Chapter 9 Abnormal Labor and Intrapartum Fetal Surveillance
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 22 ABNORMAL LABOR
TOPIC 26 INTRAPARTUM FETAL SURVEILLANCE
Students should be able to distinguish characteristics of normal and abnormal labor using the physical examination as well as fetal monitoring and tocometry.
They should understand the indications and options for operative vaginal delivery.Clinical Case
After walking for 2 hours, your patient returns to Labor and Delivery, where she is reexamined and found to be 5 cm dilated with regular uterine contractions. She is admitted, given an epidural for pain management, and, after 6 hours, has not progressed past 6 cm dilated. How will you manage her labor at this time? What further evaluation of the patient and fetus might assist in determining the proper management of her labor?
 ABNORMAL LABOR
ABNORMAL LABOR
Abnormal labor, or labor dystocia (literally, “difficult labor or childbirth”), is characterized by the abnormal progression of labor. Dystocia is the leading indication for primary cesarean delivery in the United States. Despite the high prevalence of labor disorders, considerable variability exists in the diagnosis, management, and criteria for dystocia that requires intervention. Because dystocia can rarely be diagnosed with certainty, the relatively imprecise term “failure to progress” has been used, which includes lack of progressive cervical dilation or lack of descent of the fetal head or both.
Factors That Contribute to Normal Labor—The Three Ps
Labor is the occurrence of uterine contractions of sufficient intensity, frequency, and duration to bring about demonstrable effacement and dilation of the cervix. Dystocia results from what have been categorized classically as abnormalities of the “power” (uterine contractions or maternal expulsive forces), “passenger” (position, size, or presentation of the fetus), or “passage” (pelvis or soft tissues).
Uterine Contractions: “Power”
Uterine activity can be monitored by palpation, by external tocodynamometry, or by using intrauterine pressure catheters [IUPCs] (Fig. 9.1). A tocodynamometer is an external strain gauge that is placed on the maternal abdomen. It records the frequency of uterine contractions and relaxations as well as the duration of each contraction. An IUPC, in addition to recording contraction frequency and duration, also directly measures the pressure generated by uterine contractions via a catheter inserted into the uterine cavity. The catheter is attached to a gauge that measures intrauterine pressure in mm Hg.
Recent studies suggest that the use of an IUPC instead of external tocodynamometry does not affect the outcome in cases of abnormal labor. However, an IUPC may be useful in specific situations, such as maternal obesity and other factors that may prevent accurate clinical evaluation of uterine contractions.
For cervical dilation and fetal descent to occur, each uterine contraction must generate at least 25 mm Hg of peak pressure. Optimal intrauterine pressure is 50 to 60 mm Hg. The frequency of uterine contractions is also important in generating a normal labor pattern: the optimal frequency of uterine contractions is a minimum of three contractions in a 10-minute interval, often described as “adequate.” Uterine contractions that are too frequent are not optimal, because they prevent intervals of uterine relaxation. During this “rest interval,” the fetus receives unimpeded uteroplacental blood flow for oxygen and waste transport. Without these rest periods, fetal oxygenation may be compromised.


FIGURE 9.1. Tocodynamometer and intrauterine pressure catheter.
Another unit of measure commonly used to assess contractile strength is the Montevideo unit (MVU).
This unit is the number of uterine contractions in 10 minutes times the average intensity (above the resting baseline intrauterine pressure). Normal progress of labor is usually associated with 200 or more MVU.Fetal Factors: “Passenger”
Evaluation of the passenger includes clinical estimation of fetal weight and clinical evaluation of fetal lie, presentation, position, and attitude. If a fetus has an estimated weight greater than 4,000 to 4,500 g, the risk of dystocia, including shoulder dystocia and fetopelvic disproportion, is greater. Because ultrasound estimation of fetal weight is often inaccurate by as much as 500 to 1,000 g when the fetus is near term (40 weeks of gestational age), this information must be used in conjunction with other parameters when making management decisions.
Fetal attitude, presentation, and lie also play a role in the progress of labor (Fig. 9.2). If the fetal head is turned to one side (asynclitism) or extended (extension), a larger cephalic diameter is presented to the pelvis, thereby increasing the possibility of dystocia. A brow presentation (about 1 in 3,000 deliveries) typically converts to either a vertex or face presentation, but, if persistent, may cause dystocia requiring cesarean delivery. Likewise, a face presentation (about 1 in 600–1,000 deliveries) requires cesarean delivery in most cases. However, a mentum anterior face presentation (chin toward mother’s abdomen) may be delivered vaginally if the fetal head undergoes flexion, rather than the normal extension. A persistent occipitoposterior position is also associated with longer labors (approximately 1 hour in multiparous patients and 2 hours in nulliparous patients). In compound presentations, when one or more limbs prolapse alongside the presenting part (about 1 in 700 deliveries), the extremity usually retracts (either spontaneously or with manual assistance) as labor continues. When it does not, or in the 15% to 20% of compound presentations associated with umbilical cord prolapse, cesarean delivery is required.
Fetal anomalies, such as hydrocephaly and soft tissue tumors, may also cause dystocia. The routine use of prenatal ultrasound for other causes has allowed identification of these situations, significantly reducing the incidence of unexpected dystocia of this kind.
Maternal Factors: “Passage”
A number of maternal factors are associated with dystocia. Dystocia can result from maternal skeletal or soft tissue anomalies that obstruct the birth canal. Cephalopelvic disproportion, in which the size of the maternal pelvis is inadequate to the size of the presenting part of the fetus, may impede fetal descent into the birth canal. Clinical, radiographic, and computed tomography (CT) measurements of the bony pelvis are poor predictors of successful vaginal delivery, due to the inaccuracy of these measurements as well as case-by-case differences in fetal accommodation and mechanisms of labor.

FIGURE 9.2. Some of the fetal factors associated with dystocia.
Clinical pelvimetry, the manual evaluation of the diameters of the pelvis, is also a poor predictor of successful vaginal birth, except in rare circumstances when the pelvic diameters are so small as to render the pelvis “completely contracted.” Although radiographic and CT pelvimetry can be helpful in some cases, the progress of descent of the presenting part in labor is the best test of pelvic adequacy.
Soft tissue causes of dystocia include abnormalities of the cervix, tumors or other lesions of the colon or adnexa, distended bladder, uterine fibroids, an accessory uterine horn, and morbid obesity. Epidural anesthesia may contribute to dystocia by decreasing the tone of the pelvic floor musculature.
Risks
Dystocia may be associated with serious complications for both the woman and the fetus. Infection (chorioamnionitis) is a consequence of prolonged labor, especially in the setting of ruptured membranes. Fetal infection and bacteremia, including pneumonia caused by aspiration of infected amniotic fluid, is linked to prolonged labor.
In addition, there are the attendant risks of cesarean or operative delivery, such as maternal soft tissue injury to the lower genital tract and fetal trauma.Diagnosis and Management of Abnormal Labor Patterns
Graphic documentation of progressive cervical dilation and effacement facilitates assessing a patient’s progress in labor and identifying abnormal labor patterns. The Friedman curve (see Chapter 8) is commonly used for this purpose. Labor abnormalities can be categorized into two general types: protraction disorders, in which labor is slow to progress, and arrest disorders, in which labor ceases to progress (Table 9.1). Protraction can occur during both the latent and active phases of labor, whereas arrest is recognized only in the active phase. Although the definition of the latent phase of labor is controversial, in general it can be defined as the phase in which the cervix effaces but undergoes minimal dilation (see Chapter 8).

Management of abnormal labor encompasses a wide range of options, from observation to operative or cesarean delivery.
Management choice depends on several factors:
• Adequacy of uterine contractions
• Fetal malposition or cephalopelvic disproportion
• Other clinical conditions, such as nonreassuring fetal status or chorioamnionitis
Management decisions should be balanced between ensuring a positive outcome for mother and fetus and avoiding the concomitant risks of operative and cesarean delivery.
First-Stage Disorders
A prolonged latent phase is one that exceeds 20 hours in a nulliparous patient or 14 hours in a multiparous patient. A prolonged latent phase does not necessarily predict an abnormal active phase of labor. Some patients who have initially been diagnosed as having a prolonged latent phase are subsequently found to have been in false labor. A prolonged latent phase does not in itself pose a danger to the mother or fetus.
Options for management of women with a prolonged latent phase of labor include observation and sedation. With either of these options, the patient may stop having contractions, in which case she is not in labor; may go into active labor; or may continue experiencing prolonged labor into the active phase. In the latter case, other interventions as described below may be administered to augment uterine contractions.Once the patient is in active labor, the first stage is considered prolonged when the cervix dilates less than 1 cm/hour in nulliparous women, and less than 1.2 to 1.5 cm/hour in multiparous women. Management options for a prolonged first stage include observation, augmentation by amniotomy or oxytocin, and continuous support. Cesarean delivery is usually warranted if maternal or fetal status becomes nonreassuring.
Augmentation
Augmentation refers to stimulation of uterine contractions when spontaneous contractions have failed to result in progressive cervical dilation or descent of the fetus. Augmentation can be achieved with amniotomy (artificial rupture of membranes [ROM]) and oxytocin administration. Augmentation should be considered if the frequency of contrac-tions is less than 3 contractions per 10 minutes, the intensity of contractions is less than 25 mm Hg above the baseline, or both. Before augmentation, the maternal pelvis and cervix as well as fetal position, station, and well-being should be assessed. If there is no evidence of disproportion and fetal well-being is reassuring, oxytocin can be used if uterine contractions are judged to be inadequate. Contraindications to augmentation are similar to those for labor induction (see Chapter 8).
If the membranes have not ruptured, amniotomy may enhance progress in the active phase and negate the need for oxytocin augmentation. Amniotomy allows the fetal head, rather than the otherwise intact amniotic sac, to be the dilating force. It may also stimulate the release of prostaglandins, which could aid in augmenting the force of contractions.
Amniotomy is usually performed with a thin, plastic rod with a sharp hook on the end. The end is guided to the open cervical os with the examiner’s fingers, and the hook is used to snag and disrupt the amniotic sac. Risks of amniotomy include fetal heart rate (FHR) decelerations due to cord compression and an increased incidence of chorioamnionitis. For these reasons, amniotomy should not be routine and should be used for women with prolonged labor. The FHR should be evaluated both before and immediately after ROM.
It has been shown that amniotomy combined with oxytocin administration early in the active stage reduces labor by up to 2 hours, although there is no change in the rate of cesarean delivery with this treatment protocol. The goal of oxytocin administration is to effect uterine activity sufficient to produce cervical change and fetal descent while avoiding uterine tachysystole (defined as more than five contractions in a 10-minute period, averaged over 30 minutes). Typically, a goal of a maximum of five contractions in a 10-minute period with resultant cervical dilation is considered adequate. Uterine activity > 200 MVUs may also be defined as adequate when utilizing an IUPC to monitor contractions. Oxytocin may be administered in low-dose or high-dose regimens. Low-dose regimens are associated with a decreased incidence and severity of uterine hyperstimulation. High-dose regimens are associated with decreased labor times, incidence of chorioamnionitis, and cesarean delivery for dystocia.
Continuous Labor Support
Continuous support during labor from caregivers (e.g., nurses, midwives, and lay individuals) may have a number of benefits for women and their newborns. Continuous care has been associated with reduced need for pain relief and oxytocin administration, lower rates of cesarean and operative deliveries, decreased incidence of 5-minute Apgar scores lower than 7, and increased patient satisfaction with the labor experience. However, there are insufficient data comparing differences in benefits on the basis of level of training of support personnel—that is, whether the caregivers are nurses, midwives, or doulas. There is no evidence of harmful effects from continuous support during labor.
Second-Stage Disorders
A second-stage protraction disorder should be considered when the second stage exceeds 3 hours if regional anesthesia has been administered, 2 hours if no regional anesthesia is used, or if the fetus descends at a rate of less than 1 cm/hour if no regional anesthesia is used. Second-stage arrest is diagnosed when there is no descent after 1 hour of pushing. In the past, the fetus was thought to be at increased risk for morbidity and mortality when the second stage exceeded 2 hours. Currently, more intensive intrapartum surveillance provides the ability to identify the fetus that may not be tolerating labor well.
Thus, the length of the second stage of labor is not in itself an absolute or even a strong indication for operative or cesarean delivery.
As long as heart tones continue to be reassuring and cephalopelvic disproportion has been ruled out, it is considered safe to allow the second stage to continue. If uterine contractions are inadequate, oxytocin administration can be initiated or the dosage increased if already in place.
Bearing-down efforts by the patient in conjunction with uterine contractions help bring about delivery. Labor positions other than the dorsal lithotomy position (e.g., knee– chest, sitting, squatting, and sitting in a birthing chair) may bring about subtle changes in fetal presentation and facilitate vaginal delivery. Fetal accommodation may also be facilitated by allowing the effects of epidural analgesia to dissipate. The absence of epidural analgesia may increase the tone of the pelvic floor muscles, thereby facilitating the cardinal movements of labor and restoring the urge to push. In some cases of fetal malpresentation, manual techniques can facilitate delivery. If the fetus is in the occipitoposterior position and does not spontaneously convert to the normal position, rotation can be performed to turn the fetus to the anterior position (Fig. 9.3).

FIGURE 9.3. Manual rotation of a fetus in the occipitoposterior position to the occipitoanterior position. (A) The physician’s hand is placed palm upward into the vagina. (B) The hand serves as a wedge to flex the fetal head while the fingers exert a rotating force to bring the occiput to anterior. AF, anterior fontanel. (Adapted from Shields SG, Ratcliffe SD, Fontain P, Leeman L. Dystocia in nulliparous women. Am Fam Physician. 2007;75(11):1675.)
The decision to perform an operative delivery in the second stage versus continued observation should be made on the basis of clinical assessment of the woman and the fetus and the skill and training of the obstetrician. Nonreassuring status of the fetus or mother is an indication for operative or cesarean delivery.
OPERATIVE DELIVERY
Operative vaginal deliveries are accomplished by applying direct traction on the fetal skull with forceps or by applying traction to the fetal scalp by means of a vacuum extractor. The incidence of operative vaginal delivery in the United States is estimated to be 10% to 15%. Although considered safe in appropriate circumstances, operative vaginal delivery has the potential for maternal and neonatal complications. Operative vaginal delivery should be performed only by individuals with privileges for such procedures and in settings in which personnel are readily available to perform a cesarean delivery in the event the operative vaginal delivery is unsuccessful. However, the incidence of intracranial hemorrhage is highest among infants delivered by cesarean delivery following a failed vacuum or forceps delivery. The combination of vacuum and forceps has a similar risk of intracranial hemorrhage. Therefore, an operative vaginal delivery should not be attempted when the probability of success is very low.
Classification
For both forceps and vacuum extraction deliveries, the type of delivery depends on the fetal station—the relationship between the leading portion of the fetal head and the level of the maternal ischial spines. Outlet operative vaginal delivery is the application of forceps or vacuum under the following conditions:
1. The scalp is visible at the introitus without separating labia. 2. The fetal skull has reached pelvic floor.
3. The sagittal suture is in anteroposterior diameter or right or left occiput anterior or posterior position.
4. The fetal head is at or on the perineum.
5. Rotation does not exceed 45°.
Low operative vaginal delivery is the application of forceps or vacuum when the leading point of the fetal skull is at station +2 or more and is not on the pelvic floor. This type of operative vaginal delivery has two subtypes:
1. Rotation of 45° or less (left or right occiput anterior to occiput anterior, or left or right occiput posterior to occiput posterior)
2. Rotation greater than 45°
Midpelvis operative vaginal delivery is the application of forceps or vacuum when the fetal head is engaged but the leading point of the skull is above station +2. Under very unusual circumstances, such as the sudden onset of severe fetal or maternal compromise, application of forceps or vacuum above station +2 may be attempted while simultaneously initiating preparation for a cesarean delivery in the event that the operative vaginal delivery is unsuccessful.
Indications and Contraindications
No indication for operative vaginal delivery is absolute. The following indications apply when the fetal head is engaged and the cervix is fully dilated:
• Prolonged or arrested second stage of labor
• Suspicion of immediate or potential fetal compromise
• Shortening of the second stage for maternal benefit
In certain situations, operative vaginal delivery should be avoided or, at the least, carefully considered in terms of relative maternal and fetal risks. Most authorities consider vacuum extraction inappropriate in pregnancies before 34 weeks of gestation because of the risk of fetal intraventricular hemorrhage. Operative delivery is also contraindicated if a live fetus is known to have a bone demineralization condition (e.g., osteogenesis imperfecta) or a bleeding disorder (e.g., alloimmune thrombocytopenia, hemophilia, and von Willebrand disease), and if the fetal head is unengaged or the position of the fetal head is unknown.
Forceps
Forceps are primarily used to apply traction to the fetal head to augment the expulsive forces, when the mother’s voluntary efforts in conjunction with uterine contractions are insufficient to deliver the infant (Fig. 9.4). Occasionally, forceps are used to rotate the fetal head before applying traction to complete vaginal delivery. Forceps may also be used to control delivery of the fetal head, thereby avoiding precipitous delivery. Different types of forceps are available for the different degrees of molding of the fetal head.
Maternal complications of forceps delivery include perineal trauma, hematoma, and pelvic floor injury. Neonatal risks include injuries to the brain and spine, musculoskeletal injury, and corneal abrasion if the forceps are mistakenly applied over the neonate’s eyes. The risk of shoulder dystocia, in which the fetus’s anterior shoulder becomes lodged against the pubic symphysis, is increased in forceps deliveries of infants weighing over 4,000 g.

FIGURE 9.4. Forceps delivery. (Adapted from Bofill JA. Forceps in Obstetrics [Slide presentation]. Washington, DC: American College of Obstetricians and Gynecologists; 2001.)

FIGURE 9.5. Vacuum extractor. Because the vacuum port can be bent at a 90° angle to the cup, it is useful in malpositions of the fetal head. (Adapted from Bofill JA. Safe Vacuum Delivery [Slide presentation]. Washington, DC: American College of Obstetricians and Gynecologists; 2001.)
Vacuum Extraction
In vacuum extraction, a soft vacuum cup is applied to the fetal head and suction is exerted by means of a mechanical pump (Fig. 9.5). Vacuum extraction is associated with less maternal trauma than forceps but carries significant potential neonatal risks. Although the amount of traction applied to the fetal skull is less than that applied with forceps, it is still substantial and can cause serious fetal injury. Neonatal risks include intracranial hemorrhage, subgaleal hematomas, scalp lacerations (if torsion is excessive), hyperbilirubinemia, and retinal hemorrhage. In addition, separation of the scalp from the underlying structures can lead to cephalohematoma. Overall, the incidence of serious complications with vacuum extraction is approximately 5%. It is recommended that rocking movements or torque should not be applied to the device and that only steady traction in the line of the birth canal should be used. Clinicians caring for the neonate should also be alerted that an operative delivery has been used so that they can monitor the neonate for signs and symptoms of injury.
BREECH PRESENTATION
Breech presentation occurs in about 2% of singleton deliveries at term and more frequently in the early third and second trimesters. In addition to prematurity, other conditions associated with breech presentation include multiple pregnancy, polyhydramnios, hydrocephaly, anencephaly, aneuploidy, uterine anomalies, and uterine tumors. The three kinds of breech presentation—frank, complete, and incomplete (footling) breech (Fig. 9.6)—are diagnosed by a combination of Leopold maneuvers, pelvic examination, ultrasonography, and other imaging techniques (Fig. 9.7). The morbidity and mortality rates for mother and fetus, regardless of gesta-tional age or mode of delivery, are higher in the breech than in the cephalic presentation. This increased risk to the fetus comes from associated factors such as fetal anomalies, prematurity, and umbilical cord prolapse as well as birth trauma.

FIGURE 9.6. Types of breech presentations. (A) Frank breech, in which the feet are near the head; (B) complete breech, in which the legs are crossed; (C) incomplete (footling) breech, in which one or both feet are extended.
External cephalic version (ECV) involves applying pressure to the mother’s abdomen to turn the fetus in either a forward or backward somersault to achieve a vertex presentation prior to labor (Fig. 9.8). The goal of ECV is to increase the proportion of vertex presentations among fetuses that were formerly in the breech position near term. Once a vertex presentation is achieved, the chances for a vaginal delivery increase. This maneuver is successful in approximately half of the properly selected cases. Patients who have completed 36 weeks of gestation are preferred candidates for ECV for several reasons. First, if spontaneous version is going to occur, it is likely to have taken place by 36 completed weeks of gestation. Second, the risk of a spontaneous reversion is decreased after ECV at term compared with earlier gestations. Selection criteria include a normal fetus with reassuring fetal heart tracing, adequate amniotic fluid, and presenting part not in the pelvis. The risks include premature ROM, placental abruption, cord accident, and uterine rupture. External version is more often successful in parous women. Existing evidence may support the use of a tocolytic agent (i.e., a drug that stops uterine contractions) during ECV attempts, particularly in nulliparous patients. Administration of anti-D immunoglobulin to Rh-negative women is recommended.

FIGURE 9.7. Leopold maneuvers. The maneuvers are used to determine fetal position: 1) determination of what is in the fundus; 2) evaluation of the fetal back and extremities; 3) palpation of the presenting part above the symphysis; and 4) determination of the direction and degree of flexion of the head.
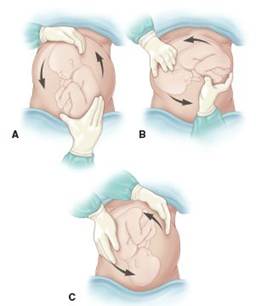
FIGURE 9.8. External cephalic version. In this maneuver, the fetus is converted from a breech to a vertex presentation.
In light of recent studies that further clarify the long-term risks of vaginal breech delivery, the decision regarding the mode of delivery should depend on the experience of the health care provider. Cesarean delivery will be the preferred mode for most physicians because of the diminishing expertise in vaginal breech delivery. Planned vaginal delivery of a term singleton breech fetus may be reasonable under hospital-specific protocol guidelines for both eligibility and labor management. The following criteria have been suggested for vaginal breech delivery:
• Normal labor curve
• Gestational age greater than 37 weeks
• Frank or complete breech presentation (because of the risk of umbilical cord prolapse, vaginal delivery of a fetus in the footling breech position is not recommended)
• Absence of fetal anomalies on ultrasound examination
• Adequate maternal pelvis
• Estimated fetal weight between 2,500 and 4,000 g
• Documentation of fetal head flexion (hyperextension of the fetal head occurs in about 5% of term breech fetuses, requiring cesarean delivery to avoid head entrapment)
• Adequate amniotic fluid volume (defined as a 3-cm vertical pocket)
• Availability of anesthesia and neonatal support
If a vaginal breech delivery is planned, the woman should be informed that the risk of perinatal or neonatal mortality or short-term serious neonatal morbidity may be higher than in a cesarean delivery, and the patient’s informed consent should be documented.
SHOULDER DYSTOCIA
Shoulder dystocia may sometimes arrest expulsion. Shoulder dystocia cannot be predicted or prevented, because accurate methods for identifying which fetuses will experience this complication do not exist. Antepartum conditions associated with shoulder dystocia include multiparity, postterm gestation, previous history of a macrosomic birth, and a previous history of shoulder dystocia. Although fetal macrosomia increases the risk of shoulder dystocia, elective induction of labor or elective cesarean delivery for all women suspected of carrying a fetus with macrosomia is not appropriate.
Diagnosis of shoulder dystocia has a subjective component, especially in less severe forms. The delivered fetal head may retract against the maternal perineum (turtle sign) and, if so, may assist in the diagnosis. Interventions that may be used to facilitate delivery include the McRoberts maneuver (hyperflexion of the mother’s legs tight to the abdomen) and the application of suprapubic pressure to assist in dislodging the impacted shoulder (Fig. 9.9). In contrast, fundal pressure may further worsen impaction of the shoulder and may also result in uterine rupture. Controversy exists as to whether episiotomy is necessary, because shoulder dystocia is typically not caused by obstructing soft tissue. Direct fetal manipulation with either rotational maneuvers or delivery of the posterior arm may also be used. In severe cases, more aggressive interventions, such as the Zavanelli maneuver (in which the fetal head is flexed and reinserted into the vagina to reestablish umbilical cord blood flow and delivery performed through cesarean section) and intentional fracture of the fetal clavicle, may be performed. Regardless of the procedures used, brachial plexus injury is associated with shoulder dystocia; incidence ranges from 4% to 40%. However, most cases resolve without permanent disability. Fewer than 10% of all cases of shoulder dystocia result in a persistent brachial plexus injury.
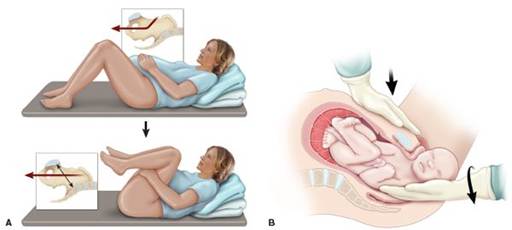
FIGURE 9.9. Procedures used to relieve shoulder dystocia. (A) McRoberts maneuver. Hyperflexion and abduction of the hips cause cephalad rotation of the symphysis pubis and flattening of the lumbar lordosis that frees the impacted shoulder. (B) Suprapubic pressure directed downward on the anterior shoulder and laterally toward the baby’s sternum.
INTRAPARTUM FETAL SURVEILLANCE
Evidence suggesting a nonreassuring fetal status during labor occurs in 5% to 10% of pregnancies. Intrapartum fetal surveillance is the indirect measurement of indicators of fetal status, such as FHR, blood gases, pulse rate, amniotic fluid volume, and fetal stimulation responses, during labor. The goal of intrapartum fetal surveillance is to recognize changes in fetal oxygenation that could result in serious complications. However, it is now recognized that many neurologic conditions previously attributed to birth asphyxia (defined as a situation of damaging acidemia, hypoxia, and metabolic acidosis) are in fact attributable to other causes not associated with labor, such as maternal infection, coagulation disorders, and autoimmune disorders; genetic causes; and low birthweight. Intrapartum fetal surveillance is a tool for detection of events that occur during labor that could compromise fetal oxygenation and, in rare cases, lead to permanent neurologic disability.
Pathophysiology
The uteroplacental unit provides oxygen and nutrients to the fetus while receiving carbon dioxide and wastes, the products of the normal aerobic fetal metabolism. Uteroplacental insufficiency occurs when the uteroplacental unit is compromised. Initial fetal responses include fetal hypoxia (decreased blood oxygen levels); shunting of blood flow to the fetal brain, heart, and adrenal glands; and transient, repetitive, late decelerations of the FHR. If hypoxia continues, the fetus will eventually switch over to anaerobic glycolysis and develop metabolic acidosis. Lactic acid accumulates, and progressive damage to vital organs occurs, especially the fetal brain and myocardium. If intervention is not timely, serious and possibly permanent damage and sometimes death can result.
Neonatal Encephalopathy
Neonatal encephalopathy is a clinically defined syndrome of disturbed neurologic function in the earliest days of life in the term infant, manifested by difficulty with initiating and maintaining respiration, depression of tone and reflexes, subnormal level of consciousness, and sometimes seizures. Neonatal encephalopathy is not always associated with permanent neonatal neurologic impairment. Hypoxic-ischemic encephalopathy (HIE) is a subtype of neonatal encephalopathy for which the cause is considered to be the limitation of oxygen and blood flow near the time of birth. Historically, it has been assumed that most cases of neonatal encephalopathy were HIE, but epidemiologic studies have established that this assumption is incorrect.
Approximately 70% of cases of neonatal encephalopathy are caused by factors that were present before the onset of labor. It is estimated that the incidence of neonatal encephalopathy caused by intrapartum hypoxia is approximately 1.6/10,000, in the absence of any other coincident preconceptual or antepartum abnormalities. HIE is, thus, one among the larger category of encephalopathies that may result from conditions such as prenatal stroke, prenatal infection, genetic abnormalities, and neonatal cerebral malformation. The criteria sufficient to suggest that an encephalopathy is associated with an acute intrapartum event are presented in Box 9.1.
BOX 9.1 Criteria to Define an Acute Intrapartum Hypoxic Event as Sufficient to Cause Cerebral Palsy
I. Essential criteria (must meet all four)
a. Fetal metabolic acidosis demonstrated from umbilical cord arterial blood gas measurement (pH < 7 and base deficit ≥12 mmol/L)
b. Early-onset severe or moderate neonatal encephalopathy in newborn of ≥34 weeks of gestational age
c. Spastic or, less commonly, dyskinetic cerebral palsy d. Exclusion of other identifiable causes (trauma, coagulopathy, infection, or genetic anomaly)
II. Criteria nonspecific to asphyxial insult, but suggestive of intrapartum timing (close proximity to labor and delivery, within 48 hours)
a. Sentinel hypoxic event immediately before or during labor
b. Sudden nonreassuring fetal heart rate pattern (e.g., sudden, sustained fetal bradycardia or absent variability in the presence of persistent late or variable decelerations)
c. Apgar scores of 0 to 3 beyond 5 minutes
d. Onset of multisystem illness (e.g., acute bowel injury, renal failure, hepatic failure, cardiac damage, and hematologic abnormalities) within 72 hours of birth e. Early cerebral imaging with evidence of acute nonfocal cerebral abnormality
From ACOG Task Force on Neonatal Encephalopathy and Cerebral Palsy. Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology. Washington, DC: American College of Obstetricians and Gynecologists; 2003:74.
Cerebral Palsy
Cerebral palsy is a chronic disability of the central nervous system (CNS) characterized by aberrant control of movement and posture appearing early in life and not as a result of progressive neurologic disease. Only one type of cerebral palsy, spastic quadriplegia, is associated with antepartum or intrapartum interruption of the fetal blood supply. Disorders not associated with intrapartum or peripartum asphyxia include dyskinetic or ataxic cerebral palsy (which commonly has a genetic origin) and epilepsy, mental retardation, or attention-deficit hyperactivity disorders.
Intrapartum Fetal Heart Rate Monitoring
FHR monitoring is a modality intended to determine if a fetus is well oxygenated. The majority of neonates (approximately 85%) born in the United States are assessed with electronic fetal monitoring (EFM), making it the most common obstetric procedure. Intermittent auscultation of the FHR after a contraction is also used to assess intrapartum fetal well-being. Beginning in the 1980s, EFM became more common; the rates of its use have doubled over the past 35 years.
EFM may be performed externally or internally. Most external monitors use a Doppler device with computerized logic to interpret and count the Doppler signals. Internal FHR monitoring is accomplished with a fetal electrode, which is a spiral wire placed directly on the fetal scalp or other presenting part.
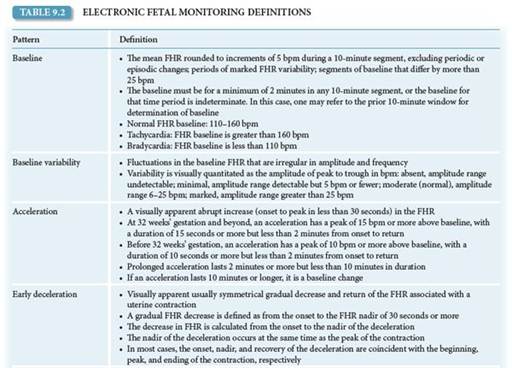
FHRs by EFM are described in terms of baseline rate, variability, presence of accelerations, periodic or episodic decelerations, and the changes in these characteristics over time (Table 9.2) and classified by a three-tier FHR interpretation system (Box 9.2). The goal of FHR monitoring is to detect signs of fetal jeopardy in time to intervene before irreversible damage occurs. Despite the liberal use of continuous EFM in both high-risk and low-risk patients, there has been no consistent decrease in the frequency of cerebral palsy in the last two decades. Fetuses who are severely asphyxiated during the intrapartum period will have abnormal heart rate patterns. However, most patients with nonreassuring FHR patterns give birth to healthy infants. In addition, the false-positive rate of EFM for predicting adverse outcomes is high. Guidelines for intrapartum FHR monitoring are given in Table 9.3.
Fetal Heart Rate Patterns
The normal baseline FHR is 110 to 160 beats per minute (bpm). An FHR less than 110 bpm is considered bradycardia. Fetal bradycardia between 100 and 110 bpm can usually be tolerated for long periods when it is accompanied by normal FHR variability. An FHR between 80 and 100 bpm is nonreassuring. An FHR that persists below 80 bpm is an ominous sign and may presage fetal death.
An FHR above 160 bpm is considered tachycardia. The most common cause of fetal tachycardia is chorioamnionitis, but it may also be due to maternal fever, thyrotoxicosis, medication, and fetal cardiac arrhythmias. Fetal tachycardia between 160 and 200 bpm without any other abnormalities in FHR is usually well tolerated when accompanied by normal FHR variability.
Fetal Heart Rate Variability
FHR variability refers to the fluctuations in the FHR of two cycles or more, visually quantified as the amplitude of peak to trough in bpm. FHR is graded according to amplitude range (Fig. 9.10; also see Table 9.2). Moderate variability is a reassuring sign that reflects adequate fetal oxygenation and normal brain function. In the presence of normal FHR variability, regardless of what other FHR patterns exist, the fetus is not experiencing cerebral tissue asphyxia.
Decreased variability is associated with fetal hypoxia, acidemia, drugs that may depress the fetal CNS (e.g., maternal narcotic analgesia), fetal tachycardia, fetal CNS and cardiac anomalies, prolonged uterine contractions (uterine hypertonus), prematurity, and fetal sleep.

BOX 9.2 Three-Tier Fetal Heart Rate Interpretation System
CATEGORY I
Category I fetal heart rate (FHR) tracings include all of the following:
• Baseline rate: 110 to 160 bpm
• Baseline FHR variability: moderate
• Late or variable decelerations: absent
• Early decelerations: present or absent
• Accelerations: present or absent
CATEGORY II
Category II FHR tracings include all FHR tracings not categorized as category I or category III. Category II tracings may represent an appreciable fraction of those encountered in clinical care. Examples of category II FHR tracings include any of the following:
Baseline Rate
• Bradycardia not accompanied by absent baseline variability
• Tachycardia
Baseline FHR Variability
• Minimal baseline variability
• Absent baseline variability not accompanied by recurrent decelerations
• Marked baseline variability
Accelerations
• Absence of induced accelerations after fetal stimulation
Periodic or Episodic Decelerations
• Recurrent variable decelerations accompanied by minimal or moderate baseline variability
• Prolonged deceleration ≥2 minutes but 7.20 if delivery were to occur at the time of measurement. For this reason, fetal scalp stimulation is sometimes used as a test of fetal well-being. External vibration stimulation, also termed vibroacoustic stimulation, elicits the same response and is also used for this purpose (see Section “Ancillary Tests”).

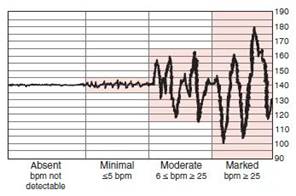
FIGURE 9.10. Fetal heart rate (FHR) variability. bpm, beats per minute.
Decelerations
FHR decelerations are visually apparent decreases in FHR from the baseline. They can be either gradual (onset to nadir in 30 seconds or more) or abrupt (onset to nadir in less than 30 seconds). Early decelerations are associated with uterine contractions: the nadir of the deceleration occurs at the same time as the peak of the uterine contraction and, thus, is a “mirror image” of the contraction (Fig. 9.11). Early decelerations are the result of pressure on the fetal head from the birth canal, digital examination, or forceps application that causes a reflex response through the vagus nerve with acetylcholine release at the fetal sinoatrial node. This response may be blocked with vagolytic drugs such as atropine. Early FHR decelerations are considered physiologic and are not a cause of concern.

FIGURE 9.11. Fetal heart rate (FHR) patterns. (A) Early deceleration. Notice how the nadir of the deceleration occurs at the same time as the peak of the uterine contraction; they are mirror images of each other. (B) Variable deceleration. These decelerations may start before, during, or after a uterine contraction starts. (C) Late deceleration. The onset, nadir, and recovery of the deceleration occur, respectively, after the beginning, peak, and end of the contraction.
Late FHR decelerations are visually apparent decreases in the FHR from the baseline FHR, associated with uterine contractions. The onset, nadir, and recovery of the deceleration occur, respectively, after the beginning, peak, and end of the contraction. Late decelerations are considered significantly nonreassuring, especially when repetitive and associated with decreased variability. Repetitive late decelerations are defined as occurring after 50% or more of contractions in a 20-minute period. Late decelerations are associated with uteroplacental insufficiency, as a result of either decreased uterine perfusion or decreased placental function, and, thus, with decreased intervillous exchange of oxygen and carbon dioxide and progressive fetal hypoxia and acidemia.
Variable FHR decelerations are abrupt, visually apparent decreases in the FHR below the baseline FHR. These variable decelerations may start before, during, or after uterine contraction starts, hence the term “variable.” Variable decelerations are also mediated through the vagus nerve, with sudden and often erratic release of acetylcholine at the fetal sinoatrial node, resulting in their characteristic sharp deceleration slope. They are usually associated with umbilical cord compression, which may result from wrapping of the cord around parts of the fetus, fetal anomalies, or even knots in the umbilical cord. They are also commonly associated with oligohydramnios, in which the buffering space for the umbilical cord created by the amniotic fluid is lost. Variable decelerations are the most common periodic FHR pattern. They are often correctable by changes in the maternal position to relieve pressure on the umbilical cord. Infusion of fluid into the amniotic cavity (amnioinfusion) to relieve umbilical cord compression in cases of oligohydramnios or when ROM has occurred has been shown to be effective in decreasing the rate of decelerations and cesarean delivery.
Ancillary Tests
Because the rate of false-positive diagnosis of EFM is high, attempts have been made to find ancillary tests that help confirm a nonreassuring FHR tracing.
Fetal Stimulation
In the case of an EFM tracing with decreased or absent variability without spontaneous accelerations, an effort should be made to elicit one. Four techniques are available to stimulate the fetus: 1) fetal scalp sampling, 2) Allis clamp scalp stimulation, 3) digital scalp stimulation, and 4) vibroacoustic stimulation. Each of the first three techniques involves accessing the fetal scalp through the dilated cervix. In vibroacoustic stimulation, the fetus is stimulated when the device is placed on the maternal abdomen over the area of the fetal head. In digital scalp stimulation, the physician uses his or her finger to gently stroke the scalp.
Each of these tests is a reliable method to exclude acidosis if accelerations are noted after stimulation. Because vibroacoustic stimulation and scalp stimulation are less invasive than the other two methods, they are the preferred methods. When there is an acceleration following stimulation, acidosis is unlikely and labor can continue.
Determination of Fetal Blood pH or Lactate
When a nonreassuring FHR tracing persists without spontaneous or stimulated accelerations, a scalp blood sample for the determination of pH or lactate can be considered (Fig. 9.12). However, the use of scalp pH has decreased, and it may not be available at some tertiary hospitals. Furthermore, the positive predictive value of a low scalp pH to identify a newborn with HIE is only 3%.
Pulse Oximetry
The use of pulse oximetry has been suggested as a modality to reduce the false-positive diagnosis of a nonreassuring FHR. However, research has demonstrated that neither the overall rate of cesarean delivery nor the rate of umbilical arterial pH less than 7 decreased when pulse oximetry was used in association with EFM in cases of nonreassuring fetal status. Because of the uncertain benefit of pulse oximetry and concerns about falsely reassuring fetal oxygenation, use of the fetal pulse oximeter in clinical practice cannot be supported at this time.

FIGURE 9.12. Fetal scalp sampling.
Diagnosis and Management of a Persistently Nonreassuring Fetal Heart Rate Pattern
A reassuring FHR pattern (category I) may include a normal baseline rate, moderate FHR variability, persistence of accelerations, and absence of decelerations. Patterns believed to be predictive of current or impending fetal asphyxia (category III) include absence of FHR variability and recurrent late decelerations, recurrent severe variable decelerations, and sustained bradycardia. An indeterminant FHR pattern (category II) is one that falls between these two extremes.
In the presence of an indeterminate (category II) or nonreassuring (category III) FHR pattern, the etiology should be determined, if possible, and an attempt should be made to correct the pattern by addressing the primary problem. If the pattern persists, initial measures include placing the patient in the left lateral position, administering oxygen, correcting maternal hypotension, and discontinuing oxytocin, if appropriate. Where the pattern does not respond to change in position or oxygenation, the use of tocolytic agents has been suggested to abolish uterine contractions and prevent umbilical cord compression. Uterine tachysystole can be identified by evaluating uterine contraction frequency and duration and can be treated with β-adrenergic drugs. Amnioinfusion may also be used to prevent umbilical cord compressions. Awaiting vaginal delivery is appropriate if it has been determined that delivery is imminent. If it is not, and there is evidence of progressive fetal hypoxia and acidosis, cesarean delivery is warranted.
MECONIUM
Meconium is a thick, black, tarry substance that is present in the fetal intestinal tract. It is composed of amniotic fluid, lanugo (the fine hair that covers the fetus), bile, and fetal skin and intestinal cells. The neonate’s first stool consists of meconium. However, the fetus may pass the meconium in utero, which is a sign of fetal stress. Meconium passage is detected during labor when the amniotic fluid is stained dark green or black. Meconium-stained amniotic fluid is present in about 10% to 20% of births, and most meconium-stained neonates do not develop problems.
Meconium aspiration syndrome, a condition caused by inhalation of meconium-stained amniotic fluid by the fetus, occurs in about 6% of births in which meconium is present. Severe cases of this syndrome may cause pneumonitis, pneumothorax, and pulmonary artery hypertension.
When there is thick meconium at delivery, interventions to prevent or decrease meconium aspiration syndrome should be considered. Because meconium passage may predate labor, amnioinfusion should not be used as a preventive measure for meconium aspiration syndrome. Suctioning of the upper airway on the perineum does not prevent or alter the course of meconium aspiration syndrome. If the infant is not vigorous and thick meconium is present, the fetus should be intubated and suctioning to remove material below the glottis should be performed before initiating positive pressure ventilation. If the infant is active, suctioning and intubation are therapeutic options that are part of ongoing stabilization and care; however, they are likely unnecessary in the vigorous infant.
Clinical Follow-Up
The fetal heart rate is a category I, and your patient previously delivered an 8-lb infant vaginally. You decide to artificially rupture her membranes, and, if her contractions do not subsequently become adequate, you plan to augment her labor with oxytocin. You evaluate the estimated fetal weight and position of the fetal vertex in the pelvis prior to augmenting her labor.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!