Chapter 8 Intrapartum Care
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 11 INTRAPARTUM CARE
Students should be able to discuss the management of the laboring patient, including appropriate triage and diagnosis.
They should understand the options for pain management and describe deviations from normal labor as well as maternal and fetal monitoring. They should be able to describe how to perform a vaginal delivery and to list indications for cesarean delivery.Clinical Case
A healthy, 28-year-old patient presents to labor and delivery at 39 weeks of gestation complaining of “crampiness” overnight. Her vital signs are all stable. The fetal heart tracing is reassuring, and there do not appear to be any regular contractions. What are the next steps in evaluation of this patient? If it appears she is in labor, how might you manage this patient?
 MATERNAL CHANGES BEFORE THE ONSET OF LABOR
MATERNAL CHANGES BEFORE THE ONSET OF LABOR
As a patient approaches term, she experiences uterine contractions of increasing strength and frequency. Spontaneous uterine contractions, which are not felt by the patient, occur throughout pregnancy. Late in pregnancy they become stronger and more frequent, resulting in the patient’s perception of discomfort. These Braxton Hicks contractions (false labor) are not associated with dilation of the cervix, however, and do not fit the definition of labor. It is frequently difficult for the patient to distinguish these often uncomfortable contractions from those of true labor. As a result, it is difficult for the physician to determine the true onset of labor by history alone. Braxton Hicks contractions are typically shorter in duration and less intense than true labor contractions, with the discomfort being characterized as over the lower abdomen and groin areas. It is not uncommon for these contractions to resolve with ambulation, hydration, or analgesia.
True labor is associated with contractions that the patient feels over the uterine fundus, with radiation of discomfort to the low back and lower abdomen. These contractions become increasingly intense and frequent.
Another event of late pregnancy is termed “lightening,” in which the patient reports a change in the shape of her abdomen and the sensation that the baby is lighter, the result of the fetal head descending into the pelvis. The patient may also report that the baby is “dropping.” The patient often notices that her lower abdomen is more prominent, and she may feel a need to urinate more frequently as the bladder is compressed by the fetal head. The patient may also notice that she is breathing more easily, because there is less pressure on the diaphragm as the uterus becomes smaller.
Patients often report the passage of blood-tinged mucus late in pregnancy. This “bloody show” results as the cervix begins thinning (effacement) with the concomitant extrusion of mucus from the endocervical glands and a small amount of bleeding from small vessels in the area. Cervical effacement is common before the onset of true labor, when the internal os is slowly drawn into the lower uterine segment. The cervix is often significantly effaced before the onset of labor, particularly in the nulliparous patient. The mechanism of effacement and dilation and the vectors of the expulsive forces are demonstrated in Figure 8.1.
EVALUATION FOR LABOR
Patients should be instructed to contact their health care provider for any of the following reasons: 1) if their contractions occur approximately every 5 minutes for at least 1 hour, 2) if there is a sudden gush of fluid or a constant leakage of vaginal fluid (suggesting rupture of membranes [ROM]), 3) if there is any significant vaginal bleeding, or 4) if there is significant decrease in fetal movement.
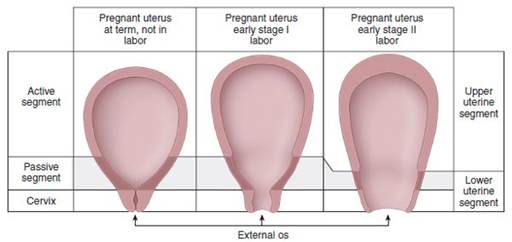
FIGURE 8.1.
Mechanism of effacement, dilation, and labor. With continuing uterine contractions, the upper uterus (active segment) thickens, the lower uterine segment (passive segment) thins, and the cervix dilates. In this way, the fetus is moved downward, into, and through the vaginal canal.Initial Evaluation
At the time of initial evaluation, the prenatal records are reviewed to 1) identify complications of pregnancy up to that point, 2) confirm gestational age to differentiate preterm labor from labor in a term pregnancy, and 3) review pertinent laboratory information. A focused history helps in determining the nature and frequency of the patient’s contractions, the possibility of spontaneous ROM or significant bleeding, or changes in maternal or fetal status. A focused review of systems should look for common complications of pregnancy resulting in altered labor management. A limited general physical examination is performed (with special attention to vital signs), along with the abdominal and pelvic examinations. If contractions occur during this physical examination, they may be palpated for intensity and duration by the examining physician. Auscultation of fetal heart tones is also of critical importance, particularly immediately following a contraction, to determine the possibility of any fetal heart rate deceleration. A limited transabdominal ultrasound may also be useful if there is a question of fetal lie, placental location, or decreased amniotic fluid volume or other abnormalities.
Abdominal Examination
The initial examination of the patient’s abdomen may be accomplished using Leopold maneuvers, a series of four palpations of the uterus and fetus therein through the abdominal wall that helps accurately determine fetal lie, presentation, and position (see Fig. 9.7).
Lie is the relation of the long axis of the fetus to the maternal long axis. It is longitudinal in 99% of cases, occasionally transverse, and rarely oblique (when the axes cross at a 45° angle, usually converting to transverse or longitudinal lie during labor).
presentation is determined by the “presenting part,” that is, that portion of the fetus lowest in the birth canal, palpated during the examination. For example, in a longitudinal lie, the presenting part is either breech or cephalic. The most common cephalic presentation is the one in which the head is sharply flexed onto the fetal chest such that the occiput or vertex presents. position is the relation of the fetal presenting part to the right or left side of the maternal pelvis (Fig. 8.2).The four Leopold maneuvers (see Fig. 9.7) include the following, facilitating several obstetric measurements:
1. Determining what occupies the fundus. In a longitudinal lie, the fetal head is differentiated from the fetal breech, the latter being larger and less clearly defined.
2. Determining location of small parts. Using one hand to steady the fetus, the fingers on the other hand are used to palpate either the firm, long fetal spine or the various shapes and movements indicating fetal hands and feet.
3. Identifying descent of the presenting part. Suprapubic palpation identifies the presenting part as the fetal head, which is relatively mobile, or a breech, which moves the entire body. The extent to which the presenting part is felt to extend below the symphysis suggests the station of the presenting part.
4. Identifying the cephalic prominence. As long as the cephalic prominence is easily palpable, the vertex is not likely to have descended to 0 station.
Palpation of the uterus during a contraction may also be helpful in determining the intensity of that particular contraction. The uterine wall is not easily indented with firm palpation during a true contraction, but may be indented during a Braxton Hicks “contraction.”
Vaginal Examination
A digital vaginal examination allows the examiner to determine the consistency and degree of effacement and degree of dilation of the cervix. This examination should be avoided in women with premature ROM or vaginal bleeding.
Effacement is the shortening of the cervical canal from a length of about 2 cm to a mere circular orifice with almost paper-thin edges. Effacement is expressed as a percent of thinning from a perceived uneffaced state (Fig. 8.3). A cervix that is not effaced, but is softened, is more likely to change with contractions than one that is firm, as it is earlier in pregnancy. If the cervix is not significantly effaced, it may also be evaluated for its relative position, that is, anterior, midposition, or posterior in the vagina. A cervix that is palpable anterior in the vagina is more likely to undergo change in labor sooner than one found in the posterior portion of the vagina. This suggests that the presenting part has descended into the pelvis, creating more pressure on the cervix, thereby rotating it anteriorly. With more effective force on the lower uterine segment, contractions would cause a greater change in dilation and effacement of the cervix.
FIGURE 8.2. Various positions in vertex presentation. LOP, left occiput posterior; LOT, left occiput transverse; LOA, left occiput anterior; ROP, right occiput posterior; ROT, right occiput transverse; ROA, right occiput anterior.

FIGURE 8.3. Effacement and dilation.
Fetal Station
Fetal station is determined by identifying the level of the fetal presenting part in the birth canal in relation to the ischial spines that are located approximately halfway between the pelvic inlet and the pelvic outlet (Fig. 8.4). If the presenting part has reached the level of the ischial spines, it is termed “zero station.” The distance between the ischial spines to the pelvic inlet above and the distance from the spines to the pelvic outlet below are divided into fifths, and these measurements are used to further define station. These divisions represent centimeters above and below the ischial spines.
Thus, as the presenting fetal part descends from the pelvic inlet toward the ischial spines, the designation is −5, −4, −3, −2, −1, then 0 station. The clinical significance of the fetal head presenting at 0 station is that the biparietal diameter of the fetal head, the greatest transverse diameter of the fetal skull, is assumed to have negotiated the pelvic inlet. Below the ischial spines, the presenting fetal part passes +1, +2, +3, +4, with +5 station corresponding to the fetal head being visible at the introitus.
FIGURE 8.4. Station and engagement of the fetal head.
The fetal head is said to be engaged at 0 station, a crucial functional “landmark” in the labor path. However, caput succedaneum, cephalohematoma, and molding of the fetal head may mislead the examiner to erroneously describe a more advanced station than has been actually attained.
STAGES OF LABOR
Although labor is a continuous process, it is divided into four functional stages because each has differing physiological activities and requires differing management.
• The first stage of labor is the interval between the onset of labor and full cervical dilation (10 cm). The first stage is further divided into two phases: 1) The latent phase of labor encompasses cervical effacement and early dilation and 2) the active phase of labor, during which more rapid cervical dilation occurs, usually beginning at approximately 4 cm.
• The second stage of labor encompasses complete cervical dilation through the delivery of the infant.
• The third stage of labor begins immediately after delivery of the infant and ends with the delivery of the placenta.
• The fourth stage of labor is defined as the immediate postpartum period of approximately 2 hours after delivery of the placenta, during which time the patient undergoes significant physiologic adjustment.
Table 8.1 outlines the duration of various stages of labor, which was first described in the research by Emmanuel Friedman, and Figure 8.5 represents this information graphically, known as the Friedman curve. New data, derived since the advent of epidural labor analgesia, suggest that the maximum slope of the normal labor curve during active phase may actually be slightly less steep.
MECHANISM OF LABOR
The mechanisms of labor (also known as the cardinal movements of labor) refer to the changes of the position of the fetus as it passes through the birth canal, as shown in Figure 8.6. The fetus usually descends to where the occipital portion of the fetal head is the lowermost part in the pelvis, and it rotates toward the largest pelvic segment. Because vertex presentation occurs in 95% of term labors, the cardinal movements of labor are defined relative to this presentation. To accommodate to the maternal bony pelvis, the fetal head must undergo several movements as it passes through the birth canal. These movements are accomplished by means of the forceful contractions of the uterus. These cardinal movements of labor do not occur as a distinct series of movements but, rather, as a group of movements that overlap as the fetus accommodates and moves progressively through the birth canal.


FIGURE 8.5. Graphic representation of cervical dilation and station during the first and second stages of labor.
These movements are
1. Engagement
2. Flexion
3. Descent
4. Internal rotation
5. Extension
6. External rotation or restitution
7. Expulsion
Engagement is defined as descent of the biparietal diameter of the head below the plane of the pelvic inlet, suggested clinically by palpation of the presenting part below the level of ischial spines (0 station). Engagement commonly occurs days to weeks prior to labor in women who have not delivered a child, whereas in women who have had children, it more commonly happens at the onset of active labor. In any event, the importance of this event is that it suggests that the bony pelvis is adequate to allow significant descent of the fetal head, although the extension of this to the idea that delivery through the pelvis will happen in the labor does not follow. Flexion of the fetal head allows for the smaller diameters of the fetal head to present to the maternal pelvis. Descent of the presenting part is necessary for the successful completion of passage through the birth canal. The greatest rate of descent occurs during the latter portions of the first stage of labor and during the second stage of labor. internal rotation, like flexion, facilitates presentation of the optimal diameters of the fetal head to the bony pelvis, most commonly from transverse to either anterior or posterior. Extension of the fetal head occurs as it reaches the introitus. To accommodate the upward curve of the birth canal, the flexed head now extends. External rotation occurs after delivery of the head as the head rotates to “face forward” relative to its shoulders. This is known as restitution, followed rapidly by delivery of the body, expulsion.
NORMAL LABOR AND DELIVERY
Ideally, a pregnant woman has a principal, designated health care provider. Beginning with admission to the labor and delivery area, the obstetric team monitors the patient’s progress. Once the patient is in active labor, her provider should be readily available.
General Management
Ambulation and Position in Labor and at Delivery
Walking may be more comfortable than being supine during early labor. Women in early labor are confined to bed if they are too uncomfortable to move about safely or if care maneuvers require it. Supine labor is common in the United States. However, this position obstructs venous return, thence cardiac output, leading to hypotension (supine hypotensive syndrome). The supine left lateral position keeps the uterus off the inferior vena cava, thereby improving cardiac output. The dorsal lithotomy position is most commonly used for spontaneous and operative vaginal delivery in the United States. Elsewhere in the world, many other laboring positions are common, including sitting or crouching, in special “birthing chairs,” on labor balls, or in variously configured tubs of warm water.



FIGURE 8.6. Cardinal movements of labor: engagement (A), flexion (B), descent (c), internal rotation (D), extension (E), and external rotation (F).
Fluid Management and Oral intake
Because labor is associated with decreased gastrointestinal peristalsis, aspiration during the administration of anesthesia is a concern. Patients in active labor should avoid oral ingestion of anything except moderate intake of clear fluids, occasional ice chips, and preparations for moistening the mouth and lips.
When oral intake is not possible or is insufficient, intravenous therapy with 1/2 normal saline or D5 1/2 normal saline is indicated. Normal saline can be used if increased oncotic pressure is desired, but lactated fluids are generally contraindicated because of the metabolic acid deficit incurred by the lactate administration.
Evaluation of Fetal Well-Being
Measurement of the fetal heart rate and its changes during labor is the primary means of intrapartum assessment of fetal well-being, which may be done by intermittent auscultation with a stethoscope or hand-held Doppler or by the use of electronic fetal monitoring. The method chosen may depend on risk assessment at admission, the preference of the patient and the obstetric staff, and department policy. Risk factors may include, but are not limited to, vaginal bleeding, acute abdominal pain, temperature > 100.4°F, preterm labor or ROM, hypertension, and nonreassuring fetal heart rate pattern.
In the absence of risk factors on admission, the standard approach to fetal monitoring is to determine, evaluate, and record the fetal heart rate every 30 minutes in the active phase in the first stage of labor, and at least every 15 minutes in the second stage. In the presence of risk factors, fetal surveillance should be performed using either intermittent auscultation or continuous fetal monitoring. During the active first stage of labor, auscultation should be performed every 15 minutes, preferably before, during, and after a contraction, and continuous monitoring should be evaluated at least every 15 minutes. During the second stage of labor, the fetal heart rate should be monitored every 5 minutes using either the intermittent or continuous procedure. If electronic fetal monitoring is used, an external tocodynamometer is initially used to assess uterine activity, providing information regarding the frequency and duration of contractions but not their intensity. Electronic fetal monitoring is not necessary for a low-risk term pregnancy.
Pain Control
Management of discomfort and pain during labor is an essential part of good obstetric practice. Some patients tolerate pain by using techniques learned in childbirth preparation programs. It is important that bedside staff be knowledgeable about these pain management techniques and be supportive of the patient’s decisions. Unless contraindicated, pharmacologic analgesics to ameliorate pain of contractions should be made available on request to women in labor.
During the first stage of labor, pain results from the contraction of the uterus and dilation of the cervix. This pain travels along the visceral afferents, which accompany sympathetic nerves entering the spinal cord at T10–T12 and L1. As the fetal head descends, there is also distension of the lower birth canal and perineum. This pain is transmitted along somatic afferents that comprise portions of the pudendal nerves that enter the spinal cord at S2–S4. To provide relief from obstetric pain, the following methods of anesthesia and analgesia are used:
• Epidural block: infusion of local anesthetics or narcotics through a catheter into the epidural space. The most effective form of intrapartum pain relief in the United States, it can be used in either vaginal or abdominal deliveries and in postpartum procedures such as tubal ligation.
• Spinal anesthesia: a single injection of anesthetic.
• Combined spinal–epidural: combination of the above two techniques.
• Local block: local injection of anesthetic into the perineum or vagina (e.g., pudendal block; Fig. 8.7).
• General anesthesia: inhaled or intravenous administration of anesthetic agents that results in a loss of maternal consciousness (reserved only for cesarean deliveries in selected cases).
To determine which method of obstetric pain control should be used, the positive and negative aspects of each should be considered. Of the regional modes of analgesia, epidural anesthesia is superior to spinal anesthesia in that it can be left as a continuous source of analgesia and anesthesia during both the labor and delivery process. The advantage of this technique is its ability to provide analgesia during labor as well as excellent anesthesia for delivery, yet is titrated to maintain the patient’s sense of touch and motor ability, facilitating participation in the birth process. Spinal anesthesia provides good pain relief for procedures of limited duration, such as cesarean delivery or vaginal delivery when labor is rapidly progressing. Combined spinal–epidural anesthesia has advantages of both techniques, including the ability to titrate medications throughout labor with the epidural catheter and the rapid onset associated with spinal techniques. All of these types of regional anesthesia may be associated with a postdural puncture headache. However, combined spinal–epidural anesthesia greatly decreases the risk of spinal headache in the mother when using newer atraumatic needles and reduces the risk of sympathetic blockade, which could lead to hypotension. There is also less motor blockade than with spinal anesthesia alone. Local block may provide anesthesia for episiotomy and repair of vaginal and perineal lacerations; however, paracervical block may result in fetal bradycardia. General anesthesia is associated with complications such as maternal aspiration and neonatal depression. If properly administered, it is effective for most cesarean deliveries, but regional anesthesia is preferable.
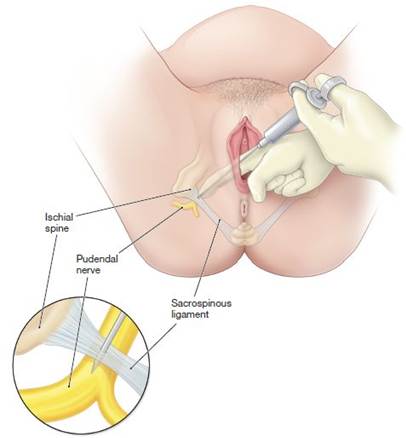
FIGURE 8.7. Pudendal block. Local anesthesia can be administered easily at the time of delivery to provide perineal anesthesia for a vaginal delivery.
Management of Labor
First Stage
Evaluation of the progress of labor is accomplished by means of a series of pelvic examinations. At the time of each vaginal examination, a sterile lubricant is used. Each examination should identify cervical dilation, effacement, station, position of the presenting part, and the status of the membranes. These findings should be noted graphically on the hospital record, so that abnormalities of labor may be identified. During the latter portions of the first stage of labor, patients may report the urge to push, which may indicate significant descent of the fetal head with pressure on the perineum. Pushing should be discouraged at this time in order to avoid traumatic swelling of the cervix caused by the attempt to force the fetus through an incompletely dilated cervix. Should this occur, additional time is needed for the swelling to resolve before complete dilation can be achieved. More frequent vaginal examinations during this time may be necessary. Similarly, if there are significant fetal heart rate decelerations, more frequent examinations may be necessary to determine whether the umbilical cord is prolapsed or if delivery is imminent.
In addition to rupturing the membranes to insert an intrauterine pressure catheter or a fetal scalp monitor, if needed, artificial ROM, known as AROM, may be beneficial in other ways. The presence or absence of meconium (fetal stool) can be identified. However, rupture of the membranes does carry some risk, because the incidence of infection may be increased if labor is prolonged, or umbilical cord prolapse may occur if rupture of the membranes is undertaken before engagement of the presenting fetal part. Spontaneous ROM has similar risks. The fluid should be observed for meconium and blood. Fetal heart tones should be assessed after membranes spontaneously rupture.
Second Stage
Once the second stage of labor has been reached (i.e., complete cervical dilation to 10 cm), voluntary maternal effort (pushing) can be added to the involuntary contractile forces of the uterus to facilitate delivery of the fetus. With the onset of each contraction, the mother is encouraged to inhale, hold her breath, and perform an extended Valsalva maneuver. This increase in intra-abdominal pressure aids in fetal descent through the birth canal.
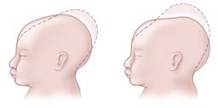
FIGURE 8.8. Molding of head.
During the second stage of labor, the fetal head may undergo further alterations. Molding is an alteration in the relation of the fetal cranial bones, even resulting in partial bone overlap (Fig. 8.8). Some minor degree of molding is common as the fetal head adjusts to the bony pelvis. The greater the disparity between the fetal head and the bony pelvis, the greater the amount of molding. caput succedaneum is the edema of the fetal scalp caused by pressure on the fetal head by the cervix. Molding and caput succedaneum are the two most common causes of overestimation of the amount of descent, that is, of the station of the presenting fetal part. When there is a large amount of space “between the back of the fetal head and the curve of the sacrum,” the physician is alerted to the possibility that the biparietal diameter of the fetal head is higher than might be thought based upon the physical level to which the presenting part’s farthest dimension has reached. An extended second stage may last as long as 2 to 3 hours, and the prolonged resistance encountered by the fetal vertex may prevent appropriate identification of fontanels and sutures. Both caput and molding resolve in the first few days of life. If identified before the second stage of labor, these changes should be noted on the pelvic examination and may indicate a potential problem in negotiation of the birth canal.
An episiotomy facilitates delivery by enlarging the vaginal outlet and may be indicated in cases of instrumental delivery and/or protracted or arrested descent. With progressive labor and control of the fetal head and body at delivery, the risk of obstetric laceration with a normal-sized infant is low, so that the need for episiotomy is minimal. If an episiotomy is needed, it should be performed only after the perineum has been thinned considerably by the descending fetal head. The incision should be somewhat longer on the mucosal surface when compared with the perineal surface of the incision (Fig. 8.9). However, it is important to note that the American College of Obstetricians and Gynecologists (College) recommends that the routine use of episiotomy is not necessary and may lead to an increase in the risk of third-degree and fourth-degree perineal lacerations and a delay in the patient’s resumption of sexual activity. Episiotomy should only be done for a specific medical indication. Median episiotomy is associated with higher rates of injury to the anal sphincter and rectum, and mediolateral episiotomy may be preferable to median episiotomy in selected cases.
As the fetal head crowns (i.e., distends the vaginal opening), it is delivered by extension to allow the smallest diameter of the fetal head to pass over the perineum. This natural mechanism decreases the likelihood of laceration or extension of an episiotomy. To support the perineal tissues and facilitate extension of the head, a modified Ritgen maneuver is performed (Fig. 8.10). This maneuver involves placing one hand over the vertex while the other hand exerts pressure through the perineum onto the fetal chin. A sterile towel is used to avoid contamination of this hand by contact with the anus. The chin can then be delivered slowly, with control applied by both hands.

FIGURE 8.9. Episiotomy.

FIGURE 8.10. Vaginal delivery assisted by modified Ritgen maneuver.
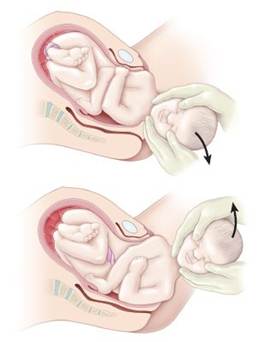
FIGURE 8.11. Delivery of anterior and posterior shoulders.
After delivery of the head, the shoulders descend and rotate to a position in the anteroposterior diameter of the pelvis. The attendant’s hands are placed on the chin and vertex, applying gentle downward pressure, thus delivering the anterior shoulder. To avoid injury to the brachial plexus, care is taken not to put excessive force on the neck. The posterior shoulder is then delivered by upward traction on the fetal head (Fig. 8.11). Delivery of the body now occurs easily in most cases. Immediately after delivery, the uterus significantly decreases in size.
Third Stage
Delivery of the placenta is imminent when the uterus rises in the abdomen, becoming globular in configuration, indicating that the placenta has separated and has entered the lower uterine segment; a gush of blood and/or “lengthening” of the umbilical cord also occur. These are the three classic signs of placental separation. Pulling the placenta from the uterus by excessive traction on the cord should be avoided. Inappropriate application of force may result in inversion of the uterus, an obstetric emergency associated with profound blood loss and shock. Instead, it is appropriate to wait for spontaneous extrusion of the placenta, sometimes up to 30 minutes. As the placenta passes into the lower uterine segment, gentle downward traction is applied to the umbilical cord, while the abdominal hand applies gentle suprapubic counterpressure (posterior and cephalad) to secure the uterine fundus and prevent uterine inversion (Fig. 8.12). If necessary, the placenta may be removed manually. This is accomplished by passing a hand into the uterine cavity and using the side of the hand to develop a cleavage plane between the placenta and the uterine wall. Anesthesia may be required. The umbilical cord should be evaluated for the presence of the expected two umbilical arteries and one umbilical vein.

FIGURE 8.12. Delivery of the placenta.
After the placenta has been removed, the uterus should be palpated to ensure that it has reduced in size and become firmly contracted. Excessive blood loss at this or any subsequent time should suggest the possibility of uterine atony. The use of uterine massage as well as oxytocic agents, such as oxytocin, methylergonovine maleate (methergine), and prostaglandins (carboprost or misoprostol) may be used routinely in the circumstance of excessive postpartum blood loss.
Inspection of the birth canal should be performed in a systematic fashion. The introitus, vagina, perineum, and the vulvar area, including the periurethral area, should be evaluated for lacerations. Ring forceps are commonly used to hold and evaluate the cervix. Lacerations, if present, are most commonly found at the 3 o’clock and 9 o’clock positions of the cervix. Repair is accomplished with an absorbable suture. Obstetric lacerations are classified in Table 8.2.
Fourth Stage
For the first hour after delivery, the likelihood of serious postpartum complications is at its greatest. Postpartum uterine hemorrhage occurs in approximately 1% of patients. It is more likely to occur in cases of rapid labor, protracted labor, uterine enlargement (such as from a large fetus, polyhydramnios, and multiple gestation), or intrapartum chorioamnionitis. Immediately after the delivery of the placenta, the uterus is palpated to determine that it is firm. Uterine palpation is done in this period to ascertain uterine tone. Perineal pads are applied, and the amount of blood on these pads and maternal pulse and blood pressure are monitored closely for the first several hours after delivery to identify excessive blood loss.

LABOR INDUCTION
Labor can be induced when the benefits to either the woman or the fetus outweigh those of continuing the pregnancy. Labor induction can be achieved with intravenous oxytocin administration, cervical ripening, and manipulation of the amniotic membranes.
Oxytocin Administration
The device used to administer oxytocin should permit precise control of the flow rate to ensure accurate, minute-to-minute control. Various regimens exist for stimulation of uterine contractions. These regimens vary in initial dose, amount of incremental dose increase, and interval between dose increases. Lower and less frequent dosage increases are associated with a lower incidence of uterine hyperstimulation. Higher and more frequent dosage increases may result in shorter time in labor and reduce the incidence of chorioamnionitis and the number of cesarean deliveries performed for dystocia (abnormal labor) and also in increased rates of uterine hyperstimulation.
Cervical Ripening
Cervical ripening may be beneficial if the cervix is unfavorable for induction. Several techniques are available. Misoprostol, a prostaglandin E analog, is an effective agent for cervical ripening and induction of labor. It is administered vaginally. Prostaglandin E2 can also be administered vaginally or intracervically. Because of the increased risk of uterine hyperstimulation, both drugs are contraindicated in patients who have had a previous cesarean delivery or previous uterine surgery.
Cervical ripening can also be accomplished with mechanical dilation. One method uses laminaria—hygroscopic rods made from the stems of the seaweed Laminaria japonica that are inserted into the internal cervical os. As the rods absorb moisture and expand, the cervix is slowly dilated (Fig. 8.13). The risks associated with laminaria use include failure to dilate the cervix, cervical laceration, inadvertent ROM, and infection. A synthetic form is also available. Another cervical ripening method is the placement of a 30 mL Foley catheter in the cervical canal.

FIGURE 8.13. Use of laminaria. (A) Laminaria properly inserted just beyond the cervical os. (B) Properly placed laminaria that has expanded, causing cervical dilation.
Membrane Manipulation
Induction of labor by “stripping” or “sweeping” the amniotic membranes has associated risks including infection, bleeding from an undiagnosed placenta previa or low-lying placenta, and accidental ROM.
Artificial ROM is another method of labor induction that may be used, particularly when the cervix is favorable. Routine early amniotomy results in a modest reduction in the length of labor but may result in an increased rate of intraamniotic infection and cesarean delivery for fetal heart rate abnormalities. For these reasons, routine amniotomy is not universally recommended.
CESAREAN DELIVERY
Cesarean delivery is the most common major operation performed in the United States. Until 1965, the rate of cesarean delivery was stable at less than 5%; when it began to increase, it was more than 30% in 2005. Reasons for this increase include the ready availability of improved neonatal intensive care units in which premature and term infants with complications have a significantly greater survival rate, use in breech deliveries, and use in situations in which more sophisticated fetal monitoring is nonreassuring. However, no major improvements in newborn outcomes have occurred as a result.
Decision Making: Mode of Delivery
The decision regarding the mode of delivery should be made by the health care provider together with the patient. Advantages of a successful vaginal delivery include reduced risks of hemorrhage and infection; shorter postpartum hospital stay; and a less painful, more rapid recovery. However, cesarean delivery may be necessary. Examples of indications for cesarean delivery include hemorrhage from placenta previa, abruptio placentae, prolapse of the umbilical cord, and uterine rupture, because these conditions require prompt delivery. Planned vaginal delivery may be a reasonable approach for a fetus in breech presentation but depends on the experience of the health care provider. In such circumstances, women should be informed that the risk of perinatal and neonatal mortality as well as short-term serious neonatal morbidity may be higher with a vaginal delivery than with a cesarean delivery, and the patient’s informed consent should be documented.
Cesarean by Maternal Request
An estimated 2.5% of all births in the United States are cesarean delivery on maternal request. This procedure should not be performed before 39 weeks of gestation. It is not recommended for women desiring several children, because the risks of placenta previa, placenta accreta, and gravid hysterectomy increase with each cesarean delivery.
Risk of Maternal Mortality
Decisions regarding cesarean delivery have important ramifications, because the maternal mortality rate associated with cesarean delivery is two to four times that of a vaginal birth (i.e., 1 per 2,500 to 1 per 5,000–10,000 operations). Cesarean delivery can be performed through various incisions in the uterus. An incision through the thin, lower uterine segment allows for subsequent trials of vaginal birth after cesarean (VBAc) delivery if the patient has had one prior cesarean delivery. An incision through the thick, muscular upper portion of the uterus, a classical cesarean section, carries such a great risk of subsequent uterine rupture that repeat cesarean delivery for these patients is recommended.
TRIAL OF LABOR AFTER CESAREAN DELIVERY
Cesarean deliveries may be performed as repeat procedures. Prior to the mid-1980s, it was believed that a previous cesarean delivery mandated that all subsequent deliveries be abdominal. Trial of labor after cesarean (TOLAc) has long been referred to as a VBAC. Recently, a distinction has been made between the actual trial, or attempt, at VBAC versus the successful occurrence of a VBAC. Publication of data suggesting the safety of TOLAC led to a decade-long clinical trend away from the nearly 70-year-old adage, “Once a cesarean, always a cesarean.” Success rates of VBAC were found to be 60% to 80%. More recently, the pendulum has again swung, resulting in an increasing trend for patients and their physicians to opt for scheduled elective repeat cesarean delivery. Reasons for this change vary from patient to patient. Avoiding uterine rupture (although a small risk) is a worry for many patients. The possibility of a difficult labor without the assurance of a vaginal birth is a concern voiced by many patients. Although the recovery is more prolonged, some patients feel that having a birth experience with which they are familiar makes the repeat cesarean less daunting. The convenience and predictability of a scheduled date for delivery is also attractive to the expectant family.
BOX 8.1 Selected Clinical Factors Associated with Trial of Labor After Previous Cesarean Delivery Success
Increased Probability of Success (Strong Predictors)
• Prior vaginal birth
• Spontaneous labor
Decreased Probability of Success (Other Predictors)
• Recurrent indication for initial cesarean delivery (labor dystocia)
• Increased maternal age
• Non-white ethnicity
• Gestational age greater than 40 weeks
• Maternal obesity
• Preeclampsia
• Short interpregnancy interval
• Increased neonatal birth weight
American College of Obstetricians and Gynecologists. Vaginal Birth after Previous Cesarean Delivery. Practice Bulletin No. 115, Washington, DC: American College of Obstetricians and Gynecologists; August 2010:3.
The risks and benefits of a trial of labor versus repeat cesarean delivery should be discussed with the patient who has had a prior cesarean delivery. Although uterine rupture does occur more often with TOLAC, the frequency is generally less than 1%.
The College’s guidelines for TOLAC include the availability of a 24-hour blood bank, continuous electronic fetal heart rate monitoring, a physician capable of performing a cesarean delivery, in-house anesthesia services, and ability to meet a 30-minute “decision-to-incision” time frame if cesarean delivery becomes necessary. Box 8.1 summarizes clinical considerations for TOLAC.
Clinical Follow-Up
On examination, the patient appears to be in early labor. You offer her the opportunity to walk around for a couple of hours and then return for reexamination. You explain how you will determine if she is in active labor. She is concerned about pain management in labor and you explain her options.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!