Chapter 10 Immediate Care of the Newborn
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 12 IMMEDIATE CARE OF THE NEWBORN
Students should be able to discuss techniques for care and assessment of the newborn and to recognize more acute situations requiring more immediate intervention or resuscitation.
Students should understand the risks and benefits of circumcision.Clinical Case
You are attending the birth of the much awaited child of a young couple. The father and both sets of grandparents are in the delivery room looking forward with anticipation of the baby boy being handed into his mother’s arms. The labor had been unremarkable except for mild meconium staining of the amniotic fluid until the last minutes of the second stage when descent to delivery seemed beyond the expulsive efforts of the exhausted patient, and deep variable decelerations are noted. Prenatal clinical pelvimetry had been judged as gynecoid and normal. The estimated fetal weight was 6 lb, and the vertex was occiput-anterior and just at the level of the perineum. The cervix, of course, was fully dilated and effaced. It was suggested to the parents that a vacuum-assisted vaginal delivery would be prudent, and, with explanation, they gave consent for the operative obstetric procedure.
 INITIAL CARE OF THE WELL NEWBORN
INITIAL CARE OF THE WELL NEWBORN
Delivery Room Assessment of the Newborn
In accordance with the American Heart Association (AHA) and the American Academy of Pediatrics (AAP), at least one person skilled in neonatal assessment and resuscitation should be available at every delivery to care for the newborn. Thus, every delivering physician should know the initial assessment, resuscitation, and care of a newborn infant and, if not able to perform all the tasks of resuscitation, should strive to have someone who is proficient in these skills immediately available at delivery.
The preterm newborn has special needs; these complications are discussed in Chapter 15.
Immediately following delivery, the newborn infant should be first assessed to decide whether resuscitation is necessary. Four characteristics define a newborn that requires no additional resuscitation:
1. A full-term infant
2. Clear amniotic fluid with no evidence of meconium and infection
3. Spontaneous breathing and crying
4. Good muscle tone
Ballard Scoring System
In an effort to predict which newborns will require more intensive resuscitation, the gestational age should be estimated as accurately as possible prior to delivery. This allows the appropriate neonatal team to be present and prepared for resuscitation. It is also possible to assess the infant gestational age after delivery using the Ballard scoring system. The Ballard scoring system uses a specified set of physical examinations of neuromuscular and physical maturity which, when scored, yields an estimated gestational age (Fig. 10.1).
Apgar Scoring System
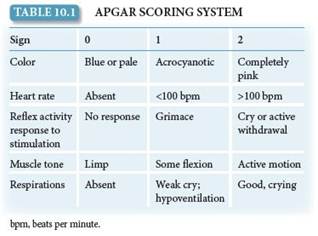
The Apgar scoring system is commonly used as an objective means to assess the newborn’s condition (Table 10.1). Five signs are given scores of 0, 1, or 2, for a total of up to 10. Scores are assigned at 1 and 5 minutes, and at every 5 minutes until 20 minutes thereafter if the 5-minute Apgar score is less than 7. Although these continued assessments are not part of the original Apgar scoring system, many clinicians find them to be of value in evaluating how an infant is responding to resuscitation. An Apgar score of 7 to 10 is indicative of an infant who requires no active resuscitative intervention; a score of 4 to 7 is considered indicative of a mildly to moderately depressed infant; and a score of less than 4 is suggestive of a severely depressed infant who requires immediate resuscitative efforts. The Apgar score should not be used to define birth asphyxia, because it is not designed to do so and, indeed, does not provide such information.
Likewise, the term asphyxia should not be loosely used in relation to Apgar scores. This term is well defined and is addressed in Section “Umbilical Cord Blood Gases.”
FIGURE 10.1. (A) The Ballard score. The Ballard scoring system uses points assigned to observations about neuromuscular maturity and physical maturity. (B) The points are summed, yielding a score used to arrive at an estimated age in weeks. (Guidelines for Perinatal Care. 6th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2007:216–217. Original source: Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard Score expanded to include extremely premature infants. J Pediatr. 1991;119(3):417–423.)
Likewise, the Apgar score cannot be used to identify the causes of the newborn illness. In general, a low 1-minute Apgar score identifies the newborn that requires particular attention. The 5-minute Apgar score can be used to evaluate the effectiveness of any resuscitative efforts that have been undertaken or to identify an infant who needs continuing evaluation and management. It should not be used to predict neurologic outcome in term infants.
Routine Care
Basic routine care is necessary for all newborn infants, regardless of the need for resuscitative efforts. For infants who do not require resuscitation at birth, routine care is performed immediately following delivery. It is important for the delivery team to remember to perform these tasks at a later time for newborns that require resuscitation.
Warming
First, the newborn infant is thoroughly dried to maintain appropriate body temperature. Warm blankets, skin-to-skin contact with the mother, or a radiant warmer can all accomplish this task. For healthy, vigorous, term neonates, skin-to-skin contact promotes maternal–infant bonding and initiation of breastfeeding in the first hour of life.
Premature infants have more difficulty maintaining their body temperature and are more susceptible to cold stress. These infants require warming pads, heated towels, and a preheated radiant warmer to stay warm.
Umbilical cord care
Second, after the umbilical cord is clamped and cut, it is left exposed to air to facilitate drying and separation. Local application of antimicrobial agents (e.g., triple-dye, iodophor ointment, and hexachlorophene powder) is common. The umbilical cord loses its bluish-white appearance within the first 24 hours after delivery. After a few days, the blackened, dried stump sloughs, leaving a granulating wound. If cord blood banking has been requested, the sample should be obtained and stored at the time of delivery.
Vital Signs
Another essential component of routine care is the assessment of vital signs. An infant’s temperature, heart and respiratory rate, core and peripheral color, level of alertness, tone, and activity should be monitored at delivery and every 30 minutes thereafter until these measures are stable for at least 2 hours.
If the mother plans to breastfeed, the newborn should be placed at the breast in the delivery room within the first hour after delivery. In general, healthy neonates should remain with their mothers (whether breastfeeding or not).
TRANSITIONAL CARE
Following the initial assessment and routine care of a healthy neonate, continued close observation is necessary for the subse-quent stabilization–transition period (the first 6–12 hours after birth) to identify any problems that may arise. The following findings should raise concern and result in closer observation: temperature instability; change in activity, including refusal of feeding; unusual skin coloration; abnormal cardiac or respiratory activity; abdominal distention; bilious vomiting; excessive lethargy or sleeping; delayed or abnormal stools; and delayed voiding.
Following delivery, all newborns should receive prophylactic application of antibiotic ointment (containing erythromycin [0.5%] or tetracycline [1%]) to both eyes to prevent the development of gonococcal ophthalmia neonatorum. This is recommended regardless of the mode of delivery. This prophylactic measure can be delayed up to 1 hour to allow for breastfeeding.
Every newborn should also receive a parenteral dose of natural vitamin K1 oxide (phytonadione, 0.5–1 mg) following delivery to prevent vitamin K–dependent hemorrhagic disease of the newborn. This form of administration is efficacious, and no commercial oral vitamin K preparation is approved for use in the United States at this time. This measure also can be delayed for up to 1 hour to allow breastfeeding in the first hour of life.
A newborn infant’s voiding pattern and bowel movements should be closely observed within the first 24 hours following birth. Concern about an obstruction or congenital defect of the urinary tract is appropriate if voiding has not occurred within the first day of life. Ninety percent of newborns pass stool within the first 24 hours. A congenital abnormality such as imperforate anus should be considered if this does not occur. For the first 2 or 3 days of life, the stool is greenish brown and tar-like in consistency. With the ingestion of milk, the stool becomes yellow in color and semisolid.
Jaundice
Jaundice, which occurs in most newborns, is usually benign, but because of the potential toxicity of bilirubin, all newborns should be assessed prior to hospital discharge to identify those at high risk for severe hyperbilirubinemia. Two methods of assessment can be used: 1) predischarge measurement of total serum bilirubin or transcutaneous bilirubin levels in infants who are jaundiced in the first 24 hours and 2) application of clinical risk factors for predicting severe hyperbilirubinemia. Late preterm (35–37 weeks of gestation) infants are at higher risk for hyperbilirubinemia than are term infants.
Acute bilirubin encephalopathy or kernicterus is associated with total serum bilirubin levels greater than 30 mg/dL. If possible, the cause of the hyperbilirubinemia should be determined. Breastfeeding has a significant effect on unconjugated hyperbilirubinemia (breast milk jaundice and “breast-non-feeding jaundice”). Jaundice that persists for 2 weeks requires further investigation, including measurement of both total and direct serum bilirubin concentrations. Elevation of the direct serum bilirubin concentration always requires further investigation and possible intervention, which includes phototherapy or exchange transfusion.
 INITIAL CARE OF THE ILL NEWBORN
INITIAL CARE OF THE ILL NEWBORN
Although most deliveries are uncomplicated, requiring only basic neonatal care, resuscitation may be necessary in up to 10% of all deliveries; 1% of these require major resuscitative efforts. The need for these efforts increases in circumstances such as premature birth, low-birthweight infants, prolonged labor, and nonreassuring measures of fetal well-being. Not all deliveries occur in a setting with intensive pediatric care immediately available. In the absence of such staff and facilities, maternal transport to a facility with a greater capacity to provide appropriate care should be attempted before delivery. Alternatively, the transport of a neonatal team from a tertiary care center to the primary care site is a possible option.
Neonatal Resuscitation
The normal newborn breathes within seconds of delivery and usually has established regular respirations within 1 minute of delivery. If the neonate is having difficulty breathing, ventilation, chest compression, and epinephrine should be instituted, as shown in the protocol in Figure 10.2. If an infant does not respond to epinephrine, hypovolemic shock should be considered, especially if there is evidence of blood loss. In this case, intravenous normal saline at 10 mL/kg should be given. A newborn who is apneic or gasping and has a heart rate of less than 100 bpm usually requires positive pressure ventilation, which may be done with a face mask after clearing the airway.

FIGURE 10.2. Algorithm for neonatal resuscitation. (Source: 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, © 2005, American Heart Association.)
The same principles of adult resuscitation (airway, breathing, and circulation) apply to neonatal resuscitation (Fig. 10.3). First, the newborn is transported to a radiant warming unit to be thoroughly dried. When drying the infant, it is important to remove wet towels to minimize the effect of evaporation that would otherwise lead to a rapid drop in core body temperature. The nose and oropharynx are suctioned to ensure an open airway as the infant is placed in the supine position. The head should be positioned with the neck slightly extended—the “sniffing position”—to allow for maximal air entry. Drying and suctioning, along with providing mild stimulation by rubbing the back or soles of the feet—or flicking the soles of the feet—help to stimulate the infant to breathe and cry.

FIGURE 10.3. Airway management in newborn resuscitation. (A) Management with mask and Ambu bag. Most newborns can be safely and effectively managed with a face mask, elevating the chin [1] so that the airway is pulled up and opened [2] into the “sniffing position.” (B) Management with endotracheal intubation. Intubation should only be performed by trained personnel to avoid iatrogenic injury.
Respiratory distress may occur as a consequence of situations such as preterm delivery, blockage of the newborn’s airway, or maternal narcotic administration during labor. A narcotic antagonist can be considered only if pressure ventilation has improved the heart rate and color, and the mother has received narcotics within 4 hours of delivery. Narcotic antagonists, such as naloxone, may be useful in immediate newborn care when the mother has received a narcotic near the time of birth but may cause life-threatening withdrawal in the infant born of a narcotic-addicted mother insofar as the infant is also addicted.
Umbilical Cord Blood Gases
During the resuscitation process, the metabolic well-being of an ill newborn is most accurately assessed using umbilical cord blood gases. Cord blood gases should be obtained in cases of cesarean delivery for fetal compromise, a low 5-minute Apgar score, severe growth restriction, abnormal fetal heart rate tracing, maternal thyroid disease, intrapartum fever, and multifetal gestations. A segment of the umbilical cord is double-clamped and cut and placed on the delivery table pending assessment of the 5-minute Apgar score, so that it may be taken for assessment of pH, po2, pco2, HCO3–, and base deficit. It should be remembered that, in the fetus, freshly oxygenated blood from the placenta travels to the fetus through the umbilical vein and blood metabolized by the fetus travels back to the placenta through two umbilical arteries. The most meaningful assessment of metabolic status of the infant at the time of delivery is through analysis of umbilical artery blood gases. Analysis of paired arterial and venous specimens should prevent debate over whether a true arterial specimen was obtained. Therefore, where possible, obtaining both venous and arterial samples (paired specimen) is recommended. Normal values for umbilical arterial and venous samples are given in Table 10.2.
Acidemia is generally accepted as an increase in hydrogen ion concentration in an umbilical arterial sample resulting in a pH of compromised. Ten percent of newborns with a base deficit of 12 to 16 mmol/L and 40% of newborns with a base deficit of >16 mmol/L will have moderate to severe complications, such as newborn encephalopathy and cardiovascular and respiratory complications. The terms acidemia, acidosis, and asphyxia should be used carefully when applied to the newborn condition, because each term defines a series of changes that may or may not represent true metabolic compromise.
Umbilical Cord Blood Banking
Umbilical cord blood is now known to contain potentially lifesaving hematopoietic stem cells for possible adult transplant for the correction of inborn errors of metabolism, hematopoietic malignancies, and genetic disorders of the blood and immune system. If a patient requests information on umbilical cord banking, balanced and accurate information regarding the advantages and disadvantages of public or private banking should be provided. The remoteness of the chance of an autologous unit of umbilical cord blood being used for a child or a family member (approximately 1 in 2,700 individuals) should also be disclosed.

MALE CIRCUMCISION
Circumcision is the surgical removal of a distal portion of the foreskin of the penis, exposing the underlying glans penis. It is usually performed within the first 2 days of life on healthy male term infants using a variety of instruments specific to the surgery (Fig. 10.4). Local anesthesia should always be used for circumcision, for example, by ring block or by dorsal penile block (Fig. 10.5). Complications from circumcision are rare and include local infection and bleeding.


FIGURE 10.4. Instruments used for circumcision include the Gomco clamp, Plastibell, and Mogen clamp. Local anesthesia is requisite from, for example, a dorsal penile block.
Male circumcision is an elective procedure usually performed for cultural or religious reasons. It is estimated that 1.2 million newborn males are circumcised annually in the United States. In some communities, the pediatrician performs the procedure, whereas in others, it is under the purview of the obstetrician. In a policy statement published in 2012, the American Academy of Pediatrics states that evidence shows that the health benefits of circumcision outweigh its risks. Although the health benefits of newborn male circumcision are not sufficient to recommend routine circumcision for all newborn males, they do justify making the procedure available to families who choose it. These benefits include a decrease in urinary tract infections, especially in newborns; a decrease in cancer of the penis; and lower risk of transmission of sexually transmitted infections, including human papillomavirus and human immunodeficiency virus. Because male circumcision is an entirely elective procedure, parents should be given accurate and impartial information about the procedure and its complications as well as the controversy over potential benefits. Parents should be allowed to ask questions and should be given full and complete answers prior to providing informed consent for the performance of the procedure. This discussion is an excellent example of how the power of emphatic communication enhances patient–physician communication and the quality of shared decision making.
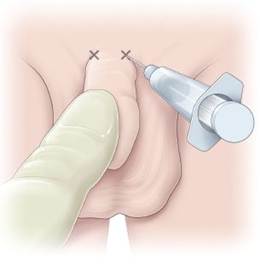
FIGURE 10.5. Dorsal block local anesthesia for circumcision.
NEWBORN SCREENING
Newborn screening programs, which should be available to all newborns, include tests designed to detect infants with specific conditions who may benefit from early diagnosis and treatment. These conditions include disorders of metabolism, endocrinopathies, hemoglobinopathies, hearing loss, and cystic fibrosis. The tests may also identify parents who are carriers of inherited conditions.
To obtain a sample for testing, heelstick-derived blood is collected and placed onto filter paper. If the initial sample is collected before 12 to 24 hours after delivery, a second sample should be collected at 1 to 2 weeks of age to decrease the probability that phenylketonuria and other disorders with metabolite accumulation are missed as a result of early testing. Premature infants, neonates receiving parenteral feeding, or those treated for illness should have a newborn screening test performed at or near 7 days of age, regardless of feeding status.
Each state has a system in place for notification, timely follow-up, and evaluation of any infant with a positive screening result. Positive results are usually reported to the newborn’s primary care provider and the parents.
Clinical Follow-Up
A soft plastic vacuum extractor was easily applied at the first attempt. Traction assistance was provided with each maternal contraction (occurring about every 2½ minutes), with delivery of the head on the third expulsive effort over a midline episiotomy, followed rapidly by completion of the delivery. At this time, a true knot was noted in the umbilical cord, and examination of the newborn revealed acrocyanosis, a heart rate of 80 bpm, limp muscle tone with absent reflex responsiveness, and a weak cry. The planned “handoff ” to the new mother was replaced by immediate full neonatal resuscitation. These findings were consistent with a 1-minute Apgar score of 4. There was a rapid positive response with Apgar scores of 8 and 9 at 5 and 10 minutes, respectively, the incident attributed to the tightening of an unknown true umbilical knot during the vacuum-assisted vaginal birth.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!