Chapter 10Care in labour
Analgesia and anaesthesia in obstetrics
Breech
Brow presentation
Cord prolapse
Episiotomy and obstetric perineal trauma
Face presentation
Fetal surveillance in labour
Home birth
Induction of labour
Labour
Maternal collapse
Meconium-stained liquor
Placenta praevia
Placental abruption
Postpartum haemorrhage
Prelabour rupture of membranes at term
Resuscitation of the newborn
Retained placenta
Shoulder dystocia
Shoulder presentation
Uterine inversion
Analgesia and anaesthesia in obstetrics Analgesia for labour
Definition
Although labour and delivery can be extremely painful, not every woman’s experience is the same.
Regional analgesia, non-regional techniques, and pharmacological agents are used to provide pain relief for the parturient. Non-regional methods of labour analgesia include acupuncture, aromatherapy, hydrotherapy (birthing pool), transcutaneous electrical nerve stimulation (TENS), sterile water blocks, relaxation and breathing techniques, and massage. The most frequently used pharmacological agents are Entonox (50% nitrous oxide in oxygen) and meperidine (pethidine), but morphine and other opioids such as fentanyl, diamorphine, and remifentanil are also increasingly used. Epidural and spinal analgesia provide very effective and reliable pain relief by blocking the transmission of pain signals through spinal nerves in or near the spinal cord.Epidemiology
Pain relief not facilitated by regional anaesthesia is still most frequently used during labour, although an increase in the uptake of epidural analgesia can be seen in many parts of the world. The type of labour analgesia used can be significantly influenced by the woman’s epidemiological, cultural, or religious background.
Non-regional techniques
TENS has been put forward as a way of providing analgesia by blocking the transmission of pain signals through stimulation of Aβ-fibres and local release of β-endorphines.
However, there is no evidence that TENS is more effective than placebo; TENS has minimal side-effects and may be appropriate for women who decline all other methods of pain relief in labour. Equally, there is no clear evidence that aromatherapy, acupuncture, hydrotherapy, and sterile water blocks are effective to relieve pain in labour; and only continuous support throughout labour and delivery has been shown to have a positive influence on analgesia requirements and the spontaneous vaginal delivery rate.Pharmacological agents
Nitrous oxide mixed 50:50 with oxygen (Entonox), which has been used in obstetric practice for over a century, is widely available and provides analgesia within 60 seconds of inhalation. Besides its clear advantages, ease of use, a very short half-life and its safety profile, nitrous oxide can have significant side-effects such as drowsiness, disorientation, and nausea, and current evidence suggests that it provides only incomplete analgesia in most women. Nitrous oxide can be useful in places where other analgesic options are limited or unavailable. The phenylpiperidin derivate Meperidine (Pethidine), which can be given by a registered midwife without a physician’s prescription, is usually administered intramuscularly (0.5–1.0 mg/kg). Despite its still widespread use many investigators have suggested that Meperidine provides merely sedation rather than analgesia, and that Pethidine is less efficacious than Entonox. Like any other opioid, Meperidine causes dose-dependent respiratory depression, pruritus, and obstipation and can delay gastric emptying; the metabolite Normeperidine has convulsant properties. Meperidine crosses the placenta and the highest fetal plasma concentration can be measured 2–3 hours after its maternal intramuscular administration. Babies of women who have received meperidine in labour have been shown to be sleepier and less able to establish breastfeeding despite normal Apgar scores. Morphine, diamorphine, fentanyl, and remifantanil do not have convulsant effects but tend to be less frequently used for labour analgesia.
Fentanyl, and especially remifentanil, have been successfully used with patient-controlled analgesia (PCA), for example in cases where regional analgesia is not available or is contraindicated. Remifentanil is an ultra-short-acting opioid that is rapidly hydrolysed by unspecific esterases; it does not accumulate even after prolonged infusions. Bolus doses of 0.25–0.5 µg/kg with a 1–3-minute lockout interval have been used successfully. However, careful instruction of all staff and the patient herself, as well as close monitoring of both parturient and neonate, is essential; supplementary oxygen may be required in some cases.Regional techniques
Uterine pain is transmitted to the dorsal horns of T10–L1 of the spinal cord via sensory fibres, vaginal pain via the S2–S4 nerve roots; neuraxial techniques can effectively attenuate or completely block the transmission of pain signals.
Indications for regional techniques in labour
These include
• maternal request
• obstetric reason (e.g. pre-eclampsia, twin pregnancy)
• maternal cardiovascular, respiratory or neurological disease (e.g. mitral or aortic regurgitation; asthma; intracranial lesions)
• anticipated operative delivery.
Contraindications (absolute) for regional techniques in labour
These include
• maternal refusal
• severe hypovolaemia/haemorrhage
• allergy to local anaesthetics
• local infection at site of insertion
• systemic sepsis
• known clotting disorder, coagulopathy (a platelet count >80 ? 109/L and normal clotting will be adequate in most cases).
Oral or written consent should be obtained prior to performing any regional technique. Ideally, discussions about neuraxial analgesia should take place antenatally, as many women are unable to recall information which is given during labour.
Epidural analgesia
Like any other neuraxial regional technique, epidural analgesia requires secure i.v. access, a full lateral or sitting position of the parturient, a sterile technique and monitoring of the fetal heart rate.
The maternal blood pressure should be measured at 3–5-minute intervals for at least 20 minutes after every bolus of local anaesthetic is administered.The combination of spinal and epidural analgesia (CSE) will achieve a rapid onset of very effective pain relief but can be technically more challenging.
Recent studies clearly indicate that epidural analgesia does not result in an increase in the Caesarean section rate; it may, however, cause an increase in the operative vaginal delivery rate. Careful management of epidural analgesia is paramount to its success rate. Side-effects such as hypotension, motor block, unilateral or ‘patchy’ blocks, total spinal, fetal bradycardia, and maternal respiratory depression can be avoided by
• gentle and ‘appropriate’ administration of low concentration local anaesthetics (e.g. Bupivacaine 0.075–0.125%), supplemented with opioids (e.g. Fentanyl 2 µg/mL). Patient-controlled epidural analgesia (PCEA) with or without a continuous background infusion can be superior to bolus administration of local anaesthetics
• regular assessment of height and quality of the block (e.g. Bromage scale)
• insertion of soft and multiport epidural catheters into the epidural space (approximately 5 cm of catheter should be positioned within the epidural space)
• limiting intrathecal opioids to small doses if spinal analgesia or combined spinal epidural (CSE) analgesia is used.
The most frequent side-effect of epidural, spinal, or CSE analgesia is mild hypotension but a fall in systolic blood pressure of only 10–20% is usually accepted. If more severe hypotension occurs, it has to be treated without delay:
• left lateral tilt in order to prevent, treat or avoid aortocaval compression
• administration of 100% oxygen, vasoconstrictors such as phenylephrine (e.g. 100 µg bolus) and crystalloid fluid through a large bore cannula.
Severe complications of regional techniques are rare; global or partial failure of epidural analgesia is the most frequently experienced complication.
If positioning towards the failing side, manipulation of the catheter itself and top-ups with more potent local anaesthetics (e.g. bupivacaine 0.25%) are unsuccessful, the epidural has often to be re-sited. It is even more important to check the quality of the block regularly if an operative vaginal delivery/Caesarean section is anticipated. The insertion of an epidural catheter can lead to a marked rise in maternal temperature; however, the reason for this and the significance for mother and fetus remain uncertain. Postdural puncture headache (PDPH) occurs in less than 1% of all paturients who have received neuraxial analgesia. Loss of cerebrospinal fluid through the punctured dura with stretching of the meninges is thought to cause this headache. If the dural puncture is recognized while the epidural puncture is performed, the ‘epidural’ catheter can be passed into the intrathecal space and subsequently used as a ‘spinal catheter’; further top-ups should then be given only by an anaesthetist. Pain relief will be excellent and the incidence of PDPH is thought to be reduced. PDPH can be seen in 70–85% of cases of accidental dural puncture and occurs typically 24–48 hours after the event. Late management includes the prescription of oral analgesics (e.g. paracetamol and/or diclofenac); aggressive fluid administration and strict bed rest do not appear to be beneficial. Therapeutic blood patches are currently thought to be efficacious in up to 85% of cases, but definitive advice on the timing and the volume to be injected must await further evidence.A ‘total spinal’, nerve damage, and back pain are discussed in the next chapter Anaesthesia in obstetrics. Local anaesthetics given in too large doses, or accidentally injected intravenously, can provoke cerebral convulsions or cause apnoea, unconsciousness and cardiac arrest. Intralipid 20% has been successfully used in patients to treat, in combination with standard cardiopulmonary resuscitation, local anaesthetic toxicity.
For women with pre-eclampsia epidural analgesia is usually the method of choice. Dramatic increases in blood pressure associated with contraction pain are avoided and the uteroplacental perfusion may be improved. It is important to obtain a platelet count (and test for normal clotting parameters in more severe cases) prior to the epidural or spinal puncture; current guidelines recommend a platelet count of at least 80 ? 109/L.
Paturients who receive prophylactic (or therapeutic) low molecular weight heparin (LMWH) must wait at least 12–24 hours after their last dose of LMWH before neuraxial analgesia or anaesthesia can be performed safely. Anaesthesia in obstetrics
Anaesthesia is mainly required for Caesarean sections and instrumental deliveries but can also be necessary postpartum (e.g. removal of retained placenta). General anaesthesia or, far more frequently, regional anaesthetic techniques are used to eliminate pain and inhibit motor activity almost completely during obstetric operations.
Anaesthetists are involved in the care of paturients in 25–75% of cases. This number obviously correlates with the local Caesarean section rate and the demand for epidural analgesia during labour. Regional anaesthesia is the method of choice for elective and most emergency Caesarean sections. Regional anaesthesia rates well above 90% or even 95% are not unusual in places where modern obstetric anaesthesia is practised.
Spinal anaesthesia and CSE are most commonly used for elective Caesarean sections.
Epidural anaesthesia
Epidural anaesthesia is typically established by using epidural catheters, already in situ for labour analgesia, for the injection of stronger local anaesthetics (e.g. Bupivacaine 0.5%). Rapid haemodynamic effects are less likely to occur with epidural or CSE anaesthesia and are frequently performed in women who would not tolerate sudden changes in peripheral vascular resistance (e.g. maternal cardiovascular disease).
Technique
Regardless of the regional technique planned, informed consent must be obtained prior to the procedure and maternal refusal is an absolute contraindication for regional anaesthesia.
Good intravenous access with at least one large bore cannula (14G or 16G) must be established and the parturient should also have received antacid prophylaxis. For elective surgery 150 mg ranitidine is commonly given orally 12 hours and 2–4 hours before surgery, combined with 10 mg metoclopramide orally 2–4 hours before surgery and, immediately prior to the procedure, 30 mL of 0.3 M sodium citrate orally. For emergency cases 50 mg ranitidine and 10 mg metoclopramide is injected slowly i.v., combined with 30 mL of 0.3 M sodium citrate orally.
Neuraxial anaesthesia is typically performed in the lumbar region between L2 and L3, L3 and L4, or L4 and L5 of the vertebral segments of the spine. The full lateral position can be associated with less hypotension and is probably slightly more comfortable for the patient. Many anaesthetists prefer the paturient to be in the sitting position which makes anatomical landmarks along the spine easier to identify.
Neuraxial anaesthesia can cause significant hypotension by the inhibition or an almost complete blockade of the sympathetic nerve system. Crystalloid solutions have been commonly administered for ‘pre-loading’ the patient’s intravascular space. However, the effect of spinal or epidural anaesthesia on the incidence of hypotension reported in the literature is not consistent. The use of colloid solutions appears to be more efficacious but the potential for side-effects such as anaphylaxis and the additional costs involved must also be considered. Hypotension should be treated promptly to avoid side-effects such as dizziness, nausea, and vomiting for the mother, and potential risks such as hypoperfusion of the placenta and acidaemia for the fetus. Phenylephrine (50–100 µg i.v. bolus) is usually very effective and has recently been shown to be associated with fetal acidosis less often than is ephedrine (Table 10.1.1).
Epidurals which are only partly effective in labour will be unlikely to provide good anaesthesia for instrumental or surgical deliveries. These epidurals shouldn’t be topped up prior to the procedure and spinal anaesthesia would provide better (and safer) anaesthesia in these cases.
Severe complications after epidural, spinal or (CSE) anaesthesia are rare; the incidence of temporary and permanent nerve damage is probably in the region of 1 in 10 000 and 1 in 50 000 respectively. Neurological deficits can also result from prolonged vaginal or instrumental deliveries (lithotomy position) and studies have shown that neurological symptoms after general anaesthesia are as (un-)common as they are after regional anaesthesia.
A ‘total spinal’ can occur if too much local anaesthetic has been injected into the intrathecal space and is characterized by a rapid onset of weakness of arms and respiratory muscles, followed by apnoea, cardiovascular depression, and unconsciousness; it is rare (1 in 5000–1 in 50 000) but must be treated immediately with intubation of the trachea and ventilation of the patient; cardiovascular support with vasoactive drugs is often also necessary.
Back pain is frequently reported to be a typical complication after neuraxial anaesthesia but several controlled trials appear to show that ‘new, long-term postpartum back pain is not caused by intra-partum epidural analgesia or anaesthesia’. The annual prevalence of back pain among women of reproductive age is reported to be up to 50% and can increase to 76% during pregnancy (Table 10.1.2).
General anaesthesia
General anaesthesia is commonly reserved for patients who are unsuitable for regional techniques, where there is immediate threat to the life of mother or fetus (Category I Caesarean sections), or for other emergencies. Indications for general anaesthesia include
• maternal request
• need for immediate delivery/surgery (e.g. Category I Caesarean section)
• regional anaesthesia is contraindicated (severe haemorrhage, clotting disorder, eclampsia)
• failed or insufficient regional block (pre- or intra-operative conversion to general anaesthesia).
Table 10.1.1 Comparison epidural and spinal anaesthesia

Table 10.1.2 Complications of regional anaesthesia

Technique
At term, the risk for aspiration of gastric content is significantly higher in pregnant women and antacid prophylaxis and a ‘rapid sequence induction of anaesthesia’ (RSI) are obligatory in order to minimize this risk. Sufficient pre-oxygenation with 100% oxygen in the left lateral tilt position, intubation and subsequent ventilation with 50% oxygen, as well as keeping the maternal blood pressure at a stable level are all measures to avoid hypoxaemia or hypoperfusion of the uteroplacental unit. Careful assessment of the woman’s airway is very important but it is interesting to know that difficult and failed intubations occur in parturients with approximately the same frequency as in non-pregnant patients (grade 3 or 4 laryngoscopy in 1–6% of cases, failed intubations in 0.1–0.6% of cases). Obstetric anaesthetists have to manage difficult airways only infrequently because most procedures are nowadays performed under regional anaesthesia. It is therefore essential that equipment for difficult intubations is up to date, always available and that all anaesthetic staff are familiar with a difficult airway drill.
In contrast to general anaesthesia for Caesarean sections, regional anaesthesia techniques allow the woman to be awake during the delivery of her baby, and the partner can also be present. There are additional advantages such as a slightly reduced peri-operative blood loss, improved 1-minute Apgar scores in infants born by Caesarean section and better and more prolonged analgesia after neuraxial blockade. However, current data do not support the view that maternal mortality is higher in patients who receive general anaesthesia. The individual patient’s situation and risk factors, and the experience of the anaesthetist, should determine the technique to be used. In women with pre-eclampsia for instance, regional anaesthesia is considered to be safe as long as platelet count and clotting remain within the normal range; blood pressure changes after epidural or spinal anaesthesia are typically less severe in pre-eclamptic patients, and general anaesthesia carries the significant risk of uncontrolled pressure responses to laryngoscopy and intubation.
Anaesthesia-related maternal (and neonatal) mortality is nowadays extremely low and aspiration of gastric contents, a major cause of maternal deaths in the 1950s, is fortunately a rare occurrence. However, there is still a certain amount of controversy about whether paturients should be allowed to eat during labour. Recent studies indicate that the intake of solid food leads to an increased risk of vomiting and aspiration, especially if opioids are administered during labour. Until more evidence is available, it appears rational to restrict solid foods but allow calorie-containing clear fluids such as energy drinks) for maternal comfort. Further reading
Comparative Obstetric Mobile Epidural Trial (COMET) Study Group UK. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial. Lancet. 2001;358:19–23.
Halpern SH, Douglas MJ (eds). Evidence-based obstetric anesthesia. Oxford: Blackwell Publishing 2005.
Hodnett ED, Gates S, Hofmeyr GJ, et al. Continues support for women during childbirth. Cochrane Database Sys Rev 2003; 3.
Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med 2003;28:172–97.
Lee A, Ngan Kee W D, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anesth Analg 2002;94:920–6.
O’Sullivan G, Liu B, Shennan AH. Oral intake during labor. Int Anesthesiol Clin 2007;45:133–47.
Rosenblatt MA, Abel M, Fischer GW, et al. Successful Use of a 20% Lipid Emulsion to Resuscitate a Patient after a Presumed Bupivacaine-related Cardiac Arrest. Anesthesiology 2006;105:217–8.
To WW, Wong MW. Factors associated with back pain symptoms in pregnancy and the persistence of pain 2 years after pregnancy. Acta Obstet Gynecol Scand. 2003;82:1086–91.
Wilson MJ, Cooper G, MacArthur C, et al.; Comparative Obstetric Mobile Epidural Trial (COMET) Study Group UK. Randomized controlled trial comparing traditional with two ‘mobile’ epidural techniques: anesthetic and analgesic efficacy. Anesthesiology 2002;97:1567–75. Internet resources
The Obstetric Anaesthetists’ Association (OAA): www.oaa-anaes.ac.uk
International Journal of Obstetric Anesthesia (IOJA): www.elsevier.com/wps/find/journaldescription.cws_home/623045/description#description
Breech Definition
A malpresentation in which the fetus is in longitudinal lie and the presenting part is buttocks (or ‘breech’), with the head occupying the upper pole of the uterus. Epidemiology and predisposing factors
The incidence of breech presentation at term is between 3% and 4% and shows an inverse relationship with the gestational age. It is estimated that about 25% of fetuses would present by breech and 28 weeks and this figure falls to 5% at 34 weeks, suggesting that there is a progressive ‘spontaneous version’ to cephalic presentation as the pregnancy advances.
The main factors that result in spontaneous version to cephalic presentation include progressive calcification of the fetal skull bones (i.e. the head becomes heavier and therefore sinks down due to gravity, occupying the lower pole); gradual reduction of the amniotic fluid volume as the gestation advances that enables the uterus to exert its ‘piriform’ shape (i.e. in earlier gestations, due to the relatively large amniotic fluid volume, the uterus loses its ‘piriform’ shape and becomes ‘globular’, thereby allowing the fetus more flexibility with regard to lie and presentation); as the fetus grows, the larger (and bulkier) breech is forced to occupy the more spacious upper pole, whereas the head moves down to occupy the smaller lower pole of the ‘piriform’ uterus. It has been postulated that ‘fetal kicking’ plays an important role in facilitating spontaneous version and therefore an intact and functioning neuromuscular system appears to be essential for this process.
Predisposing factors
Prematurity is the commonest cause of breech presentation as the mechanisms described above that result in spontaneous version to cephalic presentation, gradually operate over time, with advancing gestation. Hence, it is obvious that earlier the gestation, greater the chance of breech presentation.
Factors that alter any of the variables that have been described are likely to predispose to breech presentation. These include alterations in amniotic fluid volume (oligoor polyhydramnios), changes in uterine shape that eliminate the ‘piriform effect’ (congenital malformations such as septate or bicornuate uterus, fibroids in the lower segment, placenta praevia, cornual implantation of the placenta), and fetal factors that alter the normal anatomy such as congenital malformations (e.g. hydrocephalus that makes the head bulkier than breech), intrauterine growth restriction (smaller baby has more ‘space’ to occupy, nullifying the restrictive effects of piriform uterus), and multiple pregnancy. Abnormalities of the central nervous system or neuromuscular defects can affect fetal ‘kicking movements’ that may prevent spontaneous version.
True cephalopelvic disproportion (CPD) due to a contracted pelvis (rare) and congenital uterine anomalies may predispose to recurrent breech presentation. This term is used when three or more consecutive pregnancies are complicated by breech presentation (also termed ‘habitual breech’). Types of breech
There are three main types of breech presentation.
Frank breech (or extended breech)
This is the commonest type of breech presentation (60–70%) that is characterized by flexion at the hip joint and extension at the knee joint. It is the commonest breech in primigravidae and possibly reflects firm (i.e. previously unstretched) uterine and abdominal wall muscles that do not allow enough intrauterine space for the fetus to flex its knees. Frank breech is ideal when vaginal breech delivery is contemplated because it is firmly applied to the cervix during labour. This enables good cervical dilatation during labour and does not allow any free space between the breech and the cervix, resulting in reduced incidence of cord prolapse. In fact, the incidence of cord prolapse with frank breech is similar to cephalic presentation (0.5%).
Complete breech (or flexed breech)
Characterized by flexion at both hip and knee joints. Common in multigravidae possibly due to lax abdominal and uterine muscles (due to stretching and loss of tone as a consequence of previous pregnancies) that allows sufficient space for the fetus to flex the knees. It is also common in cases where there is an increase in the intrauterine space–fetus ratio, such as polyhydramnios or intrauterine growth restriction. Complete breech is not very well applied to the cervix and hence it is a poor dilator of the cervix during labour and has an increased risk of cord prolapse (5%) as compared to frank breech.
Footling presentation (incomplete breech)
Characterized by extension at both hip and knee joints, the feet being the presenting part. Sufficient intrauterine space is essential for the extension to occur both at knee and hip joints and hence, footling breech presentation is common in extreme preterm fetuses. Footling breech is associated with significant perinatal morbidity and mortality due to increased incidence of cord prolapse (15%) and head entrapment. The latter is due to the possibility of the feet and trunk passing through a partially dilated cervix, up to the neck of the fetus, and the head being ‘entrapped’. This is especially common in a preterm fetus that has a relatively larger head–trunk ratio than a term fetus.
• Knee presentation is very rare and is characterized by extension at the hip joint and flexion at the knee joints. Risks are similar to footling breech presentation.
• When breech presentation occurs in the absence of any obstetric (maternal and fetal) or medical complications, it is termed ‘uncomplicated breech’. Conversely, when any of these risk factors (e.g. previous Caesarean section, placenta praevia, intrauterine growth restriction) coexist, it is termed ‘complicated’ breech presentation. Pathophysiology
In contrast to cephalic presentation, the largest and least compressible part (i.e. the fetal head) presents last during vaginal breech delivery. This has many implications.
• It is possible for the fetal body to be passed through a partially dilated cervix, especially in case of a preterm fetus with footling presentation. This may lead to head entrapment, fetal hypoxia and fetal demise.
• The base of the skull which presents in breech presentation consists of skull bones, which are fused, as opposed to bones of the cranial vault in cephalic presentation, which are joined by membranous sutures. The latter facilitates moulding (overriding of skull bones on each other) and helps in the correction of mild degrees of cephalopelvic disproportion. Hence, in breech presentation, the fetal skull bones do not have the capacity to undergo moulding and this may result in fetopelvic disproportion.
• Absence of moulding and relatively quicker delivery than cephalic presentation may result in sudden ‘compression–decompression’ injury to the fetal brain, especially, if the delivery of after-coming head is not controlled. This may result in intracranial haemorrhage and possible long-term neurological sequelae.
• Owing to rapidity of delivery as well as malconducted breech delivery, especially by inexperienced birth attendants, fetal injuries may occur. These include fracture of the femur, dislocation of the hip, soft tissue injury (rupture of liver, spleen), fracture of humerus and injury to the spinal cord (including laceration and complete transaction of the spinal cord) as well as skull fractures and intracranial haemorrhage.
• Sentinel hypoxic events during labour such as cord prolapse may cause hypoxic–ischaemic encephalopathy. Preterm fetuses with breech presentation may not have the necessary physiological reserve to cope with hypoxia and also have increased risk of birth trauma. Clinical approach
History
History of uterine anomalies, previous breech presentation, placenta praevia, and fibroids should raise a clinical suspicion of abnormal lie and malpresentation, including breech presentation.
Clinical examination
On abdominal palpation, hard and round head will be felt in the upper pole of the uterus and is ballotable, whereas the soft, ‘more bulky’ breech will be felt in the lower pole. On auscultation, fetal heart sounds are audible usually at or above the umbilicus (fetal heart is located closer to the fetal head). In cases of undiagnosed (or misdiagnosed) breech presenting in labour, an irregular, broad, soft tissue mass may be felt on vaginal examination. The presence of the anal orifice in the same plane as bony prominences on either side (ischial tuberosities) may help differentiate a breech presentation from a cephalic presentation. In the latter, the mouth and two bony prominences on either side (malar eminences) are on different planes (like a triangle). It is also sometimes possible to elicit a ‘sucking response’ if the examiner’s finger is inserted into the mouth of the fetus during a vaginal examination in face presentation as opposed to a ‘gripping action’ in case of breech presentation due to the constriction of the anal sphincter.
Investigations
Ultrasonography is the gold standard to confirm the diagnosis of breech presentation. This may also provide additional information such as number of fetuses, estimated fetal weight (EFW), the amniotic fluid volume, location of the placenta, presence of nuchal cord, hypertension of fetal head, and other information such as coexisting soft tissue masses (e.g. fibroids), which may aid in planning the mode of delivery. Earlier, some advocated radiological (X-ray) and CT pelvimetry to exclude fetopelvic disproportion prior to planning a vaginal delivery. However, there is no evidence to support this and these investigations are not recommended in current practice. Management
There are three management options: vaginal breech delivery (spontaneous, assisted, and breech extraction); external cephalic version (ECV) and elective Caesarean section.
Vaginal breech delivery
The Term Breech Trial by Hannah et al. (2000) concluded that vaginal breech delivery is associated with increased perinatal mortality, neonatal mortality, and serious neonatal morbidity compared with an elective Caesarean section (1.6% versus 5%; RR 0.33, 95% CI 0.19–0.56; pthe risks and benefits, makes an informed choice to have a vaginal birth
• preterm breech deliveries (the findings of the Term Breech Trial is applicable for ‘term’ fetuses only)
• previously undiagnosed breech presentation in advanced labour (risks of an emergency caesarean section to both the mother and her baby may outweigh any potential benefits)
• a patient who has been planned to have an elective Caesarean section for breech presentation is admitted in advanced labour. It is estimated that up to 10% of women may go into labour prior to the date of their planned (elective) caesarean section
• twin pregnancy with second twin presenting by breech. The Term Breech Trial is applicable to singleton pregnancies at term
• in centres where facilities for an elective Caesarean section are not freely available (e.g. developing countries).
If vaginal breech delivery is contemplated, there are three approaches:
• spontaneous breech delivery (especially in multipara)—clinician does not perform any manoeuvres and allows nature to take its course
• assisted vaginal breech delivery (AVBD) is recommended. Delivery of the baby up to the level of the umbilicus is unaided (sometimes Pinard’s manoeuvre in an extended breech to flex the knee). Assistance is then offered for the delivery of the shoulder, especially in cases of extended or nuchal arms (Lovset’s manoeuvre) and the ‘after-coming’ head (Burns–Marshall technique, Mauriceau–Smellie–Viet (MSV) technique or the use of forceps). It is important not to pull in haste (may cause extension of the fetal head or nuchal arms), hold the fetus on the pelvic brim and not the abdomen (avoids injury to intraperitoneal organs), avoid hyperextension of the neck (avoids cervical spine injury), and to have a controlled delivery of the ‘after-coming’ head (avoids intracranial haemorrhage due to sudden compression–decompression injury)
• breech extraction refers to an accelerated process of delivering the fetus by pulling on the feet, with no or minimum effort by the mother. It is contraindicated in modern obstetric practice due to potential fetal and maternal trauma. However, when there is cord prolapse or acute fetal distress of the second twin, after the delivery of the first twin, this procedure may be attempted to expedite delivery if the cervix is fully dilated.
External cephalic version (ECV)
This refers to ‘manipulation of the fetus through the mother’s abdomen, with a view to turning the fetus from breech to cephalic presentation, thereby to avoid a caesarean section’.
• ECV should be offered at term (ideally 37–38 weeks, when there is sufficient amniotic fluid).
• Contraindications for normal delivery should be excluded (placenta praevia, hyperextended head, previous uterine scars, large fetus (>4 kg), clinically inadequate pelvis, and growth-restricted fetus). In addition, absolute contraindications include major uterine abnormality, multiple pregnancy, ruptured membranes, abnormal cardiotocograph (CTG), and significant antepartum haemorrhage within the preceding 7 days.
• Overall success rate of ECV is between 50–60% and this may be improved, especially in primigravidae by tocolysis (terbutaline 0.25 µg subcutaneously) 20 minutes prior to the procedure.
• Fetal heart rate should be monitored both before (to assess fetal wellbeing) and after (to detect complications) the procedure.
• Women should be informed of potential risks, including placental abruption, fetomaternal haemorrhage (may require Anti-D if Rhesus negative), cord accidents, and, rarely, uterine rupture. The chance of an emergency caesarean section is about 0.5%.
• Women should be informed that there is a spontaneous reversion rate (to breech presentation) of 5% and the possibility of intrapartum emergency Caesarean section.
Elective Caesarean section
Lower segment Caesarean section (LSCS) should be offered to all patients who have had a failed ECV or have declined ECV, as well as those who have an absolute contraindication for vaginal delivery or ECV.
• Adequate exposure is essential to facilitate a ‘non-traumatic’ delivery. The manoeuvres during a Caesarean section are similar to assisted vaginal breech delivery: the breech, trunk and shoulders, as well as the ‘after-coming’ head should be delivered in that order, using the same manoeuvres, where necessary (Pinard’s to deliver the legs, Lovset’s to deliver the shoulders, Burns–Marshall or obstetric forceps to deliver the ‘after-coming’ head). In cases of extended head (‘star-gazing’), flexing the head prior to delivery is likely to make delivery easier.
• It may be prudent to use tocolysis in established labour (especially late first stage or second stage of labour) to abolish uterine contractions and to facilitate easy delivery during caesarean section. Post ‘Term Breech Trial’
• A 2-year follow up study by the Term Breech Trial Group has concluded that there is no significant difference with regard to neurodevelopmental delay between the vaginal and planned Caesarean section groups, at 2 years of age. Subsequently, Glezerman (2006) has suggested that analysis of the original and new data gives rise to serious concerns as far as study design, methods, and conclusions are concerned (with respect to the original ‘Term Breech Trial’). In a substantial number of cases, there was a lack of adherence to the inclusion criteria. There was a large interinstitutional variation of standard of care; inadequate methods of antepartum and intrapartum fetal assessment were used, and a large proportion of women were recruited during active labour.
• More recently, an observational prospective study with an intent-to-treat analysis concluded that in units where planned vaginal delivery is a common practice and when strict criteria are met before and during labour, planned vaginal delivery of singleton fetuses in breech presentation at term remains a safe option that can be offered to women.
• In light of recent studies that further clarify the long-term risks of vaginal breech delivery, the American College of Obstetricians and Gynecologists (ACOG) recommends that the decision regarding mode of delivery should depend on the experience of the healthcare provider.
• Despite of its shortcomings, the Term Breech Trial was a randomized controlled trial that concluded that vaginal breech delivery is associated with an increased perinatal morbidity and mortality compared with an elective Caesarean section. Hence, before a vaginal breech delivery is planned, women should be informed that the risk of perinatal or neonatal mortality or short-term serious neonatal morbidity may be higher than if a Caesarean delivery is planned, and the patient’s informed consent should be documented. Failure to do so may have medicolegal implications. Further reading
ACOG Committee Opinion No. 340. Mode of term singleton breech delivery. Obstet Gynecol 2006;108:235–7.
Chandraharan E, Arulkumaran S. Acute tocolysis. Curr Opin Obstet Gynecol 2003;17:151–6.
Glezerman M. Five years to the term breech trial: the rise and fall of a randomized controlled trial. Am J Obstet Gynecol 2006;194:20–5.
Goffinet F, Carayol M, Foidart JM, et al. PREMODA Study Group. Is planned vaginal delivery for breech presentation at term still an option? Results of an observational prospective survey in France and Belgium. Am J Obstet Gynecol 2006;194:1002–11.
Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Lancet 2000;356:1375–83.
Royal College of Obstetricians and Gynaecologists. Pelvimetry: clinical indications. Green-top Guideline No. 14. London: RCOG 1998.
Royal College of Obstetricians and Gynaecologists. External cephalic version and reducing the incidence of breech presentation. Green-top Guideline No. 20a. London: RCOG 2006.
Royal College of Obstetricians and Gynaecologists. Vaginal breech delivery. Green-top Guideline No. 20b. London: RCOG; 2006.
Whyte H, Hannah M, Saigal S. Term BreechTrial Collaborative Group. Outcomes of children at 2 years of age in the Term Breech Trial. Am J Obstet Gynecol 2003; 189: S57. Internet resources
Breech presentation: www.patient.co.uk/showdoc/40000237/ Patient resources
Turning a breech in your womb (external cephalic version): Information for you: www.rcog.org.uk/resources/public/pdf/PITurningECV0208.pdf.
A breech Baby at the end of pregnancy: information for you: www.rcog.org.uk/resources/public/pdf/PIBreechBaby0208.pdf.
Brow presentation Definition
A rare malpresentation in which the area between the orbital ridges (inferiorly) and bregma (superiorly), becomes the presenting part. This is due to deflexion (i.e. partial extension) of the fetal neck, which results in the largest diameter of the fetal skull, the mentovertical diameter (13.5 cm) to be the engaging diameter. Hence, there is no mechanism of labour in persistent brow presentation as the mentovertical diameter is larger than all the diameters of the bony pelvis. The denominator for brow presentation is the forehead (frontum). Epidemiology
It is difficult to estimate the true incidence of brow presentation as the vast majority change into face or vertex presentations during labour. Reported incidence varies from 1 in 3000–1 in 500 (0.03–0.5%). Predisposing factors are similar to face presentation and include multiparity, cephalopelvic disproportion (CPD), uterine malformation, abnormalities in amniotic fluid volume (polyhydramnios or oligohydramnios). Conditions that cause deflexion of the fetal head such as congenital goitre or branchocoele, multiple cord round the fetal neck (‘nuchal cord’) and rarely musculoskeletal abnormalities that cause spasm (or shortening or contracture) of the muscles of the extensor compartment of the neck may also predispose to brow presentation. Mechanism of labour
Brow presentation may undergo further flexion to become a vertex presentation or further extension to become a face presentation. Prerequisites for such favourable outcomes are roomy pelvis, average size fetus, and strong and effective uterine contractions. Absence of favourable factors results in a persistent brow presentation. There can be no mechanism of labour because the mentovertical diameter (13.5 cm) is larger than the dimensions of the pelvis and hence, there can be no progress of labour. Prompt diagnosis and timely Caesarean section is necessary to improve maternal and perinatal outcome. Rarely, if the fetus is preterm or macerated, vaginal birth may still be possible with persistent brow presentation. Clinical approach
Diagnosis of a brow presentation may be difficult prior to the onset of labour. The presence of a high (non-engaged) head at term and prominent occiput should alert the clinician. As in face presentation, there is a groove between the occiput and the fetal back. However, unlike the face presentation where the entire fetal head is felt at the same side as the fetal spine due to extension, the head is felt on both sides of the fetal spine due to deflexion (partial extension). An ultrasound scan may be performed antenatally or during labour to help diagnose or exclude abnormalities of amniotic fluid (oligo- or polyhydramnios), placenta praevia, congenital abnormalities (anencephaly, branchocoele, fetal goitre). Doppler examination may be helpful when nuchal cord is suspected.
On vaginal examination during labour, the root of the nose, orbital ridges, frontal sutures, and anterior fontanelle can be palpated. Unlike the face presentation, the mouth and chin cannot be felt on vaginal examination. Management
Brow presentation should be clinically suspected in any multipara with a non-engaged head at term or in early labour. Owing to ‘ill-fitting’ presenting part, membranes may herniate and rupture early leading to increased risk of cord prolapse. Hence, the patient should be counselled about this possibility and advised to attend early in labour if brow presentation is suspected or diagnosed antenatally. Sometimes, persistent decelerations on a cardiotocograph, despite of a high fetal head may arouse clinical suspicion of brow presentation. This is because repeated pressure on the eyeballs during contractions may stimulate parasympathetic nervous system, leading to decelerations of the fetal heart rate.
During early labour, in the absence of unfavourable factors that have been discussed earlier, vaginal delivery can be anticipated, especially if CPD and fetal macrosomia have been excluded. Optimum uterine contractions may change brow presentation into a face presentation (extension) or vertex presentation (flexion). However, up to 33–50% of brow presentations may present with secondary arrest or failure to progress, despite adequate contractions. Emergency Caesarean section is the safest mode of delivery in such cases. In cases of preterm infants (i.e. very small) and a roomy pelvis in the presence of good uterine contractions and anterior brow presentation, vaginal delivery may be possible. Similar to mentoposterior face presentation, there is no mechanism of labour in posterior brow presentation. During Caesarean section, care should be taken to flex the fetal head prior to delivering through the uterine incision to avoid extension of the incision at the uterine angles. As in face presentation, atonic or traumatic postpartum haemorrhage may occur following delivery and these should be anticipated and managed appropriately. Further reading
Bashiri A, Burstein E, Bar-David J, Levy A, Mazor M. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med2008;21:357–60.
Chandraharan E, Arulkumaran S. Operative delivery, shoulder dystocia and episiotomy. In: Arulkumaran S, Penna LK, Bhasker Rao K (eds) The management of labour, 2nd edn. Orient Longman 2005.
Stitely ML, Gherman RB. Labor with abnormal presentation and position. Obstet Gynecol Clin N Am 2005;32:165–79.
Cord prolapse Definition
Cord prolapse (or prolapse of the umbilical cord) occurs when a loop of umbilical cord lies below the presenting part and the membranes have ruptured. Cord presentation refers to the presence of a loop of cord below the presenting part when the membranes are intact. Occult cord prolapse is said to occur when a loop of umbilical cord lies alongside the presenting part. Epidemiology
It has been estimated that overall, cord prolapse occurs in 1 in 3000 deliveries. However, the incidence of cord prolapse is believed to vary with the nature of the presenting part and the lie of the fetus. The incidence is estimated to be 0.5% with cephalic and frank breech presentations; 5% with complete breech; 15% with footling breech presentations; and 20% with transverse lie. It is difficult to estimate the exact incidence of occult cord prolapse. Variable decelerations on the cardiotocograph suggest cord compression and are known to occur in over 50% of established labour. These are often transitory and often disappear with changes in the maternal position. Hence, it would appear that occult cord prolapse is quite common during labour and often goes undiagnosed. Risk factors
• Unstable lie (transverse lie)/malpresentation such as breech (especially a footling breech)
• Polyhydramnios
• Prelabour rupture of membranes, especially in preterm pregnancies
• Twins and higher order multiple pregnancy
• High presenting part in labour (e.g. true or relative cephalopelvic disproportion or CPD, placenta praevia and rarely fibroids in the lower segment of the uterus)
• Obstetric interventions: artificial rupture of membranes (ARM), fetal blood sampling (FBS), or application of a scalp electrode or pulse oximeter when the presenting part is high
• Multiparity (predisposes to abnormal lie and malpresentations)
• Long umbilical cord (rare). Pathophysiology
Prolapse of the umbilical cord may result in two detrimental processes that may reduce the oxygen supply to the fetus. First, there may be a mechanical effect due to the compression of the umbilical cord between the presenting part (head, breech) and the maternal birth passage. Second, there may be a physiological effect of umbilical cord spasm, as the fetal blood vessels (umbilical arteries and vein) are exposed to the cold air. Both these processes would threaten to reduce the blood supply from the placenta to the fetus, resulting in acute fetal hypoxia. Degree of fetal hypoxia and the resultant neurological damage (risks of cerebral palsy, long-term neurological sequelae, and neonatal death) would depend on the degree of cord compression, placental reserve, ability of the fetus to withstand the acute hypoxic stress (preterm, post-term, and growth-restricted fetuses may not effectively cope with hypoxia), and the time interval between cord prolapse and delivery. Diagnosis
• In frank or overt cases of cord prolapse, the umbilical cord can be seen protruding from the introitus or loops of cord can be seen or palpated within the vagina during a vaginal examination.
• Occult cord prolapse is often suspected based on abnormalities of the fetal heart rate (repeated variable decelerations) seen on a cardiotocograph (CTG). Rarely the umbilical cord may be felt beside (not below) the presenting part on vaginal examination.
• Cord presentation may be diagnosed when loops of cord are palpated through an intact membrane.
• Ultrasound examination (especially colour Doppler) may help identify a loop of cord below the presenting part and hence, may help in the diagnosis of cord presentation prior the onset of labour. This is not routinely used in clinical practice as it has poor sensitivity and specificity. However, is selected cases such as polyhydramnios and vasa praevia (insertion of the umbilical cord on to the fetal membranes that results in cord vessels traversing fetal membranes below the presenting part), Doppler may be a useful tool. Management
Cord prolapse is an acute obstetric emergency and is considered to be a sentinel hypoxic event during labour. Delay in delivery would increase the chances of hypoxic injury to the fetus and worsen the outcome. Principles of management involves a rapid assessment of fetal viability (Pinard’s fetoscope, Dopplertone, ultrasound examination to confirm fetal heart activity) and immediate delivery by the safest and most appropriate method. If the fetus is viable, institute measures to avoid further cord compression to improve oxygenation until delivery. Neonatal resuscitation is an important aspect of management as there is a likelihood that the neonate would be born in a poor (asphyxiated) condition.
• If the fetus is dead at the time of diagnosis of cord prolapse or on admission (e.g. transfer from home or another unit with cord prolapse), then no further intervention is needed. The woman and her partner should be informed and sympathies expressed. Labour should be allowed to progress, anticipating a vaginal birth unless there is a maternal indication (transverse lie or major degree placenta praevia) that necessitates a Caesarean section.
• If the fetus is viable (i.e. fetal heart rate is present), the safest and most appropriate mode of delivery should be contemplated with a view to deliver the fetus within the shortest possible time. This would necessitate an immediate vaginal examination to assess the dilatation of the cervix and the station of the presenting part.
• In the first stage of labour (i.e. cervix is not fully dilated) or if the cervix is fully dilated, but the presenting part is high (above the ischial spines) an immediate (Category 1) Caesarean section should be performed. However, prior to the operative procedure, the clinical situation may be reassessed by performing a vaginal examination, as some labours progress rapidly (e.g. multigravida with 9 cm or fully dilated cervix with the vertex below spines). In such situations the safest and quickest option may be an assisted vaginal delivery.
• In the second stage of labour (i.e. fully dilated cervix and presenting part below the spines) an instrumental delivery (ventouse or forceps) could be attempted as this is likely to be the safest and most expedient mode of delivery. However, difficult rotational deliveries are best avoided, especially in the presence of fetal heart rate abnormalities associated with cord prolapse as birth trauma may compound the detrimental effects of hypoxia, leading to an unfavourable outcome.
• Immediate (Category 1) Caesarean section should be carried out in cases of cord prolapse occurring with an abnormal lie (e.g. transverse lie) or breech presentation. In cases of cord prolapse of the second twin (after the birth of first twin) a breech extraction may be attempted as this is likely to be the safest and most expedient method in this situation.
Measures to improve fetal outcome prior to delivery
Measures to improve oxygenation to the fetus include reducing the chances of vasospasm, relieving cord compression, and reducing the intensity and frequency of uterine contraction to allow for ‘intrauterine resuscitation’.
• Reduce the chance of vasospasm by gently replacing the cord within the vagina and retaining it inside the vagina with a warm saline pack. This is likely to reduce the exposure to cold air that triggers the spasm of the cord vessels. However, excessive handling of the cord itself may trigger a spasm.
• Relieve cord compression by placing the patient in an exaggerated Simms position with the hips and buttocks elevated by a wedge or pillow. This is likely to mobilize the presenting part away from the cord due to the effect of gravity. The foot-end of the bed could be elevated to achieve the same results.
• The clinician who diagnosed cord prolapse could insert two fingers into the vagina in order to push up the presenting part during contractions. This may be useful when cord prolapse is diagnosed in a ‘home birth’ situation while awaiting additional help to transport the patient to the hospital.
• Urinary bladder could be catheterized with a 16G Foley catheter and approximately 500 mL of normal saline be instilled into the bladder via a standard giving set. The balloon is then inflated and the catheter clamped. A ‘full bladder’ displaces the presenting part upwards, thus relieving the pressure on the umbilical cord. This method eliminates the need for the examiner’s fingers to displace the presenting part. However, the clamp should be removed prior to Caesarean section to avoid inadvertent bladder injury.
• Acute tocolysis (Terbutaline 0.25 mg subcutaneously) may be attempted to abolish uterine contractions. This is likely to improve uteroplacental blood flow and, hence, fetal oxygenation.
Anticipation and prevention of cord prolapse
• Cord prolapse should be anticipated in the presence of risk factors and measures should be taken to minimize its occurrence. In the presence of polyhydramnios, a controlled artificial rupture of membranes (ARM) should be attempted. A ‘stabilizing induction’ may allow the presenting part to fit in snugly within the pelvis at the time of rupture of membranes and thereby reduce the space available for cord prolapse.
• Early diagnosis of cord prolapse is likely to improve the outcome. Vaginal examination should be performed in the presence of repeated variable decelerations, especially after ARM, application of fetal scalp electrode or fetal blood sampling as the displacement of the presenting part during these procedures may predispose to cord prolapse.
Risk management issues
It is important to explain the events and the possible causes to the patient and her partner and this discussion should be clearly documented in the notes. Cord blood gases (arterial and venous pH, base excess, PO2, and PCO2) should be determined and documented. An incident report form should be completed and regular audit of Category 1 Caesarean sections should be carried out to determine whether the ‘decision-to-delivery’ interval standards are met. Further reading
Chamberlein G, Steer P. ABC of labour care: unusual presentations and positions and multiple pregnancy. BMJ 1999;318:1192–4.
Chandraharan E, Arulkumaran S. Acute tocolysis: Review Article. Curr Opin Obstet Gynecol 2003;17:151–6.
Chandraharan E, Arulkumaran S. Prevention of birth asphyxia: responding appropriately to cardiotocograph (CTG) traces. Best Pract Res Clin Obstet Gynaecol 2007;21:609–24.
Critchlow CW, Leet TL, Benedetti TJ, Daling JR. Risk factors and infant outcomes associated with umbilical cord prolapse: A population-based case control study among births in Washington state. Am J Obstet Gynecol 1994;170:613–8.
Katz Z. Management of labour with umbilical cord prolapse: a 5 year study. Obstet Gynaecol 1998;72:278–81.
Murphy DJ, MacKenzie IZ. The mortality and morbidity associated with umbilical cord prolapse. Br J Obstet Gynaecol 1995;102:826–30.
Prabulos AM, Philipson EH. Umbilical cord Prolapse; so far so good. J Reprod Med 1998;43:129–32.
Episiotomy and obstetric perineal trauma Definition
Perineal trauma may occur spontaneously during vaginal birth or intentionally when a surgical incision (episiotomy) is made to facilitate delivery.
Perineal trauma is classified as follows:
• first degree: laceration of the vaginal epithelium or perineal skin only
• second degree: involvement of the perineal muscles (bulbocavernosus, transverse perineal) but not the anal sphincter
• third degree: disruption of the anal sphincter muscles which should be further subdivided into 3a, 50% thickness of external sphincter torn; 3c, internal sphincter also torn
• fourth degree: a third degree tear with disruption of the anal epithelium as well.
Episiotomy is a surgical incision made with scissors or a scalpel into the perineum in order to increase the diameter of the vulval outlet and facilitate delivery.
There are two main types of episiotomy incision:
• a midline episiotomy is an incision from the midpoint of the posterior fourchette directed vertically towards the anus
• a mediolateral episiotomy is an incision from the midpoint of the posterior fourchette directed 40 to 60 degrees away from the midline. Incidence
Perineal trauma is dependent on variations in obstetric practice including rates and types of episiotomies, which not only vary between countries but also between individual practitioners within hospitals.
• In the UK approximately 85% of women sustain some form of perineal trauma during vaginal delivery and of these 69% will require stitches
• In centres where mediolateral episiotomies are practised, the rate of obstetric anal sphincter injuries (OASIS) occurs in 1.7% compared to 12% in centres practising midline episiotomy. Indications for episiotomy
• To accelerate vaginal delivery in cases of fetal distress.
• Reduce the occurrence of multiple lacerations in the presence of a thick or rigid perineum.
• To facilitate manoeuvres during shoulder dystocia.
• To minimize severe perineal trauma during a forceps delivery.
• In situations where prolonged ‘bearing down’ maybe harmful for the mother (e.g. severe hypertensive or cardiac disease). Management and repair of perineal trauma
Ensure that the wound is adequately anaesthetized prior to commencing the repair with 10–20 mL of lignocaine 1% injected evenly into the perineal wound. If the woman has an epidural it may be ‘topped-up’ and used to block perineal pain during suturing instead of injecting local anaesthetic. Repair of obstetric anal sphincter trauma should be undertaken in theatre, under general or regional anaesthesia.
First-degree tears and labial lacerations
Women should be advised that in the case of first-degree trauma, the wound should be sutured in order to improve healing, unless the skin edges are well opposed.
Episiotomy and second-degree tears
Perineal trauma should be repaired using the continuous non-locking technique to reapproximate all layers (vagina, perineal muscles, and skin) with absorbable polyglactin 910 material (Vicryl rapide).
The steps in Fig. 10.5.1 should be followed
• The first stitch is inserted above the apex of the vaginal laceration and the vaginal wound is closed with a loose, continuous, non-locking technique down to the hymenal remnants. Insert the needle through the skin at the four-chette to emerge in the centre of the perineal wound.
• Check the depth of the trauma and close the perineal muscle (deep and superficial) with continuous non-locking stitches.
• At the inferior end of the wound, bring the needle out just under the skin surface reversing the stitching direction. Continue to take bites of tissue from each side of the wound edges until the hymenal remnants are reached. Secure the finished repair with a loop or Aberdeen knot placed in the vagina behind the hymenal remnants. Third- and fourth-degree tears
• Intraoperative antibiotics should be administered.
• In the presence of a fourth-degree tear, the torn anal epithelium is repaired with interrupted Vicryl 3/0 sutures with the knots tied in the anal lumen.
• The internal anal sphincter should be identified and if torn, repaired separately from the external anal sphincter. The ends of the torn muscle are grasped with Allis forceps and an end-to-end repair is performed with interrupted sutures (3-0 PDS (Polydioxanone) or 2-0 Vicryl (polyglactin-Vicryl)).
• The torn ends of the EAS therefore need to be identified and grasped with Allis tissue forceps. When the EAS is only partially torn (Grade 3a and some 3b) then an end-to-end repair should be performed using two or three mattress sutures. If there is a full thickness EAS tear (some 3b, 3c, or fourth degree), either an overlapping or end-to-end method can be used with equivalent outcome, although in experienced hands superior results have been reported with the overlap technique.
• The perineal muscles should be sutured to reconstruct the perineal body in order to provide support to the repaired anal sphincter.
• Finally, the vaginal skin should be sutured and the perineal skin approximated with a Vicryl 2-0 subcuticular suture. Basic principles after repair of perineal tears
• Check that complete haemostasis is achieved and confirm that the finished repair is anatomically correct.
• A rectal and vaginal examination should be performed to confirm adequate repair so as to ensure that no other tears have been missed and that a suture is not inadvertently placed through the rectal mucosa. Confirm that all tampons or swabs have been removed.
• Detailed notes should be made of the findings and repair. Postoperative care
• The use of broad-spectrum antibiotics and laxatives is recommended following third- and fourth-degree tears
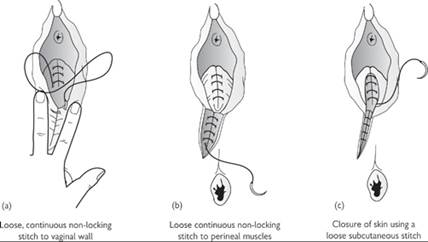
Fig. 10.5.1 Continuous suturing technique for mediolateral episiotomy. Sultan AH, Thakar R. Repair of episiotomy, first and second degree tears. In Sulatn AH, Thakar R, Fenner D (eds) Perineal and anal sphincter trauma (2009); 20–32. With kind permission of Springer Science Business and Media.
• All women who have had obstetric anal sphincter repair should be reviewed 6–12 weeks postpartum by a senior clinician. Further reading
Carroli G, Belizan J. Episiotomy for vaginal birth. Cochrane Database Syst Rev 1999; 3: CD00081.
Intrapartum Care. NICE Clinical Guideline. Guideline 55 2007 Available from: URL: www.nice.org.uk/CG055
Kettle C, Hills RK, Ismail KM. Continuous versus interrupted sutures for repair of episiotomy or second degree tears. Cochrane Database Syst Rev 2007; 4: CD000947
Sultan AH, Thakar R, Fenner D (eds). Perineal and anal sphincter trauma. London: Springer 2007
Henderson C, Bick D (eds). Perineal care: an international issue. Wiltshire: Quay Books 2005
Royal College of Obstetricians and Gynaecologists. Management of third and fourth degree perineal tears following vaginal delivery. Guideline No 29. London, RCOG Press 2007.
Royal College of Obstetricians and Gynaecologists. Methods and materials used in perineal repair. Guideline No. 23. London: RCOG press 2004.
Sultan AH, Thakar R. Third and fourth degree tears. In: Sultan AH, Thakar R, Fenner D (eds) Perineal and anal sphincter trauma. London: Springer-Verlag 2007: 33–51. Internet resources
www.perineum.net
www.patient.co.uk/showdoc/40000277
Face presentation Definition
A malpresentation in which the presenting part is the face bounded superiorly by orbital ridges (glabella), laterally by the malar eminences and inferiorly by the chin (or mentum). The head is hyperextended and the chin forms the denominator with submentobregmatic diameter as the presenting diameter. Epidemiology
Overall incidence of face presentation is approximately 1 in 500 births (0.5%). Incidence increases in the presence of fetal congenital malformations (15%) such as iniencephaly or dolichocephalic head. Anencephaly is associated with an increased incidence of face presentation (30%) because of the absence of vault of the fetal skull. Other predisposing factors include multiparity, cephalopelvic disproportion (CPD), uterine malformation, and abnormalities in amniotic fluid volume (polyhydramnios or oligohydramnios). Any condition that causes hyperextension of the fetal neck is likely to predispose to face presentation. These include congenital goitre or branchocoele, multiple cord round the fetal neck (‘nuchal cord’), and rarely musculoskeletal abnormalities that cause spasm (or shortening or contracture) of the muscles of the extensor compartment of the neck. Primary and secondary face presentation refers to diagnosis of face presentation during the antenatal period and labour, respectively. Mechanism of labour
Mentum or chin is the denominator in face presentation. And the engaging diameter is submentobregmatic, which is similar to the biparietal diameter in vertex presentation (9.5 cm). When chin is anterior (i.e. in relation to the iliopectineal eminence), it is termed left or right mentoanterior (LMA or RMA) position. Similarly, if the mentum is posterior (i.e. in relation to the sacroiliac joints) it is termed left or right mentoposterior (LMP or RMP) positions. If the chin is along the transverse diameter of the pelvis, it is termed mentolateral (ML) or mentotransverse (MT).
The largest diameter of the skull (biparietal diameter or BPD) is about 7 cm behind the advancing face presentation during labour. This means that the BPD engages only when the face is at +2 or +3 station (i.e. almost crowning the vulva). Failure to appreciate this anatomical fact may lead to increased perinatal and maternal morbidity due to earlier intervention to expedite vaginal delivery when the largest diameter is still above the pelvic brim.
The majority of face presentations occur during labour, secondary to extension of a brow presentation, in the presence of strong and effective uterine contractions in the presence of an adequate pelvis. Mentoanterior positions are delivered by flexion. Mentoposterior positions (LMP, RMP, or direct) behave similar to occipitoposterior positions (OP) and hence, need to undergo a long anterior rotation (three-eighths of a circle) during labour, prior to delivery. The chance of a successful long rotation is only about 45–65% during the second stage of labour. Failure of this long anterior rotation makes further progress of labour impossible in mentoposterior positions (except in cases of extreme prematurity or macerated fetus).
• In mentoposterior positions, delivery should occur by extension. However, the head is already maximally extended and hence, further extension is not possible.
• As the length of the sacrum is about 10–12 cm and that of neck is only 5 cm, the shoulders enter the pelvis and become impacted while the head is still in the pelvis, thus the labour is obstructed. Entry of the thorax into the pelvis makes it difficult for the sternobregmatic diameter (18 cm) to enter the pelvis. Clinical approach
Primary face presentation is diagnosed prior to the onset of labour. On abdominal palpation, the cephalic prominence is on the same side as the fetal back, with a ‘groove’ separating the occiput from the spine. The occiput is above the level of the sinciput. If face presentation is suspected on clinical examination prior to the onset of labour it may be confirmed by ultrasound examination. Intervention is not necessary because, in the absence of any predisposing factors such as nuchal cord or congenital goitre, the majority of these would revert to vertex presentation during labour. It is reasonable to expect that effective uterine contractions during labour in the presence of an adequate, roomy pelvis may aid conversion of the face presentation to a more favourable vertex presentation.
Secondary face presentation is diagnosed during labour. Abdominal examination may reveal the above findings. However, vaginal examination is more reliable. Orbital ridges, malar eminences, and the mouth can be felt. Clinically, face presentation can be differentiated from breech presentation as the mouth and malar eminences on either side form three angles (or apices) of a triangle. In contrast, the anal orifice and ischial tuberosities on either side are on a straight line in breech presentation. Also, inserting the tip of the finger into the mouth enables the palpation of hard gums and may stimulate fetal sucking. In breech presentation, if the tip of examiner’s finger is inadvertently introduced into the anus, a ‘gripping’ action of the anal sphincter may be elicited. Sometimes it may be difficult to palpate the mouth and malar eminences due to gross oedema of the face (called ‘tumefaction’), which is similar to ‘caput’ in a vertex presentation. In this situation, the eyeballs, nose, and lips are swollen.
Role of ultrasound
In modern obstetric practice, an ultrasound scan can be performed antenatally or during labour to confirm face presentation. Ultrasonography can also help diagnose or exclude abnormalities of amniotic fluid (oligo- or polyhydramnios), placenta praevia, and congenital abnormalities (anaencephaly, branchocele, fetal goitre). Doppler examination may be helpful when nuchal cord is suspected. Management
An elective Caesarean section should be offered if there is clinical evidence of contracted pelvis (i.e. true CPD), if the ultrasound scan identifies any predisposing factor that may preclude a vaginal delivery, or if there are any absolute contraindication for vaginal delivery (major degree placenta praevia). In all other cases, after careful counselling, a vaginal birth may be attempted with careful monitoring of the fetal heart rate as well as progress of labour. The presence of strong, effective uterine contractions is essential for progress of labour and for successful internal rotation. Hence, judicious use of oxytocin to achieve effective uterine contractions is not contraindicated.
Overall, the success rate of vaginal delivery for face presentation is about 60–70% and about 10–20% require an emergency Caesarean section during labour.
Mentoanterior face presentation
Approximately 60–70% of fetuses with face presentation have mentoanterior position and approximately 90% of these will achieve a vaginal birth. Labour may be prolonged compared with vertex presentation because the face is a poor dilator of the cervix compared with the occiput. An episiotomy may be indicated to avoid perineal tears and gain adequate access. Prolonged second stage of labour (or fetal distress in the second stage) may warrant a forceps delivery (ventouse or vacuum delivery is contraindicated in face presentation), if CPD has been excluded. The operator should understand the anatomy prior to application of the forceps blades. The mouth (face presentation) substitutes for the posterior fontanelle (vertex presentation), whereas the chin or mentum (face presentation) substitutes for the occiput (vertex presentation). The direction of traction should be downward initially to maintain extension until the chin passes under the symphysis. The direction of traction should then be gradually changed (i.e. forceps handle elevated) to allow the delivery of the fetal head by flexion. Utmost care must be taken to avoid hyperextension of the fetal head during delivery, as this can result in injury to cervical spine.
Mentolateral (ML) or mentotransverse (MT) position
Ten to 12% of fetuses with face presentation have a mentotransverse position. If rotation to the mentoanterior position does not occur during labour, an emergency Caesarean section is indicated. This is because deep transverse arrest is common and there may not be further progress of labour. Manual rotation to the mentoanterior position under a general anaesthetic and forceps delivery (Thorn’s manoeuvre) and rotation with Kielland’s forceps have been described. However, these are likely to have a limited role in modern obstetric practice.
Mentoposterior (MP) position
20–25% of fetuses with face presentation have a mentoposterior position during labour. With strong uterine contractions and adequate pelvis, 45–65% of these will rotate to a mentoanterior position. Persistent mentoposterior despite strong and effective uterine contractions and an adequate pelvis is an indication for an emergency Caesarean section. As mentioned earlier, the mechanism of labour is not possible due to anatomical factors. However, in early labour, a conservative approach is entirely acceptable if the fetal heart rate is normal and true CPD is excluded. In such cases, judicious use of oxytocin can be used to achieve optimum uterine contractions, sufficient to achieve internal rotation to the mentoanterior position. It is wise to perform a Caesarean section if there is lack of progress for 3–4 hours despite good contractions with oxytocin infusion. Manual rotation and Kielland’s rotation have been described but these are associated with perinatal and maternal morbidity, especially in inexperienced hands. In modern obstetric practice, a Caesarean section is the preferred option for persistent mentoposterior face presentation.
Delivery during Caesarean section
A Caesarean section should be performed or supervised by an experienced obstetrician. Flexion of the head should be attempted prior to delivery through the uterine incision. Uterine angles should be carefully inspected to exclude angular extensions. Postpartum complications
These include complications because of prolonged labour and genital tract trauma, both of which may result in post-partum haemorrhage. The neonate may have laryngeal oedema as an extension of facial oedema (‘tumefaction’) and may need resuscitation after birth. The neonate should also be examined to exclude injury to the cervical spine, especially if hyperextension during delivery was suspected. Parents should be reassured that the facial oedema, which is cosmetically very unappealing, will settle with time. Further reading
Chandraharan E, Arulkumaran S. Operative delivery, shoulder dystocia and episiotomy. Chapter In: Arulkumaran S, Penna LK, Bhasker Rao K (eds) The management of labour, 2nd edn. Orient Longman 2005.
Gee H. Malpresentation and malposition. In: James DK, Mahomed K, Stone P, Wijngaarden, Hill LM (eds) Evidence-based obstetrics. Saunders 2003.
Nassar AH, Fayyumy R, Saab W, et al. Grandmultiparas in modern obstetrics. Am J Perinatol 2006;23:345–9.
Sahid S, Sepulvida W, Dezerega W. Iniencephaly: prenatal diagnosis and management. Prenat Diagn 2000;20:202–5.
Vialle R, Pietin-Vialle C, Ilharrebode B. Spinal cord injuries at birth: a multicenter review of nine cases. J Matern Fetal Neonatal Med 2007;20:435–40.
Fetal surveillance in labour Definition
Fetal surveillance is recommended in labour with the intention of detecting fetal hypoxia prior to the development of asphyxial damage in the fetus. The ideal fetal surveillance would have a high sensitivity (detect all fetuses with developing hypoxia) and a high specificity (be reassuring about all fetuses with no hypoxia). The test should also be easy to perform, not interfere with labour progress, and have a high acceptability to women. Unfortunately the ideal monitoring technique does not currently exist.
Currently available diagnostic tests include
• fetal blood sampling (FBS) for pH and base-excess
• FBS for lactate (this is less well validated than pH and is less widely used but requires a small sample of fetal blood)
• neonatal assessment after delivery (Apgar scores, cord blood pH, neonatal outcome).
As the available diagnostic tests are expensive and invasive they are used selectively. Therefore, routine fetal surveillance in labour aims to identify a group of fetuses with a high chance of developing hypoxia so that a diagnostic test can be used.
Currently available screening tests
Universal
• Maternal history: to assess for risk factors
• Observation of amniotic fluid for meconium
• Intermittent auscultation (IA)
In women with a low-risk that their fetus will develop hypoxia, evidence shows that routine use of continuous fetal monitoring increases the rate of intervention in labour (assisted vaginal delivery and Caesarean section) with no improvement in neonatal morbidity and mortality when compared with intermittent auscultation. Any abnormality detected in any of these screening tests requires that a higher level of screening be implemented.
Selective
• Continuous electronic fetal monitoring using a cardiotocograph (CTG).
• Analysis of the ST segment of the fetal ECG (STAN) used in combination with the CTG. Epidemiology
Abnormalities of the fetal heart rate are very common; 75% of cardiotocographs will show at least one abnormality during labour and almost 1 in 5 will show a serious abnormality. 1 in 10 CTGs show recurrent decelerations and more than 1 in 20 fetuses will have a period of prolonged deceleration during labour. A true hypoxic event occurs in only 3/1000 labours so most observed CTG abnormalities are false positives. Unfortunately, some CTGs are misdiagnosed or are false negatives (falsely reassuring) as intrapartum deaths occur (0.75/1000 births) in the UK and neonates exhibit clinical features of ischaemic brain injury (hypoxic ischaemic encephalopathy) in 2.25/1000 neonates (ischaemic injury can occur due to other causes).
Worldwide, the World Health Organization has estimated that 1 million infants die each year as a result of birth asphyxia with about the same number surviving with long-term neurological disability. Pathology
• Hypoxaemia describes a common situation where there is a reduction in placental or cord blood flow causing a reduction in the level of oxygen in the peripheral arterial circulation of the fetus. This occurs as a normal part of labour as uterine contractions reduce blood flow to the placenta. Fetuses are able to cope with hypoxaemia for relatively long periods of time without injury occurring. Fetal growth and activity reduces but the oxygen delivery to tissues is maintained and so no metabolic acidosis develops. Hypoxaemia due to cord compression is also associated with an increase in carbon dioxide levels and the appearance of respiratory acidosis.
• Hypoxia describes the situation where the blood flow is interrupted for more prolonged periods and as a result there is a reduction in the delivery of oxygen to the peripheral tissues The fetus may show some stress response (such as a developing tachycardia) but there are mechanisms to allow this situation to occur for short periods of time (hours) without fetal damage. The fetus must switch to anaerobic metabolism to create energy from glucose and stored glycogen. The byproduct of this process is lactic acid and thus a metabolic acidosis develops. Buffering will allow a normal pH to be maintained for a period of time. Some fetuses have lower reserves of glycogen and/or a lower ability to buffer if metabolic acidosis occurs (preterm, infants of diabetic mother, growth restricted fetuses).
• Asphyxia describes the situation where the oxygen delivery fails to such an extent that there is reduction in oxygen delivery leading to metabolic acidosis in the tissues due to anaerobic metabolism in addition to hypoxia. This causes critical organ damage with fetal demise in utero or damage. Neonates who have been asphyxiated suffer multi-organ failure after delivery with a high risk of mortality. Asphyxial injury to the brain results in hypoxic ischaemic encephalopathy (HIE). The severity of the injury is variable but there is a significant risk of cerebral palsy in survivors of a severe asphyxial episode.
• Fetal infection reduces the reserve to cope with hypoxia and certain fetal heart rate changes may occur in the presence of significant fetal infection.
• Fetal anaemia either acute (due to fetomaternal haemorrhage) or chronic (due to parvovirus or red-cell immunization) causes the characteristic findings of a sinusoidal pattern on a cardiotocograph. A fetus with anaemia is at greater risk of hypoxia and also has a very reduced reserve to cope with hypoxia as haemoglobin acts as a buffer in metabolic acidosis.
Aetiology
• Acute hypoxia occurs as a result of sudden reduction in placental/cord blood flow and develops rapidly over minutes. Most causes are irreversible once the process begins. Management requires rapid delivery or reversal of the acute insult in cases of hyperstimulation, if the fetus is viable, to prevent death or damage:
• uterine dehiscence
• cord prolapse (with cord spasm or compression)
• critical cord compression (e.g. the cord along side the fetal head as it descends in the second stage)
• significant abruption with detachment of a large area of the placenta or due to uterine hypertonia
• hypertonic uterine contractions secondary to the administration of prostaglandins or oxytocin.
• Chronic hypoxia occurs due to a reduction in the placental blood flow over a long period. It can occur in any condition where there is placental vascular disease. The common examples are fetal growth restriction and recurrent antepartum haemorrhages. The fetus will cope with this for a significant period of time by redistributing blood to vital organs, reducing growth and activity, and by buffering against the lactic acid formed during low levels of anaerobic metabolism. However, the point can be reached where the disease process worsens or the ability to buffer is exhausted and lactic acidosis develops. Surveillance with fetal Dopplers in the antenatal period helps to detect the point where decompensation becomes likely so that delivery can be recommended in the fetus that is viable. This will allow the diagnosis of chronic hypoxia prior to the onset of labour in most cases. A fetus with chronic hypoxia will not cope with the reduction in placental blood flow that occurs during labour and fetal heart rate abnormalities are seen. A reduction in variability in the trace of any fetus at the onset of labour may be ominous if it does not improve with time, and there is a risk of poor outcome, as it suggests a significant degree of metabolic acidosis and a failure of compensatory mechanisms.
• Gradually developing hypoxia is the most common type of intrapartum hypoxia. Early recognition that the fetus may be at risk of developing hypoxia allows interventions aimed at improving the fetal condition. This type of hypoxia develops in labour as a result of recurrent cord compression. Cord compression occurs to some degree in all labours but is worsened by a number of clinical situations:
• strong contractions (e.g. in the second stage or during administration of oxytocin)
• oligohydramnios (e.g. following ruptured membranes or in post-term pregnancy)
• cord around the neck in the first or the second stage Prognosis
Prolonged reduction in oxygenated cerebral blood flow due to any cause can result in an acute brain injury with the clinical features of hypoxic ischaemic encephalogathy (HIE). Asphyxial birth injury due to hypoxia during labour is only one cause of HIE. The severity of the injury is related to the length of time of hypoxia but certain fetuses may also be more susceptible to injury due to less fetal reserve (such as in fetal growth restriction).
The mortality from severe HIE is 50–75% with over half of the deaths occurring in the first week of life. Of infants who survive with a diagnosis of severe HIE, 80% will have severe complications, 10–20% will have mild or moderate complications, and up to10% will develop normally. In infants surviving with moderate HIE there is a 30–50% chance of serious long-term complications and 10–20% risk of minor complications, with 30–70% of infants developing normally. The infants with mild HIE invariably develop normally with no complications. The sequelae of HIE include mental retardation, epilepsy, and cerebral palsy. Clinical approach
Decide what surveillance should be recommended
Risk assessment
• The antenatal and intrapartum history must be assessed for all women in labour to allow appropriate monitoring to be recommended. The presence of risk factors for pathologies that may increase the risk of fetal hypoxia should be considered:
• increased risk of cord compression: breech, oligohydramnios, strong contractions due to syntocinon or induction of labour
• reduced retroplacental pool of blood as in cases of suspected fetal growth restriction, pre-eclampsia, diabetics, antepartum or intrapartum haemorrhage, severe maternal disease
• reduced fetal reserve; prematurity, fetal infection, fetal anaemia, multiple pregnancy, growth restriction
• increased risk of severe acute hypoxic event, e.g. scar rupture during vaginal birth after Caesarean section
• at times monitoring is needed for maternal reassurance: previous stillbirth or other poor pregnancy outcome may result in a maternal desire for the fetus to be monitored as closely as possible.
Meconium
• If the membranes have ruptured then the liquor can be assessed for the presence of meconium. The presence of meconium has an independent association with poor fetal outcome and therefore if present it necessitates a review of the recommendations for fetal surveillance.
Recommend appropriate monitoring
Intermittent auscultation
• If the woman has no risk factors (low risk) and there is no meconium then intermittent auscultation should be recommended. If this is acceptable to the woman it is recommended that the operator listen for one minute soon after a contraction using a pinnard stethoscope or a hand-held Doppler machine. This should be done every 15 minutes in the first stage of labour and every 5 minutes in the second stage of labour. Continuous electronic fetal monitoring should be commenced if any of the following occur:
• a baseline abnormality
• any audible deceleration (variable or late)
• new meconium staining of the liquor is observed
• a new risk factor develops during the course of labour (such as oxytocin therapy or intrapartum haemorrhage)
Continuous electronic fetal monitoring
• If the woman has risk factors then continuous fetal monitoring should be recommended. The reasons for this should be discussed with her and the fact that it may reduce her mobility in labour. Some women may decide that they wish to decline continuous monitoring and request intermittent auscultation. As long as the woman understands the implications of this decision her wishes should be supported.
• Cardiotocograph (CTG) will be used in the majority of situations. It can be used with an external transducer and does not require the membranes to be ruptured. A fetal scalp electrode may be used but this is only required if a good quality trace cannot be obtained from the external transducer.
• ST analysis of the fetal ECG (STAN) can be used if resources are available for this and the cervix is sufficiently dilated for a fetal scalp electrode to be connected (with amniotomy if the membranes are intact).
Effective interpretation of CTG
FIGO and the UK (NICE/RCOG) guidelines
• FIGO published guidelines for the interpretation of fetal monitoring in 1985 and these were the most commonly used guidelines worldwide. They continue to be used in many countries. In the UK the NICE guidelines published in 2008 along with the Intrapartum Care guidelines are used. These are built on and refined from the recommendations made by FIGO. It is important that local guidelines are developed and adhered to by healthcare professionals working in that unit. The following describes the guidelines for interpretation recommended in the UK.
• Assessment of four features of the fetal heart rate tracing.
Baseline
This describes the average level of the fetal heart rate in between contractions. It should be observed over a period of 5–10 minutes to allow the true baseline to be established. In the presence of significant accelerations or recurrent decelerations it may be difficult to be certain of the true baseline within this time frame and a longer period of monitoring maybe required. If the mother reports associated fetal movements it makes recurrent decelerations less likely than recurrent accelerations. The baseline is associated with gestation and this should be considered when the level of the baseline is reviewed. A preterm fetus may have a heart rate at the upper limit of normal whereas a post-term fetus may have a baseline at the lower limit of normal. The converse may occur but should prompt more careful scrutiny of the clinical risk factors and the other features of the CTG.
A tachycardia develops slowly over a period of time (hormonally mediated) and may be a sign of developing fetal hypoxia but can also indicate fetal infection if the rise of baseline rate is associated with no recurrent decelerations. It may occur if a woman develops pyrexia or is dehydrated.
A bradycardia develops suddenly (mediated via the vagal nerve) and is a sign of acute hypoxia. If a bradycardia does not show signs of recovery over a 6–9-minute period, urgent delivery is required. A fall in the baseline that recovers should be described as a prolonged deceleration, this may indicate intermittent severe fetal hypoxia due to placental or cord issues but may also occur due to maternal hypotension such as following an epidural top-up or following a period where the woman has been overly supine such as a vaginal examination.
Variability
This describes the variation in the fetal heart occurring three to five times per minute giving a ‘spiky’ appearance to the CTG. This is caused by interplay of the fetal autonomic nervous system, which acts continuously to maintain the heart rate within normal limits. Variability is normally more than 4bpm and less than 25 bpm. Variability that is persistently outside these limits has a high correlation with fetal hypoxia. Persistently reduced variability suggests a hypoxic effect on the autonomic nervous system and is associated with a poor prognosis. Reduced variability that is intermittent is of no clinical significance and may occur as part of a normal fetal sleep–wake cycle and even if persistent is not abnormal in the presence of definite accelerations. A CTG with persistently increased variability >25 bpm is known as saltatory. This type of pattern is uncommon but may have an association with fetal hypoxia or fetal fitting and should be managed based on the other features of the trace and the clinical situation.
Accelerations
An acceleration is a rise of the fetal heart rate of 15 bpm or more for 15 seconds or more. They occur in response to fetal movements or other stimulation of the fetus and are almost always a sign of fetal wellbeing. Accelerations should be intermittent and if they occur without a period of normal baseline for a prolonged period (more than 90 minutes) they should be considered to be a saltatory pattern CTG (see Variability). Accelerations become less common during active labour, which may reflect the mild hypoxaemia that occurs in fetuses in normal labour
Decelerations
A deceleration is a transient fall in the fetal heart rate of 15 bpm for 15 seconds or more. If the deceleration lasts for longer than 60 seconds it is defined as a prolonged deceleration. A fall in the fetal heart rate that does not recover is a bradycardia (see Baseline).
There are four types of deceleration that may be seen:
• Early decelerations occur due to fetal head compression with consequent stimulation of the vagal nerve. They require a significant degree of head compression and are only seen in the late last 1st stage or more commonly the second stage when the contractions are expulsive and the head is deeply engaged. As they represent a physiological response of the fetus to an ongoing standard stimulus they are of the same size and shape. The deceleration must occur within the time that the contraction occurs with a return to normal baseline by the end of the contraction. Fetuses experiencing early deceleration have normal cord blood flow and placental gas transfer and thus early decelerations are benign.
• Variable decelerations occur due to cord compression. During this type of deceleration the blood flow between the fetus and the placenta is interrupted and thus a short period where the level of carbon dioxide rises and the oxygen saturation falls is inevitable. As this is a dynamic process with movement of the mother and fetus between contractions they may vary in appearance from one contraction to the next. This type of deceleration shows that the fetus has the physiological reserve to respond to intermittent period of hypoxia. The deceleration will have a transient small rise on the baseline immediately before and after the deceleration (shouldering). The deceleration must occur within the contraction with return to baseline by the end of the contraction.
• Atypical variable decelerations occur due to cord compression but have lost the features to reassure that the fetus has a good physiological reserve to cope with the intermittent period of hypoxia caused by the cord compression. Atypical features include:
• a loss of the pre and post shouldering
Table 10.7.1 Description of the features of the fetal heart rate (FHR) tracing

• a biphasic deceleration (a second deceleration occurs before the first has fully recovered)
• the variability during the deceleration is reduced
• the deceleration is slow to recover lasting beyond the contraction subsiding
• the depth of the deceleration >60 beats and the duration >60 seconds.
• Late decelerations occur due to an abnormality in the retroplacental pool. During every contraction the blood flow into the placenta is reduced. In normal circumstances the fetus is able to maintain normal oxygen levels by gas transfer with a residual volume of oxygenated blood contained in the retroplacental area. In certain situations the retroplacental pool is reduced so that the oxygen levels of the fetus fall during the contraction. The late deceleration shows the fetus responding to the hypoxia. The retroplacental pool is reduced in conditions such as fetal growth restriction, recurrent antepartum haemorrhage with loss of placental area due to infarcts, or in conditions such as diabetes where the placental structure may be abnormal. A fetus in this situation will develop a progressive metabolic acidosis. There is no reliable way of improving the retroplacental pool. Reducing oxytocin, hydration, and positioning of the mother may help in some situations. In the others, early delivery to avoid hypoxia in labour is the only option.
Categorize CTG
The CTG should be reviewed with assessment of all four features and then categorized to decide on further management (Table 10.7.1).
Normal CTG: all four features are reassuring
Suspicious CTG: one non-reassuring feature
Pathological CTG: any two non-reassuring features or any single abnormal feature
Management of CTG following interpretation and categorization
Normal CTG
The risk factors should be reviewed as a CTG may have been commenced unnecessarily in a low risk situation and may be discontinued with conversion to intermittent auscultation to allow the woman to mobilize more effectively.
No specific action is required if the CTG is normal. Occasional variable decelerations in early labour should prompt early action to try to alter the maternal position to relieve cord compression in the anticipation that the degree of cord compression may increase as the labour progresses.
Although the baseline may not show a frank tachycardia a rise in the baseline of 20 bpm during monitoring should prompt a review of the clinical situation with consideration of the need to screen the woman for infection or to improve her hydration.
Suspicious CTG
A full risk factor reassessment should occur. The likely reserve of the fetus to withstand hypoxia should be considered. The woman’s parity, current cervical dilatation, progress in labour and the presence of heavy meconium are also important in deciding further management. A suspicious CTG in early labour in a primigravida woman with a fetus likely to have poor fetoplacental reserve (such as severe growth restriction) requires that the option of delivery should be considered as the probability of developing significant hypoxia is high.
In all other women efforts should be made to try to improve the fetal condition:
• rehydration of the mother with intravenous crystalloid
• administer antipyretic drugs such as paracetamol
• administer antibiotics after appropriate maternal screening if infection is suspected
• change maternal position to avoid the supine dorsal position with use of a lateral (left or right), an upright position or all-fours as these position will reduce caval compression but more importantly reduce cord compression (e.g. cord positioned between the maternal sacrum and the fetal head)
• review of oxytocin therapy to ensure that the contraction frequency is no more than four or five contractions every 10 minutes.
• avoidance of episodic hypotension if this is seen to be precipitating factor in an abnormal fetal heart rate as occurs sometimes following epidural top-ups or vaginal examination in the dorsal position.
A plan should be clearly documented of when the trace will be reviewed again and it is imperative that this review occurs with earlier review if the trace deteriorates further.
Pathological CTG
The management is as for a suspicious trace with the addition of either
• assessment of the fetus for acidaemia by fetal blood sampling (FBS)
• delivery of the fetus by assisted vaginal delivery or Caesarean section. If assisted vaginal delivery is possible but is technically (especially mal-positions) difficult fetal blood sampling should be performed first. Delivery is more appropriate than fetal blood sampling if there is heavy meconium staining and delivery is unlikely to occur in a reasonable time period of a few hours (i.e. in very early labour). Likewise delivery rather than fetal blood sampling should be considered in situations with a poor fetal reserve (infection or prematurity) unless there is a realistic expectation that delivery will occur soon. The ultimate decision will depend on the whole clinical picture in complex cases such as these.
Fetal blood sampling
General comments
• FBS should be performed with the woman in left lateral as lithotomy position increases maternal postural hypotension. If a fetal blood sample cannot be achieved due to early cervical dilatation or the level of the fetal head is high, then delivery rather than fetal blood sampling is appropriate.
• FBS is an intrusive and uncomfortable assessment and the appropriate verbal consents must be obtained from the mother. If a woman declines FBS and the trace is pathological then delivery must be undertaken.
• The cervix must be at least 3 cm dilated with ruptured membranes. BS can occasionally be achieved at dilatations of less than 3cm. The membranes may be ruptured if FBS is required. Membranes were often ruptured to “see the colour of the liquor” if a trace was abnormal. If the trace is suspicious, presence of thick scanty meconium may prompt delivery but amniotomy may also worsen the condition of the fetus by increasing the frequency and severity of cord compression.
• The head should be fixed within the pelvis. A presenting part that moves out of the pelvis on pressure risks increasing cord prolpase during the procedure or immediately after if the cord was in the vicinity of the fetal head.
• FBS can be performed on a breech but should only be done following review by a senior obstetrician as the plan for vaginal delivery should be reviewed. In current practise, Caesarean section is preferred in such situations.
Contraindications to FBS include
• Lack of maternal consent
• Maternal HIV, hepatitis B (including low-infectivity) or hepatitis C infection
• Known maternal immunothrombocytopaenia (gestational thrombocytopaenia is not a contraindication) as this may cause a low fetal platelet count
• Possible fetal bleeding disorder (e.g. male fetus in a haemophilia carrier)
• Non-recovering prolonged deceleration (bradycardia) or pre-terminal CTG pattern (absent variability with recurrent decelerations)
• Independent reason for early delivery
• Grade 3 meconium with a pathological CTG is a relative contra-indication to FBS unless it is expected that either spontaneous or assisted vaginal delivery is likely to be possible within a short time period.
Management of result from first FBS
Normal >7.25
Repeat in no later than 1 hour if CTG abnormality persists
Repeat sooner if the CTG deteriorate or there is heavy meconium or other risk factor for poor fetal reserve to compensate for developing hypoxia (such as infection, growth restriction, prematurity). If the CTG returns to normal a further fetal blood sample is not required.
Borderline 7.20–7.25
Repeat in no more than 30 minutes. As FBS takes an average of 18 minutes to perform the sampling procedure should be commenced almost immediately.
If the CTG deteriorate during this time delivery should be undertaken rather than repeat fetal blood sampling. If there is heavy meconium or other risk factor for poor fetal reserve to compensate for developing hypoxia (such as infection, growth restriction, prematurity) arrangements to expedite delivery should be made with repeat fetal blood sampling only to assess fetal condition if assisted vaginal delivery is possible. If the CTG returns to normal with acceleration a further fetal blood sample is not required but normalisation with the absence of accelerations still requires fetal blood sampling.
Abnormal in response to the procedure or there has been further deterioration in the appearances of the CTG then immediate delivery should be undertaken.
Management of a result from a second and subsequent FBS
If the pH result remains stable then a further sample is only required if the CTG deteriorates with new abnormalities or worsening of existing abnormalities, e.g. rise in baseline rate, increase in depth and duration of the deceleration and reduction of baseline variability.
A third fetal blood sample is rarely indicated as in most cases the whole picture of the labour may suggest delivery. A senior obstetrician should be involved in the decision to perform a third fetal blood sample. Further reading
Gibb D, Arulkumaran S. Fetal monitoring in practice. Churchill Livingstone 2007.
Guidelines for the use of fetal monitoring (FIGO news). Int J Gynecol Obstet 1987;25:159–67.
NICE guideline on fetal surveillance during labour 2001.
NICE intrapartum care guideline 2007 (Chapter 13). Internet resources
RCOG guidelines 2001 www.rcog.org.uk/index.asp?pageid=695
NICE guidelines 2007 www.nice.org.uk/cg055
FIGO guidelines: www.onlinetog.org/cgi/reprint/1/2/18.pdfRCOG Patient resources
MIDIRS: www.choicesforbirth.org/booklets.php?id=2
NICE: www.nice.rg.uk/guidance/cg00/publicinfo/pdf/english
Home birth Definition
Home birth refers to giving birth at one’s home, away from the hospital, midwifery-led unit, or a birth centre. The concept is based on the notion that childbirth is a normal physiological process and, hence, is most likely to succeed in a non-medicalized environment (i.e. home) surrounded by family and friends. Home birth may also facilitate the involvement of fathers in planning and attending the home-birth, which may lay the foundation for their engagement in both childbearing and child rearing in the future. Epidemiology
Prior to 1900, about 90% of births worldwide occurred at home. Recent figures suggest that home birth rate in the UK remains at about 2–3% and this figure has not changed significantly over the last 10 years. It has been suggested that if all women were given a choice, about 8–10% of women may opt to have a home birth. There is evidence to suggest that about 16% of women who have planned for home birth may need to be transferred to the hospital to manage complications (4% antenatally and 12% during labour). In primigravidae, the rate of transfer is about 40%. It has been recognized that financial constraints, culture, beliefs and attitudes of organizations, and lack of competent staff contribute to low home birth rate in the UK. Eligibility criteria
Home birth should be recommended to ‘low-risk women’ without any medical, obstetric, or fetal conditions that may necessitate closer monitoring and intervention. The healthcare system should be able to provide resources (trained and competent community midwives) and supporting services (facilities for transport to a hospital in emergency). Women should be fully counselled regarding their birth choices, which include a home birth, birth in a midwiferyled unit or a birth centre, and birth in hospital with obstetric input. Women with risk factors such as pre-eclampsia, diabetes mellitus, heart disease, malpresentation, previous uterine scars, and fetal complications such as intrauterine growth restriction (IUGR) and any other medical, obstetric, or fetal complications should be advised to have a hospital birth. This is because closer monitoring and therapeutic interventions may be necessary to improve maternal and/or fetal outcome in these situations. Hence, a risk assessment should be carried out both in the antenatal period as well as at the onset of and during labour, to identify any risk factors that may necessitate transfer to a hospital unit. It is important to realize that risk assessment tools do not have sufficient predictive value and risk assessment is a dynamic process throughout pregnancy and labour. Antenatal preparation
Woman should develop confidence in the safety of the home environment. Continuity of care with her community midwife, attending antenatal classes and considering the options for pain relief (hypnotherapy, yoga, aromatherapy, acupressure bands, Transcutaneous electric nerve stimulation or TENS machine) are of paramount importance.
Apart from required cloths for the mother and baby, birthing stool, birthing pool or a birth ball may be used at home to facilitate labour. Advantages of home birth
Home birth avoids unnecessary medicalisation of a normal physiological process and enables the woman to labour at home in the comfort of her familiar environment, with the support of family and friends. It gives greater control for her and her partner over the birthing experience. Hospital acquired infections and other inconveniences (food, environment, disturbance from parturients) are minimized. Home birth also facilitates bonding and a quicker return to normal life.
In low-risk women, there is evidence to suggest that home birth reduces the requirement for analgesia, obstetric interventions (instrumental vaginal delivery and caesareans sections) and improves maternal satisfaction. There is no significant difference in maternal or fetal complications between home births and hospital births. Possible complications
These include failure to progress in first or second stage of labour, fetal distress, intrapartum abruption, maternal collapse, requirement for analgesia, shoulder dystocia, and postpartum complications such as postpartum haemorrhage, inversion of uterus, maternal collapse, gential tract trauma, and retained placenta. Neonatal complications include cardiorespiratory collapse or meconium aspiration. Women should be counselled about the rare possibility of fetal compromise (rarely, intrapartum fetal death), maternal compromise due to postpartum haemorrhage as well as the possibility of transfer to the hospital. They should be made aware that these life-threatening complications are rare but immediate operative interventions may not be available, as in the hospital setting, but arrangements would be made to receive the case quickly by ambulance transfer.
It is recommended that at least two midwives are present during a home birth, especially during the second stage of labour to manage these complications. It is good practice to inform the labour ward of the local hospital about women who are actively labouring at home, so that staff can anticipate a potential admission.
• Failure to progress in first stage of labour can be initially managed by amniotomy. If there is further delay (at least 2 cm of cervical dilatation in 4 hours in active stage of labour), the woman should be transferred for augmentation of labour. Similarly, failure to progress in second stage of labour (2 hours in a primigravidae and 1 hour in a multigravida without epidural anaesthesia) would require transfer to an obstetric unit.
• If the woman does not cope with pain and requires stronger analgesia, transfer may need to be considered.
• If intermittent fetal heart rate monitoring (every 15 minutes during first stage of labour and every five minutes during second stage of labour, after a contraction) reveals evidence of decelerations and if delivery is not imminent, immediate transfer to the closest maternity unit should be arranged. Intravenous fluids and changing the position (e.g. left lateral position) may help improve placental circulation during transfer. Similarly, if meconium staining of liquor is noted, the woman should be transferred for continuous electronic fetal heart rate monitoring (EFM).
• Shoulder dystocia and neonatal cardiorespiratory resuscitation are emergencies that need to be managed by midwives in attendance. It is paramount that midwives who conduct home births regularly update themselves on skills and drills on shoulder dystocia, and neonatal resuscitation. In both these situations, transfer to a hospital is unlikely to improve perinatal outcome as delay in treatment may cause irreversible hypoxic injury.
• Postpartum haemorrhage (atonic, traumatic, or due to retained placenta or coagulopathy) needs immediate measures to resuscitate the patient. Insertion of large-bore intravenous cannulae, administration of oxytocin or ergometrine and intravenous fluids as well as uterine massage can be performed by the attending midwives prior to transfer. Dilemma: maternal choice versus safety
Clinicians may be faced with a situation whereby a woman who is at high risk, requests a home birth, against medical advice. In the author’s experience, women with previous Caesarean section, intrauterine growth restriction, breech presentation and known group B streptococcal (GBS) colonization of the vagina have all requested a home birth. If the woman has the capacity to consent or to refuse treatment, after careful counselling, maternal choice should be respected. It is good practice to refer the woman to another colleague for counselling. Clear and detailed documentation of the discussion should be made in the mother’s hand-held maternity notes, with emphasis of potential complications and outcome. Home birth: future challenges
Following the confidential survey carried out by the National Birthday Trust, it was anticipated in 1999 that the home birth rate in the UK would rise to 4–5% in the following decade. Unfortunately, the recent joint statement by the Royal College of Obstetricians and Gynaecologists (RCOG) and the Royal College of Midwives (RCM) in 2007, suggests that that the home birth rate is still round 2% and, hence, has not changed dramatically over the last decade. In contrast, about a third of all births occur at home in some Scandinavian countries. Financial constraints, shortage of competent and experienced community midwives, concerns about safety by both staff and patients, as well as inherent negative attitude towards home birth, are some of the factors that have prevented an increase in home births in the UK.
Recently, National Drivers such as National Service Framework (NSF) and the National Institute of Clinical Excellence (NICE) have emphasized the importance of home birth as a choice that should be offered to all low-risk women. There is no doubt that for a group of low-risk women, home birth would remain the safest and the best option. Every effort should be made by all clinicians to promote home birth for these women, to improve their birth experience. Further reading
Anderson RE, Murphy PA. Outcomes of 11,788 planned home births attended by certified nurse-midwives. A retrospective descriptive study. J Nurse Midwifery 1995;40:483–92.
Christiaens W, Gouwy A. Bracke P. Does a referral from home to hospital affect satisfaction with childbirth? A cross-national comparison. BMC Health Service Res 2007; 12; 7: 109.
Department of Health. The National Service Framework for Children and Young People. Maternity Services. Standard 11. London: Department of Health; 2004 www.dh.gov.uk/assetRoot/04/09/05/23/04090523.pdf.
Janssen PA, Lee SK, Ryan EM, et al. Outcomes of planned home births versus planned hospital births after regulation of midwifery in British Columbia. CMAJ 2002;166:315–23.
Janssen PA, Lee SK, Ryan EM. An evaluation of process and protocols for planned home birth attended by regulated midwives in British Columbia. J Midwifery Womens Health 2003;48:138–45.
Johnson KC, Daviss BA. Outcomes of planned home births with certified professional midwives: large prospective study in North America. BMJ 2005; 330: 1416.
Mehl-Madrona L, Madrona MM. Physician- and midwife-attended home births. Effects of breech, twin, and post-dates outcome data on mortality rates. J Nurse Midwifery 1997;42:91–8.
Olsen O. Meta-analysis of the safety of the home birth. Birth 1997;24:4–13.
RCOG/RCM. Home births. Royal College of Obstetricians and Gynaecologists/Royal College of Midwives Joint statement No.2, April 2007.
Royal College of Midwives. Home birth hand book: Vol. 1: Promoting home birth. London: RCM 2002.
Royal College of Midwives. Home birth hand book: Vol. 2: Practising home birth. London: RCM 2003. Patient resources
www.homebirth.org.uk
www.homebirth.net
Induction of labour Definition
Induction of labour is defined as the artificial initiation of labour at any point after viability of the fetus (24 weeks). Cervical ripening is referred to as the process of cervical effacement and softening that precedes cervical dilatation. Frequency
Induction rates vary hugely worldwide, and have increased rapidly over the last three decades. Quoted national rates vary between 1% and 40%, although individual units quote rates as high as 55%. In a recent English survey, the rates in units varied from 13% to 44% (median 26%, HCC 2008). Indications
Irrespective of the country studied, the commonest causes of induction are post-date pregnancy (Chapter 9.14, Prolonged pregnancy) and hypertension (Chapter 8.22, Hypertension). Other causes included ruptured membranes (Chapter 10.16, Prelabour rupture of membranes), fetal compromise, maternal disease, intrauterine fetal death, and maternal request (see below) make up the remainder. Risks of induction
• Induction of labour is associated with an increased risk of Caesarean section (CS) (typically ? 1.5; Cammu 2002). However, this effect occurs primarily as a result of the indication for induction: in randomized controlled trials (RCTs) of elective induction at term for maternal request the risk of Caesarean section appears to be reduced (NCCWCH 2007).
• Uterine hyperstimulation after low-dose prostaglandin induction occurs in about 5% of women (one-third of these will have fetal heart rate abnormalities). It can be rapidly reversed with β2-adrenergic therapy (e.g. terbutaline 250 µg subcutaneously) without maternal or fetal complications.
• In well-resourced settings, uterine rupture is a complication usually only found in women who have had a previous CS. In women undergoing VBAC (after a single delivery by CS) the rupture rate of 1 in 210 in spontaneous labours is increased to 1 in 70 in women induced with prostaglandins (Smith 2004). The rupture rate in women induced with amniotomy and oxytocin alone, or in women who have also previously delivered vaginally, was not significantly increased. Pharmacological methods
Dinoprostone (PGE2)
• In women with an unfavourable cervix, vaginal PGE2 improves cervical status and reduces the need for oxytocin augmentation. The risk of hyperstimulation is, however, increased (?4) over placebo rates.
• Vaginal prostaglandin tablets and gel are equally effective, but intracervical prostaglandins result in a slower induction. The three have otherwise no difference in maternal or fetal outcomes. Oral prostaglandins are also effective, but have a high rate of gastrointestinal side-effects.
Oxytocin
• When combined with artificial rupture of membranes (ARM), oxytocin is as effective as vaginal dinoprostone for labour induction but with less maternal satisfaction. There are no differences in hyperstimulation rates.
• When used alone, oxytocin is less effective than vaginal prostaglandins for induction of women with either intact or ruptured membranes.
• Oxytocin is usually used for labour augmentation following induction, or with ARM following cervical priming. The only alternative for this indication is oral misoprostol (see below).
Misoprostol
• Misoprostol (an orally active PGE1 analogue) is effective for labour induction when used at low dose. Its price and heat stability make it an attractive option.
• Although 25 µg vaginal pessaries are available in some countries, most misoprostol tablets are 200 µg. To obtain small doses, the tablets need to be cut and this makes dosaging inaccurate. A more accurate regimen is to dissolve a 200 µg tablet in 200 mL water–this solution is stable at room temperature for at least 24 hours. The solution should be stirred before every use.
• Oral misoprostol solution (20 µg 2 hourly) is as effective as vaginal dinoprostone, and has a lower CS rate. Vaginal misoprostol (25 µg 4 -hourly) had equivalent outcomes to vaginal dinoprostone.
• Titrated oral misoprostol solution has also been used during induced labour for augmentation (instead of oxytocin). Women are given 5–20 µg orally every 1–2 hours to keep contractions at 3 in 10 minutes. This regimen is commonly used following induction with oral misoprostol solution, and appears to be as effective and safe as oxytocin (Hofmeyr 2001).
Mifepristone
• Mifepristone is a progesterone antagonist that sensitizes the uterus to prostaglandins.
• When used alone, it results in labour in only 50% of women after 48 hours.
• When given 24–48 hours before induction in women with intrauterine fetal deaths, it reduces the induction to delivery interval.
• There are reports of neonatal antiglucocorticoid effects, as well as fetal renal and hepatic dysfunction when used with live fetuses. Its use is therefore restricted to women with intrauterine fetal deaths.
Others
• Vaginal nitric oxide donors (e.g. isosorbide mononitrate, or glyceryl trinitrate) also induce labour, but are much slower than vaginal dinoprostone (with corresponding lower rates of hyperstimulation). There is a high rate of mild maternal side-effects (headache in 90%), but maternal satisfaction is higher than for dinoprostone. Their gentle uterine effects may make them suitable for outpatient cervical ripening (Osman 2006)
• Oral corticosteroids, intracervical hyaluronidase injection, and oestrogens have all shown some effect, but there is not enough RCT evidence to comment on their safety and efficacy. Surgical methods
Amniotomy
• Amniotomy is rarely used alone for induction. When combined with oxytocin it is as effective as vaginal dinoprostone (see above).
• Amniotomy may be a useful adjunct to allow visualization of liquor and placement of a fetal scalp electrode.
Transcervical balloon catheter
• A Foley catheter may be inserted through the cervix (manually or using ‘sponge holders’) and the balloon filled to 30–50 mL. The catheter is then taped to the inner thigh under slight tension. Some also infuse saline extra-amniotically at 50 mL/hour. When the catheter falls out, an ARM is performed and oxytocin commenced.
• Balloon catheters appear to be as effective at labour induction as vaginal prostaglandins, with comparable rates of uterine hyperstimulation.
Laminaria tents
• Laminaria tents are made from sterile seaweed or synthetic hydrophilic materials, and are introduced into the cervical canal. As these devices absorb water, they increase in diameter and so stretch the cervix.
• Laminaria appear to be as effective at labour induction as vaginal prostaglandins, but with a reduced incidence of uterine hyperstimulation. This may make them safer for women who have had a previous CS. Non-pharmacological methods
Membrane sweeping
• Membrane sweeping involves inserting a finger through the cervical os and sweeping it around between the chorion and the uterine wall to release prostaglandins.
• The clinical effects of membrane sweeps are to reduce the need for formal induction of labour (especially in multiparous women) and to increase the rate of spontaneous labour, if performed more than once from 38 weeks of gestation. In view of this it is recommended in the UK for all women at clinic visits following their due date and before formal induction (NCCWCH 2008).
• If the cervix will not admit a finger it may not be possible to do a formal membrane sweep. In such cases massaging around the cervix in the vaginal fornices may achieve a similar effect.
• A small amount of bleeding is common following the procedure.
Complimentary and natural methods
• Herbal medicines, acupuncture, enemas, castor oil, and homeopathy have all been used for labour induction. There are Cochrane reviews of all these interventions, but all find insufficient scientific research to recommend their use.
• Sexual intercourse has been subjected to two randomized trials, but neither has shown any benefit in clinical outcome.
• There is some evidence to support breast stimulation as an induction method. Clinical approach
Prior to induction
• The indication and gestation should be rechecked.
• Fetal health should be rechecked just prior to induction, usually using electronic fetal heart rate monitoring.
• The modified Bishop score (Table 10.9.1) should be assessed to decide on the need for pre-induction cervical ripening. A Bishop score of 8 or more indicates a ‘ripe’ or favourable cervix.
During induction
• Induction of labour should ideally be carried out in settings with electronic fetal monitoring, facilities for accurately measuring infusion rates, and access to emergency CS.
• Outpatient induction is an option, but methods with low rates of hyperstimulation should be used (e.g. mechanical methods, nitric oxide donors or controlled release prostaglandins). RCTs suggest no difference in clinical outcome, but higher maternal satisfaction rates (Biem 2003).
• Inductions should ideally be started in the morning as they are associated with higher maternal satisfaction and lower operative vaginal delivery rates.
• Electronic fetal heart rate monitoring should be conducted before and after every drug administration, and once contractions start. Once in labour, most women have continuous monitoring. The only exception is women who have had an uncomplicated pregnancy (i.e. they have no fetal indication for induction) and who have not needed oxytocin augmentation (NCCWCH 2008).
• Induced labours are more painful than spontaneous labours. However, women (and staff) can be reassured that administering epidural analgesia prior to painful contractions or in early labour has no adverse effects on clinical outcomes and increases maternal satisfaction. Special indications
Intrauterine fetal death (IUFD)
• Without therapy 90% of women with an IUFD will deliver within 3 weeks. In the absence of abruption, the risk of clotting disorders is low for the first 2 weeks.
• Standard dinoprostone or oxytocin regimens may be used at term, or gemeprost 1 mg 3 h
• Mifepristone 200mcg given orally 48 hours prior to induction may reduce the time to delivery.
• Vaginal misoprostol is useful in that its dose can be adjusted according to gestation. Lower doses of misoprostol are needed for labour induction following IUFD. A typical regimen (Gomez 2007) is:
• 13–17 weeks: misoprostol 200 µg 6 hourly (?4)
• 18–26 weeks: misoprostol 100 µg 6 hourly (?4)
• >26 weeks: misoprostol 25-50 µg 4 hourly (?6)
• There is an increased risk of chorioamnionitis following IUFD and so ARM should be delayed as long as possible to prevent ascending infection.
Maternal request for induction of labour (37–40 weeks)
• Despite being widely discouraged, there is no evidence that the outcomes are any worse for women induced without medical indication. Indeed the limited evidence suggests that the CS rate may actually be decreased, albeit with increased operative vaginal delivery rates. It obviously prevents stillbirths following the induction date, although these are very rare (Gulmezoglu 2006).
Suspected fetal macrosomia
• Diagnosis is an initial problem—only about 50% of babies >4 kg are detected with either ultrasound or palpation.
• From the limited RCT evidence, there is no reduction in delivery complications, and the need for CS is doubled (Sanchez-Ramos 2002). However, shoulder dystocia is rare even in suspected macrosomia (5% in the Cochrane meta-analysis) and so it would take very large studies to demonstrate an effect.
Table 10.9.1 Bishop score table. The score for each factor is added giving a score between 0 and 13

High risk inductions
Previous Caesarean section
• The risk of uterine rupture in spontaneous labourers with a previous CS is around 1 in 210. Induction of labour with prostaglandins increases this risk to around 1 in 70 (and possibly even higher with misoprostol). The risk is not increased in those who have had a previous vaginal delivery (even if induced with prostaglandins) or in those suitable for ARM/oxytocin (Smith 2004).
• Successful vaginal delivery is achieved in approximately 70% of spontaneously labouring women undergoing VBAC. This is reduced in women undergoing induction (to 50%) and in those with an unfavourable cervix.
• The use of intrauterine pressure catheters does not prevent uterine rupture.
‘High head’ (controlled ‘ARM’)
• Induction of labour when the head is high in the pelvis increases the risk of cord prolapse and malpresentation. Medical methods (e.g. dinoprostone) should therefore always be used initially.
• When ARM is necessary, this should be performed along with fundal pressure. With polyhydramnios, it is useful to keep the examining hand in the vagina until the liquor has drained and the head descended. The woman should sit upright after the ARM to encourage head descent.
• If the head is very high, some practitioners prefer to conduct the ARM in theatre so that CS can rapidly be carried out in the event of a cord prolapse.
Induction in low resource settings
• Induction indications in low resource settings are similar to those in high resource settings, except that there are fewer inductions for fetal reasons (e.g. IUGR).
• With limited resources for fetal monitoring, induction is more hazardous for mother and baby and the threshold for induction is consequently raised. In these settings the stillbirth rate is doubled and need for neonatal resuscitation increased fourfold (Dujardin 1995). This reflects both the lack of monitoring and the fact that the women being induced have more advanced clinical disease.
• In these settings there are great benefits to the use of oral misoprostol solution for induction as it is cheap, requires no infusion apparatus, and can be continued at low dose (typically 5–20 µg/hour) through labour in place of oxytocin (Kundodyiwa 2009).
Failed induction
• In around 15% of women it is not possible to do an ARM even after cervical ripening with 2 doses of prostaglandin.
• Management options depend on the urgency and indication for the induction. If low risk and no urgency, then the induction process may be repeated after a 24–48-hour rest period. If more urgent, then alternative induction methods may be attempted or a CS performed.
Frequently asked questions
• Can cervical ripening be performed as an outpatient?
• This has been done safely, but experience is limited (see above). A CTG is done after the dinoprostone is inserted, and the woman returns once contractions start or at the time of next planned dose.
• Are induced labours more painful?
• Yes: analgesic requirements are higher in induced labours.
• Does the use of an epidural early in the induction have any adverse effects on labour outcome?
• No. Early, rather than late, administration of epidural analgesia does not prolong labour or increase the incidence of instrumental or caesarean section births. There is no benefit in waiting until labour has started to give epidural (NCCWCH 2008). Further reading
Beukens P. Overmedicalization of maternal care in developing countries. Antwerp: ITGT Press; 2001.
Biem SR, Turnell RW, Olatunbosun. A randomized controlled trial of outpatient versus inpatient labour induction with vaginal controlled release prostaglandin-E2: effectiveness and satisfaction. J Obstet Gynaecol Canada 2003;25:23–31.
Cammu H, Martens G, Ruyssinck G, Amy J. Outcome after elective labor induction in nulliparous women: A matched cohort study. Am J Obstet Gynecol 2002;186:240–4.
Dujardin B, Boutsen M, De Schampheleire I, et al. Oxytocics in developing countries. Int J Gynaecol Obstet 1995;50:243–51.
Gomez Ponce de Leon R, Wing D, Fiala C. Misoprostol for intrauterine fetal death. Int J Gynecol Obstet 2007; 99(Suppl. 2): S190–3.
Gülmezoglu AM, Crowther CA, Middleton P. Induction of labour for improving birth outcomes for women at or beyond term. Cochrane Database Syst Rev 2006; 4: CD004945.
Hofmeyr GJ, Alfirevic Z, Matonhodze B, et al. Titrated oral misoprostol solution for induction of labour: a multicentre, randomised trial. Br J Obstet Gynaecol 2001;108:952–9.
Kundodyiwa T, Alfirevic Z, Weeks A. Low dose oral misoprostol for induction of labor: a systematic review. Obstet Gynecol 2009;13:374–83.
National Collaborating Centre for Women’s and Children’s Health (NCCWCH). Induction of Labour. London: RCOG Press; 2008.
Osman I, MacKenzie F, Norrie J, et al. The ‘PRIM’ study: A randomized comparison of prostaglandin E2 gel with the nitric oxide donor isosorbide mononitrate for cervical ripening before the induction of labor at term. Am J Obstet Gynecol 2006;194:1012–21.
Sanchez-Ramos L. Expectant management versus labor induction for suspected fetal macrosomia: a systematic review. Obstet Gynecol 2002;100:997–1002.
Smith GC. Factors predisposing to perinatal death related to uterine rupture during attempted vaginal birth after caesarean section: retrospective cohort study. BMJ 2004; 329: 375. Internet resources
Health Care Commission 2008 (HCC): www.healthcarecommission.org.uk/healthcareproviders/nationalfindings/surveys/health-careproviders/surveysofpatients/maternityservices.cfm
www.misoprostol.org
Labour
This section covers the management of normal labour and slow labour. Other sections cover the complications of labour, place of birth (Chapter 10.8, Home birth), fetal assessment (Chapter 10.7, Fetal surveillance in labour), analgesia (Chapter 10.1, Analgesia and anaesthesia in obstetrics), episiotomy (Chapter 10.5, Episiotomy and obstetric perineal trauma), Caesarean section (Chapter 11.2, Caesarean section), and operative vaginal delivery (Chapter 11.5, Ventouse delivery). Definitions
Labour is defined as painful contractions with progressive cervical change (NCCWCH 2007). The latent phase of labour is a period of time during which there are painful contractions and some cervical changes (effacement or dilatation up to 4 cm dilated). The established first stage is when there are regular painful contractions and progressive cervical dilatation from 4 cm. The passive second stage is the finding of full dilatation prior to involuntary expulsive contractions. The active second stage occurs when there are expulsive contractions or active pushing with full dilation or the head is visible. The third stage of labour is from the time of birth of the baby to the expulsion of the placenta and membranes. Schools of labour management
Labour management has varied hugely over the years in response to scientific advances, public health priorities, fashion, and opinion-formers. The major schools are listed below.
Medicalized labour (1950s)
This school arose in an attempt to reduce the very high maternal and fetal complication rates. Proponents believed that complications of labour could be largely resolved by the use of medical technology. As such, it advocated the extensive, and largely uncritical use of all available technology such as episiotomy, electronic fetal monitoring, and operative vaginal delivery.
Natural labour (1950s to date)
In response to the increased medicalization of labour, an alternative school grew up that recognized the dangers of medical intervention in normal labours. Leaders such as Kitzinger and Odent promoted the benefits of home and water birth, relaxation, and physiology.
Active management of labour (1970–90)
This regimented style of labour management was developed in the National Maternity Hospital in Dublin. It was characterized by clearly defined protocols for the diagnosis of labour (painful contractions with a fully effaced cervix, ruptured membranes, or show) and the early diagnosis of dystocia (hourly vaginal examinations for the first 3 hours), which was treated with oxytocin. The impressive outcome data from this hospital seemed to provide evidence of its benefit and ‘active management’ became extensively practiced worldwide.
Evidence-based labour management (1990 to date)
The arrival of the Cochrane Database of Pregnancy and Childbirth in the late 1980s injected a new rigour into the assessment of evidence, and Thornton and Lilford went on to challenge the use of active management (Thornton 1994). An RCT of ‘active management’ finally showed it to provide no benefit on labour outcomes (Frigoletto 1997). Since then, the evidence-based medicine (EBM) school has been largely unchallenged.
This chapter is written using EBM methods and draws extensively on the 2007 guidelines from the UK National Institute of Clinical Excellence (NICE), produced by the National Collaborating Centre for Women’s and Children’s Health (NCCWCH 2007). Assessment of labour progress
Clinical examination
• Although helpful in assessing labour progress, vaginal examinations should be minimized due to discomfort and the risks of infection. The risk of postpartum endometritis has been found to be closely related to the number of internal examinations after membrane rupture.
• The digital vaginal assessment of head descent is notoriously difficult. The use of abdominal palpation may improve accuracy, but is difficult in the obese or tense. A new device called the StationMaster has been shown to increase the accuracy of assessment in clinical models (Awan 2009).
• Likewise, the accuracy of digital cervical dilation is poor, especially between 4 and 8 cm dilatation (Awan 2009). An electronic device called Birthtrack increases accuracy but is invasive.
The partogram
• The partogram (Fig. 10.10.1) is based on the original cervicogram, developed by Friedman in the 1950s. Philpott (1972) added an ‘action line’ set 4 hours to the right of the alert line to aid the correct timing of intervention.
• A cluster RCT of partogram versus no partogram found that use of the partogram halved the rate of prolonged labour and use of oxytocin while increasing the rate of spontaneous birth (Anon 1994). Recent studies show that placement of the action line 2 hours to the right of the alert line (rather than 4 hours) increased intervention without improving clinical outcomes.
• With increasing lengths of the second stage in epidural labours, a second-stage partogram might help to predict and time for delivery intervention (Sizer 2000). Efforts so far have been hampered by difficulties in accurately assessing head descent. First stage of labour
Normal progress
• In nulliparous women, the average latent phase lasts 7 hours (upper limit 15 hours) and the active first stage lasts 8 hours (upper limit 19 hours). In multiparous women, the average length of the active first stage is 5 hours (upper limit 15 hours). The NICE guideline suggests that a rate of less than 0.5 cm/hour in the active phase should be used as a cut off for intervention rather than the customary 1 cm/hour (NCCWCH 2007).
Optimizing outcomes
• Clinical intervention is not advised where labour is progressing normally.
• Birth at home and in birthing centres (Chapter 10.8) are all associated with an increased chance of normal birth.
• Routine amniotomy shortens the length of labour but has no other beneficial effects on outcome.
• Early oxytocin use has not been shown to be of benefit: it increases the pain without beneficial effects on labour outcome.

Fig. 10.10.1 The partogram. The head descent is in fifths palpable abdominally, and the shading of the contractions relates to the duration of the contractions.

Fig. 10.10.2 Manual rotation for correcting malposition in the second stage of labour.
• One-to-one midwifery care was originally thought to be a minor part of the active management of labour package. But when the various components were unpicked, this proved to be the only component that significantly improved clinical outcomes with reductions in analgesia use, operative delivery, and low APGAR scores (Thornton 1994). The Cochrane analysis now shows that the care is at least as effective if the continuous support is provided by a friend rather than member of staff.
Managing delay
• Prolonged latent phase (over 18 hours in a nulliparous woman) is best treated with reassurance and analgesia. Use of oxytocin in this situation increases the need for Caesarean (CS) and poor outcomes in the neonate without benefit.
• Primary dysfunctional labour (progress of under 0.5 cm/hour) should be treated with amniotomy and oxytocin with continuous fetal heart rate monitoring (NCCWCH 2007). NICE’s suggested timeline for nulliparous women (in hours) is
• Time 0: diagnosis of labour
• 4 hours later: if less than 2 cm progress→amniotomy
• 2 hours later: if less than 1 cm further dilated→oxytocin
• 4 hours later: if less than 2 cm progress on oxytocin → consider the option of further augmentation or CS.
• There are multiple oxytocin regimens available and conflicting evidence as to their relative benefits. Infusion rates should be increased every 30 minutes until there are around four contractions in every 10 minutes.
• Secondary arrest of labour (cessation of progress following normal active phase dilation) is usually caused by disproportion and or malposition of the fetal head. Improving contraction strength with oxytocin may help to correct the disproportion, although the risk of a CS remains high.
• Late secondary arrest with delay between 7 and 10 cm is associated with difficult instrumental vaginal deliveries, despite reaching full dilatation. Second stage of labour
Normal progress
• The mean length of the second stage in primigravid women (without epidurals) is 54 minutes with an upper limit (mean + 2 SD) of 2 hours 22 minutes. For mutigravid women the mean is 18 minutes, with an upper limit of 60 minutes (NCCWCH 2007).
Optimizing outcomes
• Lying in a supine position increases both pain and the need for operative vaginal delivery. Women should be encouraged to adopt any other position that they find comfortable.
• Techniques for reducing perineal trauma are discussed in Chapter X.
• Epidurals are associated with an increased need for operative vaginal deliveries but provide higher rates of maternal satisfaction with analgesia.
• In primiparous women with epidurals, the use of routine oxytocin in the second stage of labour can reduce the need for non-rotational forceps delivery.
• Primiparous women with epidurals have fewer rotational or mid-cavity operative interventions when pushing is delayed for 1–2 hours or until they have a strong urge to push
Managing delay
• A diagnosis of delay is made after 2 hours of pushing in a nulliparous or after 1 hour in a multiparous (NCCWCH 2007).
• Oxytocin can be used in nulliparous women if contractions are poor. Oxytocin should not be used (or with extreme caution based on contractions observed) for delay in multiparous women due to the risk of uterine rupture.
• Caesarean section (Chapter 11.2) or instrumental delivery (Chapter 11.3) are the definitive treatments for delay. The choice of instrument depends on operator experience. Operative vaginal delivery should not be attempted if the head is more than one-fifth palpable abdominally.
• Manual rotation is sometimes used to improve outcomes with malposition during the second stage, but there is little evidence to support its use. It should be undertaken with care due to the risks of fetal trauma and cord accidents. The classic technique is to slide the fingers right behind the occiput so that the head can be flexed and rotated at the same time (Fig. 10.10.2). The operator’s right hand is used for LOPs and the left hand for ROPs (Donald 1979). It has been used both prophylactically at the start of the second stage (Le Ray 2007) and as an alternative to rotational operative delivery after delay. Third stage of labour
Normal physiological progress
• The median length of third stage is 15 minutes if physiologically managed and 8 minutes if actively managed (Rogers 1998).
• For a physiologically managed third stage the third stage is prolonged if it lasts over 60 minutes. This time limit is reduced to 30 minutes when prophylactic oxytocics are used (NCCWCH 2007).
• Median measured blood loss in a physiological third stage is 496mls with 17% loosing over 1000 mL of blood (Hoj 2005).
Physiology
• Four phases of the normal third stage are described (Herman 1993). In the latent phase there is contraction of the entire uterus except for the retroplacental myometrium. The length of this phase determines the length of the third stage. This is followed by phases of retroplacental contraction, placental detachment, and expulsion.
• The retroplacental contraction compresses the radial arteries as they pass through the myometrium, thus cutting off the blood supply to the placental site and minimising haemorrhage.
Optimizing outcomes
Active management package
• Classic active management is a combination of routine oxytocic use, early cord clamping, and controlled cord traction using the Brandt–Andrews method. In view of the adverse effects of early cord clamping, FIGO has now amended this package to replace the early cord clamping with uterine massage (FIGO 2003).
• In an actively managed third stage, the median measured blood loss is reduced with only 3% loosing over 1000 mL.
• Multiple oxytocics have been studied. Oxytocin 10 IU i.m. (effective in 2 minutes, lasts 15 minutes) is now the oxytocic of choice as it combines high efficacy with few side-effects (FIGO, NCCWCH 2007). Ergometrine 500 µg i.m. (effective in 6 minutes, lasts 30 minutes) is slightly more effective than oxytocin, but causes vomiting and hypertension, and, when given i.v., retained placenta. Syntometrine 1 ampoule i.m. (contains 5 IU of oxytocin and 500 µg of ergometrine) combines the benefits and side-effects of both. Misoprostol 600 µg po (effective in 8 minutes, lasts 120 minutes) is less effective than oxytocin 10 IU i.m., but is heat stable and easy to administer.
Timing of cord clamping
• The neonate receives about 30% of its final blood volume in the first 3 minutes after delivery from the placenta.
• Early cord clamping reduces neonatal cord haemoglobin concentrations and the rate of hyperbilirubinaemia, but increases the rate of neonatal anaemia (with associated reduced iron stores for up to 6 months of age). This could have important public health implications in populations with already high rates of iron deficiency anaemia.
• In premature babies, early cord clamping increases the rate of intraventricular haemorrhages and the need for transfusion to treat anaemia and hypotension.
• There is no known benefit to the woman of early cord clamping in terms of reduced postpartum haemorrhage outside of the active management package. Indeed, small trials of cord drainage suggest that it might even have benefits by reducing the rate of retained placenta.
Controlled cord traction
• This was introduced as part of the active management package so as to reduce the rate of retained placenta. In the Brandt–Andrew’s method once there are signs of placental separation (a small gush of blood and lengthening of the cord) the cord is held taut while the other hand on the abdomen presses the uterus away.
• There are dangers of cord traction: premature cord traction may cause bleeding by separating the placenta from an uncontracted myometrium, and overenthusiastic traction may detach the cord from the placenta.
• The first major trial of controlled cord traction is currently in progress and is expected to finish in 2010.
Uterine massage
• Postnatal uterine massage has only been investigated in one small trial and this showed some reduction in blood loss.
Managing delay
Retained placenta is covered in Chapter 10.18. Further reading
Akmal S, Kametas N, Tsoi E, et al. Comparison of transvaginal digital examination with intrapartum sonography to determine fetal head position before instrumental delivery. Ultrasound Obstet Gynecol 2003;21:437–40.
Anonymous. Managing complications in pregnancy and childbirth. A guide for midwives and doctors. Geneva: WHO 2006.
Anonymous. World Health Organization partograph in management of labour. World Health Organization Maternal Health and Safe Motherhood Programme. Lancet 1994; 343 (89: 1399–404.
Awan N, Rhoades A, Weeks AD. The validity and reliability of the StationMaster: a device to improve the accuracy of station assessment in labour. Eur J Obstet Gynecol Reprod Biol 2009;145:65–70.
Chalmers I, Enkin M, Kierse MJNC (eds). Effective care in pregnancy and childbirth. Oxford: Oxford University Press 1989.
Crichton D. A reliable method of establishing the level of the fetal head in obstetrics. S Afr Med J. 1974;48:784–7.
Donald I. Practical obstetric problems, 5th edn. London: Lloyd-Luke 1979.
FIGO/ICM. Prevention and treatment of post-partum haemorrhage: new advances for low resource settings. A joint statement of the International Confederation of Midwives (ICM) and International Federation of Gynaecology and Obstetrics (FIGO). Available at: www.figo.org/docs/PPH%20Joint%20Statement%202%20English.pdf
Frigoletto FD Jr, Lieberman E, Lang JM, et al. A clinical trial of active management of labor. N Engl J Med 1995;333:745–50.
Gülmezoglu AM, Villar J, Ngoc NT, et al. WHO multicentre randomised trial of misoprostol in the management of the third stage of labour. Lancet 2001;358:689–95.
Herman A, Weinraub Z, Bukovsky I, et al. Dynamic ultrasonographic imaging of the third stage of labor: new perspectives into third-stage mechanisms. Am J Obstet Gynecol 1993;168:1496–9.
Hoj L, Cardoso P, Nielsen BB, et al. Effect of sublingual misoprostol on severe postpartum haemorrhage in a primary health centre in Guinea-Bissau: randomised double blind clinical trial. BMJ 2005; 331: 723.
Kitzinger S. The new pregnancy and childbirth, 4th edn. London: Dorling Kindersley 2003.
Le Ray C, Serres P, Schmitz T, et al. Manual rotation in occiput posterior or transverse positions: risk factors and consequences on the cesarean delivery rate. Obstet Gynecol 2007;110:873–9.
National Collaborating Centre for Women’s and Children’s Health (NCCWCH). Intrapartum Care. London: RCOG Press 2007.
O’Driscoll K, Meagher D, Boylan P. Active management of labour, 3rd edn. London: Mosby 1993.
Odent M. Birth and breastfeeding: rediscovering the needs of women during pregnancy and childbirth. Forest Row: Clairview Books 2003.
Philpott RH, Castle WM. Cervicographs in the management of labour in the primigravida. II. The action line and treatment of abnormal labour. J Obstet Gynaecol Br Commonw 1972;79:599–602.
Rogers J, Wood J, McCandlish R, et al. Active versus expectant management of third stage of labour: the Hinchingbrooke randomised controlled trial. Lancet 1998;351:693–9.
Sizer AR, Evans J, Bailey SM, Wiener J. A second-stage partogram. Obstet Gynecol. 2000;96:678–83.
Thornton JG, Lilford RJ. Active management of labour: current knowledge and research issues. BMJ 1994;309:366–9.
Maternal collapse Definition
Maternal collapse can occur for many underlying reasons. It describes a reduction in the level of consciousness related to cerebral hypoperfusion or a primary neurological insult. If not promptly diagnosed and managed then there is a significant risk of serious long-term morbidity and mortality. Epidemiology
• The UK confidential enquiry into maternal death gives prevalence of maternal death due to specific conditions. Data regarding the incidence of maternal collapse where the woman recovers is less good as the condition is not a single entity. Likewise data regarding the incidence worldwide is very poor, as in most developing countries figures are not collected. Overall like maternal death, collapse is a very rare occurrence in developed countries and this creates issues related to training. The World Health Organization (WHO) publishes statistics on maternal mortality by country and these data are a stark reminder of the inequities in healthcare that exist around the world.
• Pregnancy is an independent risk factor for a number of conditions that can cause collapse:
• thromboembolism (pulmonary embolus) 5 ? increase in risk
• ischaemic stroke 9 ? increase in risk in the puerperium
• haemorrhagic stroke 26 ? increase in risk
• subarachnoid haemorrhage 20 ? increase in risk.
• The incidence of some of the important causes of collapse in pregnancy in developed countries are
• cardiac arrest in pregnancy 1 in 30 000 pregnancies
• myocardial infarction 1 in 10 000
• amniotic fluid embolism 1 in 8000–20 000
• septic shock 1 in 800
• massive postpartum haemorrhage (blood loss of more than 1500 mL) 1 in 200
• Certain maternal characteristics are associated with an increased risk of collapse: increased maternal age, social deprivation, late booking, lack of antenatal care, pre-existing maternal disease (e.g. cardiac, diabetes), maternal obesity (BMI >30), asylum seekers.
• Drugs used during pregnancy may result in maternal collapse due to toxicity or anaphylaxis:
• magnesium (eclampsia/pre-eclampsia)
• antibiotics (group B Streptococcus prophylaxis/pyrexia treatment)
• lignocaine/bupivicaine (epidural and local anaesthetic)
• synthetic prostaglandins (postpartum haemorrhage possibly due to coronary artery spasm)
• latex (gloves, catheters)
• blood products (blood transfusion, coagulation factors).
• A past medical history of certain conditions increases the risk of collapse in pregnancy:
• pre-existing cardiac disease increases the risk of collapse due to ischaemia, arrhythmia, or cardiac failure
• Marfan’s syndrome increase the risk of aortic dissection
• essential hypertension cardiomyopathy
• inherited thrombophilia pulmonary embolism Prevention
Appropriate antenatal care
All women should be seen by a healthcare professional at an early stage in pregnancy to allow a full history to be taken; in the UK this visit is recommended to occur before the end of the thirteenth completed week of gestation. This will allow the identification of risk factors increasing the risk of a disease process occurring that will result in collapse. This allows the care of the pregnancy to be planned with optimization of underlying disease and the use of prophylactic treatments to reduce the chances of collapse occurring. Pre-conception counselling and support should be offered to all women of childbearing age with any serious pre-existing medical or mental health problem. This should include women with significant risk factors such as obesity.
Modified obstetric early warning systems
Early warning signs of impending maternal collapse often go unrecognized, and this has led to the recommendation that modified early obstetric warning system (MEOWS) with the routine use of early warning charts that allow changes in vital signs to be flagged up and referred are used in all units. Such charts are already used in critical care units.
Training skills and drills
Maternal collapse although very serious is a rare occurrence even in a busy maternity unit, and individuals will have only rare exposure to clinical occurrences. It is therefore essential that all units have regular ‘skills’ training sessions and that mock ‘drills’ of maternal collapse are scheduled to allow staff to practise management and reflect on this process. There are now a number of courses that aim to teach the essential skills and team working. Aetiology
Maternal collapse may be due to a number of different causes (see individual entries).
Non-serious causes
Although these are common, more serious causes of collapse must always be considered prior to making these diagnoses:
• hyperventilation
• vasovagal attack (faint).
Potentially life-threatening causes of collapse
Haemorrhagic causes
• Massive antepartum haemorrhage (abruption or placenta praevia)
• Massive intrapartum haemorrhage (abruption or uterine rupture)
• Massive postpartum haemorrhage (uterine atony, genital tract trauma including uterine rupture, retained placenta)
• Rupture of a splenic artery aneurysm,
• Liver capsule rupture
• Ruptured aortic aneurysm.
Neurological (cerebral)
• Eclampsia
• Haemorrhagic stroke
• Ischaemic stroke
• Subarachnoid haemorrhage
• Cerebral arterial/venous thrombosis.
Cardiac/pulmonary
• Tension pneumothorax
• Amniotic fluid embolism
• Pulmonary embolism
• Severe pulmonary oedema (pre-eclampsia)
• Cardiomyopathy
• Myocardial infarction
• Dissecting aortic aneurysm
• Pre-existing cardiac disease
• Heart failure or arrhythmia.
Non-haemorrhagic
• Hypogylcaemia
• Uterine inversion
• Septic shock
• Drug toxicity
• Anaphylaxis
• Anaesthetic complications
• Suicide attempts (poisoning). Prognosis
In developed countries maternal mortality is a rare event. In the UK, the confidential enquiry into maternal death collects statistics regarding death due to particular conditions. However, the morbidity associated with maternal collapse is less well documented. Prompt management will improve prognosis and reduce the risk of long-term disability. Clinical approach
In cases of collapse, history taking, examination, and resuscitation must all occur simultaneously to reduce delay in diagnosis and management. This is often called the primary survey.
Team-working is essential and a call for help from other disciplines is essential and should be immediate:
• osenior obstetrician
• ojunior obstetrician(s) to assist and for training
• oexperienced anaesthetist
• senior midwife
• junior midwife to assist and for training
• porter to take sample to laboratory
• recorder to note times of steps in resuscitation
• the cardiac arrest team may be requested if respiratory or cardiac arrest is suspected at the time of collapse
• the appropriate specialists (e.g. neurologist, cardiologist) should be involved in management early where specific pathologies are suspected.
• the laboratory should informed if a major obstetric haemorrhage is suspected.
Diagnosis
History
• A history should be obtained from people witnessing the collapse as the behaviour leading up to the event may give indicators to the underlying cause.
• All history taking is simultaneous with assessment and resuscitation, which must be commenced without delay.
• Antenatal or intrapartum risk factors should be established from a relative or midwife. An individual not essential to resuscitation can review the notes and report to the resuscitation teams relevant findings.
Examination
Initial examination is based on the identifying life-threatening problems to allow appropriate resuscitation. However the possible causes of collapse must be identified as soon as possible to allow appropriate management.
• Is the woman responsive?
• Is she fitting?
• Pulse, BP, capillary filling time, heart auscultation?
• Respiratory rate, tracheal position, auscultation for air entry.
• Abdominal palpation for rebound/guarding, uterine tenderness, tone and size.
• Vaginal examination for bleeding &and cervical dilatation.
• Fetal heart auscultation to assess whether fetus is alive.
Monitoring
• Intravenous access must be established using wide-bore peripheral cannulae or central venous line.
• Pulse, non-invasive blood pressure, oxygen saturation, and ECG monitoring should be commenced in all cases.
• A urinary catheter should be inserted after initial resuscitation.
• Consider arterial and central venous pressure lines.
• Fetal monitoring is a secondary consideration to maternal monitoring. Fetal hypoxia will occur if the mother is hypotensive for any reason. Maternal resuscitation must always take priority over any fetal consideration, and ultimately the best way to resuscitate the fetus is to resuscitate the mother. Delivery should only be considered once the woman has been stabilized or if cardiac arrest has occurred and resuscitation is unsuccessful at 5 minutes.
Investigations
• Group and cross-match.
• A full blood count, coagulation screen, full liver and renal profile and C-reactive protein (CRP) should be sent in all women
• Selective investigations depending on differential diagnosis
• Arterial blood gases
• A bedside assessment of blood glucose (backed-up by a laboratory sample)
• A 12-lead ECG
• Chest X-ray
• Abdominal/pelvic ultrasound to assess fetal position and presence of free fluid
• Consider need for specialist investigations CT/MRI, CTPA, echocardiography
Management and immediate resuscitation
Assessment and resuscitation occur simultaneously with the aim of identifying life-threatening problems in the order that they will cause death. It is imperative that the steps are performed in order with movement onto the next step only once any identified problem has been corrected.
Tilt
A 30-degree left lateral tilt should be instituted for all women greater than 20 weeks’ gestation. A tilt is recommended for collapse in the immediate puerperium when a clot-filled uterus may still cause significant caval compression. This can be achieved by the use of a wedge or by manual displacement if a wedge is not available.
Step A AIRWAY
• Visually assess airway by looking in mouth.
• Suction if necessary to clear secretions or vomit.
• Consider possible airway obstruction.
• Causes of airway obstruction (rare in pregnancy):
• severe pre-eclampsia with swelling of the tongue and larynx
• post-fitting tongue oedema due to biting
• smoke inhalation
• trauma (road traffic accident).
• In an unconscious or semi-conscious woman the tongue may fall back and a head tilt/chin lift manoeuvre or a jaw thrust may improve the patency of the airway.
• An airway adjunct such as an oropharyngeal (Guedel) airway can be considered in an unconscious woman but may not be tolerated in a conscious or semi-conscious woman).
• The airway must remain patent and if breathing and circulation are confirmed the woman should be moved into the ‘recovery’ position.
Step B Breathing
• The respiratory system should be assessed, initially by looking, listening, and feeling for evidence of spontaneous respiration (no more than 10 seconds).
• If not breathing a respiratory arrest is diagnosed and a cardiac arrest call should be made.
• Commence assisted ventilation with a pocket mask or a bag and valve mask.
• Intubation should be performed as soon as an anaesthetist arrives to give assistance.
• Causes of respiratory arrest:
• drug toxicity (lignocaine or magnesium sulphate)
• total spinal anaesthesia
• amniotic fluid embolism
• anaphylaxis.
• A witnessed respiratory arrest may not progress to cardiac arrest if effective assisted ventilation is commenced promptly. However, an untreated respiratory arrest will rapidly progress to collapse (cerebral hypoxia) and cardiac arrest (myocardial hypoxia).
• If breathing spontaneously commence high-flow oxygen (facemask with a non-rebreathing bag gives 60% oxygen) at 15 L/minute should be administered.
• If breathing is occurring respiratory rate (normal 12–20) and oxygen saturation (normal >95%) should be checked and if these are abnormal repeat a full respiratory examination (with chest expansion observation, percussion and auscultation).
Step C Circulation
• The pulse should be checked (simultaneous to the assessment of breathing by checking the carotid pulse).
• The blood pressure, pulse (normal Professional counselling may be required to reduce post-traumatic stress. The risks of recurrence in a future pregnancy must be discussed and any preventative strategies that can be used in a future pregnancy.
• Contraceptive advice should be offered to women who do not wish to have further children. Further reading
Al-Shabibi N, Penna L, Postpartum collapse. Curr Obstet Gynaecol 2006;16:72–6.
Clarke J, Butt M. Maternal collapse. Curr Opin Obstet Gynecol 2005;17:157–60.
Lewis G. Saving mother’s lives 2003–2005. London: CEMACH publications 2007.
Howell C, Grady K, Cox C. Managing obstetric emergencies and trauma: The MOET course manual. RCOG Press 2007. Internet resources
www.alsg.org
www.also.org.uk
www.resus.org.uk
www.cemach.org.uk Patient resources
www.jessicastrust.org.uk
Meconium-stained liquor Definition
Meconium is the sterile material produced by the fetal digestive tract. It is composed of material ingested by the fetus from the amniotic cavity, such as epithelial cells, lanugo, blood, amniotic fluid and is pigmented by bile. The majority of fetuses will not pass meconium in utero with passage occurring in the first few days after birth. A minority of fetuses pass meconium in utero, resulting in the amniotic fluid becoming stained with meconium.
Obstetric convention grades meconium:
• Grade 1 describes a large volume of amniotic fluid lightly stained with meconium.
• Grade 2 describes a good volume of amniotic fluid heavily stained with meconium.
• Grade 3 describes absent or reduced volume of amniotic fluid so that the meconium is very thick.
The terms light, moderate and heavy are equally acceptable. Whatever classification is used visual assessment has poor accuracy with studies showing high interoperator variability in grading. Epidemiology
Meconium stained liquor (MSL) occurs in 8–20% of all births after 34 weeks. The incidence increases with gestation with an incidence of more than 30% after 42 weeks’ gestation. Conversely, the incidence is lower in gestations below 34 weeks with an incidence of less than 5%. There are no other demographic associations and the incidence is expected to be the same worldwide. Aetiology
Meconium is passed due to active peristalsis of the fetal gut. Abnormal peristalsis of the bowel may occur due to an external stress, resulting in increased sympathetic drive in the fetus.
Normal variant
• Peristaltic activity in the bowel increases as central nervous system and gastrointestinal tract matures and thus the passage of meconium may occur without any particular stimulus as a part of normal physiology in some term fetuses. The incidence of MSL increases as gestation increases and may be normal in any fetus beyond 34 weeks’ gestation. MSL is usually only lightly (grade 1) stained as a normal variant.
• Passive pressure on the fetal abdomen can cause passage of meconium. Breech presentation may be associated with the passage of meconium in the late first stage and second stage due to pressure on the fetal abdomen as it descends in the pelvis. The meconium staining may appear moderate to heavy in this situation but is obviously fresh in nature.
• Women with obstetric cholestasis may have an increased incidence of MSL before and during labour, with a number of studies suggesting an incidence of up to 25% in term pregnancies and 18% in preterm pregnancies. The reasons for this increase are unknown.
Abnormal
• Many fetuses show an adrenergic stress response to developing hypoxia; this causes a developing tachycardia and may result in an increase in gut peristalsis with the development of intrapartum MSL; the staining is usually moderate to severe (grades 2 or 3) in these situations.
Not all fetuses with subacute hypoxia will pass meconium. Fetuses who experience a sudden severe hypoxic event such as uterine rupture may not pass meconium, and the absence of MSL in the presence of an abnormal fetal heart rate patterns in not reassuring.
• The passage of meconium has an association with perinatal infection. Fetal infection may result in a stress response with the passage of meconium. In addition to this, infection reduces the ability of a fetus to compensate for developing hypoxia. In preterm gestations, MSL has an association with listeria infection. However, this association is not strong and infections with common agents such as group B streptococcus need not present with MSL. Prognosis
The majority of labours complicated by MSL have normal outcomes, but the presence of MSL increases the risk of a number of adverse neonatal outcomes. The risk of poor outcome increases with the grade of meconium seen in the liquor (see Management).
Meconium aspiration
• MSL is a risk factor for meconium aspiration syndrome. Meconium aspiration most likely occurs as a result of fetal gasping in utero. A fetus will gasp in response to sudden severe hypoxia or when a gradual onset subacute hypoxia becomes severe. MSL meconium aspiration can be a life-threatening condition and is known to account for 2% of perinatal deaths. It is more likely to occur with heavy MSL than with light MSL but it can occur with both types. It may not be initially apparent at birth and therefore neonatal protocols should recommend increased surveillance of babies with MSL in labour. This will result in longer hospitalization for the majority of mothers and their babies where meconium aspiration does not occur.
Poor condition at birth and hypoxic ischaemic encephalopathy
• A fetus that is becoming hypoxic may pass meconium and thus MSL is a risk factor for poor neonatal outcome (low pH, low APGAR scores, neonatal seizures). Heavy MSL also implies a relative oligohydramnios, which has an association with placental insufficiency and more profound cord compression during labour. Fetal heart rate monitoring remains a valid tool even in the presence of meconium
Cerebral palsy
• As both meconium aspiration and severe hypoxic ischaemic encephalopathy (HIE) are associated with a long-term risk of mental retardation and cerebral palsy, this means that MSL is a risk factor for this outcome. However, the link is weak with MSL a common occurrence and cerebral palsy a rare outcome (3/10 000 births in England and Wales). However, among infants with meconium aspiration, recent research has suggested a risk of about 20% for cerebral palsy or global developmental delay. Clinical approach
Diagnosis
History
• Elicit history suggesting ruptured membranes.
• Confirm gestational age and history of onset of labour.
• Review antenatal history for risk factors for fetal hypoxia, chorioamnionitis or obstetric cholestasis.
Examination
• Maternal observations for signs of infection (pyrexia or tachycardia)
• Meconium staining can be assessed by looking at the colour of the liquor on a (white) pad. A speculum examination is only required if the diagnosis is uncertain or a high vaginal swab is required.
• Review of fetal heart rate pattern (if on continuous monitoring).
Differential diagnosis
• Women who have had antepartum haemorrhage can have greenish liquor due to blood products contaminating the liquor or a greenish discharge from blood breakdown products.
• Bile staining of the amniotic fluid may occur in fetuses with bowel obstruction (who are less likely to pass meconium).
• Vaginal infections such as thrush can cause a creamy greenish discharge. Initial management
Initial management decisions at diagnosis
• If there is MSL (light or heavy staining) following prelabour rupture of membranes after 34 weeks’ gestation, arrangements should be made for stimulation of labour as soon as possible. Conservative management is contraindicated for heavy MSL and is controversial even in light MSL at gestations above 37 weeks. Labour can be induced with prostaglandin or an oxytocin infusion, but continuous monitoring must be carried out throughout.
• If meconium is suspected with preterm prelabour rupture of membranes there is a high risk of perinatal infection. Clinical signs of infection should be reviewed (uterine tenderness, maternal or fetal tachycardia, pyrexia, offensive vaginal discharge) and investigations to assist in diagnosing chorioamnionitis should be sent (vaginal swab, white cell count, and C-reactive protein). In the absence of signs of infection, steroids should be given and labour stimulated after the course has been completed. If there is a high risk of chorioamnionitis, then delivery should be expedited even though the course of steroids has not been completed. Induction of labour in not absolutely contraindicated but the decision regarding mode of delivery should take into consideration the current likely fetal condition and the length of time likely to allow vaginal delivery. There is no evidence that Caesarean section improves the prognosis of an infected fetus as long as fetal hypoxia does not occur; however, an infected fetus is more likely to become hypoxic and thus if a long and difficult labour is anticipated (e.g. an unfavourable cervix in a primigravida) then delivery by lower segment caesarean section (LSCS) may offer benefits for neonatal prognosis.
• There is no evidence that amnio-infusion in women with MSL reduces the risk of meconium aspiration or other poor fetal outcomes, and it is not recommended for routine clinical practice.
• If the woman is in active labour management decisions depend on the grading of the liquor.
Grade 1 meconium
Review antenatal and intrapartum history carefully. Consider whether continuous electronic fetal monitoring (EFM) should be recommended if the labour is being monitored by intermittent ausculation. If any fetal heart rate abnormality is suspected, electronic fetal monitoring should be recommended immediately. If there are clinical factors that can explain the presence of meconium (usually post-term pregnancy) then the labour can be managed in the same way as a pregnancy with non-MSL; however, if the meconium staining increases the possibility of infection or hypoxia EFM must be considered immediately and the management plan changed accordingly. If any risk factor (or borderline risk factor) exists recommend fetal monitoring. If no risk factors exist intermittent auscultation can be continued but must be performed strictly according to guidelines for the first and second stages of labour (see Chapter 10.7, Fetal surveillance in labour) and the liquor should be reassessed regularly to see if the level of meconium staining is increased.
Grades 2 and 3 meconium
Continuous fetal heart rate monitoring should be recommended and commenced without delay. Further management
This depends of the fetal heart rate pattern.
Normal fetal heart rate
• No specific action is required but continuous monitoring should be continued. Regular vaginal examinations must be performed to ensure the labour is progressing normally. If labour progress is poor, then augmentation with syntocinon can be considered to reduce the length of labour. The risk of oxytocin is that subacute hypoxia is more likely to develop and so it is important that the fetal heart rate remains normal.
Suspicious fetal heart rate pattern
• The usual actions should be performed to try to improve the fetal heart rate pattern (see Section 10.7 Fetal surveillance). Syntocinon should be reduced or stopped if the uterus is contracting more than 4 in 10. Fetal blood sampling should be performed and repeated if normal in 30 minutes if the heart rate abnormality persists. If the repeat shows any deterioration in the pH and increase in the base excess then delivery should be expedited unless spontaneous delivery is likely in a short time (for example a multigravid woman in the late first stage). Any abnormal pH or base excess requires plans to be made for immediate delivery. If there is poor labour progress, syntocinon can only be considered if the pH of the fetus is stable.
Pathological fetal heart rate pattern
• A fetal blood sample can be considered if it is likely that vaginal delivery will be possible in a short time. However, if vaginal delivery is unlikely for a few hours and especially if there is con current poor labour progress, delivery by Caesarean section should be undertaken without fetal blood sampling. If an uncomplicated assisted vaginal delivery is possible, this should be recommended instead of fetal blood sampling. Oxytocin therapy should not be continued until the results of blood sampling are available. Management in special situations
Prematurity
• Meconium staining is very rare in gestations below 34 weeks. If MSL is noted then the possibility of chorioamnionitis should be considered even in the absence of any other clinical signs. Antibiotics are routinely prescribed in all preterm labours and consideration should be given to broad-spectrum antibiotics. Continuous fetal heart rate monitoring should be recommended and if the fetal heart rate pattern becomes suspicious delivery by caesarean section is recommended due to the reduced fetal reserve to cope with hypoxia. In cases of preterm prelabour rupture of membranes, a change in the colour of the liquor to green requires urgent review as the passage of meconium in this situation may be the first sign of chorioamnionitis. The diagnosis can be difficult as sometimes a greenish discharge may occur in the absence of passage of meconium (possibly due to the breakdown of blood in the cervical canal).
Home birth
• If grade 2 or 3 MSL is diagnosed during a homebirth, then transfer to hospital should be arranged unless the woman declines or transfer is impractical (e.g. second stage of labour). If grade 1 meconium is diagnosed then the clinical situation should be reviewed, including consideration of the ease that transfer to hospital can be arranged. Transfer to hospital is not mandatory if the woman is low risk with clinical features supporting the likelihood of the meconium being a normal variant (post-term pregnancy) and transfer can be achieved rapidly if required, but the threshold for transfer should be reduced if the labour progress is slow or any other problem develops. If the labour continues at home, careful auscultation of the fetal heart must occur throughout labour, neonatal resuscitation equipment should be available and checked, the hospital should be aware of the situation and in case of very heavy (grade 3) meconium an ambulance should be on standby for immediate neonatal transfer to hospital.
Gastroschisis and other fetal bowel obstruction
• The amniotic fluid may appear green in cases of fetal bowel obstruction but in these cases the passage of meconium is very unlikely, as the fetus is unable to ingest significant material to produce large volumes of meconium. The green staining in this situation most likely represents staining with bile. However, aspiration of bile stained liquor can also cause a severe aspiration syndrome and therefore severe fetal hypoxia must be avoided to prevent fetal gasping so that the finding should be managed as if it were heavy MSL.
Counselling
• If a woman declines continuous electronic fetal monitoring in spite of recommendation the reasons for monitoring should be discussed and documented. The association between MSL and meconium aspiration should be discussed and the importance of prompt diagnosis of hypoxia to try to prevent fetal gasping. Intermittent ausculation should be continued, but the woman must be informed that this may not diagnose subtle indicators of fetal hypoxia and result in a delay of up to 15 minutes of detecting even serious changes in the fetal heart rate.
Neonatal resuscitation
General comments:
• The need for a paediatrician/neonatal nurse practitioner to be present at delivery should be considered in any birth with light MSL. If the electronic fetal monitoring or intermittent auscultation is normal attendance is not mandatory.
• A paediatrician/neonatal nurse practitioner should be requested to be present at delivery of all babies with heavy MSL even if the monitoring is normal. If the fetal heart rate monitoring is abnormal the chance that the baby will require advanced neonatal resuscitation is increased, and appropriately experienced personnel should be asked to be present at the birth.
• Suctioning of the nose and mouth on the perineum prior to the delivery of the shoulders is not beneficial and is not required. As part of resuscitation the upper airway should only be suctioned if thick meconium is seen in the mouth.
• Further resuscitation depends on the condition of the baby
Depressed
A baby with a low heart rate and no breathing requires a trained individual to carry out suction under direct vision during laryngoscopy. Depending on the response to resuscitation these infants may require admission to a neonatal unit for careful observation.
Good condition
No suction or additional resuscitation is required in a vigorous baby.
Postnatal neonatal observation by midwifery team
The midwifery team performs neonatal observations after delivery and any abnormality requires urgent referral to a neonatologist for review. No special maternal observations are required.
Heavy meconium
The baby should be observed closely for signs of respiratory distress with observations at 1 and 2 hours and then 2 hourly until 12 hours of age. Observations should include general wellbeing and feeding, and assessment of heart rate, respiratory rate, temperature, capillary refill, muscle tone, and chest movements.
Light meconium
The baby should be observed at 1 and 2 hours as above, but if all is normal no special review is required after this.
Recurrence/future pregnancy planning
Women can be reassured that meconium is not a recurrent problem and that the risk in future pregnancy is the same as that in the general population. Induction of labour at 41weeks reduces the incidence of meconium aspiration and women who have experienced this outcome in a pregnancy may wish to discuss this option in future pregnancies. Further reading
Beligere N, Rao R. Neurodevelopmental outcome of infants with meconium aspiration syndrome: report of a study and literature review. J Perinatol 2008; 28 (Suppl 3): S93–101.
Clinical Effectiveness Support Unit, The use of electronic fetal monitoring, RCOG press 2001.
Gibb D, Arulkumaran S. Fetal monitoring in practice. Churchill Livingstone 2007.
National Collaborating Centre for Women’s and Children’s Health, Intrapartum Care: care of healthy women and their babies during childbirth-clinical guideline, RCOG press 2007.
Rao S, Pavlova Z, Incerpi MH, Ramanathan R, Meconium-stained amniotic fluid and neonatal morbidity in near-term and term deliveries with acute histologic chorioamnionitis and/or funisitis. J Perinatol 2001;21:537–40.
Xu H, Mas-Calvet M, Wei SQ, et al. Abnormal fetal heart rate tracing patterns in patients with thick meconium staining of the amniotic fluid: association with perinatal outcomes. Am J Obstet Gynecol 2009; 200: 283.e1–7. Internet resources
www.nice.org.uk/nicemedia/pdf/IPCNICEGuidance.pdf
www.rcog.org.uk/files/rcog-corp/uploadedfiles/NEBEFMGuidelineFinal2may2001.pdf Patient resources
www.patient.co.uk/showdoc/40000245/
www.pregnancy.about.com/od/laborcomplications/a/meconium.htm
Placenta praevia Definition
The implantation of a placenta in the lower uterine segment. This can cause potentially life-threatening antepartum and postpartum haemorrhage. Incidence
Four or five per 1000 pregnancies. Aetiology
Unknown cause. Risk factors
• Previous uterine scars
• Smoking
• Advanced maternal age
• Grand muliparity
• Recurrent miscarriage
• Low social class
• Infertility treatment.
Associations with placenta praevia
• Placental abruption
• Congenital malformations
• Abnormal presentations
• Preterm delivery Clinical presentation
History
• Painless vaginal bleeding, which may be catastrophic
• May be associated with labour
• Abdominal pain may occur as 10% of cases will have associated abruption, making diagnosis difficult
• In 30–50% of cases there may be no antenatal vaginal bleeding
• Usually normal fetal movements
• In most cases, a low placenta has already been identified at the 21–23-week scan.
Examination
• General condition and vital signs
• Abdominal assessment including lie of fetus to exclude malpresentation
• Fetal assessment: unlikely to show signs of compromise unless maternal compromise
• Vaginal examination is contraindicated as may exacerbate bleeding. Therefore, inspection should be carried out to quantify blood loss.
Investigations
• Full blood count
• Blood grouping and cross match
• Ultrasound to confirm placental site, presentation (Fig. 10.13.1)
Diagnosis
Placenta praevia is diagnosed with ultrasound, which is safe, accurate, and convenient. Transvaginal ultrasound is superior to the transabdominal approach and is safe (Fig. 10.13.2). Prior to routine use of ultrasound in antenatal care, the diagnosis was made on clinical examination in theatre. Screening for placenta praevia
The 20–22-week anomaly scan provides a screening test to predict the likelihood of placenta praevia at delivery.
Traditionally it is routine practice to repeat the scan in later pregnancy if the placenta is found to be low lying at 20–22 weeks. Evidence shows that unless the placental edge reaches or overlaps the internal os, the placenta is likely to have moved by the third trimester. The placenta is known to migrate as the pregnancy progresses and explains why midpregnancy ultrasound overdiagnoses placenta praevia. This apparent migration is due to the differential growth of the lower and the upper part of the uterus. The average rate of migration is 4.1 mm/week. In cases with significant overlap (>10 mm) the rate of migration was minimal at 0.1 mm/week. The rate of migration was higher if the placental edge is thin.
All cases where the placenta is less than 2 cm from the internal os at the anomaly scan should have a scan at 36 weeks.

Fig. 10.13.1 Abdominal ultrasound scan carried out at 22 weeks shows the placenta implanted over the internal os.

Fig. 10.13.2 Transvaginal scan showing the proximity of the placental edge to the internal os. The distance is measured by the markers.
Counselling
Women found to have a low-lying placenta at their anomaly scan should be advised
• that the majority of placentas will move by term and allow vaginal delivery
• if the placenta is anterior and there is a previous Caesarean section, it is more likely to remain low
• to seek medical advice if vaginal bleeding
• they should not have coitus in pregnancy if there is a history of vaginal bleeding
• need for rescan at 36 weeks
If a woman is confirmed to have placenta praevia at term it is essential to provide counselling on:
• the mode of delivery
• the possible need for blood products
• the potential need for additional surgical measures to control bleeding such as hysterectomy. Management
In 30–50% of cases of placenta praevia, there will be no antepartum bleeding. The RCOG guideline in the management of placenta praevia recommends extensive counselling of these women to assess their suitability for outpatient management and to consider factors such as proximity to hospital.
In the case of women who present with antepartum haemorrhage their management will depend on:
• the degree of bleeding and maternal compromise
• gestation.
Conservative management
• This is appropriate if the fetus is not mature and the bleeding is not compromising the mother.
• Corticosteroids should be administered before 34 weeks to promote fetal lung maturity.
• Tocolysis may be considered if there is no evidence of active bleeding and no fetal compromise.
• Transfusion of blood and blood products may be required.
• Anti-D is needed for Rhesus-negative mothers.
• The RCOG recommends that women who bleed with placenta praevia after 34 weeks be hospitalized until delivery.
Mode of delivery with placenta praevia
A trial of vaginal delivery is appropriate if the placental edge is at least 2 cm away form the internal os. If the placental edge is less than 2 cm from the os Caesarean section at 38 weeks is recommended
Caesarean section for placenta praevia
• Senior consultant obstetrician should be present
• Senior anaesthetist
• Availability of HDU facilities
• Counselling and obtain consent
• Usually able to perform traditional lower uterine segment Caesarean section
• May be surgically challenging due to poorly formed lower uterine segment and dilated veins
• Knowledge of whether the placenta is anterior or posterior. If anterior, it can usually be swept off the uterine wall and not cut in order to deliver the fetus
• May require additional procedures to control bleeding such as use of haemostatic balloon, uterine artery ligation, brace sutures and hysterectomy if intractable bleeding (Section 10.15, Postpartum haemorrhage.
• Be prepared for placenta accreta
• Increased incidence of postpartum haemorrhage. Advice for future pregnancies
The risk of recurrence is low. Placenta accreta
Definition
An abnormally firm attachment of placental villi to the uterine wall.
Incidence
Varies from 1 in 540 to 1 in 70 000. The incidence has increased by 10-fold, probably due to the increased caesarean section rate.
Pathology
Abnormally deep attachment of chorionic villi to the uterine wall with the absence of the normal intervening decidua basalis.
There are three variants:
• placenta accreta, where the placenta is attached directly to the myometrium
• placenta increta, where the placenta extends into the myometrium
• placenta percreta, where the placenta extends through the entire myometrium.
Risk factors include
• Placenta praevia
• Previous Caesarean section
• Advanced maternal age
• Grand multiparity
• Previous vigorous curettage
• Myomectomy
• Submucous myoma
• Asherman’s syndrome
• A short Caesarean to conception interval
Prognosis
Placenta accreta is associated with a 7% mortality rate in addition to increased morbidity caused by massive blood transfusion, infection, and damage to adjacent organs. The recent CEMACH report highlighted the need for women who have had previous Caesarean section and placenta praevia in their subsequent pregnancy to have further investigations to try and identify placenta accrete. This is with a view to developing safe management strategies for their delivery.
Diagnosis
Imaging using ultrasound has limited ability to exclude placenta accreta. Anticipation of placenta accreta in cases with identifiable risk factors is likely to be the most useful strategy.
Presence of multiple linear irregular vascular spaces within the placenta on ultrasound has the highest positive predictive value for prospective identification of placenta accreta. In the largest series, placental lacunae with turbulent flow was associated with a 80–90% sensitivity for detection of placenta accrete. Colour Dopplers and magnetic resonance imaging have not been sufficiently studied, but may be helpful.
Management
• Adequate counselling pre-delivery regarding possible hysterectomy
• Availability of blood and blood products
• Experienced obstetrician with other specialists available
• Pre-surgery radiologically assisted cannulation of uterine arteries for embolization should there be massive bleeding
• Leaving placenta in situ and tying off the umbilical cord if there is no bleeding to conserve the uterus
• There is no evidence for use of methotrexate in cases of placenta percreta if placenta was left behind after delivery Vasa praevia
Definition
Fetal blood vessels unsupported by either the placenta or umbilical cord traverse the membranes in the lower segment of the uterus.
Incidence
Approximately 1 in 6000 deliveries.
Prognosis
If these vessels precede the presenting part they can rupture and lead to fetal haemorrhage. The perinatal loss rate has been reported as high as 33–100%.
Diagnosis
Can be diagnosed by ultrasound showing echogenic parallel or circular lines near the cervix representing the umbilical cord. This finding can be confirmed using Doppler.
Higher incidence in women who have had a low-lying placenta in second trimester which later recedes.
Women may present with intrapartum bleeding, and cardiotocography (CTG) abnormalities if antenatal diagnosis has been missed.
Management
If a prospective diagnosis has been made, delivery by Caesarean section at or near term is recommended. Emergency Caesarean will be needed if the diagnosis is made intrapartum.
Antepartum identification of vasa praevia leads to significant improvement in perinatal mortality. Further reading
Placenta previa and placenta previa accreta: Diagnosis and mamangement. Green top guideline No. 27, Royal College of Obstetricians and Gynaecologists, 2005.
Bhide A & Thilaganathan B. Recent advances in the management of placenta previa. Curr Opin Obstet Gynecol 2004;16:447–51.
Saving mothers lives. The Seventh Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom, 2007: www.cemach.org.uk Internet resources
Causes of Maternal Mortality: www.maternityworldwide.org/causes.html.
Placental abruption Definition
Complete or partial separation of a normally implanted placenta. Incidence
0.52–1.29% of all pregnancies.
30–35% of cases of antepartum haemorrhage with recognized causes are due to placental abruption. Complications of placental abruption
Fetal
• Prematurity
• Hypoxia
• Death
• Hypoxic brain injury.
Maternal
• Hypovolaemia due to blood loss
• Coagulopathy
• Renal failure
• Postpartum haemorrhage. Pathology
Placental abruption is multifactoral
• An association of reduced invasiveness of the cytotrophoblast, which leads to inadequate placentation
• Dysregulation of the maternal immune response
• Folate deficiency has been shown to have an association
It is postulated that arterial spasm followed by relaxation and subsequent venous engorgement and arteriolar rupture into the decidua basalis with the accumulation of blood clot causes the separation of the placenta.
Two of the potential mechanisms of abruption are:
• acute inflammation-related conditions
• chronic inflammation or vascular dysfunction. Risk factors for placental abruption
Pre-pregnancy
• Previous history of abruption
• Previous Caesarean section
• Uterine malformations
During pregnancy
• Smoking
• Alcohol abuse
• Placenta praevia
• Pre-labour rupture of membranes
• Hypertension/pre-eclampsia
• Cocaine use
• Choriomanionitis
• Positive uterine artery Doppler screen in the second trimester.
Other risk factors for abruption have historically been reported but not conclusively proven in large series on abruption. These include
• assisted conception
• polyhydramnios and oligohydramnios
• maternal diabetes
• uterine trauma
• external cephalic version
• short umbilical cord and velamentous insertion of cord
• coagulation defects
• invasive intrauterine procedures like amniocentesis. Clinical presentation
History
• Painful vaginal bleeding is the most common presentation. This occurs in 70–80% of patients and may be very heavy. In other cases, there may be no vaginal bleeding if the abruption is concealed.
• Abdominal pain.
• Reduced or absent fetal movements.
Examination
• Tender and irritable uterus is the classical clinical feature.
• The uterus may be tonically contracted making fetal palpation difficult.
• Signs of shock: pallor, tachycardia, hypotension.
• Coexisting hypertension may mask fall of blood pressure due to blood loss.
• Signs of fetal distress may be present if the fetus is alive. The fetus may be dead at presentation.
Investigations
• Full blood count
• Coagulation screen
• Blood for grouping and cross match
• Urea and electrolytes
• Assessment of fetal wellbeing.
Diagnosis
• The diagnosis is based on the clinical presentation and examination findings
• Ultrasound is not sensitive in the diagnosis of abruption but is useful to exclude placenta praevia, confirm fetal viability, and presentation Management
The management will be depend on the grade of abruption and the gestation. Severe cases of placental abruption can make the mother very unwell.
• Delivery is usually required in cases of placental abruption. Conservative management is rarely justified other than in the very minor abruptions.
• Replace blood volume.
• In women presenting with placental abruption and intrauterine fetal death, preparations for blood transfusion should be commenced as there is likely to have been a major placental separation with significant retroplacental blood loss.
• Look for and correct clotting abnormality.
• Involve senior obstetrician.
• Multidisciplinary team involvement of anaesthetist, haematologist, and neonatologist. In cases of severe bleeding an interventional radiologist and vascular surgeon may be needed.
• Decision regarding delivery.
Vaginal delivery
May be appropriate if
• abruption occurs near term and the maternal and fetal condition is reassuring
• abruption occurs in labour and delivery can be expedited
• if there is fetal demise and Caesarean delivery is to be avoided
• there are no other contraindications to vaginal delivery such as abnormal lie or previous Caesarean section
• complications such as disseminated intravascular coagulation (DIC), which increase the risks of blood loss with surgical management
if vaginal delivery is attempted there must be close surveillance of maternal and fetal condition during labour as the clinical picture may deteriorate rapidly.
Caesarean delivery
Is appropriate for
• abruption with signs of significant fetal compromise
• abruption which has significantly compromised maternal condition such that waiting for vaginal delivery could be life-threatening
• in cases of fetal demise if there is a failed attempt at vaginal delivery. This may occur if the uterus becomes atonic as a result of blood infiltrating the myometrium (Couvelaire uterus)
Care of the baby
• In most cases, there is insufficient time for benefit with antenatal steroid administration.
• Neonatologists should be alerted to anticipate birth of a preterm (if the abruption is in preterm period) and hypoxic baby. Counselling
Counselling is difficult due to the unpredictable nature of abruption. However, it is important to keep the mother and her partner well informed, including the need for blood products and the potential need for additional haemostatic measures such as uterine artery ligation or hysterectomy.
With all deliveries there must be provision made for
• NNU facilities for the birth of a potentially hypoxic or acidaemic fetus.
• The need for HDU/ITU facilities for the mother. Management of complications
Delay in treating abruption increases the risk of hypovolaemic shock, coagulation failure, renal failure and post partum haemorrhage.
In cases of concealed abruption the degree of shock may be out of proportion with the blood loss seen before delivery. Disseminated intravascular coagulation
The progressive separation of the placenta releases thromboplastin-like substances that activate the coagulation cascade. This activation consumes coagulation factors, which leads to secondary thrombocytopenia. Which in turn triggers the formation of fibrin degradation factors and D dimers.
Complications of DIC
These include
• renal failure
• pulmonary hypoperfusion
• PPH
• postpartum pituitary necrosis.
Clinical signs of DIC
Bleeding from multiple sites, e.g. wound, venepuncture, gums.
Diagnosis of DIC
• Prolonged prothrombin time (PT) and partial thromboplastin time (PTT)
• Low fibrinogen (2000 mL). The Scottish Confidential Audit of Severe Maternal Morbidity defines an estimated blood loss ≥2500 mL, or transfused 5 or more units of blood, or received treatment for coagulopathy (fresh frozen plasma, cryoprecipitate, platelets) as ‘major haemorrhage’. These definitions are rather arbitrary as visual assessment of blood loss is unreliable. The effect that haemorrhage has on the woman depends not only on the amount, but also on the rapidity of blood loss, on her blood volume and any underlying health factors. For this reason a definition would include any blood loss that causes a significant haemodynamic change. Primary PPH occurs within the first 24 hours after delivery, and secondary PPH occurs between 24 hours and 6–12 weeks postpartum. Epidemiology
Postpartum haemorrhage (PPH) occurs in 5–15% of deliveries. PPH is the most common cause of maternal mortality and accounts for one-quarter of all maternal deaths worldwide. Fourteen million cases of PPH occur each year with a case fatality rate of 1%. In the UK, PPH is the third most common cause of maternal mortality and accounts for 10.6% of all direct maternal deaths according to the Confidential Enquiries into Maternal and Child Health. Aetiology and risk factors
The major aetiological factors of PPH are uterine atony (tone), retained placental tissues (tissue), membranes or blood clots, genital tract trauma (trauma), and coagulation abnormalities (thrombin).
Overdistension of the uterus due to multiple pregnancy, polyhydramnios, or fetal macrosomia is a common risk factor for PPH by increasing the risk of uterine atony. Other risk factors for PPH include placental abruption or placenta praevia, antepartum haemorrhage, pre-eclampsia, obesity, coagulation disorders, primigravidity, chorioamnionitis, prolonged rupture of membranes, fibroid uterus, previous Caesarean delivery, induction of labour, prolonged labour, instrumental delivery, and prior PPH. However, PPH can occur even in women without identifiable risk factors. Pathophysiology
Following delivery of the fetus, myometrial contraction results in placental separation and constriction of the blood vessels by retracting myometrial fibres (‘living ligatures’). Uterine atony or retained placenta causes a failure of this mechanism and bleeding from the placental bed. Young and healthy women can compensate for moderate blood loss without demonstrating any haemodynamic changes. When up to 20% of the blood volume is lost, the perfusion of non-vital organs and tissues is decreased, with pale and cool skin as a common clinical feature. Moderate shock occurs when 20–40% of the blood volume is lost resulting in decreased perfusion of visceral organs (liver, the gut, and kidneys) resulting in oliguria or anuria, hypotension, and tachycardia. When 40% or more of the blood volume is lost, severe shock results in decreased perfusion of the essential organs, the heart and brain, leading to restlessness, coma, and possibly cardiac arrest. Prevention
Prevention of PPH may be feasible with identification and modification of risk factors antenatally, and appropriate management of labour and delivery. Anaemia or other health conditions should be diagnosed and treated. Women with risk factors for PPH should have their haemoglobin levels as well as general health status optimized in anticipation of PPH and should be delivered in centres with transfusion facilities and an intensive care unit (ICU). However, it is not possible to predict and prevent all cases of PPH, as only 40% of women who develop PPH have an identified risk factor.
Active management of the third stage of labour consists of administration of uterotonic agents, controlled cord traction and uterine massage after delivery of the placenta. The aim of these interventions is to facilitate the delivery of the placenta by increasing uterine contractions and to prevent uterine atony and PPH. This approach reduces the risks of PPH, postpartum anaemia, blood transfusion requirements, prolonged third stage of labour, and use of therapeutic drugs for PPH. The International Confederation of Midwives (ICM) and the International Federation of Gynecology and Obstetrics (FIGO) advocate active management of the third stage of labour for all women. It is recommended that active management should be routine for maternity hospitals and births at home or birth centres.
Oxytocin is a first-line uterotonic agent in active management as it is effective 2–3 minutes after injection and has minimal side-effects. Other uterotonics include ergometrine maleate, ergometrine with oxytocin 5 IU/mL (Syntometrine, Alliance Pharmaceuticals), misoprostol, or carbetocin. Misoprostol (Cytotec, Pfizer), a prostaglandin E1 analogue, is more stable than oxytocin and has been administered by oral, sublingual, and rectal routes; however, misuse of misoprostol can lead to significant maternal morbidity and even death. The main side-effects are nausea, vomiting and diarrhoea, shivering, and pyrexia. A Cochrane review on the use of prostaglandins for the prevention of PPH concluded that neither intramuscular prostaglandins nor misoprostol is preferable to conventional injectable uterotonics as part of the management of the third stage of labour, especially for low-risk women. Carbetocin is a long-acting oxytocin agonist, which has been used for the prevention of PPH. Intramuscular carbetocin has longer duration of action than intramuscular oxytocin, but there is insufficient evidence that intravenous carbetocin is as effective as oxytocin to prevent PPH. A Cochrane review suggests that carbetocin is associated with reduced need for additional uterotonic agents and uterine massage, and there are no significant differences in adverse effects between carbetocin and oxytocin.
Although the active management of the third stage of labour originally included early cord clamping, delayed cord clamping is associated with less anaemia, intraventricular haemorrhage, and late-onset sepsis, especially in preterm infants. As there is little evidence to suggest that the timing of cord clamping has an impact on the incidence of PPH, the collaborative ICM/FIGO group decided not to include early cord clamping in the active management protocol. The cord may be clamped at the time the baby is dried and wrapped and passed to the mother to breastfeed.
FIGO also advises that if oxytocin or misoprostol are unavailable, skilled birth attendants should use physiological (or expectant) management of the third stage. This means that cord traction should not be applied before the uterus has contracted and placental separation has begun. The placenta should be allowed to be delivered without interference. Early or prophylactic interventional radiology for the prevention of PPH should be considered for high-risk cases. Treatment
Medical management
Early diagnosis, prompt resuscitation, and restoration of the blood volume lost are essential in the initial management of PPH. Major PPH should be managed by a multidisciplinary team approach with senior obstetricians, anaesthetists, midwives, and theatre staff. Haematologists, blood bank staff, hospital porters, and the intensive care unit should be alerted.
General resuscitation measures include assessment of the woman’s haemodynamic status, level of consciousness, blood pressure, heart rate, and oxygen saturation. Two large-bore cannulae should be inserted and blood samples taken for full blood count, group, and cross-match (the number of units will depend on the severity of haemorrhage), coagulation screen, and renal and liver profiles.
Fluid resuscitation should be based on the volume and rapidity of blood loss. A total volume of up to 2l of warmed Hartmann’s solution should be given rapidly and followed by up to a further 1.5 L of warmed colloid until cross-matched blood is available, as most of the infused fluid shifts from the intravascular to the interstitial space.
A systematic examination to identify the cause of PPH should be undertaken simultaneously with resuscitation and treatment measures. Assessment of the uterine size and tone should be followed by vigorous uterine massage and administration of uterotonic agents if the uterus is atonic. Uterine massage, manually or bimanually, is a simple and very effective first-line measure and reduces bleeding even if the uterus remains atonic, allowing resuscitation to take effect. Manual exploration of the uterine cavity is essential to exclude or remove retained placental tissues and membranes and is best done with sufficient anaesthesia. If bleeding persists despite a well-contracted uterus, examination under anaesthesia should look for cervical or vaginal lacerations, as these may extend into the uterus or the broad ligament or they may cause pelvic haematomas. If retained tissue or trauma is excluded and bleeding continues despite a well-contracted uterus, a coagulation disorder as a possible cause should be excluded.
Uterotonic agents
As uterine atony is the most common cause, medical management consists of slow intravenous oxytocin (10 units) or ergometrine (0.5 mg), methergine 0.2 mg intramuscularly, oxytocin infusion, 15-methyl PGF2α (Carboprost or Haemabate) intramuscularly or intramyometrially, dinoprostone vaginally or rectally, or misoprostol.
Oxytocin, can be administered as slow intravenous bolus of 5 units or as an infusion (40 units in 500 mL of 0.9% normal saline, infused at a rate of 125 mL/hour) in order to maintain uterine contractions. Although there are no absolute contraindications, an antidiuretic effect may develop with high doses.
Ergometrine is an ergot alkaloid. Hypertension and cardiac disease are contraindications as ergometrine can potentially cause severe hypertension and myocardial ischaemia.
Carboprost (Haemabate; Pfizer, Pharmacia & Upjohn, Kalamazoo, MI) is a prostaglandin F2 analogue, which is administered intramuscularly or intramyometrially. It is a second-line agent for uterine atony (0.25 mg repeated every 15 minutes to a maximum dose of 2 mg). This is 80% to 90% effective in arresting PPH in cases that are refractory to oxytocin and ergometrine. It has bronchoconstrictive properties and is contraindicated in asthma. Side-effects include diarrhoea, vomiting, fever, headache, and flushing.
Dinoprostone (Prostin) is a prostaglandin E2 analogue that may be given vaginally (may get washed off with blood) or rectally. It can cause temperature elevations. It should be stored at –20°C (–4°F) and brought to room temperature before use. This is a limitation for its use in acute severe haemorrhage.
Misoprostol is a synthetic prostaglandin E1 analogue. As the time taken for peak serum concentration of oxytocin is much shorter than oral misoprostol, which reaches its serum peak concentration at 20 minutes, a combination of these two agents could provide a sustained uterotonic effect. However, a Cochrane review concluded that there is insufficient evidence that the addition of misoprostol is superior to the combination of oxytocin and ergometrine.
Recombinant activated factor VII (rFVIIa, NovoSeven; Novo Nordisk, Bagsvaerd, Denmark) has originally been used in treating haemorrhage in patients with haemophilia or other bleeding disorders. It has also been used in nonhaemophilic haemorrhage, including life-threatening obstetric haemorrhage and may be considered as an alternative haemostatic agent when the standard treatment is ineffective.
Transfusion
Blood and blood product transfusion should be commenced if bleeding continues, if the estimated blood loss is over 30% of the blood volume, or if the patient is haemodynamically unstable despite aggressive resuscitation. Group-specific or O group, Rh-negative blood should be transfused until cross-matched blood becomes available. Dilutional coagulopathy occurs when approximately 80% of the original blood volume has been replaced. Four units of fresh frozen plasma (FFP) should be administered with every 6 units of blood transfused (12–15 mL/kg or total 1l). Platelet concentration should be more than 50 ? 109/L or more than 80–100 ? 109/L if surgical intervention is likely. Cryoprecipitate should be administered if there is disseminated intravascular coagulation (DIC) or if the fibrinogen level is less than 1 g/L.
Surgical management
Ongoing bleeding indicates the need to transfer and assessment in the operating theatre. Bimanual compression and direct pressure over lacerations may help control bleeding while resuscitation continues and preparations are made for surgical intervention. Obstetricians must consider all available interventions to stop haemorrhage, including balloon tamponades compression sutures, uterine artery embolization, pelvic devascularization, or radical surgery.
Uterine tamponade
Uterine balloon tamponade has been used as a prognostic test (‘tamponade test’) and is therapeutic, with success rates between 70% and 100%. The anterior lip of the cervix is secured with a sponge forceps and a balloon catheter (usually a Sengstaken-Blakemore catheter) is inserted into the uterine cavity. The balloon is then filled with warm sterile water or a warm saline solution until it becomes visible in the cervical canal. When the pressure exceeds that of the pressure with which blood is entering the uterine cavity, the bleeding should stop. If there is no bleeding, the ‘tamponade test’ result is successful and no further fluid is added. The ‘tamponade test’ allows the obstetrician to identify which women will require laparotomy. Advantages include easy and rapid insertion with minimal anaesthesia, rapid identification of failed cases and painless removal. No immediate complications such as bleeding or sepsis, or long-term sequelae such as menstrual problems or problems with conceiving have been reported in women who underwent uterine tamponade. If bleeding continues despite the ‘tamponade test’, laparotomy and compression suture should be next step.
Compression sutures
In cases of PPH at the time of Caesarean section or in cases of failed ‘tamponade test’, if haemostasis is achieved with bimanual compression of the uterus, compression sutures are likely to arrest haemorrhage. The ease of application is an advantage, and fertility is preserved. The obvious disadvantages are the need for laparotomy and usually hysterotomy (although some modified types to the original ‘B-Lynch’ suture technique have avoided this surgical step). Complications are extremely rare and include erosion through the uterine wall, pyometra, and uterine necrosis.
Pelvic devascularization
Failure of compression sutures to arrest haemorrhage warrants stepwise pelvic devascularization by ligation of the uterine, ovarian, and finally internal iliac arteries. This procedure is usually effective but it can be time-consuming. Ligation of internal iliacs can be technically challenging and carries risks of surgical injury. Prerequisites include a haemodynamically stable patient and surgical expertise. The reported success rates vary between 40% and 100%. When arterial ligation fails, hysterectomy is usually associated with higher morbidity than a hysterectomy without previous attempted arterial ligation.
Uterine artery embolization
Arterial embolization has success rates as high as 70–100% and the potential of preservation of fertility. Prophylactic embolization may have a role in a planned Caesarean section with a morbidly adherent placenta. Complications include haematoma formation, infectious complications, contrast-related side-effects, and ischaemia resulting in uterus and bladder necrosis. The requirement of equipment and an interventional radiologist are limitations of this procedure.
A systematic review of the management of PPH when medical measures fail showed that the success rates for arresting PPH are as high as 84.0% for balloon tamponade, 90.7% for arterial embolization, 91.7% for compression sutures, and 84.6% for pelvic devascularization (including uterine or internal iliac artery ligation). As none of these methods is significantly superior to any other, the choice should depend on the availability of facilities, the degree of ongoing bleeding, the estimated blood loss, and the haemodynamic status of the woman.
Hysterectomy
Subtotal or total abdominal hysterectomy is usually the last resort in the management of PPH and should not be delayed if the conservative measures have failed. Hysterectomy is associated with numerous postoperative complications, including urinary tract injury, fistula formation, bowel injury, vascular injury, pelvic haematoma, and sepsis. Subtotal hysterectomy may not be effective when the cause of the bleeding is at the lower segment, cervix, or vaginal fornices. Further reading
CEMACH. Saving mothers’ lives: reviewing maternal deaths to make motherhood safer. 2003–2005. The Seventh Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. CEMACH: London 2007.
Clinical Management Guidelines for Obstetrician-Gynecologists. ACOG Practice Bulletin: Number 76, October 2006: Postpartum Hemorrhage. Obstet Gynecol 2006;108:1039–47.
Condous GS, Arulkumaran S, Symonds I, et al. The ‘tamponade test’ in the management of massive postpartum hemorrhage. Obstet Gynecol 2007;101:767–72.
Doumouchtsis SK, Papageorghiou AT, Arulkumaran S. Systematic review of conservative management of postpartum hemorrhage: what to do when medical treatment fails. Obstet Gynecol Surv 2007;62:540–7.
Doumouchtsis SK, Papageorghiou AT, Vernier C, Arulkumaran S. Management of postpartum hemorrhage by uterine balloon tamponade: prospective evaluation of effectiveness. Acta Obstet Gynecol Scand 2008;87:849–55.
Gulmezoglu A, Forna F, Villar J, Hofmeyr G. Prostaglandins for preventing postpartum haemorrhage. Cochrane Database Syst Rev (3) 2007; CD000494.
Lalonde A, Daviss BA, Acosta A, Herschderfer K. Postpartum hemorrhage today: ICM/FIGO initiative 2004–2006. Int J Gynaecol Obstet 2006;94:243–53.
Mousa HA, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev 2007; 1: CD003249.
Penney G, Kernaghan D, Adamson L. Scottish Confidential Audit of Severe Maternal Morbidity. 3rd Annual Report 2005, Scottish Programme for Clinical Effectiveness in Reproductive Health.
Prendiville WJ, Elbourne D, McDonald S. Active versus expectant management in the third stage of labour. Cochrane Database Syst Rev 2009; 3: CD000007.
Rabe H, Reynolds G, Diaz-Rossello J. Early versus delayed umbilical cord clamping in preterm infants. Cochrane Database Syst Rev 2004; 4: CD003248.
Ramanathan G, Arulkumaran S. Postpartum hemorrhage. J Obstet Gynaecol Can 2006;28:967–73.
Razvi K, Chua S, Arulkumaran S, Ratnam SS. A comparison between visual estimation and laboratory determination of blood loss during the third stage of labour. Aust NZ J Obstet Gynaecol 1996;36:152–4.
RCOG. The role of emergency and elective interventional radiology in postpartum haemorrhage. Good Practice Guidelines. London: RCOG 2007.
Royal College of Obstetricians and Gynaecologists (RCOG) Prevention and management of postpartum haemorrhage. Green Top Guideline No 52. London: RCO 2009.
Su L, Chong Y, Samuel M. Oxytocin agonists for preventing postpartum haemorrhage. Cochrane Database Syst Rev 2007; 3: CD005457.
WHO. Maternal mortality in 2000: Estimates developed by WHO, UNICEF, and UNFPA. Geneva: Department of Reproductive Health and Research 2004.
WHO. WHO Recommendations for the prevention of postpartum haemorrhage. Geneva: WHO 2007.
World Health Organization (WHO) The World Health Report 2005. Make every mother and child count. Geneva: WHO. Patient resources
www.patient.co.uk/showdoc/40000261/
Prelabour rupture of membranes at term Definition
Prelabour rupture of membranes (PROM) at term is defined as spontaneous rupture of fetal membranes for an hour or more before the onset of labour at or over 37 completed weeks of gestation. The time from rupture to the onset of labour has been variably defined in clinical studies. Epidemiology
The incidence of PROM ranges between 5% and 20% depending on the series and the method of dating of the pregnancies studied. The natural history of PROM is the spontaneous onset of contractions and labour within 24 hours in 60–80% of cases. After the first 24 hours, the rate of onset of spontaneous labour falls off to an additional 5% per day. Aetiology
Unlike preterm PROM, term PROM is a physiological event in the vast majority of cases. Indeed a proportion of PROM near term (≥34 weeks’ gestation) is believed to be of physiological origin. In a small but significant proportion of cases of term PROM, lower genital tract or intra-amniotic infection, abruption, or trauma may be the cause of the membrane rupture. Diagnosis and initial assessment
The diagnosis of PROM is frequently made on the basis of maternal history alone, sometimes with erroneous results, particularly in nulliparous women. A speculum examination and simple bedside tests may be required in equivocal cases. Although maternal history was found to have an accuracy of 90% for the diagnosis of PROM, it is good practice to confirm the diagnosis before instituting the management steps for PROM. The presence of a pool of amniotic fluid in the posterior fornix on speculum examination is confirmatory of PROM, provided that copious but clear and viscid cervical secretion has been excluded. There may be a role for nitrazine pH-based paper testing when there is a very small amount of fluid in the posterior fornix and the observer is uncertain. However, a positive nitrazine test is not specific for PROM and has a false-positive rate of 17%. The pH of the normally acidic vaginal fluid changes to alkaline if there is vaginitis, bacterial vaginosis, contamination with cervical secretion, blood, semen, or urine. In doubtful cases the patient may be asked to cough gently while visualizing the external cervical os for any trickle of amniotic fluid. An extended pad test is also useful. A panel of newer and more sensitive/specific tests based on insulin-like growth factor binding protein-1 (IGFBP-1) in cervicovaginal secretions have been evaluated.
A digital vaginal examination should be avoided after PROM unless there is a strong suspicion of labour or imminent delivery. In our institution we obtain a low vaginal and peri-anal swab for group B streptococcal colonization in all women that present with PROM. The colour of the amniotic fluid is documented and the presentation of the fetus confirmed. Clinical questions associated with term PROM
• Should PROM be managed expectantly in the first instance or by induction of labour on diagnosis?
• If induction of labour is indicated, what agents should be used, what route and for how long?
• If conservative management is selected, how long is it safe without increasing the risk of infection?
• Is monitoring or surveillance indicated during expectant management, and what tests are appropriate?
• How frequently should these tests be applied and what tests results should prompt an intervention?
• Who should be performing these tests? Management of term PROM
The most frequently discussed aspect of the management of term PROM is the risk of feto-maternal infectious morbidity. However, there are other risks such as acute cord prolapse and acute cord compression. Furthermore, there are resource implications associated with aggressive and immediate induction of labour for PROM and these should be appraised by the individual maternity unit, in the context of its activity level. Provided that vaginal delivery is appropriate, immediate induction of labour should be undertaken if there is evidence of chorioamnionitis, non-reassuring fetal status, meconium staining of the amniotic fluid, abruption, or evidence of other maternal compromise.
The risk of serious neonatal infection with term PROM is 1% compared with 0.5% for babies born to women with intact membranes. However, the evidence reviewed by the NICE Guideline Development Group (GDG) suggests that maternal and fetal outcomes were similar between those that were managed with planned induction of labour and those managed expectantly. The GDG recommended that induction of labour is appropriate 24 hours after term PROM as expectant management up to 24 hours is not associated with a significant increase in neonatal infection rates, and approximately 60% of women with term PROM will go into spontaneous labour within 24 hours. Women who elect to be managed expectantly should be advised to monitor their own temperature readings every 4 hours during waking hours and to report immediately any alteration in the colour or smell of their vaginal loss. They should be advised that sexual intercourse may increase the risk of infection. The fetal heart rate and movement should be reviewed every 24 hours after term PROM, and any reduction of fetal movements brought to the attention of the clinical team. Delivery should be conducted in the hospital with access to neonatal services if labour has not started after 24 hours of term PROM. The baby should be observed for at least 12 hours for any signs of infection.
The current NICE guidelines advise against intrapartum antibiotic prophylaxis even with PROM over 24 hours unless the woman displays evidence of infection, in which case a full course of intravenous broad-spectrum antibiotic should be administered. The baby should be referred for specialist neonatal care immediately after birth. Asymptomatic term babies born to women with term PROM >24 hours should be monitored closely for the first 24 hours. Elements of these recent guidelines are at odds with the risk-based approach for the prevention of early-onset GBS disease. With the exception of infection, there are no differences in other neonatal outcomes between immediate induction of labour and expectant management for up to 96 hours following term PROM.
There are no differences in instrumental vaginal delivery rates or Caesarean section rates between immediate induction and expectant management for up to 96 hours after term PROM. There is significant increase in the risk of maternal infectious morbidity including chorioamnionitis and endometritis with expectant management over 24 hours. There is no data on fetal or maternal outcomes with expectant management beyond 96 hours as the vast majority of women would have delivered by this stage. Further reading
Intrapartum care: care of healthy women and their babies during labour. NICE clinical guideline 55. www.nice.org.uk/CG55
Resuscitation of the newborn Introduction
Resuscitation of the newborn infant differs from that of any other age group. The newborn is small, wet, and therefore prone to getting cold and has lungs that contain lung liquid. Therefore the approach to resuscitation needs to be adapted to their needs.
Although the majority of infants will not require resuscitation at birth, approximately 3–5% of newborn infants may need some support. Most of the time, the potential need for resuscitation can be anticipated from the maternal and obstetric history such as the presence of a congenital anomaly on the antenatal scans, preterm gestation, fetal distress (for example as indicated by an abnormal cardiotocograph trace or abnormal fetal scalp blood sample), or by the presence of meconium. In these cases trained members of the midwifery and/or neonatal team should be present prior to delivery. Very occasionally a newborn infant may be unexpectedly delivered in poor condition and while the neonatal team are being alerted, resuscitation must be commenced. Physiology
The primary reason for need for resuscitation in the newborn infant differs from that in adults. Whereas adults requiring resuscitation will normally have had a cardiac event, the newborn infant’s heart is healthy and it will usually be a hypoxic or ischaemic event initially that will have compromised the newborn. Therefore, particular attention to management of the airway and breathing is imperative.
In normal circumstances, the process of labour and delivery will aid most resorption of lung liquid, but the first breaths a newborn takes are vital in making that transition from in utero to ex utero life. If the newborn does not breath at birth, or has an inadequate respiratory effort such as gasping or apnoea, then unless additional help is given, there will be a fall in PaO2, a rise in PaCO2, and a rise in lactic acid; this will result in a fall in heart rate and also antagonize the ability to respond to resuscitation when it is initiated.
The process of compromise will initially start with a transition from regular breathing to ‘primary apnoea’. At this stage the infant may then go into a phase of gasping. The effect of gasping may be enough for the infant to ‘resuscitate itself’ or if given resuscitation in the form of airway management should respond quickly. After the gasping phase ‘terminal apnoea’ follows. At this stage there will normally already have been a significant compromise to the infant with a low PaO2, high PaCO2, high levels of lactic acid, and a slow heart rate. This infant will need more resuscitative measures if airway management is not sufficient. Equipment needed
The items mentioned are not an exhaustive list and when faced with the delivery of the newborn infant out of the hospital setting making a note of the time, drying the infant, and considering providing warmth with skin to skin contact between the infant and mother may be all that is needed. Using a piece of string to tie the umbilical cord should also be undertaken while awaiting help to arrive.
In a planned delivery at home, midwives will take with them a bag–valve–mask device with facemasks, oral airways, a laryngoscope, a small oxygen cylinder and suction with catheters at least size 12Fr. They should also have cord clamps, scissors, and disposable gloves.
In the hospital setting, all of this equipment should be more easily available including a resuscitaire to provide a flat surface, which is also able to provide warmth, radiant heat, a clock, pressure limited delivery of air/oxygen, and suction. In addition, face masks, oral airways, laryngoscopes, and endotracheal tubes should be present. Equipment for placement of an umbilical venous catheter should also be made available if required and also drugs. Priorities
Warmth
Maintaining temperature is imperative and indeed hypothermia is associated with worsening morbidity and mortality. Therefore, when present at the delivery of any newborn, irrespective of it’s need or not for resuscitation, drying the infant, disposing of the wet towels, and wrapping the infant with a dry warm towel is necessary before further steps are taken. After drying and wrapping, the infant should be immediately assessed. The assessment comprises respiratory effort, heart rate, tone, and colour. Based on this assessment, the need for resuscitation will be determined. Should resuscitation be required, call for help early. Starting the clock on the resuscitaire when the baby is born should also be undertaken in order to guide resuscitation and also for documentation.
Airway
Newborn infants have a large occiput and when placed on the resuscitaire or a hard surface the tendency is for the head to flex forward thereby obstructing the airway. To overcome this, place the head in the neutral position by extending the neck very slightly (Fig. 10.17.1). This will result in the plane between the nose and mouth being parallel to the plane of the ceiling. This is different from adults in whom you tilt the head and apply a chin lift. Sometimes this simple manoeuvre is all that is needed in order to assist the newborn’s respiratory effort, although there are further airway manoeuvres one can apply (see below).
If, having placed the head in the neutral position, the baby’s respiratory effort remains poor or absent, with a heart rate that is slow (receives the inflation breaths.

Fig. 10.17.1 Newborn infants have a large occiput and when placed on the resuscitaire or a hard surface have a tendency for the head to flex forward thereby obstructing the airway (a). Placing the infant’s head in the ‘neutral position’ opens the airway (b). Care must be taken not to overextend the head.
Other airway manoeuvres include a single-handed jaw thrust, whereby the third or fourth finger of the hand used to keep the facemask on the infant is placed behind the angle of jaw and pushed up. This will aid opening the airway by bringing the lower jaw in line with the upper jaw and helping to bring the tongue, which may have propped backwards into the airway, out of the way. Having carried out this manoeuvre, five inflation breaths should again be given. If this does not result in a rise in heart rate or chest wall movement, and if help is available, the two-person jaw thrust can be attempted, where by one person applies the jaw thrust behind both jaw angles and holds the facemask in place while the other gives the inflation breaths.
If this does not work or there is no help available, if competent, the larynx and vocal cords should be directly visualized using a laryngoscope placed in the left hand and suction should be performed if a blood clot, vernix, or meconium is seen. Alternatively, if there is no obstruction, an appropriately sized oral airway should be placed using the laryngoscope or a tongue depressor should be performed.
To size an oral airway the length should be equal to the distance from the midline of the lips to the angle of the jaw. The airway is inserted in the anatomical position that is desired, i.e. it is not rotated in the mouth because of the fragile palate.
Following these manoeuvres, five inflation breaths should be given. One can only feel reassured if there is a rise in heart rate or you visualize chest movement. If, using these manoeuvres, the chest wall moves with the inflation breaths but there is no rise in heart rate you then need to undertake chest compressions. You may at any of these points intubate if trained and skilled to do so.
Breathing
Having made sure that the chest wall has moved with the inflation breaths, if there is a rise in heart rate but the newborn continues not to breath or has poor respiratory effort, ventilation breaths should be given. These breaths are to ‘breath for the baby’ and are therefore given with shorter inspiratory times and a quicker rate of 30 breaths per minute. Having overcome the initial stiffness of the lungs, pressure given should also be reduced to a pressure sufficient to get chest wall movement (normally around 20–25 cmH2O).
If after 30 seconds the infant is still not breathing effectively, you may need to consider admission of the infant to the neonatal unit for ventilation and further management.
There is growing evidence from both animal and human studies that resuscitation of infants with room air is as effective as 100% oxygen. There is a theoretical risk that 100% oxygen can cause tissue damage via free radicals. Tan et al. (2008) undertook a Cochrane review looking at air versus oxygen for resuscitation of infants at birth. They concluded that if you choose to resuscitate using air, supplementary oxygen should be available as a back-up.
Some devices are now available which allow you give a set positive end expiratory pressure (PEEP) as well as a peak inspiratory pressure, such as the Neopuff. There is a theoretical benefit to the infant for using PEEP, as this establishes and maintains functional residual capacity. Although there have been several papers showing the benefit particularly in preterm infants where there is an association between absence of functional residual capacity and subsequent respiratory distress syndrome in those requiring ventilation, a Cochrane review undertaken in 2003 and recently updated in 2008 concluded that there was insufficient evidence to determine the efficacy and safety of PEEP in ventilation breaths given during resuscitation of the newborn infant and that further randomised clinical trials were needed.
Circulation
If despite good chest movement with inflation breaths, there is no rise in heart rate, chest compressions must be given. The aim of these chest compressions is to move oxygenated blood from the lungs to the coronary arteries. The best method for administering chest compressions is to encircle the whole of the infant’s chest with both hands and place the tips of your thumbs just below and imaginary inter nipple line (Fig. 10.17.2).
The compressions need to compress the chest by one-third and are given at a ratio of one ventilation breath to three chest compressions. After approximately 15 cycles or 30 seconds, the infant must be assessed with regards to colour, tone, respiration, and heart rate. If the heart rate has improved (>60/minute) then chest compressions can stop and depending on the respiratory effort ventilation breaths may or may not need to be continued.
If however despite good airway management with chest movement and chest compressions the heart rate does not increase, drugs should be considered.
Drugs
If you need to obtain vascular access and give drugs, the outcome for this newborn infant is likely to be poor. The drugs used in resuscitation are sodium bicarbonate, adrenaline, and dextrose. Occasionally volume (0.9% sodium chloride or O Rhesus-negative blood) can be given particularly if there is an obvious history of blood loss. Refer to the BNF for children for appropriated drug doses. The best method of administering drugs is via central access. In the newborn infant, this will be by way of a catheter that has been inserted into the umbilical vein of the cord. Alternatively an intra-osseous needle may be used.
If access is difficult the only drug that can be given via an endotracheal tube is adrenaline but due to variable absorption the efficacy of this route is questionable and therefore it is not recommended if alternative access is available. Preterm infants
Infants born prematurely will have less reserve, and therefore attention to temperature control is important. For those born at 30 weeks’ gestation or less, immediately placing the body of the infant (without prior drying) into a plastic bag/wrap under a radiant heater has been shown to improve maintenance of normothermia. Preterm infants are more likely to require stabilization rather than resuscitation. The approach to resuscitation is exactly the same as the approach to that of a term newborn.

Fig. 10.17.2 Position of hands for cardiac compression in a newborn infant.
Owing to the fragility of their lungs, pressures required to inflate their lungs and move the chest wall will be less and if inflation breaths are required, starting with pressures of 20–25 cmH2O should be adequate. Having given inflation breaths due to prematurity, their respiratory effort may not be sufficient and hence intubation by a trained and skilled member of the team may need to be undertaken. One may consider using a device that is able to provide PEEP when delivering ventilation breaths. If intubation is required, administration of surfactant at this time via the endotracheal tube should be considered. Having stabilized the infant, they should be transferred to the neonatal unit for ongoing assessment and management. Meconium aspiration
Most babies that pass meconium in utero are either term or post-term. The presence of meconium is normally an indicator of fetal stress. The fetus must be gasping in order to aspirate meconium.
If a newborn cries at delivery, despite the presence of meconium, it will imply that the infant has an open airway and therefore no action is required. If however the infant is born with no respiratory effort (i.e. apnoeic), there may have been a period of gasping in utero and this infant is at risk of meconium aspiration. Therefore, it is important, having firstly paid attention to keeping the infant warm, to directly visualize the larynx and vocal cords in order to suction any large plugs of meconium that may be present. Having directly visualized the cords and either assessed that there is no obstruction or removed the obstruction to the normal approach to newborn resuscitation can proceed. Known congenital problems
The majority of antenatal problems, such as oesophageal atresia with a tracheo-oesophageal fistula or a congenital diaphragmatic hernia, that could alter the approach to resuscitation will be picked up antenatally and these should be delivered at an appropriate tertiary centre if indicated.
However, potential congenital problems with the airway, such as Pierre-Robin sequence, can be difficult to pick up on an antenatal scan and therefore the use of adjunct airways may be required if an infant needing resuscitation fails to inflate their chest with airway positioning and jaw thrust. Insertion of an appropriately sized oral airway or a nasopharyngeal airway can aid the maintenance of a patent airway by preventing the tongue, which is large in relation to the size of the oral cavity, flopping backwards, and occluding the larynx. Stopping resuscitation
The Resuscitation Council (UK) has suggested that if there are no is signs of life after 10 minutes of continuous and adequate resuscitation then discontinuation of resuscitation may be justified. This is supported with data published by Patel and Beeby (2004), which looked at outcome of term newborn infants who had resuscitation beyond 10 minutes. Twenty-nine babies were included in their observation study. 20/29 babies died before leaving hospital. Of the nine who were discharged alive, eight had severe disability and one had moderate disability. Summary
Newborn resuscitation follows a systematic stepwise approach with emphasis placed on temperature control and airway. The majority of newborn infants will not need resuscitation but should they do so, the vast majority will respond when airway and breathing are managed. It is estimated that more aggressive resuscitation will be required in 1 in 2000 deliveries. In the small minority who need further resuscitative measures the outcome of resuscitation is likely to be poor, and good documentation of time of birth and intubation, cardiac compressions, and administration of drugs will help with further management and the counselling of parents. An approach to newborn resuscitation may be summarized in Fig. 10.17.3 by the algorithm provided by the Resuscitation Council.

Fig. 10.17.3 Newborn life support. With permission from the Resuscitation Council UK. Further reading
Barber CA, Wyckoff MH. Use and efficacy of endotracheal versus intravenous epinephrine during neonatal cardiopulmonary resuscitation in the delivery room. Paediatrics 2006;118:1028–34.
Bhatt DR, White R, Martin G, et al. Transitional hypothermia in preterm newborns. J Perinatol 2007; 27: S45–S47.
Morley CJ, Davis PG. Advances in neonatal resuscitation: supporting transition. Arch Dis Child Fetal Neonat Edn 2008; 93: F334–F336.
National Institute for Health and Clinical Excellence (NICE). Intrapartum care: management and delivery of care to women in labour. Clinical Guidelines (UK) 2007: 42.
O’Donnell C, Davis P, Morley C. Positive end-expiratory pressure for resuscitation of newborn infants at birth. The Cochrane Database Syst Rev 2008; 2: CD004341.
Patel H, Beeby PJ. Resuscitation beyond 10 minutes of term babies born without signs of life. J Paediatr Child Health 2004;40:136–8.
Saugstad OD. Practical aspects of resuscitating newborn infants. Eur J Pediatr 1998; 157: S11–S15.
Soll RF. Heat loss prevention in neonates. J Perinatol 2008; 28: S57–S59.
Tan A, Schulze A, O’Donnell CPF, Davis PG. Air versus oxygen for resuscitation of infants at birth. Cochrane Database Syst Rev 2008; 2: CD002273.
Upton CJ, Milner AD. Endotracheal resuscitation of neonates using rebreathing bag. Arch Dis Child 1991;66:39–42. Internet resources
Resuscitation Council (UK) 2008 www.resus.org.uk.
BNF for children. www.bnfc.org
Retained placenta Definition
A retained placenta occurs when the placenta fails to deliver 30 minutes following delivery of the fetus with active management of the third stage or 60 minutes with a physiological third stage (NCCWCH 2007). Epidemiology
The retained placenta (RP) rate is dependent on both definition and third–stage management. It also varies historically and geographically, with rates increasing with time and degree of industrialization (Weeks in press). In actively managed third stages, rates of around 1 in 200 are typical for the developing world (or the UK in the 1950s) while current rates in the USA and UK are around 1 in 50. The reason for this is unclear, but may relate to the association between retained placenta and induction, previous uterine surgery, and birth position (see Aetiology below). Pathology
Three types of retained placenta are recognized, with the first two being readily distinguished on ultrasound. The quoted frequencies are taken from retained placentas at a mean of 3 hours postpartum in the Release Study (Weeks et al. 2008).
Placenta adherens (60%)
Caused by a failure of contraction of the retroplacental myometrium. On ultrasound, a thin layer of myometrium can be seen behind the retained placenta (the remainder of the myometrium is thickened and contracted). At manual removal of placenta (MRP), the placenta is easily separated from the myometrium.
Trapped placenta (15%)
Where the placenta is already expelled from the uterus, but trapped behind the cervix. On ultrasound, the uterus is seen to be empty with a thick, contracted myometrium throughout. The placenta is seen external to the uterine body, held in the lower segment by a closed cervix.
Placenta accreta (25%)
Caused by invasion of the placenta into (or through) the underlying myometrium. The invasion can be localized or widespread. Most commonly the placenta can still be manually removed, but there is a small area that is ‘torn away’ rather than separated, or it needs to be removed ‘piecemeal’. Aetiology
The strongest association of RP is with gestational age but increased rates of RP are also found with delivery in a labour bed (rather than standing or squatting), pre–eclampsia, previous termination of pregnancy, extremes of parity or age, use of oxytocin, non–Asian race, and midwifery deliveries (Coombs and Laros 1991). In addition to these, RP has also been found to be associated with induced labour, previous uterine injury, and uterine abnormalities. These studies suggest that interventions common in the most developed countries (labour induction, use of oxytocin, termination of pregnancy) may be contributing to their high RP rates.
Delivery of the placenta is much faster with active management of the third stage. However, by 60 minutes most placentas have been expelled in both groups, and there is no difference in the need for manual removal. The one exception is when intravenous ergometrine is used as prophylactic when the MRP rate is greatly increased (relative risk 19.5, 95% CI 2.6–145.4) (Hammar et al. 1990; Prendiville et al. 2000).
Lack of patience in the third stage of labour can lead to iatrogenic RP due to a snapped cord, or haemorrhage due to partial removal of an undetached placenta. It is therefore crucial that the signs of separation are awaited and undue cord traction avoided. In an audit of RPs in Liverpool, UK, 20% of all RPs had snapped cords. Once this is done it becomes very difficult to extract the placenta, even if it detaches from the uterus, and a MRP is needed. Prognosis
The prognosis for RP is dependent on the facilities available for treatment. Although in the UK there has only been one death since 1967 from a RP following vaginal delivery, studies from the developing world have found much higher mortality rates. In the South African confidential enquiry into maternal deaths, there were 13 RP deaths in 1999, the single biggest contributor to death from PPH (NCCEMD 1999). Clinical approach
Diagnosis
Authorities disagree about the time limit for a normal third stage. In developed countries the time taken for 95% of placentas to expel is around 15 and 50 minutes for actively managed and physiological third stages respectively (Prendiville et al. 2000). Blood loss increases after an actively managed third stage of 18 minutes, but waiting for a further 30 minutes leads to the delivery of a further 40% of placentas (Carroli and Bergel 2007). Most authorities suggest that a diagnosis of RP be made at 30 minutes, but that a vaginal examination is performed prior to transfer to theatre for MRP in case of spontaneous delivery in the meantime.
The differentiation between a placenta that is ‘trapped’ or adherent (placenta adherens) is not easy unless ultrasound is used. Clues to a trapped placenta will be if the fundus feels small and contracted, or if the edge of the placenta is palpable through a tight cervical os. In contrast, with placenta adherens the fundus is usually soft and wide. Placenta accreta is rare in women having a vaginal delivery, and will usually be discovered only at the time of attempted MRP.
Ultrasound can be used to differentiate between a trapped and adherent placenta. With a trapped placenta the uterus is empty with a clear endometrial echo. The placenta can be seen lying outside the uterine body within a distended lower segment. In contrast, with an adherent placenta the myometrium will be thickened in all areas, except where the placenta is attached, where it will be very thin or even invisible.
General management
• Women with RPs are at high risk of postpartum haemorrhage and so should be transferred to a high-risk area with an intravenous line in situ.
• Care should be taken in making further attempts at cord traction to remove the placenta as it can lead to a snapped cord or further haemorrhage.
Medical management
• Infusions of oxytocin have been widely used for the treatment of RP, even though they make a MRP more difficult by contacting the cervix. This treatment has never been subjected to a randomized trial, although there is some evidence that intravenous prostaglandins may be beneficial (van Beekhuizen et al. 2006). Given the lack of convincing evidence and the potential difficulties that they cause, it would seem sense to reserve their use for those women who bleed while awaiting MRP.
• The use of umbilical vein injections have been recommended widely (NCCWCH 2007, Carroli and Bergel 2001). This technique allows the oxytocic to be directed specifically at the area with the contractile failure, while sparing the remainder. However, emerging data from the Release Study (RCT of 577 women having intraumbilical injections of either oxytocin 50 IU or water) show no benefit of oxytocin. There appears therefore to be no benefit of intraumbilical oxytocin injection.
• Intraumbilical prostaglandins may cross the placenta more efficiently and there is some evidence that they may be an affective alternative. However, more research is needed before they can be recommended.
• Glyceryl trinitrate (GTN) may be effective for the management of RP. This was based on numerous observational studies, most of which used intravenous boluses of 50–200 µg. Sublingual GTN tablets (1 mg, as used for angina) have also been shown to be effective in a small randomized trial (Bullarbo et al. 2005). A large trial is needed to confirm these findings.
Surgical management
• MRP is the standard management for RP and it is recommended that this is carried out at around 30 minutes postpartum to keep blood loss to a minimum. A wait of 90 minutes will however lead to the delivery of 55% of placentas without the need for MRP and with a median extra blood loss of only 400 mL (Release Study data). There is therefore a balance to be achieved for each woman to keep intervention and blood loss to a minimum.
• If the cervix is tightly closed when it comes to the manual removal, uterine relaxation may be achieved with the aid of GTN in an intravenous bolus of 50–500 µg or 1 mg sublingually. Marked uterine relaxation occurs after 30–40 seconds and the uterus recovers its tone after 1–2 minutes.
• MRP following either vaginal delivery or CS carries with it an increased risk of endometritis and bleeding. Full aseptic procedures should therefore be followed and a prophylactic broad-spectrum antibiotic used. MRP should also be followed by the use of a long-acting oxytocic (ergometrine or oxytocin infusion). Recurrence
Following a RP in any previous pregnancy there is an overall recurrence rate of 6.25% (Hall et al. 1985). The risk of RP in the second pregnancy rises from 2% to 4.8% if there was a RP in the first. Further reading
Bullarbo M, Tjugum J, Ekerhovd E. Sublingual nitroglycerin for management of retained placenta. Int J Gynaecol Obstet 2005;91:228–32. Erratum in Int J Gynaecol Obstet 2006; 92: 337.
Carroli G, Bergel E. Umbilical vein injection for management of retained placenta. Cochrane Database Syst Rev 2001; 4: CD001337.
Combs CA and Laros RK. Prolonged third stage of labour: morbidity and risk factors. Obstet Gynecol 1991;77:863–7.
Hall MH, Halliwell R, Carr-Hill R. Concomitant and repeated happenings of complications of the third stage of labour. Br J Obstet Gynaecol 1985;92:732–8.
Hammar M, Bostrom K, Borgvall B. Comparison between the influence of methylergometrine and oxytocin on the incidence of retained placenta in the third stage of labour. Gynecol Obstet Invest 1990;30:91–3.
National Collaborating Centre for Women’s and Children’s Health (NCCWCH). Intrapartum Care. Care of healthy women and their babies during childbirth. London: RCOG Press 2007.
National Committee for Confidential Enquiries into Maternal Deaths (NCCEMD). Second Interim Report on Confidential Enquiries into Maternal Deaths in South Africa. www.doh.gov.za/docs/reports/1999/interim-rep.pdf
Prendiville WJ, Elbourne D, McDonald S. Active versus expectant management in the third stage of labour. Cochrane Database Syst Rev 2000; 3: CD000007.
van Beekhuizen HJ, de Groot AN, De Boo T, Burger D, et al. Sulprostone reduces the need for the manual removal of the placenta in patients with retained placenta: a randomized controlled trial. Am J Obstet Gynecol 2006;194:446–50.
Weeks AD. Alia G, Vernon G et al. Umbilical vein oxytocin for the treatment of retained placenta (RELEASE study); a double blind randomised controlled study. Lancet 2010;375:141–7.
Shoulder dystocia Definition
Shoulder dystocia is defined as ‘a delivery that requires additional obstetric manoeuvres to release the shoulders after gentle downward traction has failed. It occurs when either the anterior or, less commonly, the posterior fetal shoulder impacts on the maternal symphysis or sacral promontory’. Shoulder dystocia has also been defined as a prolonged head–to–body delivery time (e.g. more than 60 seconds), although many birth attendants usually await the next contraction after the delivery of the head to deliver the shoulders. Epidemiology
The incidence of shoulder dystocia ranges between 0.2% and 3% of births. Significant variations have been observed in different populations. In North America and the UK the incidence is 0.6% and in African American women it is 2.6%. Pathophysiology
Shoulder dystocia occurs due to a ‘mismatch’ between the fetal shoulder dimensions and the maternal bony pelvis. During vaginal delivery the fetal head descends through the pelvic brim in an occipito-transverse position. The shoulders rotate and are accommodated in the pelvic inlet at an oblique position as this has a larger diameter than the anteroposterior. The posterior shoulder descends first followed by the anterior one. If the fetal shoulders remain in an anteroposterior position or descend simultaneously, then the anterior shoulder becomes impacted behind the symphysis pubis and rarely the posterior shoulder behind the sacral promontory. Although at this stage the fetal head is delivered, the fetal chest remains compressed and respiratory efforts cannot be initiated. As the uterus is contracted, blood flow to the fetus is impeded. Delay in completing the delivery may result in fetal asphyxia, as the umbilical cord pH falls by 0.04 units per minute. Complications
Fetal
Severe cases of hypoxia can result in permanent brain injury and death. The rates of perinatal mortality secondary to shoulder dystocia are 0–2.5%. The risk of fetal hypoxic injury depends on the fetal condition prior to the occurrence of shoulder dystocia and on the time required for the completion of delivery.
Brachial plexus injury is a common fetal complication with wide variations in the reported incidence from 4% to 40%. In the majority of cases the injury is transient and will resolve within a year, with less than a 10% rate of persistent injury.
Fractures are also common and are usually clavicular or humeral. Clavicular fractures complicate 3–9.5% of shoulder dystocia cases. Most of these fractures heal well without sequelae.
Maternal
Postpartum haemorrhage and vaginal and perineal injuries are common maternal complications. Shoulder dystocia is one of the most significant risk factors for anal sphincter injuries. Uterine rupture is a rare complication, which may occur following fundal pressure.
Risk factors
The large majority of cases occur in the absence of risk factors. Antenatal risk factors include a previous pregnancy complicated by fetal macrosomia, gestational diabetes or shoulder dystocia, pre-existing or gestational diabetes mellitus, maternal obesity or excessive weight gain, multiparity, and prolonged gestation. Induction of labour is also a risk factor for shoulder dystocia.
Intrapartum risk factors include a prolonged first stage of labour, secondary arrest, a prolonged second stage of labour, oxytocin augmentation, and assisted vaginal delivery. The incidence of shoulder dystocia is increased by approximately 35–45% in assisted deliveries of non-diabetic and diabetic mothers. Sequential use of instruments is associated with even higher rates.
Fetal macrosomia
The risk of shoulder dystocia increases significantly with increased birthweight. Nesbitt et al. (1998) conducted a large population-based study and reported the following rates of shoulder dystocia for unassisted births of non-diabetic mothers: 5.2% for birthweight 4000–4250 g, 9.1% for 4250–4500 g, 14.3% for 4500–4750 g, and 21.1% for 4750–5000 g.
Although fetal macrosomia is the most significant risk factor and associated with most of the other risk factors (maternal diabetes, multiparity, previous macrosomic infant, prolonged gestation, maternal obesity, or excessive weight gain), almost half of the cases of shoulder dystocia occur in infants 4750 g, respectively. The risk of shoulder dystocia for assisted births to diabetic mothers was even higher: 12.2% for infants 4000–4250g, 16.7% for those 4250–4500g, 27.3% for those 4500–4750g, and 34.8% for those 4750–5000g. Prediction and prevention
Although shoulder dystocia is largely unpredictable, statistical models have been developed to predict the risk. Parameters used in these models are birthweight, maternal height and weight, gestational age, and parity. Some studies suggest that it is possible to identify combinations of factors that are associated with shoulder dystocia and neonatal injury. In general, the presence of multiple risk factors appears to be a predictor for shoulder dystocia.
Identification of risk factors and an antenatal care plan that aims to modify them may reduce the incidence of shoulder dystocia. For example, tight control of glucose levels in diabetic pregnant women may reduce the risks of fetal macrosomia and shoulder dystocia. When risk factors are present, a plan for delivery should include a senior midwife and an experienced obstetrician available at the second stage, which may facilitate a successful management.
Mode of delivery
Induction of labour has been considered as an option for managing suspected macrosomia, thus reducing the risk of shoulder dystocia and subsequent birth trauma. However, early induction of labour for non-diabetic women with suspected fetal macrosomia does not appear to improve either maternal or fetal outcome.
The RCOG guidelines do not recommend elective Caesarean section for suspected fetal macrosomia (estimated fetal weight >4500 g) in non-diabetic women. Elective Caesarean section can be considered in diabetic women when the estimated fetal weight is >4500g and in non-diabetic women when the estimated fetal weight is >5000 g. Elective Caesarean section can be discussed with the parents in cases of a previous birth affected by shoulder dystocia, brachial plexus injury, or associated asphyxial injury.
Prophylactic manoeuvres at delivery (McRoberts manoeuvre and direct suprapubic pressure) have been considered for the prevention of shoulder dystocia, but there are no clear findings to support or refute their use.
Recurrence of shoulder dystocia
The recurrence risks vary between 11.9% and 16.7%. In a large population study by Moore et al. (2008), the annual incidence of primary and recurrent shoulder dystocia was 2.3% and 13.5% respectively. This study highlighted birth-weight ˇ3500 g, assisted vaginal delivery and severe shoulder dystocia in the previous delivery as the most significant independent risk factors for recurrence. The only identifiable risk factor may often be the prior history itself. Management of shoulder dystocia
The aim of management should be prevention of fetal asphyxia, while avoiding fetal and maternal injury (Fig. 10.19.1). The attending midwife or obstetrician should be able to recognize a shoulder dystocia immediately and proceed through a stepwise sequence of manoeuvres to expedite delivery.
First-line manoeuvres
McRoberts manoeuvre
The woman is on supine position with the hips acutely flexed and the knees close to the chest. This position straightens the lumbosacral angle, allowing descent of the posterior shoulder. The maternal pelvis is rotated cephalad and the pelvic inlet is now perpendicular to the direction of the maternal expulsive forces. This manoeuvre has success rates as high as 90%.
Directed suprapubic pressure
Continuous or ‘rocking’ (cyclical compression/relaxation) pressure on the posterior aspect of the anterior shoulder may facilitate its rotation to an oblique position, adduction of the shoulders and a reduction of the bisacromial diameter (Fig. 10.19.2).
Second-line manoeuvres
Delivery of the posterior arm
The hand enters the vagina posteriorly and gentle pressure is applied at the antecubital fossa to flex the fetal forearm, which is then grasped and swept across the fetal chest. With this manoeuvre, delivery of the posterior arm may be achieved, allowing the anterior arm to rotate posteriorly or descend behind the symphysis pubis as Kung et al. (2006) showed that the shoulder dimensions are reduced by 2.5 cm with this manoeuvre, especially in larger fetuses.
Rubin’s manoeuvre
If the posterior arm is not deliverable, rotation can be attempted by placing two fingers in the vagina behind the anterior shoulder. The shoulder is pushed forward and the bisacromial diameter rotates into an oblique position. If unsuccessful, this can then be combined with the Woods’ screw manoeuvre.
Woods’ screw
Two fingers are inserted vaginally, on the anterior aspect of the posterior shoulder and apply pressure aiming to rotate the fetus towards the same direction as the Rubin’s manoeuvre.
Reverse Woods’ screw
Two fingers are placed behind the posterior shoulder and an attempt is made to rotate in the opposite direction to the original Woods’ screw.
All these manoeuvres aim to rotate the shoulders 180 degrees and enable delivery by bringing the anterior shoulder posteriorly. Recent studies have indicated that insertion of the whole hand in the vagina may enable better thrust on the shoulder and facilitate rotation (Crofts et al. 2008) (Fig. 10.19.3). It has also been suggested that knowledge of the concepts that underlie manoeuvres and the practical details of their execution is much more effective than knowledge of the precise definitions or eponyms of each manoeuvre.

Fig. 10.19.1 Downward traction should be avoided.

Figure 10.19.2 Directed suprapubic pressure.

Fig. 10.19.3 Insertion of the whole hand posteriorly in the vagina.
All-fours
With the woman on her hands and knees, gentle traction is applied aiming to deliver the posterior shoulder first, which may descend downwards due to gravity and to a possible increase of the anteroposterior diameter of the maternal pelvis.
Clavicular fracture
This manoeuvre will reduce the bisacromial diameter, but may be associated with brachial plexus injury or vascular and soft tissue fetal trauma.
Third-line manoeuvres
Zavanelli manoeuvre
The fetal head is flexed, restitution is reversed, the head is rotated back to the occipitoanterior position, and replaced into the uterine cavity. Tocolytics can be used along with general anaesthetic agents for uterine relaxation. The fetus is then delivered by Caesarean section. High success rates up to 92% have been reported, but this manoeuvre is associated with significant fetal and maternal morbidity, including fetal injuries and deaths, uterine and vaginal rupture. It is likely that most injuries are not necessarily due to the procedure itself but may occur following other unsuccessful manoeuvres and prolonged fetal hypoxia. Nevertheless, this manoeuvre should only be performed in cases of severe shoulder dystocia unresponsive to first- and second-line manoeuvres and the fetal condition should be evaluated first, taking into account the potential irreversibility of fetal asphyxia.
Table 10.19.1 Modified ‘HELPERR’ algorithm (obtained from ALSO programme manual)

Symphysiotomy
This procedure requires a degree of surgical expertise and is associated with significant risks of lower urinary tract injury. It should only be used as a last resort manoeuvre. The patient is in a supine position and the thighs are abducted no more than 45° from the midline. A urethral catheter is inserted and the urethra is displaced laterally. Following local infiltration with lignocaine, a vertical stab incision is made on the symphysis with a scalpel. Cutting through the fibres by rotational movement of the blade usually allows partial separation of the symphysis and the anterior fetal shoulder to be disimpacted. Training
As for all the obstetric emergencies and especially the rare ones with high morbidity and mortality rates, regular training sessions for the management of shoulder dystocia with fire drills and the use of mannequins should be organized by all obstetric units. Unit protocols should advise a multi-disciplinary and systematic approach. Algorithms and mnemonics such as the HELPERR algorithm (Table 10.19.1) are commonly used and may facilitate a prompt and sequential use of the manoeuvres. Further reading
American College of Obstetricians and Gynecologists. Shoulder dystocia. ACOG practice bulletin clinical management guidelines for obstetricians–gynecologists. Number 40. Obstet Gynecol 2002;100:1045–50.
Athukorala C, Middleton P, Crowther CA. Intrapartum interventions for preventing shoulder dystocia. Cochrane Database Syst Rev 2006; 4: CD005543.
Belfort MA, Dildy GA, Saade GR, et al. Prediction of shoulder dystocia using multivariate analysis. Am J Perinatol 2007;24:5–10.
Cheng YW, Norwitz ER, Caughey AB. The relationship of fetal position and ethnicity with shoulder dystocia and birth injury. Am J Obstet Gynecol 2006;195:856–62.
Crofts JF, Fox R, Ellis D, et al. Observations from 450 shoulder dystocia simulations: lessons for skills training. Obstet Gynecol 2008;112:906–12.
Dyachenko A, Ciampi A, Fahey J, et al. Prediction of risk for shoulder dystocia with neonatal injury. Am J Obstet Gynecol 2006;195:1544–9.
Kung J, Swan AV, Arulkumaran S. Delivery of the posterior arm reduces shoulder dimensions in shoulder dystocia. Int J Gynaecol Obstet 2006;93:233–7.
Mehta SH, Blackwell SC, Chadha R, Sokol RJ. Shoulder dystocia and the next delivery: outcomes and management. J Matern Fetal Neonatal Med 2007;20:729–33.
Moore HM, Reed SD, Batra M, Schiff MA. Risk factors for recurrent shoulder dystocia, Washington state, 1987–2004. Am J Obstet Gynecol 2008; 198: e16–24.
Nesbitt TS, Gilbert WM, Herrchen B. Shoulder dystocia and associated risk factors with macrosomic infants born in California. Am J Obstet Gynecol 1998;179:476–80.
Royal College of Obstetricians and Gynaecologists (RCOG) Shoulder dystocia. Guideline No 42. Green Top Guidelines. London: RCOG 2005
Spong CY, Beall M, Rodrigues D, Ross MG. An objective definition of shoulder dystocia: prolonged head-to-body delivery intervals and/or the use of ancillary obstetric maneuvers. Obstet Gynecol 1995;86:433–6. Internet resources
www.erbspalsygroup.co.uk
Shoulder presentation Definition
It is a malpresentation in which one of the fetal shoulders occupies the lower pole of the uterus and is the first to engage when labour commences. It is associated with an abnormal lie (i.e. transverse lie), in which the fetal spine is at right angles to the long axis of the uterus) with the head in one iliac fossa and the breech occupying the other iliac fossa. In this situation, one of the shoulders comes to occupy the lower pole of the uterus. Acromion process of the scapula is the denominator and depending on its relationship to the ilio-pectineal eminence (right and left) and sacro-iliac joints (right and left), the following positions are described:
• left scapulo (or dorso): anterior
• right scapulo (or dorso): anterior
• left scapulo (or dorso): posterior
• right scapulo(or dorso): posterior
However, there is no mechanism of labour in transverse lie as the engaging diameter (fetal back) cannot enter the pelvic brim, except in rare cases of extreme prematurity or in a macerated fetus, in which an acute angulation of the fetal spine is possible (i.e. folding of the fetal trunk). Epidemiology
Transverse lie with shoulder presentation occurs in about 2–3% of pregnancies in early gestations. However, at term, only about 0.3% of fetuses have shoulder presentation (1 in 300 deliveries). Predisposing factors
Any factor that hinders a longitudinal lie may predispose to transverse lie and shoulder presentation. The majority of transverse lie (over 90%) occur in multipara due to laxity of the abdominal wall muscles as well as the uterine myometrium that enables the uterus to lose its piriform shape. Similarly, alterations in amniotic fluid volume (polyhydramnios) as well as other factors that obliterate the piriform shape of the uterus (congenital malformations such as arcuate or subseptate uterus, fibroids in the lower segment, major degree placenta praevia) would prevent the fetus from assuming a longitudinal lie. True or relative cephalopelvic disproportion will also reduce the space available in the longitudinal axis of the uterus, thereby forcing the fetus to assume a transverse lie.
Fetal factors are congenital malformations, prematurity, intrauterine growth restriction (smaller baby has more ‘space’ to occupy, nullifying the restrictive effects of piriform uterus) and multiple pregnancy. Approximately 40% of transverse lie (i.e. shoulder presentation) is associated with multiple pregnancy and a majority of these involve the second twin. In about a third of cases, no specific cause for transverse lie could be identified. Natural history of shoulder presentation
• Spontaneous rectification—it is estimated that approximately 80% of transverse lie diagnosed antenatally may correct itself to a longitudinal lie, by the onset of labour. Absence of predisposing factors (placenta praevia, contracted pelvis) increases the chances of spontaneous rectification. It is called spontaneous rectification when the vertex becomes the presenting part and spontaneous version when the presenting part is breech.
• Spontaneous evolution—in the presence of strong uterine contractions, head is retained above the pelvic brim, the neck elongates and the breech descends into the pelvis, followed by the trunk and ‘after coming head’. This is similar to spontaneous version but occurs in the pelvis after the onset of uterine contractions.
• Spontaneous expulsion is common if the fetus is dead (is macerated) or is extremely small (may necessitate a low vertical or a ‘J shaped’ incision. The membranes should not be ruptured early to prevent the uterine walls clamping on to the fetus that may make delivery through the uterine incision difficult. Fetal feet could be grasped through the membranes and the fetus may be delivered by breech.
• In the presence of additional risk factors (advanced labour, neglected shoulder presentation, major degree placenta praevia), a classical (upper segment) caesarean section should be considered. If the patient presents in advanced labour with an impacted shoulder, acute tocolysis (terbutaline 250 µg subcutaneously) could be tried to abolish uterine contractions to facilitate delivery.
• In developing countries, neglected shoulder presentation with intrauterine death may still occur due to lack of easy access to the healthcare system. In such cases, the mother may have ketosis, dehydration, chorioamnionitis, and septic shock due to prolonged and obstructed labour. In such cases, performing a Caesarean section increases the risk of maternal morbidity and mortality, especially if facilities are not available for intensive treatment therapy after surgery, to provide multi-organ support. Destructive operations such as decapitation with a Blond–Heidler saw or decapitation hook, and evisceration and decompression of the fetus may be safer options in these circumstances. However, it is important to recognize that destructive operations performed by inexperienced hands can also result in maternal morbidity and mortality due to unintended trauma (uterine perforation and injury to adjacent organs). Further reading
Chandraharan E, Arulkumaran S. Operative delivery, shoulder dystocia and episiotomy. In: Arulkumaran S, Penna LK, Bhasker Rao K (eds) The management of labour, 2nd edn. Orient Longman 2005.
Chandraharan E, Arulkumaran S. Acute tocolysis: Review Article. Curr Opin Obstet Gynecol 2003;17:151–6.
Chhabra S, Bhagwat N, Chakravorty A. Reduction in the occurrence of uterine rupture in Central India. J Obstet Gynaecol 2002;22:39–42.
Fox AJ, Chapman MG. Longitudinal ultrasound assessment of fetal presentation: a review of 1010 consecutive cases. Aust NZ J Obstet Gynaecol 2006;46:341–4.
Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section vs planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Collaborative Group. Lancet 2000;356:1375–83.
Nassar N, Roberts CL, Cameron CA, Olive EC. Diagnostic accuracy of clinical examination for detection of non-cephalic presentation in late pregnancy: cross sectional analytic study. BMJ 2006 16;333:578–80.
Seffah JD. Maternal and perinatal mortality and morbidity associated with transverse lie. Int J Gynaecol Obstet 1999; 65: 115.
Sharma JB. Evaluation of Sharma’s modified Leopold’s maneuvers: a new method for fetal palpation in late pregnancy. Arch Gynecol Obstet 2009;279:481–7.
Uterine inversion Definition
Uterine inversion is a complication of the third stage of labour. After delivery of the fetus, the uterus is partially or completely inverted and protrudes through the cervix, in or outside the vagina. Puerperal uterine inversion can occur after a vaginal delivery or Caesarean section. It can be acute (24 hours postpartum), or chronic (>1 month postpartum). Chronic, non-puerperal uterine inversions can occur rarely and are usually associated with uterine tumours. A simple classification categorizes uterine inversion by severity in four degrees. The first degree (incomplete) involves extension of the inverted fundus to the cervical ring. In second-degree (incomplete) inversion the fundus protrudes through the cervical ring but the inverted uterus remains within the vagina. In the third degree (complete) the inverted fundus extends to the introitus. The fourth degree is a total inversion where the vagina is also inverted (Figs 10.21.1 and 10.21.2). Epidemiology
Uterine inversion is rare with a reported incidence varying between 1 in 2000 and 1 in 6400 deliveries. An even lower incidence of 1 in 20 000–25 000 deliveries has also been reported. The introduction of active management of the third stage of labour may have led to a significant decrease in the incidence of uterine inversion. Aetiology
The most common cause is excessive cord traction on an umbilical cord before complete placental separation. Downward traction on the fundus, usually in combination with uterine atony, results in partial or complete prolapse of the uterine wall through the dilated cervix. A short umbilical cord, fundal implantation of the placenta, morbidly adherent placenta, or uterine anomalies are contributing factors. Clinical presentation
Uterine inversion is often associated with major life-threatening haemorrhage in 94% of cases and shock disproportionate to the estimated blood loss with bradycardia due to increased vagal tone. Other symptoms and signs include acute lower abdominal pain in the third stage. The placenta may or may not be in situ. The uterus is not palpable abdominally. In partial inversion there may be a uterine dimple palpable suprapubically. Pelvic examination may reveal a mass in or outside the vagina.

Fig. 10.21.1 Third-degree uterine inversion.

Fig. 10.21.2 Fourth-degree uterine inversion. Management
Early recognition, rapid, systematic assessment, and simultaneous initiation of resuscitation and management measures are essential, as delay may result in severe morbidity or mortality. Treatment consists of aggressive fluid and blood replacement and appropriate manoeuvres to replace the uterus.
Help
Assistance, including an experienced obstetrician, an anaesthetist, and a senior midwife, is summoned immediately. The blood bank should be notified urgently, and blood and blood products requested.
Assessment and resuscitation
The level of consciousness should be ascertained and airway maintained. Continuous monitoring of blood pressure, pulse, respiratory rate, oxygen saturation, and urine output is mandatory. Oxygen administration should be commenced. Two wide-bore intravenous cannulae are inserted to enable fluid resuscitation and blood transfusion. Blood samples are sent for urgent full blood count, cross-match of 4–6 units, and clotting screen. Intravenous crystalloid infusion is commenced. If the patient is in shock with bradycardia, intravenous atropine is administered. Syntocinon infusion should be stopped until the uterus is replaced. At the same time, appropriate analgesia is administered and preparations are made for transfer to theatre.
Non-surgical management
Replacement of the uterus should be attempted without delay and concurrently to anti-shock measures, as resuscitation may not be successful until the inversion is corrected. Replacement is also more likely to be achieved if attempted before the development of a constriction ring and oedema of the uterus. Immediate non-surgical measures are successful in the vast majority of cases of uterine inversion. The uterine fundus can be replaced manually or by hydrostatic pressure.
Manual replacement (the Johnson manoeuvre)
This should be attempted preferably under general anaesthesia. The uterus may require relaxation for successful manual replacement. Different regimes of tocolytic agents have been used including magnesium sulphate (4–6 g intravenously over 20 minutes), terbutaline (250 µg subcutaneously), ritodrine or a volatile agent for general anaesthesia. The inverted uterus may be replaced by applying constant pressure with the palm on the fundus and the tips of the fingers at the uterocervical junction. The tension that is applied on the uterine ligaments may widen the constriction ring and allow the repositioning of the uterus through the cervix (Fig. 10.21.3).
If the placenta is still in situ, it is not removed until fluid resuscitation has been commenced, and anaesthesia has been administered. Once the uterus is repositioned, the tocolytic agent is discontinued and a hand is kept in the uterine cavity until intravenous oxytocin is given and the uterus is contracted. Then, if still in situ, the placenta is removed and the cavity is gently explored to exclude retained placental tissues or trauma. Bimanual compression may be applied at this stage to improve uterine tone and arrest haemorrhage. After the uterus is well contracted, continuous monitoring is necessary to exclude haemorrhage or recurrence of inversion.
Hydrostatic replacement (O’Sullivan’s technique)
If the attempt to replace the uterus manually immediately is unsuccessful, the woman is transferred to the operating theatre and placed in lithotomy position. Uterine rupture must be excluded and 2 L of warm normal saline are infused into the vagina via a giving set. A silastic ventouse cup may be attached to the giving set. The ventouse cup is placed just inside the introitus and the fluid ran under gravity from a height of 2 m maintaining a seal manually. The hydrostatic pressure that is developed will distend the vaginal walls and the constriction ring and push the uterine fundus upwards.

Fig. 10.21.3 Reduction of uterine inversion. The inverted uterus is replaced by applying firm pressure with a gloved hand. Taken from Sarris et al., Training in obstetrics and Gynaecology (2009), with permission from Oxford University Press.
Surgical management
Laparotomy is the next step if manual attempts fail, usually due to a dense constriction ring around the cervix. In the Huntington’s procedure, after laparotomy, tenaculum or Allis forceps are placed on the fundus of the inverted uterus and gentle traction is applied.
The fundus is pushed from the vagina upwards and simultaneously pulled abdominally. A traction suture placed in the inverted fundus may facilitate replacement. An alternative technique involves passing the suture through the whole thickness of the uterus threading it through a small plastic tube to avoid pulling through the myometrium.
If the constriction ring still prohibits replacement, a longitudinal incision posteriorly, will release the constriction and allow uterine placement (Haultain’s technique). Laparoscopically assisted replacement has also been described. The uterine incision is repaired after replacement. Uterotonics should be commenced after repositioning to keep the uterus contracted. Prevention
Uterine inversion may be prevented by avoiding mismanagement of the third stage. Traction on the umbilical cord should not be excessive and not be applied before the placenta is separated. Further reading
Baskett TF. Acute uterine inversion: a review of 40 cases. J Obstet Gynaecol Can 2002;24:953–6.
Bhalla R, Wuntakal R, Odejinmi F, Khan RU. Acute inversion of the uterus. Obstet Gynaecol 2009;11:13–18.
Brar HS, Greenspoon JS, Platt LD, Paul RH. Acute puerperal uterine inversion. New approaches to management. J Reprod Med 1989;34:173–7.
Calder AA. Emergencies in operative obstetrics. Baillieres Best Pract Res Clin Obstet Gynaecol 2000;14:43–55.
Livingston SL, Booker C, Kramer P, Dodson WC. Chronic uterine inversion at 14 weeks postpartum. Obstet Gynecol 2007;109:555–7.
MOET Managing Obstetric Emergencies and Trauma, The MOET Course Manual. London: RCOG Press 2003.
Paterson-Brown S. Obstetric emergencies. In: Edmonds DK (ed.) Dewhurst’s textbook of obstetrics and gynaecology. Oxford: Blackwell Publishing 2007: 145–58.
Shamsudin F, Morton K. Novel correction technique of chronic puerperal inversion of the uterus. J Obstet Gynaecol 2007;27:197–8.
Thomson AJ, Greer IA. Non-haemorrhagic obstetric shock. Baillieres Best Pract Res Clin Obstet Gynaecol 2000;14:19–41.
Vijayaraghavan R, Sujatha Y. Acute postpartum uterine inversion with haemorrhagic shock: laparoscopic reduction: a new method of management? Br J Obstet Gynaecol 2006;113:1100–2. Internet resources
www.patient.co.uk
More on the topic Chapter 10Care in labour:
- Chapter 10Care in labour
- Spinal anaesthesia
- Arulkumaran S., Regan L., Papageorghiou A.T., Monga A., Farquharson D.I.M.. Oxford Desk Reference: Obstetrics and Gynaecology. Oxford University Press,2011. — 1434 p., 2011
- Detailed contents