Conjoined Twinning
Diagnosis and Management
Alice King and Michael A. Belfort
The Facts
Conjoined twins are a rare anomaly where identical twins are born physically connected. The incidence is reported to be 1 in 50,000-200,000 births, and conjoined twins occur in approximately 1% of monozygotic twins.1 There is a significant prevalence of female gender (75% or greater).
The inheritance is sporadic and there is no increased incidence of conjoined twinning in subsequent pregnancies.Although the exact survival rate is unknown, there is a very high perinatal mortality rate. Approximately 40-60% of prenatally diagnosed conjoined twins undergo in utero fetal demise. Following delivery, a persistently high mortality rate continues with 30% dying within the first 24 hours of life. The risk of death of one or both of the twins is dependent on their anatomy and physiology.2
The embryology of conjoined twins is thought to be a result of abnormal monozygotic twinning with two prevailing theories: an abnormality in either fission or fusion. Normal monozygotic twins are the result of fission, in which a single fertilised ovum splits into two identical diploid cells that develop into two identical embryos. Depending on the stage at which the split occurs, the extent of shared amnion and chorion between the fetuses varies. When the split occurs later (days 14-18) at the primitive streak stage, one embryonic axis splits into two parallel axes and this is thought to greatly increase the risk of forming conjoined twins, with abnormal or incomplete division of the single axis into two. An alternate (although largely discarded) theory proposes that there is complete division with subsequent rejoining at vulnerable locations through fusion of the axes. Conjoined twins tend to be joined at a few specific anatomic locations. This fusion theory helps to better explain atypical conjoined twinning, such as chimeric, asymmetrically conjoined and fetus-in-fetu.
This chapter focuses on symmetric twins.Conjoined twins are joined in ventral, lateral or dorsal unions at homologous anatomic locations (i.e. chest to chest and pelvis to pelvis).3 They are most commonly classified according to the site of anatomic attachment followed by the suffix -pagus, derived from the Greek term for fixed. This standardised anatomic classification was championed by Spencer in 1996 in order to improve consistency in the nomenclature and in reports in the literature.4
Ventral Unions
Cephalopagus
Cephalopagus twins fused from the top of the head to the umbilicus represent 11% of conjoined twins. There may be a common cranium with either one composite face or two faces on opposite sides of the conjoined head. The thorax and upper abdomen show fusion of liver, heart and the upper gastrointestinal system down to Meckel's diverticulum. The lower abdomen and pelvis are not involved and each twin will have two arms and two legs. These twins tend to be non-viable.
Thoracopagus
Thoracopagus twins represent 20-40% of conjoined twins and are joined from the chest to the umbilicus. There is always involvement of the heart; however, the degree of involvement varies from a single shared organ to the presence of a single interatrial vessel. Liver parenchyma is always fused in thoracopagus twins, but the biliary system is shared in only 25% and the upper digestive tract in 50%. The pelvis is not typically involved and each twin will have two arms and two legs.
Omphalopagus
Omphalopagus twins occur in 18-33% of conjoined twins and are similar to thoracopagus twins with union primarily around the umbilicus with possible extension superiorly to the lower thorax. However, there is never involvement of the heart. The liver parenchyma is shared in 80% of omphalopagus twins. They typically have separate upper digestive tracts, although approximately one-third will share terminal ileum and proximal colon. Each twin typically has a separate pelvis with two arms and two legs.
Ischiopagus
Ischiopagus twins occur at a reported incidence of 6-11% and involve joining from the umbilicus to the pelvis. There is typically a single, large, conjoined pelvis with two sacra and one or two symphysis pubi. There is always involvement of the external genitalia and anus. These twins are mostly commonly joined end to end, but may also be joined face to face. Each twin always has two arms and two legs.
Lateral Union
Parapagus
Parapagus twins represent 28% of conjoined twins and are primarily joined ventral- laterally from the umbilicus, lower abdomen and pelvis. These twins always share a conjoined pelvis with one symphysis pubis. They may have one or two sacra, depending on the extent of ventrolateral rotation. The degree of fusion may extend superiorly and involve the thorax. The variable degree of union leads to a wide range in phenotype, from two separate thoraces with more inferior fusion of the abdomen and pelvis (dithoracic), to a single trunk with two separate heads (dicephalic), to a shared trunk and head with two faces (diprosopic). In diprosopic paragus twins, the faces typically present on the same side of the head. Parapagus twins may have two, three or four arms and two or three legs.
Dorsal Union
Craniopagus
Craniopagus twins are rare and represent 2% of conjoined twins. They are characterised by the union of any portion of the skull except the face and foramen magnum. Each twin always has two arms and two legs. These twins may share cranium, meninges and brain. Additional classification systems have been developed to further characterise these twins in an effort to give a more comprehensive description of their union. These classifications are based on different variables, including the deepest structure shared (Winston classification), the angle between the shared dural venous sinus and longitudinal axes (Stone and Goodrich classification) or the size of union and extracranial versus intracranial involvement (O'Connell classification).
Ultimately, multiple subclassifications are often used together to fully describe these twins, leading to difficulty in obtaining a clear understanding of the literature.Pygopagus
Pygopagus twins have been reported to represent 18-28% of conjoined twins. They are joined along the back with involvement of the sacrococcygeal and perineal regions. There is typically a single anus with two rectums. A variable amount of spinal cord may be shared between the twins. Each twin has two arms and two legs.
Rachipagus
Rachipagus twins are very rare with fusion along the back above the sacrum. There may be involvement of the occiput and/or the vertebral column.
The Issues
Prenatal Imaging
Early and accurate prenatal diagnosis of conjoined twins is important in order to facilitate clinical care and provide thorough prenatal counselling. Prenatal diagnosis of conjoined twins was initially described in 1976. With the advent of high-resolution transvaginal ultrasound, the diagnosis has been made at an increasingly early gestational age. The majority of conjoined twins are diagnosed around 11-14 weeks of gestation at the time of first-trimester screening. However, initial diagnosis may be suspected as early as 7-8 weeks of gestation. At an earlier gestational age, there is a higher risk of false-positive diagnosis due to less fetal movement of the twins, which may result in overlapping body parts. Fetal movement slowly increases after 8 weeks of gestation and may demonstrate distinctly separate twins to rule out conjoining. Therefore, if conjoined twins are suspected at a very early stage of pregnancy, a repeat ultrasound is highly recommended prior to final decision-making in order to confirm the diagnosis, as well as to better delineate the anatomy of the suspected conjoined twins.6
Early sonography will demonstrate one yolk sac alongside two embryos consistent with monoamniotic-monochorionic twins. Sonographic findings suspicious for conjoined twinning will usually show fixed fetal position with the lack of a separating membrane between the twins and the inability to separate the fetal bodies when following skin contours.7 In most cases, further evaluation will demonstrate fixed relative positions of the fetal heads with possible scoliosis and neck hyperextension, as well as atypical limb positioning.
Oftentimes, the umbilical cord will present with more than three vessels. Care should be taken when assessing suspected conjoined twins since in cases where there is a small zone of fusion the twins may rotate through as much as 180 degrees, giving an impression of vertex and breech presentations which can be confusing. Another potential error occurs when there are such high degrees of fusion that the twins are difficult to distinguish and a singleton is diagnosed. Close serial follow-up is required throughout pregnancy to monitor for polyhydramnios as well as hydrops.A referral to a dedicated fetal centre with experience in diagnosis and management of conjoined twins is recommended for further evaluation when conjoined twins is suspected. Special attention should be focused on the fusion site to delineate the vascular connections in the liver and heart with colour Doppler to diagnose common arterial and intra-cardiac connections.
On initial evaluation, the twins are assigned designations, such as twin A and twin B. This naming convention is maintained throughout later imaging studies and permits more clear and succinct communication. Typically, evaluation begins with two-dimensional ultrasonography which allows for categorisation of the type of union, such as ventral, dorsal or lateral. All limbs should also be identified and labelled. As noted earlier, Doppler techniques are applied to help evaluate shared vasculature. Additional adjuncts include transvaginal scans as needed, as well as the use of a high-resolution linear probe for increased detail. During each ultrasound evaluation, it is also important to assess the uterine environment, including placental location, umbilical cord position and the number of vessels within the umbilical cord, as well as an estimate of the amniotic fluid volume and the status of the cervix.
Fetal magnetic resonance imaging (MRI) is used alongside sonography for more detailed evaluation of shared anatomy. Different sequences are obtained in order to best visualise different aspects of the twins' anatomy.
T2-weighted single-shot fast spin echo (SSFSE) can be very helpful in visualising vasculature, while T1-weighted gradient echo (GRE) can help delineate bowel where meconium will typically appear T1-hyperintense. Additional sequences which may be helpful include echoplanar imaging (EPI) for bone and cartilage, as well as diffusion-weighted imaging (DWI) for brain and kidneys. A second-trimester MRI can be very helpful, as most major anomalies may be detected prenatally to help guide counselling and postnatal care.Fetal echocardiography is an essential component of prenatal evaluation. Cardiac involvement has a profound effect on outcomes. Prenatal echocardiogram has been suggested to be superior to postnatal scans, as the amniotic fluid can act as a buffer for the scans. Postnatally, echocardiography may be limited depending on where the twins are physically connected. There may be very limited pericardial windows, particularly for thoracopagus twins. Some series have compared the severity of disease predicted by prenatal echocardiography to autopsy results and have suggested that prenatal echo tends to underestimate the severity of disease. The clinical implications of these findings suggest that prenatal prediction of poor outcomes and mortality in conjoined twins are often very accurate.7
After initial evaluation and confirmation of the diagnosis of conjoined twins, if appropriate, termination of the pregnancy should be discussed and offered. In the event of termination being chosen, a destructive procedure may be required, and this frequently requires special expertise to safely accomplish. If possible, it is in the best interests of the mother to have a vaginal delivery and to avoid a hysterotomy.
In ongoing pregnancies, it is important to continue to follow closely throughout the remainder of gestation. During serial ultrasounds, each twin should be assessed individually, as conjoined twins may show differing growth rates and body compositions. Conjoined twins have been shown to have discrepant sizes, with the hypothesis that the smaller twin is supplying nutrients to the larger twin. Additionally, other complications including polyhydramnios (up to 75% of cases) or hydrops may be detected and warrant intervention such as amnioreduction or delivery if the viability of one or both twins may be affected.
The most common complication of monoamniotic twin pregnancy - that is, cord strangulation due to entanglement - is less likely to occur in conjoined twins because of the fixed positions of the babies. Close monitoring is still indicated because of the polyhydramnios and the potential for the extremities to become entangled in the cords.
Intra-partum Management
Timing of the delivery is important and a scheduled caesarean section is the preferred method for viable babies. Given the amount of pre-delivery organisation required to set up for delivery and initial resuscitation of the babies, it is not advisable to allow the patient to labour. A scheduled caesarean section with the entire team fresh and ready provides the optimum environment for the best outcome. Gestational age at delivery is dependent on prior obstetric history, current pregnancy circumstances and available resources. This should be individualised. There is no need for deliberate very preterm delivery unless obstetrically indicated since the larger the babies are at birth, the better they will do. Given that the majority of conjoined twin pregnancies have polyhydramnios there is a risk of preterm contractions, preterm premature rupture of the membranes (PPROM) and preterm delivery. Because of the abnormal shape of the uterine contents, PPROM is associated with a very real risk of umbilical cord prolapse, and careful consideration should be employed when considering prolongation of the pregnancy.
At the time of caesarean section care, we recommend a midline abdominal incision which allows for extension if required. Care should also be taken with the uterine incision because of the large fetal mass and potential difficulty in getting this mass delivered (especially when the babies are conjoined in such a way as to prevent easy manipulation and flexion). A bulky and inflexible fetal mass with multiple intertwined extremities can be very confusing and pre-hysterotomy ultrasound examination is advised to establish the lie and presentation of the twins in order to plan their orderly exit from the uterus. Given the extensive manipulation frequently required to effect the delivery there is an increased risk of inadvertently extending the hysterotomy into the uterine arteries with subsequent massive blood loss. We generally advise a lower-segment vertical hysterotomy (DeLee incision) which can be extended into the upper segment (classical hysterotomy) if required to give additional space. Attention should be given to managing uterine atony aggressively (and pre-emptively), and this should be anticipated given the frequently attendant polyhydramnios and overextended uterine cavity. An experienced anaesthesiology and surgical team familiar with the various medical and surgical approaches to reversing and controlling uterine atony and haemorrhage should be present. Adequate blood supplies and attention to blood loss, with early packed red cell transfusion and blood product replacement, cannot be overstressed. There is a very real risk of postpartum haemorrhage.
Postnatal Imaging
Following delivery, postnatal imaging is needed in the process of neonatal resuscitation and stabilisation, as well as to evaluate the anatomy to plan for further care and possible surgical separation.
Plain radiographs are needed to help confirm placement of endotracheal tubes, venous and arterial lines, as well as to evaluate the hearts and lungs. X-rays are also used to help assess bowel gas patterns. Depending on the twins' anatomic configuration, strategies to obtain and interpret radiographs are needed. Ventral union conjoined twins will need to be placed on their side, resulting in lateral views, while lateral union conjoined twins are usually positioned on their backs, resulting in anterior-posterior views.
Perinatal ultrasonography is very helpful in the evaluation of conjoined twins. This modality can be performed at the bedside and is used to evaluate a broad array of systems from cranial structures to abdominal solid organs. It is particularly helpful for vascular structures. For example, in cases of shared liver parenchyma, the hepatic vasculature will be evaluated with greyscale, colour Doppler and pulse-wave techniques. For vessels that bridge shared portions of the liver, waveforms can be examined for possible sharing. Additionally, vessels can be accurately traced back to each twin to delineate areas of involvement.
Fluoroscopy is used to help distinguish shared gastrointestinal and genitourinary tracts in conjoined twins. If prenatal imaging is suggestive of urinary tract anomalies, a voiding cystoureterogram (VCUG) should be performed postnatally. In addition to obtaining a roadmap or an outline of the shared anatomy, it will also help assess any vesicoureteral reflex. In cases of ambiguous external genitalia, a combination of retrograde fluoroscopic studies to delineate anatomy is helpful. Along with VCUG, fistula or anomalous communications and connections can be evaluated with the help of a contrast enema or genitogram. These are usually obtained via retrograde injection into the rectum or vagina respectively and may be performed with or without sedation. Often, a cystoscopy may be performed to augment the evaluation of the genitourinary system and to check for abnormal connections between the bladder, vagina and gastrointestinal system.
Further evaluation with cross-sectional computed tomography (CT) or MRI may be obtained to better understand the unique anatomy of each set of conjoined twins. Both CT and MRI are typically performed under anaesthesia in order to eliminate motion-related artifacts which can significantly degrade image quality. With the use of an angiography protocol, both CT angiography and MR angiography can help provide understanding of the sharing of organs and vessels. CT angiography (CTA) is superior to MR angiography for spatial resolution and has faster imaging acquisition, which helps obviate the need for breath-holding. The major disadvantage of CTA over magnetic resonance is the exposure to excess ionising radiation, an issue which is compounded if multiple CTAs are needed.
Due to the complexity of conjoined twin anatomy and the large degree of crosscirculation noted between many conjoined twins, multidisciplinary discussions to develop optimal radiographic strategies for contrast imaging are needed to formulate the best plan for each case. Computerised tomogram angiography has largely replaced the use of traditional angiography. In order to gain a complete understanding of their anatomy, separate scans with contrast injected into each baby may be needed. Selecting different gating will help optimise the visualisation of different systems. Computerised tomogram angiography of the thorax with electrocardiographic (ECG) gating can effectively delineate cardiac anatomy, even if the heart rates vary between the twins. This imaging is critical for surgical planning and may identify fused or shared chambers, which may render successful separation impossible. Computerised tomogram angiography of the chest will also exclude other vascular anomalies which may need surgical correction, including ventricular septal defects, aortic coarctation and anomalous pulmonary venous connections. Aortic branching, pulmonary artery anatomy and patency of the ductus arteriosus may also be assessed. Shared abdominal organs and vasculature may be evaluated with a CT of the abdomen during the early aortic phase of the injected twin. Visceral organs evaluated well by CT include the spleen, pancreas, kidneys, adrenal glands and the biliary system. Early aortic phase CT scanning can help demarcate a plane of separation between the two twins in the liver. Further evaluation of delayed equilibrium can give further information on the portal and hepatic vessels, helping to assess the size and number of vessels shared between the twins. A CT angiogram of the abdomen will show visceral arteries shared between the twins that may prevent successful separation. In addition to intravenous contrast, oral contrast is used to evaluate the gastrointestinal tract. Oral contrast is typically only administered to one twin in order to discriminate shared bowel. CT scans can also provide excellent detail of bony structures to help plan for separation of axial and appendicular skeletons. CT angiography data can be translated into more and more sophisticated three-dimensional (3-D) models, which are immensely helpful for surgical guidance and planning. These models are generated from digital 3-D imaging and printed 3-D models from cross-sectional imaging. They have been used in preoperative simulation planning at multiple specialised fetal centres and can demonstrate anatomic details not immediately apparent in two-dimensional imaging.
Magnetic resonance imaging (MRI) remains superior in some respects to CT and may provide helpful information for management. The biliary system is particularly amenable to interrogation with magnetic resonance technology. Classically, hepatobiliary scintigraphy with an iminodiacetic acid (HIDA) scan including radioactive technetium-99 m has been used to visualise the gallbladders and bile ducts in conjoined twins. This evaluation of suspected shared biliary anatomy has largely been replaced with MRI through magnetic resonance cholangiopancreatography (MRCP). If two gallbladders are visualised, the twins are highly unlikely to have an extra-hepatic bile duct communication. Magnetic resonance also allows evaluation for a single common pancreas, which is most commonly identified in thoracopagus and omphalopagus conjoined twins and which, if present, adds complexity to surgical planning. MRI can also help elucidate the genitourinary system, including the number, location and extent of fusion of the kidneys, as well as identify internal genitalia and anomalous ureteral insertions.
One of the most critical organs for prognosis and patient management is the heart. A thorough cardiac examination is recommended for every set of conjoined twins, even those who typically do not present with cardiac anomalies, such as ischiopagus or craniopagus twins. A combination of postnatal electrocardiography (EKG) and echocardiography can be used to initially evaluate the extent of organ sharing, orientation and sites of fusion. If necessary, cardiac MRI can be employed. The presence of a single heartbeat on EKG indicates extensive cardiac fusion, where separation is most likely not possible.8 Conversely, the presence of two heartbeats on EKG does not necessarily portend a better outcome or guarantee separation. Postnatal echocardiography is usually attempted in all cases, but frequently the anatomy precludes optimal pericardial views due to anatomy preventing appropriate probe placement. Therefore, if initial screening suggests cardiac fusion between the twins, a multi-detector computed tomography angiogram (CTA) and 3-D magnetic resonance angiogram (MRA) are typically obtained to track vessels, evaluate the anastomoses and assess the individual blood supply of each twin. Some centres have described different methods to determine the degree of circulatory exchange, including injection of radioactive albumin, or use of methylene blue or indigo carmine dyes.
Most commonly a combination of these radiographic modalities is used to help identify the anatomic issues associated with each type of conjoined twins. The presence of other anomalies can affect survival and should be taken into consideration, even if the anatomy of the conjoined twins suggests that separation is technically feasible. Such associated anomalies include scoliosis, congenital diaphragmatic hernia, cystic hygroma, myelomeningocele and club foot deformity. Additional gastrointestinal anomalies such as oesophageal atresia and imperforate anus have also been described. Interestingly, chromosomal abnormalities are rare in conjoined twins.
The Management Options
Women with prenatally suspected conjoined twins should be referred to a specialised fetal centre with experience in confirming and managing such patients. Prenatal counselling should be initiated in order to help with informed decision-making. Important topics that should be discussed include possible termination of pregnancy, the need for prenatal intervention, delivery considerations and postnatal work up and interventions.
If a family chooses termination of the pregnancy, it is important to take into consideration the fixed orientation of conjoined twins, which can make transvaginal termination especially difficult after 18-20 weeks of gestational age. Expertise in dilatation and curettage and fetal destructive procedures is key to avoid serious maternal injury. Second-trimester pregnancy termination via a hysterotomy may be the safest option to terminate the pregnancy.5
Approximately 600 sets of conjoined twins are born and undergo surgery every year.1 These twins require close monitoring throughout their pregnancy. The presence of polyhydramnios is reported in as many as 50% of conjoined twins, and in many cases, multiple amnioreductions have been required to mitigate the attendant risks of preterm labour and rupture of membranes. The presence of hydrops may prompt early delivery for fetal indication if one or both twins are deemed viable. Because of the large placenta and fetal mass these pregnancies are at increased risk of preeclampsia and mirror syndrome, both of which may prompt delivery at any time after 20 weeks.
Postnatal management for conjoined twins can be categorised into three main categories as determined by specific anatomy. These are: (i) non-operative management, (ii) emergency separation, or (iii) planned elective separation.
Separation is typically not offered if there is significant risk to one or both twins, or if the anticipated resultant deformities following separation are regarded as too severe. Thoracopagus conjoined twins with complex cardiac fusion are typically managed with non-operative management. However, if the cardiac fusion is relatively simple, such as the presence of a single inter-atrial vessel, postnatal separation may be an option. As with major cardiac sharing, craniopagus conjoined twins with extensive cerebral fusion may not be suitable for separation. Beyond the feasibility of separating cerebral vasculature and obtaining sufficient bony and soft tissue coverage, neurologic function is always a major consideration before considering separation of inter-digitating brain matter. In these cases, there may be significant compromise of the physical abilities of one or both twin if separation is pursued, and this should be fully discussed and appropriately weighed in the development of any management plans.9
Emergency separation may be necessary when the anatomy of either twin is threatening the survival of the other and immediate separation presents the opportunity to save the life of one or both twins. The need for emergency separation carries significant risk with a mortality rate of 71%. This drastically contrasts with the 80% reported overall survival rate of twins undergoing planned scheduled separation. The poorer outcomes associated with immediate separation are likely a result of multiple factors, including the increased risks associated with emergency induction of general anaesthesia and the inability to fully evaluate the anatomy. Emergency separation may also preclude the use of staged separation with the added disadvantage of being unable to place tissue expanders to ensure adequate wound coverage.
Emergency separation may be inevitable and required based on prenatal findings that suggest that such separation may be lifesaving for one or both twins. Cardiac unions may result in one twin not receiving sufficient circulation with anticipated death soon after delivery. One such example might be the presence of two very different heart rates on fetal echocardiography, associated with dilated cardiac chambers in one twin, indicating a situation of significant cardiac dysfunction in one baby with the other twin supporting both itself and its twin. Following delivery, the pump baby, is likely to rapidly go into cardiac failure, and in so doing significantly increase the mortality of both. This scenario warrants consideration of the separation of the twins as soon as possible. Ex utero intra-partum treatment (EXIT) has been performed successfully in this clinical setting to facilitate separation whilst on maternal-placental circulation.7
Each set of twins is a unique anatomic challenge, and significant and individualised planning is needed to facilitate a safe and successful surgical separation. The best outcomes are obtained when surgical resection is staged. Another guiding principle is the combination of prenatal and postnatal diagnostic testing such that the relevant anatomy is fully understood.10 Oftentimes, the most critical organ for the prognosis of the separation is the heart. The most commonly shared system is the gastrointestinal system, which is shared in most types of conjoined twins with the exception of craniopagus twins.
Once the affected physiologic systems are identified, the relevant subspecialists who will address these systems should be involved in early planning. Scheduled, formal, multidisciplinary meetings to discuss the separation prior to the actual operation will help to identify the critical steps of the operation and to develop contingency plans under different scenarios.
Role of Surgical Simulation
The use of surgical simulation in these high-complexity, rare cases is invaluable. It allows for care to be tailored to the specific case and helps to identify specific critical steps peculiar to that individual case. Simulation has been applied to every phase of care, including delivery, neonatal resuscitation and the various stages of separation. Simulation sessions may be facilitated with different types of aids, including 3-D-printed models or high-fidelity mannequins with custom modifications, but should be accurate in terms of anticipated gestational age, size and weight of the specific patients. This hands-on simulation helps to familiarise the team with the spatial orientation, airway management
Table 10.1 Conjoined twins anatomic classification
| Type | Per cent(%) | Area of Fusion |
| Ventral Unions | ||
| Cephalopagus | 11 | Head to umbilicus |
| Thoracopagus | 20-40 | Chest to umbilicus, always involved the heart |
| Omphalopagus | 18-33 | Lower chest to umbilicus, never involves the heart |
| Lateral Unions | ||
| Ischiopagus | 6-11 | Umbilicus to pelvis, genitalia and anus are always involved |
| Parapagus | 28 | Umbilicus to lower abdomen/pelvis, highly variable and may extend to thorax |
| Dorsal Unions | ||
| Craniopagus | 2 | Any portion of the skull, except face and foramen magnum |
| Pyopagus | 18-28 | Along the back with involvement of sacrococcygeal and perineal areas |
| Rachipagus | rare | Along the back above the sacrum |
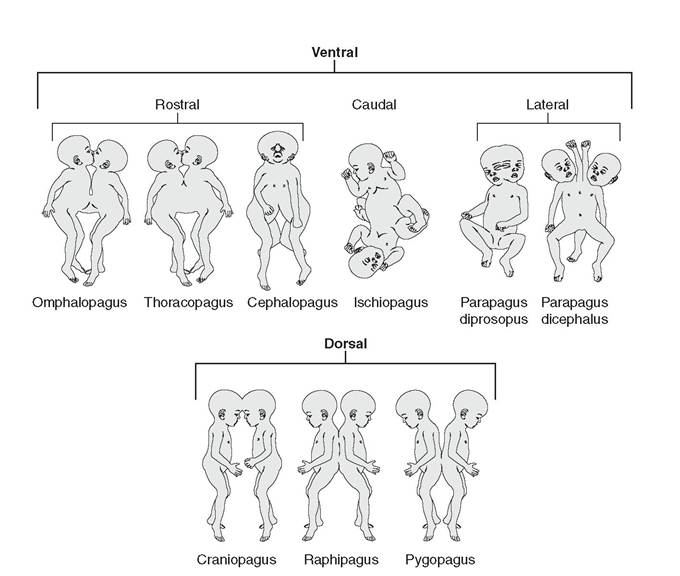
Figure 10.1 Schematic of different types of conjoined twins showing (A) thoracopagus, (B) omphalopagus, (C) pygopagus, (D) ishiopagus, (E) craniopagus, (F) parapagus, (G) cephalopagus and (H) rachipagus
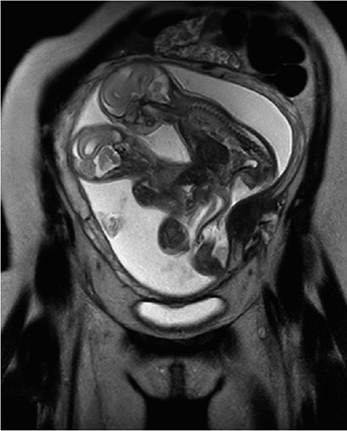
Figure 10.2 Fetalmagnetic resonance imaging of omphalopagus conjoined twins at 21 weeks of gestationalage showing fused liver
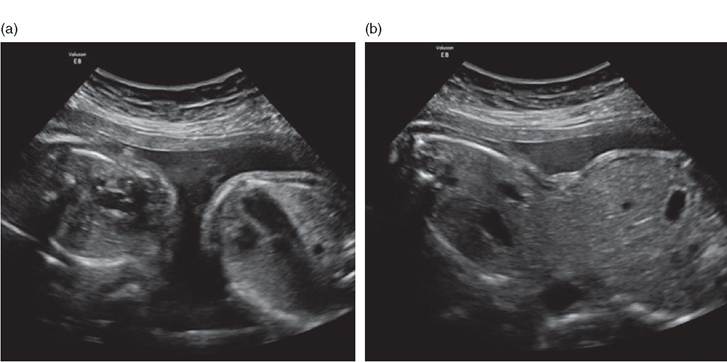
Figure 10.3 Fetalultrasound imaging of omphalopagus conjoined twins at 21 weeks of gestationalage showing separate heart and thorax (a) and fused liver parenchyma (b)
and vascular access needed in the delivery room.11 For example, endotracheal intubation may present a significant technical challenge in the case of thoracopagus twins and warrant the availability of additional equipment, such as fibre-optic laryngoscopes in the delivery room.12
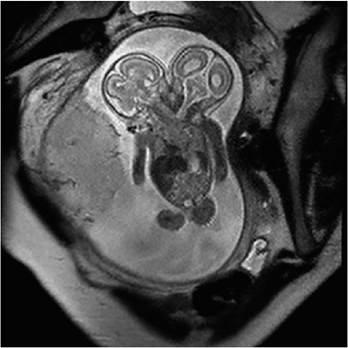
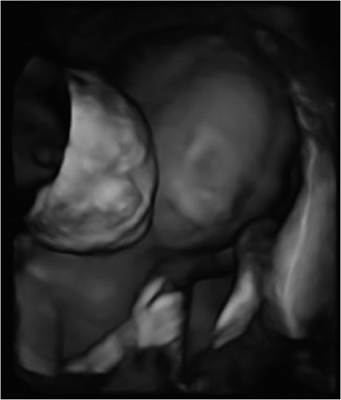
Figure 10.4 Fetalmagnetic resonance imaging of dicephalic parapagus conjoined twins at 19 weeks of gestationalage showing two fetalheads and a common thorax and abdomen
Figure 10.5 Three-dimensionalultrasound of dicephalic parapagus conjoined twins at 19 weeks of gestationalage. (A black and white version of this figure willappear in some formats. Forthe colour version, please refer to the plate section.)
Key Points
• Conjoined twins are a rare anomaly with high in utero and perinatal mortality.
• The use of a standardised anatomic classification helps to improve consistency in diagnosis and facilitates communication between providers.
• Referral to a fetal centre with experience in the evaluation and management of conjoined twins is recommended to optimise counselling and care for these complex patients.
• Extensive prenatal and postnatal diagnostic imaging with advanced radiographic techniques help to delineate the affected anatomy.
• Postnatally, twins may be managed non-operatively, with emergency separation or with planned scheduled (staged or not) surgical separation.
• Involvement of the cardiovascular and neurovascular systems has the greatest impact on successful surgical separation and survival.

Figure 10.6 Fetalultrasound of
Craniopagusconjoined twins at 18 weeks of gestationalage showing shared cranium
References
1. Mian A, Gabra NI, Sharma T, Topale N, Gielecki J, Tubbs RS et al. Conjoined twins: from conception to separation, a review. Clin Anat NYN 2017;30(3):385-96.
2. O'Brien P, Nugent M, Khalil A. Prenatal diagnosis and obstetric management. Semin Pediatr Surg 2015 Oct;24(5):203-6.
3. Pierro A, Kiely EM, Spitz L. Classification and clinical evaluation. Semin Pediatr Surg 2015 Oct;24(5):207-11.
4. Spencer R. Anatomic description of conjoined twins: a plea for standardized terminology. J Pediatr Surg 1996 Jul;31 (7):941-4.
5. Pajkrt E, Jauniaux E. First-trimester diagnosis of conjoined twins. Prenat Diagn 2005 Sep;25(9):820-6.
6. Mehollin-Ray AR. Prenatal and postnatal radiologic evaluation of conjoined twins. Semin Perinatol 2018;42(6):369-80.
7. Mackenzie TC, Crombleholme TM, Johnson MP, Schnaufer L, Flake AW, Hedrick HL et al. The natural history of prenatally diagnosed conjoined twins. J Pediatr Surg 2002 Mar;37(3):303-9.
8. Andrews RE, Yates RWM, Sullivan ID. The management of conjoined twins: cardiology assessment. Semin Pediatr Surg 2015 Oct;24(5):217-20.
9. Harvey DJ, Totonchi A, Gosain AK. Separation of craniopagus twins over the past 20 years: a systematic review of the variables that lead to successful separation. Plast Reconstr Surg 2016 Jul;138(1):190-200.
10. Fallon SC, Olutoye OO. The surgical principles of conjoined twin separation. Semin Perinatol 2018;42(6):386-92.
11. Yamada NK, Fuerch JH, Halamek LP. Modification of the Neonatal Resuscitation Program Algorithm for Resuscitation of Conjoined Twins. Am J Perinatol 2016 Mar;33(4):420-4.
12. Parmekar S, McMullen L, Washington C, Arnold JL. Role of simulation in preparation for the care of conjoined twins: prenatal preparation to separation. Semin Perinatol 2018;42(6):329-39.