Chapter 8 Maternal medicine and infections
Adrenal disorders in pregnancy
Anaemia in pregnancy
Autoimmune disease
Bacterial vaginosis
Chicken pox/herpes zoster
Chlamydia
Coagulation disorders
Connective tissue disorder
Cytomegalovirus
Dermatology
Diabetes in pregnancy
Drugs in pregnancy
Epilepsy and other neurological conditions
Gonorrhoea
Perinatal group B streptococcus
Haemoglobinopathies
Heart disease
Hepatitis B
Herpes simplex infection
HIV infection
Human papillomavirus
Hypertension
Immunization
Inflammatory bowel disease
Jaundice
Listeriosis
Liver disease
Measles: rubeola
Parvovirus
Pituitary disorders in pregnancy
Psychiatric disorders in pregnancy
Renal disease
Respiratory disease
Rubella
Substance abuse in pregnancy
Syphilis
Thromboembolic disease
Thyroid and parathyroid disease
Toxoplasmosis in pregnancy
Vulvovaginal candidiasis Adrenal disorders in pregnancy Addison’s disease
Addison disease is adrenocortical insufficiency due to the destruction or dysfunction of the entire adrenal cortex.
It affects both glucocorticoid and mineralocorticoid function. The onset of disease usually occurs when 90% or more of both adrenal cortices are dysfunctional or destroyed. Prevalence is 40–60 cases per 1 million population and so is very rarely encountered in pregnancy. Most cases (90%) are due to autoimmune destruction or tuberculosis.Effect of Addison’s disease on pregnancy
If treated, no complications are encountered.
Effect of pregnancy on Addison’s disease
Pregnancy has no effect on the disease if properly treated. Steroid replacement may need to be altered at certain times during pregnancy.
Clinical approach
History
• Patients usually present with features of both glucocorticoid and mineralocorticoid deficiency and they may present with clinical features of chronic Addison’s disease or in acute addisonian crisis.
Chronic presentation
• Hyperpigmentation of the skin and mucous membranes often precedes all other symptoms by months to years.
• Weakness, fatigue, poor appetite, and weight loss.
• Nausea, vomiting, and occasional diarrhoea.
• Dizziness.
• Myalgias and flaccid muscle paralysis may occur due to hyperkalaemia.
• Other reported symptoms include muscle and joint pains; a heightened sense of smell, taste, and hearing; and salt craving.
Acute presentation
• Abdominal symptoms may take on features of an acute abdomen, nausea, and vomiting. Other symptoms may include hyperpyrexia and vascular collapse.
Examination
• Increased pigmentation of the skin and mucous membranes, with or without areas of vitiligo.
• Evidence of dehydration, hypotension, and orthostasis.
• Female patients may show an absence of axillary and pubic hair and decreased body hair.
Investigations
Short synacthen test and long corticotrophin releasing hormone test.
Management
The vast majority of cases are diagnosed before conception and are well established on replacement therapy. This is usually in the form of hydrocortisone (a total of 30 mg daily in divided doses) and fludrocortisone (up to 100 mg daily).
The patients feeling of wellbeing and the lack of postural hypotension, hyponatraemia, or hyperkalaemia gauge the adequacy of replacements.
The maintenance doses are not changed by pregnancy per se. However, an increase in dosage is vital during periods of stress such as hyperemesis gravidarum, surgical procedures and infections, or during labour.
Hydrocortisone is administered intravenously in doses of 100 mg every 6 hour throughout the period of stress and reduced gradually over a period of days. Congenital adrenal hyperplasia
Congenital adrenal hyperplasia (CAH) is a family of inherited disorders of adrenal steroidogenesis, resulting from a deficiency of one of several enzymes necessary for normal adrenal steroid synthesis. It occurs in 1 in 5000 and 1 in 15 000 births in most populations.
21 hydroxylase deficiency (21-OHD) is the commonest deficiency, with a particularly high frequency and carrier rates of between 1.2% and 6% of the population. The gene frequency is 1 in 200–400 and is autosomal recessive.
The risk of a subsequent child having the disorder is 1:4, if a couple have one affected child.
21-OHD deficiency leads to impaired production of glucocorticoids and mineralocorticoids. The sex steroid pathway is intact and thus provides the only option for the accumulating metabolites. The consequence is a markedly enhanced adrenal androgen production.
Affected female fetuses are at risk of masculinization. Male neonates are at risk of salt-losing crises due to miner-alocorticoid deficiency as well as precocious puberty.
Effect of CAH on pregnancy
There is an increased risk of miscarriage, Caesarean section, pre-eclampsia, and intrauterine growth restriction.
Effect of pregnancy on CAH
No effect in treated patients.
Clinical approach
Key points
Aim of treatment is to ensure adequate glucocorticoid and mineralocorticoid replacement for the mother and preventing virilization of an affected female fetus.
• In women with CAH, increased antenatal surveillance should be put in place because of the increased risk of pre-eclampsia.
• Corticosteroid replacement is the mainstay of treatment. Mineralocorticoids are necessary in salt losing classical CAH.
• Monitoring with 17-hydroxyprogesterone levels is unreliable in pregnancy.
• In pregnancies with a fetus at risk of CAH, suppressing adrenocorticotrophic hormone (ACTH), the drive for the intact sex steroid production pathway, by giving dexamethasone in a dose of 250–500 μg daily is commonly used and continued throughout pregnancy.
• Fetal diagnosis should be made with sex determination, human leucocyte antigen (HLA) status and 21-hydroxylase zygosity.
• Treatment should be started preconception or before 5 weeks’ gestation, prior to differentiation of the genitalia.
• All female neonates should receive corticosteroids to treat the CAH and because their adrenal glands will be suppressed following long-term high-dose maternal dexamethasone therapy.
• Male fetuses do not need to be treated in utero.
• Prevention of virilization is not always successful, therefore parents should be counselled regarding benefits and risks, and termination of the pregnancy should be offered if the fetus is female. Phaeochromocytoma
These are chromaffin tumours that secrete catecholamines. It is known as the 10% tumour as approximately 10% of the disease is bilateral, malignant, located in chromaffin tissue outside of the adrenal gland, arises in childhood, familial, and recurs after being resected. They are mostly located in the adrenal medulla.
Mutations of the genes VHL, RET, NF1, SDHB, and SDHD are all known to cause familial phaeochromocytoma/extra-adrenal paraganglioma. Phaeochromocytomas may occur in certain familial syndromes, including multiple endocrine neoplasia (MEN) 2A and 2B, neurofibromatosis, and von Hippel–Lindau (VHL) disease.
Effect of phaeochromocytoma on pregnancy
These tumours are rare but dangerous if they occur in pregnancy. Fetal mortality is about 25% in undiagnosed cases and 15% in diagnosed cases. Maternal mortality most recently had decreased to about 5% in undiagnosed cases, with no maternal death when the diagnosis is made antepartum. The main causes of maternal mortality are cardiac arrythmias, cerebrovascular accidents, or pulmonary oedema.
Effect of pregnancy on phaeochromocytoma
Moribund hypertensive crisis may be precipitated by labour, delivery, general anaesthesia, or opiates. The gravid uterus may cause hypertensive attacks due to pressure on the tumour in the supine position.
Clinical approach
History
• The classic symptoms are headaches, palpitation, and excessive sweating.
• Other symptoms include tremor, nausea and vomiting, anxiety, weakness, epigastric pain, flank pain, and weight loss.
Examination
• Signs include hypertension, weight loss, pallor, fever, tremor, and tachyarrhythmias.
Investigations
• Biochemistry may reveal impaired glucose tolerance and hypercalcaemia.
• Diagnosis is from measuring plasma metanephrine and/or 24-hour urinary creatinine, total catecholamines, vanillylmandelic acid, and metanephrines
• MRI is the preferred imaging modality in pregnancy.
Management
Management of hypertension and symptoms with an alpha-blocking agent such as phenoxybenzamine is mandatory. The dose is 10–30 mg, two to four times daily. Beta-blocking agents to control tachycardia can be added if required.
Surgical removal is the only cure after control of the blood pressure is achieved by medication.
If the patient is prior to 23 weeks’ gestation, then surgical resection is recommended. After 24 weeks, it is recommended that the surgery is postponed until fetal maturity is achieved and then performed either concurrently with Caesarean section or postpartum.
Adequate alpha-blockade for at least 3 days prior to surgery and expert anaesthetic care are essential. Conn’s syndrome
It is a rare disease of primary hyperaldosteroneism, caused by adrenal aldesteronomas in about 75% of cases and idiopathic bilateral adrenal hyperplasia in the remainder.
Clinical approach
History
Hypertension and hypokalaemia are sometimes the only indicators.
Examination
Symptoms and signs of hypokalaemia. Alkalosis may also be present.
Investigations
Diagnosis is by low serum potassium, suppressed renin activity and high plasma aldosterone.
Management
Treating hypertension is vital and is in the usual way. Potassium supplementation is also important. Spirinolactone, commonly used outside pregnancy, should be avoided in pregnancies with a male fetus because of its anti-androgen effects. Tumour resection is curative and laparoscopic adrenalectomy may prove to be useful during pregnancy. Cushing’s syndrome
Long-term exposure to glucocorticoids may lead to Cushing’s syndrome.
The most common cause is iatrogenic, from corticosteroid therapy.Increased adrenal cortisol production causes endogenous Cushing’s syndrome. Most cases are due to corticotrophin-producing pituitary adenomas leading to bilateral adrenal hyperplasia (Cushing’s disease). The condition is very rare in pregnancy as most women with the disorder will have subfertility.
Effect of Cushing’s syndrome on pregnancy
Maternal complications include hypertension in about 75% and gestational diabetes in about 50% of patients. Heart failure and severe pre-eclampsia are common. Buescher et al. (1992) reported a 5% maternal mortality rate among 65 pregnancies. Wound infection due to poor tissue healing is common. Perinatal morbidity, with 60% preterm delivery, and mortality (25%) are also high.
Clinical approach
History and examination
The classical clinical features can be attributed to pregnancy and include weight gain, striae, hypertension, diabetes, hirsutism, headache, and easy bruising.
Investigations
Low ACTH and high cortisol are suggestive of an adrenal cause. However, pregnancy-specific ranges for plasma and urinary cortisol must be used and the cortisol should be measured after a high-dose dexamethasone suppression test. Localization is possible with adrenal ultrasound, CT, or MRI, or pituitary CT or MRI.
Management
Long-term medical treatment is usually ineffective; however, ketoconazole blocking steroid production has been successful. Few cases during pregnancy have been successfully treated with oral ketoconazole, but there are concerns in a pregnancy with a male fetus due to blockage of testicular steroidogenesis. Surgery is the treatment of choice and it has been undertaken successfully during pregnancy. Further reading
Nelson-Piercy C. A Handbook of obstetric medicine, 3rd edn. London: Informa Healthcare 2006.
Buescher MA, McClamrock HD, Adashi EY. Cushing syndrome in pregnancy. Obstet Gynecol 1992;79:130–7.
Burrow GN, Ferris TF. Medical complications during pregnancy, 4th edn. London: W.B. Saunders 1995.
Grossman A. Clinical endocrinology, 2nd edn. Oxford: Blackwell Scientific Publications 1997.
Shehata HA, Ahmed K. Other endocrine disorders in pregnancy. Curr Obstet Gynaecol 2004;14:387–94. Internet resources
www.emedicine.com/
www.mayoclinic.com/
Anaemia in pregnancy Definition
Anaemia is defined as a reduction in the absolute number of circulating red blood cells (RBCs), which is indirectly measured by a reduction in haemoglobin concentration, haematocrit, or RBC count. In practice, anaemia in pregnant women is said to exist when the haemoglobin level in venous blood is below 11 g/dL (WHO 1968). Prevalence
Published rates of prevalence for developing countries range from 35% to 60% for Africa, Asia, and Latin America. This is in sharp contrast to industrialized countries where anaemia in pregnancy occurs in less than 20% of women. Causes
• Acquired
• nutritional : iron deficiency; folate deficiency; vitamin B12 deficiency
• acute blood loss
• aplastic anaemia
• drug-induced haemolytic anaemia
• infections: malaria, HIV
• chronic disease: renal
• neoplasia: leukaemia, lymphoma.
• Hereditary
• haemoglobinopathies: thalassaemias—β,α (heterozygotes); sickle cell disease
• congenital haemolytic anaemia.
In all of these conditions, anaemia results from one or more of three independent mechanisms: decreased RBC production, increased RBC destruction, and blood loss. Iron deficiency is the commonest cause of anaemia in the pregnant woman and is usually a result of nutritional deficiency or chronic blood loss. In both situations, the availability of iron is the rate limiting factor for RBC production by the bone marrow. Iron deficiency is relatively common in pregnancy because of the increased iron demand (500–1000 mg) and because many women start pregnancy with poor or depleted iron stores.
Effects of anaemia on mother
Suspect anaemia if mother complains of easy fatigue, pica, and appears pale. Decreased aerobic work performance in iron deficiency anaemia could result from a lack of iron-containing cellular enzymes. Anaemia is usually diagnosed on FBC, which is a part of routine antenatal screening blood tests.
Effects of anaemia on pregnancy and fetus
Fetuses of iron-deficient mothers are not anaemic at birth because of placental active transport of iron to the fetus. However, severe anaemia in the mother (Hb and i.v. route. Two newer i.v. preparations, iron sucrose and ferric gluconate, are associated with lesser side-effects.
Iron can be given intravenously at one shot as total dose infusion (TDI). Utmost caution is needed for total dose iron therapy via intravenous route because of severe anaphylactic reaction that may occur. Blood transfusion is not indicated unless the patient has decompensated due to a drop in haemoglobin concentration and needs a more rapid rise in haemoglobin. Packed red cell transfusion may be indicated for pregnant women with severe anaemia (Hb 6 g/100 mL or less) close to due date or < 8 g/d if they have an increased likelihood of blood loss at delivery.
Prophylaxis
Pregnant women need iron to cover their basic losses (0.6 mg/day for 300 days = 180 mg), the demands of the fetus (250–300 mg) and of the placenta (75 mg). In addition, 300–400 mg of iron is required for an increase in the RBC mass. Consequently, the total iron demand of pregnancy amounts to 900 mg or approximately 3 mg/day (30–40 mg of dietary iron). This requirement cannot be met by the food consumed by most pregnant women, especially from the developing world, and oral supplementation of medicinal iron is justifiable. The data from randomized trials suggest that daily antenatal iron supplementation increases haemoglobin levels in maternal blood both antenatally and postnatally (Pena-Rosas and Viteri 2006). Infant outcomes of routine supplementation have not been studied adequately. Megaloblastic anaemias
Megaloblastic anaemias are caused by impaired DNA synthesis in the marrow secondary to either folic acid or vitamin B12 deficiency. In pregnancy it is almost always secondary to folate deficiency. Folic acid deficiency during pregnancy is usually secondary to dietary deficiency, occurring commonly in women who do not eat enough green vegetables or animal proteins. It is also commoner in multiple pregnancies, women with intestinal malapsorption and women on anticonvulsants.
Folic acid deficiency has been associated with increased risk of fetal neural tube defects, and routine supplementation periconceptually has been shown to reduce its occurrence. Although folic acid deficiency has been implicated in the occurrence of other pregnancy complications, such as placental abruption and pre-eclampsia, this has never been confirmed.
Clinical features
• Glossitis—painful red tongue with papillary flattening
• Apthous oral ulcers
• Retinal and subcutaneous haemorrhages.
Laboratory features
• Macrocytosis, megaloblasts, neutrophil hypersegmentation, anisocytosis, and Howell–Jolly bodies on peripheral smear.
• There may be associated neutropenia and thrombocytopenia:
• serum folate levels are unreliable. Red cell folate estimate is a more accurate measure of deficiency.
Management
• A marked haematological response is seen within 7 days of starting as little as folic acid 1 mg per day orally. Treatment with folic acid should be continued throughout pregnancy. Further reading
Pena-Rosas JP, Viteri FE, Effects of routine oral iron supplementation with or without folic acid for women during pregnancy. Cochrane Database Syst Rev 2006;3:CD004736.
WHO. Nutritional anaemias. Report of a WHO scientific group. World Health Organization Technical Report Series. 1968;405:5–37.
Frewin R, Henson A, Provan D. ABC of clinical haematology. Iron deficiency anaemia. BMJ 1997;314:360–3.
Autoimmune disease Multiple sclerosis
Multiple sclerosis (MS) is an inflammatory demyelinating disease of the central nervous system. It affects women more commonly than men and this often coincides with bringing up a family. It is the commonest cause of neurological disability in young adults in the UK. Pregnancy has no long-term effects on MS progression.
Aetiology
There are many causes, including viruses, autoimmune disorders, environmental and genetic factors.
Prognosis
Effect of pregnancy on multiple sclerosis
The majority of studies reported that there is a reduced frequency of relapse during pregnancy, especially during the third trimester, followed by an increase in relapse rates in the puerperium, especially in the first 3 months. There is some evidence to suggest that pregnancy may slow the rate of progression, more so in parous women than nulliparous women.
Effect of multiple sclerosis on pregnancy
There is no evidence that MS has an adverse effect on the outcome of pregnancy and delivery. Although MS is not an inherited disease, there is a slightly higher chance of the offspring developing the disease than the general population: estimated at 1–4% if one of the parents has the disease.
Clinical approach
Diagnosis
The diagnosis is one of exclusion as there is no single test that can confirm MS. Symptoms of MS vary from mild to severe and may appear in various combinations, ranging from difficulty in concentrating, poor attention, memory, and judgement. MRI can show areas of scarring and inflammation in the myelin (there are no data about safety of MRI in pregnancy). Lumbar puncture and visual evoked potentials can be helpful.
Management
There is little conclusive evidence to support a role for spinal or epidural anaesthesia precipitating exacerbations of MS postpartum. Further evidence is needed to allow a fully informed discussion about pain relief during labour for patients with multiple sclerosis. A retrospective study found the relapse rate in puerperium to be independent of breastfeeding status. Steroids are not contraindicated in pregnancy but should be used with caution after discussing the risks and benefits. Intravenous immunoglobulins have been suggested to reduce the incidence of postpartum relapse. Several new medications such as β-interferon and glatiramer acetate have demonstrated a reduction in the number and severity of MS exacerbations, but none is licensed for use in pregnancy. There are reported cases of normal pregnancies and healthy infants in women who were placed on these medications. Little is known, however, about how the use of these medications affect pregnancy and childbearing and further research is required. Planning adequate postnatal support for a family should take into account the increased risk of relapse postpartum. Myasthenia gravis
Myasthenia gravis (MG) is a neuromuscular disease leading to fluctuating muscle weakness and fatigability. It is an autoimmune disease in women, that occurs in the second and third decades of life, caused by circulating antibodies that block the acetylcholine receptors at the postsynaptic neuromuscular junction, inhibiting the stimulative effect of acetylcholine. These antibodies are IgG and may cross the placenta causing transient neonatal MG.
Aetiology
MG is often associated with other autoimmune mediated diseases. In large series in patients with MG, 7% had diabetes mellitus, 6% had thyroid disease, 3% had non-thymic neoplasm, and more than 2% had rheumatoid arthritis. Transient MG has been observed in HIV infection and after bone marrow transplantation.
Prognosis
Effect of pregnancy on myasthenia gravis
In the long term, pregnancy does not affect MG. The course of this disease is variable and unpredictable during pregnancy and can change during subsequent pregnancies. The first trimester and the first month postpartum seem to be the most critical periods for exacerbation of the disease. Complete remission can occur in some mothers.
Effect of myasthenia gravis on pregnancy
The reported incidence of preterm delivery or low birth weight is variable. The perinatal death rate is unaffected but the death rate because of fetal anomalies is increased. About 10% of infants born to MG mothers show signs of neonatal MG, which responds well to the acetylcholine inhibitors. Very rarely, an infant can be born with arthrogryposis multiplex congenita, secondary to profound intrauterine weakness, due to maternal antibodies that target an infant’s acetylcholine receptors.
Clinical approach
Diagnosis
MG can be a difficult diagnosis. Physical examination can reveal easy fatiguability, ptosis, and diplopia. If diagnosis is suspected, serology can be performed to identify acetylcholine receptor antibodies and has a sensitivity of 80–96%. Other tests are electromyography, imaging, edrophonium test, pulmonary function tests, and immunofluorescence.
Management
Acetylcholinesterase inhibitors, such as pyridostigmine and immunosuppressive therapy (corticosteroids, azathioprine, or cyclosporine A) should be continued throughout pregnancy as this reduces the chances of neonatal muscle weakness as well as controlling the mother’s MG. Higher doses may be required as pregnancy advances. Serial plasmapheresis and immunosuppressive therapy have successfully been used to treat MG crisis in pregnancy. Regional anaesthesia is safe with the right choice of drugs. A Caesarean section is recommended for obstetric reasons. Large doses of acetylcholinesterase drugs may be a contraindication to breastfeeding because they can cause gastrointestinal upsets in the breastfed newborn. Corticosteroids can be safely used during lactation. Autoimmune liver disorders
There are three different autoimmune liver disorders:
• autoimmune chronic active hepatitis (CAH)
• primary biliary cirrhosis (PBC)
• primary sclerosing cholangitis (PSC). Autoimmune chronic active hepatitis
Autoimmune hepatitis is a chronic necroinflammatory hepatitis of unknown aetiology, caused by autoantibodies against liver-specific and non-liver-specific antigens and increased immunoglobulins IgG levels. Females make up 75% of patients with this form of chronic active hepatitis, particularly in the second and third decades of their life. It can occur by itself, but can coexist with other autoimmune diseases, such as systemic lupus erythematosus or antiphospholipid syndrome.
Clinical approach
Diagnosis
The onset is insidious with fatigue, anorexia, jaundice, but can also resemble viral hepatitis. Liver enzymes are not specifically indicative of CAH; however, elevated aminotransferases and hypergammaglobulinaemia represent another characteristic. Prothrombin time is prolonged. The presence of antinuclear, anti-smooth muscle, and anti-liver microsomal antibodies are disease specific for CAH. Liver biopsy confirms the diagnosis.
Management
Pregnancy may be uncomplicated in patients with mild treated autoimmune CAH, but there is some evidence that this group of patients has an increased risk of pre-eclampsia, prematurity, and fetal wastage. Immunosuppressive therapy with steroids or in combination with azathioprine results in remission of the disease and therapy should be continued throughout gestation to prevent relapse. Liver transplantation should be considered for end-stage cirrhosis. Primary biliary cirrhosis
PBC is a chronic and slowly progressive cholestatic liver disease of auoimmune aetiology characterized by injury of the intrahepatic bile ducts that may eventually lead to liver failure. This disease affects predominantly women, usually in the middle age
Aetiology
PBC is associated with other autoimmune diseases such as Sjogren’s syndrome, scleroderma, and Raynaud’s phenomenon and is regarded as an organ-specific disease. Genetic susceptibility as a predisposing factor has been suggested. Environmental factors (e.g. infection, chemicals, and smoking) may have a causative role.
Clinical approach
Diagnosis
The majority of patients are asymptomatic, however some may present with symptoms of fatigue and pruritis. PBC may be diagnosed outside pregnancy on routine liver testing with elevated levels of alkaline phosphatase (liver isoenzyme) and γ-glutamyl transpeptidase. Diagnosis is usually confirmed by detection of antimitochondrial antibodies (AMAs). Liver biopsy may be required for those AMA-negative patients who are severely symptomatic.
Management
Maternal and fetal outcomes are variable, but the prognosis is good for well-compensated disease. Drug therapy is non-specific and aimed at relieving symptoms such as pruritis. Currently, the first line of therapy is ursodeoxycholic acid (UDCA) and an anticholestatic. Liver transplantation is an option for those with liver failure. Primary sclerosing cholangitis
PSC is a rare, chronic, fibrosing, inflammatory disorder of unknown aetiology affecting the biliary tree. PSC often accompanies other autoimmune disorders. It is mostly observed in male patients with irritable bowel disease.
Clinical approach
Diagnosis
Patients may present with jaundice, fever, pruritis, and right upper quadrant pain. There is a hypothesis suggestive of hormonal influence which is supported by reports of patients developing the disease during or shortly after pregnancy. Patients have elevated alkaline phosphatase and γ-glutamyl transpeptidase levels and underlying bile duct abnormalities seen on ultrasound, cholangiography, magnetic resonance cholangiography, or liver biopsy.
Management
Treatment is directed at controlling symptoms with ursodeoxycholic acid to reduce itching and malabsorption and immunosupressants to reduce inflammation. In advanced cases, liver transplantation has been used successfully. In one reported series of pregnancies in women with PSC, pregnancy outcome was good. The only serious complication was severe pruritis (2 out of 13) leading to discontinuation of pregnancies. Most patients had marked disappearance or reduction of symptoms after delivery. Consequently, the cause of pruritis could have been obstetric cholestasis. Further reading
Beth A, Mueller JZ, Critchlow C. Birth outcomes and need for hospitalisation after delivery among women with multiple sclerosis. Am J Obstet Gynecol 2002;186:446–52
Giesser B. Pregnancy and multiple sclerosis: the current view. Mult Scler Q Rep 2001;20:68.
Janczewska I, Olsson R, Hultcrantz R, et al. Pregnancy in patients with primary sclerosing cholangitis. Liver 1996;16:326–30.
Plauche WC. Myasthenia gravis. Clin Obstet Gynecol 1983;26:592–604.
Shehata HA, Okuson H. Neurological disorders in pregnancy. Current Opin Obstet Gynecol 2004;16:119.
Bacterial vaginosis Definition
Bacterial vaginosis is an ecological condition of the vaginal flora characterized by variable degrees of depletion of the resident and protective, hydrogen peroxide-producing lactobacillus species and an overgrowth of vaginal anaerobes. An intermediary and less stable subtype, possibly reflecting a transitional phase between normal flora and bacterial vaginosis, is also recognized and is equally associated with adverse perinatal and gynaecological outcomes. Intermediate flora may include a range of pathological floral shifts that are unrelated to bacterial vaginosis, including aerobic vaginitis. Bacterial vaginosis has been recognized for over a hundred years albeit documented under a host of different names, including non-specific vaginitis, Haemophilus vaginitis, Gardnerella vaginitis, Corynebacterium vaginitis and Anaerobic vaginosis. Epidemiology
The prevalence of bacterial vaginosis is population dependent. In both the USA and the UK, African American and women from African and Afro-Caribbean ethnic backgrounds have the highest prevalence of bacterial vaginosis ranging between 20% and 35% compared with their Caucasian counterparts with a prevalence rate of 10–15% (Goldenberg et al. 1996). The prevalence rates are also higher among women attending genitourinary medicine clinics, smokers, lesbians, and users of intrauterine devices. Aetiology
The exact stimulus that initiates the transformation of the vaginal flora is unknown. The condition is polymicrobial and participating organisms include anaerobes, Gardnerella vaginalis and more recently Atopobium vaginale. Three main risk factors have emerged as possible causes of the shift from a lactobacilli-dominated flora to bacterial vaginosis, namely sexual activity, douching, and the absence of hydrogen peroxide-producing lactobacilli in the vagina. Women from African and Afro-Caribbean ethnic backgrounds practise vaginal douching more commonly than their white counterparts (Stock et al 1973; Aral et al. 1992), in the erroneous belief that douching is a health-promoting practice. Some of the antiseptic solutions used for douching may weaken the protective lactobacillus species or reduce their numbers, thereby encouraging colonization by other organisms. Douching has been independently associated with a significantly increased risk of acquisition of bacterial vaginosis. After adjusting for vaginal douching, Black race was no longer significantly associated with bacterial vaginosis (Rajamanoharan et al. 1999), suggesting that differing rates of bacterial vaginosis between racial groups may be due to cultural differences rather than genetic and socioeconomic variations. Clinical features
Bacterial vaginosis does not elicit a cellular inflammatory response in the vagina, and up to 60% of affected women are asymptomatic. Of the minority of women with symptoms, a thin fishy smelling vaginal discharge is common, which may be accentuated by menstrual discharge or semen from unprotected sexual intercourse. Diagnosis
Bacterial vaginosis can be diagnosed by
• amsel composite criteria: this consists of the presence of any three of the following four features: characteristic vaginal discharge, positive Whiff (10% KOH) test, pH >4.7, or the presence of clue cells
• wet mount and direct microscopy
• gram stain
• affirm VP III: this is a commercially available DNA hybridization assay for the detection of G. vaginalis. Since G. vaginalis is part of the normal flora of the vagina, it is designed to be positive only for pathological concentrations of G. vaginalis (>2 ? 105 bacterial cells).
Complications
• Early and late miscarriage
• Preterm labour and preterm delivery
• Preterm prelabour rupture of membranes
• Chorioamnionitis
• Postpartum endometritis
• Wound infections
• Low birthweight
• Acquisition of HIV
• Cervical dysplasias. Management
Pregnant and non-pregnant women who have symptoms attributable to bacterial vaginosis should be treated. At present, there is insufficient evidence to recommend routine screening and treatment of all pregnant women (McDonald et al 2005). However, there is strong evidence that women with a prior history of preterm delivery or late pregnancy loss benefit significantly from screening and treatment. Treatment when indicated should be initiated early in the second trimester preferably before 20 weeks’ gestation. Treatment programmes initiated after 20 weeks have not been shown to reduce adverse pregnancy outcomes. Early oral or topical clindamycin therapy eradicate bacterial vaginosis effectively, and are both associated with a reduction in the risks of late miscarriage and preterm birth (Ugwumadu et al 2003). Some authors advocate oral therapy for bacterial vaginosis in pregnancy as this is believed to eradicate sub-clinical endometritis, which may be important (Ugwumadu et al 2003).
Oral or topical metronidazole is also effective in the treatment of bacterial vaginosis. However, metronidazole has a narrower spectrum of activity than clindamycin acting chiefly against anaerobes, and with no activity against many aerobes and other key organisms such as mobiluncus, Ureaplasma urealyticum and Mycoplasma hominis, which are associated with bacterial vaginosis. Metronidazole has a neutral effect on the protective lactobacillus species in contrast to clindamycin, which has activity against lactobacilli. A combination of oral and intravaginal clindamycin has been suggested to ensure eradication of organisms resident in the upper genital tract through the oral component and achieve sufficient intravaginal antibiotic levels to eradicate the large burden of bacterial innoculum in the vagina, which may not be achieved easily by oral therapy. In the literature, there are no reports of embryotoxic effects attributable to clindamycin use in human pregnancy. It is well tolerated and widely used during pregnancy in the USA. Its side-effects profile compares favourably with that of other broad-spectrum antibiotics including the risk of antibiotic associated colitis. Further reading
Aral SO, Mosher WD, Cates W, Jr. Vaginal douching among women of reproductive age in the United States: 1988. Am J Public Health 1992;82;210–14.
Goldenberg RL, Klebanoff MA, Nugent R, et al. Bacterial colonisation of the vagina during pregnancy in four ethnic groups. Vaginal Infections and Prematurity Study Group. Am J Obstet Gynecol 1996;174:1618–2161.
McDonald H, Brocklehurst P, Parsons J. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst Rev 2005;CD000262.
Rajamanoharan S, Low N, Jones SB, Pozniak AL. Bacterial vaginosis, ethnicity, and the use of genital cleaning agents: a case control study. Sex Transm Dis 1999;26:404–9.
Stock RJ, Stock ME, Hutto JM. Vaginal douching. Current concepts and practices. Obstet Gynecol 1973;42;141–6.
Ugwumadu A, Manyonda I, Reid F, Hay P. Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: a randomised controlled trial. Lancet 2003;361:983–8.
Chicken pox/herpes zoster
Chicken pox/herpes zoster is caused from infection with the varicella zoster virus. Varicella infection is usually seen as a childhood illness, but can occur in pregnant women and the effects vary based on the gestational age at infection. Herpes zoster is reactivation can be reactivated from latent varicella infection in a dermatomal distribution. Epidemiology
Ninety per cent of adults in the USA demonstrate immunity to varicella zoster virus. Adult infection with varicella accounts for only about 2% of the total cases, but 25% of all varicella-related deaths. In pregnant women with varicella pneumonia, even with treatment the mortality rate is approximately 14%, with the highest rates among women infected in the third trimester of pregnancy. Aetiology
Varicella zoster virus is a highly infectious agent that is transmitted from person to person by direct contact with respiratory droplets or aerosolization of vesicular fluid from skin lesions. Clinical approach
Patient presentation
• The virus enters its host via the respiratory tract and has an incubation period of 14–16 days.
• The newly infected person is contagious for 1–2 days before the onset of a rash.
• Once the rash is present, it will take 4–5 days for the skin lesion to crust over
• Once the skin lesions have crusted over a person is generally considered not contagious.
Diagnosis
• Varicella infection is a clinical diagnosis and rarely requires laboratory confirmation. Patients may present with generalized symptoms of headache, fever, and malaise prior to the development of a rash.
• The classic rash will appear a few days after the generalized symptoms and begins as small pruritic macules that progress to papules and vesicles.
• Varicella pneumonia occurs in up to 20% of cases of varicella infections in pregnancy. The symptoms begin about 4 days after the initial presentation and can include cough, shortness of breath, chest pain, and haemoptysis. Characteristic radiographic findings include bilateral peribronchial nodular infiltrates.
Management
• All pregnant women diagnosed with varicella zoster infection during pregnancy should receive oral acyclovir 800 mg five times per day or valcyclovir 1 g three times a day.
• Clinicians should educate their patients about the severity of this diagnosis and encourage them to present immediately to the hospital if any respiratory symptoms develop.
• Patients diagnosed with varicella pneumonia should be hospitalized for intravenous acyclovir (10–15 mg/kg every 8 hours) and to closely monitor their respiratory status. Varicella pneumonia is considered self-limited and usually resolves within 7 days, but it can be severe enough to require mechanical ventilation.
• Intravenous acyclovir should also be used for patients with neurological symptoms, hemorrhagic rash, continued fever, or appearance of new lesions after 6 days of treatment with oral antiviral therapy.
Because pregnant women are at a higher risk for severe varicella, use of varicella zoster immune globulin (VZIG) has been previously recommended for women without evidence of immunity. According to the CDC, the only US licensed manufacturer of VZIG discontinued production in 2004. There is an investigational VZIG product known as VariZIG that is available under an investigational new drug application. This product can be requested from the sole authorized US distributor, FFF Enterprises (24-hour telephone, 800-843-7477), for patients who have been exposed to varicella who are felt to be at increased risk for severe disease. Prior to administration, patients must be counselled that this is an investigational product and should give written informed consent. Investigational VariZIG is expected to provide maximum benefit when administered as soon as possible after exposure, although it can be effective if administered as late as 96 hours after exposure. If it is not possible to administer VariZIG within 96 hours of exposure, Administration of immune globulin intravenous (IGIV) should be considered. The recommended IGIV dose for post exposure prophylaxis of varicella is 400 mg/kg administered once.
Congenital varicella syndrome
This syndrome is represented by:
• dermotomal scarring (70%)
• limb hypoplasia (68%)
• ocular abnormalities (cataracts, chorioretinitis, micropthalmos, Horner’s syndrome, nystagmus; 66%)
• low birthweight (50%)
• cortical atrophy and mental retardation (46%)
• early death (28%)
• survivors can also have long-term learning defects and other developmental problems.
First trimester exposure
First trimester exposure to primary varicella zoster virus may result in stillbirth or a baby born with the stigmata of the congenital varicella syndrome at a rate of 0.55%. Maternal infection following the critical first trimester of organogenesis may be associated with reactivation zoster in utero, with a characteristic pattern of cicitrical skin scarring associated with the distribution of dermatomes.
Second trimester exposure
The incidence of congenital varicella syndrome is up to 2% when maternal infection occurs between 13 and 20 weeks’ gestation.
Third trimester exposure
Asymptomatic infants born to women who are infected with varicella zoster virus between 25 and 36 weeks’ gestation have an increased risk of zoster in the first year of life.
Peripartum exposure
Infection with primary varicella zoster virus in the peripartum period can result in neonatal varicella, which carries a significant mortality rate despite appropriate antiviral therapy. If the varicella infection is from 5 days before delivery to 2 days after delivery, an estimated 17–30% of the newborns contract severe varicella infection because of the lack of maternal antibody to protect the neonate and the relative immaturity of the neonatal immune system. If untreated, the risk of death among neonates is 31%. With varicella immunoglobulin treatment the rate of neonatal death is 7%.
Fetal outcome
• The risk to the fetus is directly dependent on when the mother was infected. Consultation with a perinatalogist should be obtained to follow the fetus by ultrasound to look for anatomic abnormalities associated with congenital varicella syndrome.
• Herpes zoster in an otherwise healthy pregnancy is not associated with intrauterine infection, even when the dermatomes innervating the uterus are involved.
Varicella screening
• Since the disease is preventable with vaccination, one should know the prior exposure status of their patient.
• If the status is negative or not known, consider sero-logical testing to confirm prior exposure before conception.
• If the testing confirms that the patient is susceptible to varicella, she should be immunized with the vaccine on two occasions 4–8 weeks apart.
• The vaccine is a live-attenuated viral vaccine and carries a theoretical risk of causing congenital infection. Therefore, pregnancy should be deferred for at least 1 month after vaccination. Further reading
Daley A, Thorpe S, Garland S. Varicella and the pregnant woman: Prevention and management. Austral NZ J Obstet Gynaecol 2008;48:26–33.
Gardella C, Brown Z. Managing varicella zoster infection in pregnancy. Cleveland Clin J Med 2007;74:290–6.
CDC. Varicella vaccine: questions and answers about pregnancy. 2007; www.cdc.gov/vaccines/vpd-vac/varicella/vac-faqs-clinic-preg.htm
CDC. Varicella treatment questions and answers. 2007; www.cdc.gov/vaccines/vpd-vac/varicella/dis-faqs-gentreatment.htm
CDC. A new product (VariZIG) for post exposure prophylaxis of varicella available under an investigational new drug application expanded access protocol (ACIP). MMWR 2006; 55.
Perinatal Viral and Parasitic Infections. ACOG Practice Bulletin Number 20. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 2002;76:95–107.
Chlamydia Aetiology
Chlamydia is an obligate intracellular bacterium that relies on its host cells for nutrient, energy, and DNA and RNA synthesis. Of the four recognized species Chlamydia trachomatis, psittaci, pneumoniae, and pecorium, only the first three are known to infect man. Epidemiology
The prevalence rate of chlamydia in the UK is approximately 10%, with higher rates among sexually active 20–24-year-old men, and 16–19-year-old women, perhaps reflecting the fact that the host immune system gradually eradicates the infection such that lower prevalence rates are observed in the older population. There were over 120 000 new cases of chlamydia reported by genitourinary medicine clinics in the UK in 2007, a 150% increase from 10 years ago. The wide spectrum of the disease presentations has hampered the epidemiological control of chlamydia infection. Pathogenesis
C. trachomatis exists in two phases during its life cycle in man: the infective extracellular form known as the elementary body and the metabolically active and dividing intracellular form known as the reticulate body. Infection occurs with the attachment and uptake into the host cell of the elementary body. The elementary body undergoes a transformation and reorganizes itself into the active reticulate body, encapsulating itself in a cytoplasmic vacuole thus evading the activity of cellular lysosomes and most probably antibiotics too.
The reticulate body proliferates rapidly for 8–48 hours, condenses back to the elementary body and ruptures the host cell by sheer weight of numbers, resulting in the infection of neighbouring cells. The extracellular elementary bodies, the dead and dying epithelial cells activate the host’s cell-mediated immunity orchestrated by interferon (IFN)-γ and interleukin (IL)-12. There is increased macrophage and natural killer cell activity with resultant tissue damage, repair, and fibrosis. The circulating IFN-γ suspends the intracellular multiplication of the of the reticulate body but does not kill or eliminate it and once the elementary bodies are cleared the stimulus for the production of IFN-γ is removed and with it the control of the reticulate body, which becomes activated, multiplies, and damages some more cells to repeat the cycle of tissue damage, repair, and fibrosis. These repeated cycles of cellular damage, immune activation, repair by fibrosis, and scarring are responsible for the tissue damage that is so characteristic of chlamydia infection. Screening
The National Chlamydia Screening Programme (NCSP) is an opportunistic screening intervention targeted at those aged sexually active, but who may not otherwise seek a test, are screened. The overall aim of the NCSP is to control chlamydia through the early detection and treatment of asymptomatic infection in the under-25-year-old population to prevent the development of complications such as pelvic inflammatory disease, infertility, miscarriage, ectopic pregnancy, or infection in neonates. Clinical features
At least 70% of women with chlamydia infection are asymptomatic and may present with complications in the long term. This is one of the most important arguments for a mass screening approach. The symptomatic minority may complain of lower abdominal or pelvic pain, intermenstrual or postcoital bleeding, dysuria, and vaginal discharge. In uncomplicated cases (approximately 70%) the infection is limited to the cervix and/or urethra, and bimanual examination is usually normal with no tenderness. In men, uncomplicated infection is limited to the urethra and also is mostly asymptomatic (approximately 52%).
Complicated chlamydia infection is associated with chronic urethritis, dysuria, inflammation of the Bartholin’s glands, mucopurulent cervicitis, pelvic inflammatory disease, Fitz–Hugh Curtis syndrome, reactive arthritis, proctitis, and pharyngitis. Tubal infertility, chronic pelvic pain, and ectopic pregnancy may follow complicated infections in about 10% of affected women.
Neonatal Chlamydia trachomatis
In some series, up to 60% of infants born to women with chlamydia manifest disease including:
• inclusion conjunctivitis, affecting 15–50% of neonates of chlamydia-positive women. This presents as mucopuru-lent discharge, oedema of the eyelids, and erythema of the palpebral fissures, usually within the first 5–7 days of life
• pneumonia, 10–20% of cases and appears between 3 weeks and 3 months of life
• otitis media
• nasopharyngitis
• failure to thrive. Diagnosis
Screening for and the diagnosis of chlamydia infections have become simplified and enhanced by the introduction of tests based on DNA amplification such as the polymer-ase and ligase chain reaction tests. Urine and self-administered low vaginal swab samples are sufficient and the sensitivity and specificities of these DNA-based tests approach 100%, a good 25–40% above previous tests based on antigen detection and cell culture.
Chlamydia is a fragile obligate intracellular organism and like viruses can only be cultured in cells, which until very recently was the sole method of diagnosis. Cell cultures were laborious, expensive, needed regional centres, live chlamydia organisms and therefore transport media, and special storage facilities.
Antigen detection tests such as the enzyme-linked immunosorbent assay (ELISA) and direct fluorescent antibody do not depend on maintaining a live organism and therefore do not require special transport or storage. They can also be automated, and therefore handle large quantities of samples with rapid turnover times. Management
• A single oral dose of azithromycin 1 g has an excellent compliance record, is better absorbed, and achieves higher tissue concentration than erythromycin, which is maintained for up to 4 days after ingestion of the single dose. The safety profile during pregnancy has not been established.
• Alternative antibiotic regimens include oral doxycycline 100 mg once or twice daily or erythromycin 500 mg four times daily for 7 days. Emphasis should be placed on completing the course.
• Refer to GUM clinic for comprehensive screening for other sexually transmitted infections and follow up.
• Contact tracing: 65% of female and 53% of male sexual contacts are concordant for chlamydia infection.
• Provide verbal and written information. Further reading
Chief Medical Officer’s Expert Advisory Group. Main report of the CMO’s expert advisory group on Chlamydia trachomatis. London: Department of Health, 1998.
House of Commons. Select Committee on Health. Third report on sexual health. Available at www.parliament.the-stationery-ffice.co.uk/pa/cm200203/cmselect/cmhealth/69/6902.htm
LaMontagne DS, Fenton KA, Randall S, et al. Establishing the National Chlamydia Screening Programme in England: results from the first full year of screening. Sex Transm Infect 2004;80:335–41
Department of Health. Chlamydia screening pilot: report of 1999–2000 study. London: DH 2002.
Department of Health. The national chlamydia screening programme in England, Programme overview, core requirements and data collection. London: DH 2004.
Health Protection Agency, SCIEH, ISD, National Public Health Service for Wales, CDSC Northern Ireland, the UASSG. Renewing the focus. HIV and other sexually transmitted infections in the United Kingdom in 2002. London: Health Protection Agency 2003.
Cates W, Wasserheit JN. Genital chlamydial infections: epidemiology and reproductive sequelae. Am J Obstet Gynecol 1991;164:1771–81.
Honey E, Augood C, Templeton A, et al. Cost effectiveness of screening for Chlamydia trachomatis: a review of published studies. Sex Transm Infect 2002;78:406–12.
Pimenta JM, Catchpole M, Rogers PA, et al. Opportunistic screening for genital chlamydial infection I: Acceptability of urine testing in primary and secondary healthcare settings. Sex Transm Infect 2003;79:16–21.
Pimenta JM, Catchpole M, Rogers PA, et al. Opportunistic screening for genital chlamydial infection II: Prevalence among health care attenders, outcome and evaluation of positive cases. Sex Transm Infect 2003;79:22–7. Internet resources
Additional information on the epidemiology of genital chlamydia infections diagnosed in GUM clinics in the United Kingdom is available: www.hpa.org.uk/infections/topics_az/hiv_and_sti/sti-chlamydia/epidemiology/epidemiology.htm.
Coagulation disorders
The coagulation disorders are a group of disorders where there is an alteration in the coagulability of the blood. This could either result in a state of (1) bleeding disorder from coagulation defect or (2) hypercoagulable state with an increased tendency to thrombus formation in the circulation. Coagulation defects leading to bleeding disorders
Although coagulation disorders can arise as a result of pregnancy complications (acquired defects), women with inherited coagulation defects can also become pregnant. Inherited coagulation defects
Von Willebrand’s disease: von Willebrand’s disease (vWD) is the most common hereditary coagulation abnormality described in humans. It has a prevalence of approximately 1% of the population. It arises from a qualitative or quantitative deficiency of von Willebrand factor (vWF), a multimeric protein that is required for platelet adhesion. This functions as a carrier protein for Factor VIII, forming circulating vWF–Factor VIII complex. The vWF gene is located on chromosome 12. There are three main types of vWD and all, except Type 3, are inherited as autosomal dominant traits. Type 3, the most severe form, is inherited as autosomal recessive trait. Type 1 is the commonest form and is usually mild.
These patients often have a family history and/or a personal history of bleeding tendency. During pregnancy, the major haemorrhagic risk is postpartum because of the rapid decrease in Factor VIII and vWF following delivery. Laboratory diagnosis is based on assessment of vWF activity, and antigen level and Factor VIII levels.
Antenatally these patients should be managed in conjunction with the haematologists. Desmopressin (DDAVP) therapy may be useful, as some patients (Type 1) respond well with the release of vWF from endothelial cells. The majority of cases require no haemostatic support during pregnancy. In known responders, intranasal DDAVP and tranexamic acid can be used during the last few weeks to minimize the risk of postpartum bleeding.
In labour, invasive monitoring, fetal blood sampling, episiotomy, and instrumental delivery should be avoided. The third stage should be actively managed. Factor VIII replacement and i.v. DDAVP and tranexamic acid may be required for postpartum bleeding.
Haemophilias
Haemophilias are inherited deficiencies in Factor VII (haemophilia A) or Factor IX (haemophilia B). Haemophilia A is the common type. Both are X-linked conditions and hence women are usually carriers and are not usually affected.
Prenatal diagnosis is an important issue since an affected child (usually male) would require regular expensive factor replacement therapy and is at risk of significant haemorrhage.
Thrombophilia
Thrombophilia is the increased tendency to thrombosis, secondary to any hypercoagulable state. Inherited and acquired factors may determine thrombophilia. Some physiological conditions, such as pregnancy are themselves ‘thrombophilic’.
Changes of coagulation system during pregnancy: Normal pregnancy is a recognized prothrombotic period.
• There is an increase in several of the coagulation factors, including fibrinogen, factors VII, VIII, X, and vWF.
• There is a decrease in the natural anticoagulant system, especially significantly lower levels of protein S and increased resistance to activated protein C (APC).
• Diminished fibrinolysis occurs as pregnancy proceeds, as evidenced by increased levels of plasminogen activator inhibitor-1 and-2 (PAI-1 and PAI-2) and increased levels of thrombin activatable fibrinolysis inhibitor (TAFI).
It has been well established that women with thrombophilic disorders are at a higher risk of venous thromboembolism (VTE) in pregnancy and puerperium. It has also been observed that those women have higher prevalence of obstetric complications in which microplacental thrombosis may play a pathogenetic role, such as placental abruption, pre-eclampsia, intrauterine growth restriction, intrauterine fetal death, and repeated spontaneous miscarriage, particularly late fetal loss.
Types of thrombophilia
Inherited thrombophilias are a heterogeneous group of conditions that have been implicated in a variety of pregnancy complications. The risk for thrombotic complications are much higher in the rarer homozygous states than in the more common heterozygous states of these inherited abnormalities.
The most common inherited thrombophilias are
• Factor V Leiden (FVL): this is the most common cause of APC resistance
• the G20210A mutation of the prothrombin gene (PGM).
Rarer causes of inherited thrombophilia include:
• antithrombin (AT) deficiency
• protein C deficiency
• protein S deficiency
• homozygosity for the thermolabile variant of methylene tetrahydrofolate reductase (MTHFR); this in conjunction with insufficient dietary intake of B vitamins, is associated with hyperhomocysteinaemia and, in turn, increased thrombotic risk
• protein Z deficiency (recently being linked to preterm delivery).
Collectively, inherited thrombophilias are present in 8–15% of Caucasian populations and they appear to be responsible for up to half of venous thromboembolism during pregnancy. Large numbers of case–control and cohort studies have now evaluated associations between thrombophilia and pregnancy loss. These studies overall suggest an association between FVL mutation, anti-thrombin, protein C and protein S deficiency, and recurrent and late fetal loss. The data are not consistent with regard to an association between recurrent and late fetal loss and prothrombin G20210A and MTHFR C677T homozygotes. There is no consistent evidence for an association between maternal thrombophilia and recurrent early first trimester loss (at less than 10 weeks). A recent meta-analysis, did not find an association between preeclampsia and FVL, prothrombin G20210A, or MTHFR C677T. When the analysis was restricted only to severe pre-eclampsia, there was a significant association with FVL and with MTHFR C677T homozygotes (Lin and August 2005).
Acquired thrombophilia
The most important cause of acquired thrombophilia is antiphospholipid antibody syndrome (APS). APS is characterized by the presence of antibodies directed against phospholipids or plasma proteins bound to anionic phospholipids. Patients may present with venous or arterial thrombosis, recurrent fetal loss, and/or thrombocytopenia. The disorder may be primary or associated with systemic lupus erythematosus and other rheumatic diseases.
The antiphospholipid antibodies in APS may be detected as
• anticardiolipin antibodies
• lupus anticoagulants
• antibodies to β2-glycoprotein-I
• other antibodies, including those to prothrombin, annexin V, phosphatidylserine, phosphatidylinositol, and others.
The mechanisms by which antiphospholipid antibodies cause thrombosis are not completely understood. The pathogenesis of the APS-associated clinical manifestations appears to result from a variety of effects of antipospholipid antibodies upon pathways of coagulation, including the procoagulant actions of these antibodies upon protein C, annexin V, platelets, and fibrinolysis.
Adverse pregnancy outcomes attributed to the presence of antiphospholipid antibodies are
• late fetal death
• early, severe pre-eclampsia/eclampsia
• fetal growth restriction
• maternal thromboembolic disease (venous or arterial)
• recurrent pregnancy loss. Many investigators believe APS is not a cause of embryonic loss before 10 weeks.
Who should be tested for thrombophilia?
The following conditions in a pregnant woman should warrant a thrombophilia evaluation:
• previous history of thrombosis
• strong family history of thrombosis
• history of unexplained loss beyond 10 weeks
• history of severe pre-eclampsia/HELLP(haemolysis, elevated liver enzymes, low platelets)
• history of severe intrauterine growth restriction
• history of placental abruption.
Management of thrombophilias during pregnancy
• Patients with known thrombophilic defect and no prior VTE or pregnancy complication; treatment is controversial.
• Women with antithrombin deficiency (AT) deficiency, protein C deficiency, homozygous Factor V Leiden (FVL) or prothrombin gene mutation (PGM) (high-risk thrombophilia) are at higher risk of venous thromboembolism (VTE) during pregnancy. They should receive both antepartum and postpartum thromboprophylaxis with low molecular weight heparin (LMWH).
• Women with other heterozygous thrombophilic states with no previous history of VTE need not be given antepartum prophylaxis. Low-dose aspirin may be used. Postpartum prophylaxis with LMWH should be considered.
• Patients with thrombophilia and previous history of VTE:
• they should receive antepartum and postpartum prophylaxis with LMWH.
• Patients with thrombophilia and previous related pregnancy complications.
• There is no good evidence that thromboprophylaxis improves obstetric outcome in women with inherited thrombophilia. Good randomized controlled trials are required before clear recommendations can be made.
• In cases with acquired thrombophilia secondary to APS, a combination of low dose aspirin and LMWH is effective in reducing fetal loss rate. Acquired coagulation defects
Disseminated intravascular coagulation
There is generalized stimulation of coagulation activity resulting in consumption of clotting factors and platelets. This results in defective clotting and stimulation of fibrinolysis. Fibrin degradation products (FDP) interfere with clot formation and myometrial activity and might contribute to further haemorrhage. Disseminated intravascular coagulation (DIVC) is never primary. In obstetrics, it usually occurs in association with
• placental abruption
• severe pre-eclampsia
• retained dead fetus in utero (beyond 3–4 weeks)
• sepsis
• prolonged shock from any cause
• amniotic fluid embolism.
Diagnosis
In the appropriate clinical setting, diagnosis is confirmed by a low platelet count, prolonged prothrombin time (PT), international normalization ratio (INR), and partial thromboplastin time (PTT), and high levels of circulating FDPs.
General management principles
• Treatment of the underlying triggering factor, e.g. evacuation of uterus in placental abruption and retained dead fetus.
• Component therapy:
• fresh frozen plasma (FFP), which contains all the clotting factors
• packed RBC (for haemorrhage)
• platelets
• cryoprecipitate.
• Anticoagulant therapy: controversial. It might be useful in selected cases of retained dead fetus.
• Volume replacement and maintenance of circulation. Further reading
Brenner B, Aharon A. Thrombophilia and adverse pregnancy outcome. Clin Perinatol 2007;34:527–41.
Kujovich JL. Thrombophilia and pregnancy complications. Am J Obstet Gynecol 2004;191:412–24.
Lin J, August P. Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol 2005;105:182–92.
Connective tissue disorder Rheumatoid arthritis
Rheumatoid arthritis (RA) is a systemic, chronic, autoimmune inflammatory disease affecting the joints mainly. There is an excessive immune response against body cells, and that leads to synovitis, pannus formation (i.e. thickening of synovium) cartilage breakdown, and bone erosion.
Epidemiology
RA affects about 1% of population, with a female to male ratio of (3:1) and approximately 1 in every 1000–2000 pregnancies is affected.
Aetiology
There is an association with the human leucocyte antigen HLA-D4 (70%). About 80–90% of patients are positive for rheumatoid factor (RhF), and 30% of cases are positive for antinuclear antibodies (ANAs).
Clinical picture
RA is characterized by periods of flares and remission. The prominent symptoms are joint pains and morning stiffness, with signs including swelling, and tenderness with limitation of movement.
The disease can affect other parts of the body causing pleuritis, pericarditis, Felty’s syndrome, rheumatoid nodules, and vasculitis.
Effect of pregnancy on RA
About 70–80% of women with RA experience improvement during pregnancy. In about 25% of patients the disease is active or even worsens, requiring treatment throughout pregnancy. Of those who experience remission, 90% suffer postpartum exacerbations.
Effect of RA on pregnancy
There seems to be no adverse affect of RA on pregnancy. Rarely, limitation of hip abduction is severe enough to impede a vaginal delivery.
Management
The main concerns relate to the safety during pregnancy and lactation of the medications used to treat rheumatoid arthritis. Paracetamol, aspirin, and corticosteroids can be used safely. Non-steroidal anti-inflammatory drugs (NSAIDs) are relatively safe, but best avoided in the last 6 weeks of pregnancy to avoid their effect on the ductus arteriosus. Azathioprine, and D-penicillamine are relatively safe. Antimalarials and sulphasalazine can also be used as a second line treatment safely.
The alkylating agents cyclophosphamide and chlorambucil, and the folic acid antagonist methotrexate are all teratogenic and fetotoxic and are contraindicated in pregnancy and lactation. Systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is a chronic, multifaceted inflammatory disease that can affect every organ system of the body. It involves multisystem microvascular inflammation with the generation of autoantibodies such as ANAs, double-stranded DNA (dsDNA), extractable nuclear antigens (ENAs), including anti Ro/La antibodies and antiphospholipid antibodies (APA). There are congenital deficiencies of complement (especially C4, C2, and other early components).
Epidemiology
The prevalence of SLE is variable. It is more common in women of child bearing age (6–10-folds higher). Almost 6% of patients have other autoimmune disorders.
Clinical picture
Non-specific fatigue, fever, arthralgia, arthritis, and weight changes are the most frequent symptoms. Discoid lesions often develop in sun-exposed areas. The kidney is the most commonly involved visceral organ in SLE, which could cause hypertension, haematuria, oedema, and anasarca. Leucopenia and, more specifically, lymphopenia are common.
Effect of pregnancy on SLE
SLE flares may be difficult to diagnose during pregnancy since many features are commonly seen in pregnancy. Whether pregnancy exacerbates SLE and increases the likelihood of flare particularly postpartum is controversial. In women with lupus nephritis, pregnancy does not seem to jeopardize renal function in the long term. There is a greater risk of deterioration in patients with a higher baseline serum creatinine.
Effect of SLE on pregnancy
SLE is associated with increased risks of spontaneous miscarriage, fetal death, pre-eclampsia, preterm delivery, and intrauterine growth restriction (IUGR). These risks may be attributed to the presence of APA, lupus nephritis or hypertension, and either active disease at the time of conception or first presentation of SLE during pregnancy. Pregnancy outcome is particularly affected by renal disease. For women in remission, but without hypertension, renal involvement, or APA, the risk of pregnancy loss and pre-eclampsia is probably no higher than in the general population. Pregnancy, and especially the postpartum period, represents an additional thrombotic risk in patients with SLE who have APA.
Management
Ideally this should begin with preconception counselling. Knowledge of the anti-Ro and APA, renal and blood pressure status allows prediction of the risks to the woman and her baby. It is advised to conceive during remission. Pregnancy care is best undertaken in multidisciplinary combined clinics where physicians and obstetricians can monitor disease activity and the fetus regularly. Disease activity is monitored by appearance of symptoms, rising anti-DNA antibody titre, cellular casts in urine, and fall in the complement levels. Fetal growth should be monitored. Uterine artery and umbilical artery Doppler blood flow studies are useful.
Disease flares must be actively managed. The use of azathioprine, NSAIDs and aspirin is covered in the section on Rheumatoid arthritis. Hydroxychloroquine should be continued since stopping may precipitate flare.
Neonatal lupus syndromes
It occurs as congenital heart block or as lupus rash. It occurs in 3.5% of cases. Neonatal lupus is highly associated with maternal anti-Ro (present in about 30% of patients with SLE), although the rash may occur with anti-RNP antibodies. The risk of neonatal lupus is increased if a previous child has been affected.
There is no indication for prophylactic treatment; nevertheless, fetal four-chamber cardiac echocardiography is recommended at 16–28 weeks and if heart block is found dexamethasone 4 mg/day is given to the mother. The cutaneous form of neonatal lupus usually manifests in the first 2 weeks of life. The infant develops typical geographical skin lesions usually on the face and scalp, which appear after sun or UV light exposure. The rash disappears spontaneously within 6 months and scarring is unusual. Antiphospholipid syndrome
Antiphospholipid syndrome (APS) is a disorder characterized by recurrent thrombosis and/or fetal loss associated with elevated levels of antibodies directed against membrane anionic phospholipids (i.e. anticardiolipin (aCL) antibody), or evidence of lupus anticoagulant.
Clinical picture
Criteria for diagnosis are
• thrombosis: venous or arterial
• pregnancy morbidity: three or more consecutive miscarriages (10 weeks’ gestation with normal fetal morphology), and one or more premature birth (features of APS. The risk of fetal loss is directly related to the antibody titre, particularly the IgG aCL. There is also a high incidence of intrauterine IUGR and placental abruption.
Management
Women with APS and previous thromboembolism are at extremely high risk in pregnancy and the puerperium and should be given antenatal thromboprophylaxis with heparin. Many are on long-term warfarin and the change from warfarin to heparin should be achieved prior to 6 weeks’ gestation to avoid warfarin embryopathy. Heparin should be continued intrapartum and postpartum until they are re-warfarinized.
The management of pregnancy in women with APS, recurrent pregnancy loss, but without a history of thromboembolism is debated. Most centres now advocate low-dose aspirin (75 mg–100 mg) for all women, often prior to conception. Any additional benefit of heparin must be balanced against the risk of heparin-induced osteoporosis. Immunosuppression with intravenous immunoglobulin (IVIG) is extremely expensive, and its use is limited to occasional salvage therapy in women who develop complications despite aspirin and heparin.
Ultrasound monitoring of fetal growth and uteroplacental blood flow is crucial. This allows for timely delivery. Assessment of uterine artery Doppler waveforms is performed in the midtrimester, and the presence of bilateral artery notches in high-risk pregnancies is associated with pre-eclampsia, IUGR, and intrapartum asphyxia. Abnormal uterine artery Doppler velocimetry is also of some value in predicting placental abruption. Scleroderma
It is a systemic disease characterized by skin induration and thickening in addition to tissue fibrosis and chronic inflammatory infiltration in other organs, prominent fibroproliferative vasculopathy, and humoral and cellular immune alterations.
Epidemiology
The estimated incidence of systemic sclerosis is 19 cases per million population.
Clinical picture
It may be divided into a localized cutaneous form (morphoea) with areas of thickened skin usually on the forearms and hands, and systemic sclerosis associated with Raynaud’s phenomenon and organ involvement. The skin in systemic sclerosis is typically bound down to produce sclerodactly, beaking of the nose, a fixed facial expression, and limitation of mouth opening. Systemic involvement usually takes the form of progressive fibrosis and includes the oesophagus most commonly (80%), the lungs (45%), the heart (40%), and the kidneys (35%).
Effect of pregnancy on scleroderma
In the localized type there is no adverse effect, but with the early diffuse type (>4 years) there is a significant risk of deterioration especially in reflux oesophagitis and renal crisis. It may be appropriate to advise women with severe organ involvement against pregnancy. Raynaud’s disease improves due to vasodilatation. Postpartum deterioration occurs in cases of severe pulmonary fibrosis and pulmonary hypertension.
Effect of scleroderma on pregnancy
Pregnancy in women with systemic sclerosis is considered a high risk because of a higher risk of pregnancy loss and higher complication rates. Pregnancy risk is greatest in those who have had the disease for less than 4 years and who also have diffuse cutaneous involvement. Fetal outcome is impaired and there is an increased risk of premature delivery, pre-eclampsia, IUGR, and perinatal mortality. Venepuncture, venous access, and blood pressure measurement may be difficult because of skin or blood vessel involvement. General anaesthesia may be complicated by difficult endotracheal intubation, and regional anaesthesia may also be difficult.
Management
The management is symptomatic. Raynaud’s phenomenon may be helped by heated gloves or nifedipine. Early assessment by an anaesthetist is advisable if problems with regional or general anaesthesia are anticipated. Further reading
Chakravarty EF, Colon I, Langen ES, et al. Factors that predict prematurity and preeclampsia in pregnancies that are complicated by systemic lupus erythematosus. Am J Obstet Gynecol 2005;192:1897–904.
Shehata HA, Nelson-Piercy C, Other endocrine, connective tissue disease, and skin disorders in pregnancy. Curr Obstet Gynaecol 2001; 11:329–35.
Shehata HA, Nelson-Piercy C, Khamashta MA. Management of pregnancy in antiphospholipid syndrome. Rheum Dis Clin North Am 2001;3:643–59.
Arya R, Shehata HA, Patel RK, et al. Internal jugular vein thrombosis after assisted conception therapy. Br J Haematol 2001;115:153–5.
Nelson-Piercy CA. Handbook of obstetric medicine, 3rd edn. London: Informa Healthcare 2006.
Brennan P, Barrett J, Fiddler M, et al. Maternal-fetal HLA incompatibility and the course of inflammatory arthritis during pregnancy. J Rheumatol 2000;27:2843–8. Internet resources
www.emedicine.com/
www.miscarriageclinic.co.uk
Cytomegalovirus Definition
Cytomegalovirus (CMV) is a DNA virus of the herpesvirus group which causes cytomegalic inclusion disease. This name is derived from the characteristic large cells containing prominent intranuclear inclusion bodies that have been identified with this disease since the early twentieth century. Epidemiology
The epidemiology of CMV infection is complex, but it is key to understanding disease manifestations. CMV is a ubiquitous virus. Overall, CMV can be cultured from the cervix or urine in 2–28% of pregnant women. In the USA and Europe, 40% of reproductive age women are susceptible to CMV. The rate of seroconversion in women in the reproductive age range is approximately 2–6% annually.
Even though CMV infection is common, serious illness occurs only in fetuses and immunodeficient or immuno-suppressed individuals. Over 90% of adult infections are subclinical, with the remainder having a mononucleosis-like illness. Congenital CMV infection is acquired in utero, primarily from transplacental transmission. Neonates with congenital CMV are culture positive (most often in the urine) for the virus at birth. About 1% of all newborns excrete CMV at birth and are congenitally infected; an additional 3–5% of infants acquire CMV perinatally, from infected cervical secretions, infected milk, or exposure to infected transfused blood.
In utero CMV infections are the major concern, because of potentially serious adverse effects on development. On the other hand, perinatally acquired CMV infection does not result in serious complications or sequelae except in very-low-birthweight neonates. With CMV, congenital infections may occur after either primary or recurrent maternal infection, and most intrauterine infections occur in immune, rather than in susceptible, women. Symptomatic congenital CMV infection occurs mainly with primary maternal infection. Sequelae have been noted in 25–40% of the infants in the primary infection group, compared with only 8% in the recurrent CMV infection group. Common manifestations of intrauterine CMV infection are mental impairment and hearing loss.
CMV is transmitted by sexual contact or by spread within households or daycare centres.
The public health impact of congenital CMV infection is large. In the USA, for example, over 7000 infants annually either die or develop significant neurological sequelae.
The prognosis is very guarded for infants with clinically apparent disease at birth, with mortality as high as 20–30%, and with 90% having late complications. Of the 90% of congenitally infected neonates who appear normal at birth, about 15% do not develop normally, as neurological sequelae such as hearing loss, low IQ, and behaviour problems may become apparent. Clinical approach
Diagnosis
As noted, only 10% of maternal infections with CMV are symptomatic, producing a heterophil-negative mononucleosis syndrome.
The spectrum of disease in the fetus and neonate is wide. Clinically apparent disease occurs in only 10% of infants with congenital CMV. In severely infected neonates, manifestations are hepatosplenomegaly, jaundice, thrombocytopenia, purpura, microcephaly, deafness, chorioretinitis, optic atrophy, and cerebral calcifications. A characteristic tetrad includes mental retardation, chorioretinitis, cerebral calcification, and microcephaly or hydrocephaly.
CMV infection may be documented by serological testing using one of several Ig antibody tests. Demonstration of seroconversion is the best documentation of primary infection. If infection has occurred within the previous 4–8 months, IgM-specific antibody can be detected in the serum. Avidity assays may also be helpful as low avidity indicates recent infection whereas high avidity indicates recurrent infection.
CMV infection may also be detected through culture or by PCR, but isolation does not differentiate primary and recurrent infections.
Prenatal diagnosis of CMV infection has been made by using ultrasound, amniocentesis, and cordocentesis (percutaneous umbilical cord sampling). Common ultrasound abnormalities are microcephaly (10%), hepatosplenomegaly (18%), ventriculomegaly (32%), calcifications of the brain, liver, or placenta (40%), intrauterine growth restriction/oligohydramnios (55%), ascites, pericardial or pleural effusion, hypoechogenic bowel, and hydrops.
Detection of CMV by culture or PCR in the amniotic fluid is an excellent method for detection of in utero CMV infection. Amniotic fluid testing for CMV should be offered to pregnant women with documented primary CMV infection or when ultrasonography suggests CMV infection. The diagnostic sensitivity of a single amniocentesis is about 80–85%. Thus, a repeat amniocentesis may be indicated. High CMV viral load in amniotic fluid is associated with clinically evident fetal or neonatal outcomes.
Fetal blood sampling may be used to gain additional information about the fetal complications such as thrombocytopenia, anaemia, or hepatic involvement. The combination of these tests has a diagnostic sensitivity of about 80–90% in antenatal diagnosis of CMV.
Treatment
Specific treatments of CMV infection are available and include adenosine arabinoside, cytosine arabinoside, ganciclovir, and foscarnet, all of which have been used for severe clinical infection. However, these drugs are quite toxic, and their use should be undertaken in consultation with experts in perinatal infection.
Recently, one group has reported decreased symptomatic infection at birth by use of CMV-specific intravenous immunoglobulin in pregnancies complicated by documented CMV infection and abnormal ultrasound findings. In this non-randomized trial, use of the CMV-specific IVIG led to a rate of symptomatic infection at birth of 7% (1 of 15) in fetuses with abnormal ultrasounds versus a rate of 100% (7 of 7) in those not given the IVIG. Methodological problems with the study are important, however, and this approach to treatment remains to be established.
Despite the potential hypothetical advantages of a CMV vaccine in preventing congenital CMV infection, no CMV vaccine is currently available.
Routine screening for CMV infection in pregnancy is not recommended. Further reading
Antsaklis AJ, Daskalakis GJ, Mesogitis SA, et al. Prenatal diagnosis of fetal primary cytomegalovirus infection. Br J Obstet Gynecol 2000;107:84–8.
Guerra B, Lazzarotto T, Quarta S, et al. Prenatal diagnosis of symptomatic congenital cytomegalovirus. Am J Obstet Gynecol 2000;183:476–82.
Nigro G, Adler SP, LaTorre R, Best AM. Congenital Cytomegalovirus Collaborating Group. Passive immunization during pregnancy for congenital cytomegalovirus infection. New Engl J Med 2005;353:1350–62.
Revello MG, Gerna G. Pathogenesis and prenatal diagnosis of human cytomegalovirus infection. J Clin Virol 2004;29:71–83.
Stagno S. Cytomegalovirus. In: Remington JS, Klein JO, (eds) Infectious diseases of the fetus and newborn. Philadelphia: Elsevier Saunders 2006:739–81.
Dermatology Physiological changes
Increased pigmentation
This begins in the first trimester and fades after delivery. Existing pigmented areas (e.g. areolae and axillae) become darker. Specific areas (e.g. linea nigrum, from the umbilicus to the symphysis pubis in the midline) become pigmented.
Melasma
Patches of light-brown facial pigmentation developing in about 70% of women in the second half of pregnancy. The usual distribution involves the forehead, cheeks, upper lip, and chin.
Spider naevi
Occur on the face, upper trunk and arms. They can be numerous and in some cases almost confluent. Most appear in early pregnancy and regress following delivery, although 25% may persist.
Palmar erythema
Present in up to 70% of women by the third trimester and fades within 1 week of delivery.
Hair fall
A normal feature of the postpartum period, occurring in most women at between 4 and 20 weeks after delivery. It results from the increased conversion of hairs from the anagen (growing) to telogen (resting) phase, following the increased proportion of hairs in the anagen phase during pregnancy. Hair is lost diffusely, but recovery is usual within 6 months.
Striae gravidarum
These develop in most women, but are more common in obese women and multiple pregnancy. They appear perpendicular to skin tension lines as pink linear wrinkles. They fade and become white and atrophic, although never disappear completely.
Pruritus without rash or cholestasis
This may be a feature of normal pregnancy. Liver function tests should however be checked in any pregnant woman, especially if onset occurs in the third trimester. Pre-existing conditions
Eczema
This often, but not invariably, improves during pregnancy. Women should be reassured that if they require topical steroids to control their eczema, these are not contraindicated in pregnancy.
Psoriasis
This can improve, remain unchanged or deteriorate during pregnancy. Psoriasis may present for the first time in pregnancy. Dithranol and coal tar may be safely used in pregnancy. Methotrexate is an antimetabolite and is contraindicated in pregnancy. Rarely, a severe form of pustular psoriasis, impetigo herpetiformis, may develop. Urticated erythema, beginning in the flexures and especially the groins, is associated with sterile pustules which may become widespread and affect mucosa. This condition is associated with severe systemic upset, including fever, neutrophilia, and hypocalcaemia. An increased perinatal mortality rate is also reported and these women require intensive treatment and regular fetal surveillance. Coincidental conditions
Acne
This may develop for the first time in pregnancy. Preexisting acne may improve or worsen during pregnancy. Both tetracyclines and retinoids (vitamin A analogues, e.g. isotretinoin) are contraindicated in pregnancy. Erythromycin may be used safely.
Erythema nodosum
This may occur in pregnancy, without any demonstrable known underlying precipitating cause. Tuberculosis and sarcoidosis should be excluded with a chest X-ray and the woman asked about symptoms of streptococcal infection and inflammatory bowel disease, as well as any recent medications (particularly sulphonamides). If no underlying cause is discovered, the prognosis is excellent.
Erythema multiforme
This also may complicate pregnancy without any obvious underlying cause. The commoner precipitating causes should be sought (e.g. drugs and viral infections), before attributing the eruption to pregnancy alone. Dermatoses specific to pregnancy
Polymorphic eruption of pregnancy
Occurs in about 0.5% of pregnancies, usually after 35 weeks’ gestation with rapid resolution after delivery. It is more common in primiparous and twin pregnancies. The rash is pruritic in nature with urticarial papules and plaques, rarely vesicles (but not bullae) and target lesions. It is mainly distributed around the abdomen (with umbilical sparing), along striae, with spread to thighs, buttocks, and upper arms. There are no known harmful effects on the fetus.
Treatment options include 2% phenol in oily calamine or 0.5% menthol in aqueous cream, 1% hydrocortisone cream of ointment, sedative antihistamine (e.g. chlorpheniramine (Piriton) 4 mg three or four times daily or promethazine (Phenergan) 25 mg at night). Systemic steroids may occasionally be required.
Pemphigoid gestationis
It has an incidence of 1 in 10 000 to 1 in 60 000 pregnancies. It is autoimmune disorder (possibly related to exposure to fetal antigens). It is associated with bullous pemphigoid and other autoimmune conditions, e.g. Graves’ disease, vitiligo, insulin-dependent diabetes, rheumatoid arthritis. The onset of rash may occur at any time (9 weeks to 1 week postpartum; usually about 20–22 weeks), with no relationship to parity. The rash is intensely pruritic with urticated erythematous papules and plaques, target lesions and annular wheals. Distribution includes abdomen (umbilicus affected), with lesions begin in periumbilical region in most patients, spreading to limbs, palms, and soles. Eruption occurs after variable delay, usually 2 weeks with vesicles and large tense bullae. If it occurs in the second trimester, there is usually an improvement at the end of the pregnancy, but a flare postpartum. Urticated plaques may persist for several months after delivery.
Diagnosis
Diagnosis is usually made by direct immunofluorescence, showing complement (C3) deposition at the basement membrane zone. This distinguishes pemphigoid gestationis from polymorphic eruption of pregnancy in which immunofluorescence is negative.
An increased risk to the fetus has been reported, and recent studies have shown an association with low birth-weight and premature delivery. As this is an autoimmune disease, the neonate may be affected with a similar rash, but this only occurs in 10% of cases and is mild and transient.
Treatment
Treatment options include topical corticosteroid (1% hydrocortisone cream or ointment) and sedative antihista-mines. Most require systemic steroids (e.g. Prednisolone 40 mg/day) and these should not be withheld in pregnancy.
It usually recurs in future pregnancies (with possibly earlier onset and more severe course). It may recur with use of combined oral contraceptive pill.
Prurigo of pregnancy
It has an incidence of 1 in 300 pregnancies. It is associated with atopy and occurs at about 25–30 weeks. The rash is pruritic with groups of red/brown excoriated papules. It affects mainly the abdomen and the extensor surfaces of limbs. The pruritus improves at delivery, but papules may persist for several months after delivery. There are no known harmful effects on the fetus.
Treatment is as polymorphic eruption of pregnancy. Recurrence is possible.
Pruritic folliculitis of pregnancy
The incidence is not known. It occurs in the second or third trimester. The pruritic rash is widespread and acnei-form in nature with erythematous, follicular papules and pustules, mainly distributed in the trunk and thighs. Resolution occurs within 2 weeks after delivery.
There are no known harmful effects on the fetus.
Treatment options are as in pruritis of pregnancy in addition to topical 10% benzoyl peroxide. Further reading
Nelson-Piercy C. A handbook of obstetric medicine, 3rd edn. London: Informa Healthcare 2006.
Shehata H A, Nelson-Piercy C. Connective tissue and skin disorders in pregnancy. Curr Obstet Gynaecol 2001;11:329–35.
Diabetes in pregnancy Prevalence of diabetes mellitus in relation to pregnancy
Of the estimated 650 000 annual births in England and Wales, 2–5% are to women with Diabetes mellitus (DM). Pre-existing type 1 and type 2 DM account for 0.27% and 0.10% of births respectively. The prevalence of both types of DM is rising, but type 2 more so, and particularly among ethnic groups, including Afro-Caribbeans, South Asians, Middle Eastern, and Chinese. The prevalence of gestational DM (GDM) is estimated as in the range 3–5% in England and Wales, with considerable regional variation depending on ethnic diversity of the populations. Approximately 87.5% of pregnancies affected by DM are thought to be due to GDM, with 7.5% due to type 1 and the remainder to type 2. However, due to a variety of factors there are immense difficulties with the accurate estimation of the prevalence of GDM. Types of diabetes mellitus
Four types/categories of DM are described.
Type 1
Formerly type I, insulin-dependent diabetes mellitus (IDDM), or juvenile diabetes: this is characterized by β-cell destruction caused by an autoimmune process, usually leading to absolute insulin deficiency. The onset is usually acute, over a period of a few days to weeks, with the majority of patients at the onset of disease being under the age of 25.
Type 2
Formerly type II, non-insulin dependent diabetes mellitus (NIDDM), or adult-onset diabetes: This is characterized by insulin resistance in peripheral tissues and an insulin secretory defect of β-cells. This is the most common form of DM and is associated with a familial predisposition, increasing age, obesity, and lack of exercise. It is more common in women, especially those with a history of GDM.
Other specific types of diabetes mellitus
In this category are grouped types of DM of various known aetiologies, including people with genetic defects of β-cell function (formerly called maturity-onset diabetes of the young (MODY)), people with disease of the exocrine pancreas such as pancreatitis, cystic fibrosis, pancreatic dysfunction associated with other endocrinopathies such as acromegaly and also those caused by drugs, chemicals, or infection.
Gestational diabetes mellitus
This is defined as carbohydrate intolerance of variable severity with onset or first recognition during the present pregnancy. These women have normal glucose homeostasis during the first half of pregnancy and develop a relative insulin deficiency during the latter half of pregnancy leading to hyperglycaemia. This resolves after delivery in most women but increases the risk of developing type 2 DM in later life.
It should be noted that the oral glucose tolerance test (OGTT) previously recommended by the National Diabetes Data Group (NDDG) and still the criterion recommended by the World Health Organization (WHO) has been replaced with the recommendation that the diagnosis of DM be based on two fasting plasma glucose levels of 7 mmol/L (126 mg/dL) or higher.
Table 8.11.1 Diagnostic criteria for diabetes

Screening for GDM
Controversy reigns supreme on the issue of screening for GDM: who should be screened, when, and how remain unresolved questions. On one side of the debate is the assertion that evidence does not support routine screening for GDM and, therefore, it should not be offered, whereas on the other is the acknowledgement that the evidence is limited but does not conclusively support not screening for GDM. In the UK, current trends are to suggest that women with no risk factors for GDM, and therefore considered low risk, should not be screened. Similar advice is given by the American College of Obstetricians and Gynaecologists (ACOG), the American Diabetes Association (ADA), and the Joslin Diabetes Center guidelines, while the WHO and International Diabetes Centre guidelines suggest universal screening at 24–28 weeks. All guidelines advocate screening high-risk women early rather than at 24–28 weeks.
The results of recent studies may swing the debate in favour of routine/universal screening. The ACHOIS trial has provided evidence that purports to show that treatment of a screening-detected population with mild GDM reduces serious neonatal (as a composite outcome) and maternal (pre-eclamptic toxaemia (PET) or gestational hypertension) outcomes. The even more recently published HAPO study also shows a continuous relationship between glucose concentration at 28 weeks OGTT and pregnancy outcomes and makes a strong case for universal screening.
Where screening is advocated there is no universally accepted screening method, although either risk factor assessment or laboratory-based testing are the common methods. Risk factor assessment (see box Risk factors for GDM) is a common international practice and 80% of obstetric units in the UK employ this method.
Risk factors for GDM
Maternal age >37 years
Ethnicity
Prepregnancy weight >80 kg or BMI >28 kg/m2
Family history of diabetes in first-degree relative
Previous macrosomia/polyhydramnios
Previous unexplained stillbirth
Polycystic ovarian syndrome
Other screening tests used include glycosuria, HbA1c, fructosamine, random plasma glucose, fasting glucose, the 50-g 1-hour glucose challenge test (GCT) and the OGTT. The GCT remains the most popular screening test for GDM, advocated in the USA by the ADA, the ACOG, the International Diabetes Centre, and the Joslin Diabetes Center, and is generally regarded as the yardstick for comparing all screening tests for GDM. It has a sensitivity of 79% and specificity of 87%. The fasting glucose as a screening test has the attraction of being easy to administer, well tolerated, inexpensive, reliable, and reproducible. However, it has given varied results in different populations and its use as a screening test in pregnancy remains ambiguous.
To underscore the debate surrounding screening, there is also no universal agreement on a diagnostic test for GDM. The OGTT is the gold standard diagnostic test for GDM, but its many disadvantages include the argument that it is non-physiological, that it is unpleasant for use in subjects where nausea may already be an issue, that it is not reproducible, and appears to have variable predictive values in different ethnic origin. All expert panels agree that OGTT is the confirmatory diagnostic test for GDM despite the added problem of nausea and vomiting in pregnant women. There is no agreement on the glucose load (75 g versus 100 g) or the criteria used for diagnosis of GDM. The common diagnostic tests and criteria for diagnosis of GDM are illustrated in the Table 8.11.2. Aetiology and pathogenesis
Type 1 diabetes mellitus
This is an organ-specific autoimmune disease associated with serological evidence of autoimmune destruction of the pancreas and presence of islet cell antibodies. There is a genetic component, and the HLA region on chromosome 6 was identified very early on as a potential site of a major susceptibility gene for type 1 diabetes. Genes have been identified for rare, monogenic, or syndromic forms of diabetes. Rare variations in insulin genes result in the autosomal dominant form of diabetes. Rare syndromes like Wolfram syndrome and Wolcott Rallison syndrome with linkages to specific genes have now been described, but the discussion of these is beyond the scope of this chapter. Genes accounting for susceptibility to MODY have also been identified.
Table 8.11.2 Various threshold values for diagnosis of GDM

Type 2 diabetes mellitus
In contrast to type 1, there is no evidence of immune pathogenesis in type 2 DM. However, there is a much stronger genetic component. The incidence increases with age and there is a strong association with obesity. Over 25 genome-wide linkage scans for type 2 diabetes have been completed to date and the regions showing the greatest replication among studies include 1q, 12q, and 20q. An association has been reported between type 2 diabetes and a variation in the gene for transcription factor 7-like 2 (TCFL2).
Pathophysiology of GDM
Significant changes in maternal fuel metabolism occur in pregnancy: in early pregnancy fasting plasma glucose concentration decreases and there is a slight decrease in endogenous glucose production. By the end of first trimester insulin sensitivity starts to fall and by the third trimester insulin-mediated glucose utilization declines by approximately 50% in lean and 40% in obese women. There is accelerated ketosis in the fasting state and a rise in maternal fasting glucose and free fatty acids.
The cause of the insulin sensitivity in the first trimester is not known. The subsequent rise in insulin resistance is due to several factors. A rise in plasma concentration of hormones such as placental lactogen, prolactin, cortisol, and progesterone correlates with this insulin resistance in mid-pregnancy. However, a rise in the inflammatory cytokine tumour necrosis factor (TNF)-α, produced by cells of immune system, suggests the involvement of intermediate mechanisms. Compared with other potential markers such as leptin, cortisol, human placental lactogen, or prolactin, the increase in TNF-αconcentration appears to be the best predictor of insulin resistance in pregnancy, independent of BMI An increase in insulin resistance in mid-pregnancy is compensated by an increase in fasting and post-meal plasma insulin concentration due to increased insulin production by the pancreatic β-cells.
Compared with normal pregnancy, there is increased insulin resistance in GDM. It has been suggested that women with GDM already have chronic underlying insulin resistance upon which pregnancy-related changes in insulin sensitivity is superimposed. The chronic insulin resistance of GDM could partly be due to increased fat mass, as GDM has a strong association with maternal obesity. Additional factors might be genetically determined defects in insulin receptor signalling.
Pancreatic β-cell dysfunction is another key feature observed in those with GDM. The exact mechanism of this is unclear. The initial response to insulin resistance is expansion of β-cell mass which is then probably followed by increased beta cell apoptosis.
Genetics of GDM
Studies have shown some links between familial clustering of GDM and type 1 and type 2 diabetes. It has been observed that the HLADR3 and DR4 antigens were uncommon overall but occur more frequently in women with GDM than in women with normal pregnancy.
Effects of diabetes on pregnancy
Congenital malformation
Poorly controlled DM in women is strongly associated with an increased risk of congenital malformation. Although there is strong evidence that good glycaemic control significantly reduces this, there is still a three to five times higher incidence of congenital malformation in women with DM, suggesting that either the efforts at glycaemic control are inadequate or, more likely, that DM may have a permanent and irreversible effect on reproduction. The exact underlying mechanisms are poorly understood, but glucose metabolism is likely to be central, influencing oocyte maturation and the quality of any subsequent embryo. Poor glucose control in the mother will also be reflected in poor control in the fetus, and recent research suggests that hyperglycaemia in the fetus may predispose the offspring of a diabetic mother to develop metabolic disease later in life.
Spontaneous miscarriage
Research has that women with poorly controlled diabetes, defined as a glycosylated haemoglobin (HbA1c) value greater than 6 SD above the mean, have a spontaneous abortion rate of 28% compared with 10–17% in well-controlled diabetic women. The mechanism of miscarriage is likely to be linked to abnormal embryonic development in the early period of organogenesis, which in turn is linked to early abnormal metabolic control. It is therefore not surprising that interventions designed to decrease the rate of congenital malformation have also resulted in a decrease in the risk of spontaneous miscarriage in women with DM.
Diabetes associated stillbirth and perinatal mortality
The stillbirth, neonatal, and perinatal mortality rates for babies born to diabetic women are substantially higher than those observed in the general population, although these have improved over the last decades. This increased risk is most commonly associated with insulin requiring pregestational diabetes, but may also involve GDM. Table 8.11.3 shows the stillbirth, perinatal mortality rate, and neonatal death in type 1 and type 2 diabetes. Previous studies have reported perinatal mortality in the offspring of women with type 2 diabetes to be equivalent or higher than that seen in women with type 1 diabetes. There was no evidence from the recent CEMACH report of a difference in the mortality rates of babies born to women with type 1 compared with those from type 2 diabetic women.
Risk factors for stillbirth in diabetic women include obesity, previous Caesarean section, congenital birth defect, and intrauterine growth (restriction) IUGR. IUGR is particularly associated with vascular complications of diabetes.
The pathophysiology of fetal compromise in diabetes is poorly understood and is most likely to be multifactorial. Although at least three pathological processes have been implicated, the final common pathway leading to fatal damage or death appears to be fetal asphyxia. The three processes are fetal hypoxia, fetal acidosis, and an alteration in fetal and/or maternal metabolism, details of which are beyond the scope of his chapter.
Fetal macrosomia
Excessive fetal growth is associated with all types of DM and maternal obesity. Although different definitions have been applied to macrosomia, the conventional definition is a birthweight greater than 4.5 kg or greater than 90th or 95th percentile or the mean +2 SD for a given gestational age.
In the majority of instances it is not possible to give a convincing explanation of why macrosomia develops, but some factors appear to be contributory. It has been found that maternal glycaemia is significantly higher by the early third trimester in diabetic women destined to deliver a large baby than those destined to have a baby of average weight. There is lack of agreement however about whether the post-meal glucose and/or HbA1c or a fasting glucose taken at 29–32 weeks is a better predictor of macrosomia. Other factors having an effect on birthweight are maternal prepregnancy weight and BMI, and maternal weight gain during pregnancy, although the latter appears to have a weak correlation where GDM is concerned. Increased insulin resistance in GDM leads to increased shunting of substrate from the maternal to the fetal circulation throughout pregnancy and this excessive supply of nutrients diminishes the relative influence of maternal weight gain on birthweight. Finally the modified Pederson’s hypothesis, which explains various fetal and neonatal complications, can also explain macrosomia.
Modified Pederson’s hypothesis

Maternal considerations
There is an increased risk of pre-eclampsia, further increased if there is pre-existing hypertension or renal disease. In the presence of concomitant nephropathy or hypertension the risk is about 30%. Proteinuria significantly worsens in women with diabetic nephropathy, leading to severe oedema and hypo-albuminaemia. There is also often a normocytic normochromic anaemia which responds only to recombinant erythropoietin. There is increased risk of infection particularly urinary tract, respiratory, endometrial, and wound infections. Vaginal candidiasis is relatively more common. The Caesarean section rate is increased to about 60%, at least partly due to early induction. Effect of pregnancy on diabetes
Diabetic nephropathy
All women with pre-existing diabetes should have a 24-hour urine collection for total protein and creatinine clearance. In women with nephropathy, changes in creatinine clearance are variable during pregnancy and most women will not exhibit a normal rise in creatinine clearance. Protein excretion will frequently rise to the nephrotic range. However, the majority of young diabetic women with overt nephropathy demonstrate only baseline proteinuria without a reduction in creatinine clearance, and in pregnancy many will have successful outcomes without renal disease progression. Angiotensin-converting enzyme (ACE) inhibitors are considered to have teratogenic potential, and therefore current standard practice is to stop them as soon as a woman falls pregnant and substitute with a calcium channel blocker or equivalent.
Pregnancy outcomes are surprisingly good in women with diabetic nephropathy, although compared with diabetic women without vasculopathy, excess morbidity is clearly present. Preterm delivery often complicates more than 50% of pregnancies and IUGR more than 15%. Preeclampsia also often exceeds 50% and Caesarean section is often in excess of 70%. The outcome seems to be related to baseline renal function and women with initial serum creatinine of more than 1.5 mg/dL or urine protein excretion of more than 3 g/24 hours have an increased risk of the complications mentioned above.
Other effects of pregnancy on diabetes
Normal pregnancy is associated with increased insulin production and resistance. Therefore women with IDDM and NIDDM require increasing doses of insulin as pregnancy progresses and maximum requirements at term can be at least twofold of prepregnancy doses.
Hypoglycaemia is more common and probably related to tight control. For the same reason diabetic ketoacidosis (DKA) seems to be rare. The risk is increased in the presence of hyperemesis, infection, tocolysis or corticosteroid therapy. DKA is discussed below.
Retinopathy is a common ocular complication of diabetes with a prevalence of 17% among patients diagnosed before the age of 30 with disease duration of 5 years. After 15 years, the prevalence is over 90%. There are two well-characterized stages: non-proliferative or background retinopathy and proliferative retinopathy. Certain factors in pregnancy, such as duration of diabetes, degree of metabolic control, and hypertensive disorders influence the progression of proliferative retinopathy. It is also clearly associated with the severity of the pre-existing disease. Rapid normalization of glucose is another factor that contributes to worsening of retinopathy.
Diabetic neuropathy is a heterogeneous group of abnormalities involving both autonomic and peripheral nervous systems. Earlier studies suggested that pregnancy could enhance progression of neuropathy. This was however challenged by more recent data which concluded that parity does not influence long-term prevalence or severity of diabetic autonomic neuropathy.
Gastroparesis, which is a form of autonomic neuropathy, interferes with food absorption and is therefore associated with difficulties in blood glucose control and severe nausea and vomiting. The most worrisome aspect of diabetic autonomic neuropathy during pregnancy is the occurrence of gastroparesis diabeticorum. It may result in significant maternal complications including pulmonary oedema or aspiration, the need for parenteral nutrition, and poor glucose control. Severe fetal complications such as IUGR, preterm labour, and fetal loss have also been reported. Fortunately, severe gastroparesis in pregnancy is rare, with only a few cases being reported in the world literature. Prognosis in GDM
Recurrence of GDM
Given that most of the risk factors for GDM persist or become worse in subsequent pregnancies, it is not surprising that the recurrence rate is high and ranges between 35% and 70%. The wide range of recurrence rate is in part due to various screening methods and different diagnostic threshold values for various GTTs. It is clear from the literature however that GDM in the index pregnancy increases both the risk of recurrence in subsequent pregnancies and also the risk of developing type 2 diabetes later in life (see box).
Risk factors for GDM and recurrence
Previous history of GDM
Previous diagnosis of GDM before 24 weeks
Insulin requirement in previous pregnancy
Previous GDM and weight gain of ≥15 lbs (6.8 kg) in between pregnancies
Previous GDM and interval between pregnancies of ≥24 months
Previous history of macrosomia (birthweight ≥9 lbs or 4.1 kg)
Previous history of adverse pregnancy outcome (not clearly attributable to a condition other than diabetes during pregnancy)
Ethnic group with an elevated risk of GDM and type 2 DM
First-degree relative with diabetes
Advanced maternal age
Obesity (BMI = 30–35 kg/m2)
Glucosuria
Conditions with insulin resistance, for example polycystic ovarian syndrome (PCOS)
Metabolic syndrome, which is defined by the presence of three or more of the following criteria:
Abdominal obesity (waist circumference >88 cm), elevated triglycerides (= 150 mg/dL), (HDL is also used by some women with type 1 diabetes, particularly those who have a hectic lifestyle and need maximum flexibility in their diet and insulin regimen. Modern pumps are small and lightweight and different basal rates can be set and boluses given as required. Potentially CSII maintains the basal rate of insulin and therefore reduces the risk of hypoglycaemia. However, patients with type 1 DM may become hyperglycaemic rapidly if there is pump failure or intercurrent infection. Of note, infection at infusion site is relatively rare. Research to date has not shown any significant difference in either maternal outcome (CS rate, mean HbA1c, hypo- or hyperglycaemia) or baby outcome (perinatal mortality rate, fetal anomaly, gestational age at delivery, and small for gestational age) between use of CSII and multiple dose injection (MDI). There was a significant increase in mean birthweight associated with CSII compared with MDI; however, there was no significant difference in macrosomia (birthweight >4000 g).
Diet therapy
A schedule consisting of three meals and several snacks is used in most patients. Diet should consist of 50–60% carbohydrate, 20% protein, and 25–30% fat with less than 10% saturated fats, up to 10% polyunsaturated fatty acid, and the remainder derived from a monounsaturated source. Caloric intake depends on prepregnancy weight and weight gain during gestation. Carbohydrate counting helps patient to determine appropriate insulin boluses for meals and snacks.
Role of oral antidiabetic agents in pregnancy
Recent research using oral antidiabetic agents (OAAs) in GDM and polycystic ovarian syndrome (PCOS) suggest that they are safe and often effective. Contrary to earlier fears, drugs such as glyburide do not increase above background the rates of major congenital malformations or neonatal deaths. Metformin has been associated with decreased rates of spontaneous miscarriage and GDM, and similar rates of pre-eclampsia, major birth defects, and similar birthweight compared with healthy controls. It has been hypothesized that type 2 women needing exceptionally high doses of insulin during pregnancy can be sensitized by using metformin, allowing a lower dose of insulin to be used. The recently published Metformin in Gestational Diabetes (MiG) trial, in which 751 women with GDM were randomly assigned at 20–33 weeks’ gestation to open treatment with metformin (with supplemental insulin if required) or insulin, concluded metformin (alone or with supplemental insulin) is not associated with increased perinatal complications compared with insulin, and that women preferred metformin to insulin treatment. Management of acute emergencies
Hypoglycaemia
Most pregnant patients with pre-existing diabetes are followed up with outpatient visits at 1–2-week intervals. However, an open-access policy should be in place, so that women should be able to call at any time with any concerns, but especially if hypoglycaemia (200 mg/dL). The risk of hypoglycaemia is particularly high at 10–15 weeks because of a relative increase in oestrogen, decreased carbohydrate intake due to nausea and vomiting or overly aggressive treatment of the patient when she first presents in pregnancy. The patient and her family members should be taught to manage hypoglycaemia: mild attacks respond to drinking a glass of milk or juice, and the more severe attacks may require glucagon injections. The patients should carry candy, crackers or glucose tablets to treat themselves in an emergency when away from home.
Diabetic ketoacidosis
With the implementation of antenatal programs DKA during pregnancy has fortunately become an uncommon event, estimated at 1–2 % in women using insulin. The occurrence of DKA in GDM is extremely rare and its occurrence strongly suggests the possibility of pre-existing but undiagnosed type 1 diabetes.
The true incidence of maternal mortality in DKA is unknown although historically reported at 5–15%. Fetal loss rates are much higher and vary widely between 35% and 85%, although more recent research has reported loss rates as low as 9%.
Comprehensive details of the management of DKA are beyond the scope of this chapter. Suffice to say that this should be a multidisciplinary effort mounted on an ICU in the first instance. Although DKA represents a substantial risk to the fetus, even if late decelerations are present on cardiotocography, the aim should be to correct maternal acidosis because the fetus usually recovers with the correction of maternal acidosis.
Fetal surveillance
All women should have early booking and an early dating scan as documentation of viability is essential due to high rates of miscarriages, especially in women with poor glycaemic control. They should be offered a 11–13-week nuchal translucency scan and a detailed anomaly scan in the second trimester, as well as a cardiac scan at 22 weeks’ gestation, preferably performed by a fetal cardiologist or sonoligist with appropriate expertise. Careful attention should be given to the evaluation of the great vessels.
In the third trimester evaluation of fetal growth and well-being are the mainstays in evaluating pregnancies complicated by diabetes. Accelerated fetal growth has been associated with a significant risk of fetal mortality. The limitations of ultrasound in consistently diagnosing and evaluating fetal macrosomia must, however, be recognized.
Other tests of fetal wellbeing include maternal monitoring of fetal movements, cardiotocography, biophysical profile, and umbilical artery Doppler flow studies. All add to the increased fetal surveillance that is required for women with DM, although efficacy is often doubtful. Management of mother and baby around delivery
Controlling maternal blood glucose over the few hours before delivery is crucial to reduce the risk of neonatal hypoglycaemia. Blood glucose concentration of 4–8 mmol/L should be the target, and usually best achieved using glucose and insulin infusion. As soon as the cord is cut the rate of infusion should be halved as insulin sensitivity returns to normal within minutes of shut down of the uteroplacental circulation. Subcutaneous insulin administration can be resumed as soon as the mother is able to eat.
Table 8.11.3 Stillbirth, perinatal mortality rate and neonatal death in type 1 and type 2 diabetes

If the baby’s blood glucose is checked too early in life, then it almost certainly will be low as 5% of babies of non-diabetic women have blood glucose concentrations of less than 1.7 mmol/L within 2 hours of life. If blood glucose is checked too early then the baby will unnecessarily be sent to the special care baby unit: to avoid this, early feeding should be strongly encouraged and the blood glucose checked only before the second feed. This will decrease the mother–baby separation rates as two-thirds of the separations are potentially avoidable. Blood glucose should however be checked if hypoglycaemia is suspected. These babies are also at risk of hyperbilirubinaemia, respiratory distress syndrome, asphyxia and injuries such as those associated with shoulder dystocia. It is highly recommended that all units have a written policy for care of infants of mothers with diabetes.
Timing and mode of delivery
Two arguments have been put forward for delivery of an infant of a diabetic mother 1–2 weeks before term. The first is the avoidance of unexpected fetal demise, and the second is avoidance of fetal trauma accompanying the vaginal delivery of a large infant. However, there is remarkably little hard research on the issue of the mode and timing of delivery in pregnancies complicated by DM. NICE have recommended the following with regard to timing and mode of delivery: (i) pregnant women with diabetes who have a normally grown fetus should be offered elective birth through induction of labour, or by elective Caesarean section if indicated, after 38 completed weeks; (ii) diabetes should not in itself be considered a contraindication to attempting vaginal birth after a previous Caesarean section; (iii) pregnant women with diabetes who have an ultrasound-diagnosed macrosomic fetus should be informed of the risks and benefits of vaginal birth, induction of labour and caesarean section.
Management of GDM
The management goals in GDM are similar to those of preexisting diabetes. The first step is usually dietary and exercise advice. If diet and exercise fail to achieve the target levels of glucose, insulin therapy should be commenced. Therapy should also be considered if there is ultrasound evidence of fetal macrosomia.
With regard to OAAs, metformin is the logical choice in GDM where insulin resistance seems to be the main problem. The findings of the MiG trial have provided an evidence base for the use of metformin in GDM.
If there is satisfactory glycaemic control, pregnancy can be allowed to progress until 40 weeks. Women who need insulin/metformin are usually induced at 40 weeks, ostensibly to reduce the risk of macrosomia and/or unexplained stillbirth, but the evidence for either is at best tenuous. Women who do not need any medical intervention and are controlled by diet alone can be safely managed as other low-risk non-GDM women. Following delivery insulin or metformin can be stopped immediately, and glucose monitoring can stop after the establishment of normal fasting glucose levels. All women with GDM should be followed up with an OGTT (usually 75 g, but centres in the USA mostly use 100 g) performed 6 weeks postpartum.
Postpartum care and education
Women with type 1 diabetes often require very little insulin during the first 24–72 hours after delivery, and insulin dosing is best achieved by continuation of the sliding scale. Women with type 2 diabetes often have adequate glycaemic control following delivery and may not require any medical intervention for a while. If resumption of OAAs is necessary, glyburide, glipizide, or metformin have been shown to have little or no transfer into the breast milk and can be prescribed to breast feeding women.
Dietary counselling should also take place and the general guideline for caloric intake are about 25 kcal/kg/day in nonbreastfeeding and 27–30 kcal/kg/day in breastfeeding women.
Exclusive breastfeeding is strongly recommended for the first 6 months of life, although this is not always achievable. The offspring of diabetic mothers are at increased risk of childhood obesity and type 2 diabetes later in life. Breastfed infants appear to be at lower risk of both. A delayed introduction of formula milk also appears to be protective of β-cell autoimmunity and later risk of type 1 diabetes. In GDM, evidence also suggests that women who breastfeed are themselves protected against the later development of type 2 diabetes.
In women with pre-existing diabetes the ABCs of diabetes should be stressed: A1c (controlling glucose), B (blood pressure), C (cholesterol). All these go a long way in preventing long-term complications of diabetes, especially the microvascular complications. Use of ACE inhibitors in these women is thought to be renoprotective.
Reproductive health and contraception during the postpartum period
Exclusive breastfeeding provides contraception via lactational amenorrhoea, and this can be enhanced with the use of condoms. For those desiring hormonal contraception, reassurance should be given that less than 1% of the dose is transferred in breast milk. Progestin-only methods, which can be started on day 21 postpartum, are preferred as there is no demonstrable effect on the volume of milk secretion. The use of combined oral contraceptives (COCs) should be withheld until 6 weeks postpartum because of the risk of thromboembolism, and then only in non-breastfeeding women. The short-term use of low-dose COCs and progestin-only OCs seem to have minimal metabolic effects, but data on long-term effects are lacking. In women with GDM COCs do not seem to have either short-term or long-term adverse metabolic effects or increase the risk of developing diabetes. Progestin-only OCs however appear to increase the risk of developing diabetes almost by threefold. It is therefore recommended that the lowest dose and potency progestin and oestrogen combination OC be selected to minimize glucose intolerance and adverse effect on lipid metabolism and blood pressure. Intrauterine devices can be used safely in women with diabetes without increasing the risk of pelvic inflammatory diseases. When used, the insertion should be delayed by at least 4 weeks postpartum, although copper medicated devices can be inserted 48 hours postpartum. Further reading
Crowther CA, Hiller JE, Moss JR, et al. Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med. 2005; 352:2477–86.
Hillier TA, Vesco KK, Pedula KL, et al. Screening for gestational diabetes mellitus: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2008;148:766–75.
Hunt K, Schuller K. The increasing prevalence of diabetes in pregnancy. Obstet Gynecol Clin N Am 2007;34:173–99.
Metzer BE, Lowel LP, Dyer AR, et al. The HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008;358:1991–2002.
Nice Clinical Guideline 8. Diabetes in pregnancy: management of diabetes and its complications from the preconception to the postnatal period; March 2008. http://www.nice.org.uk
Reece EA, Eriksson UJ. Congenital malformations: epidemiology, pathogenesis and experimental methods of induction and prevention. In: Reece EA, Coustan DR, Gabbe SG (eds) Diabetes in women: adolescence, pregnancy and menopause, 3rd edn. Philadelphia: Lippincott Williams & Wilkins Philadelphia 2004:169–204.
Rowan JA, Hague WM, Gao W, et al, for the MiG Trial Investigators. Metformin versus insulin for the treatment of gestational diabetes. N Engl J Med 2008;358:2003–15.
World Health Organization. Definition and diagnosis of Diabetes Mellitus and intermediate Hyperglycemia. Report of a WHO/IDF consultation. Geneva: WHO 2006.
Drugs in pregnancy
Pharmacological agents are not necessary during pregnancy; however, some women go through pregnancy with medical conditions that need continuing or episodic treatment (e.g. asthma, epilepsy, and hypertension). During pregnancy new medical problems may develop or the old ones can aggravate (e.g. migraine headaches), requiring pharmacological therapy. Drugs given in pregnancy can adversely affect the fetus in many ways. Studies have shown that many pregnant women use either prescribed or over-the-counter medications during pregnancy (Bonati et al. 1990; Lacroix 2000). A comparison of therapeutic drug use in pregnancy across Europe showed that 64% of women used at least one drug during pregnancy (De Vigan 1999), while in France, pregnant women were prescribed an average of five drugs during the first trimester (Lacroix 2000). In the UK about a third of women take pharmacological agents at least once in pregnancy, but only 6% take these agents in the first trimester (Moore 1988). In puerperium, the use of drugs increases substantially, with no difference in the pattern of prescribing between mothers who breastfeed and those who bottlefeed. Although most doctors are cautious with medication use in their pregnant patients, it is estimated that at least 10% of birth defects are attributed to maternal drug exposure in pregnancy. Drug metabolism in pregnancy
The safety and efficacy of drugs for a dosage regimen is established by Phase 3 clinical trials, involving typical representatives from the target patient population. Pregnant women and those who fall pregnant during the trial are excluded from these studies. Thus, at a drug’s first marketing, except for products developed to treat conditions specific to pregnancy (e.g. oxytocics, cervical ripening agents), there are seldom human data on the proper dosage and frequency of administration during pregnancy. The placenta is a relative lipid barrier between the maternal and fetal circulation and most drugs cross the placenta by passive diffusion. The practical view to take on prescribing drugs in pregnancy is that transfer of drugs to the fetus is unavoidable. Low-molecular-weight, lipid-soluble, and unionized drugs cross the placenta more readily than polar drugs. There are several physiological changes during pregnancy that have a marked impact on pharmacokinetics and hence some of the established therapeutic ranges might be inappropriate.
Based on all the evidence available about congenital abnormalities and its association with the drugs, the FDA has divided the drugs into different categories (Table 8.12.1).
In this section we aim to provide a quick reference guide for drug use in pregnancy. The drugs here listed here are in groups according to how they appear in the WHO 11th model list of essential drugs.
General anaesthetics
Intravenous anaesthetics induce anaesthesia rapidly and commonly used drugs are thiopentone and Propofol (risk factor B). Propofol has not been used during the first and second trimesters in humans. Reproduction studies in rats and rabbits at doses six times the recommended human induction dose revealed no evidence of impaired fertility or fetal harm.
Inhalational anaesthetics commonly used are halothane and nitric oxide. A collaborative perinatal project showed no embryonic or fetal effects of nitric oxide. Its use during delivery will lead to neonatal depression and fetal accumulation of nitric oxide, which increases over time; therefore, it is safer to keep the induction to delivery time as short as possible.
Table 8.12.1 US FDA pregnancy category definitions

Neuromuscular blocking agents
These agents are used in adjunct to anaesthetics to provide muscle relaxation. Succinyl choline (risk factor C) is the only depolarizing agent used. The Collaborative Perinatal Project recorded 50 282 mother–child pairs, 26 of whom had first trimester exposure to succinylcholine. No congenital malformations were observed in any of the newborns.
Non-opioid analgesics and antipyretics and non-steroidal anti-inflammatory drugs
Aspirin (Risk Factor C) and non-steroidal anti-inflammatory drugs (NSAIDs) do not produce structural defects. Salicylates (in analgesic doses) and NSAIDs may increase the risk of neonatal haemorrhage by inhibition of platelet function. NSAIDs may also lead to oligohydramnios by its effect on the fetal kidney. The use of NSAIDs in the last trimester causes premature closure of the ductus arteriosus, leading to neonatal primary hypertension. Both premature closure of the ductus and the oligohydramnios are reversible. If used during pregnancy, they should be discontinued at least 6–8 weeks before delivery.
Opioid analgesics
In a surveillance study of Michigan Medicaid recipients 375 (4.9%) major birth defects were noted (325 expected). Specific data were available for six defect categories, including (observed/expected) 74/76 cardiovascular defects, 14/13 oral clefts, 4/4 spina bifida, 25/22 polydactyly, 15/13 limb reduction defects, and 14/18 hypospadias. Only with the total number of defects is there a suggestion of an association between codeine and congenital defects, but other reasons, including the mother’s disease, concurrent drug use, and chance may be involved. In an investigation of 1427 malformed newborns compared with 3001 controls, first trimester use of narcotic analgesics (codeine (risk factor C) most common) is associated with inguinal hernias, cardiac and circulatory defects, cleft lip and palate, dislocated hip, and other musculoskeletal defects. Alimentary tract defects occur when used in the second trimester. The data serve as a possible warning that indiscriminate use of codeine may present a risk to the fetus. Use of codeine during labour produces neonatal respiratory depression to the same degree as other narcotic analgesics. Neonatal codeine withdrawal has also been reported.
Disease modifying agents of rheumatic disorders
• Sulphasalazine (risk factor B): no increase in human congenital defects or newborn toxicity has been observed from its use in pregnancy. Milk concentrations were roughly 40–60% of maternal serum levels. Bloody diarrhoea in an infant only breastfed was attributed to the mother’s sulphasalazine therapy (3 g/day). Cautious use of sulphasalazine in nursing women because of significant adverse effects in some nursing infants is recommended.
• Cyclophosphamide (risk factor D): various abnormalities ranging from karyotyping abnormalities to multiple structural anomalies have been described with the use of cyclophosphamide in first trimester. Use of cyclophosphamide in the second and third trimesters does not place the fetus at risk for congenital defects. Except in a few individual cases, long-term studies of growth and mental development in offspring exposed to cyclophosphamide during the second trimester, the period of neuroblast multiplication, have not been conducted. Cyclophosphamide is contraindicated during breastfeeding because of the reported case of neutropenia and because of the potential adverse effects of immune suppression, growth, and carcinogenesis. Anticonvulsants/antiepileptics (risk factor D)
Phenytoin, primidone, phenobarbitone, carbamazepine, and sodium valproate all cross the placenta and are teratogenic. The major abnormalities produced by anticonvulsants are neural tube, orofacial, and congenital heart defects. The neural tube defects are mainly caused by sodium valproate (1–2%) and carbamazepine (0.5–1%). Orofacial defects are mainly from phenytoin, which also produces the fetal hydantoin syndrome.
The risk for any single drug is about 6–7% (i.e. double to three times the background level). The risk increases with the multiple drugs. Patients on two or more anticonvulsants the risk is 15%, and for those taking combinations of valproate, carbamazepine, and phenytoin the risk is as high as 50%. The risk of neural tube defects may be decreased with preconceptual and first trimester folic acid (5 mg). The newer anticonvulsant drugs vigabatrin, lamotrogine, topiramate, and gabapentin are often prescribed in combination with other anticonvulsants and it is therefore difficult to ascertain the teratogenic risk of these drugs in isolation. Monotherapy should be used wherever possible and special care should be taken to keep the dose as low as is compatible with seizure prophylaxis. The traditional anticonvulsants, such as phenytoin, carbamazepine, and valproic acid are considered safe for use during breastfeeding; however, observation for adverse effects such as drowsiness is recommended for women receiving high doses.
Anti-helminthic—intestinal, anti-filarials, anti-schistosmals, anti-trematode drugs
• Mebendazole(risk factor C): it has been found to be embryotoxic and teratogenic in rats and is therefore not recommended for use during pregnancy.
• Albendazole (risk factor C): observation of limb reduction defects at all doses in one animal study and limited human pregnancy data suggest that Albendazole during pregnancy is not recommended. There is no data on the safety of albendazole in breastfeeding.
Antibacterials
• Tetracycline (risk factor D): tetracycline is contraindicated during pregnancy. This broad-spectrum antibiotic crosses the placenta, chelates with calcium and is deposited in the developing teeth and bones of the fetus. Staining of the permanent teeth is most likely when tetracyclines are administered after 24 weeks’ gestation.
• Ciprofloxacin (risk factor C): quinolone treatment in developing adolescents of several animal species is associated with acute arthropathy of the weight-bearing joints. A recent study examining the effect of intrauterine exposure to quinolones on the fetus inferred that the use of the ciprofloxacin during the first trimester of pregnancy is not associated with an increased risk of malformations or musculoskeletal problems. Long-term follow up is required to exclude subtle cartilage and bone damage.
• Aminoglycosides: except for eighth cranial nerve damage, no reports of congenital defects caused by streptomycin have been found. The Collaborative Perinatal Project monitored 50 282 mother–child pairs, 135 of whom had first trimester exposure to streptomycin (risk factor D). For use any time during pregnancy, 355 exposures were recorded. In neither group was evidence found to suggest a relationship to large categories of major or minor malformations or to individual defects. Aminoglycoside antibiotics have no detectable teratogenic risk for structural defects. They also concluded that the risk of deafness after in utero aminoglycoside exposure was small. Streptomycin is compatible with breastfeeding.
• Chloramphenicol (risk factor C): it should be avoided in late pregnancy and during labour because of the potential for the ‘grey baby syndrome’ in the newborn infant. Therefore, it should only be used in pregnancy in life-threatening conditions, when no alternative is available.
• Nitrofurantoin (risk factor B): nitrofurantoin may be administered in pregnancy, but should be avoided near term. Low levels of glutathione may predispose the foetus to haemolytic anaemia if it is exposed to nitrofurantoin shortly before birth.
• Vancomycin (risk factor B): vancomycin is a bactericidal antibiotic with a fetal ototoxic effect. It should be avoided unless benefit outweighs potential risk.
• Trimethoprim (risk factor C): the use of trimethoprim in pregnancy was associated with an approximate quadrupling the risk of cardiovascular defects and/or an oral cleft. The risk was increased with use during the second and third months after the last menstrual period but not before or after this period. It is therefore advisable to avoid trimethoprim in the first trimester unless benefit outweighs potential risk and is always used with folic acid.
Antiprotozoal drugs (anti-amoebic and anti-malarial drugs)
• Metronidazole (risk factor B): most of the published evidence now suggest that metronidazole does not present a significant risk to the fetus. A possible small risk for cleft lip with or without palate has been reported, but the validity and the clinical significance of this finding is questionable. It is also not possible to assess the risk to the fetus from the potential carcinogenic potential of metronidazole. Metronidazole is contraindicated during the first trimester in patients with trichomoniasis or bacterial vaginosis.
• Chloroquine: chloroquine is not a major teratogen, but a small increase in birth defects cannot be excluded. The amount of chloroquine excreted into milk is not considered to be harmful to a nursing infant.
• Quinine (risk factor D): quinine has effectively been replaced by newer agents to treat malaria. Although no increased teratogenic risk can be documented, its use during pregnancy should be avoided. Quinine is compatible with breastfeeding.
Adrenocortical steroids
The adrenal cortex synthesizes two classes of steroids: the corticosteroids (glucocorticoids and mineralocorticoids) having 21 carbon atoms and the androgens, which have 19. Cortisone is the main glucocorticoid and aldosterone is the main mineralocorticoid. Glucocorticoids are administered in multiple formulations for disorders that share an inflammatory or immunological basis. Except in patients receiving replacement therapy for adrenal insufficiency, glucocorticoids are neither specific nor curative, but rather are palliative because of their anti-inflammatory and immunosuppressive actions.
• Prednisolone (risk factor C) is the biologically active form of prednisone. The placenta can oxidize prednisolone to inactive prednisone or even less active cortisone. The Michigan Medicaid surveillance study looked at 229 101 patients exposed to prednisolone, prednisone and methyl-prednisolone during the first trimester. These data do not support an association between the drugs and congenital defects. There are isolated reports of cataracts in the newborn if prednisolone was used throughout the pregnancy. At maternal doses of 20 mg the infant would be exposed to minimal amounts of steroid. At higher doses (>20 mg), it is recommended to wait at least 4 hours after a dose before nursing the baby.
• Betamethazone (risk factor C) use in preterm labour is associated with a decrease in respiratory distress syndrome, periventricular leucomalacia, and IVH in preterm infants. It can precipitate myasthaenic crisis in patients with myasthaenia gravis, induce hyperglycaemia, and, rarely, a hypertensive crisis. Single courses of betamethasone have no effects on the fetus but multiple courses of betamethasone have been associated with lower birthweights and reduced head circumference at birth. Follow-up studies have not shown any differences in cognitive and pscychosocial development when compared with controls.
• Hydrocortisone (risk factor C) and its inactive precursor, cortisone, present a small risk to the human fetus. These corticosteroids produce dose-related teratogenic and toxic effects in genetically susceptible experimental animals consist of cleft palate, cataracts, spontaneous abortion, IUGR, and polycystic kidney disease.
Although the large numbers of data support no effects in much of human pregnancies, adverse outcomes have been observed and may have been caused by corticosteroids. Moreover, the decrease in birthweight and a small increase in the incidence of cleft lip with or without cleft palate are supported by large epidemiological studies. Because the benefits of corticosteroids far outweigh the fetal risks, these agents should not be withheld if the mother’s condition requires their use. The mother, however, should be informed of the risks so she can actively participate in the decision on whether to use these agents during her pregnancy.
Immunosuppressive drugs
• Azathioprine (risk factor D): azathioprine is a 6-mercaptopurine derivative, which acts as a ‘steroid-sparing’ agent. Current evidence indicates that maternal use of azathioprine is not associated with an increased risk of impaired fetal immunity, growth restriction, and prematurity. There is no increase in congenital abnormalities or subsequent problems such as childhood malignancy in children followed for up to 20 years. There has been conflicting information on breastfeeding while taking azathioprine. Despite little or no drug being found in breast milk most rheumatologists advise avoidance of azathioprine if possible, or would counsel against breast-feeding because of theoretical risks of immune suppression of the neonate.
• Cyclosporin (risk factor C): based on relatively small numbers, the use of cyclosporine during pregnancy apparently does not pose a major risk to the fetus. No pattern of defects has emerged in the few newborns with anomalies. Skeletal defects, other than the single case of osseous malformation, have not been observed. Cyclosporine is contraindicated during breastfeeding due to the potential for immune suppression and neutropenia, an unknown effect on growth, and a possible association with carcinogenesis.
Anti-angina drugs
Nitroglycerin (risk factor B): the use of nitroglycerine during pregnancy does not seem to present a risk to the fetus. However, the number of women treated during pregnancy is limited, especially during the first trimester. With the smaller doses reported, transient decreases in the mother’s blood pressure may occur, but these do not appear to be sufficient to jeopardize placental perfusion. Nitroglycerin appears to be a safe, effective, rapid-onset, short-acting tocolytic agent. The use of transdermal nitroglycerine patches is also effective when longer periods of tocolysis are required.
Anti-arrhythmic drugs
Amiodarone (risk factor D) is an iodine-rich anti-arrhythmic drug with proven benefit in the treatment of patients with ventricular and atrial arrhythmias. It can reach the fetus by transplacental passage and induce fetal hypothyroidism. It inhibits the conversion of thyroxine to triiodothyronine in most tissues. It may also inhibit thyroid hormone synthesis and secretion, causing hypothyroidism in 5–25% of patients. There may be neurotoxicity associated with transplacental exposure to amiodarone. Amiodarone-exposed toddlers showed expressive language skills that were relatively poorer than verbal skills when compared with controls. One amiodarone-exposed toddler exhibited global developmental delay. Amiodarone exposed older children had well-developed social competence, favourable global IQ scores but had problems with reading comprehension, written language, and arithmetic. This picture is reminiscent of non-verbal learning disability syndrome. In another report, a normal psychomotor development was observed in two patients with full-scale IQ score, verbal, and performance IQ scores within normal range. These data need to be validated by larger studies. In conclusion, drug therapy with amiodarone should be avoided during the first trimester of pregnancy if possible and drugs with the longest record of safety should be used as first-line therapy. Conservative therapies should be used when appropriate.
Anti-hypertensive drugs
β-Adrenergic antagonists
β-Adrenergic antagonists have fewer side-effects than most antihypertensives, but their safety in pregnancy is not so well established. Some studies have found no adverse effects on the outcome of pregnancy while others have described a variety of foetal and neonatal complications. The concern is that if these drugs are used before 28 weeks’ gestation, they may increase the risk of intrauterine growth restriction. Later complications include bradycardia, hypotension, hypoglycaemia, and respiratory distress. However, many studies suggest that they are safe antihypertensives for use in the third trimester. If treatment of hypertension is required before 28 weeks, methyldopa should be the first drug of choice. Guidelines of the International Society for the Study of Hypertension in Pregnancy (ISSHP) do not recommend the use of oral β-adrenergic antagonists for mild hypertension in pregnancy.
Angiotensin converting enzyme inhibitors
These drugs have been associated with prolonged renal failure and hypotension in the newborn, decreased skull ossification, hypocalvaria, and renal tubular dysgenesis. In addition, there are several case reports of intrauterine growth restriction, oligohydramnios, patent ductus arteriosus, and neonatal hypotension. The use of these drugs in the first trimester is not thought to produce structural malformations, so it is acceptable to cease treatment early in pregnancy and not necessarily preconception.
Antithrombotic drugs
Warfarin (risk factor D)
Warfarin is a form of coumarin with vitamin K antagonist action. Its use in pregnancy is associated with a high incidence of fetal loss, congenital malformations, and physical disability. Exposure to the drug between the sixth and ninth weeks of gestation is associated with defective ossification of bone resulting in nasal hypoplasia and chondrodysplasia punctata. On a molecular level, vitamin K inhibitors may alter calcium binding for several proteins, affecting bone ossification causing the characteristic bony abnormalities of the ‘fetal warfarin’ syndrome. The use of warfarin in the second and third trimester is not without serious complications. The effects are mainly CNS abnormalities and are thought to be due to microhaemorrhages in the brain. The defects include dorsal midline dysplasia (agenesis of corpus callosum and Dandy-Walker malformations) or ventral midline dysplasia (optic atrophy), mental retardation, delayed development, seizures, and microcephaly. The risk of teratogenicity with warfarin has led to the recommendation that heparin should be substituted for the treatment and prophylaxis of venous thromboembolism. However, heparin is not as effective as warfarin in preventing arterial thromboembolism in women with artificial heart valves or mitral disease with atrial fibrillation. In these situations, the risk of thrombosis may exceed the risks of warfarin use, and warfarin therefore may be indicated. It should be used with great caution and close monitoring of both the mother and fetus.
Heparin (risk factor C)
This is the anticoagulant of choice from the fetal perspective, as it does not cross the placenta.
Thyroid hormone and other antithyroid drugs
• Propylthiouracil (risk factor D): in a surveillance study of Michigan Medicaid recipients involving 229 101 completed pregnancies conducted between 1985 and 1992, 35 newborns had been exposed to propylthiouracil (PTU) during the first trimester. One (2.9%) major birth defect was observed (one expected), a case of hypospadias (none expected). A 1992 abstract and a later full report described a retrospective evaluation of hyperthyroid pregnancy outcomes treated with either PTU (N = 99) or methimazole (N = 36). Three (3.0%) defects were observed in those exposed to PTU (ventricular septal defect, pulmonary stenosis, patent ductus arteriosus in a term infant), whereas one newborn (2.8%) had a defect (inguinal hernia) in the methimazole group. No scalp defects were observed. In comparison with other antithyroid drugs, propylthiouracil is considered the drug of choice for the medical treatment of hyperthyroidism during pregnancy. PTU is compatible with breastfeeding.
• Methimazole (risk factor D) and carbimazole (risk factor D): a specific pattern of rare congenital malformations secondary to exposure to methimazole during the first 7 weeks of gestation that consists of some or all of the following: scalp or patchy hair defects, choanal atresia, oesophageal atresia with tracheoesophageal fistula, minor facial anomalies, hypoplastic or absent nipples, and psychomotor delay is reported. These defects may indicate a phenotype for methimazole embryopathy. Because of the possible association with aplasia cutis and other malformations, and the passage of methimazole into breast milk, PTU is the drug of choice for the medical treatment of hyperthyroidism during pregnancy. Methimazole and carbimazole are compatible with breastfeeding. Psychotherapeutic drugs
Drugs used in psychotic disorders
Antipsychotic drugs: lithium (risk factor D)
It is estimated that 7.8% of lithium-exposed embryos develop abnormalities. Early data showed that the cardiovascular system is the most affected, with Ebstein anomaly affecting a third of the malformed babies. Although initial information regarding the teratogenic risk of lithium treatment was derived from biased retrospective reports, more recent epidemiological data indicate that the teratogenic risk of first trimester lithium exposure is lower than previously suggested. The clinical management of women with bipolar disorder who have childbearing potential should be modified with this revised risk estimate. If lithium is used for prophylaxis, it is advisable to discontinue it during the first trimester, unless its withdrawal would jeopardize the woman or the pregnancy. During pregnancy, the smallest dose possible for acceptable therapeutic effects should be used. Frequent small dosages should be used to avoid larger fluctuations in maternal plasma concentrations, and each dosage should not exceed 300 mg, with even spacing throughout the 24-hour period.
Drugs used in depressive disorders
Maternal depression in pregnancy can have deleterious effects on the neonate because of the potential for poor maternal weight gain or malnutrition. If supportive counselling is not adequate, tricyclic antidepressants and fluoxetine are the first-line choices in the management of depression. Tricyclic antidepressants have a long history of use without increasing teratogenic risk in pregnant women. Fluoxetine has been studied in prospective trials and no evidence for a higher incidence of malformations or other teratogenecity was found. Doses of tricyclic antidepressants may need to be higher in pregnancy due to increased hepatic metabolism. Where appropriate, to avoid withdrawal symptoms in the neonate, antidepressants should be slowly withdrawn or reduced to the minimum dose prior to delivery. Further reading
Banks BA, Cnaan A, Morgan MA, et al. Multiple courses of antenatal corticosteroids and outcome of premature neonates. North American Thyrotropin-Releasing Hormone Study Group. Am J Obstet Gynecol 1999; 181:709–17.
Bonati M, Bortolus R, Marchetti F, et al. Drug use in pregnancy: an overview of epidemiological (drug utilization) studies. Eur J Clin Pharmacol. 1990;38:325–8.
De Vigan C, De Walle HE, Cordier S, et al. Therapeutic drug use during pregnancy: a comparison in four European countries. OECM Working Group. Occupational Exposures and Congenital Anomalies. J Clin Epidemiol 1999;52:977–82.
French NP, Hagan R, Evans SF, et al. Repeated antenatal corticosteroids: size at birth and subsequent development. Am J Obstet Gynecol 1999;180:114–21.
Lacroix I, Damase-Michel C, Lapeyre-Mestre M, Montastruc JL. Prescription of drugs during pregnancy in France. Lancet 2000;356:1735–6.
MacArthur BA, Howie RN, Dezoete JA, Elkins J. Cognitive and psychosocial development of 4-year-old children whose mothers were treated antenatally with betamethasone. Pediatrics 1981;68:638–43.
MacArthur BA, Howie RN, Dezoete JA, Elkins J. School progress and cognitive development of 6-year-old children whose mothers were treated antenatally with betamethasone. Pediatrics 1982;70:99–105.
Moore K. The developing human: clinically oriented embryology, 4th edn. Philadelphia: WB Saunders 1988.
Schmand B, Neuvel J, Smolders-de Haas H, et al. Psychological development of children who were treated antenatally with corticosteroids to prevent respiratory distress syndrome. Pediatrics 1990;86:58–64.
Terrone DA, Rinehart BK, Rhodes PG, et al. Multiple courses of betamethasone to enhance fetal lung maturation do not suppress neonatal adrenal response. Am J Obstet Gynecol 1999;180:1349–53.
Epilepsy and other neurological conditions Epilepsy
Epilepsy is the most common chronic neurological disorder affecting 0.8% of the general population. Similar prevalence is given in pregnant women. The incidence of epilepsy is 0.05% and will be certainly lower in pregnancy as peaks of incidence are in childhood/adolescents and in older age.
Classification of epilepsy includes idiopathic generalized epilepsies (e.g. juvenile myoclonic epilepsy, juvenile absence epilepsy, epilepsy with grand mal at awakening), partial or focal epilepsies (e.g. malformations of cortical development, posttraumatic epilepsies), epilepsies with generalized and focal features and specific syndromes (e.g. reflex epilepsies, febrile convulsions, isolated seizures). Treatment of people with epilepsy should be tailored according to seizure type and epilepsy syndrome. A neurologist or epilepsy specialist should manage diagnosis and treatment of epilepsy.
Epilepsy and preconception advice
• All women in childbearing age on AEDs (anti-epileptic drugs) and with active sex life should be on folic acid 5 mg once daily to prevent folic acid-deficient induced spina bifida.
• Woman with epilepsy should consult their neurologist/epilepsy specialist for preconceptional advice.
• Women with epilepsy on AEDs should avoid falling pregnant unplanned.
Risks in pregnancy
• Teratogenic risk of AEDs
• Uncontrolled generalized tonic clonic seizures (GTCS) can induce fetal hypoxia/acidosis and five or more GTCS can reduce verbal IQ of fetus.
• Risk of traumatic fetal injury with maternal seizures
• Slightly increased maternal death rate in woman with epilepsy (3.8% of all maternal death).
• Risk of seizures during the 48 hours around delivery is 2%, indicating a 10-fold increase compared with any other 48-hour period in pregnancy.
Teratogenic effect of AEDs
AEDs have a teratogenic risk. Monotherapy with AEDs will have a lower risk then polytherapy. But uncontrolled generalized tonic clonic seizures are more hazardous to mother and fetus than AEDs.
Teratogenic risk for MCMs (major congenital malformations) for
• carbamazepine does not significantly differ from baseline
• lamotrigine is around 2.9% in low dose (400 mg/day). Within this figure is a particular risk of open cleft palates
• sodium valproate has a dose-dependent risk from 5.5% (1000 mg/day). Additionally, the risk for fetal valproate syndrome (abnormalities in face, developmental delay, occasionally major organ abnormalities and autistic traits). Recent studies suggest risk of reduced verbal IQ in children with maternal valproate exposure
• figures for other AEDs in pregnancy registers are statistically less valuable because of small patient groups. However, most AEDs seem to have a slightly increased risk for MCM. Some of the newer AEDs might be associated with a lower risk (levetiracetam) but sample sizes are still too small.
Although risks for MCMs with AEDs are thought to be an effect of exposure in the first trimester additional effects with valproate suggest vulnerability of fetus in all trimesters of pregnancy.
Peaks of AED serum levels will increase the risk for MCMs. To avoid serum level peaks, slow-release AED preparations in two or even three divided dosages should be suggested. It should be kept in mind that non-compliance (i.e. forgetting lunch time dose frequently) might increase the serum level oscillations and risk for seizures.
Genetic aspects
Children of mothers with epilepsy have a slight increased risk to develop epilepsy. This depends on the seizure syndrome and its aetiology. In maternal focal epilepsy the risk is about 3% compared with approximately 0.8% in the normal population. Idiopathic generalized epilepsies may have a higher risk for genetic predisposition (approximately 10%), in particular with positive family history.
Management
Most women with epilepsy will have no change of seizure frequency during pregnancy. Approximately 15% will have a reduction of seizure frequency and a similar percentage will have an increase in seizure frequency.
• Antenatal screening includes detailed high resolution ultrasound scanning to detect neural tube, cardiac and skeletal abnormalities.
• Serum levels of antiepileptic drugs might decrease during pregnancy with the increased liver and renal clearance. This is applicable in particular for Lamotrigine but might apply for other AEDs as well. AED dosages should be adjusted accordingly. Trough serum level control before pregnancy or during the first trimester might be helpful to ascertain a base line figure for further reference (regular serum level controls in e.g. lamotrigine and oxcarbazepine). This is of particular importance in women whose epilepsy is fully controlled.
• Folic acid 5 mg od during the first trimester at least.
• Inform/involve neurologist/epilepsy specialist.
• Advise women with epilepsy to continue AEDs regularly. In case of increased vomiting, AEDs should be taken again if vomiting occurs within 45 minutes after drug intake. Recurrent vomiting may reduce serum levels of AEDs.
• In case of hospital admission ensure that AEDs are continued without gap!
• In case of enzyme-inducing AED risk of haemorrhagic disease during delivery might be increased. Vitamin K prophylaxis 10 mg od should be given to mother for 4 weeks prior to delivery. (Enzyme inducing AEDs: carbamazepine, phenytoin, phenobarbital, primidone; to lesser extent: oxcarbazepine, topiramate, lamotrigine.)
• Home delivery is not recommended, but spontaneous delivery in the hospital environment is regarded as safe unless there are very frequent seizures.
• Pain relief during delivery can include epidurals, gas and air, TENS machine, which are regarded as safe for women with epilepsy. Pethidine and other opioids should be avoided if possible as they may trigger seizures in some patients.
• In case of seizure during delivery: Administer magnesium and 1–2 mg of lorazepam i.v. (2 mg with GTCS).
Postpartum management
All newborns should receive vitamin K prophylaxis post-partum to reduce the risk of haemorrhagic disease.
In case of AED dose increase during pregnancy, dosage of AED should be reduced to previous dosage within 3–4 weeks postpartum. However, should side-effects occur after delivery (particularly in women who had increase in lamotrigine dose) dosage should be readjusted more quickly, sometimes within a few days.
Advice for breastfeeding should be discussed prior to delivery with epilepsy nurse specialist or neurologist/epilepsy specialist. Concentration of some AEDs is higher in breast milk then in serum but in general breastfeeding in mother with AEDs is not restricted unless the newborn presents with side-effects, i.e. sedation and related feeding difficulties.
Contraception
Contraception should be discussed postpartum.
• Depot injections (Depo-provera) should be repeated every 10 weeks instead of 12.
• Standard strength combined oral contraceptive pill (COCP) will be safe with non-enzyme-inducing drugs (sodium valproate, levetiracetam, benzodiazepines, pregabaline, zonisamide, gabapentin, tiagabine, vigabatrin). Enzyme-inducing AEDs including carbamazepine, phenytoin, phenobarbital, and primidone require a higher dose COCP (50 μg or more of oestradiol) and/or tricyclic might be necessary. The safety might be still compromised. Breakthough bleeds would indicate reduced effectiveness of COCP. AEDs with lesser extent of enzyme induction (oxcarbazepine, topiramate particular >200 mg/day, and lamotrigine) are likely to affect the effectiveness of COCP as well. The same rules apply.
• COCP will reduce the plasma concentration of lamotrigine. Lamotrigine serum levels pre and post COCP are recommended. The lamotrigine dose should be increased by 50% when COCP is started. This is particularly important in women with full seizure control to avoid breakthrough seizures.
• Intrauterine devices (IUDs) with local hormone release (Mirena coil) have no interaction with AEDs.
• Progesterone-only pills and contraceptive implants are not recommended for women with epilepsy on AEDs.
• Other neurological conditions.
Most frequent other neurological conditions in pregnancy include migraine, peripheral nerve compression syndromes (e.g. carpal tunnel syndrome), reversible posterior leucoencephalopathy, sinus venous thrombosis, and multiple sclerosis. Eclampsia and pre-eclampsia are discussed in section 9.10.
Migraine
Migraine without aura tends to reduce in frequency during pregnancy, particularly after the first trimester. Migraine with aura is more likely to continue during pregnancy and it rarely gets worse. Some patients might present with aura only, and do not develop the typical headaches. Aura would usually present with the same symptoms as previously. New onset migraine presenting during pregnancy is rare but it is more likely to be with aura. Caution is advised as symptoms can be similar to eclampsia.
Postpartum headache occurs in 34% of women 3–6 days postpartum. It is more common in women with migraine. The headache usually presents slightly differently, bifrontal, less severe than migraine with nausea and vomiting. If the headache is disabling and there are no contraindications (e.g. coronary or cerebrovascular disease), subcutaneous sumatriptan injection is the treatment of choice even for breastfeeding women.
Management
• Migraine attacks should be treated with paracetamol 1000 mg orally. If necessary some antiemetic should be added (e.g. chlorpromazine or prochlorperazine).
• Sumatriptan has not shown to cause a significant increase of birth defects in more then 500 patients suggesting that it does not carry a risk for mother or fetus.
• Prophylactic medication should be avoided but if necessary, low dose propanolol might be helpful.
Peripheral nerve compression syndromes
Peripheral nerves might be compressed due to changes of connective tissue in pregnancy. Most commonly this presents with a carpal tunnel syndrome (CTS) causing tingling and pains (often nocturnal) in hand/wrist or even in the upper arm. Referral to neurology clinic for nerve conduction studies is advised. Treatment of CTS during pregnancy includes splint at night in neutral position or in severe cases decompressive surgery. However, it should be kept in mind that most CTS reverse spontaneously after delivery.
Reversible posterior leucoencephalopathy
This is a rare condition presenting late in pregnancy or puerperium. It is often associated with high blood pressure, although this might be a very moderate increase.
Clinically it presents with headaches and frequently visual symptoms including visual field defects up to hemianopia or anopia, possibly also agitation, dys-or aphasia, hallucinations and other cognitive disturbance.
Management
• Urgent neurology review
• Urgent MRI brain with DWI and MRV
• Control blood pressure!
• Symptomatic treatment of headache and other symptoms (e.g. hallucinations) if necessary.
Diagnosis is made by clinical picture and MRI result (posterior vasogenic oedema). Prognosis is good and syndrome is usually fully reversible.
Sinus venous thrombosis
This is a rare condition but slightly more prone to occur in women in pregnancy or puerperium due to activation of coagulation.
Clinical symptoms might present in an acute (within hours), subacute (within days or weeks) or rarely in a hyperacute fashion (thunderclap headache). Symptoms might include headaches, seizures, nausea and vomiting, alteration in consciousness level, paresis, aphasia, ataxia, and potentially other neurological signs depending on its location.
Management
• Urgent neurological review
• Urgent MRI with DWI and MRV (contrast CT brain: delta sign, i.e. rim of contrast around thrombus in posterior sagittal sinus only in 20% of cases positive)
• If diagnosis is confirmed, anticoagulation with heparin (aPTT twice the baseline but >120 seconds) even if haemorrhage on scan. Anticoagulation to be continued on warfarin for 6 months.
• AED during the acute phase of disease (e.g. clobazam) for up to 6 months maximum. No phenytoin (increases thrombophlebitis risk).
• Symptomatic treatment of headache.
No clear figures are at hand but prognosis seems to be better in women in pregnancy or puerperium than other aetiologies of sinus venous thrombosis. In one study 80% showed good outcome, but mortality was 9% in the pregnant patient group compared with up to 33% in all other cases.
Multiple sclerosis
Pregnancy in MS is safe. Particularly during the third trimester relapse rate will reduce but might rise in the first 3 months postpartum. However, only 28% of women with MS will suffer a relapse in this period. Higher the prepregnancy relapse rate and relapse during pregnancy might increase the risk for postpartum relapse. In the long-term pregnancy will have no impact on disability outcome.
Management
• Disease-modifying treatment should be stopped at least 3 months prior to conceiving.
• During pregnancy MS symptoms such as fatigue or incontinence might increase. Patients should seek advice from neurology or urology services.
• Spontaneous delivery is most often appropriate.
• Epidural or anaesthesia for Caesarean section is safe. Further reading
Cantu C and Barinagarrementeria F. Cerebral venous thrombosis associated with pregnancy and puerperium. Review of 67 cases. Stroke 1993;24:1880–4.
EURAP Study Group. Seizure control and treatment in pregnancy: observations from the EURAP epilepsy pregnancy registry. Neurology 2006;66:354–560.
Goadsby PJ, Goldberg J, Silberstein SD. Migraine in pregnancy. BMJ 2008;336:1502–4.
Hinchey J, Chaves C, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996;334: 494–500.
Kimber J. Cerebral venous sinus thrombosis. QJM 2002:95: 137–42.
Morrow J, Russell A, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. J Neurol Neurosurg Psychiatry 2006;77:193–8.
NICE guidelines CG20: The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care. October 2004. www.nice.org.uk/Guidance/CG20
Vukusic S, Hutchinson M, et al. Pregnancy and multiple sclerosis (the PRIMS study): clinical predictors of post-partum relapse. Brain 2004;127:1353–60. Useful websites
www.epilepsynse.org.uk
www.epilepsyandpregnancy.co.uk
www.migrainetrust.org
www.mssociety.org.uk
Gonorrhoea Definition
Gonorrhoea is a sexually transmitted infection caused by Neisseria gonorrhoeae, a gram-negative diplococcus. Epidemiology
Gonorrhoea is spread by contact with the penis, vagina, mouth, or anus. In the USA, approximately 700 000 new cases occur each year. In 2006, the rate of reported gonorrhoeal infections was 120.9 per 100 000 persons in the USA, but only half of cases are reported. In the UK, there were 18 710 new cases in 2007; cases of uncomplicated gonorrhoea increased by 42% between 1998 and 2007. Approximately one-third of UK cases are in women. In the USA, slightly more cases are reported in women than in men. In women attending selected prenatal clinics in 20 states, Puerto Rico, and the Virgin Islands, the median gonorrhoea positivity was 1.0% (range 0.0–3.2%)
Risk factors
• Younger age (funded four randomized trials of EPT by PDPT. Both clinical and behavioural outcomes of the available studies indicate that EPT is a useful option to facilitate partner management among heterosexual men and women with gonorrhoea or chlamydia. Pregnant women were not separately analysed in these trials, but because of the potential adverse effects of gonococcal or chlamydial infection on the course of pregnancy and neonatal health, preventing reinfection may have a higher priority than in non-pregnant women. Thus it is reasonable to use EPT by PDPT in a population of pregnant women.
In some jurisdictions, EPT by PDPT may not be legal. Some jurisdictions require an examination of a patient before any treatment can be given, thus making EPT by PDPT illegal. Other jurisdictions specifically allow the practice. Further reading
Centers for Disease Control and Prevention (CDCP). Sexually Transmitted Disease Surveillance 2006 Supplement, Gonococcal Isolate Surveillance Project (GISP) Annual Report 2006. Atlanta: US Department of Health and Human Services, CDCP 2008.
Centers for Disease Control and Prevention. Sexually transmitted diseases. Treatment Guidelines 2006. MMWR, 2006;55 (No.RR-11).
Centers for Disease Control and Prevention. Expedited partner therapy in the management of sexually transmitted diseases. Atlanta: US Department of Health and Human Services 2006.
Centers for Disease Control and Prevention. Update to CDC’s sexually transmitted diseases treatment guidelines, 2006: fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR, 2007;56:332–6.
Health Protection Agency. All new episodes seen at GUM clinics: 1998-2007. United Kingdom and country specific tables. London: Health Protection Agency 2008. Internet resources
Centers for Disease Control: www.cdc.gov; www.cdc.gov/STD/treatment/
Planned Parenthood Federation of America: www.planned-parenthood.org
National Institute of Allergy and Infectious Diseases www.niaid.nih.gov/publications/stds.htm Patient resources
CDC-INFO Contact Center, 1-800-CDC-INFO (1-800-232-4636), Email: cdcinfo@cdc.gov
American Social Health Association (ASHA), 1-800-783-9877: www.ashastd.org
National Women’s Health Information Center, 1-800-994-9662 Perinatal group B streptococcus Background
Group B streptococcus (GBS) emerged in the 1970s as the leading cause of neonatal sepsis, and also as an important cause of maternal septicaemia and uterine infection. Approximately 20–30% of pregnant women are GBS carriers, with higher rates of colonization in Black than in White or Asian women (Regan et al. 1991). Early clinical trials showed that intravenous penicillin or ampicillin administered during labour was effective in preventing neonatal disease (Boyer and Gotoff 1986), in contrast to antenatal treatment to eradicate GBS genital colonization before labour (Hall et al. 1976; Gardner 1979). There are no efficacy data to assess oral or intramuscular antibiotic prophylaxis during labour. Available data on oral penicillin, ampicillin (Merenstein et al. 1980), erythromycin (Klebanoff et al. 19995), and long-acting benzathine penicillin (Weeks et al. 1997; Bland et al. 2000), administered for 1 or more weeks in pregnancy, show that 20–30% of women were still colonized at the time of delivery. Prevention of early onset neonatal GBS disease
There are two competing strategies for the prevention of early-onset neonatal GBS infection, namely a cheaper and relatively less effective monitoring of women for known obstetric risk factors (intrapartum fever (20% of GBS positive women), preterm labour, prolonged rupture of membranes (ˇ18 hours), GBS bacteriuria, previously affected infant and isolation of GBS at any other time), and a culture-based screening of all women before labour (35–37 weeks in practice) to identify those colonized with GBS. The first national consensus guidelines in the USA in 1996 presented both approaches as equally acceptable, and their implementation resulted in a 70% reduction in the incidence of invasive neonatal GBS disease (from 1.5–2 cases/1000 live births to 0.5 cases/1000 live births) (MMWR 2000). A subsequent large retrospective cohort study showed that late antenatal culture-based screening was over 50% more effective in reducing the GBS attack rate than the alternative risk-based approach (Schrag et al. 2002a), leading to the adoption of a single prevention strategy, namely universal antenatal culture-based screening at 35–37 weeks of gestation (Schrag et al. 2002b). This improvement may be related to the detection on culture and intrapartum treatment of the 20% of colonized women who do not display any risk factors. For optimal detection rates (up to 27%) a rectovaginal or vaginal/perianal swab inoculated into a selective medium was recommended. In addition, women who have had a previously affected infant, GBS bacteriuria, or unknown GBS status were also eligible to receive intrapartum antibiotic prophylaxis. Intrapartum antibiotic prophylaxis
The recommended regimens for intrapartum antibiotic prophylaxis included Penicillin G, 5 million units i.v. initially, then 2.5 million units i.v. every 4 hours until delivery or alternatively Ampicillin 2 g i.v. initially, then 1 g i.v. every 4 hours until delivery. Patients who are allergic to penicillin but not at risk of anaphylaxis should receive cefazolin 2 g i.v. initially, then 1 g i.v. every 4 hours until delivery, or either clindamycin 900 mg i.v. every 8 hours or erythromycin 500 mg i.v. every 6 hours until delivery, if they were at risk of anaphylaxis. If the GBS was found to be resistant to clindamycin or erythromycin or the susceptibility was unknown, vancomycin 1 g i.v. every 12 hours until delivery should be given.
In the UK, the risk-based approach is adopted by most units with approximately 55% reduction in the incidence of invasive neonatal GBS disease. It is important to recognize that the baseline incidence of early-onset GBS disease in the UK is estimated at 0.5–1.15/1000 live births (Beardsall et al. 2000) in contrast to the 1.5–2.5/1000 rate in the USA prior to the introduction of mass screening in late pregnancy. Introduction of US-style mass screening for the prevention of early-onset disease in the UK may not be appropriate or cost-effective. The current UK NICE guidelines on intrapartum care do not recommend intrapartum antibiotic prophylaxis for women with prolonged rupture of membranes ˇ24 hours or their babies, if there is no evidence of infection such as pyrexia in labour (http://www.nice.org.uk/CG55). This deviates significantly from current understanding of the risk factor-based approach to prevention of neonatal GBS sepsis, particularly as 20% of colonized women do not display any risk factors. Emergence of resistant organisms
At present, GBS remain universally sensitive to penicillin and the narrow spectrum of activity exhibited by penicillin G (preferred over ampicillin for intrapartum antibiotic prophylaxis) drive the continuing belief that there is less selective pressure for the emergence of resistant organisms. However, recent studies have shown that both intrapartum benzylpenicillin and ampicillin were associated with a 35% increase in vaginal colonization with ampicillin-resistant Enterobacteria species, 36 hours postpartum (Moore et al. 2003). One large study found a significant increase in the rate of early-onset Escherichia coli sepsis, although this was restricted to low-birthweight neonates (Stoll et al. 2002), and the total gram-negative bacterial sepsis declined despite the increase in E. coli infections. Other studies report stable or declining rates of non-GBS sepsis.
The risk of life-threatening maternal anaphylactic reactions to penicillin or cephalosporin is very low but increased use of intrapartum antibiotics is expected to lead to more neonatal testing. Some clinicians assume that clindamycin or erythromycin is automatically effective as prophylaxis for GBS in women who are sensitive to penicillin. This is not necessarily so as some 4% and 11% of GBS are resistant to clindamycin and erythromycin respectively. Clinicians should request sensitivity studies when taking samples for possible GBS colonization from women that volunteer a history of penicillin allergy. Late-onset neonatal disease
Intrapartum antibiotic prophylaxis to prevent early-onset neonatal GBS disease does not modify the risk of acquisition of late-onset disease. This is because at least 50% of late-onset disease is due to nosocomial spread from other infants, hospital staff, or other adults. Not surprisingly, the dramatic reduction in the incidence of early-onset disease in the USA has at least in some parts, led to the emergence of the late-onset disease as the more common variant. At present, no preventive intervention has been identified, mostly because of the low baseline incidence rate of late-onset disease (0.5/1000 live births) and the much longer period of acquisition required in comparison to the early-onset disease.
Group B streptococci and preterm birth or low birthweight
There is some evidence those women who have heavy lower genital tract colonization with GBS have a significant, albeit small, risk of delivery of a low birthweight infant (OR 1.2, 95% CI 1.01–1.5) (Regan et al. 1996) but do not have an increased risk of other adverse outcomes including preterm birth. Other studies have not confirmed these findings. The 2002 CDC guidelines therefore recommend not treating GBS-colonized women antepartum, because it has no benefit and will expose a large number of women to unnecessary antibiotics. Further reading
Beardsall K, Thompson MH, Mulla RJ. Neonatal group B streptococcal infection in South Bedfordshire, 1993–1998. Arch Dis Child Fetal Neonatal Ed 2000;82:F205–7.
Bland ML, Vermillion ST, Soper DE. Late third-trimester treatment of rectovaginal group B streptococci with benzathine penicillin G. Am J Obstet Gynecol 2000;183:372–6.
Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. N Engl J Med 1986;314:1665–9.
Gardner SE, Yow MD, Leeds LJ, et al. Failure of penicillin to eradicate group B streptococcal colonisation in the pregnant woman. A couple study. Am J Obstet Gynecol 1979;135:1062–5.
Hall RT, Barnes W, Krishnan L, et al. Antibiotic treatment of parturient women colonized with group B streptococci. Am J Obstet Gynecol 1976;124:630–4.
Klebanoff MA, Regan JA, Rao AV, et al. Outcome of the Vaginal Infections and Prematurity Study: results of a clinical trial of erythromycin among pregnant women colonised with group B streptococci. Am J Obstet Gynecol 1995;172:1540–5.
Merenstein GB, Todd WA, Brown G, et al. Group B beta-hemolytic streptococcus: randomised controlled treatment study at term. Obstet Gynecol 1980;55:315–18.
MMWR Early onset group B streptococcal disease, US 1998–1999. MMWR 2000;49:793–6.
Moore MR, Schrag SJ, Schuchat A. Effects of intrapartum antimicrobial prophylaxis for prevention of group-B-streptococcal disease on the incidence and ecology of early-onset neonatal sepsis. Lancet Infect Dis 2003;3:201–13.
Regan JA, Klebanoff MA, Nugent RP. The epidemiology of group B streptococcal colonization in pregnancy. Vaginal Infections and Prematurity Study Group. Obstet Gynecol 1991;77:604–10.
Regan JA, Klebanoff MA, Nugent RP, et al. Colonisation with group B streptococci in pregnancy and adverse outcome. VIP Study Group. Am J Obstet Gynecol 1996;174:1354–60.
Schrag SJ, Zell ER, Lynfield R, Roome A, Arnold KE, Craig AS et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med 2002a;347:233–239.
Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC. MMWR Recomm Rep 2002b;51:1–22.
Stoll BJ, Hansen N, Fanaroff AA, et al. Changes in pathogens causing early-onset sepsis in very-low-birth-weight infants. N Engl J Med 2002;347:240–7.
Weeks JW, Myers SR, Lasher L, et al. Persistence of penicillin G benzathine in pregnant group B streptococcus carriers. Obstet Gynecol 1997;90:240–3.
Haemoglobinopathies Definition
A group of inherited disorders of haemoglobin synthesis or haemoglobin structure that have highly variable but significant clinical manifestations. Epidemiology
About 5% of the world’s population are carriers of a potentially pathological haemoglobin gene. Each year, about 300 000 infants are born (worldwide) with sickle cell anaemia (70%) and thalassaemia syndromes (30%) (WHO 2006).
There are ethnic differences in the prevalence of sickle cell disease and the thalassaemias. Sickle cell trait/anaemia is more common in individuals of African, Greek, Turkish, and Middle-Eastern descent. Sickle cell trait (HbAS) is much more common than Sickle cell disease/anaemia (HbSS). The thalassaemias, especially α-thalassaemia, are common among the Asian population. β-Thalassaemia is also prevalent in the Mediterranean islands and Southern Italy. But the demographics are slowly changing; with more interracial marriages and population migrations, these conditions are not uncommonly seen in the UK and most major cities. Pathology
The α-globin cluster is located on the human chromosome 16, and the β-globin cluster is located on chromosome 11. Each individual normally has two paired α-globin genes, one pair on the maternal chromosome and the other pair on the paternal chromosome. The γ, δ-, and β-globin genes are encoded on chromosome 11.
Each haemoglobin (Hb) molecule has two pairs of globin chains. The usual adult haemoglobins are HbA, HbA2, and HbF. The production of normal haemoglobins require an intact gene, intact promoters, enhancers, and silencers, and an intact locus control region (LCR).
In sickle cell disease, an abnormal form of globin chains is synthesized. An A-to-T point mutation in the sixth codon of the β-globin chain gene leads to a glutamine-to-valine substitution on position six of the β-globin chain. In deoxy conditions, the resultant Hb has decreased solubility, increased viscosity, and forms tactoids. These phenomena alter the shape of the red blood cell into the characteristic sickle shape.
In thalassaemias, production of functional haemoglobin is impaired. In general, but not always, α-thalassaemia is due to partial/total deletions of the α-globin genes, whereas β-thalassaemia arises from missense/nonsense mutations within the β-globin gene.
The phenotypic expression of α-thalassaemia is extremely varied, but generally depends on the number of functional α-globin genes present. Patients who inherit three normal α-globin genes are phenotypically normal and may be haematologically normal as well, but are silent carriers of α-thalassaemia. Patients who inherit two normal α-globin genes are phenotypically normal, but have a mild anaemia, low mean corpuscular volume (MCV) and low mean corpuscular haemoglobin (MCH) levels. Cis-type double gene deletions are common in the Asian population, and can lead to haemoglobin Bart’s hydrops fetalis (below). Patients who inherit only one normal α-globin gene have HbH disease, with haemolytic anaemia, defective erythropoiesis, and splenomegaly. Functional deletion of all four α-globin genes leads to an inability to produce any HbA, HbA2, or HbF. In utero, this leads to hydrops fetalis and intrauterine/early neonatal demise. In the Asian population, Hb Bart’s hydrops fetalis occurs because of fetal inheritance of two defective parental chromosomes, each with a cis double gene deletion of both α-globin genes on chromosome 16.
In β-thalassaemia minor (heterozygous/carrier state/trait), one of the β-globin genes is defective. In β-thalassaemia major (homozygous), both genes are affected so the production of β-globin chains is severely impaired. Clinical approach
Screening and diagnosis
The implications of the major haemoglobinopathies are significant in pregnancy, especially for the fetus and newborn child. All pregnant women in the UK are offered a screening test for thalassaemia, and sickle cell disease forms part of the antenatal and newborn screening programme.
History
• Sickle cell disease is usually diagnosed in childhood, so it is unusual to diagnose this condition in pregnancy. Moderately severe anaemia (Hb Heart disease Definition
Heart disease in pregnancy refers to any pre-existing or pregnancy-related heart disorder that became symptomatic or detected during pregnancy, for which treatment may or may not be required. The condition or its residual effects may persist after pregnancy. Epidemiology
Heart disease is one of the leading causes of maternal death in developed countries such as the UK. Heart disease complicates about 1% of all deliveries, but the reported figures can vary depending on the extent and type of investigations performed to confirm or exclude the diagnosis, and whether the denominator includes miscarriages and therapeutic abortions in addition to deliveries, and whether it is the number of mothers or total pregnancies that are counted. In general there is a progressive decline in the prevalence of chronic rheumatic heart disease (RHD) but an increase in congenital heart disease (CHD), especially in women after corrective surgery, so that the proportion of pregnant women with CHD had increased from 5% to 80%. The improvement in medical care, and delayed child-bearing, also mean that conditions in women who are previously advised against pregnancy, as well as age-related conditions, will be encountered more and more often in the future. Pathology
In normal pregnancy, cardiac output is increased by 50%, which peaks between the mid-second and third trimesters. This is achieved by increase in stroke volume and heart rate, and is in response to the increase in blood volume of 50%. There is a concomitant fall in peripheral vascular resistance with a disproportionately greater lowering of diastolic blood pressure and a wide pulse pressure. The decrease in blood pressure lasts up to 34 weeks’ gestation, when the peripheral resistance begins to rise again. There is increased pulmonary blood flow, which is balanced by a reduction in pulmonary vascular resistance. Myocardial hypertrophy and chamber enlargement are demonstrable by the third trimester, and mild multivalvular regurgitation is often found. Inferior vena caval and aortic compression by the gravid uterus in the supine position can result in a marked decrease in the blood pressure and uterine perfusion, especially during labour, and results in maternal hypotension, weakness, lightheadedness and may reduce placental perfusion. During labour, cardiac output is increased further by 10–14%, so that any conditions that restrict cardiac output can easily lead to cardiac decompensation in labour.
Pregnancy is also associated with a hypercoagulable state. Increased circulating oestrogens can interfere with collagen in the media of the muscular arteries, whereas elastase can weaken the aortic media, and relaxin can decrease collagen synthesis. Thus pregnancy is a predisposing factor to dissection of blood vessels, even in the absence of an underlying connective tissue disorder.
The severity of cardiac symptoms is classified by the New York heart Association (NYHA) classification as follows.
• Class I—no limitation of activity, no symptoms from ordinary activity.
• Class II—slight or mild limitation of activity, comfortable with mild exertion.
• Class III—marked limitation of activity, comfortable only at rest.
• Class IV—confined to rest in bed/chair; any physical activity leads to discomfort and symptoms occur at rest.
Heart diseases constitute a big heterogeneous group and are traditionally categorized into congenital, rheumatic, arrhythmias, and other acquired conditions. However, to facilitate discussion on pathology, the conditions can be categorized as follows.
Valvular diseases
Valvular heart diseases constitute the largest group and include congenital and acquired conditions, as well as native and prosthetic valves. In general, women tolerate valvular regurgitation better than stenosis, because the reduction in systemic vascular resistance limits the effect of regurgitation and accentuates the effect of stenosis.
Native valves
The valves involved in descending frequency are mitral, aortic, pulmonary, and tricuspid. There may be multiple valvular involvement in RHD.
Mitral valve
Mitral stenosis, which is almost always due to RHD, is more common than mitral regurgitation, which often accompanies mitral stenosis but is more commonly due to mitral valve prolapse (MVP). In cases of mixed mitral stenosis and mitral regurgitation, the clinical problem is predominantly due to mitral stenosis. Mitral stenosis is regarded as severe when the valve area is 10 mmHg, and mild when the valve area is >1.5 cm2 and gradient PS rarely causes any significant effect on pregnancy outcome. For PS associated with other CHDs, the outcome is related mainly to the presence or absence of cyanosis and the type of CHD. Severe PS refers to a maximum gradient of 60 mmHg while severe regurgitation refers to a dense continuous wave Doppler signal with a steep deceleration slope.
Tricuspid valve
Tricuspid valvular lesions are rare and may be congenital in association with other lesions (Ebstein’s anomaly, tricuspid atresia) or acquired (endocarditis). Regurgitation (TR) is the more common pathology, in which case connective tissue disorders such as Marfan’s syndrome, and other structural heart abnormalities should be looked for. Isolated TR usually has little impact on pregnancy outcome. Severe stenosis refers to a valve area of 0.7 cm and systolic flow reversal in hepatic veins.
Prosthetic valves
Prosthetic valve replacement is used to treat rheumatic heart disease as well as congenital valvular stenosis, most commonly involving the mitral followed by the aortic valve, and not infrequently more than one valve is involved. There are two types of prosthetic heart valves, the mechanical and the biological valves. There are two main concerns that are related to the type of valves. For mechanical valves, it is the increased risk of thromboembolism and problems associated with the use of anticoagulants. For the biological valves, these can be heterografts (porcine) or homografts (limited data in pregnant women). There is a substantial risk of structural valve deterioration (SVD) with both types. At 10 years, the risk of SVD is between 55% and 77%. Hence the interval between valve replacement and pregnancy and the age at prosthetic valve implantation are important factors to consider. The rate of SVD is 24% on average, which can be threefold higher than non-pregnant patients. Mitral bioprosthesis has a higher rate of SVD than aortic bioprosthesis. The mortality of reoperation during pregnancy is 3.8% to 8.7%. Other complications include prosthetic valve endocarditis, thromboembolism, and sudden death.
The best approach is probably autografts, based on the Ross principle, using pulmonary autograft for aortic valve replacement. When inserted in children, the valve increases in size with growth of the children. The limited available data suggest that the autograft is associated with lower risks of thromboembolism, infective endocarditis, and the need for reoperation. An early series of 14 pregnancies in eight women reported no valve-related complications during pregnancy, and no pregnancy-induced effect on the function of the pulmonary valve autograft or right-sided homograft. Rheumatic valvulitis can occur in the autograft in patients with rheumatic heart disease, and other reported complications included peripartum cardiomyopathy (PPCM) and valvular obstruction.
Complex and surgically corrected CHDs
These patients, especially those who have undergone surgery, are particularly prone to have arrhythmias, which can lead to functional deterioration. Those with atrial surgery, such as the Mustard or Fontan procedure, and those with right ventricular impairment, are vulnerable to atrial flutter. Surgical correction for tetralogy of Fallot (TOF) may increase the risk of atrial flutter or ventricular tachycardia arising from the right ventricular outflow tract.
For TOF, there is increased fetal loss, the majority of which are in the form of miscarriages (27%), and a 6% incidence of cardiac and other congential anomalies. In women with unrepaired TOF, the incidence of miscarriage and small-for-gestational age infants were 20% and 30% respectively. Unrepaired TOF and morphological pulmonary artery abnormality impact on birthweight. Even in women with surgically corrected TOF, there was a 21% spontaneous miscarriage rate, and among the successful pregnancies, cardiac complications occurred in 12%, but there was no clear relationship between cardiac characteristics of the mother with perinatal complications, but there was a 2.2% risk of recurrence for CHD. Other exceptional causes reported included coronary artery spasm, Kawasaki disease, and aortic prosthetic valve thrombosis. Coronary artery spasm may be induced with drugs such as methylergometrine, ergonovine, and even bromocriptine. Acute myocardial infarction (AMI) in the presence of morphologically normal coronary arteries might be due to transient thrombus and emboli that had undergone resorption, with or without preceding coronary vasoconstriction. The hypercoagulation state of pregnancy, aggravated by the release of tissue-plasminogen activator inhibitor at the time of placental separation, could be a contributing factor. Anecdotal reports of myocardial ischaemia and infarction has been reported with the use of betasympathomimetics, with/without the addition of nifedipine, for the treatment of preterm labour. This potential complication must be borne in mind in treating preterm labour even in patients without known heart diseases.
Pulmonary hypertension can arise from CHD with a left to right shunt as in ventricular septal defect, which can result in the Eisenmenger syndrome, or as an idiopathic primary event. Maternal mortality is 30–50%, usually due to further increase in pulmonary vascular resistance consequent to thrombosis or fibrinoid necrosis, which can develop rapidly in the peripartum and postpartum period with little forewarning. In Eisenmenger syndrome, right to left shunting is increased during pregnancy due to the decrease in systemic vascular resistance and right ventricular overload.
For all types of cyanotic CHD, the overall maternal mortality is 2%, and there is high risk of complications such as infective endocarditis, arrhythmias, congestive heart failure, and thromboembolism. Adverse pregnancy outcomes include spontaneous miscarriage (50%), preterm delivery, fetal growth restriction, and pre-eclampsia (up to 50%).
Dextrocardia is uncommon, with an incidence of 1 per 5000–20 000 live births. The condition includes isolated dextrocardia as well as situs inversus. There is apparently no maternal cardiac deterioration or obstetric complications, and all cases of fetal growth restriction belonged to the patients with situs inversus (67%).
Cardiomyopathies and myocarditis
There are three main categories of cardiomyopathy. The commonest is PPCM, followed by cardiomyopathies due to other conditions (hypertrophic, dilated, hypertensive, endocrine related, such as thyroid and diabetic, infection, and connective diseases), and cardiomyopathy of unknown type.
Peripartum cardiomyopathy
This condition is diagnosed mainly by exclusion, and the diagnostic criteria are
• cardiac failure developing in the last month of pregnancy or within 5 months of delivery
• absence of an identifiable cause for the cardiac failure
• absence of recognizable heart disease prior to the last month of pregnancy
• left ventricular systolic dysfunction on echocardiography, such as depressed shortening fraction or ejection fraction.
Recently, it was reported that among patients with a history of cardiomyopathy diagnosed during pregnancy that fulfilled the traditional diagnostic criteria for PPCM, onefifth were diagnosed earlier than the last month of pregnancy, and that there was no difference between patients diagnosed earlier versus those diagnosed within the last month of pregnancy with respect to maternal demographics, associated conditions, left ventricular ejection fraction, rate and time of recovery, and outcome. Therefore, some of the cases categorized as cardiomyopathy of unknown cause might have represented the continuum of a spectrum of the same disease. The actual incidence of PPCM could therefore be higher than the reported incidence of between 1 per 1485 to 1 per 15 000 pregnancies, and a reasonable estimate is 1 per 3000–4000 live births. The classical risk factors are multiparity, advanced age, multifetal pregnancy, pre-eclampsia/gestational hypertension, and Black women. Endomyocardial biopsies have consistently revealed features of myocarditis with the highest incidence of 100%, which could be due to an underlying viral infection, or autoimmune response. Coincident with clinical improvement was the resolution of the myocarditis. The finding of myocarditis is dependent on the interval from onset of symptoms, and the focal nature of the inflammatory infiltrates may give rise to false-negative results. Evidence of a maternal inflammatory reaction and associated cell death in PPCM is suggested by the significantly elevated plasma levels of C-reactive protein (CRP), tumour necrosis factor (TNF)-α, and Fas/Apo-1 (an apoptosis-signalling surface receptor that triggers cell death) at diagnosis. In fact, baseline CRP was correlated positively with baseline left ventricular end-diastolic and end-systolic diameters and inversely with left ventricular ejection fraction. Normalization of left ventricular ejection fraction occurred in 54% and was more likely in patients with left ventricular ejection fraction ˇ30% at diagnosis, and maternal mortality was 9%.
Hypertrophic cardiomyopathy
These women tolerated pregnancy well, and no complications were reported with either general or regional anaesthesia.
Lymphocytic myocarditis
This is extremely rare but case fatality has been reported. The case presented with nausea, vomiting, and hepatic dysfunction in the first trimester, and deteriorated rapidly with cardiopulmonary arrest.
Cardiac arrhythmias
In the general population, arrhythmias can be found on Holter recordings in up to 60% of normal individuals up to the age of 40 years, and symptomatic atrial re-entrant and atrioventricular nodal re-entry tachycardias are more common in females. Furthermore, in pregnancy, the heart rate increases by 25%, especially in the third trimester, and ectopic beats and non-sustained arrhythmias can be encountered in >50% of women. Therefore, palpitations and arrhythmias are often encountered in pregnancy, but the physiological adaptation of the cardiovascular and endocrine systems to pregnancy may render sustained arrhythmias more likely to develop. However, sustained tachycardias are found in 0.2–0.3%, whereas pathological bradycardias, usually due to congenital heart block, are found in of a third system are required. For cases of mutation, one major criterion and involvement of a second organ system must be present. The cardiac features include mitral and tricuspid valve prolapse and regurgitation, aortic dilatation, regurgitation, and dissection.
The average age of presentation is 35 years. The mortality can be as high as 30% in the older patients. The prognosis is better if there is minimal cardiovascular involvement and the aortic root diameter is 4 cm, or an increase in aortic root size during pregnancy, is associated with high risk of type A dissection.
Pulmonary vascular disease
This group is rarely encountered, as pregnancy is contraindicated in view of the high maternal mortality, which peaks on days 2–9 postpartum from refractory heart failure.
The precipitating factors for deterioration include increase in pulmonary vascular resistance and volume overload. Echocardiography is not as accurate as pulmonary artery catheterization in assessing pulmonary arterial pressure as it tended to overestimate the value, leading to misclassification in 30% of patients with normal pulmonary arterial pressure.
Primary pulmonary hypertension
This condition refers to the finding of persistently increased pulmonary arterial pressure without an aetiology. It is rare but more commonly encountered in women. In general, pregnancy is contraindicated as the maternal mortality is as high as 50% but more recent data have suggested a rate of 30%. Preterm birth and fetal growth restriction are common.
Secondary pulmonary hypertension and Eisenmenger’s syndrome
This is secondary to congenital and acquired disorders, and Eisenmenger’s syndrome is the final stage where reversal of the left-to-right shunt, or bidirectional shunting, occurs thus resulting in cyanosis. Maternal mortality rate is 20–52%. Aetiology
Rheumatic heart disease occurs following rheumatic fever in childhood, and with the control and prevention of rheumatic fever, its incidence has been on the decline.
The aetiology of PPCM remains uncertain, but the following have been suggested: myocarditis, abnormal immune response to pregnancy, maladaptive response to the haemodynamic stresses of pregnancy, stress-activated cytokines, prolonged tocolysis, familial, abnormalities of relaxin, and deficiency of selenium. A recent series reported that the common associated factors were gestational hypertension (43%), tocolytic therapy (19%), and twin pregnancy (13%).
Cardiac arrhythmias can be related to a structurally normal or abnormal heart in relation to the following conditions
• CHDs: acyanotic, e.g. ASD, VSD; cyanotic, e.g. TOF; valvular, e.g. bicuspid aortic valve
• acquired heart disease: valvular heart disease, e.g. RHD, endocarditis; cardiomyopathy; degenerative disease of conducting system; acquired long QT syndrome, e.g. drugs, metabolic conditions
• congenital ‘electrical-only’ disease: dual AV nodal pathways causing AV nodal re-entry
• Wolf Parkinson White (WPW)/accessory pathways
• channelopathy. Prognosis
In the literature, the incidences of various complications and adverse outcomes vary according to the period of study, the nature/combination of the lesions and functional classification, and the degree of objective assessment with imaging studies. Adverse neonatal outcome is increased overall, including birth before 37 weeks, fetal growth restriction, respiratory distress syndrome, and perinatal death.
The prognosis of some of the uncommon conditions is described here.
For cardiomyopathies, the mortality rate is related to the type of cardiomyopathy. Overall, PPCM accounted for up to 70%, whereas other cardiomyopathies and cardiomyopathy of unknown type accounted for 20% and 10% respectively. Of the deaths, 50% occurred between 43 days and 1 year postpartum, and 2% occurred before delivery. The rate was 0.88 per 100 000 live births.
For PPCM, adverse prognostic factors for maternal mortality include symptoms at >2 weeks postpartum, Black women, age >30 years, multiparity, significantly lower mean left ventricular ejection fraction and smaller LV enddiastolic diameter at diagnosis, and persistent cardiomegaly. The reported incidences of persistent cardiomegaly and progressive cardiomyopathy varied from 50% to >90%, and mean survival was 0.04 ng/mL predicted persistent LV dysfunction with a sensitivity of 54.9% and a specificity of 90.9%.
In general, persistent LV dysfunction is found in about half of the survivors (59%). On echocardiography performed at diagnosis, a LV end-diastolic dimension of ˇ6 cm and a fractional shortening value of (Group 1, from 56% to 49%) as well as those with persistent LV dysfunction (Group 2, from 36% to 32%). Symptoms of heart failure and maternal mortality were 21% and 0% respectively in Group 1, and 44% and 19% respectively in Group 2. Group 2 also had higher incidences of preterm delivery (37% versus 11%) and therapeutic abortion (25% versus 4%). Women with persistent LV dysfunction should therefore avoid subsequent pregnancies due to the increased risk of morbidity and mortality.
For hypertrophic cardiomyopathy, cardiac symptoms during pregnancy were reported in 28%, mostly (90%) among women who were symptomatic before pregnancy. Symptoms deteriorated in especially at the pulmonary area. In patients without a history of heart disease, further assessment and investigations are warranted when unusual symptoms are reported. These include chest pain, dyspnoea on exertion (especially if progressive), orthopnoea, paroxysmal nocturnal dyspnoea, persistent cough, anorexia, extensive oedema, and easy fatigability. For patients with history of heart disease, these specific symptoms should be elicited in each visit and the relevant physical examination performed when necessary. On examination, auscultation of the heart and chest should always be performed in addition to counting the peripheral pulse. General features such as jugular venous congestion, tachycardia, and peripheral oedema may be normal features of pregnancy. Abnormal features include tachypnoea, hepatomegaly, hepatojugular reflux, ascites, oedema of 3-plus or more, mental status changes, and thromboemboli phenomena, and a gallop rhythm, diastolic murmur or systolic murmur of grade 3 and above, loud P2, and rales, on auscultation.
Patients with a history of heart disease should be seen in the antenatal clinic at 4-weekly intervals initially till 24–28 weeks, then fortnightly afterwards till 32–34 weeks, and then weekly thereafter. Apart from features of cardiac deterioration, one should watch out for fetal growth restriction, preterm labour, pregnancy-induced hypertension, and other conditions that can lead to cardiac deterioration such as anaemia and infection. When features suggestive of deterioration in cardiac function appear, or at the first signs of obstetric complications, the patient should be admitted for assessment and further investigations. Following discharge from hospital, the subsequent antenatal and postnatal visits of the patient should be arranged at a conjoined medical–obstetric clinic in a tertiary centre.
Antenatal inpatient assessment should be arranged in case of suspicion of deterioration or complications. In addition to the standard examination and investigations, further assessment include daily bodyweight, temperature, blood pressure and pulse rate monitoring (screen for arrhythmias), charting fluid intake and output, pulse oximetry recording, spirometry, repeat ECG, chest X-ray, blood tests, and screening for infection. Cardiac consultation and echocardiography will be performed both in patients with and without a history of symptoms of heart disease for prognostication. A 24-hour rhythm tape should be arranged if arrhythmia is suspected. After assessment, a management plan should be drawn up, and the appropriate management team be formed under the coordination of the obstetrician in charge or preferably under a maternal–fetal medicine specialist. The team may include a neonatologist, anaesthetist, haematologist, physiotherapist, and a clinical psychologist or psychiatrist if necessary. The points to be laid down in documentation include the use of medications and monitoring of the therapeutic effects, especially drugs that can affect the fetus like anticoagulants, the frequency, methods, and venue of the follow-up assessment, predicted complications and adverse outcomes with the appropriate response plans, fetal monitoring and assessment, timing and mode of delivery, anaesthetic concerns and treatment, preventive measures such as for thromboembolic complications, and maternal psychological wellbeing. The patient and her partner should be fully informed, and, if possible, be involved in the decision-making process. The wishes of the patient should be respected. Both the maternal and fetal status should be regularly reviewed so that the management plan can be revised when necessary.
Investigations
• General aspects: chest X-ray with shielding of the abdomen can help to reveal abnormal heart size or contour, and pulmonary congestion or other lesions. Baseline blood tests include complete blood count, renal and liver function, and blood gas and acid–base measurement. Urine, sputum, and blood culture should be performed according to clinical suspicion.
• Electrocardiogram (ECG): a baseline ECG is helpful for future comparisons, and help in documenting arrhythmias. In normal women, the ECG usually shows a normal sinus or sinus tachycardia rhythm. Normal changes include decreased PR, QRS, and QT intervals, left axis deviation, Q wave and inverted T wave in the inferior leads, ectopics and non-sustained atrial arrhythmias. Abnormal features include left ventricular hypertrophy, inverted T waves, Q waves, and non-specific ST-T changes, and delta waves of the Wolff–Parkinson–White (WPW) syndrome. A 12-lead ECG should be recorded during symptoms, and 24/48-hour Holter monitor may be necessary, but the documentation may be difficult owing to the frequency of the attacks and the presence of precipitating events, and whether the patients are taking normal activities or resting. For outpatients, a diary and patient-activated event recorder may help to establish the diagnosis.
• Echocardiography: in normal pregnancy, there is mild ventricular enlargement with physiological regurgitation in most of the valves in the absence of valvular disease. Serial echocardiographic examination is warranted in conditions where structural changes and functional deterioration cannot be easily determined from physical signs and symptoms alone. Echocardiography allows the serial assessment of the dimensions of the chambers, particularly the LV at different stages of the cardiac cycle and to document LV function and dysfunction, measuring valvular area, flow gradient, and measurement of the aortic root to exclude aneurysm.
Arrhythmias are frequently encountered in pregnancy. The following approach can be arranged in the clinic:
• confirm the diagnosis, using 24-hour (Holter) recordings if necessary;
• rule out underlying heart disease with echocardiography
• exclude systemic disorders including thyroid dysfunction, haemorrhage, pulmonary embolism, infection, and inflammatory state, through appropriate examination and investigations.
Fetal assessment
There are two aspects. In general, women with heart disease are at increased risk of fetal growth restriction and preterm labour. Fetal growth should be monitored with serial ultrasound scanning. Fetal wellbeing should be assessed and monitored if there is maternal functional deterioration, and/or the presence of obstetric complications. In patients with CHD, there is a variable risk of recurrence. While the overall incidence is usually cited as 3–5%, more recent findings suggested much higher risks in relation to the type of maternal lesion as follows:
• Marfan’s syndrome: 50%
• aortic stenosis: 15–17.9%
• pulmonary stenosis: 6.5%
• ventricular septal defect: 9.5–15.6%
• atrial septal defect: 4.6–11.0%
• patent ductus arteriosus: 4.1%
• coarctation of the aorta: 14.1%
• tetralogy of Fallot: 2.6%.
Therefore, appropriate referral for detailed ultrasound scanning and prenatal diagnosis is warranted. The availability of first trimester screening for fetal aneuploidy using nuchal translucency measurement can also help to screen out fetuses with CHD, 90% of which are associated with increased nuchal translucency. First trimester ultrasound scan may identify some of the significant heart malformations, but a detailed ultrasound scan for fetal cardiac and other anomalies should always be arranged for all patients with heart disease. The option of therapeutic abortion should be made available for the parents before 24 weeks gestation should significant cardiac and/or other anomalies be found. There is little point in jeopardizing the safety of the mother by continuing the pregnancy in the presence of significant fetal anomalies, even if these are compatible with neonatal survival, because looking after such a child, as well as caring for the rest of the family or coping with employment, would be too demanding especially for the mother whose health is already affected by the underlying heart disease. If therapeutic abortion is indicated, medical termination with prostaglandin analogues such as misoprostol would be preferable.
Treatment
Since the same groups of medications are used to treat different conditions, medical treatments are grouped together for discussion. Owing to increased plasma volume, protein binding, and drug metabolism, in pregnancy, the dose of medications may need to be regularly adjusted to maintain therapeutic level for adequate treatment.
General measures
• Bed rest with non-medication prophylaxis for deep vein thrombosis (DVT) such as physiotherapy and pressure stocking
• Salt and fluid restriction, ensuring a balanced intake and output but avoid dehydration and haemoconcentration which may be detrimental to placental perfusion and increase the risk of DVT
• Adequate nutrition, including iron and vitamin supplements to prevent anaemia
• Antenatal exercise, which can be performed on the bed, and is important in minimizing muscle wasting in the lower body following bed rest, so that the ability for vaginal delivery would not be seriously compromised
• Prevention of constipation by increasing fibre intake and avoiding dehydration, as the Valsalva manoeuvre increases the risk of bradycardia and syncope
• Sleeping in the lateral position helps to avoid the supine hypotension syndrome
• Vagotonic manoeuvres such as carotid sinus massage can terminate episodes of tachycardias
• Oxygen may be necessary in symptomatic patients, especially those with functional deterioration, and during labour and delivery
• Resuscitation of cardiac arrest may be necessary and the cardiac arrest team should be called. Relief of aortocaval compression using a ‘Cardiff wedge’ on the right side, raising the right hip, or manual displacement of the uterus to the left side, may contribute to a successful resuscitation. Early intubation reduces the risk of aspiration. Peri-arrest Caesarean section also aids resuscitation and facilitates external cardiac massage, in addition to possibly saving the fetus.
Medical treatment
Diuretics
Furosemide
This is used to decrease congestion and blood volume in valvular heart disease and heart failure in cardiomyopathy. Excessive or prolonged use can deplete maternal intravascular volume and decrease placental perfusion. Maternal potassium level should be monitored and supplement may be needed. For the fetus there is risk of hypoglycaemia, hyponatraemia, hypokalaemia, and thrombocytopenia. The usual dose is 20–40 mg daily by mouth. For acute treatment, intravenous boluses of 10–40 mg can be given.
Antihypertensives
Methyldopa
This is considered to be the safest antihypertensive agent in pregnancy, well tolerated by the mother and with no major adverse effects in the fetus. The usual dose is from 500 mg to 4 g daily orally in divided doses.
Beta-blockers
This lowers blood pressure and controls heart rate in case of supraventricular tachycardia, and atrial fibrillation in clinically significant mitral stenosis. It is also indicated in Marfan’s syndrome, aortic aneurysm, myocardial ischaemia, and hypertrophic cardiomyopathy. It is the drug of choice for the WPW syndrome, as digoxin and calcium channel blockers may accelerate conduction through the accessory pathway leading to deterioration of the maternal condition. It is effective for VT with a left bundle branch block pattern. It has been associated with fetal growth restriction, bradycardia, apnoea, hypoglycaemia, and hyperbilirubinaemia in the newborn. This group is safe for breast feeding. Examples include propranolol, acebutolol, labetolol, metoprolol, and atenolol. Metoprolol is preferred to atenolol, which is associated with a higher incidence of fetal growth restriction. The dose may need to be titrated to achieve heart rate control, usually 100–200 mg daily in one or two divided doses. Selective beta-1-blockers are preferred since they are less likely to interfere with beta-2-mediated uterine relaxation..
Vasodilators
Hydralazine
This is indicated in aortic regurgitation and LV dysfunction, usually in a dose of 75–150 mg daily in divided doses. There are no major adverse fetal effects.
Nitrates
This can be used in myocardial ischaemia and infarction, hypertension, and pulmonary oedema, but in pregnant women it is used to decrease venous congestion. There are minimal fetal effects.
Angiotensin-converting-enzyme inhibitors
This group of agents is contraindicated in pregnancy because of the well-documented effect of fetal urogenital defects, renal failure, anaemia, growth restriction, and death.
Antiarrhythmics
Digoxin
This is used for suppression of supraventricular tachycardia (SVT) and control of the ventricular rate in atrial fibrillation associated with severe mitral stenosis. There are no major fetal adverse effects and is safe for breastfeeding. The usual dose is 0.25 mg daily, and one or two rest days per week may be necessary since it can accumulate with long-term use. Maternal serum potassium level should be monitored especially if a diuretic is given, and potassium supplement may be required. There is no evidence of significant fetal side-effects.
Adenosine
This is used for immediate conversion of SVT, using escalating IV boluses up to a maximum of 18–24 mg until the target is achieved. Most women respond to 6–12 mg due to a reduction in adenosine deaminase. It is possible that an arrhythmia may be accelerated due to enhanced conduction down an accessory pathway, so that treatment should be monitored and resuscitation equipment is available during its administration. Owing to its very short half-life, there are no adverse fetal effects and is safe for breastfeeding.
Quinidine
This is used occasionally for the suppression of atrial or ventricular arrhythmias. It can have oxytocic effect at high dose and may lead to premature labour. Rare complications include fetal eighth nerve damage and neonatal thrombocytopenia, but is safe for breastfeeding.
Procainamide
This is used occasionally for the suppression of atrial or ventricular arrhythmias like atrial fibrillation. It is safe for short-term use, but lupus-like syndrome, gastrointestinal disturbance, hypotension, and agranulocytosis may be associated with long-term use. It is safe for the fetus and breastfeeding.
Amiodarone
This is used to suppress atrial or ventricular arrhythmias in high-risk patients but is seldom used in pregnancy because it can be associated with fetal hypo-and hyperthyroidism, goitre, growth restriction, and preterm birth.
Lignocain
This is indicated for VT with IV administration. It is safe for pregnancy and breast feeding.
Sotalol
It is a preferred drug for treating atrial fibrillation. Transient fetal bradycardia may occur but it is generally safe for pregnancy and breastfeeding.
Verapamil
This is now the second-line IV medication for SVT, using doses up to 10 mg without effect on fetal heart rate. It can also control ventricular rate in atrial fibrillation, and is effective in VT with a right bundle branch block pattern. It may cause maternal hypotension and fetal distress with rapid injection, but no other adverse fetal side-effects have been reported. It is safe for breastfeeding.
DC cardioversion
This is indicated in VT. It is safe in all stages of pregnancy, with only a small risk of inducing fetal arrhythmia due to the small amount of current reaching the fetus, but the fetus should be monitored before and during the procedure. In the third trimester, general anaesthesia and intubation may be preferred to avoid problems with the airway and aspiration of gastric contents.
Implantable cardioverter defibrillators
Good maternal and fetal outcomes have been reported in pregnant women with this device. Fetal monitoring is advisable after each therapy, but fetal distress is usually related to the hypotension associated with the arrhythmias. This is an option for women who failed pharmacological treatment, and the leads can be positioned using ECG guidance, thus avoiding fetal radiation exposure.
Cardiac pacing
This is indicated in bradycardia due to heart block to ensure an adequate heart response to the demands of pregnancy. Temporary overdrive pacing may be life saving in polymorphic VT.
Anticoagulant and antithrombotic agents
Unlike in the case of prevention of DVT and pulmonary embolism, anticoagulant therapy for cardiac indications has to be more aggressive in the sense that an adequate therapeutic level must be achieved in order to minimize the chance of thromboembolic complications, especially for patients with prosthetic heart valves. The indications for anticoagulant therapy are
• mechanical prosthetic heart valves
• atrial fibrillation
• tight mitral stenosis with dilated right atrium
• cardiomyopathies.
Warfarin
The dose of warfarin is adjusted to maintain an international normalized ratio (INR) of between 2.5 and 3.5. Warfarin crosses the placenta, and its use, especially if it is given between the sixth and twelfth weeks of gestation, may lead to ‘warfarin embryopathy’ in the offspring, with an overall incidence of 3.9% among the total exposed pregnancies and 6.4% to 7.4% among the total live births. This is characterized by nasal hypoplasia and stippled epiphyses. Other features include central nervous system (hydrocephalus, microcephaly, mental retardation), cleft lip and cleft palate, and eye and other miscellaneous abnormalities, some of which are attributable to warfarin exposure in later gestation. There is also increased risk of other fetal complications that include spontaneous miscarriage (24.7%) and fetal wastage (33.6%). The overall incidence of fetal complications is apparently dose related, being 15% and 88% among pregnancies in women taking a daily dose of ˛5 mg versus >5 mg, and the probability of fetal complications is correlated with the dose (Vitale et al 1999). To minimize the fetal risk, including that of haemorrhage during and after birth, the use of heparin in the first trimester and in the last 2–3 weeks before delivery is generally recommended. The combined warfarin–heparin regimen is associated with a spontaneous abortion rate of 14.7–42.2%, a fetal wastage rate of 16.3–44.4%, and a congenital anomalies rate of 0–11.1%. Despite achieving the therapeutic target as assessed by the INR, warfarin cannot prevent maternal valve thrombosis (3.9%), while the use of heparin from the sixth to the twelfth weeks’ gestation was associated with a risk of 9.2%), while the corresponding incidence of maternal death were 1.8% and 4.2% respectively. Major bleeding events occurred in 2.5% of all pregnancies, usually in the peripartum period.
Heparin
Given subcutaneously, it is usually considered to be less effective than warfarin in patients with prosthetic heart valves, as the incidence of thromboembolism in pregnant patients with mechanical prosthesis is fourfold higher, with a higher maternal mortality and no improvement in fetal outcome. In general unfractionated heparin is used, either in an adjusted-dose regimen (to maintain the activated partial thromboplastin time at 2.0–2.5 times control) or low-dose regimen (˛ 15 000 units per day). The spontaneous abortion and fetal wastage rates were 25.0% and 43.8%, and 20.0% and 40.0%, for the adjusted-dose and low-dose regimens respectively. The congenital anomalies rate was 0% for both regimens. The incidence of thromboembolic complications was 25% and 60% for the adjusted-dose and low-dose regimens respectively, respectively, while that of maternal death was 6.7% and 40% respectively.
Recently the use of LMWH, including nadroparin 0.1 mL/10 kg twice daily, enoxaparin 40 mg daily to 80 mg twice daily, tinzaparin 175 units/kg daily, and dalteparin 100 units/kg twice daily, with or without monitoring with the peak anti-Xa level 3 hours after injection to keep it between 0.4–1.0 units/mL, has been reported for this purpose. There were both successful cases and cases of thromboembolic complications, but the numbers are too small for any meaningful conclusion. The advantages of LMWH are reduced incidence of heparin-induced thrombocytopenia, allergy, osteoporosis, ease of administration, and monitoring of anticoagulant effect is usually not required. However, each LMWH is unique with different bioavailability, half life, and safety profile, so that this group of agents must be used with caution and on an individual basis until data from randomized controlled trials of adequate size are available.
Antiplatelet agents
Aspirin and dipyridamole have also been reported as the only treatment for patients with prosthetic heart valves. Although the incidences of thromboembolic complications and maternal death were 29% and 4.3% respectively, those for spontaneous abortion, congenital fetal anomalies, and fetal wastage were lower than the aforementioned regimens. Nevertheless, the use of these agents alone should not be recommended as a reasonable alternative to the above regimens and more data from prospective studies are required. Aspirin is more often given as adjunct to heparin and LMWH, prescribed in a low dose that varies between 60 and 100 mg daily in different regimens. High doses are not given as the therapeutic effect is not proven, and this approach is associated with fetal complications including haemorrhage, prolonged labour, and growth restriction.
The recommendation from the American College of Chest Physicians (ACCP) is shown in Table 8.17.1.
Surgical treatment
Balloon valvuloplasty/valvotomy can be considered in tight mitral/aortic stenosis with symptomatic deterioration and refractory to medical treatment. The optimal timing for the procedure is the second trimester.
Valvular repair/replacement should be avoided in pregnancy. If such surgery is indicated before delivery, there is a high chance of fetal death or hypoxic damage, miscarriage, or premature labour. Since fetal prognosis is poor, other options such as therapeutic termination or elective preterm delivery before the cardiac surgery should be considered, and a management plan involving all the relevant specialties be made following thorough discussion. The plan is then recommended to the patient who should be involved in the final decision.
Surgical repair for special conditions
Surgical repair is necessary in Marfan’s syndrome, but the aorta is inherently fragile and difficult to work with. Replacement of the aortic root and ascending aorta, with composite mechanical valved-conduits using the modified Bentall approach, is associated with a mortality rate of 0–2.6% and 5.6–11.7% for elective and emergent replacement. Therefore this should be arranged before pregnancy is contemplated. The conduits are at risk of endocarditis and thromboembolic disease, and are less ideal than the newer approach using valve-sparing aortic root replacement techniques involving remodelling or reimplantation which has a survival rate of 90–92%. In a series of four patients with acute type A aortic dissection during pregnancy, three underwent composite graft replacement combined with reimplantation of the coronary artery and aortic valve replacement and the other had aortic valve replacement with coronary bypass grafting of the right coronary artery. Three patients had aortic arch repair utilizing antegrade cerebral perfusion and deep hypothermia with total circulatory arrest. The three patients with cardiac surgery performed either combined with Caesarean section (n=2) or after vaginal delivery (n=1) survived and were discharged with their babies in good condition, although the remaining patient with the fetus in situ during cardiac surgery had fetal demise just after surgery and then died 4 days later with disseminated intravascular coagulation and multi-organ failure. Therefore, Caesarean section with concomitant cardiac surgery appears to give better results in this situation.
Table 8.17.1 Recommendations from the American College of Chest Physicians (ACCP)

Operative intervention in Ehlers–Danlos syndrome should be avoided because the vessels tear easily.
Management of labour and delivery
Two issues have to be considered separately, that is the timing and the mode of delivery. As the safe delivery of the infant with minimal maternal consequences is the penultimate objective, labour and delivery should be an event that is planned or anticipated well beforehand, and the necessary precautions must be undertaken accordingly.
Timing of delivery
For well-controlled and asymptomatic women, the pregnancy is likely to be carried to 37 weeks or later. In the absence of any obstetric complications, it is preferable to allow spontaneous labour at term. In case of obstetric indications for early delivery, the date of delivery should be decided ahead of time and appropriate consultation (with anaesthetist and cardiologist) and arrangement for peri-and postpartum care, such as the setting up of invasive monitoring and an ICU bed, must be organized beforehand. The delivery should be conducted in the daytime under the charge of the MFM team and not left to the on-call team to deal with a complicated patient having what is to them unfamiliar problems.
Mode of delivery
In the absence of obstetric or medical contraindications, vaginal delivery is preferred to Caesarean section, and a planned induction of labour can be safely conducted as for any high-risk patients with close maternal and fetal monitoring. However, if after careful assessment the mother or fetus is thought to be unable to withstand the stress of labour, or that the duration of labour may be uncertain due to an unfavourable cervix, or that the delivery could be difficult due to cephalopelvic disproportion, an elective Caesarean section to minimize the time required for the delivery may be in the best interest of the mother and infant. The most important concern is to avoid having to perform an emergency or crash caesarean section for maternal or fetal distress in a mother with significant underlying cardiac disorder, as there would be considerable maternal and fetal risks. Another concern is the difficulty in timing the administration of medications which are necessary for the mother but which would increase the risk of complications, such as anticoagulants. An elective caesarean section would be preferred under such circumstance.
Intrapartum management
Invasive monitoring: the decision for the use of invasive maternal monitoring during labour and the early postpartum period should be left to the cardiologist and ICU specialist, but this is unnecessary for most of the women. Monitoring of blood pressure, pulse rate, SaO2, and respiratory rate is often sufficient for the mother, and cardiotocography is necessary for the fetus. If internal monitoring of the mother or fetus is indicated, watch out and cover for potential problems such as bleeding and infection.
Fluid balance: fluid restriction in the intrapartum and postpartum period is important to avoid fluid overload and iatrogenic pulmonary oedema. Diuresis induced with intravenous furosemide may be necessary after delivery if fluid intake significantly exceeds output, in order to prevent pulmonary oedema. An indwelling Foley catheter is preferred especially if epidural analgesia is given. The catheter should be removed in the second stage to avoid trauma inflicted by the balloon on the bladder sphincter and urethra.
Antibiotic cover: although routine antibiotic cover for the prophylaxis of bacterial endocarditis is considered unnecessary, the use of antibiotic cover should be individualized, taking into consideration the duration of rupture of membranes, internal monitoring, e.g. fetal scalp electrode or intrauterine pressure cannula, operative delivery, and vaginal/perineal lacerations or abdominal wound haematoma. Clinical suspicion of chorioamnionitis and previous positive vaginal culture are other indications. Intravenous antibiotic administration is necessary since anticoagulant therapy is often required in these patients.
Analgesia: adequate analgesia is necessary for labour management in cardiac patients, and epidural analgesia is the preferred option except for patients on anticoagulant treatment, in which case all intramuscular injections should also be avoided.
Prevention of postpartum haemorrhage: the usual prophylaxis for postpartum haemorrhage should be given. Oxytocin infusion should be given in a higher concentration with reduced volume of infusion fluid. Any ergot-containing medications should be avoided. Careful repair of episiotomy or caesarean section wound with good haemostasis is necessary, and additional measures like pressure dressing for the abdominal wound and packing for the vaginal wound may be necessary for the first day to avoid haematoma collection, especially in patients who has been or will be on anticoagulant therapy.
Postnatal management and breastfeeding
The management in the postpartum period follows the principle for all high-risk patients who require specific medications such as anticoagulants, antihypertensives, and antibiotics, etc. The complications to watch out for are
• infections
• wound complications
• cardiac decompensation or related complications
• thromboembolic complications
• postpartum depression.
The postpartum stay in the hospital should be flexible and premature discharge from the hospital should be avoided. Breastfeeding is not contraindicated but this should not be enforced either. One should ensure that the mother can look after herself and is coping with her baby before discharge, and assessment for depression using instruments such as the Edinburgh Postpartum Depression Scale should be performed before discharge. Early postnatal follow-up is essential, not only for patients requiring adjustment of warfarin dose, but also for patients requiring other medications. Again a flexible approach with assessment at a special clinic run by MFM specialist would ensure the optimal care for these patients. Further reading
Adamson DL, Nelson-Piercy C. Managing palpitations and arrhythmias during pregnancy. Postgrad Med J 2008;84:66–72.
Ayhan A, Yucel A, Bildirici I, Dogan R. Fetomaternal morbidity and mortality after cardiac valve replacement. Acta Obstet Gynecol Scand 2001;80:713–18.
Bedard E, Shore DF, Gatzoulis MA. Adult CHD: a 2008 overview. Br Med Bulletin 2008;85:151–80.
Ben Farhat M, Gamra H, Betbout F, et al. Percutaneous balloon mitral commissurotomy during pregnancy. Heart 1997;77:564–7.
Bhatla N, Lal S, Behera G, et al. Cardiac disease in pregnancy. Int J Gynecol Obstet 2003;82:153–9.
Boggess KA, Watts DH, Hillier SL, Krohn NA, Benedetti TJ, Eschenbach DA. Bacteremia shortly after placenta separation during cesarean delivery. Obstet Gynecol 1996;87:77–984.
Burn J, Brennan P, Little J, et al. Recurrence risks in offspring of adults with major heart defects: results from first cohort of British collaborative study. Lancet 1998;351:311–16.
Campuzans K, Rogue H, Bolwick A, Leo MV, Campbell WA. Bacterial endocarditis complicating pregnancy: case report and systematic review of the literature. Arch Gynecol Obstet 2003;268:251–5.
Carvalho JS. Early prenatal diagnosis of major congenital heart defects. Curr Opin Obstet Gynecol 2001;13:155–9.
Chan WS, Anand S, Ginsberg JS. Anticoagulation of pregnant women with mechanical heart valves. Arch Intern Med 2000;160:191–6.
Chapa JB, Heiberger HB, Weinert L, et al. Prognostic value of echocardiography in peripartum cardiomyopathy. Obstet Gynecol 2005;105:1303–8.
Dore A, Somerville J. Pregnancy in patients with pulmonary autograft valve replacement. Eur Heart J 1997;18:1659–62.
Drenthen W, Pieper PG, Roos-Hesselink JW, et al. Pregnancy and delivery in women after Fontan palliation. Heart 2006;92:1290–4.
Elkayam U, Akhter MW, Singh H, et al. Pregnancy-associated cardiomyopathy. Clinical characteristics and a comparison between early and late presentation. Circulation 2005;111:2050–5.
Elkayam U, Bitar F. Valvular heart disease and pregnancy. Part I: native valves. JACC 2005;46:223–30.
Elkayam U, Ostrzega E, Shotan A, Mehra A. Cardiovascular problemsin pregnant women with the Marfan syndrome. Ann Intern Med 1995;123:117–22.
Elkayam U, Tummala PP, Rao K, et al. Maternal and fetal outcomes of subsequent pregnancies in women with peripartum cardiomyopathy. N Engl J Med 2001;344:1567–71.
Elkayam U. Pregnancy through a prosthetic heart valve. JACC 1999;33:1642–5.
Ellison J, Thomson AJ, Walker ID, Greer IA. Use of enoxaparin in a pregnant woman with a mechanical heart valve prosthesis. Br J Obstet Gynaecol 2001;108:757–9.
Fawzi ME, Kinsara AJ, Stefadouros M, et al. Long-term outcome of mitral balloon valvotomy in pregnant women. J Heart valve Dis 2001;10:153–7.
Felker GM, Thompson RE, Hare JM, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N Engl J Med 2000;342:1077–84.
Fung TY, Chan DLW, Leung TN, Leung TY, Lau TK. Dextrocardia in pregnancy. 20 years’ experience. J Reprod Med 2006;51:573–7.
Furman B, Shohan-Vardi I, Bashire A, et al. Clinical significance and outcomes of preterm pre-labor rupture of membranes: population-based study. Eur J Obstet Gynecol Reprod Biol 2000;92:209–16.
Gei AF, Hankins GD. Cardiac disease and pregnancy. Obstet Gynecol Clin North Am 2001;28:465–512.
Gleason TG. Heritable disorders predisposing to aortic dissection. Thorac cardiovasc Surg 2005;17:274–81.
Hameed A, Akhter MW, Bitar F, et al. Left atrial thrombosis in pregnant women with mitral stenosis and sinus rhythm. Am J Obstet Gynecol 2005;
Hameed A, Karaalp IS, Tummala PP, et al. The effect of valvular heart disease on maternal and fetal outcome of pregnancy. JACC 2001;37:893–9.
Hu CL. Li YB, Zou YG, et al. Troponin T measurement can predict persistent left ventricular dysfunction in peripartum cardiomyopathy. Heart 2007;93:488–90.
Hung L, Rahimtoola SH. Prosthetic heart valves and pregnancy. Circulation 2003;107:1240–6.
Hyett J, Perdu M, Sharland G, et al. Using fetal nuchal translucency to screen for major congenital heart defects at 10–14 weeks of gestation: population based cohort study. BMJ 1999;318:81–5.
Immer FF, Bansi AG, Immer-Bansi AS, et al. Aortic dissection in pregnancy: analysis of risk factors and outcome. Ann Thorac Surg 2003;76:309–14.
James AH, Jamison MG, Biswas MS, et al. Acute myocardial infarction in pregnancy. A United States population-based study. Circulation 2006;113:1564–71.
Khairy P, Ouyang DW, Fernandes SM, et al. Pregnancy outcomes in women with CHD. Circulation 2006;113:517–24.
Lind J, Wallenberg HC. The Marfan syndrome and pregnancy: a retrospective study in a Dutch population. Eur J Obstet Gynecol Reprod Biol 2001;98:28–35.
Lupton M, Oteng-Ntim E, Ayida G, Steer PJ. Cardiac disease in pregnancy. Curr Opin Obstet Gynaecol 2002;14:137–43.
Malhotra M, Sharma JB, Tripathii R, et al. Maternal and fetal outcome in valvular heart disease. Int J Gynecol Obstet 2004;84:11–16.
Moore RC, Briery CM, Rose CH, et al. Lymphocytic myocarditis presenting as nausea, vomiting, and hepatic dysfunction in the first trimester of pregnancy. Obstet Gynecol 2006;108:815–17.
Nabhan A. Peripartum cardiomyopathy. ASJOG 2005;2:231–7.
Oei SG, Oei SK, Brolmann HAM. Myocardial infarction during nifedipine therapy for preterm labor. N Engl J Med 1999;340:154.
Pearson GD, Veille J-C, Rahimtoola S, et al. Peripartum cardiomyopathy. National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) Workshop Recommendations and Review. JAMA 2000;283:1183–8.
Penning S, Robinson KD, Major CA, Garite TJ. A comparison of echocardiography and pulmonary artery catheterization for evaluation of pulmonary artery pressures in pregnant patients with suspected pulmonary hypertension. Am J Obstet Gynecol 2001;184:1568–70.
Petanovic M, Zagar Z. The significance of asymptomatic bacteremia for the newborn. Acta Obstet Gynecol Scand 2001;80:813–17.
Roberts N, Ross D, Flint SK, Arya R, Blott M. Thromboembolism in pregnant women with mechanical prosthetic heart valves anticoagulated with low molecular weight heparin. Br J Obstet Gynaecol 2001;108:327–29.
Romano-Zelekha O, Hirsh R, Blieden L, et al. The risk for congenital heart defects in offsprings of individuals with congenital heart defects. Clin Genet 2001;59:325–9.
Roth A, Elkayam U. Acute myocardial infarction associated with pregnancy. JACC 2008;52:171–80.
Rowan JA, McCowan LM, Raudkivi PJ, North RA. Enoxaparin treatment in women with mechanical heart valve during pregnancy. Am J Obstet Gynecol 2001;185:633–7.
Sakaguchi M, Kitahara H, Seto T, et al. Surgery for acute type A aortic dissection in pregnant patients with Marfan syndrome. Eur J Cardiol Thorac Surg 2005;28:280–5.
Salem DN, Stein PD, Al-Ahmad A, et al. Antithrombotic therapy in valvular heart disease—native and prosthetic. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:457S–482S.
Salem DN, Stein PD, Al-Almad A, et al. Antithrombotic therapy in valvular heart disease—native and prosthetic. The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:457S–482S.
Silversides CK, Colman JM, Sermer M, Siu SC. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol 2003;91:1382–5.
Siu SC, Colman JM, Sorensen S, et al. Adverse neonatal and cardiac outcomes are more common in pregnant women with cardiac disease. Circulation 2002;105:2179–84.
Siu SC, Sermer M, Colman JM, et al. Prospective multicenter study of pregnancy outcomes in women with heart disease. Circulation 2001;104:515–21.
Sliwa K, Forster O, Libhaber E, et al. Peripartum cardiomyopathy: inflammatory markers as predictors of outcome in 100 prospectively studied patients. Eur Heart J 2006;27:441–6.
Thaman R, VarnavaA, Hamid MS, Firoozi S, Sachdev B, Condon M, et al. Pregnancy related complications in women with hypertrophic cardiomyopathy. Heart 2003;89:752–6.
The Task Force on the Management of Cardiovascular Diseases During Pregnancy of the European Society of Cardiology. Expert consensus document on management of cardiovascular diseases during pregnancy. Eur Heart J 2003;24:761–81.
Thorne SA. Pregnancy in heart disease. Heart 2004;90:450–6.
Tsui BCH, Stewart B, Fitzmaurice A, Williams R. Cardiac arrest and myocardial infarction induced by postpartum intravenous ergonovine administration. Anesthesiology 2001;94:363–4.
Uebing A, Steer PJ, Yentis SM, Gatzoulis MA. Pregnancy and CHD. BMJ 2006;332:401–6.
Veldtman GR, Connolly HM, Grogan M, et al. Outcomes of pregnancy in women with tetralogy of Fallot. JACC 2004;44:174–80.
Vitale N, De Feo M, De Santo LS, et al. Dose-dependent fetal complications of Warfarin in pregnant women with mechanical heart valves. JACC 1999;33:1637–41.
Weiss BM, Hess OM. Pulmonary vascular disease and pregnancy: current controversies, management strategies, and perspectives. Eur Heart J 2000;21:104–15.
Yentis SM, Steer PJ, Plaat F. Eisenmenger’s syndrome in pregnancy: maternal and fetal mortality in the 1990s. Br J Obstet Gynaecol 1998;105:921–2. Internet resources
www.clevelandclinicmeded.com
Hepatitis B
The hepatitis B virus (HBV) is a 3.2-kb, partially double-stranded DNA virus, which predominantly infects hepatocytes. HBV infection is a global health problem with a wide spectrum of clinical manifestations, ranging from acute hepatitis, through asymptomatic carriage to liver cirrhosis and hepatocellular carcinoma (HCC). Although antiviral treatments are increasingly effective, the prevention of transmission by vaccination, particularly from mother to child, remains the main route to reducing global morbidity and mortality. Epidemiology
The World Health Organization (WHO) has estimated that there are over 350 million people worldwide with chronic HBV infection, defined as persistence of HBV surface antigen (HBsAg) for more than 6 months. The prevalence of chronic infection varies from high prevalence regions (>8%, such as sub-Saharan Africa, Asia, and the Pacific islands), through intermediate regions (2–8%, southern and eastern Europe, the Middle East, and the Indian subcontinent) to low prevalence regions (preschool and school children and adults. This programme has demonstrated that HBV infection rates, the incidence of HCC, and fulminant hepatitis in childhood can be reduced successfully. In the USA, antenatal screening includes HBsAg but not HBeAg. Every infant is recommended to receive HBV vaccination, while those born to HbsAg-positive mothers also receive HBIg within 24 hours of birth, regardless of HBeAg status (passiveactive immunization). This strategy is considerably more expensive as HBIg is used more frequently. Some countries with intermediate or low prevalence of chronic HBV infection or insufficient resources perform no antenatal screening and vaccinate all infants (without using HBIg). This approach (used for example in Thailand) is less efficacious than the first two. In the UK, there is not a policy of universal infant vaccination. Infants of seropositive mothers receive vaccination with or without HBIg (see below). Vaccination is also recommended for other high risk categories such as injection drug users and health workers. Treatment of chronic HBV infection
There have been major advances in the treatment of chronic HBV infection in recent years. There are two main therapeutic strategies: the use of α-IFN, which enhances T-cell-mediated viral clearance through immunomodulatory activities and the use of oral antiviral agent to suppress HBV replication. The aims of antiviral treatment are to achieve suppression of viral replication and to prevent progression to cirrhosis, end stage liver disease and HCC. Antiviral therapy should be considered in patients with active HBV replication, raised ALT levels and/or liver histology showing active inflammation, necrosis, or fibrosis. In the absence of elevated transaminases, the response to treatment is often poor. Pregnant women with high levels of viral replication may have a lower risk of vertical transmission if oral antiviral therapy is used. However, there remain concerns regarding the safety of such treatments and only limited data are available at present (see below). α-IFN is given in injectable form, often conjugated to a polyethelene glycol (PEG) moiety. In HBeAg-positive patients, seroconversion to anti-HBe or loss of HBV DNA occurs in 30–40% but HBsAg clearance occurs in less than 10%. Its use is limited by significant side-effects and reduced efficacy in HBeAg-negative patients. The oral antiviral agents include lamivudine, adefovir, entecavir, tenofovir, and telbivudine. They reduce HBV DNA levels and may induce seroconversion to anti-HBe. The loss of HBsAg occurs rarely and treatment is often long term. Their use is limited by the development of antiviral resistance. Lamivudine was the first nucleoside analogue to be used in HBV infection. Monotherapy with this agent results in resistance rates of up to 70% at 5 years due to mutations in the HBV DNA polymerase. The newer antivirals appear to have significantly lower risks of resistance and are being licensed for routine use in chronic HBV infection. Hepatitis B in pregnancy
Risk during pregnancy and at delivery
Acute HBV infection in pregnancy does not increase maternal morbidity or mortality and does not increase the risk of fetal complications such as death or congenital abnormalitites. An increased risk of preterm labour has been reported. The risk of perinatal transmission, in the absence of appropriate immunoprophylaxis, is very high in acute infection (>70–90%).
In chronic HBV infection the risk of perinatal infection depends on the HbeAg status of the mother: 90% of babies born to HBeAg-positive mothers and approximately 10% of babies born to HBeAg-negative mothers become infected in the absence of immunoprophylaxis. This risk is also related to maternal serum HBV DNA levels. Although passive–active immunization is highly effective in the prevention of vertical transmission, high maternal serum HBV DNA levels have been associated with the failure of immunoprophylaxis. In a Dutch meta-analysis, the efficacy of passive–active immunization was 100% in infants born to HBeAg-negative mothers and 92% in those born to HbeAg-positive mothers. If the maternal HBV DNA level was greater than 107 IU/mL, transmission was only prevented in 68%. This may be related, in part at least, to intrauterine infection, which is thought to occur via transplacental leakage of maternal blood. There is ongoing debate about whether such patients should commence antiviral therapy in the third trimester of pregnancy (see below).
Acute or fulminant infection in infancy occurs very rarely, predominantly as a result of transmission of HbeAg-negative strains. It does not cause early neonatal viral hepatitis, occurring only after 6 weeks of age.
Clinical approach
Diagnosis: history, examination, investigations
The evaluation of pregnant women who have been identified to have HBV infection (seropositive for HBsAg) should encompass a thorough history including alcohol consumption, risk assessment for co-infection with hepatitis C or HIV and family history of HBV infection and hepatocellular carcinoma. Full clinical examination should be performed with particular attention to stigmata of chronic liver disease (e.g. evidence of ascites, asterixis, spider naevi, etc.). Laboratory tests should include routine liver function tests, standard tests for other forms of potentially coexisting liver disease (e.g. testing for diabetes mellitus, dyslipidaemias, iron storage disorders, autoimmune hepatitis, etc.) and tests for potential co-infection in those at risk (hepatitis A, C, D, E, and HIV). Once the diagnosis of chronic HBV infection has been made, it is important to further define the virological status, i.e. HBeAg status and HBV DNA levels need to be established. HBV levels are measured by the polymerase chain reaction (PCR). A liver ultrasound should be performed to look for evidence of progressive fibrosis and cirrhosis. Where advanced liver disease is suspected, the serum levels of α-fetoprotein (AFP), a marker of HCC, should be determined. All women should be referred to a hepatology specialist for an assessment of liver disease to determine the need for antiviral therapy before or after delivery.
Table 8.18.1 US FDA categories for antiviral drugs

Counselling
Every patient with chronic HBV infection should be counselled regarding lifestyle changes to prevent transmission to sexual partners and household contacts. The need for disease monitoring in specialist clinics and the importance of alcohol, a risk factor for the development of cirrhosis, should be discussed. Robust systems should be in place to ensure that maternity services for pregnant HBsAg-positive women are informed to ensure immunoprophylaxis of the newborn.
Management
Acute HBV infection during pregnancy
Treatment of acute HBV infection is supportive only as currently no specific treatments are available. Fetal infection after an acute self-limiting maternal HBV infection in early pregnancy is rare. In contrast, if acute infection occurs in the third trimester or in the immediate postpartum period, the maternal–infant transmission rates are very high. Passive–active immunization is required.
Management of chronic HBV infection in pregnancy Management decisions regarding women with chronic HBV infection who become pregnant while on oral antiviral therapy need to be made on an individualized basis. The drugs that are currently used in antiviral therapy have been allocated to categories B (no evidence of risk in humans) and C (risk cannot be ruled out) by the United States Food and Drug Administration (Table 8.18.1).
The benefit of the treatment must be weighed against the potential small risk of the antiviral drugs to the fetus. Surveys have not demonstrated substantial increases in birth defect rates in first trimester exposures to Lamivudine over rates in the general population (Antiretroviral Pregnancy Registry Steering Committee report). Early in the first trimester it may be appropriate to stop treatment with careful monitoring through pregnancy. Alternatively, depending on the stage of liver disease and treatment history, it may be optimal to continue treatment or switch drugs (Liaw 2005).
The current UK guidance recommends passive–active immunization at birth (HBIg plus vaccination; injection at different sites if given simultaneously) for infants who
• are born to HBeAg-positive mothers
• are born to mothers who are HbeAg negative but have no anti-HBe Ab
• are born to mothers where the e-markers are not known
• are born to mothers who had acute HBV infection during pregnancy
• weigh less than 1500 g at birth.
It is recommended that newborns to mothers who are anti-HBe positive (HBsAg-positive, HBeAg-negative) receive active immunization only, starting at birth. The accelerated immunization schedule is preferable, i.e. the first dose at birth and further doses at 1 and 2 months of age and a fourth dose at 12 months. HBsAg testing should take place at the same time as the last dose of vaccine to identify those babies for whom immunoprophylaxis was not successful and to ensure further specialist management.
A number of strategies have been tested to reduce the rate of failure of immunoprophylaxis in mothers with high viral loads. Studies have shown that administration of Lamivudine in the last trimester of pregnancy results in lower rates of perinatal transmission. A small study published in 2003 treated eight highly viraemic mothers (HBV DNA >1.2 ? 109 IU/mL) with 150 mg of Lamivudine daily during the last month of pregnancy. Twenty-four children born to untreated HBsAg-positive mothers with similarly high HBV DNA levels served as controls. All newborns received passive–active immunization at birth and were followed-up for 12 months. Seven of the eight Lamivudine-treated mothers had a significant decrease in HBV DNA. One of the eight children (12.5%) remained HBsAg and HBV DNA positive at 12 months while all others seroconverted to anti-HBs. In the untreated control group perinatal transmission occurred in 28% of children (van Zonneveld 2003). Li and colleagues compared the use of antenatal HBIg with Lamivudine in mothers who were HBsAg positive (56 women received 200 IU of HBIg intramuscularly every 4 weeks from 28 weeks of gestation, 43 women were given 100 mg of Lamivudine daily from week 28 until day 30 after delivery and these were compared to 52 women (controls) who received no specific treatment): neonatal infection was significantly lower in those receiving HBIg (16%) or Lamivudine (16%) than in controls (33%; p107 IU/mL, there are no clinical trial data to inform optimal management of this group of women and further studies are required. At present, women with viral loads greater than 107 IU/mL may be considered for antiviral therapy during the third trimester of pregnancy. Clinicians caring for pregnant patients with chronic HBV infection should liaise with a viral hepatitis specialist to optimise treatment in individual cases.
Vaccination of preterm babies
There is evidence that preterm, low-birthweight babies have a suboptimal response to HBV vaccination. Therefore, the recommendations suggest the full paediatric dose of HBV vaccine on schedule. Babies weighing 1500 g or less should be given HBIg together with the vaccine (independent of the eAg-status of the mother). Further reading
Alter MJ. Epidemiology of hepatitis B in Europe and worldwide. J Hepatol 2003; 39:S64–S69.
Chang MH, Chen CJ, Lai MS, et al. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. N Engl J Med 1997;336:1855–9.
Chang MH. Hepatitis B virus infection. Semin Fetal Neonatal Med. 2007;12:160–7.
Chen HL, Chang CJ, Kong MS et al. Fulminant hepatic failure in children in endemic area of hepatitis B virus infection:15 years after universal hepatitis B vaccination, Hepatology 2004;39:58–63.
del Canho R, Grosheide PM, Mazel JA, et al. Ten-year neonatal hepatitis B vaccination program, The Netherlands, 1982–1992:protective efficacy and long-term immunogenicity. Vaccine 1991 5:1624–1630
Dusheiko G, Antonakopoulos N. Current treatment of hepatitis B. Gut 2008;57:105–124.
Liaw YF, Leung N, Guan R, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2005 update. Liver Int 2005;25:472–89.
Lin HH, Lee TY, Chen DS et al. Transplacental leakage of HbeAg-positive maternal blood as the most likely route in causing intrauterine infection with hepatitis B virus. J Pediatr 1987;111:877–81.
Realdi G, Fattovich G, Hadziyannis S, et al. Survival and prognostic factors in 366 patients with compensated cirrhosis type B: a multicenter study. The Investigators of the European Concerted Action on Viral Hepatitis (EUROHEP). J Hepatol 1994;21:656–66.
Terrault NA, Jacobson IM (). Treating chronic hepatitis B infection in patients who are pregnant or are undergoing immunosuppressive chemotherapy. Semin Liver Dis 2007;27(Suppl 1):18–24.
van Zonneveld M, van Nunen AB, Niesters HG, et al. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Hepat 2003;10:294–7. Internet resources
Antiretroviral Pregnancy Registry Steering Committee report: www.apregistry.com/forms/apr_report_106.pdf
Department of Health. Immunization against infectious disease—the Green Book: www.dh.gov.uk
Health Protection Agency: www.hpa.org.uk Patient resources
British Liver Trust: www.britishlivertrust.org.uk
The Hepatitis B Foundation: www.hepb.org.uk
Herpes simplex infection Definition
Genital herpes is a sexually transmitted infection that is caused by the herpes simplex virus (HSV). This infection is typically characterized with recurrent ulcerative lesions on the genital mucosa. During pregnancy, genital herpes causes concern for morbidity and mortality associated with neonatal infection. Epidemiology
Genital herpes is one of the most common ulcerating diseases of the genital mucosa. The WHO estimates that 40–60 million people in the USA are HSV-2 infected, with an incidence of 1–2 million infections and 600 000–800 000 clinical cases per year. HSV-2 causes most of the genital infections whereas HSV-1 is primarily responsible for herpes labialis (‘cold sores’) gingivostomatitis, and keratoconjunctivitis. Given changing sexual practices, genital HSV-1 infections are becoming increasingly common, responsible for up to 80% of new genital HSV infections. Pathology
HSV belongs to the family Herpesviridae. The virus enters the skin and travels to the sensory neurons, and then the infection becomes latent in the sensory ganglia. This plays an important role in the clinical presentation of HSV. Aetiology
HSV is a double-stranded DNA virus that can be subdivided into HSV type 1 and HSV type 2. HSV is transmitted from person to person through direct contact. Infection is initiated when the virus contacts mucosa or abraded skin. The incubation period of HSV ranges from 2 days to 12 days. HSV then replicates, with resulting cellular destruction and inflammation. During the initial infection, vesicles appear on the vulva, which soon break to leave shallow, painful ulcers. The ulcers heal in 2–3 weeks. This primary infection is then followed by reactivation. Reactivation of viral replication usually presents as recurrent ulcerative lesions or as asymptomatic viral shedding.
Risk factors
• Female gender
• Duration of sexual activity
• Minority ethnicity
• Family income
• Number of sexual partners.
Types of infection
There are three main clinical types to HSV: primary, non-primary first episode, and recurrent. Distinguishing what type a woman presents with can have consequences on perinatal transmission rates. Serological testing and viral isolation would be required to establish type of infection. Each of the presentations can be symptomatic or asymptomatic.
• Primary infection refers to infection in a patient without preexisting antibodies to HSV-1 or HSV-2. This typically presents with systemic symptoms, including fever and malaise.
• Non-primary first episode infection refers to the acquisition of genital HSV-1 in a patient with pre-existing antibodies to HSV-2 or the acquisition of genital HSV-2 in a patient with pre-existing antibodies to HSV-1.
• Recurrent infection refers to reactivation of genital HSV in which the HSV type recovered in the lesion is the same type as antibodies in the serum.
Maternal–fetal transmission
The maternal–fetal or vertical transmission rate is dependent on clinical type and timing of episode. The mode of transmission most commonly occurs via direct contact of the fetus with infected vaginal secretions during delivery. Less commonly, ascending intrauterine infection or postnatal infection may be the cause.
Neonatal clinical manifestations
Acquisition of primary herpes in the first trimester has been associated with neonatal chorioretinitis, microcephly, and skin lesions in rare cases. HSV infection acquired in the late third trimester is associated with one of three patterns in the newborn. Initial symptoms usually occur within the first 4 weeks of newborn life. The three patterns are:
• localized to the skin, eyes, and mouth
• localized central nervous system (CNS) disease
• disseminated disease involving multiple organs. Prognosis
The most important determinants of prognosis of neonatal infection are type and timing of the episode. Primary infections acquired during pregnancy yield a greater risk of perinatal transmission than recurrent episodes. Of those who acquire a primary HSV infection during pregnancy, the risk of vertical transmission is greatest around the time of labour. This risk is approximately 30–60%. For the newborn, mortality can be up to 4% with CNS disease and up to 30% with disseminated disease. Approximately 20% of survivors of neonatal herpes have long-term neurological problems. Clinical approach
Diagnosis
It is not possible to distinguish primary from non-primary herpes simplex virus infection on clinical findings alone. Diagnosis is based on the combination of positive viral detection and negative serological test results or evidence of seroconversion. Even with our diagnostic tools, approximately 80% of infected infants are born to mothers with no reported history of HSV infection.
History
• Personal history of genital herpes
• If personal history of genital HSV: date of diagnosis, medications used, numbers of outbreaks per year
• Sexual history, including partners’ HSV status.
Examination
• Multiple painful vesicles or shallow ulcers on the genitals
• Normal examination findings may be present in a HSV carrier.
Investigations
• Isolation of virus through viral culture or PCR
• Direct fluorescent antibody testing
• Tzank test (microscopic identification)
• Serological testing for type-specific antibodies.
Counselling
For pregnant patients with no known history of genital HSV, counselling should emphasize prevention habits. Avoiding or decreasing exposure to HSV-infected partners when active lesions are present will decrease risk of acquistion. It is important to know that acquistion can still occur with asymptomatic partners. For women with serological test results that indicate susceptibility to HSV infection, the incidence of new HSV infection during pregnancy is about 2%. The most critical time to avoid acquistion is during late pregnancy.
For pregnant patients with a primary outbreak during pregnancy, counselling should include risks and transmission rates as described above.
For pregnant patients with a history of genital HSV, counselling should include awareness of a decreased vertical transmission rate of less than 2%. For patients with multiple outbreaks, suppressive therapy may be initiated at 36 weeks of gestation.
If active lesions are present at the time of labour (preferably prior to rupture of membranes), a Caesarean section should be performed to decrease the vertical transmission risk. The neonatal risks as described above should be explained.
Management
The most common antiviral agents used during pregnancy are Category B medications. They are approved for the treatment of primary and recurrent genital herpes, and the daily treatment for outbreak suppression. There are no documented increases in adverse fetal effects secondary to medication exposure. Topical therapy offers limited benefit and should not be used.
Primary outbreak during pregnancy
Oral antiviral therapy can be initiated to reduce the duration and severity of symptoms and reduce duration of viral shedding. Intravenous antiviral therapy can be initiated in severe disseminated cases of HSV. HSV suppression may be indicated at 36 weeks to decrease recurrence. There is no evidence to support Caesarean delivery before labour to prevent vertical transmission.
Recurrent outbreak during pregnancy
Oral antiviral therapy can also be initiated to reduce number of outbreaks. Women with active recurrent genital herpes should be offered suppressive viral therapy at 36 weeks. Women with recurrent lesions at the time of delivery have a low rate of transmission at about 3%. The transmission rate decreases considerably to 2/10 000 in women with no visible lesions at the time of delivery. There is no indication for Caesarean delivery in women with a history of HSV and no active lesions or prodromal symptoms at time of delivery.
Active outbreak at the time of delivery
Cesarean delivery is indicated with active lesions or prodromal symptoms, which may indicate an impending outbreak, during labour or with ruptured membranes at or near term. This significantly decreases vertical transmission in a primary outbreak. The transmission rate is low in a recurrent outbreak, but Caesarean delivery is still recommended because of the potentially serious nature of the disease. Caesarean delivery does not eliminate the transmission risk. There is no timeframe after rupture of membranes at which a Caesarean delivery is not indicated. Further reading
ACOG Committee on Practice Bulletins. ACOG Practice Bulletin: Management of Herpes in Pregnancy No. 82. Obstet Gynecol 2007;109:1489–98.
Brown ZA, Selke S, Zeh J, et al. The acquisition of herpes simplex virus during pregnancy. N Engl J Med 1997;337:509–15.
Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant. JAMA 2003;289:203–9.
Paz-Bailey G, Ramaswamy M, Hawkes SJ, Geretti AM. Herpes simplex virus type 2: epidemiology and management options in developing countries. Postgrad Med J. 2008 Jun;84:299–306.
Roberts CM, Pfister JR, Spear SJ. Increasing proportion of herpes simplex virus type 1 as a cause of genital herpes infection in college students. Sex Transm Dis 2003;30:797–800.
Sauerbrei A, Wutzler P. Herpes simplex and varicella-zoster virus infections during pregnancy: current concepts of prevention, diagnosis and therapy. Part 1: herpes simplex virus infections. Med Microbiol Immunol 2007;196:89–94.
Sexually transmitted diseases treatment guidelines, 2006 [published in MMWR Recomm Rep 2006;55:997]. Centers for Disease Control and Prevention. MMWR Recomm Rep 2006;55 (RR-11):1–94. Internet resources
World Health Organization: www.who.int
Centers for Disease Control and Prevention: www.cdc.gov/std/herpes
UptoDate: Genital Herpes Simplex Virus Infection in Pregnancy: www.utdol.com
HIV infection Definition
Acquired immunodeficiency syndrome (AIDS) was first described in San Francisco in 1981. It is caused by infection with a retrovirus human immunodeficiency virus (HIV). Following infection cell-mediated immunity, in particular, becomes impaired as the level of CD4 (T-helper cells) cells declines. A normal CD4 count is between 500 and 1500 cells/mm3. Four-fifths of people with AIDS present with a CD4 count 106 copies/mL. After 12 weeks the viral load drops to a lower level, which is usually stable for a number of years before rising again with the onset of AIDS. During seroconversion the CD4 count also falls from the normal level: >500 cells/mm3 and can drop below 200, which is the threshold for the onset of AIDS in chronic infection. It usually recovers to a normal level before progressively declining.
A steady decline in immune function over the first few years may be manifest by non-life-threatening opportunistic conditions such as
• recurrent oral and vaginal candidiasis
• single dermatome herpes zoster (shingles)
• frequent and prolonged episodes of oral or genital herpes
• persistent genital warts (Fig. 8.20.2), CIN, VIN and AIN
• hairy oral leukoplakia (HOL) (Fig. 8.20.3)
• persistent generalized lymphadenopathy (PGL)
• skin problems, including seborrhoeic dermatitis, folliculitis, dry skin, tinea pedis, and a high frequency of allergic reactions.
Without antiretroviral treatment the median time to the development of AIDS is 10 years. Essentially AIDS is defined by the onset of life-threatening opportunistic infections, or malignancies associated with immunodeficiency. The commonest presentations are listed in Table 8.20.1.
A few individuals are resistant to infection through genetic polymorphisms such as those with a Δ32 mutation in the chemokine receptor CCR-5, which is a coreceptor for viral entry into cells. If they become infected they become immunosuppressed only slowly, if at all. ‘Elite controllers’ have undetectable viral loads, but can still develop immunosuppression associated with the inflammatory response to the virus. History
Assessing risk of infection if undiagnosed
In Europe where the epidemic has been linked with particular risk factors they can be used to identify those at greatest risk. However, risk may be undisclosed by a patient or her partner, occasionally vertical infection stays asymptomatic until adulthood, and HIV is spreading in apparently low risk people so the safest course is to test all patients. The main risk factors are:
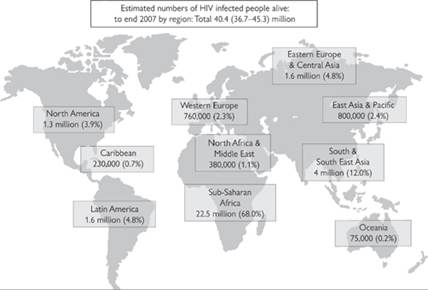
Fig. 8.20.1 Summary of estimated worldwide epidemic 2007 from UNAIDS.
• injecting drug use in patient or partner
• bisexual male partner
• partner originating from a country of high prevalence (mostly sub-Saharan Africa and South East Asia)

Fig. 8.20.2 Extensive genital warts in a pregnant woman presenting with a CD count of 170 cells/mm3. See also colour plate section.
• commercial sex
• blood products that have not been screened
• partner known to be HIV positive.
A sexual history (qv) and travel history should also be obtained.
Person known to be HIV positive
Liaison with the appropriate specialist team is essential, particularly in pregnancy. Obtain the following information:
• when diagnosed, and where
• any AIDS diagnoses or other clinical manifestations of HIV
• current treatment
• current CD4 count and viral load.

Fig. 8.20.3 Hairy oral leukoplakia is seen as white patches on the side of the tongue in HIV infection with often only moderate immunosuppression. The brown discolouration is related to smoking. See also colour plate section.

Fig. 8.20.4 Kaposi’s sarcoma on the face (a) and large lesion on the palate (b). When this occurs multiple lesions are usually present in the gut and lungs as well. See also colour plate section.
If the CD4 count is >200 a new AIDS-defining illness is unlikely to develop. If on antiretroviral treatment for 6 months or more the viral load should be undetectable. Examination and investigations
In an untested individual in whom the diagnosis of HIV is suspected look for the features of opportunistic conditions described above. HOL, oral candidiasis, and evidence of weight loss should all raise suspicion. A full description of the protean manifestation of HIV is outside the scope of this chapter.
Additional features of laboratory tests should raise suspicion of HIV infection. There is usually a polyclonal hyper-immunoglobulinaemia due to the immune dysregulation that occurs, so total protein is elevated in serum. In the blood count, autoimmune thrombocytopenia may occur; total lymphopenia and anaemia of chronic disease are seen in advanced infection.
HIV testing
The diagnosis of HIV is confirmed by identifying HIV antibody. Ideally tests should be done for antibody to both HIV-1 and HIV-2. This is often carried out using ‘finger-prick’ enzyme-liked immunosorbent assays (ELISAs) in developing countries, with a second one for confirmation of positive tests. In the UK we use tests combining ELISA for antibodies and viral p24 antigen detection. The latter allows earlier diagnosis of seroconvertors in the ‘window period’ before antibody develops. The window period is traditionally quoted as 3 months, but current tests usually become positive 4–6 weeks after exposure. If seroconversion is suspected clinically, a viral load assay may provide earlier confirmation of diagnosis, but the difference from p24 antigen detection is a few days.
CD4 count
This is a proxy measurement of the degree of immunosuppression. A normal level is between 500 and 1500 cells/mm3. In the absence of intervention there is a 10% risk of AIDS in the year after the level reaches 200 cells/mm3. This is usually monitored every 3–6 months.
HIV viral load
In untreated individuals the viral load may vary from 107 copies/mL. Some of the assays underquantify non-B subtypes. If there is a mismatch between the CD4 count and viral load a test should be repeated using a different assay. This is usually monitored every 3–6 months. Management
Treatment guidelines are regularly updated from the USA, UK and WHO. There are two strategies used in treatment: antiretroviral therapy and prophylaxis against opportunistic infections in the immunosuppressed.
Combinations of antiretroviral drugs are prescribed. Treatment is recommended for those with a CD4 count below 350 cells/mm3, or with clinical features of disease or cofactors such as hepatitis co-infection when earlier treatment improves prognosis. Currently, where there are resources to pay for the drugs, first line regimens are usually two nucleoside or nucleotide analogues reverse transcriptase inhibitors, such as lamivudine, tenofovir or emtricitabine with a non-nucleoside reverse transcriptase inhibitor (NNRTI) such as efavirenz or nevirapine. Protease inhibitors such as lopinavir/ritonavir or atazanavir with ritonavir are used instead of the NNRTI if there is resistance or other reasons not to use an NNRTI. Newer drug classes include viral entry inhibitors: enfurvitide and maraviroc, and integrase inhibitors such as raltegravir.
Adverse reactions to antiretroviral drugs
There are many potential adverse reactions associated with antiretroviral therapy. A potentially fatal hypersensitivity reaction occurs with abacavir in HLA-B5701 positive individuals (rare in Sub-Saharan African populations). Allergic rashes occur commonly with NNRTIs: nevirapine more often than efavirenz. Nevirapine is particularly associated with Stevens-Johnson syndrome and severe hepatotoxicity. It should not be started in women with CD4 counts >250 cells/mm3 when these reactions are more likely. Tenofovir should be avoided in those with renal impairment as it can cause renal tubular acidosis and exacerbate renal failure.
Protease inhibitors are associated principally with gastrointestinal toxicity: nausea and diarrhoea. Additionally they cause elevations in lipids and increased insulin resistance. They are often used in women starting antiretroviral therapy in pregnancy when efavirenz is contraindicated and nevirapine cannot be used if the CD4 count >250 cells/mm3. Concomitant antiemetics and antidiarrhoeal medication are usually provided with the first prescription.
The newer classes of antiretroviral drugs have only been used in a limited number of pregnant women but are generally well tolerated and not known to be teratogenic (Table 8.20.2).
Table 8.20.2 FDA classification of antiretroviral drugs for safety in pregnancy

Drug interactions
Ritonavir is used with protease inhibitor drugs because it is a potent inhibitor of cytochrome P-450, which greatly increases the half life of other protease inhibitors allowing once or twice a day administration. Protease inhibitors and NNRTIs can inhibit and induce different enzymes making interactions complex and difficult to predict. NRTIs have fewer interactions. The most important ones for a gynaecologist to be aware of include
• rifampicin: contraindicated (rifabutin at reduced dose sometimes used with protease inhibitors)
• sex hormones: levels reduced so oral contraception unreliable. Give double dose of levonorgestrol (3 g) for post-coital contraception
• warfarin levels increased
• proton pump inhibitors decrease levels of atazanavir which can lead to virological failure.
Prognosis
If successful the viral load is usually in pregnancy
Pregnancy is a vulnerable time for a woman to be diagnosed with HIV. Disclosure of diagnosis to partners may lead to domestic violence or abandonment. However the benefits of treatment in reducing vertical transmission and prolonging the mother’s life mean that all women should be encouraged to test. Those that decline should be re-offered testing and reasons for declining explored in depth.
Because the rates of vertical transmission are now so low in Europe and the USA, one of the commonest reasons for it occurring are that the mother seroconverts after her initial test, whilst pregnant or breast feeding. The potential benefits of retesting in the third trimester are being evaluated, with testing of male partners as an alternative strategy.
The CD4 count falls in pregnancy and rises after delivery, so women may present with opportunistic infections in pregnancy. This is best managed in conjunction with the HIV specialist. Where effective antiretroviral therapy is available few vertical transmissions should occur.
Vertical transmission
Without intervention vertical transmission occurs in 25–40% pregnancies. It is thought that a minority of fetuses is infected during gestation. These babies can present with AIDS in the neonatal period. The majority is infected during parturition. Breastfeeding accounts for transmission in up to 15% of pregnancies, corresponding to 37% of infected infants. Transmission by this route may occur even after several months. The risk of vertical transmission is increased if there is a high HIV viral load or a preterm delivery. The role of genital infections in vertical transmission is still being assessed. Many children infected with HIV will survive into adolescence.
Three interventions have been shown to reduce the risk of vertical transmission of HIV.
• Avoiding breast feeding
• Elective Caesarean section
• Antiviral medication prescribed during the latter half of pregnancy, and to the neonate for 4 weeks.
With combination antiretroviral therapy with a viral load of partner, or carry resistance mutations.
This advice is now less clear following a statement by Swiss Physicians that if a man or woman is on treatment with an undetectable viral load the risk of transmission through vaginal intercourse is less than that of couples using condoms where the index patient is not receiving treatment. It is good practice to discuss this with couples and allow them to make their own risk assessment.
Also discuss the management of HIV in pregnancy to reduce vertical transmission. Even with an undetectable viral load caesarean section offers a reduced risk of infection but when the risk is already so low it is not clear that the benefit outweighs the risks associated with caesarean section. In a resource poor setting discuss the pros and cons of bottle feeding versus exclusive breastfeeding.
HIV-positive man
If an HIV-negative woman has a positive partner sperm washing has been shown to be safe, albeit expensive. It is more difficult when this is not available locally or there is no funding for it. A retrospective study of 70 (approx) pregnancies in HIV discordant couples from Spain reported no infections if the index patient had an undetectable viral load. The Swiss statement (above) similarly supports a low risk in this scenario. If a discordant couple choose to conceive naturally the risk of transmission can be minimised by targeting unprotected intercourse to the fertile time of the menstrual cycle, and checking for and treating genital tract infections in both of them. Internet resources
British HIV association (BHIVA) links to current guidelines: bhiva.org
United Nations UNAIDS latest worldwide statistics on the epidemic: www.unaids.org/en
World Health Organization guidelines for resource constrained settings and reports on treatment roll out programmes: www.who.int/hiv/pub/guidelines/en
US Centers for Disease Control links to current guidelines: www.cdc.gov/hiv/resources/guidelines
Antiretroviral pregnancy registry prospective reporting of pregnancies exposed to antiretroviral therapy: www.apregistry.com for
Antiretroviral drug interactions: www.hiv-druginteractions.org Patient resources
Patient support groups generally available locally. National AIDS Manual (NAM): www.aidsmap.com
Positively Women: www.positivelywomen.org.uk
Terence Higgins Trust: www.tht.org.uk
The Swiss Statement: Vernazza P, et al. Les personnes seropositives ne souffrant d’aucune autre MST et suivant un traitment antiretroviral efficace ne transmettent pas le VIH par voie sexuelle. Bulletin des medecins suisses 89 (5), 2008. summarised at www.aidsmap.com/en/news/4E9D555B-18FB-4D56-B912-2C28AFCCD36B.asp
Safety and Toxicity of Individual Antiretroviral Agents in Pregnancy: www.aidsinfo.nih.gov/contentfiles/PerinatalGL-SafetyTox_Sup.pdf
Human papillomavirus Definition
Human papillomavirus (HPV) is a non-enveloped double-stranded DNA virus that infects the epithelium, such as skin, or mucus membranes. In this case the virus is specific to humans, although there are different species-specific papillomaviruses which infect other animals. There are at least 130 different strains of HPV which can infect any part of the human integument. The consequences of infection range from warts to dysplasia, and cancer. The different strains are identified by number and tend to be associated with specific anatomic infections. There are 30–40 types that infect the genital tract in both men and women and largely transmitted by intimate sexual contact. Epidemiology
It is likely that HPV is the most common sexually transmitted infection. Because it is not reportable and not necessarily specifically screened, the true prevalence is uncertain. However epidemiological data suggest that it is well established in younger women such as adolescents and those in their early twenties; rates for HPV infection in women younger than 25 in North America and Northern Europe are 10-fold higher than in women older than 45 (Franceschi et al. 2006). In the USA the CDC estimates that 80% of women will have been infected with at least one strain of HPV by 50 years of age (CDCP 2004). Although it is fair to say that worldwide this is a common infection, there are data from the International Agency for Research on Cancer (IARC) that suggest these trends may not be universal. Their surveys have shown overall low rates of infection in certain populations of Thailand and Vietnam, and flat or rates that increase with age in India, China, Mexico, and South America(1). It is not clear if this reflects different rates of infection or differences in the natural history of HPV among various populations. Pathology
Some of these HPV types, such as 6, 11, 42, 43, and 44, are considered ‘low risk’ and rarely if ever cause cancer but do cause warts and some cases of mild dysplasia. The ‘high-risk’ types, such as 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68, are associated with dysplasia and cancer. This latter group is responsible for the development of cervical intraepithelial neoplasia (CIN) and cancer as well as vaginal (VaIN), vulvar (VIN), penile (PIN), and anal (AIN) neoplasia and cancer. It appears that the majority of genital tract cancers are caused by types 16 and 18 worldwide and may represent a more virulent type of infection (Munoz 2004). Although more than half of cervical cancer is caused by type 16 and approximately two-thirds by 16 and 18, over 90% of vulvar carcinoma is caused by type 16 alone (Srodon et al. 2006). At the same time relative rates for HPV 18 suggest it is more common in the aetiology of glandular pathology.
As for the actual infection process, it appears that the virus must find its way to the basal cell layer of the epithelium, where an interaction between virus and cell allows for some endocytotic event and subsequent transport to the nucleus. In the nucleus the virus usually remains separate from the host genome, as an episome. While the basal cell matures and differentiates becoming part of the superficial epithelial cells the virus genome multiplies and ultimately replicates copies of itself, which are then shed with the superficial desquamating cells. In higher degrees of dysplasia and invasive cancer the viral genome actually integrates into the host DNA suggesting this step is at the root of malignant transformation. The virus ultimately destabilizes the cell cycle with transcription products from the E6 and E7 oncogenes, which interrupt tumour suppressor proteins p53 and pRb respectfully in the host cell. Thus, length of time for harboring the infection correlates with severity of disease, probably by increasing the opportunity for genetic integration. Prognosis
There are multiple studies demonstrating significant clearance rates of HPV infection, particularly in younger patients. The clearance of HPV has also been correlated with the clearance of clinical disease. This premise has been challenged by the notion that perhaps there are long-term latent infections that remain clinically insignificant and are missed because the current screening tools are not sensitive enough or unable to access the virus. Perhaps the greater concern is the development of pathology from latent infection in the future, if the host’s immune status weakens. It is likely that both of these scenarios occur; however, this has little impact on current clinical management which includes continued screening. Clinical approach
The role of HPV has been defined in the development of cervical cancer thanks to the efforts of the recent Nobel laureate and molecular biologist Harald ZurHausen. He established that HPV is involved in the pathogenesis of cervical cancer. His findings along with epidemiological evidence from Munoz et al. (2006) has verified the causal relationship between HPV infection and development of cancer (Srodon et al. 2006). Given this relationship, HPV has become a tool for diagnostic modalities and a target for prophylactic vaccines and therapeutic approaches. Diagnosis
Although the pap smear alone has single-handedly reduced the mortality rate from cervical cancer by more than 70% over the last five decades, the addition of HPV typing increases the sensitivity of finding pathology. The use of HPV typing for high-risk HPV by itself has a sensitivity of greater than 89% for detecting high-grade cervical lesions. This compares favourably to the liquid-based cytology which is probably less than 80%. However, the positive predictive value of HPV typing is not robust because most women with HPV do not have cytological abnormalities. The liquid-based pap smear has a superior positive predictive value as it detects cytological abnormalities which is really the endpoint for clinical screening objectives. Liquid-based cytology is the current screening standard in Europe and was universally implemented in the UK by the end of 2008. Combining the two techniques not only improves the sensitivity but also improves the negative predictive value to nearly 100% (Arbyn et al. 2006). The latter point being that if a patient has a normal pap smear and does not harbour a high-risk HPV her chances of developing severe cervical dysplasia or cervical cancer are less than 0.1% over the next 5 years. Given this, the FDA in the USA approved clinical testing for high-risk HPV as a screening tool when combined with cervical cytology in women 30 years of age or older using the hybrid-capture test marketed by Digene to screen for 13 high-risk types of HPV. In this algorithm patients who have normal cytology and negative HPV testing are not screened for 3 years as a cost-containing measure. Thirty years of age has been selected as a slightly arbitrary age yet does reflect most epidemiological trends in screening a population with a lower prevalence of HPV and greater incidence of pathology which increases the positive predictive value for finding dysplasia. This strategy is less helpful in younger populations where the likelihood of finding HPV is very high without identifying significant neoplasia. The other scenario where High-Risk HPV typing has been approved for clinical use in the USA is as an adjunct to pap smear screening when the cytology is atypical squamous cells of undetermined significance (ASCUS). In this case approximately 50% of the patients do not have a high-risk HPV and are allowed the more conservative recommendation of a pap smear in 12 months. If they have a high-risk HPV they are referred for colposcopic evaluation (ALTS 2003). The role of HPV screening as a diagnostic tool is being evaluated in the UK. There are two major studies which should yield answers in the near future. The first is A Randomized Trial of Human Papilloma Virus Testing in Primary Cervical Screening (ARTISTIC), in which more than 24 000 attendees age 20–64 at Specific NHS Cervical Screening Programme sites are screened with liquid-based cytology and high-risk HPV typing. The HPV results are either revealed or concealed based on randomization. Outcomes will include the test characteristics for HPV typing as well as cost and efficiency. Further outcomes include insight into psychological and psychosexual differences when HPV status is known. Although publication is expected in the spring of 2009, preliminary data support previous findings where HPV prevalence is prohibitively high in younger women, which would only serve to increase the demand for follow-up measures. A second study is a Trial of Management of Borderline and other Low-grade Abnormal smears (TOMBOLA) funded by the Medical Research Council. Results should be forthcoming and will include information on the potential for HPV to be used as triage in patients with borderline or mild dyskaryosis. Management
As for preventive and therapeutic uses, HPV technology has been employed in the production of vaccines. Within the applications of vaccines there are two approaches with one being to prevent infection as a passive vaccine and the other as an active vaccine to treat infected individuals and induce regression of disease. Presently the latter approach is still being developed and is in clinical trials. There appears to be some potential in this, but certainly no consistent and compelling data at this time.
Reproducible data have been published in multiple studies disclosing the efficacy of the prophylactic vaccines in preventing HPV-related disease. This vaccine development grew out of the discovery that the outer protein capsule would essentially self-assemble into an empty viral shell, absent the DNA contents, if the correct capsid proteins were put together in the laboratory. The concept is that the body recognizes these empty viral coats and will produce antibodies that recognize and block future infection from the real virus. As it turns out, the surface proteins are unique to each strain of HPV and thus the vaccine is type specific. Gardasil, produced by Merck pharmaceuticals, one of two prophylactic vaccines, was approved in Europe in 2006 and Cervarix, GlaxoSmithKline, was approved in 2007. Gardasil provides protection against HPV types 6 and 11, which are low-risk types and responsible for 90% of genital warts, as well as high-risk types 16 and 18. Cervarix contains only capsid proteins from high-risk HPV types 16 and 18. Gardasil was approved in the USA in June 2006 for the prevention of cervical cancer and genital warts in females aged 9–26, whereas cervarix has not yet been approved in the USA. Most of the national health plans in Europe have implemented HPV vaccine programmes. The UK recently launched an HPV vaccine programme, using Cervarix, which initially will focus on 12–13-year-old girls. A ‘catch up programme’ will follow whereby 17–18-year-old girls will be vaccinated the following year and then 16–18 and 15–17-year-old girls will be vaccinated the following 2 years respectively. Further reading
Arbyn M, Sasieni P, Meijer C, et al. Clinical applications of HPV testing: a summary of meta-analyses. Vaccine 2006:24;S3/78–89.
ASCUS-LSIL Triage Study (ALTS) Group. Results of a randomized trial on the management of cytology interpretations of atypical squamous cells of undetermined significance. Am J Obstet Gynecol 2003;188:1383–92.
Centers for Disease Control and Prevention (CDCP). Genital HPV infection fact sheet. Rockville: CDC National Prevention Information Network 2004.
Franceschi S, Herrero R, Clifford GM, et al. Variations in the agespecific curves of human papillomavirus prevalence in women worldwide. Int J Cancer 2006;119:2677–84.
HPV vaccines and screening in the prevention of cervical cancer. Vaccine 2006;24(Suppl. 3).
Munoz N, Bosch FX, Castellsaque X, et al. Against which human papillomavirus types shall we vaccinate and screen? The international perspective. Int J Cancer 2004;111:278–85.
Srodon M, Stoler M, Baber G, Kurman R. The distribution of low and high-risk HPV types in vulvar and vaginal intraepithelial neoplasia (VIN and VaIN). Am J Surg Pathol 2006:30,12;1513–18.
Stanley M, Immunobiology of HPV and HPV vaccines. Gynecol Oncol 2008;109:S15–21.
World Health Organization (WHO) Human papillomavirus and HPV vaccines: technical information for policy-makers and health professionals. WHO 2007: http://who.int/reproductive-health/publications/hpvvaccines_techinfo/index.html Internet resources
www.asccp.org
www.hpa.org.uk Patient information and contacts
www.asccp.org
www.cancerresearchuk.org
www.patient.co.uk
Hypertension Definition
Hypertension is established in a pregnant woman if the blood pressure (BP) measurement is ≥140/90 mmHg for two or more occasions at least 4 hours apart using the same arm. If hypertension pre-dates pregnancy or is found before 20 weeks’ gestation, the individual is considered to have chronic hypertension. Hypertension first detected after 20 weeks’ gestation is gestational hypertension (GH) in the absence of significant proteinuria, and pre-eclampsia in the presence of proteinuria. Normotensive women with only an increase in systolic and/or diastolic pressure of 30 mmHg and 15 mmHg respectively are not associated with complications and should not be considered as having GH. Severe hypertension is defined as systolic BP ≥160 mmHg or diastolic BP ≥110 mmHg.
This chapter will be confined to discussion of chronic and gestational hypertension only. Epidemiology
• Chronic hypertension is found in 1–5% of all pregnancies. It includes both essential hypertension and hypertension secondary to underlying medical conditions. The incidences of the various underlying conditions are quite variable depending on location and population.
• Gestational hypertension (GH), found in 3–10% of all pregnancies, may represent the early phase/presentation of pre-eclampsia, which can manifest as late as the time of labour or early postpartum period. It has been shown that the great majority of women presenting with GH in the early third trimester eventually progressed to preeclampsia with time. Pathology
In normal pregnancy, cardiac output shows an early increase with a subsequent plateau after 20–24 weeks gestation, and a small decrease closer to term. Total peripheral resistance shows a similar but inversed pattern with an early decrease and a nadir is reached at 20–24 weeks’ gestation, followed by a plateau and non-significant increase closer to term. Women with GH have significantly elevated cardiac output before and during the clinical course of the condition, reflecting a hyperdynamic circulation throughout pregnancy. The increased cardiac output is demonstrable as early as 11–14 weeks’ gestation and is at a rate well in excess of that of the normal population throughout pregnancy and after the diagnosis of GH. Total peripheral resistance is generally normal throughout most of the pregnancy except towards term when it is reduced. The increased vasodilated state remained despite a clinical diagnosis of GH.
Echocardiographic Doppler studies 2–4 days postpartum revealed that women with GH had significant left ventricular dysfunction, with depressed systolic function and altered diastolic function, left atrial dysfunction, and high total vascular resistance (TVR). The most significant differences shown in the higher isovolumetric relaxation time and the Tei index (sum of both contraction and relaxation isovolumetric periods divided by the ejection time). Furthermore, the left ventricular mass index is increased due to an increase in the septal and posterior wall thickness, whereas the dimensions of the left ventricle, left atrium and aortic root do not change. There is an altered cardiac geometric pattern of concentric hypertrophy.
With respect to adverse maternal and fetal pregnancy outcomes, a stepwise increase is found from GH to preeclampsia, for severe maternal disease (26.5% and 63.4% respectively) as well as for preterm birth and small-for-gestational age (SGA) infants. Aetiology
Chronic hypertension
This may be due to the following conditions:
• essential hypertension, often with a familial history of hypertension
• secondary to chronic renal diseases, including chronic glomerulonephritis and pyelonephritis
• secondary to endocrine conditions including hyper- and hypothyroidism, Cushing’s syndrome/disease, Conn’s syndrome, phaeochromocytoma, adrenal hyperplasia, acromegaly, hyperparathyroidism, and pre-existing type I and type II diabetes mellitus.
• cardiovascular conditions including coarctation of the aorta, renal artery stenosis
• autoimmune conditions such as systemic lupus erythematosus and antiphospholipid syndrome.
Gestational hypertension
Clinically GH may evolve into pre-eclampsia, or reveals itself as the unmasking of chronic hypertension when reassessed after delivery. However, echocardiographic studies suggested different cardiac anatomical and functional changes and adaptation that are distinct from pre-eclampsia and fetal growth restriction, or from normotensive subjects. Furthermore, mild to moderate increase in BP alone is poorly predictive of adverse maternal and fetal outcome. It is therefore possible that GH is a feature of maternal physiological adaptation to the demands of pregnancy, rather than of a pathological process, in a significant proportion of women diagnosed with GH. Prognosis
BP alone is limited in its predictability for adverse outcome, and mild hypertension in isolation or appearing for the first time in labour are generally not associated with adverse outcomes. An increase in the diastolic pressure by 15 mmHg but short of 90 mmHg does not predict adverse outcome. On the other hand, GH may represent the early presentation of pre-eclampsia, and pre-eclampsia may be superimposed on chronic hypertension of all categories. Therefore, all hypertensive patients should be managed as high risk and monitored for the development of multisystem involvement and fetal compromise by clinical and laboratory means.
One new approach is to assess the aforementioned maternal cardiac adaptation to the development of hypertension. Adverse maternal and fetal outcomes can be better predicted from the total vascular resistance (TVR) and left ventricular concentric geometry, both of which are independent predictors. The TVR is calculated from maternal echocardiographic examination and measurement of BP at the brachial artery with a manual cuff, and using the formula:
TVR = (MBP(mmHg)/CO (L/minutes)) ? 80
where MBP is the mean arterial pressure. Applying a cutoff value of 1340 dyn seconds/cm5, the sensitivity and specificity are 90% and 91% respectively. Concentric geometry is defined as a left ventricular mass index >50 g/m and a relative wall thickness >0.44 ((interventricular septum diameter + posterior wall diastolic thickness)(left ventricular end-diastolic diameter)) on echocardiography. Clinical approach
Blood pressure measurement
The systolic blood pressure (SBP) reading is defined by phase I and diastolic blood pressure (DBP) reading by phase V of the Korotkoff sounds. The BP readings should be obtained using a mercury sphygmomanometer with an appropriate-sized cuff (length of 1.5 times the circumference of the arm) placed at the level of the heart with the patient in a sitting position. Any aneroid or automated BP device used should have been calibrated beforehand or validated, since automated devices may underestimate the BP. In case of consistently higher readings from one arm, this arm should be used for all BP measurement.
Conceptual understanding
In practice GH often merges into pre-eclampsia with progressive multisystem involvement and fetal compromise, and reliance on the presence of proteinuria to differentiate between the two conditions is also dependent on the methods of determining proteinuria (spot urine measurement or dipsticks, protein–creatinine ratio, 24-hour collection). Therefore it has been recommended that the appearance of multisystem involvement and/or fetal complications be used instead to define the appearance of preeclampsia. Indeed, the management should be dictated by the clinical features and complications, rather than an arbitrary definition of the condition, be it GH, pre-eclampsia, or pre-eclampsia superimposed on chronic hypertension.
Prepregnancy counselling and assessment for chronic hypertension
Women diagnosed with chronic hypertension due to whatever cause in the reproductive age group should be asked about their desire and plan for pregnancy at regular intervals in the medical clinic, and the information be clearly documented in the medical notes, since their condition and their desire might change with time. Except for severe secondary hypertension or the presence of end organ damage, pregnancy is generally not contraindicated. However, the control of hypertension should be optimized, and the types of medication be changed to ones that are safe for the fetus, when pregnancy is contemplated. For secondary hypertension, the severity and status of the underlying condition should also be assessed and the treatment optimized similarly. Referral to a prepregnancy counselling clinic managed by maternal–fetal medicine specialists is desirable, as all patients with chronic medical diseases should have a realistic picture of the likely course and outcome of pregnancy in relation to their individual condition. There is also the opportunity to discuss and adopt the most appropriate means of contraception until conception is decided. Subsequent follow-up management must be individualized, and the principle is to ensure early confirmation and dating of the pregnancy for subsequent arrangement for prenatal diagnosis and baseline clinical assessment and investigations. It will also be early enough for any change of medications to take place where necessary.
Clinical assessment
First presentation of hypertension
• For a pregnant woman found incidentally to have transient hypertension which settles after a variable period of rest in the clinic, more frequent follow-up assessment should be arranged, the interval being dependent on the gestation. At/after 28 weeks’ gestation, the patient should be seen at least weekly once before spacing out the interval, if the subsequent BP readings are normal.
• For a patient with persistently elevated BP, the fluctuation in the readings should be documented in hourly to 2-hourly measurements in the day centre/day hospital, or if this is not available, then a short stay in the ward. If the BP settles after rest, then she could be seen again the following week. If the BP remains elevated, she may be warded for workup. If only the SBP is elevated, these patients should be closely followed up for the development of diastolic hypertension.
• A comprehensive physical examination should be performed for any woman with hypertension, including auscultation of the heart and chest, looking out for radial-femoral delay, and listening for bruit in the renal area. Fundoscopy should also be carried out if the instrument is available. Even if the BP reading returns to normal subsequently, any abnormal finding should call for assessment especially in the third trimester.
Known chronic hypertension
• For patients with a known history of hypertension, particularly those who are already on antihypertensive medications, symptoms and signs of deteriorating hypertension control should be elicited. The dose of medications can be adjusted in the clinic, but the frequency of follow-up may need to be increased, and the patients should be instructed to return to the clinic or admit herself should adverse effects of either the medication or the hypertension be experienced at home or at work. Sick leave for rest at home may be necessary.
• In case of uncertainty, the patients can be seen daily in the day centre/hospital, or they can measure their BP regularly at home using a sphygmomanometer that has been previously calibrated in the clinic, and to test their urine daily using dipsticks for protein. More frequent follow-up should be arranged if the BP is persistently elevated or proteinuria is significant.
Obstetric examination
• The abdominal examination should include symphysialfundal height measurement, careful palpation for fetal parts, fetal lie and presentation, and a rough estimate of the fetal size and amount of amniotic fluid. In addition, an ultrasound scan should be carried out if available.
• Any suspected fetal growth restriction, oligohydramnios, or unexplained uterine size much larger than date (whether due to polyhydramnios or large fetus or both) would warrant admission.
• All multifetal pregnancies, and pregnancies complicated by fetal or maternal complications such as gestational diabetes mellitus, should be further assessed if hypertension is found in the clinic.
Inpatient monitoring/day-care assessment
• The women should be admitted for assessment and monitoring of maternal and fetal conditions if necessary.
• The BP should be monitored 4-hourly, watching out for the loss of the diurnal rhythm that may suggest the development of pre-eclampsia.
• Maternal symptoms should be documented daily.
• Further investigations should be arranged as indicated.
• Fetal assessment should be organized.
Investigations
Standard investigations
Serial monitoring is required to determine the progression of the condition and timing of intervention.
• Urinalysis: this should be done in the clinic at every visit. A mid-stream urine specimen for culture should always be collected if proteinuria is found. If proteinuria is 2 plus or more, a random specimen for the estimation of the protein–creatinine ratio should be sent. Confirmation of significant proteinuria calls for a 24-hour collection for quantification, which needs to be done carefully to ensure complete collection. Proteinuria is defined as a 24-hour urine protein excretion of ˇ300 mg or a protein–creatinine ratio of ˇ30 mg/mmol.
• Renal function test: this should include the measurement of serum electrolytes, urea, creatinine, and uric acid concentrations. Electrolyte disturbance, especially in the form of a low potassium concentration, should alert one to the possibility of Cushing’s or Conn’s syndrome. If the creatinine concentration is normal, there is no need to calculate the creatinine clearance, which can be done without resorting to a 24-hour urine collection nowadays.
• Liver function test: this should include serum albumen, globulin, bilirubin, alkaline phosphatase, transaminases, and γ-glutamyl transferase. An underlying liver disease may be present.
• Oral glucose tolerance test: this should be carried out if not done before, as there is an association between glucose intolerance and hypertension.
Additional investigations
These depend on the initial findings and clinical suspicion.
• Blood tests to assess and monitor the progression of the condition, including evidence of haemolysis (serum bilirubin, lactate dehydrogenase, serum iron).
• Blood test to monitor disturbance in coagulation, including prothrombin (PT) and activated partial thromboplastin time (APTT), D-dimer, and fibrin-fibrinogen degradation products (FDP), and platelet count and blood smear.
• Blood test for myocardial damage such as creatinine kinase (MB) and troponin-t.
• Test for possible underlying conditions, including blood tests for thyroid function, autoimmune markers, anticardiolipin antibodies and the lupus anticoagulant, calcium level and the calcium–phosphate ratio, other hormones such as growth hormone, cortisol, parathormone, and serum and urine catecholamines, after consultation with physicians.
• Imaging studies, including ultrasound, Doppler and echocardiographic studies, and magnetic resonance imaging and CT scan if necessary, to rule out lesions of the heart and major arteries, and endocrine tumours such as phaeochromocytoma, adrenal tumour, etc.
Fetal assessment and monitoring
For patients with chronic hypertension, screening for fetal anomalies should be organized as for any high-risk pregnancies. Serial monitoring for fetal growth and wellbeing should be commenced in the last 2 months of pregnancy, and earlier if complications or deterioration in BP control occur. For women with GH, the fetal condition should be assessed at diagnosis.
• Fetal anomalies should be excluded with a detailed ultrasound scan if this is not done before. The information helps the obstetrician and parents to decide the best course of action for the remainder of the pregnancy.
• Fetal size should be assessed with ultrasound scan to detect the fetus with unsuspected growth restriction. The information is especially helpful in multifetal pregnancies.
• Fetal wellbeing should be assessed with the biophysical profile (BPP), amniotic fluid index (AFI), especially in fetuses suspected of being growth restricted. The parameters provide a baseline for future comparison. Regular reassessment with the BPP is indicated if there is fetal growth restriction, if the initial BPP score is reduced, or if the antihypertensive medication has rendered the CTG difficult to interpret. A complete profile may not be necessary each time if the AFI is normal and not decreasing, and fetal growth is not slowing down.
• Doppler studies of the uterine and umbilical arteries may be helpful. A placental origin of the hypertension may be suggested from the uterine artery waveform. The umbilical artery indices provide early warning of placental deterioration.
• A fetal kick count to monitor fetal movements at home is helpful for the majority of patients, especially those on medications. They should be instructed to report to the clinic or ward for further assessment should there be sustained or progressive decrease in fetal movements noticed over a 48-hour period.
Antihypertensive medications
Principles
• Initial trial of rest and observation before prescription is useful. Mild hypertension does not require antihypertensive medication.
• Commence treatment promptly for severe hypertension with the aim to keep SBP induction of diuresis with a diuretic may help to minimize the effect of the sudden expansion of blood volume from the return of blood from the uteroplacental circulation.
• Frequent monitoring of BP (e.g. quarter- or half-hourly) may be necessary postpartum, especially in women previously on antihypertensives. The combined effects of changing/stopping the previously prescribed medications before/during labour, fluid dynamics, blood loss, and response to the stress and pain of labour and delivery, often lead to increased fluctuations of BP.
• Prophylaxis for postpartum haemorrhage should be undertaken for all cases with small boluses (5–10 units) of oxytocin, followed with an infusion of 40 units in 500 mL of normal saline given over 4–6 hours. Do not use ergot-containing preparations, which may lead to a sudden increase in BP and myocardial ischaemia
• Postpartum shock may be mistaken initially as the BP returning to normal postpartum. In this context care must be exercised with the peripartum use of nifedipine to control hypertension, since cases of postpartum haemorrhage associated with peripartum use of nifedipine in hypertensive women has been encountered.
Postnatal management and breastfeeding
• Postpartum monitoring of BP: a postpartum increase in BP commencing on day 3 and reaching a peak on days 5–6 is not uncommon, especially in patients whose anti-hypertensive medications have been stopped. This is attributed to fluid shift back into the circulation and the rapid decline in serum progesterone level. A significant rise in BP may be dangerous. Resumption of the original antihypertensive medication, or using a new medication and adjusting the dose according to maternal response may be required. The patient should be discharged with treatment only after the BP has been stabilized and she is asymptomatic. Early postnatal follow-up, e.g. 2–3 weeks postpartum may be necessary. The medication may be tailed off gradually over the next 3–12 weeks. Persistent hypertension after 3 months of delivery warrants referral to physicians for assessment.
• Analgesia should be given in adequate amounts since pain from whatever cause can aggravate hypertension. If an abdominal or episiotomy wound is present, persistent and unrelenting pain calls for careful inspection of the wound to exclude infection and other problems.
• For hypertension secondary to an underlying medical disorder, this should be reassessed by the appropriate specialists, especially when a change of the dose or type of treatment may be indicated, such as for endocrine and autoimmune conditions.
• Breastfeeding: hypertension or its treatment are usually not contraindications for breastfeeding, but the maternal condition should be reviewed to ensure that the mother is fit for breastfeeding.
• Hospital stay: prolonged hospital stay is not necessary provided that the mother can have easy access to the clinic or day centre for prearranged or emergent review. The patient may be discharged on day 3 in the absence of complications and rebound hypertension.
Prevention of hypertension
A number of measures, including medications/supplements, have been studied for the prevention of hypertensive disorders or the adverse effects.
Calcium
Supplementation with at least 1 g daily reduces the risk of hypertension and pre-eclampsia, maternal death, or serious morbidity. The effect is greater for high-risk women and those with low calcium intake. There is no effect on preterm birth or stillbirth.
Antioxidants
Supplementation with vitamins C and E does not appear to be effective, but may even be harmful. The data are insufficient to be conclusive.
Aspirin
Low dose (75–100 g) from prepregnancy or given after the first trimester can reduce the risk of hypertension and preeclampsia, and fetal or neonatal death.
Magnesium
Effect of supplementation not proven.
Salt restriction
Effect not proven.
Folic acid
Apart from the prevention of neural tube defects, 5 mg daily helps to minimize the effect of hyperhomocysteinaemia.
Rest/bed rest, stress reduction
May be useful but effect is small. Further reading
Abalos E, Duley L, Steyn DW, Henderson-Smart DJ. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev 2007;4:CD002252.
Blanco MV, Grosso O, Bellido CA, et al. Dimensions of the left ventricle, atrium, and aortic root in pregnancy-induced hypertension. AJH 2001;14:390–2.
Blanco MV, Roisinblit J, Grosso O, et al. Left ventricular function impairment in pregnancy-induced hypertension. AJH 2001;14:271–5.
Bosio PM, McKenna PJ, Conroy R, O’Herlihy C. Maternal central hemodynamics in hypertensive disorders of pregnancy. Obstet Gynecol 1999;94:978–84.
De Champlain J, Wu R, Girouard H, et al. Oxidative stress in hypertension. Clin Exp Hyperten 2004;26:593–601.
De Paco C, Kametas N, Rencoret G, Strobl I, Nicolaides KH. Maternal cardiac output between 11 and 13 weeks of gestation in the prediction of preeclampsia and small for gestational age. Obstet gynecol 2008;111:292–300.
Duley L, Henderson-Smart D, Knight M, King J. Antiplatelet drugs for prevention of pre-eclampsia and its consequences: systematic review. BMJ 2001;322:329–33.
Higgins JR, de Swiet M. Blood pressure measurement and classification in pregnancy. Lancet 2001;357:131–5.
Hofmeyr GJ, Atallah AN, Duley L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev 2006;3:CD001059.
Magee LA, Cham C, Waterman EJ, Ohlsson A, von Dadelszen P. Hydralazine for treatment of severe hypertension in pregnancy: meta-analysis. BMJ 2003;327:955–64.
Magee LA, Duley L. Oral beta-blockers for mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev 2003;3CD002863.
Magee LA, Sadeghi S. Prevention and treatment of postpartum hypertension. Cochrane Database Syst Rev 2005;1:CD004351.
North RA, Taylor RS, Schellenberg JC. Evaluation of a definition of pre-eclampsia. Br J Obstet Gynaecol 1999;106:767–3.
Novelli GP, Valensise H, Vasapollo B, et al. Left ventricular concentric geometry as a risk factor in gestational hypertension. Hypertension 2003;41: 469–75.
Quan A. Fetopathy associated with exposure to angiotensin converting enzyme inhibitors and angiotensin receptor antagonists. Early Hum Dev 2006;82:23-8.
Rumbold A, Duley L, Crowther CA, Haslam RR. Antioxidants for preventing pre-eclampsia. Cochrane Database Syst Rev 2007;4:CD004227.
SOGC Clinical Practice Guideline. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. JOGC 2008;30(Suppl 1):S1–S48.
Valensise H, Novelli GP, Vasapollo B, et al. Maternal diastolic dysfunction and left ventricular geometry in gestational hypertension. Hypertension 2001;37:1209–15.
Valensise H, Vasapollo B, Novelli GP, et al. Maternal total vascular resistance and concentric geometry: a key to identify uncomplicated gestational hypertension. Br J Obstet Gynaecol 2006;113:1044–52.
Zhang J, Klebanoff MA, Roberts JM. Prediction of adverse outcomes by common definitions of hypertension in pregnancy. Obstet Gynecol 2001;97:261–7. Internet resources
http://highbloodpressure.about.com Patient resources
www.rcog.org.hk
Immunization Definition
• Active immunization: protective immunity is obtained exposing a patient’s immune system to the key antigen of a pathogen so that protective antibodies are produced.
• Passive immunization: protective immunity is obtained providing the patient antibodies preformed in human or animals. Clinical approach
One of the greatest accomplishments of twentieth-century medicine has been the development of effective vaccines for immunoprophylaxis and one of the saddest failures of twentieth-century medicine has been the erratic and incomplete delivery of vaccines to populations at risk.
Pregnancy and breastfeeding are specific conditions that require attention in the administration of a specific vaccine.
Ideally preconceptional immunization to prevent disease in offspring would be preferred to vaccination during pregnancy. Unfortunately, the routine of fully immunizing women entering their reproductive age against common infection, is often unpracticable.
To date there is no evidence that vaccinating pregnant women with an inactivated virus or bacterial vaccine or toxoids poses a risk. In contrast, live vaccines pose a theoretical risk to the fetus of transmission of the virus used. So, if a woman becomes pregnant within 4 weeks after vaccination or if a live virus vaccine is given inadvertently to a pregnant woman, she should be counselled about the potential effects on the fetus.
In the decision of whether to immunize a pregnant woman using ether live or inactivated vaccines, the risk of exposure to disease and its adverse effect on mother and fetus must be balanced against the efficacy of the vaccine and any beneficial effect resulting from it.
Different issues are related to immunization during pregnancy and breastfeeding (Tables 8.23.1 and 8.23.2).
Vulnerable population
• Pregnant women have an altered immune response
• They are at increased risk of some infections
• There is an increased risk of severe outcomes (maternal, fetal, or both) of some infections
• Fetuses and newborns have immature immune system.
Theoretical concerns about efficacy
• the altered immune status of pregnant women may reduce the response to a vaccine
• the quantity of antibodies transferred to the fetus to confer protection may not be adequate
• the half-life of maternal antibodies may not be sufficient to protect fetus/newborn during relevant period of vulnerability.
Theoretical concerns about safety
• Live attenuated virus vaccines
• Use of additives/adjuvants/preservatives with limited or no safety data on exposure.
Timing of vaccination
• Safety risks may vary with time period of vaccination during pregnancy (early pregnancy versus. late pregnancy; immediately postpartum versus later). Breastfeeding
Neither inactivated nor live vaccine administered to lactating women affect the safety of breastfeeding for mothers or infants. Breastfeeding does not adversely affect immunization and is not a contraindication for any vaccine, with the exception of smallpox vaccine.
The following applies to varicella vaccine, which was licensed after the ACIP General Recommendations were published: ‘Whether attenuated vaccine VZV is excreted in human milk and, if so, whether the infant could be infected are not known. Most live vaccines have not been demonstrated to be secreted in breast milk. Attenuated rubella vaccine virus has been detected in beast milk but has produced only asymptomatic infection in the nursing infant. Therefore, varicella vaccine may be considered for a nursing mother’. Further reading
ACOG, Immunization During Pregnancy, Committee Opinion, Number 282, January 2003.
Barss VA. Immunizations in pregnant women. Uptodate, October, 2008.
General recommendation on immunization. Recommendation of the Advisory Committee on Immunization Practices (ACIP) and the American Academy of Family Physicians (AAFP). CDC. MMWR 2002; Recomm Rep; 51(RR-2):1–35.
Guidelines for Vaccinating Pregnant Women, from recommendations of the Advisory Committee on Immunization Practices (ACIP), October 1998 (Updated May 2007), Centers for Disease Control and Prevention (CDC), Department of Health and Human Services (DHHS).
Guidelines Principles for Development of ACIP Recommendations for Vaccination during Pregnancy and Breastfeeding, April 2008.
Lee EV. Infectious disease. In: Medical Care of pregnant patient. ACP Women’s Health Series. Philadelphia: American College Of Physicians 2000 Chapter 13
Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP). CDC. MMWR 1996; 45 (No. RR-15): 11. Internet resources
www.cdc.gov/mmwr/preview/mmwrhtml/rr5102a1.htm.
www.ACOG.org
www.cdc.gov/vaccines/pubs/downloads/f_preg_chart.pdf
www.cdc.gov/vaccines/pubs/preg-guide.htm
Table 8.23.1 Active immunization during pregnancy


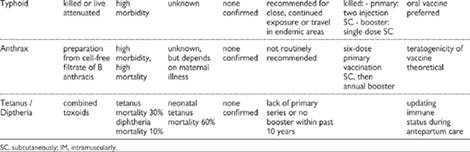
Table 8.23.2 Passive immunization during pregnancy
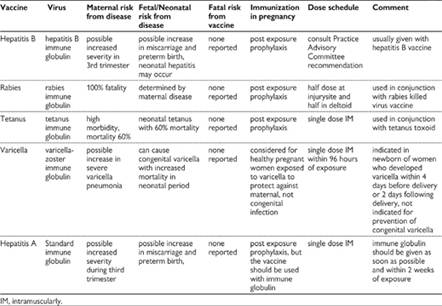
Inflammatory bowel disease Definition
Inflammatory bowel disease (IBD) is divided into Crohn’s disease and ulcerative colitis (UC). These are chronic inflammatory diseases of the gastrointestinal tract. Epidemiology
• IBD is more common in the Western World than Africa or Asia. It usually presents in young adults.
• Crohn’s affects women and men equally with incidence of 5 in 100 000 and prevalence of 0.5 in 1000.
• UC is more common in women, with an incidence of 5–10 in 100 000 and prevalence of 0.8–1 in 1000.
• The incidence and prevalence of IBD has increased over the last 50 years, but the reasons are unknown. Pathology
• Crohn’s disease: granulomatous inflammation extending beyond the submucosa, affecting any part of the gastrointestinal tract from the mouth to anus, in a patchy distribution (skip lesions).
• UC: mucosal and submucosal inflammation with crypt abscesses. It Always affects the rectum and extends proximally continuously to affect a variable proportion of the colon. Causes
The causes are unknown, although 5–20% have an affected family member. Susceptibility genes have been located. Genetics, infection, autoimmunity, and environmental toxins are all likely to play a part. Crohn’s is more common in smokers, whereas UC is more common in nonsmokers. Clinical features
• Crohn’s disease affects both the ileum and the colon in half of cases. The terminal ileum and colon may also be commonly involved in isolation. Symptoms will depend on the site of the bowel affected.
• UC affects only the colon.
General symptoms
• Malaise
• Tiredness
• Anorexia.
Symptoms related to ileitis
• Cramping mid-abdominal pain
• Diarrhoea
• Weight loss.
Symptoms related to colitis
• Liquid diarrhoea
• Urgency of defaecation and tenesmus
• Rectal bleeding (mixed in with stool)
• Passage of mucus per rectum
• Lower abdominal pain (less frequent).
Symptoms related to proctitis
• Fresh blood passed per rectum.
Signs
• Fever, dehydration, anaemia, weight loss, abdominal distension and tenderness, perianal disease (Crohn’s).
Exra-intestinal manifestations (especially with colonitis)
• Clubbing
• Mouth ulcers
• Arthritis: large joints, sacroiliitis, ankylosing spondylitis
• Eyes: conjunctivitis, iritis, episcleritis
• Biliary tract: gallstones, ascending/sclerosing cholangitis
• Skin: erythema nodosum, pyoderma gangrenosum. Investigations
• Sigmoidoscopy ± colonoscopy and mucosal biopsy to confirm mucosal inflammation. Histology will distinguish between Crohn’s disease and UC.
• ↑ WCC, ↑ C-reactive protein (CRP) (inflammation)
• ↓Ca2+, vitamin D, iron, folate, B12 (terminal ileal disease)
• Blood cultures (if febrile)
• AXR: if suspecting colonic dilatation/toxic megacolon (fetal risks minimal)
• MRI: if suspecting colonic dilatation/toxic megacolon/perforation
• Avoid barium enema and small bowel contrast studies in pregnancy Effect of pregnancy on IBD
Pregnancy does not affect IBD, but limits the ability to perform some investigations and use some treatments.
Predictors of active IBD in pregnancy
Active IBD/flare at conception: likely to stay active during pregnancy
New-onset IBD in pregnancy (usually occurs in first or second trimester)
• IBD quiescent at conception: similar frequency of exacerbations in pregnancy as when not pregnant.
• Exacerbations in inactive Crohn’s disease usually occur in the first trimester and in inactive UC are usually in the first two trimesters.
• Postpartum flare is more common in Crohn’s disease, but not in UC. Effect of IBD on pregnancy
Fertility: reduced in active Crohn’s disease
If disease quiescent at conception, rates of miscarriage, stillbirth, fetal anomaly, and live births are unaltered
Active disease is associated with worse pregnancy outcome. Flares
• at conception: increased miscarriage rates
• in pregnancy: increased prematurity.
Low birthweight babies more common irrespective of disease activity.
Previous surgery:
• tolerated well if disease inactive
• stomas and inactive disease: most women have normal deliveries at term
• ileostomy: dysfunction can occur in the second trimester with peristomal cracking and bleeding from an enlarging abdomen. Intermittent intestinal obstruction can occur and is serious.
• Ileoanal anastomosis: good outcomes and vaginal births reported. Management
Prepregnancy counselling
• Determine disease activity and optimize control.
• Recommend postponing pregnancy if IBD is active, and conceiving when IBD is in remission.
• Replace methotrexate with a more suitable drug (see below).
• Establish nutritional status and supplement with calcium, Vitamin D, iron, folic acid, and Vitamin B12 if deficient.
• If using an aminosalicylate (folate antagonist) add 5 mg of folic acid preconceptionally and during pregnancy.
• Encourage cessation of smoking.
During pregnancy
Management of chronic disease and acute attacks is similar to outside pregnancy. Multidisciplinary care with gastroenterologists and obstetricians is important with input from colorectal surgeons in severe cases.
• Continue with maintenance medications to reduce relapse rate
• Continue 5-mg folic acid if on an aminosalicylate
• Distinguish a flare of IBD from other conditions, e.g. abdominal pain
• normal pregnancy: constipation or gastro-oesophageal reflux
• unrelated to pregnancy: appendicitis, cholelithiasis, pancreatitis, pre-eclampsia
• Fetal growth scans.
If flare of IBD suspected, perform
full blood count, urea and electrolytes, liver function tests, CRP, amylase, albumin, and stool culture
flexible sigmoidoscopy or rigid proctoscopy to assess disease activity
If complications suspected, imaging may be required
Drug treatment
• Aminosalicylates (sulfasalazine, mesalazine, balsalazine): safe throughout pregnancy and breastfeeding. Sulfasalazine splits into sulfapyridine and the active compound 5-aminosalicylic acid (5-ASA) in the colon. Continue as maintenance or to induce remission in colonic Crohn’s disease or UC. Available orally or as rectal enemas.
• Oral and rectal corticosteroids can be used in pregnancy. There is a very slight increase in facial clefts with high-dose prednisolone used in the first trimester, but in a disease flare the benefits outweigh the risks.
• Azathioprine has extensive safety data from use in pregnant women with renal transplants and SLE. Azathioprine should be continued in women who require this to remain in remission. It can also be used as a steroid-sparing drug. It takes several weeks to take effect if started in pregnancy.
• Metronidazole and ciprofloxacin are not associated with adverse fetal effects with short-term use.
• Methotrexate results in miscarriage and is a teratogen and should not be used in pregnancy. Pregnancy should be avoided for at least 3 months following its discontinuation.
• Ciclosporin has good safety data from use in pregnant women with renal transplants. It is associated with intrauterine growth restriction. Its use is reserved to severe flares of IBD in pregnancy.
• Infliximab (anti-tumour necrosis factor-α): there are reports of successful use of this in severe flares of IBD. Reassuring safety data are emerging from its use in pregnant women.
Medical treatment of a flare of IBD in pregnancy Colonic disease
Start with topical corticosteroid enemas and a topical or oral aminosalicylate.
Second-line treatment is with oral steroids (20-40mg).
Hydrocortisone can be used if oral treatments are not tolerated.
Poor response to steroids demands the use of third-line treatments such as ciclosporin or infliximab. Ileal disease
Start with oral steroids and aminosalicylates.
Cyclosporin or infliximab are rarely required.
Surgery
Surgery should never be delayed because of pregnancy.
For indications similar to non-pregnant state:
• IBD not responsive to medical treatment
• obstruction
• haemorrhage
• perforation
• toxic megacolon.
Delivery
• Vaginal delivery is usually preferable, particularly in the presence of previous abdominal surgery which may have resulted in extensive intraperitoneal adhesions. Women with stomas can deliver vaginally.
• Caesarean section should be performed for
• obstetric indications
• severe active or chronic peri-anal Crohn’s disease with a scarred or deformed rectum and perineum (delayed healing of episiotomies and risks of fistula formation).
• Caesarean section can be considered in those with impaired anal continence.
• Total proctocolectomy and ileal pouch anal anastomosis: successful vaginal deliveries have been reported despite theoretical concerns regarding anal sphincter integrity at delivery. Complications
Crohn’s disease
• Perforation
• Stricture formation
• Peri-anal disease
• Fistulae
• Abscess formation.
Ulcerative Colitis
• Dilatation of colon/toxic megacolon
• Malignancy. Contraception
• Absorption of oral hormonal contraceptives may be reduced by small bowel involvement/malabsorption.
• If on antibiotics, reduced efficacy of oestrogen containing contraceptives
• Recommend:
• Copper IUCD
• Non-oral progestogen-based methods e.g. levonogestrel intrauterine system or implanon. Further reading
Ferguson CB, Mahsud-Dornan S, Patterson RN. Inflammatory bowel disease in pregnancy. BMJ 2008;337:a427.
Alstead EA, Nelson-Piercy C. Inflammatory bowel disease in pregnancy. Gut 2003;52:159–61.
Cornish J, Tan E, Teare J, et al. A meta-analysis on the influence of inflammatory bowel disease on pregnancy. Gut 2007;56:830–7.
Caprilli R, Gassull MA, Escher JC, et al. European evidence based consensus on the diagnosis and management of Crohn’s disease: special situations. Gut 2006;55(Suppl 1):i36–58.
Faculty of Family Planning and Reproductive Healthcare Clinical Effectiveness Unit. FFPRHC Guidance (July 2003). Contraceptive choices for women with inflammatory bowel disease. JFFPRHC 2003;29:127–135. www.ffprhc.org.uk Jaundice Definition
Jaundice is a yellow discolouration of the skin and sclera due to an increase in the level of serum bilirubin. Unconjugated bilirubin is produced from the breakdown of haem and is conjugated in the liver. Causes
Prehepatic
• Increased production of unconjugated bilirubin:
• haemolysis, e.g. HELLP (haemolysis, elevated liver enzymes, low platelets) syndrome, haemolytic uraemic syndrome (HUS), thrombotic thrombocytopenic purpura (TTP), malaria
• haemoglobinopathies (e.g. sickle cell disease, thalassaemia).
• Reduced hepatic uptake of unconjugated bilirubin:
• Severe congestive heart failure.
Hepatic
• Reduced hepatic conjugation of bilirubin
• Gilbert’s syndrome
• Crigler–Najjar syndrome.
• Reduced excretion of conjugated bilirubin
• hepatocellular injury, e.g. viral hepatitis, drugs (e.g. paracetamol overdose), chronic active hepatitis, sepsis
• infiltration of liver, e.g. acute fatty liver of pregnancy (AFLP), malignancy
• obstetric cholestasis (OC)
• congenital defects, e.g. Dubin–Johnson and Rotor syndromes.
Cholestatic (obstructive)
• Extrahepatic bile duct obstruction
• gallstones (choledocholithiasis)
• ascending cholangitis
• acute pancreatitis
• primary biliary crrhosis. History
• Duration of jaundice, malaise, anorexia, nausea, vomiting, fever, rash, weight loss
• Other symptoms of liver disease: Itching, abdominal pain, dark urine, pale stools, bruising, bleeding
• Recent travel abroad
• Drug treatment/abuse/overdose, amount of alcohol
• Recent tattoos or piercings
• Previous jaundice, gallstones. Signs
• Signs of chronic liver disease are common in normal pregnancy, e.g. spider naevi, palmar erythema
• Upper abdominal tenderness
• Palpable gall bladder, hepatomegaly, splenomegaly.
Worrying signs: call ITU ± liver unit Drowsiness, confusion, slurred speech, tachycardia, hypotension, severe hypertension, bleeding, tremor/flap, poor coordination, hypoxia Initial investigations
• Urine: dipstick for protein, blood, urobilinogen (prehepatic/hepatic jaundice), bilirubin (hepatic/obstructive jaundice)
• Bloods: full blood count, reticulocytes, blood film, clotting, U+E, LFT, amylase ± paracetamol levels, hepatitis serology (A, B, C ± E), EBV, CMV, blood cultures
• USS abdomen: gallstones, dilated common bile duct. Further investigations
As depicted by initial results and differential diagnoses: see individual diseases. Also refer to chapter on Liver Diseases which covers other conditions that can present with jaundice including acute fatty liver of pregnancy and obstetric cholestasis. Gilbert’s syndrome
Benign disease: develops as unconjugated hyperbilirubinaemia with an acute illness. Usually incidental finding of slightly raised bilirubin. No concerns in pregnancy. Gall bladder disease
Incidence
• Gallstones: 2–8% of pregnant women: ↑ with parity
• Biliary sludge: in 30% women by the end of pregnancy
• Acute cholecystitis in 0.1% of pregnancies.
Causes
Gall bladder stasis and lithogenic bile (from an increase in bile cholesterol and a reduction of bile acids) leads to increased formation of sludge and gallstones in pregnancy
Clinical features
• Asymptomatic
• Biliary pain in right upper quadrant
• Acute cholecystitis
• Associated with obstetric cholestasis. Acute cholecystitis
Definition
Impacted gallstone in neck of gallbladder with inflammation
Clinical
• Severe continuous right upper quadrant pain (can radiate in a band round to back)
• nausea, vomiting
• pyrexia
• tender over gall bladder (Murphy’s sign +ve)
• peritonitis
• jaundice if stones in common bile duct (CBD).
Diagnosis
• ↑ WCC, ↑ CRP
• Abnormal LFT
• Amylase can double. If higher consider pancreatitis or stones in CBD
• USS gallbladder: pericholecystic fluid, gallbladder distension and thickening of wall
• Endoscopic retrograde cholangiopancreatography (ERCP) if impacted stone suspected
• Technecium-99 HIDA scan for CBD stones (minimal fetal radiation).
Differential diagnosis
• Acute pancreatitis
• Pneumonia
• Cholangitis
• AFLP
• Peptic ulcer disease
• HELLP
• Appendicitis
• Viral hepatitis.
Management
• Similar to non-pregnant
• Conservative management resolves symptoms in 75% but increased incidence of preterm delivery and relapse in pregnancy compared with surgery. Usually defer definitive surgery until postpartum:
• Keep nil by mouth and administer i.v. fluids
• Antibiotics
• Analgesia (avoid NSAIDs)
• Surgery required if
• Non-resolution of symptoms
• Recurrent symptoms
• CBD obstruction
• Perform surgery in second trimester if necessary
• Laparoscopic cholecystectomy (difficult with later gestations)
• Open cholecystectomy
• Endoscopic removal of CBD stones.
Complications
• Pancreatitis
• Cholangitis. Acute and chronic viral hepatitis
This is the commonest cause of jaundice worldwide
Causes
• Hepatitis A, B, C, D, E (Table 8.25.1)
• Cytomegalovirus (CMV)
• Ebstein–Barr Virus (EBV)
• Herpes simplex virus (HSV)
Hepatitis E (HEV) and herpes simplex hepatitis can cause adverse pregnancy outcome. The other viral hepatitis run a similar cause outside pregnancy (Table 8.25.1).
Hepatitis D (HDV) is dependent on hepatitis B (HBV) for transmission.
• Co-infection of HBV and HDV leads to a more severe form of acute hepatitis than HBV alone.
• Superimposed infection of a chronic carrier of HBV with HDV can lead to another episode of clinical hepatitis and can hasten the course of chronic liver disease. Herpes simplex hepatitis
Incidence
Very rare.
Pathology
• Usually primary infection with HSV type 2.
• Liver focal haemorrhagic necrosis and intranuclear inclusion bodies.
Clinical
• Initial non-specific symptoms, e.g. fatigue, pyrexia
• Abdominal pain
• Herpetic vesicles may be absent
• ± jaundice
• Fulminant liver failure
• Disseminated infection.
Diagnosis
• Very high liver transaminases
• Mildly raised bilirubin
• Prolonged prothrombin time
• Serology: IgM HSV+
• Liver biopsy: histology and viral culture.
Treatment
Intravenous acyclovir
Prognosis
Poor without treatment in pregnant women Acute pancreatitis
Incidence
• Same as non-pregnant 1 in 10 000
• Attacks are usually mild and occur in the third trimester.
Causes
• Gallstones
• Alcohol
• Hypercalcaemia (primary hyperparathyroidism)
• Hypertriglyceridaemia (from underlying disorder).
Clinical features
Symptoms
• Constant severe epigastric pain radiating straight through to back, improved with sitting forward
• Nausea, vomiting, anorexia.
Signs
• Tachycardia, ±, ↑RR, ↓BP, low-grade pyrexia
• Mild jaundice
• Epigastric tenderness with peritonitis
• Reduced or absent bowel sounds (paralytic ileus)
• Cullen’s sign (bruised umbilicus), Grey–Turner’s sign (bruised flanks)
• Pleural effusions, ascites.
Diagnosis
• serum amylase four times normal (can be >1000 U/L): rise may be masked by high lipids
Severe disease: liaise with ITU
Hypoxic, pyrexial, hypotensive, marked tachypnoea, prolonged paralytic ileus, ascites, pleural effusions
• ↑serum lipase more specific
• ↑WCC, ↑CRP, ↑glucose, ↓corrected Ca2+
• Abnormal LFTs
• ± Deranged clotting
• ABG
• USS upper abdomen: gallstones
• CT abdo: pancreatic swelling.
Table 8.25.1 Viral hepatitis in pregnancy


Differential diagnosis
Mildly raised amylase also occurs in
• cholecystitis
• peptic ulcer perforation
• bowel obstruction
• ectopic pregnancy.
Management
Making the correct diagnosis is very important to avoid an unnecessary laparotomy.
Supportive NOT surgical (unless CBD obstruction: biliary pancreatitis):
• Keep nil by mouth
• Resuscitate with intravenous fluids
• Facial O2
• Analgesia: pethidine, NOT morphine (contraindicated as causes spasm of sphincter of Oddi)
• Urinary catheter and monitor fluid balance
• Nasogastric tube (usually have) paralytic ileus
• Prophylactic thromboprophylaxis with LMWH.
Regular monitoring of Pulse, BP, Hb, WCC, U+E, LFT, amylase, prothrombin time, glucose, calcium.
Complications
Requires liaising with ITU
• DIC
• Renal failure
• Respiratory failure: liaise with ITU
• Thrombosis
• Pseudocyst/abscess
• Sepsis
• Chronic pancreatitis
• Fetal loss. Further reading
Beasley RP, Hwang LY, Lee GC, et al. Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B virus infections with hepatitis B immune globulin and hepatitis B vaccine. Lancet 1983;2:1099–102.
Elinav E, Ben-Dov IZ, Shapira Y, et al. Acute hepatitis A infection in pregnancy is associated with high rates of gestational complications and preterm labour.
European Paediatric Hepatitis C Virus Network. Effects of mode of delivery and infant feeding on the risk of mother-to-child transmission of hepatitis C virus. Br J Obstet Gynaecol 2001;108:371–7.
Hernandez A, Petrov MS, Brooks DC, Banks PA, et al. Acute pancreatitis and pregnancy: a 10-year single center experience. J Gastrointest Surg 2007;11:1623–7.
Kumar A, Beniwal M, Kar P, et al. Hepatitis E in pregnancy. Int J Gynaecol Obstet 2004;85:240–4.
Mendez-Sanchez N, Chavez-Tapia NC, Uribe M. Pregnancy and gallbladder disease. Ann Hepatol 2006;5:227–30.
Patra S, Kumar A, Trivedi SS, et al. Maternal and fetal outcomes in pregnant women with acute hepatitis E virus infection. Ann Intern Med 2007;147:28–33.
Yeung LT, King SM, Roberts EA. Mother-to-infant transmission of hepatitis C virus. Hepatology 2001;34:223–9.
Listeriosis Definition
Listeriosis refers to infection by the organism Listeria monocytogenes and its manifestations are host dependent. Epidemiology
• In the USA, surveillance data from 1997 showed that 2500 people become seriously ill each year as a result of listeriosis and 500 die (CDC).
• Neonatal infection is the most common clinical form of the disease
• Listeriosis is 20 times more likely in pregnancy and 300 times more likely in AIDS
• Age >65 years is associated with increased rates of Listeriosis. Aetiology
Listeria monocytogenes is a gram-positive rod-shaped bacterium that contaminates raw food such as soft cheeses, cured meats, and prepackaged raw items such as smoked fish, sandwiches, or salads. Infection occurs when contaminated food is consumed by an at-risk individual.
The bacterium grows well at refrigeration temperatures (4–10°C)
Neonatal infection
• Caused predominantly by maternal infection in pregnancy, listeria is transmitted to the fetus via ascending or transplacental means.
• Nosocomial infection has been reported.
Pregnancy
• Pregnant women are particularly at risk in the second and third trimester due to decreased cell-mediated immunity.
Immunocompromised states and elderly people
• Immunocompromised states increase the risk of invasive infection due to decreased cell-mediated immunity.
• Ageing causes anatomic and functional changes and immune changes such as decreased macrophage efficiency increasing the risk of complicated infection. Prognosis
• Immunocompetent hosts may be asymptomatic or have acute febrile gastroenteritis, and nearly all make a full recovery within 2 days
• Among pregnant women, however, 22% of cases result in stillbirth or neonatal death, and spontaneous abortion is common.
• Seventy per cent of pregnancies with listeriosis result in preterm delivery at or Mexican-style cheeses unless they are labelled as pasteurized
• Do not eat refrigerated pâtes, meat spreads, packaged salads containing meat, or smoked seafood. Canned items are safe to eat, or smoked items may be eaten if they are cooked.
• Thoroughly wash raw vegetables before consuming
• Do not drink raw milk or other foods containing unpasteurized milk.
• Keep refrigerator at 40°F (4.4°C) or lower and freezer at 0°F (–17.8°C) or lower. Further reading
Ault K. Faro S. Bacteria and protozoans in pregnancy: a sample of each. Clin Obstet Gynecol 1993;36:878–85.
Bortolussi R, Mailman TL. Aerobic gram-positive bacilli, clinical manifestations. In: Cohen and Powderly (eds) Infectious diseases, 2nd edn. St Louis: Mosby Elsevier 2004: Chapter 226.
Eckburg PB, Montoya JG, Vosti KL. Brain abscess due to Listeria monocytogenes: five cases and a review of the literature. Medicine 2001;80:223.
Heymann D. (ed.). Control of communicable diseases manual, 18th edn. Washington, DC: American Public Health Association 2004.
Lorber B. Listeriosis. Clin Infect Disease 1997;24:1.
Lorber B. Listeria monocytogenes. In: Mandell, Bennet, and Dolin (eds) Principles and practice of infectious diseases, 6th edn. Philadelphia: Churchill Livingstone 2005: Chapter 204.
Louria D. Sen P. Sherer C, Farrer W. Infections in older patients: a systematic clinical approach. Geriatrics 1993;48:28–34.
Mylonakis E. Hohmann EL, Calderwood SB. Central nervous system infection with Listeria monocytogenes: 33 years’ experience at a general hospital and review of 776 episodes from the literature. Medicine 1998;77:313. Internet resources
Listeriosis: Center for Disease Control and Prevention: National Center for Zoonotic, Vector-Borne, and Enteric Diseases www.cdc.gov/nczved/dfbmd/disease_listing/listeriosis_g.html
Liver disease
It is important to use pregnancy-specific ranges when interpreting liver function tests (LFT) in pregnancy (Table 8.27.1). Obstetric cholestasis (OC)
Definition
Intrahepatic cholestasis occurring in the second and third trimesters of pregnancy and resolving postnatally.
Incidence
• In Europeans 0.5–1.5% of pregnancies.
• More common in South Americans and South Asians.
Causes
• Genetic predisposition to cholestatic effects of elevated oestrogen ± progesterone levels
• Mutations of MDR3 gene identified.
Clinical features
Specific points in history
• Prepregnancy pruritis on oral contraceptive pill or in luteal phase of menstrual cycle
• Personal or family history of pruritis in pregnancy
• Personal or family history of previous unexplained stillbirth
• Onset usually in third trimester, but may be earlier.
Symptoms
• Pruritis generalized, but typically includes palms of hands and soles of feet. Disappears postnatally.
• No rash
• Dark urine, pale stools
Signs
• Excoriation of skin following scratching
• Jaundice 10%.
Diagnosis (of exclusion)
• Abnormal liver enzymes* (use normal ranges for pregnancy): moderately raised
• Raised bile acids (BAs)*
• Exclude other causes if LFT or BAs abnormal:
• Serology: hepatitis A, B, C† –ve
• Serology: CMV IgM –ve, EBV IgM –ve
• Occasionally need to exclude hepatitis E
• Antimitochondrial and anti-smooth muscle Ab –ve
• Liver USS normal (may have gallstones†).
Table 8.27.1. Normal pregnancy values of liver function tests

* May be normal initially
† OC can occur in association
Differential diagnosis
• Hepatitis due to hepatitis A, B, or C, CMV, or EBV
• Chronic active hepatitis (antismooth muscle Ab +ve)
• Primary biliary cirrhosis (antimitochondrial Ab +ve)
Effect of OC on pregnancy
• Spontaneous preterm labour and delivery‡
• Meconium-stained liquor‡
• Fetal distress‡
• Stillbirth‡ 2% (when delivered 37 weeks; therefore, deliver by 37–38 weeks. Continuous fetal monitoring in labour.
Postnatal
• Neonate should be given i.m. vitamin K.
• LFT and BA normalize within days or a few weeks.
• Contraception: avoid hormonal contraception particularly oestrogen-containing methods. If used, monitor LFT and BA and discontinue if deranged.
• Hormone replacement therapy can be used.
Referral to hepatologist
• If LFT/BA remain abnormal postnatally
• Anyone diagnosed with hepatitis B or C Acute fatty liver of pregnancy (AFLP)
Definition
Reversible peripartum liver and renal impairment usually occurring in the third trimester, can be lethal
Incidence
1 in 20 000 pregnancies
Causes
• On same disease spectrum as pre-eclampsia
• Twenty per cent with AFLP are heterozygous for long-chain 3-hydroxy-acyl-coenzyme A dehydrogenase (LCHAD) deficiency (a disorder of mitochondrial fatty acid oxidation). The Fetus is homozygous.
Pathology
Microvesicular fatty infiltration of hepatocytes.
Risk factors
• Primigravidae
• Multiple pregnancies (14-fold increased risk)
• Male fetus.
Clinical features
Presentation varies from asymptomatic to fulminant liver failure, but usually gradual onset.
Symptoms
• Gradual onset nausea, anorexia, malaise (early)
• Vomiting, abdominal discomfort (later)
• Polyuria, polydipsia (transient diabetes insipidus).
Signs
• Jaundice
• Mild hypertension and mild proteinuria
• Ascites
• Hepatic encephalopathy in fulminant hepatic failure
• Confusion
• Liver flap.
Diagnosis
• ↑liver transaminases (AST up to 3000), ↑ALP
• ↑bilirubin
• ↓albumin
• hypoglycaemia
• deranged clotting (initially ↓antithrombin levels, then prolonged prothrombin time)
• ↑WCC
• renal impairment (↑urea, ↑creatinine)
• ↑urate
• ABG: metabolic acidosis
• Liver biopsy and fat stains (not done in practise due to coaglopathy)
• Imaging of liver with USS, CT or MRI is not discriminatory.
Important markers of severity of AFLP
• Hypoglycaemia
• Coagulopathy
• Falling albumin.
Differential diagnosis
• HELLP syndrome
• Fulminant viral hepatitis.
Management
• Multidisciplinary involvement of obstetricians, hepatologists, nephrologists, haematologists and intensivists is essential, usually in ITU unless mild disease
• Early discussion with specialist liver unit
• Degree of abnormality of LFT not prognostic.
Supportive management
• Adequate fluid balance (to maintain renal perfusion)
• Correct coagulopathy: FFP, ± antithrombin concentrate, platelets, cryoprecipitate
• Hypoglycaemia: 50% dextrose initially then 10% dextrose infusion
• Renal failure: dialysis
• Liver dysfunction: N-acetyl cysteine infusion.
Rapid delivery of baby (after correcting glucose and clotting)
• Remember bleeding risks with caesarean section
• Cover delivery with antibiotics
Fulminant hepatic failure and encephalopathy
• Transfer to specialist liver unit
• May need liver transplant
Postnatal
• Most women improve 1–4 weeks after prompt delivery and treatment
• Cholestatic phase with ↑bilirubin and ALP may persist longer
• Postpartum haemorrhage requiring repeated surgery not uncommon
• Avoid NSAIDs
• Screen baby for defects of fatty acid oxidation.
Table 8.27.2 differentiating features between AFLP and HELLP

Complications
• Maternal mortality varies from 1.8% (based on a UK population study) up to 19% (based on hospital studies)
• Perinatal mortality 10%.
Recurrence
More likely if heterozygous for LCHAD deficiency HELLP syndrome
Definition
Part of the spectrum of pre-eclampsia. Acronym HELLP: Haemolysis, Elevated Liver enzymes, Low Platelets
Incidence
Twenty per cent of severe pre-eclamptics.
Pathology
Endothelial dysfunction (as for pre-eclampsia)
Microangiopathic platelet activation and consumption.
Clinical features
Twenty-five per cent occur postnatally.
Symptoms
• Malaise
• Nausea
• Epigastric or right upper quadrant pain
• Vaginal bleeding from placental abruption.
Signs
• Hypertension (might not be severe) ± proteinuria
• Tender right upper quadrant
• Haematuria/coke-coloured urine
• Jaundice (occasionally).
Diagnosis
• Haemolysis (infrequent):
• peripheral blood film: red cell fragments
• ↑lactose dehydrogenase (LDH >600 U/l)
• ↑unconjugated bilirubin
• falling haemoglobin
• LFT: ↑transaminases (AST >70 U/l)
• Platelets 2005;42:1399–405.
Glanz A, Marschall HU, Mattsson LA. Intrahepatic cholestasis of pregnancy. Relationships between bile acid levels and fetal complication rates. Hepatology 2004;40:467–74.
Janczewska I, Olsson R, Hultcrantz, et al. Pregnancy in patients with primary sclerosing cholangitis. Liver 1996;16:326–30.
Katz L, de Amorim MM, Figueiroa JN, et al. Postpartum dexamethasone for women with hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome: a double-blind, placebo-controlled, randomized clinical trail. Am J Obstet Gynecol 2008;198:283. e1–8.
Knight M, Nelson-Piercy C, Kurinczuk JJ, et al. UK Obstetric Surveillance System. A prospective national study of acute fatty liver of pregnancy in the UK. Gut 2008;57:951–6.
Royal College of Obstetricians and Gynaecologists. Obstetric Cholestasis. Guideline No. 43. London: RCOG 2006. Available on-line: www.rcog.org.uk/resources/Public/pdf/obstetric_cholestasis43.pdf
Sibai BM, Ramadan MK, Usta I, et al. Maternal morbidity and mortality in 442 pregnancies with haemolysis, elevated liver enzymes and low platelets (HELLP syndrome). Am J Obstet Gynecol 1993;169:1000–6.
Sternlieb I. Wilson’s disease and pregnancy. Hepatology 2000;31:531–2.
Tan J, Surti B, Saab S. Pregnancy and cirrhosis. Liver Transpl 2008;14:1081–91. Internet resources
The Obstetric Cholestasis Support website: www.ocsupport.org.uk
Measles: rubeola Definition
Rubeola, measles, is an acute, highly infectious illness caused by the rubeola virus that is characterized by cough, coryza, fever, and a maculopapular rash. Epidemiology
Although rubeola is highly contagious, the infection is uncommon in industrialized nations because of a safe and effective vaccine; it has not been considered endemic in the USA since 2000. In developing countries, there are over 20 000 000 cases per year with an estimated 242 000 deaths, mainly children, in 2006. The majority of the deaths occurred in South-East Asia.
Most epidemics occur in the spring and summer of alternate years. Since maternally derived immunity is effective up to 6–9 months of age, the peak age of infection is about 4 years. Aetiology
The rubeola virus belongs to the Paramyxoviridae family, which are enveloped, negative single-stranded RNA viruses. Although the virion is very labile, it remains infective in droplet form in air for several hours. Spread is by direct contact with droplets from respiratory secretions of infected persons. Clinical features
Incubation period
The incubation following exposure lasts 10–14 days. Exposure to the virus results in entry via the respiratory mucosa and/or conjuctiva. The virus replicates locally before dissemination into regional lymphatics and eventually the bloodstream. Although it is typically asymptomatic during this period, there may be transient respiratory symptoms, fever, or a morbilliform rash.
Prodromal illness
A second viraemia occurs several days after the first and is associated with the appearance of symptoms that include high, spiking fevers, irritability, nasal and conjunctival discharge, a cough, and loose stools. Koplik’s spots, white, irregular lesions that appear on the buccal mucosa typically opposite the upper premolars on day 2 of the fever, are pathognomonic of prodromal measles.
Rash
On days 3–4, the erythematous maculopapular rash appears, initially at the hairline involving the forehead, behind the earlobes, and upper part of the neck. It spreads downwards to the face, neck, upper extremities, and trunk; it reaches the feet by the third day. The early lesions become confluent, although peripherally, the lesions remain discrete. It begins to fade by the third day in the order of its appearance. With disappearance, a fine branny desquamation may be noted in heavily affected areas excepting the hands and feet, a feature which distinguishes it from scarlet fever.
Convalescence
The rash appears as the temperature reaches its peak. Koplik’s spots begin to slough. The coryza and conjunctivitis become profuse and the cough is persistent. Within the next 24–36 hours, the temperature falls and the remainder of the symptoms begin to clear, although the cough may last for weeks. Fever lasting beyond the third day of the rash is probably caused by secondary infection. Diagnosis
Although the clinical course is often typical, the WHO recommends that the diagnosis be confirmed by laboratory tests. In the USA, the infection is reportable to the local health department. A serodiagnosis can be made with an IgM enzyme-linked immonosorbent assay using serum or saliva samples. Virtually 100% will be positive by the end of the first week. Differential diagnosis
This varies with the stage of the illness. The prodromal phase symptoms are typical of a common cold except for the presence of fever. Other considerations are influenza, adenovirus, dengue virus, or respiratory syncytial virus infection.
During the exanthem phase, Mycoplasma pneunomiae, rubella, Rocky Mountain spotted fever, infectious mononucleosis, scarlet fever, Kawasaki disease, toxic shock syndrome, dengue, roseola, erythema infectiosum, and drug eruptions are in the differential. The intensity of the rash followed by its brownish discolouration and the associated symptoms of coryza and conjunctivitis are distinguishing features of rubeola. Management
Vitamin A
Since measles mortality is inversely related to serum retinol levels, children from countries where health care and nutrition are compromised should receive vitamin A at the time of diagnosis. An oral dose of 10 000 IU is recommended for children up to 1 year of age; those over 1 year should receive 20 000 IU. Children with keratoconjunctivitis should receive a second dose 1 month later.
Antibiotics
Measles will generally run a fairly typical, self-limiting course, resulting in full recovery with supportive therapy such as hydration and antipyretics. Since secondary bacterial infections are frequent, however, these should be treated appropriately as soon as a diagnosis is made.
Complications
• Secondary bacterial infections, including suppurative otitis media and bronchopneumonia, are common and often severe.
• With dissemination of the virus, there can be involvement of other organ systems with manifestations that include myocarditis, pericarditis, hepatitis, mesenteric lymphadenopathy, and corneal ulceration.
• Post-infectious encephalitis occurs in 1 in 800–1600 cases and has a mortality of up to 15%. Fifty per cent of survivors have neurological sequelae.
• Subacute sclerosing panencephalitis is a rare (1 in 1 000 000 cases), late-appearing complication occurring most often in children who became infected under the age of 2 years. The onset is 3–10 years after the original illness and results in death within 2 years.
• Measles inclusion body encephalitis is seen most often in children who are immunosuppressed; the usual onset is 1–7 months after the original illness. Fever, neurological dysfunction and seizures progress over 3 or more weeks, resulting in a 75% fatality rate and severe neurological sequelae in survivors. Prevention
Pre-exposure prophylaxis
Live-attenuated measles vaccines introduced in the 1960s and 1970s have been highly effective in controlling epidemic disease as well as the rare neurological sequelae. Since immunization prior to age 9–12 months produces a short-lasting immunity and immunization after age 1 year leaves a window of susceptibility due to the loss of maternally derived antibodies, a two-step immunization programme is recommended. The first dose is given between the ages of 12 and 15 months and a second booster dose is given between the ages of 3 and 5 years. The first dose is recommended between the ages of 6 and 9 months in developing countries. A 96% seroconversion rate can be expected.
Common adverse effects from the immunization can occur and include:
• a mild febrile illness with a transient rash at 7 days following the first immunization
• mild allergic reactions such as urticaria or other, nonanaphylactic, reactions.
Although generally contraindicated in immunosuppressed patients, the measles live vaccine has been safely given to patients with asymptomatic and symptomatic HIV infection as long as the CD4 cell count is greater than 500.
Post-exposure prophylaxis
When given within 3 days of exposure, human immunoglobulin is effective in preventing measles as all commercially available immunoglobulin preparations contain high levels of antibodies. The recommended doses are as follows:
• less than 1 year of age: 250 mg of immunoglobulin
• ages 1–2 years: 500 mg of immunoglobulin
• age 3 or greater: 750 mg of immunoglobulin.
Public health initiatives
The WHO and UNICEF have developed a comprehensive strategy to sustainably reduce measles deaths. The strategy was endorsed by the World Health Assembly in 2003. The strategy includes
• strong routine immunization: vaccination of at least 90% of children at the age of 9 months
• a second opportunity for measles immunization: vaccination provided to all children aged 9 months to 15 years who did not previously receive a dose as well as those who did not develop immunity
• surveillance: confirmation of suspected cases of measles through blood collection and testing in accredited laboratories
• improved clinical management: vitamin A supplementation and antibiotic treatment of secondary infections. Further reading
Katz S. Measles (Rubeola). In: Gershon AA, Hotez PJ, Katz SL, (eds) Krugman’s infectious diseases of children, 11th edn. Philadelphia: Mosby 2004.
World Health Organization. Progress in global measles control and mortality reduction, 2000-2006. Weekly Epidemiological Record 2007;48:418–24.
Baringa JL, Skolnik PR. Clinical presentation and diagnosis of measles. UpToDate May 2008. Version 16.2.
Maldonado YA, et al. Early loss of passive measles antibody in infants of mothers with vaccine-induced immunity. Pediatrics 1995;96:447–50.
Butler JC, Havens PL, Sowel AL, et al. Measles severity and serum retinol (vitamin A) concentration among children in the United States. Pediatrics 1993;91:1176–81.
Bannister BA. Measles (Rubeola). In: Cohen J, Powderly WG, et al. (eds) Infectious diseases, 2nd edn. Philadelphia: Mosby 2004.
Strebel P, Cochi S, et al. The unfinished measles immunization agenda. J Infect Dis 2003;187(Suppl 1):S1–7. Internet resources
www.who.int/mediacentre/factsheets/fs286/en/index.html
www.measlesinitiative.org/index3.asp
Parvovirus
Parvovirus B19 is the cause of erythema infectiosum or ‘fifth disease’. These are among the smallest DNA viruses; humans are their only known hosts. It is composed of an icosahedral protein capsule without an envelope that contains a single strand of DNA.
The cellular receptor for B19 parvovirus is the erythrocyte P antigen, thus explaining their propensity to infect erythrocytes and precursors. Epidemiology
The prevalence of parvovirus B19 infection is common and it is spread worldwide. Infections are more common in schoolchildren, with 70% of cases occurring between 5 and 15 years of age. Seasonal peaks occur in the late winter and spring, with sporadic cases throughout the year. Transmission is via the respiratory route; the transmission rate is 15–30% among susceptible household contacts. In school outbreaks, secondary attack rates range from 10% to 60%. Nosocomial outbreaks show an attack rate of 30% among susceptible healthcare workers. It is also transmissible via blood or blood products; indeed the virus was first identified in blood bank specimens in the 1970s.
Sixty-five per cent of pregnant women have serological evidence of seroconversion and are thus immune. Daycare workers, teachers, and parents are at increased risk of seroconversion. Clinical approach
Clinical manifestations
The most common manifestation is erythema infectiosum, characterized by a malar rash with the characteristic ‘slapped cheeks’ appearance and a lace-like rash in the extremities. The rash may reappear for several weeks following stimulus, including changes in temperature, sunlight exposure, or emotional stress. Fever, malaise, and lymphadenopathy may accompany the infection. A symmetric arthropathy affecting most commonly the hands may also appear. Symptoms are self-limiting but may last for several months. Infection may be asymptomatic 20% of the time. Persistent infection, in patients unable to mount an appropriate immune response, is rare, and presents as pure red cell aplasia.
Fetal infection can be asymptomatic or instead an aplastic anaemia of varying severity may appear. Severe anaemia may cause high-output heart failure and non-immune hydrops.
Diagnosis
Serological testing can detect IgG and IgM antibodies to B19 Parvovirus through an enzyme-linked immunosorbent assay. Susceptible individuals will have both antibodies negative. Positive IgG and negative IgM signals immunity or infection more than 120 days prior. Recently infected patients will have positive IgM and negative IgG, and, finally, those who have had an infection more than 7 days but less than 120 days prior will show seropositivity to both G and M immunoglobulin.
Management during pregnancy
Transplacental transmission rates have been reported to be as high as 33% and fetal infection has been associated with spontaneous abortion, hydrops fetalis, and stillbirth. The rate of fetal loss is between 2% and 9%. In utero parvo-virus B19 infection is responsible for up to 18 % of cases of nonimmune hydrops.
For women exposed between the first and twelfth week of gestation, the risk of severe fetal involvement is 19%. This decreases to 15% for exposure between 13 and 20 weeks and drops down to 6% for infection occurring after 20 weeks.
Women who are exposed to Parvovirus should have their antibodies, both IgG and IgM, tested. Positive reaction to IgG shows old infection and no further workup is warranted. Susceptible women should have repeat serology in 3 weeks. In case of confirmed infection, maternal treatment is just supportive care since the infection is self-limited. Serial ultrasound examinations to evaluate the fetus for hydrops should be performed for 8–10 weeks after maternal illness; measurement of the middle cerebral artery peak systolic velocity can be useful to document fetal anaemia before hydrops ensues. It should be noted that although 33% of fetal hydrops resolves without treatment there are no reliable predictors for resolution versus fetal death, so cordocentesis and intrauterine transfusion are recommended when hydrops is present. If hydrops has not occurred by 8 weeks after maternal infection, it is unlikely to occur. Long-term developments of these fetuses appear to be normal (ACOG 2008). Preventative measures
Options for prevention are limited during outbreaks in which prolonged, close contact exposure occurs, such as schools, homes, or childcare settings. Exposure cannot be prevented by identifying and isolating affected persons since 20% of infections are asymptomatic and those who do become symptomatic are infectious before they develop symptoms. Exclusion of pregnant women from the workplace during an endemic period is controversial and excluding members of high-risk groups from work during an outbreak is not recommended (ACOG 2000). References
ACOGCompendium of selected publicationsPractice Bulletin #20. September 2008;651:654–5.
Bernstein H. Gabbe obstetrics, 5th edn. 2007: 1213–14.
Cosmi E, Mari G, Delle Chiae L, et al. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia resulting from parvovirus infection. Am J Obstet Gynecol 2002;187:1290.
Hernandez-Andrade E, Scheier M, Dezerega V, et al. Fetal middle cerebral artery peak systolic velocity in the investigation of non immune hydrops. Ultrasound Obstet Gynecol 2004;23:442.
Koch CW. Kliegman: Nelson textbook of pediatrics, 18th edn. Ch 248.
Pituitary disorders in pregnancy Physiological changes
The volume of the anterior pituitary increases progressively during pregnancy by up to 35%. This is mainly due to an increase in the number and size of the lactotrophic cells. Postpartum involution is slower if the woman breastfeeds. Prolactin levels increase up to 10-fold during pregnancy and return to normal by 2 weeks after delivery, unless the woman breastfeeds. This increase is thought to be mediated via increases in oestrogen and progesterone and is related to the initiation and maintenance of lactation.
Levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are suppressed by the concentrations of oestrogen and progesterone. Basal growth hormone (GH), antidiuretic hormone (ADH), and pituitary adrenocorticotrophic hormone (ACTH) are unaltered in pregnancy. Hyperprolactinaemia
Prolactinomas
Epidemiology
Prolactin-producing pituitary adenomas are the commonest pituitary adenomas encountered in pregnancy.
Pathology
They are classified according to size into microprolactinomas (10 mm in diameter).
Aetiology
Hyperprolactinaemia has multiple potential causes apart from prolactinomas:
• normal pregnancy
• hypothalamic and pituitary stalk lesions (leading to removal of dopaminergic suppression of prolactin secretion)
• empty sella syndrome
• hypothyroidism (thyroid-stimulating hormone stimulates lactotrophs)
• chronic renal failure
• seizures
• drugs, e.g. metoclopramide.
Prognosis
Effect of pregnancy on prolactinomas
The main risks are those posed by the potential expansion of the pituitary space-occupying lesion. This could potentially lead to visual field defects by impinging on the optic chiasma or to pituitary apoplexy with panhypopituitarism. This risk of symptomatic tumour expansion is 15% in untreated and 4.4% in treated patients with macroprolactinomas. The risk for symptomatic expansion of a microprolactinoma during pregnancy is minimal (1.6%).
Effect of prolactinomas on pregnancy
Hyperprolactinaemia is associated with amenorrhoea, reduced fertility and hypo-oestrogenaemia. Therefore, the majority are diagnosed preconceptually and the pregnancy would have been the result of treatment with dopamine-receptor agonists. There are no known adverse effects to the fetus and women with prolactinomas can breastfeed.
Clinical approach
Diagnosis
History
Prolactinomas may present with amenorrhoea, reduced fertility, galactorrhoea, frontal headache, visual field defects, or diabetes insipidus. In pregnancy, only the last three symptoms are discriminatory.
Examination and investigations
Formal visual field testing should be performed to confirm any symptoms of visual fields to confrontation.
Prolactin levels are of no value in the diagnosis of these patients as they are elevated during pregnancy. If a pituitary tumour is suspected, other pituitary function tests (thyroid function tests) should be performed.
Diagnosis in pregnancy largely relies on findings of pituitary magnetic resonance imaging (MRI) or computed tomography (CT).
Management
• Prolactin levels are unhelpful to monitor tumour activity in pregnancy as they are elevated in pregnancy.
• Women should be reviewed once in every trimester.
• Most physicians discontinue dopamine receptor agonists (bromocriptine/cabergoline) in cases of micropolactinomas once pregnancy is confirmed. Treatment with dopamine receptor agonists is electively continued by many endocrinologists in cases of macroprolactinomas.
• Regular follow up with formal visual field testing is mandatory for symptomatic women or those with macroprolactinomas.
• There should be a low threshold for performing pituitary images (MRI) in the presence of headaches or symptoms suggestive of visual field defects or diabetes insipidus.
• Dopamine receptor agonists are safe during pregnancy and breastfeeding. They should be reintroduced if there is concern about tumour expansion. Cabergoline has a more favourable side-effect profile than bromocriptine (causes less nausea).
• Hypophysectomy or radiotherapy is rarely necessary and is usually deferred to after delivery. Hypopituitarism
Hypopituitarism may precede pregnancy or present for the first time during pregnancy. The usual causes are pituitary or hypothalamic tumours, pituitary surgery, or cranial radiotherapy. Causes more specific to pregnancy include lymphocytic hypophysitis and postpartum pituitary infarction (Sheehan’s syndrome).
Pathogenesis
Sheehan’s syndrome
This usually presents postpartum following postpartum haemorrhage and hypotension and may lead to partial or complete pituitary failure. This is because the anterior pituitary is more vulnerable to hypotension in pregnancy due to its increased size.
Lymphocytic hypophysitis
This is a condition unique to pregnancy, presenting either late in the pregnancy or in the puerperium. It is characterized by autoimmune infiltration of the anterior pituitary, predominantly lymphocytes, causing pituitary expansion and hypopituitarism. Antipituitary antibodies have been described and this condition is associated with autoimmune thyroiditis or adrenalitis in 20% of cases.
Prognosis
Effect of pregnancy on hypopituitarism
Subsequent pregnancies after Sheehan’s syndrome and lymphocytic hypophysitis have been reported. Conception may require gonadotrophic stimulation of ovulation.
Effect of hypopituitarism on pregnancy
Maternal and fetal outcome is normal, if the condition is diagnosed and treated with adequate hormone replacement therapy prior to pregnancy. Poorly treated or undiagnosed hypopituitarism is associated with an increased risk of miscarriage, stillbirth, and maternal morbidity and mortality, resulting from hypoglycaemia and hypotension.
Clinical approach
Clinical features
• Sheehan’s syndrome: presenting features are due to deficiency of the relevant hormones. They include persistent amenorrhoea, failure of lactation, secondary hypothyroidism and secondary adrenocortical insufficiency.
• Lymphocytic hypophysitis: the features are those of expanding pituitary tumour with headaches, visual field defects, secondary hypothyroidism and secondary hypoadrenalism.
Diagnosis of hypopituitarism
• Investigations reveal reduced levels of thyroxine (T4), TSH, cortisol, ACTH, FSH, LH, and GH. The insulin stress test is impaired.
• Any patient with hypopituitarism should undergo pituitary imaging with MRI or CT to exclude a pituitary tumour.
• Definitive diagnosis of lymphocytic hypophysitis can only be made by histological examination of pituitary tissue.
Management
• The treatment is with replacement of deficient hormones. The vital hormone replacements are those of thyroxine and glucocorticoids.
• Requirements of the latter may change during periods of stress, and doses and route of administration may need to be changed based on the severity of the stress.
• There is a need for vigorous regular follow-up of these patients throughout pregnancy.
• The management of acute pituitary insufficiency includes intravenous fluids, dextrose and corticosteroids.
• Cases of Sheehan’s syndrome and lymphocytic hypophysitis have resolved spontaneously.
Future pregnancy
Lymphocytic hypophysitis may recur in subsequent pregnancies.
During subsequent pregnancies, requirements for thyroxine do not change, but additional parenteral corticosteroids may be required. Diabetes insipidus
Epidemiology
This is approximately the same as in the non-pregnant population, i.e. 1 in 15 000.
Pathology
Diabetes insipidus (DI) is caused by a relative deficiency of vasopressin (ADH). There are four types:
• Central: (cranial) due to decreased production of ADH by the paraventricular nuclei of the hypothalamus. Causes include prolactinomas, craniopharyngeomas, skull trauma, post-neurosurgery, rarely Sheehan’s syndrome or it may be idiopathic.
• Nephrogenic: associated with chronic renal disease, or more rarely hypercalcaemia or lithium therapy.
• Transient: increased ADH production by the placenta or decreased breakdown by the liver, usually associated with pre-eclampsia or acute fatty liver of pregnancy (AFLP).
• Psychogenic: caused by compulsive water drinking.
Prognosis
Effect of DI on pregnancy
No known adverse effects in treated cases and there is no contraindication to breastfeeding. Maternal seizures and oligohydramnios can complicate pregnancies in untreated or undiagnosed cases because of electrolyte imbalance and severe dehydration.
Effect of pregnancy on DI
Established central DI worsens in pregnancy and subclinical central DI may be unmasked for the first time during pregnancy because of increased clearance of endogenous ADH by vasopressinase. It is estimated that 60% of established cases of central DI worsen, but 25% improve, and 15% remain unchanged.
Clinical approach
Clinical features
These include excessive thirst, polyuria, or seizures (more common with transient DI).
Diagnosis
Other causes of polyuria such as diuretics, hyperglycaemia, hypercalcaemia, and hypokalaemia should be excluded.
The conventional 15–22 hours fluid deprivation test is hazardous in pregnancy. Close observation with paired urine and plasma osmolality measurements may be sufficient to exclude DI. A short deprivation test, e.g. overnight, may be all that is required to demonstrate an increasing urine osmolality with normal plasma osmolality and thus exclude cranial and nephrogenic DI.
Diagnosis is confirmed by a raised plasma osmolality (>295 mOsm/kg) or raised serum sodium (>145 mmol/L) in the presence of polyuria and a low urine osmolality (hypophysitis. Conn Med 2005;69:143–6.
Hanson RS, Powrie RO, Larson L. Diabetes insipidus in pregnancy: a treatable cause of oligohydramnios. Obstet Gynecol 1997;89:816–17.
Herman-Bonert V, Seliverstov M, Melmed S. Pregnancy in acromgaly, successful therapeutic outcome. J Clin Endocrinol Metab 1998;83:727–31.
Landolt AM, Schmid J, Wimpfheimer C, et al. Successful pregnancy in a previously infertile woman treated with SMS 201-995 for Acromegaly N Eng J Med 1989;320:671.
Beressi N, Beressir J-P, Cohen R, Modigliani E. Lymphocytic hypophysitis. Ann Med Intern 1999;150:327–34.
Psychiatric disorders in pregnancy
Subsyndromal emotional disturbances are very common in pregnancy and psychiatric disorders much more common than previously recognized. Around one in two women experience significant symptoms of anxiety and around 1 in 10 will suffer with a diagnosable anxiety disorder. These are usually pre-existing disorders that have continued into pregnancy. One in three women experience significant symptoms of depression at some stage of pregnancy and at least 1 in 10 pregnant women will develop a depressive episode. Antenatal depression is probably more common than postnatal depression.
Conception rates among women with severe and enduring psychiatric disorders appear to be increasing, probably as a consequence of more community-based care and newer treatments. Around 1 in 500 pregnant women will be suffering with schizophrenia or bipolar affective disorder. These disorders are associated with relatively high risks of perinatal relapse, treatment with potentially teratogenic medications, and higher rates of miscarriage and other obstetric complications.
Obstetricians, midwives, and general practitioners need to be aware of the risks associated with psychiatric disorders in pregnancy and will frequently need to balance the risks to the unborn child of starting or continuing any psychiatric treatment with the risks to both mother and child of stopping or changing treatment. Screening for psychiatric disorders in pregnancy
Psychiatric disorders are associated with high rates of morbidity in pregnancy and can have longer lasting effects on maternal health and child development (Oates 2003). They also are one of the leading causes of maternal mortality. It is therefore important to identify women who have a psychiatric disorder or who are at high risk of developing a psychiatric disorder as early on in pregnancy as possible. Early identification reduces risk and facilitates timely intervention.
At booking all women should be asked about
• past or present mental illness
• previous treatment by a psychiatrist or mental health team
• family history of perinatal mental illness.
Certain factors may increase the risk of developing mental illness in pregnancy or the puerperium including
• young age of mother
• family/partner conflicts
• lack of social network
• substance misuse
• unwanted pregnancy
• pre-existing mental illness.
As the risk of perinatal depression is particularly high, NICE (2007) recommends that all women are asked the following questions at booking, during pregnancy, and at 1 and 3–4 months postpartum:
• During the past month, have you often been bothered by feeling down, depressed or hopeless?
• During the past month, have you often been bothered by having little interest or pleasure in doing things?
If a woman says yes to either of these questions, a third is suggested:
• Is this something you feel you need or want help with? More detailed clinical assessment
History: key points
• Current presenting symptoms: Screen for affective symptoms (low or elated mood, tearfulness, low or increased energy, sleep disturbance, anhedonia, amotivation) and psychotic symptoms (auditory hallucinations, delusions, thought disorder).
• Past psychiatric history: Ask about first contact with psychiatric services, any history of medications taken before or during pregnancy, any history of self harm or suicide attempts, admissions to hospital with a mental health problem, particularly if under a section of the Mental Health Act (2007).
• Family history: Ask about any family history of serious psychiatric illness, particularly in the perinatal period.
• Medication history: What medications are they currently taking? What medications have they been on prior to the pregnancy and when did these stop? This is important if medications taken are contraindicated in pregnancy, e.g. sodium valproate.
• Enquire about past or current substance misuse and alcohol use.
Examination: key points
• Ensure a thorough physical examination has been done to rule out physical causes for psychiatric symptoms, such as anaemia, gestational diabetes, thyroid disease, or iatrogenic causes such as steroids.
• Perinatal psychiatric liaison opinion to confirm diagnosis by detailed mental state examination.
• Appearance and behaviour: any evidence of poor eye contact and rapport, poor self-care?
• Speech: increased/reduced rate, rhythm, volume, content?
• Mood changes: how does the patient describe their mood? How do they rate severity out of 10?
• Thoughts: any self-harm or suicidal ideas, plans or intention? Any thoughts of harm to the baby? Any distressing guilty ideas or paranoid thoughts, especially concerning the baby?
• Perceptions: any experiences of seeing or hearing things when alone that others cannot see or accept?
• Cognition: orientation to time, place, person? Impaired concentration or memory?
• Insight: Does the patient feel they are physically or mentally unwell? Do they wish to accept treatment and if required come into hospital?
• Special investigations
• Consider blood tests to exclude physical conditions (FBC, WBC, U&E, LFTs, TFTs, glucose)
• Consider blood serum levels of medication to check if levels are therapeutic, e.g. lithium level. Specific disorders
Anxiety disorders
• Anxiety disorders include phobias, panic disorder, generalized anxiety disorder, obsessive compulsive disorder, and post-traumatic stress disorder.
• Around 1 in 10 women will suffer with an anxiety disorder in any one year.
• Generic symptoms include pervasive or episodic fearfulness, avoidance, and autonomic arousal.
• Pregnant women with an anxiety disorder may present with excessive reassurance seeking and an over-preoccupation with fetal wellbeing.
• The possibility of agoraphobia, blood injury phobia, and needle phobia should be considered in women who are too fearful to attend antenatal clinic appointments.
• Depression can present with anxiety and is an important differential diagnosis to consider, as it will require treatment in its own right.
• Although invariably distressing to the pregnant woman, there is conflicting evidence that marked anxiety has an adverse effect on fetal outcome.
• High antenatal anxiety is a predictive factor for postnatal depression independently of antenatal depression.
• A relatively short-term, structured psychological treatment like cognitive behaviour therapy is the treatment of choice.
• Long-term benzodiazepine use should be avoided in pregnancy.
Bipolar affective disorder
• This affects 1 in 100 women of childbearing age.
• It is characterized by severe episodes of depression, mania (elevated mood, excitability, irritability, and over-activity) or a mixture of the two (mixed affective state) often associated with psychotic symptoms that can pose a significant risk to mother and fetus.
• It is associated with high rates of subsyndromal depression between acute episodes
• It is associated with high rates of relapse if mood-stabilizing medication is stopped precipitately in early pregnancy
• It predicts a high risk of postpartum relapse, approaching 1 in 2 without preventative treatment. Most episodes of postpartum psychosis are bipolar in nature, and most present within a week of delivery.
• It is associated with a high suicide rate.
Requires careful management by a psychiatrist familiar with the risks and benefits of psychiatric medication in pregnancy
Is best managed by a combined approach between maternity services, specialist mental health services and primary care with a formal perinatal care plan.
Depression
• This is characterized by low mood, lack of energy, or increased fatigability and loss of enjoyment or interest in association with a range of other symptoms including low self-esteem, feelings of guilt, worthlessness or hopelessness, poor concentration, poor appetite, and suicidal ideation
• It is associated with an increased risk of suicide
• It can be effectively treated with pharmacological and psychological therapy, although psychological treatments such as cognitive behavior therapy are preferred in pregnancy.
Eating disorders
• Bulimia nervosa affects 1 in 100 women of child-bearing age and anorexia nervosa around 1 in 500
• Bulimia nervosa and anorexia nervosa are characterized by disturbances in eating behaviour and abnormalities in body image
• Eating disorders tend to improve during pregnancy. Deterioration in pregnancy is predicted by more severe symptoms, younger age, and lower educational attainment.
• Pregnancy complications include poor maternal weight gain resulting in intrauterine growth retardation and small for date babies, electrolyte disturbances (hypokalaemia and hyponatraemia), metabolic alkalosis as a consequence of self-induced vomiting, laxatives or diuretic misuse, and higher rates of miscarriage, premature or instrumental delivery.
• The combination of hyperemesis gravidarum and eating disorder can be particularly problematic.
• Treatment is predominantly psychological.
Schizophrenia
• Schizophrenia affects 1 in 100 women of child-bearing age
• It is characterized by a range of cognitive, emotional, and volitional symptoms including delusions, hallucinations, and abnormalities of affect, speech, and motivation
• It is associated with a wide range of outcomes, from complete remission to long term enduring illness.
• It usually requires maintenance medication throughout and after pregnancy under the supervision of a psychiatrist familiar with the risks and benefits of psychotic medication in pregnancy. Principles of treatment
If there is evidence of mild to moderate mental illness often psychological intervention alone or regular outpatient appointments for support can be helpful. Advice can be obtained from a perinatal psychiatrist. If medication is required, then the following treatment principles should apply (NICE 2007):
• use drugs with low-risk profiles for both the mother and fetus
• start at the lowest effective dose and increase slowly if required
• aim for monotherapy
• consider increased screening of the fetus, e.g. ultrasound
• breastfeeding should always be encouraged if the woman wishes and treatment that allows the woman to do this are preferred whenever possible. Specific treatments
Anticonvulsants
• These are widely used in the treatment of bipolar disorder
• They are associated with relatively high teratogenicity, including neural tube defects. NICE (2007) recommends that valproate is not used to treat bipolar disorder in women of childbearing age unless clinically justified on the balance of risks, the woman has been carefully counselled about potential teratogenicity, and she is using adequate contraception.
• If taken during early pregnancy, the addition of high-dose folic acid is required (5 mg a day for women taking carbamazepine and valproate), although there is no evidence that this reduces the risk of neural tube defects.
• They are associated with a risk of vitamin K deficiency bleeding if taken in late pregnancy.
Antidepressants
• Antidepressants are relatively safe in pregnancy with notable exceptions. Venlafaxine may be associated with high blood pressure if taken at high doses; paroxetine should be avoided because of its reported association with cardiac anomalies, and all other selective serotonin reuptake inhibitors (SSRIs) should be used with caution after 20 weeks’ gestation because of their reported association with persistent pulmonary hypertension of the newborn.
Antipsychotics
• These are relatively safe in pregnancy they but should be used at the lowest possible dose and polypharmacy avoided.
• Newer ‘atypical’ drugs may be associated with maternal weight gain predisposing to gestational diabetes, and ‘large for date’ and heavier birth weight babies.
Electroconvulsive therapy
• This is safe in pregnancy subject to the standard precautions associated with short-term anaesthesia.
Lithium
• Lithium has an important role in the management of bipolar disorder and stopping it precipitately in early pregnancy is associated with high rates of relapse.
• It has also been associated with elevated rates of congenital heart disease if used in the first trimester of pregnancy, but estimates of risk vary between 1% and 8%.
• High-resolution fetal ultrasound and echocardiography are recommended for the assessment of lithium exposed pregnancies.
• Lithium levels should be monitored every month until 36 weeks’ gestation, then every week.
• Dehydration during prolonged labour may result in increased blood levels and intrapartum levels should be taken as required.
• Occasionally reported neonatal complications of lithium exposure include hypotonia, nephrogenic diabetes insipidus, hypothyroidism, and cardiac rhythm disturbances. The pregnant woman in the psychiatric hospital
• She requires careful multiprofessional management and a clearly formulated birth plan that considers capacity to consent to, as well as capacity to cooperate with, obstetric care
• She may require increasingly frequent midwifery assessment as term approaches if her capacity to recognize the onset of labour is compromised. References
Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers Lives: reviewing maternal deaths to make motherhood safer (2003–2007). Dec 2007.
Davies A, McIvor R, et al. Impact of childbirth on a series of schizophrenic mothers. Schizophrenia Res 1995;16:25–31.
NICE Clinical guideline 45. Antenatal and postnatal mental health National Institute of Clinical Excellence. Feb 2007.
Oates M. Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. Br Med Bull 2003;67:219–29 Patient resources
The Royal College of Psychiatrists website has a useful information leaflet: www.rcpsych.ac.uk/pnd
Mind www.mind.org.uk and www.pni.org.uk.
Renal disease Asymptomatic bacteriuria
Definition
Significant growth of a uropathogen in the absence of symptoms.
Incidence
Incidence of 2–10% of pregnant women.
Causes
As for urinary tract infections (see below). Clinical features
• Asymptomatic, usually infected in early pregnancy
• Associated with preterm delivery and low birthweight babies in some studies if untreated.
Diagnosis
• Urine dipstick: leucocytes, nitrites
• Midstream specimen of urine (MSU): >105 colony forming units of pathogen (CFC)/mL.
Management
During pregnancy
• Empirically treat with antibiotics if leucocytes and nitrites on urine dipstick. Adjust treatment according to sensitivities
• 4–6 weekly MSU (as 30% have a relapse of bacteriuria)
Complications
Development of acute pyelonephritis in
• already done so)
Diagnosis
As for asymptomatic bacteriuria (see above)
Management
Antibiotic treatment: normally for 3 days. If recurrent infection, or infection in a woman with renal disease, diabetes, sickle cell trait or disease treat for 7–10 days
• E. coli is the commonest organism and usually sensitive to:
• nitrofurantoin 100 mg bd (avoid in late third trimester due to risk of neonatal haemolysis)
• trimethoprim 200 mg b.d. (avoid in first trimester as it is a folate antagonist)
• amoxicillin and cephalosporin
• ciprofloxacin causes arthropathy in animal studies
• Increase fluid intake
• Check MSU 1 week following completion of treatment and then after every 4–6 weeks
• If ≥2 episodes of asymptomatic bacteriuria or urinary tract infections (UTIs)
• renal USS for structural abnormalities or renal stones
• prophylactic low-dose antibiotics given at night for the rest of pregnancy and 6 weeks postpartum.
Complications
Acute pyelonephritis. Acute pyelonephritis
Definition
Infection of kidney(s).
Causes
As for UTIs.
Clinical features
• Fever, rigors
• Back or loin pain
• Symptoms of UTI
• Nausea, vomiting
• Sepsis if severe.
Effect of acute pyelonephritis on pregnancy
• Uterine contractions
• Preterm labour
• Sepsis.
Diagnosis
• As for UTI plus
• FBC, U+E, CRP
• blood culture (if febrile).
Management
• Admit for empirical IV broad-spectrum antibiotics (usually a cephalosporin). Change to oral treatment for 10 days once afebrile for 24 hours.
• Aminoglycoside may be necessary (measure drug levels as theoretical risk of fetal ototoxicity).
• Intravenous fluid rehydration.
• If sepsis suspected, perform lactate level, check for haemolysis (blood film and LDH), consider CVP line and liaise with ITU.
• Renal USS.
• Following discharge, screen for bacteriuria as in UTIs (see above).
• Prophylactic antibiotics reduce risk of recurrent acute pyelonephritis.
Complications
Chronic pyelonephritis. Acute renal failure (ARF)
Incidence 25 mmol/L)
Acidosis
Pulmonary oedema refractory to diuretics
Recovery
• Dialysis is required in the short-term as most causes of ARF in pregnancy are reversible
• Acute tubular necrosis is reversible
• Acute cortical necrosis is irreversible. Haemolytic uraemic syndrome (HUS) and thrombotic thrombocytopenic purpura (TTP)
Definition
Part of the same spectrum of microangiopathic haemolytic anaemia and thrombocytopenia
Incidence
More common in women and increased incidence in late pregnancy and postpartum
Causes
• Congenital HUS/TTP: absence of ADAMTS13 (a plasma metalloprotease)
• Acquired HUS/TTP: reduction of ADAMTS13 by anti-ADAMST13 antibodies.
Pathology
• ADAMTS13 cleaves von Willebrand factor (vWF) multimers, which prevents platelets adhering to the multimers and forming microthrombi that can block end organ arterioles and capillaries (as occurs in HUS/TTP).
• ADAMST13 normally falls in pregnancy.
Clinical features
• HUS: haematuria, renal failure
• TTP: neurological or behavioural abnormalities ± symptoms of gastrointestinal vessel ischaemia.
Diagnosis
• Severe thrombocytopenia
• Severe haemolysis
• peripheral blood film (usually diagnostic): red cell fragments
• ↑lactose dehydrogenase (LDH >600 U/L)
• ↑unconjugated bilirubin
• falling haemoglobin
• Renal impairment: severe in HUS
• DIC is rare (prothrombin time and APTT usually normal).
Differential diagnosis
Pre-eclampsia: discriminating features include abnormal LFT, ± coagulopathy, lower grade haemolysis.
Management
• Plasmapharesis
• Steroids in addition if acquired HUS/TTP
• Do not administer platelets as this can lead to rapid decline. Chronic renal disease
Definition
• Normal glomerular filtration rate (GFR) plus structural kidney damage, or persistent proteinuria or
• Estimated GFR 180 μmol/L have a 1 in 3 chance of requiring renal replacement therapy within a year of pregnancy (Table 8.32.1).
• If relapsing and remitting disease, e.g. SLE, pregnancy during a flare results in a worse prognosis, for the fetus, disease activity in pregnancy and progression of renal disease.
• Escalating hypertension
• Worsening proteinuria.
Pregnancy outcome in chronic renal disease depends on:
Level of kidney dysfunction (GFR/creatinine)
Hypertension
Proteinuria
Specific disease
Best outcome for those prepregnancy without significant renal impairment, hypertension or proteinuria.
Diagnosis
• U+E, FBC, LFT, clotting, urine dipstick
• Renal screen to identify cause:
• urine microscopy (casts, rbc, wbc), culture
• protein/creatinine ratio (PCR)
Table 8.32.1 Risks of pregnancy in chronic renal disease

• ANA, anti-dsDNA Ab, ACA, ANCA, immunoglobulin subclasses, complement (C3, C4), anti-GBM Ab
• renal USS.
Management
Prepregnancy counselling
Counsel regarding maternal and fetal risks (Table 8.32.1) Advise against pregnancy if severe renal impairment (creatinine >250 μmol/L)
Genetic counselling if heritable component to the disease, e.g. APKD, reflux nephropathy.
Drugs
• Women should not conceive while on cytotoxic drugs (e.g. cyclophosphamide, methotrexate). Use effective contraception while on these drugs. Wait 3–6 months before conceiving once use discontinued.
• Mycophenolate mofetil (MMF) is teratogenic. Consider changing to another drug, e.g. azathioprine prepregnancy.
• Reassure about safety of hydroxychloroquine, azathioprine, ciclosporin A, and tacrolimus.
• ACE inhibitors (ACEI) and the closely related angiotensin 2 receptor blockers (ARB) protect kidneys from progressive renal impairment particularly when patient has proteinuria. ACEI are teratogenic in the first trimester increasing the risk of congenital anomalies from 3% to 8%. In the second and third trimesters they prevent nephrogenesis and result in oligohydramnios. As women with chronic renal disease may be subfertile stopping ACEI/ARB prepregnancy may result in loss of renal function preservation. In a planned pregnancy can consider stopping them as soon as positive pregnancy test.
During pregnancy
Multidisciplinary care involving both obstetricians and nephrologists
• If on cytotoxic agents, consider termination of pregnancy
• Stop statins (teratogenic).
• Hypertension
• Stop ACEI and ARB if still on them. If on these for hypertension, change to methyldopa or long acting nifedipine. Second line agents include labetolol, hydralazine and doxazocin.
• Maintain BP at ˛ 135/80 mmHg to protect kidneys from further damage
• Start aspirin 75 mg daily as prophylaxis against preeclampsia
• If develops pre-eclampsia reduce dose of MgSO4 for eclampsia prophylaxis if creatinine >180–200 μmol/L, and check MgSO4 levels
• Proteinuria: if nephrotic syndrome with proteinuria (>3 g/day) and albumin 180–200 μmol/L as heparin is renally cleared.
• Anaemia
• iron deficiency (due to pregnancy): replace with iron
• Erythropoietin (EPO) deficiency (due to chronic renal disease). Ensure iron replete (ferritin >200: use IV iron) prior to giving EPO to prevent blood transfusion.
• Regularly monitor, FBC, U+E, albumin, PCR (or 24 hour urinary protein).
• Regular fetal growth scans
• Women with reflux nephropathy
• MSU each visit
• prophylactic antibiotics if recurrent UTIs or very dilated renal tracts
• Serial renal USS to check for progression or obstruction if previous ureteric surgery or dilated renal tracts
• Women with diabetic nephropathy
• Worse pregnancy outcome compared to diabetics without nephropathy
• Increased risks UTIs, pre-eclampsia, proteinuria and nephrotic syndrome
• Women with APKD
• Increased risks of pre-eclampsia and UTIs in pregnancy
• Can bleed into a cyst causing loin pain and haematuria
• Associated with polycystic liver disease and Berry anuerysms.
Delivery
• Aim for a vaginal delivery: spontaneous or by induction of labour if clinical circumstances necessitate earlier delivery and no obstetric contraindications
• Caesarean section for obstetric indications only
• Delivery may need to be expedited if deteriorating renal function, pre-eclampsia or fetal compromise.
Postnatal
• Recommence ACEI (safe in breastfeeding)
• Avoid NSAIDs
• Consider thromboprophylaxis
• Screen offspring for inherited kidney disease. Dialysis
Haemodialysis
Chronic ambulatory peritoneal dialysis (CAPD)
Effect of dialysis on pregnancy
Overall successful pregnancy outcome only 30%
• Subfertility: improved with treatment of anaemia with erythropoietin
• Miscarriage and fetal loss 50–60%
• Polyhydramnios
• IUGR
• Prematurity in almost all: spontaneous or iatrogenic
• Severe pre-eclampsia
• Bleeding due to heparinization (in haemodialysis)
• Peritonitis (in CAPD)
• Maternal mortality.
Effect of pregnancy on dialysis
• More frequent dialysis required: often daily to maintain pre-dialysis urea 35 years:
On dialysis for >5 years
Late booker (dialysis frequency increased later in pregnancy)
Management
Prepregnancy counselling
Counsel regarding severe fetal and maternal risks of pregnancy
Advise effective contraception if decides against pregnancy
During pregnancy
Pregnancy should be managed in a tertiary centre with a specialised renal unit with multidisciplinary care involving both obstetricians and nephrologists
Caution with fluid balance: avoid interdialysis weight gain
Hypertension: can be severe and chaotic in pregnancy
• Stop ACEI and ARB as soon as positive pregnancy test
• Start aspirin 75 mg daily as prophylaxis against preeclampsia
• First trimester fall in BP does not occur
• Pre-eclampsia is more common but very difficult to diagnose as patients are usually hypertensive and anuric. If urine is produced, there is usually baseline proteinuria and haematuria. Do not give MgSO4, as will quickly accumulate to toxic levels
Anaemia: will become more severe in pregnancy
• Increased requirements for erythropoietin and IV iron
• Monitor FBC and iron stores regularly.
Regular fetal growth scans Do not perform CTG during dialysis A delivery pack should be kept in dialysis suite due to risk of preterm delivery
Contraception
Mirena IUS
Copper coil (not in CAPD) Renal transplant recipient
Successful outcome in 95% who remain pregnant after 12 weeks gestation
Effect of renal transplant on pregnancy
• Fertility restored quickly when renal function normalises
• If pregnancy >1 year after surgery, and good graft function, generally good outcomes
• Increased risk of
• infection
• hypertension and pre-eclampsia
• IUGR and prematurity.
Effect of drugs (see below)
Pregnancy outcome dependent the following parameters at conception:
Renal function (better if creatinine and multiple therapies, some of which may be harmful to fetus
• Viral infections e.g. CMV.
Use effective contraception until then as fertility rapidly returns after surgery
During pregnancy
Pregnancy should be managed in a tertiary centre with a specialized renal unit with multidisciplinary care involving both obstetricians and nephrologists
• careful control of blood pressure
• regularly monitor creatinine, U+E, PCR (or 24 hour urinary protein), FBC, LFT, calcium, MSU
• Fetal growth scans.
Drugs commonly used in combination for immunosuppression include:
• Azathioprine relatively safe and not teratogenic
• Ciclosporin relatively safe, not teratogenic, associated with IUGR
• Prednisolone associated with a small increased risk of fetal cleft lip and or palate if used in first trimester but benefit of use outweighs risk
• Tacrolimus appears safe with the limited available data
• Mycophenolate mofetil (MMF) teratogenic and generally avoided, but may need to be continued if this is the only drug that prevents graft rejection
• Sirolimus is an alternative to MMF but few data are available.
Continue immunosuppressive drugs at prepregnancy levels to avoid graft rejection
Monitor tacrolimus and ciclosporin levels in pregnancy
If renal function deteriorates in pregnancy
MSU to exclude infection
PET bloods
Ciclosporin levels
Renal graft USS to exclude obstruction
Renal biopsy: consider in early pregnancy if graft rejection suspected
Expedite delivery in late pregnancy if graft rejection suspected
Delivery
• Aim for vaginal delivery: the renal graft does not obstruct labour
• Caesarean section only for obstetric reasons
• Prophylactic antibiotics if surgery necessary
• If on prednisolone ˇ7.5 mg daily, cover delivery with hydrocortisone (see Section 8.33 asthma). Further reading
Armenti VT, Radomski JS, Moritz MJ, et al. Report from the National Transplantation Pregnancy Registry (NTPR): outcomes of pregnancy after transplantation. In: Cecka JM, Terasaki PI (eds) Clinical transplants 2003. UCLA Immunogenetics Centre, Los Angeles, California 131–41.
George JN. The association of pregnancy with thrombotic thrombocytopenic purpura-haemolytic uraemic syndrome. Curr Opin Hematol 2003; 10:339–44.
Haase M, Morgera S, Bamberg C, et al. A systematic approach to managing pregnant dialysis patients: the importance of an intensified haemodiafiltration protocol. Nephrol Dial Transplant 2005;20:2537–42.
Hou SH. Pregnancy in women with chronic renal insufficiency and end stage renal disease, Am J Kid Dis 1999;33:235–52.
Jones DC, Hayslett JP. Outcome of pregnancy in women with moderate or severe renal insufficiency. N Engl J Med 1996;335:226–32.
Jungers P, Chauveau D, Choukroun G, et al. Pregnancy in women with impaired renal function. Clin Nephrol 1997;47: 281–8.
Lightstone L. Chronic renal disease, dialysis and transplant. In: Gree IA, Nelson-Piercy C, Walters B (eds) Maternal medicine. 2007 Elselvier.
Pertuiset N, Grunfeld JP. Acute renal failure in pregnancy. Ballière’s Clin Obstet Gynaecol 1994;8:333–51.
Smaill F. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev 2001;2:CD000490.
Vazquez JC, Villar J. Treatments for symptomatic urinary tract infections in pregnancy. Cochrane Database Syst Rev 2003;4: CD002256.
Respiratory disease
Definition
Reversible airways obstruction.
Epidemiology
Respiratory disease affects 4–8% of pregnant women.
Precipitants
Pollen, dust, animals, exercise, emotion, change in weather, upper respiratory tract infections.
Pathology
Inflammatory disorder of airways mucosa with bronchial obstruction due to:
• bronchial hyper-responsiveness
• bronchial mucosal inflammation
• sticky mucus secretions blocking airways.
Specific points in history
• Onset: childhood/adult; identify precipitants
• Assess severity: current medication and frequency of use of ventolin inhaler, previous use of nebulizers, oral steroids, frequency of hospital admissions, any ITU admissions for ventilation.
• Ask if asthma worsens with non-steroidal anti-inflammatory drugs (NSAIDs).
Symptoms (usually diurnal)
• Wheeze
• Cough especially nocturnal and morning
• Shortness of breath
• Tight chest.
Signs
• Polyphonic wheeze
• Tachypnoea
• Tachycardia
• Accessory muscle use.
Diagnosis
• Variability of bronchial obstruction with reversibility
• PEFR (peak expiratory flow rate): 20% diurnal variation in PEFR for ≥3 days in a 2-week period
• Severity see Table 8.33.1.
Investigations
• PEFR: reduced compared with their best
• ABG: mild hypoxia, reduced PCO2 (hyperventilating). Beware a high PCO2
• CXR: to exclude pneumothorax and pneumonia
• Sputum: culture
• Spirometry: low forced expiratory volume in 1 second (FEV)1; low FEV1:FVC (forced vital capacity).
Effect of pregnancy on asthma
Rule of thirds: may improve, deteriorate, or remain unchanged
More likely to worsen if
• medications are stopped
• asthma is severe (worsens in third trimester)
• there is gastro-oesophageal reflux
Table 8.33.1 Severity of asthma

• there is postnasal drip from pregnancy rhinitis.
Asthma attacks after 36 weeks’ gestation are unusual. Attacks in labour are rare (↑ endogenous steroids). The course of asthma is similar in successive pregnancies.
Effect of on asthma on pregnancy
• Well-controlled asthma has no adverse effects on pregnancy.
• Severe, poorly controlled asthma (regular or chronic maternal hypoxia) has a small increase in adverse pregnancy outcome (pregnancy induced hypertension, preeclampsia, pre-term birth, IUGR, neonatal hypoxia)
• Asthma in mother doubles risk of asthma in offspring.
Management
Preconception
• Asthma control should be optimized with medications.
• Specifically tell women not to stop or reduce asthma treatment when pregnancy is diagnosed.
During pregnancy
• This is an excellent opportunity to improve asthma control: monitor and adjust treatment (see box)
• Emphasize the importance and safety of continuing asthma medications during pregnancy to ensure good asthma control, avoid triggers, stop smoking
• Check inhaler technique: may need spacer/breath-activated inhaler
• Treat gastro-oesophageal reflux and rhinitis
• Explain to patient indications to increase inhaled steroid dose at home.
Treatment of an acute asthma attack
Please refer to Fig. 8.33.1.
Medications
Inhaled drugs: β-agonists (short and long acting), steroids, cromoglycates, and anticholinergics (ipratropium):
• Safe in pregnancy. No adverse fetal effects. Minute proportions are systemically absorbed
• Inhaled β2-agonists do not impair uterine contractility or delay labour.
Oral/i.v. β2-agonists: may reduce uterine contractility and cause tachycardia
Stepwise treatment of asthma
Step 1 mild intermittent asthma: short-acting inhaled β2-agonist as required, e.g. salbutamol, terbutaline
Step 2 regular preventer therapy: add an inhaled steroid ‘preventer’, e.g. beclomethasone 200-800 μg/day (divide into two doses) if: symptomatic ≥3 times/week, or using short-acting inhaled β2-agonist ≥3 times/week, or waking up one night/week.
Step 3 Initial add-on therapy: add long-acting inhaled β2-agonist (LABA), e.g. salmeterol. Can use a combination inhaler containing a steroid and LABA. If inadequate/no response to LABA, continue/stop it and increase inhaled steroid to 800 μg/day
Step 4 persistent poor control: Additional treatments, e.g. slow-release oral theophylline, oral β2-agonist, increase inhaled steroid dose up to 2000 μg/day or consider leukotriene receptor antagonist.
Step 5 continuous or frequent use of oral steroids: use lowest effective dose of prednisolone and continue inhaled steroid at 2000 μg/day.
Prednisolone: 90% metabolized by placenta (only 10% crosses to fetus).
• Slight increased incidence of cleft lip/palate with first trimester use (benefit exceeds risk in asthma)
• Steroid-induced gestational diabetes (GDM): test if on regular steroids; treat GDM with diet, then insulin, not by reducing steroid dose
• Increased risk of infections
• Preterm rupture of membranes: risk increased with long-term high-dose steroids
Theophylline: if dependent on therapeutic theophylline levels for asthma control, check plasma level and increase dose accordingly. No adverse fetal effects.
Leucotriene receptor antagonists: continue in brittle asthmatics who depend on them for stability. Emerging good safety data for montelukast and zafirlukast. Avoid zileuton. Low-dose aspirin and NSAIDs: avoid in women who have had worsening asthma with these agents. Intrapartum
• Continue asthma medications
• If on prednisolone >7.5 mg for >2 weeks, cover with IV hydrocortisone 50 mg tds over labour until oral drugs recommenced.
• Prostglandin E1 (e.g. prostin) is safe

Fig. 8.33.1 Management of an acute asthma attack: treat as non-pregnant.
• Prostaglandin F2α (e.g. carbeprost) can cause bronchospasm
• Ergometrine reported to cause bronchospasm when used with general anaesthesia. No real concerns reported with syntometrine
• All forms analgesia for labour (including entonox and epidural) are safe. Avoid opiates in an asthma attack.
Postpartum
• Continue all medications: all safe with breastfeeding
• Encourage breastfeeding which is protective against the child developing atopy and asthma. Pneumonia
Epidemiology
Similar incidence to non-pregnant
More severe in pregnancy with atypical infections especially viral
Aetiology
• Bacterial pneumonia, e.g. Streptococcus pneumoniae (>50% cases), Haemophilus influenzae, Staphylococcus aureus (especially with influenza and IV drug abusers)
• Viral pneumonia, e.g. influenza, varicella (10–20% with chicken pox)
• Other, e.g. Mycoplasma pneumoniae (atypical pneumonia), Pneumocystis carinii (PCP with HIV).
Symptoms
• Cough productive of coloured sputum
• Fever ± rigors
• Shortness of breath
• Pleuritic chest pain.
Signs
• Fever, tachycardia, tachypnoea
• Consolidation (dull to percussion, increased tactile vocal fremitus, bronchial breathing)
• Coarse crackles on auscultation
• Unilateral signs in lobar pneumonia, bilateral signs in community acquired/viral pneumonia).
Diagnosis
• Sputum culture ± blood culture
• Raised inflammatory markers (↑WCC, ↑CRP)
• Chest X-ray: never withhold due to pregnancy
• S. pneumoniae lobar pneumonia
• Mycoplasma pneumoniae often clear
• PCP ground glass appearance
• Pneumococcal and legionella urine antigen tests, influenza testing (in severe pneumonia)
• Test for PCP if HIV positive
• ABG if O2 saturation 30/minute
• O2 sat Sit up and give facial O2 (maintain O2 sat >95%)
• Fluid restrict and monitor fluid balance
• Diuretics: frusemide 10–40 mg initially (lower dose in pre-eclampsia)
• Diamorphine 2.5 mg i.v. (+ antiemetic)
• Treat underlying cause, e.g. antibiotics if sepsis or pneumonia, low molecular weight heparin if pulmonary embolus, replace β2-agonists with atosiban or nifedipine for tocolysis. Sarcoidosis
Definition
Epidemiology 0.05% of pregnancies.
Pathology
Multisystem disorder with non-caseating granuloma.
Clinical features
• Often asymptomatic
• Chest symptoms, e.g. shortness of breath, cough
• Extrapulmonary features:
• Erythema nodosum
• Anterior uveitis
• Hypercalcaemia
• Arthropathy
• Fever
• CNS involvement.
Diagnosis
• CXR: bilateral hilar lymphadenopathy, pulmonary infiltration, fibrosis
• Bronchioalveolar lavage and transbronchial biopsy
• Lung function tests: reduced transfer factor (KCO)
• Serum ACE unhelpful as altered in pregnancy.
Effect of pregnancy on sarcoidosis
Disease may be unaffected or improve with pregnancy, and relapse postnatally.
Management
Continue maintenance steroids.
Initiate or increase steroid treatment if:
• Extrapulmonary disease
• Functional respiratory impairment.
If on >7.5 mg prednisolone for >2 weeks, cover labour with hydrocortisone i.v. 50 mg tds
Avoid vitamin D, which can precipitate hypercalcaemia.
Cystic fibrosis
Definition
Autosomal recessive condition combining pancreatic insufficiency and repeated respiratory tract infections
Epidemiology
1:2000 Caucasians affected. 1:25 Caucasians are carriers
Pathology
• Mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene on chromosome 7 affecting chloride channels
• All exocrine glands affected: thick mucus production (blocks ducts) and high sweat sodium.
Clinical features
• Bronchiectasis and repeated respiratory infections
• Malnutrition (loss of pancreatic digestive enzymes in >90% with CF)
• Diabetes 20%, impaired glucose tolerance 15% (loss of islet cell function).
Effect of pregnancy on CF
Most people with cystic fibrosis die in early adult life. The death rate is not increased by pregnancy, but is more likely if moderate to severe lung disease with FEV1 defects
• neurological abnormalities: microcephaly, meningoencephalitis, mental retardation
• other defects include hepatosplenomegaly, thrombocytopenia, bone defects, and purpuric skin lesions resulting in the classic ‘blueberry muffin’ presentation. Aetiology
Neonates with CRS are born to mothers who are exposed to the rubella virus during pregnancy and do not carry immunity either by vaccination or prior infection.
Perinatal transmission of the virus varies with gestational age. Risk of fetal infection is high in the first trimester (up to 80%), decreases in the second trimester, and rises again in the third trimester. However, sequelae of infection, such as CRS, are essentially limited to infection occurring during the first 16 weeks of gestation.
The defects associated with CRS are felt to be the result of viral damage to blood vessels with resultant ischaemia to the involved organ systems. Prognosis
Rubella infection is typically a self-limited infection for the mother. The prognosis for neonates affected with CRS is variable based on the organ systems involved and the associated complications. Clinical approach
Diagnosis
Evaluation for rubella infection should be performed in pregnant women with known susceptibility to the virus and clinical manifestations consistent with infection or concern for exposure.
Serology is typically the method used for diagnosis of rubella infection. Testing should be performed within 10 days of the onset of the rash and repeated 2-3 weeks later. Rubella infection can be diagnosed with the presence of rubella-specific immunoglobulin (Ig)M or a significant rise in the IgG titre between acute and convalescent phases. Cultures can also be performed as the rubella virus can be isolated from nasal, blood, throat, urine, and CSF specimens. Additionally, some advocate performing PCR on chorionic villous samples or amniotic fluid. Generally, ultrasound diagnosis of rubella infection in the fetus is difficult given the nature of abnormalities seen with CRS. However, in fetuses with growth restriction, congenital rubella infection should be a component of the differential diagnosis.
Treatment
Unfortunately, treatment for acute rubella infection during pregnancy, as well as outside pregnancy, is primarily limited to supportive measures. Some advocate the use of immune globin in the setting of acute infection; however, this remains controversial. There are currently no in utero treatments for fetuses at risk of developing CRS.
Given the limited treatment options for CRS, focus has been placed on prevention. As mentioned previously, the overall incidence of rubella infections, and thus CRS, has decreased dramatically with the implementation of vaccination.
The rubella vaccine is a live attenuated vaccine and now commonly administered as a part of the measles, mumps, and rubella (MMR) vaccine. In the USA, vaccination is recommended via two injections, separated by 1 month, after the first year of life. Vaccination results in measurable antibody in 95% of immunized individuals. The second dose is designed to foster immunity in the small percentage of individuals who do not immunilogically respond to the first dose. Booster injections may be required.
Ideally, all women of reproductive age would be screened for immunity prior to pregnancy and immunized as needed. It is recommended by the Centers for Disease Control that pregnancy be delayed by 1 month following administration of the vaccine given a theoretical risk to the fetus with the live attenuated vaccine.
All pregnant women should be screened for rubella immunity. If immunity is not identified, vaccination should be performed postpartum, again, given a theoretical risk to the fetus with live attenuated vaccines. Given an often concomitant lack of immunity in those women found to be susceptible to rubella infection for risk of mumps and measles, the American College of Obstetricians and Gynecologists recommends administration of the MMR vaccine in the postpartum period if needed. There is no contraindication to breastfeeding with the vaccine. References
Marret H, Golfier F, Di Maio M, et al. Rubella in Pregnancy. Management and prevention. Presse Med 1999;28:2117–22.
Miller E, Cradock-Watson JE, Pollock TM. Consequences of confirmed rubella at successive stages of pregnancy. Lancet 1982;2:781–4.
Reef SE, Redd SB, Abernathy E, zimmerman L, Icenogle JP. The epidemiological profile of rubella and congenital rubella syndrome in the United States 1998–2004: the evidence for absence of endemic transmission. Clin Infect Dis 2006;43(Suppl 3):126–32.
Rubella Prevention. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and reports 1998;47(RR-8):1–57.
Rubella Vaccination. American College of Obstetricians and Gynecologists Committee Opinion, #281 Dec 2002.
Substance abuse in pregnancy Definition
Substance abuse covers a wide range of behaviours from use of drugs and alcohol to dependence on the drug of choice. Both the International Classification of Disease ICD-10 (WHO 1992) and the Diagnostic and Statistical Manual for Mental Disorders DSM-IV (ASA 1994) include dependence and harmful use for alcohol, drugs, and nicotine. Harmful use is defined by the negative social consequences of the behaviour and the physical and psychological consequences, dependence as the presence of withdrawal signs and symptoms on cessation. Addiction is the term used to describe the overwhelming urge to continue use despite the harmful consequence to the individual or others and usually, but not always, includes physical dependence. Epidemiology
Drug use among 16–29-year-olds in England (General Household Survey 2002), found 25% had experienced “any drug” use, 22.7% had used cannabis and 4.9% opiates. Nicotine use was found to have declined, however 26% were nicotine users. A survey conducted in 2008 (NHS Information Centre National Centre for Social Research), of 11–15-year-olds found that 25% had tried drugs previously, 17% in the previous year, 10% in the previous month. However, smoking had decreased from 52% in 1982 to 33% in 2007. Girls were more likely to smoke regularly. Alcohol had been consumed by 3% of 11 year olds and 41% of 15 year olds. In 2004 (NHS Information Centre, 2006) 15% of men and 59% of women drank daily and 39% men and 22% women were drinking over the recommended levels per week. However, in 2000 30% of women who drank alcohol before a pregnancy reported giving up when pregnant.
It should be noted therefore that the age of exposure to drugs and alcohol is becoming lower and the proportion of using women to men in the fertile age range is increasing, that pregnancy itself has been shown to change behaviour, and that the numbers of drug users in treatment has increased significantly over the past 5 years. However, it should also be noted that patterns of drug and alcohol use have changed with polysubstance use, particularly opiates, crack cocaine, and alcohol, being more common and carrying greater risk. The baby born to the opiate-dependent mother is at risk of opiate withdrawal in the neonatal period; to the cocaine/crack using mother to neurological instability in the neonatal period and the potential for cognitive delay in infancy; to the alcohol-dependent mother to fetal alcohol syndrome and to the injecting drug using mother to infection with HIV, hepatitis B, and hepatitis C.
Injecting drug use carries the risk of infection, particularly with hepatitis B and C, and HIV. Rates of immunization against hepatitis B have increased encouragingly. The rate of HIV infection in England remains between 1% and 2% in the drug-using population but hepatitis C infection is estimated to be between 50% and 70%.
Engagement in antenatal services remains problematic for a proportion of drug and alcohol users with ‘late booking’. This is, in part, due to fear of social service involvement and also due to the irregularity of menstrual cycles, particularly in opiate users. The Hidden Harm report (ACMD 2003) estimated that there are 250 000–350 000 children of drug misusers in the UK, that drug misuse causes harm to children, and that effective treatment of the parent can have major benefits for children. Aetiology
It is noteworthy that some of the effects of exposure to drugs in utero are common across classes of drugs. Social deprivation, nicotine consumption, poor nutrition, poor compliance with healthcare, and high levels of blood-borne viral infections compound the fetal state. These common problems are those of intrauterine growth restriction, preterm deliveries, and increased rates of low birthweight and perinatal deaths.
Heroin use has a higher rate of small for date babies and preterm deliveries. There is evidence that the level of methadone exposure in utero correlates with the incidence of neonatal abstinence, although more recent evidence contests this finding.
Cocaine-exposed pregnancies have a higher rate of third trimester abruption, stillbirth, and neonatal death.
Fetal alcohol syndrome rates range from 0.5% to 1.3% of deliveries. Women who drink more than 7 units/week or 5 units/24 hours are at increased risk.
Nicotine predisposes to preterm birth and low birth-weight babies. Prognosis
Engagement in drug/alcohol treatment services, with the aim of achieving stability across parameters of behaviour, improves outcomes in terms of substance misuse and also engagement with antenatal and medical services. Cessation of illicit drug consumption with the aid of substitute opioid for the opiate-dependent woman, detoxification from alcohol, psychological interventions to reduce or cease stimulant use, medical assessment, and social interventions all improve outcomes for the neonate. All pregnant women should be screened for drug and alcohol use as early intervention and treatment reduces length of exposure by the fetus. As exemplified in the Confidential Enquiry into Maternal and Child Health (2007) ‘all women should be routinely asked in early pregnancy about current and previous mental health problems including their use of prescribed and non prescribed medicine and legal and illegal substances including tobacco and alcohol’. Clinical approach
Education about the risks to the fetus and neonate of drug and alcohol use should be routinely available to women of fertile age, in education services, in primary and in secondary care.
All drug and alcohol services in the UK now prioritize the treatment of pregnant women in recognition of the advantages of early engagement. Such services are ideally placed to assist the woman in accessing and attending antenatal services. Integrated services, although seldom available, are recommended, as these women have multiple social, psychological, medical, and psychiatric needs. There is a need for better communication about past history and present state between services and for improved assessment of drug and alcohol consumption across services.
Drug and alcohol abusers have a high comorbidity with mental illness, particularly mood disorders, and therefore assessment of mental state should be undertaken to enable early identification and treatment.
Opiate detoxification is not recommended during the first trimester; it should be undertaken at a slow rate during the second trimester and continued, with caution, during the third trimester. Detoxification should only proceed if stability is maintained as a neonate exposed to higher doses of methadone has a better prognosis than if exposed to illegal heroin.
Cocaine users should be offered psychosocial interventions as substitute prescribing is not available.
Alcohol-dependent pregnant women should be offered detoxification with benzodiazepines, the dose of benzodiazepine being kept as low as is possible to achieve abstinence.
All pregnant women should be encouraged to stop smoking and offered access to smoking cessation groups.
Services should make efforts to retain this group of women in treatment after delivery as it is evident that the families and children of drug and alcohol parents have significant need of continued help. Further reading
ACMD Hidden Harm: responding to the needs of children of problem drug users: London: Advisory Council for the misuse of drugs 2003.
Addis A, Moretti ME, Ahmed SF, Einarson TR, Koren G. Fetal Effects of cocaine: an updated meta-analysis. Reprod Toxicol 2001;15:341–367.
American Psychiatric Association (ASA). Diagnostic and Statistics Manual for Mental Disorders (DSM) American Psychiatric Association. ASA 1994.
Confidential Enquiry into Maternal and Child Health ‘Saving Mothers’ Lives’. The Seventh Report into Maternal Deaths in the UK 2007.
Confidential Enquiry into Maternal and Child Health Saving Mothers’ Lives. The seventh report into maternal deaths in the UK. London: CEMACH 2007.
Drug misuse and dependence: UK guidelines on clinical management. DH England, the Scottish Government, Welsh Assembly Government, and Northern Ireland Executive 2007.
Evidence Based Guidelines for the pharmacological management of substance misuse, addiction and comorbidity: recommendations from the British Association for Psychopharmacology 2004. J Psychopharm 18:293–335.
General Household Survey ONS 2002.
Kaltenbach K, Finnegan L. Children of maternal substance misusers. Curr Opin Psychiat 1997;10:220–4.
Lumley J, Oliver S, Waters E. Interventions for promoting smoking prevention during pregnancy. Cochrane Database Syst Rev 2000;2:CD001055.
NHS Information Centre Statistics on Alcohol England 2006.
Stratton K, Howe C, Battaglia F. Fetal alcohol syndrome: diagnosis, epidemiology, prevention and treatment. Washington DC: National Academy Press 1996.
Survey by NHS Information Centre, National Centre for Social Research, National Foundation for Educational Research; The Health and Social Care Information Centre 2008.
World Health Organization (WHO). International Classification of Diseases (ICD) WHO 1992.
Syphilis Definition
Syphilis is generally considered a sexually transmitted infection caused by the spirochete Treponema pallidum. It develops through different stages over time if undiagnosed and untreated. Syphilis is of particular concern during pregnancy secondary to the risk of transplacental transmission resulting in congenital syphilis infection in the fetus. Clinical features
The stages of syphilis are defined below.
• Primary syphilis is the first manifestation characterized by a painless papule at the site of inoculation which ulcerates into the classic chancre. The chancre will resolve spontaneously within 3–6 weeks even without treatment. Horizontal transmission is about 30%.
• Secondary syphilis is a systemic process involving widespread dissemination of spirochetes beginning approximately 6 weeks to 6 months after initial infection, and occurs in about 25% of untreated individuals. Clinical signs include lymphadenopathy, genital condyloma lata, and an extensive maculopapular rash, particularly involving the palms and soles. Horizontal transmission is about 30%.
• Latent syphilis is the diagnosis of asymptomatic infection documented with positive serology but absent manifestation on physical examination. If this occurs within 1 year of inoculation it is called early latent; if the diagnosis occurs after 1 year or cannot be determined it is defined as late latent syphilis. Congenital transmission is extremely high during the first 4 years after inoculation when spirochetaemia is common.
• Tertiary (late) syphilis occurs after the first stages of syphilis defined above, and can arise as early as 1 year after inoculation but more frequently occurs late, 20–30 years afterwards. It is slow and progressive and can involve the central nervous system, cardiovascular system, or skin and subcutaneous tissues.
• Congenital syphilis occurs via transplacental transmission of T. pallidum to the fetus and can occur at any time during pregnancy and at any stage of the maternal disease. It can result in intrauterine growth restriction, intrauterine fetal demise, neonatal death, preterm birth, and congenital infection and anomalies. Fetal effects depend on stage of development at time of infection. Epidemiology
The first well-documented outbreak of syphilis was in Naples in 1494, and subsequently spread throughout Europe. In 2001, the WHO estimated 12 million new cases per year globally in adults. Since 1998, there has been a dramatic increase in the diagnosis of syphilis in both heterosexual and homosexual populations, which has been attributed to an increase in intravenous drug abuse and human immunodeficiency virus (HIV) infection. The incidence of congenital syphilis correlates directly with the rate of syphilis in women of childbearing age. Today, most cases occur in women who did not receive prenatal care or who were inadequately treated. Global estimates of congenital syphilis range from approximately 750 000 to 1.5 million cases annually.
The risk of vertical transmission in an infected, untreated mother is significant but diminishes as maternal disease progresses. During primary syphilis perinatal transmission ranges from 70% to 100%, during secondary syphilis about 50%, during early latent disease about 40%, and during late latent and tertiary syphilis there is about 10% vertical transmission.
Treatment of maternal syphilis is the most important factor in the eradication of congenital syphilis. Vertical transmission is decreased to 1–2% in women who are adequately treated during pregnancy. Therefore, maternal screening with subsequent antenatal surveillance and adequate treatment are imperative to reducing the global impact of congenital syphilis. Implications
Congenital syphilis and its morbidity have significant economic and social implications. Numerous economic analyses of the value of universal screening of pregnant women for syphilis have indicated it is a cost-effective approach. Most industrialized countries recommend universal screening of pregnant women. In developing countries, screening of pregnant women for syphilis is a public health bargain. When using traditional screening methods for syphilis, it is about 25 times more cost-effective in preventing one disability-adjusted life year among infants compared with those born to women who are HIV positive.
Societal and emotional implications of congenital syphilis are important as well. The loss of an infant or birth of an afflicted infant with congenital syphilis could lead to feelings of guilt, blame, and depression. Clinical approach
Risk factors
• Poor socioeconomic status
• Sexual promiscuity
• Prostitution
• Use of illicit drugs
• HIV infection
• Lack of prenatal care
• Unmarried
• Black race
• Hispanic ethnicity
• Age less than 25 years
• Multiparity.
Screening and diagnosis
Although diagnosis of primary or secondary syphilis is quickest and most direct with darkfield microscopy and direct visualization of spirochetes, this requires the proper equipment and trained clinicians. In practice, darkfield microscopy is usually limited to clinics that specialize in the diagnosis of sexually transmitted infections. Alternatively, the predominance of clinical sites utilize serological testing, both non-treponemal and treponemal tests are available.
Non-treponemal tests, also known as reagin antibodies, test the patient’s serum for reactivity to cardiolipin-cholesterol-lecithin antigen. They include the venereal disease research laboratory (VDRL) test and rapid plasma reagin (RPR) test, and are inexpensive and used primarily for screening or following treatment response. Positive tests are usually reported as a titre.
Treponemal tests are more complicated and are usually used as confirmatory tests. These tests include fluorescent treponemal antibody absorption (FTA-ABS), the micro-haemagglutination test for antibodies to T. pallidum (MHATP), and the T. pallidum particle agglutination assay (TPPA) and are based on detection of antibodies against treponemal cellular antigens. These tests are qualitative and reported as either reactive or non-reactive. Acute and chronic false positive results can occur with both nontreponemal and treponemal methods; therefore, use of a single test to diagnose syphilis is inadequate. False-positive results can be associated with febrile illnesses, immunizations, autoimmune conditions particularly systemic lupus erythematosus (SLE), intravenous drug use, and chronic liver disease, and HIV infections.
Other tests for detecting syphilis include direct fluorescence antibody testing (DFA-TP) and multiplex polymerase chain reaction (M-PCR); however, these test require specialized equipment and personnel and are not widely available in most outpatient settings.
The current Centers for Disease Control (CDC) guidelines recommend syphilis screening at the first prenatal visit, and for patients at high risk again during the third trimester and at delivery.
Patients with reactive serological tests for syphilis should be assessed for the stage of progression. Major morbidity occurs in the tertiary phase, including neurosyphilis. Identifying asymptomatic neurosyphilis in the latent phase is important in the optimal management of any patient with reactive syphilis serologies. Cerebrospinal fluid analysis via lumbar puncture is essential in anyone with latent syphilis, who has ophthalmic or neurological signs or symptoms, treatment failure or coexistent HIV infection, or is thought to have active tertiary syphilis. Management
Antepartum syphilis management must consider that both maternal and likely fetal infections are present. Ultrasound can be used as a tool to determine the extent of fetal disease during the second half of pregnancy, after 20 weeks. This will assist in maternal counselling about the efficacy and potential complications associated with treatment. In the latter part of pregnancy, if there are ultrasonographic signs of fetal disease, for example, hepatosplenomegaly or hydrops fetalis, a perinatologist and neonatalogist should be consulted. An abnormal ultrasound indicates antepartum fetal heart rate monitoring prior to instituting antibiotic treatment. Sonographic signs of fetal syphilis combined with abnormal fetal heart rate pattern may indicate a severely affected fetus with possible impending fetal demise.
Penicillin continues to be the gold standard in the treatment of syphilis, both in pregnancy and outside pregnancy. Treatment should be pursued in pregnancy when there is
• evidence of spirochetes on darkfield microscopy
• positive serologies with confirmation by specific treponemal test
• history of sexual contact with someone who has confirmed syphilis
• prior history of syphilis with treatment but continues to have persistently elevated or rising titres ≥1:4.
Adequate treatment is effective in preventing maternal vertical transmission to the fetus, treating maternal disease, and treating established early fetal disease.
Primary syphilis, if there are documented negative serologies in the past year or adequate documentation of a recent chancre, can be treated with a single dose of penicillin G benzathine 2.4 millions units intramuscularly.
In all other cases, the disease should be considered latent syphilis of unknown duration and treated with a course of three intramuscular injections of penicillin G benzathine 2.4 million units spaced a week apart. However, neurosyphilis requires aqueous crystalline penicillin G between 12–24 million units daily in divided intravenous doses for 10–14 days.
Treatment of maternal syphilis is more complicated when the pregnant woman has a penicillin allergy, about 5–10% of cases. Confirmation of the penicillin allergy with skin testing is recommended, unless there is a documented anaphylactic reaction. The only well-studied and established treatment of women diagnosed with syphilis in pregnancy who have a true penicillin allergy is penicillin desensitization followed by penicillin treatment. Oral penicillin desensitization is given in small, gradually increasing doses with inpatient monitoring over approximately 4 hours, followed by the administration of the therapeutic dose intramuscularly 30 minutes after completion. Most adverse reactions can be managed supportively without discontinuation of the desensitization protocol. Complications
The Jarisch–Herxheimer reaction is a common systemic reaction to the treatment of syphilis occurring in approximately 45% of pregnant women, during the first course of penicillin. It is thought to result from an endotoxin-like substance released when a large number of T. pallidum are killed by the antibiotics, although the true mechanism has not been elucidated. It is characterized by headache, malaise, rash, and hypotension with onset usually one to 12 hours after the initial administration of antibiotic. Symptoms can last from several hours to a few days and should be managed supportively. The reaction is not seen with subsequent antibiotic doses. The Jarisch–Herxheimer reaction can precipitate preterm contractions and preterm labour, and fetal heart tracing changes that can be concerning, therefore fetal monitoring should be considered. Follow-up and future pregnancy
The same non-treponemal antibody serological titre used for diagnosis should be utilized to follow therapeutic response at 1-, 3-, 6-, 12-, and 24-month intervals. Patients with primary or secondary syphilis should have a fourfold decrease in their titre by 6 months and eightfold by 1 year. Those with early latent syphilis may only decline by fourfold over a 1-year period. If titres do not decline appropriately, at least fourfold, or show an increase, this probably represents either treatment failure or reinfection and the treatment regimen should be repeated. Consideration of testing for neurosyphilis is also recommended.
Women diagnosed with syphilis should be offered testing for other sexually transmitted infections, including HIV infection. Their sexual contacts should also be identified and offered treatment. Syphilis infection should be reported as indicated by local authorities. The infant’s paediatrician should be notified at the time of delivery if not done previously, so they can pursue a thorough evaluation of the newborn for congenital syphilis. Further reading
Ray, JG, Lues-Lues. Maternal and fetal considerations of syphilis. Obstet Gynecol Surv 1995;50:845.
Fiumara N, Fleming W, Downing J, Good F. The incidence of prenatal syphilis at the Boston City Hospital. N Engl J Med 1952;247:48–52.
Schmid GP, Stoner, BP. The need and plan for global elimination of congenital syphilis. Sexually Transmitted Dis 2007;34: S5–S10.
Chakraborty, R Luck, S. Managing congenital syphilis again? The more things change … Curr Opin Infect Dis 2007;20:247–52.
Walker DG, Walker GJ. Forgotten but not gone: the continuing scourge of congenital syphilis. Lancet Infect Dis 2002;2:432–6.
Wiwanitkit V. Screening for syphilis in pregnancy: which is the proper method? Arch Gynecol Obstet 2007;276:629–31.
Wendel GD Jr, Sheffield JS, Hollier LM, et al. Treatment of syphilis in pregnancy and prevention of congenital syphilis. Clin Infec Dis 2002;35(Suppl 2): S200–9.
Wendel GD Jr, Stark BJ, Jamison RB, et al. Penicillin allergy and desensitization in serious infections during pregnancy. N Eng J Med. 1985;312:1229–32.
Myles TD, Elam G, Park-Hwang E, et al. The Jarisch-Herxheimer reaction and fetal monitoring changes in pregnant women treated for syphilis. Obstet Gynecol 1998;92:859–64.
#MMWR Sexually transmitted diseased treatment guidelines. MMWR Recomm Rep (RR-11) 2006;55:1–95.
Thromboembolic disease Definition
Pregnancy is a hypercoagulable, thrombogenic state. This has a synergistic effect with inherited and acquired thrombophilias: a predisposition to thrombosis. The three clinical conditions that arise from abnormal clotting mechanisms in pregnancy are deep vein thrombosis (DVT), pulmonary embolism (PE), and adverse obstetric outcomes. Epidemiology
The risk of venous thromboembolism in pregnancy lies between 1 and 2 per 1000 pregnancies. The relative risk for venous thromboembolism in pregnancy and the puerperium is 4.3 compared to non-pregnant women, being five times higher in the postpartum period compared with during pregnancy. PE was also many-fold more common after than before birth. Inherited thrombophilias comprise about 15% of the population, but are responsible for up to 50% of venous thromboembolism in the pregnant and postpartum period. Pathophysiology
The classical Virchow’s triad includes venous stasis, endothelial injury and activation of coagulation status. Pregnancy is a thrombogenic physiological state. There is an increase in the circulating levels of fibrinogen and most clotting factors. Fibrinolytic activity is decreased with increased levels of fibrinolytic inhibitors. Levels and activity of protein S decrease in pregnancy, and resistance to activated protein C increases in later pregnancy.
Patients with acquired or inherited thrombophilias are at an even higher risk of thromboembolic complications during pregnancy. Patients with antiphospholipid antibody syndrome are at a greater risk of thrombosis. This is paradoxical to the in vitro prolonged partial thromboplastin time. Antiphospholipid autoantibodies, directed against plasma proteins bound to anionic phospholipids include lupus anticoagulants, anticardiolipin antibodies, and β2-glycoprotein-I antibodies.
Among the inherited thrombophilias, the guanine-to-adenine mutation at nucleotide 1691 (G1691A, factor V Leiden, FVL) is the most common abnormality in patients with thromboembolic disease. A similar autosomal dominant heterozygous G-to-A mutation in the prothrombin gene (G20210A, PGM) is associated with an elevated plasma prothrombin level and a fivefold increased risk of venous thrombosis. Other causes of inherited thrombophilias include antithrombin deficiency, protein C deficiency, and protein S deficiency. The role of the C-to-T mutation in the 5,10-methylenetetrahydrofolate reductase (C677T) causing elevated plasma homocysteine levels is uncertain, but probably not significant in pregnancy.
Maternal thrombophilias are associated with poor pregnancy outcomes, causing recurrent miscarriages, fetal growth restriction, pre-eclampsia, placental abruption, and intrauterine fetal demise. Clinical approach
Diagnosis
History
• Only half of the patients with DVT have symptoms. These include pain and swelling of the calf/leg. Symptoms of PE include dyspnoea, chest pain, cough, and haemoptysis.
• Antiphospholipid antibody syndrome (APS) should be suspected if (1) there has been at least one unexplained thrombotic/thromboembolic event, (2) at least one specific adverse pregnancy outcome, or (3) unexplained thrombocytopenia/prolonged prothrombin time/activated partial thromboplastin time (PT/aPTT).
• Inherited thrombophilias should be suspected in patients with a history of venous thromboembolism or recurrent unexplained fetal losses after 10 weeks of amenorrhoea.
Examination
• In DVT, there may be fever, and swelling, warmth, and erythema of the affected leg; Homan’s sign is not reliable.
• In PE, pyrexia, dyspnoea, tachypnoea, tachycardia, cyanosis, pleural effusion, pleural rub, raised jugular venous pressure, and right ventricular failure may be observed.
• There may be few clinical signs in acquired/inherited thrombophilias. Often, these are diagnosed on investigations. Patients with secondary APS may have physical findings such as joint swelling and tenderness that are more likely to be related to other autoimmune disorders.
Laboratory investigations
These tests are important to make the diagnosis of thromboembolic diseases, and their underlying thrombophilias.
• Compression duplex ultrasonography to detect the thrombus in the leg vein.
• Contrast venography is the gold-standard test for DVT, but may not be suitable as a first line investigation due to patient discomfort.
• Impedence plethysmography, computed tomography (CT) and magnetic resonance venography diagnosis of DVT may be available in specialised centres.
• Pulse oximetry readings in room air may be less than 95% in PE.
• Arterial blood gases in PE would usually show hypoxaemia, hypercapnia, and respiratory alkalosis.
• Serum troponin levels may be elevated in patients with a large PE.
• Electrocardiogram (ECG) changes may be typical in PE (e.g. S1Q3T3), especially in patients with massive PE and cor pulmonale.
• Chest X-ray may show cardiomegaly, atelectasis, mediastinal changes, pulmonary parenchymal abnormalities, and pleural effusion.
• Echocardiography reveals evidence of right heart strain in less than half the cases with PE.
• Ventilation-perfusion (V/Q) scan can be diagnostic.
• Spiral CT with intravenous contrast is now commonly used to diagnose PE.
• Pulmonary angiography is the gold standard in the definitive diagnosis of acute PE.
• Full blood counts could reveal leucocytosis in DVT/PE, and thrombocytopenia in acquired thrombophilias.
• D-dimers have a high negative predictive value in the diagnosis of PE, but these should be used in conjunction with other imaging techniques described above.
• Lupus anticoagulant activity by a prolonged aPTT.
• Anticardiolipin and β2-glycoprotein I antibodies, enzyme-linked immunosorbent assays for IgG and IgM.
• Protein C and Protein S activity
• Factor V Leiden activity
• Antithrombin activity.
Management
Deep vein thrombosis
When suspected, treatment with low molecular weight heparin (LMWH) should be initiated until diagnostic investigations are complete. The leg should be elevated and a graduated elastic compression (thromboembolic deterrent, TED) stocking used to reduce oedema. Intermittent pneumatic leg compression is now being used more frequently perioperatively to reduce the likelihood of DVT. LMWH is a safe and effective alternative to unfractionated heparin as an anticoagulant in pregnancy. It should be given daily in two divided doses titrated against the woman’s most recent weight. Peak anti-Xa activity need be measured in underweight or overweight women only. Treatment should be continued for 6 months from the initial episode, or up to 3 months after delivery, whichever is longer.
Low dose subcutaneous unfractionated heparin and warfarin are alternatives to LMWH, but used less frequently now.
Pulmonary embolism
Upon diagnosis, or suspicion of diagnosis, respiratory and haemodynamic support needs to be initiated immediately. Intravenous unfractionated heparin is the initial treatment of choice. This condition needs to be jointly managed by senior physicians, obstetricians and radiologists. In life-threatening cases, thrombolysis with streptokinase and surgical embolectomy can be considered. In special circumstances such as recurrent PE, temporary inferior vena caval filters can be used. Warfarin can be used in the post-partum period as maintenance therapy.
Antiphospholipid antibody syndrome
These patients should be comanaged with a physician, and any underlying autoimmune diseases treated as may be necessary. In early pregnancy, normally rising titres of human chorionic gonadotrophin (hCG) indicate a good prognosis in most cases; the corollary is also true. The patients should be counselled and examined regularly for the symptoms and signs of thromboembolic disease. They should be assessed for pre-eclampsia, fetal growth restriction, and evidence of intrauterine fetal demise at frequent intervals, and counselled to observe for contractions, bleeding, and decreased fetal movements. LMWH can be used during pregnancy in these patients, and warfarin may be used in the postpartum period. Timing and mode of delivery would depend on antenatal progress.
Inherited thrombophilias
Anticoagulant therapy in inherited thrombophilias depends on past history of thrombotic events, pre-pregnancy use of anticoagulants and history of recurrent miscarriages. The evidence for use of aspirin and low-dose heparin in patients with recurrent miscarriages is clear, but clear evidence that these are beneficial in inherited thrombophilias in those with no previous complications is still lacking. In contrast, it is generally accepted that these patients need anticoagulant therapy with prophylactic/intermediate dose unfractionated heparin or LMWH if they are homozygous for FVL or PGM mutations, compound heterzygotes for FVL/PGM, or have protein C/antithrombin deficiency. A past history of venous thromboembolism may require therapeutic doses of anticoagulation with heparin ante and post-partum.
Patients with a lower risk of thromboembolic disease such as heterozygotes for FVL/PGM and protein S deficiency may benefit from low-dose aspirin antepartum, and postpartum thromboprophylaxis. Further reading
Bertina RM et al. Mutation in blood coagulation factor V associated with resistance to activated protein C. Nature 1994;369:64–7.
Gillham JC. Haematological conditions. Obstetrics and Gynaecology. An evidence-based text for MRCOG. Luesley DM, Baker PN (ed). Arnold, 2004.
Greer IA. The challenge of thrombophilia in maternal-fetal medicine. New Engl J Med 2000;342:424–5.
Helt JA et al. Trends in the incidence of venous throm-boembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med 2005;143:697–06.
Marik, Plante. Venous thromboembolic disease and pregnancy. New Engl J Med 2008;359:2025–33.
McColl MD et al. Risk factors for pregnancy associated venous thromboembolism. Thromb Haemost 1997;78:1183–8.
Miyakis S et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4:295–306.
Rai R et al. Randomised controlled trial of aspirin and aspirin plus heparin in pregnant women with recurrent miscarriage associated with phospholipid antibodies (or antiphospholipid antibodies). BMJ 1997;314:253–7.
Ray JG et al. Common C677T polymorphism of the methyl-enetetrahydrofolate reductase gene and the risk of venous thromboembolism: meta-analysis of 31 studies. Pathophysiol Haemost Thromb. 2002;32:51–8.
Thomson AJ, Walker ID, Greer IA. Low molecular weight heparin for the immediate management of thromboembolic disease in pregnancy. Lancet 1998;352:1904.
Thromboembolic disease in pregnancy and the puerperium: acute management. RCOG Green-top Guideline No. 28, Feb 2007.
Thromboembolism in pregnancy. ACOG practice bulletin #19. American College of Obstetricians and Gynecologists, Washington, DC, 2000. Patient resources
Venous thrombosis in pregnancy and after birth: information for you: www.rcog.org.uk/index.asp?pageID=2516
Thyroid and parathyroid disease Hypothyroidism
Definition
Thyroid hormone deficiency.
Epidemiology
More common in women. Affects 1% of pregnancies.
Causes
• Autoimmune lymphocytic thyroiditis (thyroid peroxidase autoantibodies):
• atrophic thyroiditis (no goitre)
• Hashimoto’s thyroiditis (goitre)
• Following treatment for hyperthyroidism with radioiodine (131I), partial thyroidectomy, or antithyroid drugs
• Other drugs, e.g. amiodarone, lithium, iodine
• Transient hypothyroidism: subacute/postpartum
Symptoms (*good discriminators)
• Similar to pregnancy: tiredness, lethargy, weight gain, constipation, fluid retention, muscle cramps
• Cold intolerance*
• Slowness of thought
Signs
• ± goitre
• Slow pulse rate*
• Slowly relaxing reflexes (especially ankle)*
• Dry skin
• Carpel tunnel syndrome.
Associated autoimmune diseases
Type 1 diabetes, pernicious anaemia, vitiligo
Diagnosis
↓free T4 (fT4) and ↑TSH: use pregnancy ranges (Table 8.38.1)
Effect of pregnancy on hypothyroidism
Requirements for increased dosage usually related to previous under-replacement
Effect of hypothyroidism on pregnancy
Fetus produces its own thyroxine >12 weeks. Before this time, it is dependent on maternal thyroxine. Maternal thyroxine replacement does not cause fetal hyperthyroidism as only small amounts cross placenta.
• Adequately treated, euthyroid in first trimester:
• no risks.
• Untreated and overt hypothyroidism risks:
• subfertility
• miscarriage and fetal loss
• Pre-eclampsia, abruption
• IUGR, prematurity.
Table 8.38.1 Normal pregnancy ranges of thyroid function tests (TFTs)

• Untreated or undertreated (subclinical) hypothyroidism in first trimester: risks in offspring:
• reduction in IQ (small if subclinical)
• neurodevelopmental delay.
Management
Prepregnancy counselling
Ensure adequate replacement of thyroxine
During pregnancy
Check thyroid-stimulating hormone (TSH) and fT4 (free thyroxine) at booking, second, and third trimesters. Adjust thyroxine dose according to pregnancy range.
If euthyroid at booking, it is unusual to have to adjust dose
If dose is amended:
• repeat thyroid function tests (TFTs) after 4–6 weeks
• check TFTs postpartum: most women maintain higher dose postpartum (as adjustment reflects previous under-replacement)
Complications
Fetal/neonatal hypothyroidism is very rare; the maternal TSH receptor-blocking antibodies (in a few patients with atrophic thyroiditis) cross the placenta and affect the fetal thyroid (usually has goitre). Hyperthyroidism
Definition
Thyroid hormone excess.
Epidemiology
It occurs more often in women and affects 1 in 800 pregnancies; 50% have a family history of thyroid disease.
Causes
• Graves’ disease (95%): TSH receptor stimulating antibodies (TSHR Ab) and specific antibodies against eye (occur in 50%). Both are present even when the disease is inactive.
• Toxic nodule: in a multinodular goitre/toxic solitary adenoma.
• Subacute thyroiditis (de Quervain’s): usually following URTI. Fever and painful thyroid.
• Drugs: amiodarone, iodine, lithium, or inappropriate use of thyroxine.
• Hydatidiform mole, choriocarcinoma (high hCG).
Symptoms (*good discriminators)
• Similar to pregnancy: sweating, palpitations, heat intolerance, emotional lability, vomiting
• Weight loss*.
Signs
• Goitre-check for retrosternal extension
• Palmar erythema
• Persistent tachycardia*
• Tremor*
• Eye signs (with Graves’ disease)*: proptosis, lid lag, lid retraction.
Diagnosis
• ↑free T3 and or ↑free T4 and suppressed TSH (use pregnancy ranges)
• TSHR Ab (helps distinguish from hyperemesis).
Differential diagnosis
• fT4 and clinically euthyroid
• Hyperemesis gravidarum
• Non-thyroid illness: sick euthyroid.
Effect of pregnancy on hyperthyroidism
• Improvement especially second and third trimesters
• Worsening in first trimester (related to ↑hCG) and in puerperium.
Effect of hyperthyroidism on pregnancy
• Adequately treated, euthyroid patient:
• transplacental transfer of antithyroid drugs and TSHR Ab can affect fetus.
• Untreated and overt hyperthyroidism—risks:
• subfertility
• miscarriage, fetal loss
• IUGR, prematurity
• thyroid storm (see Complications).
Management
Women should not conceive for 4 months following 131I.
During pregnancy
Check fT3, fT4 and TSH in each trimester.
Antithyroid drugs: propylthiouracil (PTU), carbimazole
• Continue in pregnancy. Don’t switch drugs. Can often reduce dose maintaining free T4 at higher end of normal range for pregnancy
• Transplacental transfer: PTU less than carbimazole. They counteract stimulatory effect of TSHR Ab on fetal thyroid
• Carbimazole rarely causes aplasia cutis (scalp skin defect).
Newly diagnosed thyrotoxicosis in pregnancy
• Start PTU 200–300 mg bd/carbimazole 40–60 mg.
• Add propranolol 40 mg bd tds if significant palpitations, tremor or sweating (usually for 2–3 weeks)
• Check FBC 1 week later (agranulomatosis and neutropenia rare: must report sore throat)
• Check fT3, fT4 and TSH 2–4 weekly initially
• Usually can start to reduce dose after 4–6 weeks
• Aim to control thyrotoxicosis with smallest dose of drugs possible.
Thyroidectomy: rare in pregnancy:
• Retrosternal goitre causing stridor/dysphagia
• Thyroid cancer
• Allergies to both PTU and carbimazole.
Radioiodine (131I)
• Contraindicated in pregnancy and breastfeeding
• Avoid pregnancy for a minimum of 4 months.
Fetal wellbeing
• USS for fetal growth, goitre and heart rate if high titre of TSHR Ab, poorly controlled or newly diagnosed Graves’ disease.
Postpartum
Breastfeeding safe with PTU ≤150 mg/day and carbimazole ≤15 mg/day.
Complications
Thyroid storm (thyroid crisis)
Medical emergency: urgently liaise with endocrinologists
• Rare: can be precipitated by delivery in a patient with undiagnosed Grave’s disease
• Clinical: hypermetabolic with fever, sweating, marked tachycardia; can develop congestive cardiac failure, delirium/psychosis
• Treat with large doses of PTU, dexamethasone, hydration and paracetamol for pyrexia
• Fatal without treatment.
Fetal/neonatal thyrotoxicosis
• One per cent of babies whose mothers have current or previous Graves’ disease (even if now hypothyroid following surgery/radioactive iodine).
• Fetal tachycardia, IUGR, goitre, accelerated bone maturation.
• Without treatment fetal mortality up to 50%, neonatal mortality up to 15%.
• If fetus affected, treat mother with antithyroid drugs (maintain maternal euthyroidism with thyroxine).
• Neonate becomes symptomatic after maternal antithyroid drugs cleared. Postpartum thyroiditis
Prevalence
• Variable: 2–17%
• 25% family history autoimmune thyroid disease
• 50–70% with thyroid peroxidise antibodies
• More common in type 1 diabetics.
Pathology
Autoimmune lymphocytic destruction of thyroid gland initially causing release of pre-formed thyroxine (hyperthyroid phase) and subsequently causing hypothyroidism as stores used up.
Clinical
Vague symptoms occur 3–4 months postpartum. Variable progression often resolving spontaneously:
• Only hyperthyroidism (40%)
• Only hypothyroidism (40%)
• Hyperthyroidism initially, then hypothyroidism for several months (20%).
Diagnosis
• TFTs: identifies hypothyroidism/hyperthyroidism
• Antithyroid antibodies (in 80–85%)
• Distinguish from flare of Graves’: postpartum thyroiditis has no TSHR Ab and poor uptake on radioactive iodine/technetium scans.
Management
• Treat only if symptomatic (course unaltered):
• Hyperthyroidism: beta-blockers not antithyroid drugs
• Hypothyroidism: thyroxine—stop after 6–8 months to see if resolved
• Annual TFTs if thyroid peroxidise Ab positive as 20% develop permanent hypothyroidism in 4 years.
Prognosis
• Remain hypothyroid: 3–4%
• Recurrence after future pregnancy: 70%. Thyroid nodules/thyroid cancer
Incidence
1% (up to 40% diagnosed in pregnancy are malignant).
Cause
• Multinodular goitre
• Cyst (usually benign)
• Adenoma
• Malignancy.
Clinical
Suspect malignancy if
• Nodule is hard and fixed
• Rapid growth
• lymphadenopathy.
Diagnosis
Urgent referral to endocrine surgeon:
• TFTs and thyroid antibodies
• Thyroglobulin (can also be raised with goitre, Hashimoto’s and Grave’s disease). Level >100 μg/L suspicious of malignancy
• USS thyroid: cyst/solid
• Aspiration of cyst: fluid to cytology
• Fine needle biopsy
• Iodine scanning contraindicated in pregnancy.
Management
Malignancy:
• Pregnancy does not affect the course of differentiated thyroid cancer
• Surgery safest in second trimester (can perform in third trimester if necessary)
• postoperative thyroxine to suppress TSH (residual tumour dependent on TSH for growth)
• future pregnancies: check thyroglobulin level (should be low/undetectable) and keep TSH suppressed with thyroxine. Hyperparathyroidism
Incidence
Rare: 8 in 100 000 women of childbearing age.
Pathology
• Primary hyperparathyroidism
• hyperplasia
• adenoma
• malignancy (very rare)
• Secondary hyperparathyroidism (prolonged hypocalcaemia)
• vitamin D deficiency
• renal insufficiency
• Tertiary hyperparathyroidism.
Clinical
• Asymptomatic
• Features of hypercalcaemia: thirst, vomiting, malaise, bone pain, abdominal discomfort (pancreatitis, renal stones, constipation), depression, hypertension.
Diagnosis
• ↑corrected calcium, ↑PTH
• ↑calcium excretion in 24-hour urine collection
• USS/MRI neck: may detect parathyroid adenoma
• Isotope studies contraindicated in pregnancy
• Surgical exploration of neck.
Differential diagnosis (of hypercalcaemia)
• Sarcoidosis
• Malignant disease with bone secondaries
• Vitamin D toxicity
• Excess antacids use (contain calcium)
• Familial hypocalciuric hypercalcaemia.
Effect of pregnancy on hyperparathyroidism
↓level of calcium in pregnancy (↑GFR, fetal demands); may rebound back up postnatally
Effect of hyperparathyroidism on pregnancy
• Miscarriage and fetal loss
• Preterm labour.
Management.
Multidisciplinary care with endocrine surgeons
Aim to reduce corrected calcium level to upper limit of normal
• ↑fluids (orally, may need intravenously)
• Low calcium diet +/– oral phosphate
• Symptomatic cases/conservative measures ineffective:
• Surgical excision of abnormal parathyroid gland(s)
• Post-surgery daily bloods initially to detect low calcium.
Complications
• Acute pancreatitis: especially postpartum
• Neonatal hypocalcaemia:
• Fetal PTH suppressed by high maternal calcium
• Postnatally: neonatal seizures and tetany from neonatal hypocalcaemia as calcium no longer supplied from mother. Occurs within 2 weeks of delivery, or up to 2 months if baby breast fed. Hypoparathyroidism
Incidence
Rare.
Causes
• Inadvertent removal parathyroid glands following thyroidectomy (3%)
• Autoimmunity.
Diagnosis
↓corrected calcium, ↓PTH.
Effect of pregnancy on hypoparathyroidism
Further ↓level of calcium in pregnancy (↑GFR, fetal demands).
Effect of hypoparathyroidism on pregnancy
• Miscarriage and fetal loss
• Fetal hypocalcaemia, bone demineralisation
• Neonatal hypocalcaemia and rickets.
Management
• Vitamin D (alfacalcidol or calcitriol) and calcium supplementation
• increased requirement in pregnancy
• reduce dose postnatally
• Measure corrected calcium monthly.
Complications
• Neonatal hypocalcaemia seizures and tetany
• Maternal osteoporosis. Further reading
Feldt-Rasmussen U, Hoier-Madsen M, Rasmussen NG, et al. Antithyroid peroxidise antibodies during pregnancy and postpartum. Relation to postpartum thyroiditis. Autoimmunity 1990; 6:211–4.
Girling J. Thyroid disease and pregnancy. In: de Swiet M (ed.). Medical disorders in obstetric practice. Oxford: Blackwell Science 2002:415–38.
Haddow JE, Palomaki GE, Allen WC, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development in the child. N Eng J Med 1999;341:549–55.
Leung AS, et al. Perinatal outcome in hypothyroid pregnancies. Obstet Gynecol 1993;81:349–53.
Mestman JH. Parathyroid disorders of pregnancy. Semin Perinatol 1998;22:485–96.
O’Doherty MJ, McElhatton PR, Thomas SHL. Treating thyrotoxicosis in pregnant or potentially pregnant women. BMJ 1999;318;5–6.
Pop VJ, Kuijpens JL, van Baar AL, et al. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin Endocrinol 1999;50:149–55.
Tan GH, Gharib H, Goeller JR, et al. Management of thyroid nodules in pregnancy. Arch Intern Med 1996;156:2317–20.
Wolfberg AJ, Lee-Parritz A, Peller AJ, Lieberman ES. Obstetric and neonatal outcomes associated with maternal hypothyroid disease. J Matern Fetal Neonatal Med 2005;17:35–8.
Toxoplasmosis in pregnancy Definition
Toxoplasmosis is an infection caused by the intracellular parasite Toxoplasma gondii. It can be passed transplacentally from an infected mother to her unborn embryo/fetus causing congenital toxoplasmosis. Epidemiology
Toxoplasmosis is the most common parasitic infection worldwide. Toxoplasmosis is the third leading cause of food-borne illness death. In the USA it is estimated that 22.5% of the population has been infected with toxoplasmosis and approximately 15% of reproductive age women. Serological data indicate much higher rates of infection in France and South America. In the USA approximately 400–4000 infants are born each year with toxoplasmosis. The worldwide incidence of congenital toxoplasmosis is estimated to be 1–10/10 000 live births. Aetiology
Toxoplasma gondii exists in three stages: the oocyst, tachyozoite, and bradyzoite. The cat is the definitive host. When a cat ingests cysts of T. gondii, which are contained in the tissues of infected prey or raw meat, the parasite is released into the cat’s digestive tract. The organisms then multiply in the wall of the small intestine and produce oocysts. These oocysts are then excreted in great numbers in the cat’s faeces. Intermediate hosts, including humans, become infected when coming into contact with oocysts or ingesting other infected intermediate hosts. Oocysts and tissue cysts transform rapidly into tachyzoites upon ingestion. Tachyzoites represent an acute infection stage and localize to neural and muscle tissue. After the acute infection the tachyzoites develop into bradyzoites and they remain dormant for the remainder of the intermediate host’s life. In the tachyzoite form the parasite can be passed to an unborn child from its mother. Reproductive age women are at risk of acquiring an infection if they live in a high prevalence area (South America), eat undercooked/raw meat, have contact with contaminated soil, drink contaminated water, and/or own a cat. Prognosis
Toxoplasmosis infection, in an immunocompetent pregnant woman, is usually asymptomatic. Rarely can she develop a mononucleosis type illness including fever, fatigue, and lymphadenopathy. The risk to her unborn child is dependent on timing of seroconversion during gestation, with an approximate 10–15% transmission rate in the first trimester to a 60–70% transmission rate in the third trimester. Congenital infection tends to be more severe the earlier in gestation it is acquired, and can consist of fetal demise (rare), intracranial calcifications, hydrocephalus, and retinochoroiditis. Clinical approach
History
• Lives in or recent travel to endemic area
• Exposure to contaminated soil/water
• Cat owner
• Mononucleosis type illness with a cervical lymphadenopathy.
Examination/ultrasound findings
• Maternal vital signs/cervical lymph node palpation
• Fetus with hydrocephalus, intracranial calcifications, increased placental thickness, intrahepatic calcifications, hepatomegaly, ascites, pericardial effusion and/or pleural effusion.
Investigations
Maternal
• the difficulty in diagnosis lies in determining if the infection is active or chronic. The primary diagnostic tool is serological studies. An acute infection in pregnancy is most accurately diagnosed when at least two blood samples drawn at least 2 weeks apart show seroconversion from negative to positive, IgG or IgM. The sensitivity/specificity varies widely between laboratories; using a reference laboratory is recommended.
• Toxoplasmosis can also be isolated from infected fluids and/or tissues using special stains or PCR.
Fetal
• When primary maternal infection is suspected an amniocentesis should be performed and the fluid sent for PCR and/or mouse inoculation.
Counselling
• In proven fetal infection with ultrasound abnormalities the outcome can be poor including fetal demise, neonatal death, neurological impairment (mental retardation, seizures, need for ventricular shunt placement), and/or chorioretinitis.
• In documented fetal infection with no ultrasound findings fetal demise/neonatal death is rare. Approximately 80% of newborns show no clinical evidence of infection. Of those that do intracranial lesions and chorioretinitis are most common. A small percentage, 1–5%, will develop severe neurological impairment (as above) and up to 30% will develop retinochoroidal lesions, leading to blindness in rare cases.
Management
• Pregnancy termination
• Maternal infection: treatment with spiramycin, a macrolide antibiotic (not available in the USA), 1 g three times a day, may reduce the risk of fetal infection by up to 60%.
• Fetal infection: treatment with pyrimethamine and sulfadiazine, two drugs that act synergistically to inhibit the synthesis of folic acid, may decrease the severity of fetal manifestations. Various dosing regimes exist. Leucovorin, folinic acid, needs to be used as add back to prevent bone marrow suppression.
• Neonatal infection: treatment with pyrimethamine and sulfadiazine has been proven to decrease the rate of clinical manifestations. Various dosing regimes exist.
• Prevention is the best strategy, thorough cooking of meats, thorough washing/peeling of fruits and vegetables, thorough washing of cutting boards, dishes, counters, utensils and hands, pregnant women should wear gloves when gardening and pregnant women should avoid changing a cats litter box. Further reading
ACOG. Perinatal viral and parasitic infections. Practice Bulletin 2000, #20.
CDC. Preventing Congenital Toxoplasmosis. MMWR 2000, 49(RR02);57–75.
Foulon W, Pinon JM, et al. Prenantal diagnosis of congenital toxoplasmosis: a multicenter evaluation of different diagnostic parameters. Am J Obstet Gynecol 1999;181:843.
Foulon W, Villena I, et al. Treatment of toxoplasmosis during pregnancy: a multicenter study of the impact on foetal transmission and children’s sequelae at age 1 year. Am J Obstet Gynecol 1999;180:410.
Jones J, Lopez A, Wilson M. Congenital Toxoplasmosis: A Review. Ob Gyn Survey 2001:56:296–305.
Wallon M, Liou C, Garner P. Congenital toxoplasmosis: systematic review of evidence of efficacy of treatment in pregnancy. BMJ 199:318:1571–4. Internet resources
www.cdc.gov
www.ACOG.org
Vulvovaginal candidiasis Definition
This is a superficial fungal infection of the vulva and vagina by candidal species characterized by local inflammation, pruritus, and discomfort. There are more than 100 species of Candida but Candida albicans is responsible for more than 95% of human disease. Some of the other non-albicans Candida species that cause diseases in man include C. tropicalis, C. glabrata, C. krusei, and C. parapsilosis. Epidemiology
Candida may be detected in the vagina of 5–10% of non-pregnant women and in up to 40% of pregnant women. The overwhelming majority of these women are completely asymptomatic. Pathogenesis
• The Candida detected in the vagina of asymptomatic women usually exists in the spore or yeast format as commensals unless their numbers increase rapidly due to alteration in the local or systemic cell-mediated immunity. The characteristic symptoms associated with thrush are caused by the transformation of the Candida from the spore phase into the invasive hyphae phase. It is the cell-mediated immunity through interferon-gamma (IFN-γ) that controls and inhibits this transformation and therefore the germination, growth, and proliferation of Candida in the vagina. Almost all women have antibodies to Candida but these antibodies are not protective and do not prevent the growth of Candida. Therefore, women with genetic or acquired alteration of cell-mediated immune function are predisposed to recurrent vulvovaginal candidal infections.
• About 20% of recurrent vulvovaginal candidiasis are due to allergic reactions to seminal components, fabrics of under clothing, douches, contraceptive spermicides, condoms, hygienic products, including soaps, and even candidal antigens. The histamine release associated with the immediate hypersensitivity response stimulates the release of prostaglandin from macrophages, which in turn inhibits the production of interleukin (IL)-2 by T-lymphocytes, thereby temporarily paralysing the cell-mediated immune response. This results in diminished inhibition and regulation of the growth of candida.
Risk factors
• Diabetes mellitus: the hyperglycaemia associated with diabetes enhances the adherence of yeast to the vaginal epithelial cells, impairs phagocytosis and supplies the Candida with essential nutrients for growth.
• Pregnancy and combined oral contraceptive: pregnancy and the pill suppress T-cell immunity and generate sugar substrates in the vagina by increasing mucosal glycogen stores.
• Broad-spectrum antibiotics: these decrease the number of organisms competing for resources in the vagina. Some antibiotics such as tetracycline impair host immune response by altering phagocytosis.
• Corticosteroid: this acts by attenuating the immune system and down regulating the inflammatory response.
• Tight under clothing: these create a warm, damp and moist environment in the vulva and vaginal area, which encourages the growth and multiplication of Candida.
• Other risk factors: obesity and intrauterine device. Clinical features
• Vulval and vaginal itching, soreness and irritation are the commonest symptoms associated with female genital candidiasis. This may be associated with the characteristic thick, curdy white, and adherent discharge. In severe cases there may be erythematous rashes involving the inner thighs and most active at the periphery. The vulva may be oedematous, and dysuria and dyspareunia may be present. There is usually no associated malodour unless there is comorbidity with bacterial vaginosis or trichomoniasis.
• About 2–3 in 1000 women may have recurrent vulvovaginal candidiasis, defined as ≥4 attacks in a year. These women need specialist care to identify and address the underlying predisposing and precipitating factors. Diagnosis
• Typical thick, cheesy, and adherent discharge
• Wet mount or gram stain looking for mycelia/hyphae or spores. If candidal spores only are present in a symptomatic woman consider C. glabrata
• Culture in Sabouraud’s cornmeal media, to identify candidal species and to obtain sensitivity studies. Non-albicans candidal species are implicated in cases of recurrent vulvovaginal candidiasis and they are commonly resistant to over the counter azole agents. Treatment
• Sporadic and single episode of vulvovaginal candidiasis may be treated with a single stat dose of intravaginal clotrimazole 500 mg + cream 1–2% applied topical for symptom relief.
• Women with recurrent vulvovaginal candidiasis should be discouraged from the use of scented soaps or similar products in the genital area, wearing tight fitting underclothing, nylon tights, and excessive consumption of sweets and refined sugars.
• In addition to eliminating the predisposing and precipitating factors, women with recurrent attacks may benefit from a 6-month course of weekly Fluconazole 100 mg. At the end of the course approximately 25% of women may relapse within 6 months. The course may be repeated. Resistant cases may respond to boric acid.
• Screen sexual partners for drugs such as penicillin to which the woman may be allergic, and which may be deposited in the vagina with the seminal plasma thus provoking an allergic reaction. Further reading
Sobel JD. Vulvovaginal candidosis. Lancet 2007;369:1961–71.
Witkin SS, Linhares I, Giraldo P, et al. Individual immunity and susceptibility to female genital tract infection. Am J Obstet Gynecol 2000;183:252–6.
Witkin SS. Immunology of recurrent vaginitis. Am J Reprod Immunol Microbiol 1987;15:347.