought to be secondary to human chorionic gonadotropin. AVP continues to circulate at a sufficient concentration to stimulate water reabsorption from the renal medullary collecting ducts until the plasma osmolality decreases below the new threshold of pregnancy. Renal sodium handling is the prime determinant of volume haemostasis. In pregnancy, there is an accumulation of approximately 950 mmol of sodium in the fetus and the mother's extracellular volume. This retention occurs very gradually by just 3-4 mmol of sodium a day. It is thought to occur as a result of high circulating concentrations of progesterone acting at the distal tubule, increased natriuretic prostacyclin, atrial natriuretic peptide, and plasma prolactin. Despite this, plasma concentration of sodium is reduced by approximately 4-5 mmol/L in pregnancy due to the increase in plasma volume.
Clinical considerations
• Vesicoureteric reflux occurs in at least 3% of pregnant women due to the lateral displacement of the ureters and shortened intravesical portion. The presence of ureteric dilatation in combination with vesicoureteric reflux is associated with a high incidence of urinary stasis which may cause urinary tract infection in pregnancy.
• The normal kidney is increased in size by 1 cm in pregnancy. Dilatation of the ureters may persist until 16 weeks after delivery.
• The significant increase in GFR and plasma volume cause a reduction in the plasma concentration of solutes such as creatinine and urea. Interpretation of laboratory reports should always take this into consideration as using non-pregnant thresholds incorrectly during pregnancy may lead to failure to identify decreased renal function. Serum creatinine decreases from an average of 73 mmol/L to 65, 51, and 47 mmol/L in the successive trimesters of pregnancy (52).
• Renal tubular function also changes significantly during pregnancy. Uric acid filtration doubles and there is a decrease in net tubular reabsorption, thus serum uric acid concentrations decrease by 25% by mid pregnancy. At later gestations, less filtered uric acid is excreted so a rise in serum concentrations is normal (52). The normal pregnancy range of serum uric acid is 148-298 μmol∕L.
• Glucose excretion increases during pregnancy by tenfold. Intermittent glycosuria is a normal feature of pregnancy and not helpful in the diagnosis of diabetes mellitus which requires assessment of blood glucose (52).
• The excretion of amino acids also increases although the pattern of excretion is not constant and differs for individual amino acids. This is due to inadequate tubular reabsorption to cope with the 50% increase in GFR.
• Excretion of total protein and albumin rises during pregnancy until at least 36 weeks. In late pregnancy, the upper limit of normal is 200 mg per 24 hours of urine collection (55).
• Despite increased reabsorption of calcium from the renal tubules, urinary calcium excretion is two- to threefold higher in normal pregnancy compared to prepregnancy. This is thought to be secondary to the increased concentrations of 1,25-dihydroxyvitamin D. Renal bicarbonate reabsorption and hydrogen ion excretion remain the same, therefore the urine is usually mildly alkaline in pregnancy.