Management of Discordant Fetal Anomaly
Rajit Narayan and Jon Hyett
Introduction
Since the advent of assisted reproductive technologies, the prevalence of twins has increased and is currently 1.7% (1 in 60 pregnancies) in our local public hospital population.
Twin pregnancies may be complicated in a number of ways, including through presentation with fetal abnormality. Pregnancies that are discordant for fetal anomaly may be impacted by a range of complications that are dependent on zygosity, chorionicity and the specific anomaly concerned.Discordance is defined as ‘occurrence of a trait or disease in only one member of a matched pair of subjects, especially twins'. In this chapter, we review the prevalence of various fetal anomalies in twin pregnancies, identify means for detecting these prenatally and review a range of approaches to managing these anomalies considering the impact on the affected fetus, the co-twin and the wider family. Growth discordance does not fall within the scope of this chapter and is discussed elsewhere in this book.
Prevalence of Anomalies in Twin Pregnancies
A descriptive epidemiological review of European birth defect registries (data for 2004-7) reported that 3.6% of infants from multiple pregnancies were affected by a congenital anomaly.1 This compared to a prevalence of 2.7% in singleton births, a relative risk (RR) of 1.31 (95%CI: 1.24-1.38). Interestingly, whilst structural anomalies were more common in multiples (RR: 1.41; 95%CI 1.34-1.48), chromosomal anomalies had a lower prevalence (RR: 0.71; 95%CI 0.60-0.78).
The observation that structural anomalies are more commonly seen in twins is well established. Structural anomalies predominantly occur within monozygotic twin pairs and have been ascribed to malformations associated with splitting of the pluripotent cell mass and with vascular disruptions resulting from monochorionicity.1 Monozygotic twins have been estimated to have a threefold to fivefold increase in risk of anomalies compared to singleton fetuses.2 Eighty to ninety per cent of anomalies are reported to be discordant within a twin pair, which is surprising on face value given that most events are within monochorionic twins, but it is explained by these specific mechanistic pathways.1,2
The most common organ systems impacted by malformation are the central nervous and cardiovascular systems (Figure 11.1).2 Anomalies of ophthalmic and gastrointestinal systems are also more prevalent in twins than in singletons (Figure 11.2).
These systems appear to be more vulnerable to errors in midline fusion/processes of laterality or to disruptive processes (such as vascular accidents). In this chapter, we limit discussion to
Figure 11.1 Hypoplastic left heart syndrome demonstrated in an MCDA twin at 13 weeks of gestation. The lefthand image of the four-chamber view shows Univentricular filling and the right-hand image of the three-vesselview shows reversed flow in the ascending aorta. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)

Figure 11.2 Asmallexomphalos seen in this MCDA twin at 14 weeks of gestation. The inter-twin membrane can be seen inserting into the monochorionic placenta. (A black and white version of this figure willappear in some formats. Forthe colour version, please refer to the plate section.)
‘major’ structural anomalies, predicted either to be lethal or to require significant postnatal intervention with risks of significant morbidity and/or mortality in the affected individual.
Whilst the genetic basis for discordant anomalies is readily recognised in dizygotic twins, a number of interesting mechanisms have been described in monozygotic twins including heterokaryotypia secondary to early post-zygotic errors, single gene defects, mitochondrial and epigenetic disorders, blood or tissue chimerism, and skewed X chromosome inactivation.3
Prenatal Detection of Twins Discordant for Anomaly
Ultrasound, maternal serum biochemistry and more recently cell-free DNA testing provide means for prenatal screening for both chromosomal and structural anomalies. The European registry data suggest that rates of prenatal diagnosis are similar to those seen in singleton pregnancies, but this merits further discussion.1
The prevalence of common chromosomal abnormalities such as trisomy 21 appears to be lower in twin than in singleton pregnancies.4 Risk assessment is typically based on maternal age-related risks (derived in singleton populations).
Parental decisions regarding continuing pregnancies may depend on whether one or both fetuses are affected. In general, monozygotic twins have the same genetic constitution and if one twin is affected, the other twin will also be affected - the a priori risk is therefore the same for both twins and is based on maternal age. In dizygotic twins, the risk that one or the other twin is affected by trisomy is essentially double the maternal age-related risk and the risk that both twins are affected is the square of the maternal age-related risk.Ultrasound markers for trisomy 21 differ from maternal serum biochemistry and cell- free DNA as they are fetal specific rather than pregnancy specific. Risks can be adjusted accordingly, although zygosity is not determined (by ultrasound) and only monozygotic twins that are monochorionic can be adequately differentiated. All three methods of aneuploidy screening (second-trimester maternal serum biochemistry, first-trimester combined screening and cell-free DNA assessment) have lower efficacy in twin compared to singleton pregnancies. Some markers, such as fetal nuchal translucency (NT) thickness, may also be impacted by other pathologies - such as twin-twin transfusion - leading to inaccuracies in risk assessment.
A retrospective review of a series of > 1,000 twin pregnancies that had a first-trimester ultrasound assessment between 1996 and 2014 found that only 27% (95%CI: 15-43%) of structural anomalies were identified.5 Anomalies were more prevalent and more readily recognised in twin pairs with discordant crown-rump length (CRL) and NT measures, as well as within monochorionic twins. Central nervous system abnormalities and abdominal wall defects were most readily recognised. It should be noted that this series included twins screened between 1996 and 2014 - and that the approach to a structured anatomical survey during the 11-13+6 week scan changed markedly over this time.
Current international guidelines recommend two formal structural ultrasound assessments of the fetus at 11-13+6 and 18-22 weeks of gestation.
The time allocated for completion of the morphology scan should also be extended to allow for the fact that this assessment is technically more challenging. Careful assessment of the brain/neural tube, the heart, the midline structures of the face, and the anterior abdominal wall and the gastrointestinal tract should be completed given the increased prevalence of defects affecting these systems. In contrast to some other complications of twin pregnancies, chromosomal and structural anomalies can potentially be identified relatively early, providing parents with a wider range of options.Managing Twins Discordant for an Anomaly
Defining potential outcomes and ethical implications of various management options makes decision-making difficult in complicated twin pregnancies.6 Three parties have potentially different and competing interests: the affected fetus, whose prognosis is closely related to the severity of the anomaly; the normal co-twin, who may be impacted by complications affecting the abnormal twin or by iatrogenic preterm delivery; and the mother. Ideally, decision-making should be shared after discussion of all options and relevant risks/benefits, which typically need to be tailored to the individual situation.
Multidisciplinary input should be sought from neonatologists, paediatricians (and/or surgeons) and paediatric development physicians. Social work input should be arranged to facilitate self-exploration of moral, emotional, social, financial and/or religious values and considerations. While the mother should retain autonomy over her decision regarding management of her pregnancy, local legislative and ethical restrictions and indeed availability of clinical resources and expertise may all dictate suitability of management pathways. As a general rule, there tend to be three broad avenues of management for pregnancies affected by discordance in twins:
■ Expectant: the pregnancy continues in its current form.
■ Termination of the pregnancy.
■ Selective reduction of the anomalous twin.
A number of fundamental concepts may impact decisions about the most appropriate way forward. One of the most central of these is the issue of chorionicity. Whilst dichorionic twins are for the most part independent, monochorionic twins almost invariably have a common placental vasculature and as a consequence any detrimental impact on an anomalous twin may be reflected in the outcome of the normal co-twin. Similarly, the extent and type of an anomaly - and the prognosis for a surviving infant - will likely have a big impact on decisions for ongoing management. The gestation at which anomalies are identified will also be important as this may impact management options. Finally, there may also be issues related to maternal health and well-being as well as the potential impact of birth of a child with significant abnormalities on the whole family.
Dichorionic Twins
The architecture of dichorionic placentas allows for some leeway in management options for discordant anomaly. This simplifies decision-making, so we address this cohort of pregnancies first. Common forms of chromosomal abnormality (such as trisomies 21, 18 or 13) and some major structural anomalies (such as anencephaly) will most likely be identified at the 11-13+6 week scan. These anomalies provide an opportunity to look at some of the principles of management outlined earlier.
The majority (likely > 75%) of fetuses identified with trisomy 21 at 11-13+6 weeks of gestation will survive pregnancy, so parents who choose expectant management should anticipate they will have a live child affected by this condition. As the pregnancy advances, other structural anomalies (such as cardiac defects and/or duodenal atresia) may be recognised, but these are unlikely to impact the course of the pregnancy, which will likely continue to a similar gestation as an unaffected twin pregnancy. As some fetuses affected by trisomy 21 have no obvious phenotype in utero, and as a proportion of dichorionic twins will be monozygous, diagnostic testing should be offered for both fetuses.
An early diagnosis gives parents time to absorb information and to optimise management around and after delivery. Diagnostic testing needs to be performed with care, describing landmarks and phenotypes carefully, so that in the event selective reduction is considered this can be performed without risk to the normal co-twin.The trajectory for a fetus identified with trisomy 18 or 13 at 11-13+6 weeks is very different. These conditions have significantly higher rates of lethality and it could therefore be argued that expectant management will in itself most likely lead to fetal demise. It should, however, be remembered that there is no certainty that this will be the case and a small proportion of live-born infants will survive weeks/months and that palliation may be very difficult whilst also managing another newborn. Another complicating factor is that in an ongoing pregnancy, the anomalous twin may develop severe polyhydramnios and this may trigger preterm delivery. This in turn might injure the normal co-twin. The dilemma here is the balance of risk: if selective termination is considered, what is the risk that this will lead to miscarriage or early preterm delivery of the normal co-twin, and how does this equate with the risk that the anomalous fetus will develop polyhydramnios leading to preterm delivery?
The third scenario involves the finding of anencephaly affecting one dichorionic dia- mniotic twin at 11-13+6 weeks of gestation (Figure 11.3). In this circumstance, the condition is definitely lethal and management should be focused on achieving the best outcome for the co-twin. Approximately 50% of fetuses managed expectantly with anencephaly will develop polyhydramnios, and 15-20% of dichorionic-diamniotic pregnancies that include an anencephalic fetus will deliver < 34 weeks. In contrast, selective termination is associated with an approximate 10% risk of miscarriage and 10% risk of delivery < 34 weeks.7 Whilst it may not be immediately clear which option is least likely to cause harm, other series have suggested that risks of preterm birth with expectant management may be even higher - so intervention would be reasonable.8
Data describing outcomes in series of dichorionic twin pregnancies discordant for anomalies are conflicting. One study recently reported outcomes of a cohort of 56 dichor- ionic twin pregnancies discordant for anomaly compared to a series of 586 normal dichor- ionic twin pregnancies.9 They reported similar outcomes between the two groups (preterm labour: 21.4% vs 19.1%; preterm premature rupture of the membranes (PPRoM) < 37 weeks: 17.9% vs 19.3%; intrauterine growth restriction: 7.1% vs 9.4%; fetal demise in the structurally normal twin: 0% vs 0%; composite adverse neonatal outcome (19.6% vs 15.1%)). The authors concluded that expectant management was reasonable when parents chose that option.
In contrast, another study reporting a series of 25 anomalous cases and 547 controls found a significant increase in the rate of preterm delivery < 34 weeks of gestation (76% vs

Figure 11.3 Anencephaly identified in this dichorionic twin at 11 weeks of gestation. The inter-twin membrane appears thin - which is often reported to be typicalof monochorionic twins - but should not be used in isolation as a reliable sign for chorionicity.
55.4%; p = 0.042) and reported a lower mean gestation of delivery for the whole cohort (34 weeks vs 35.6 weeks; p = 0.019).10 As described earlier, the risk appeared to be most relevant in pregnancies involving an anomaly that could affect the swallowing mechanism of the affected twin, leading to polyhydramnios such as anencephaly, a large cleft palate, tracheoesophageal fistula, lethal skeletal dysplasia or major aneuploidies such as trisomies 13 and 18.
Several techniques for selective termination have been described. The most common approach involves ultrasound-guided percutaneous intra-cardiac injection of potassium chloride, which causes cardiac asystole. A group of eight centres with the largest known experience of selective termination worldwide published the outcome of 402 cases and found a 7% pregnancy loss rate (< 24 weeks) in twin pregnancies reduced to singletons and a further 6% preterm birth rate (< 28 weeks) with a trend towards lower pregnancy loss rates when the procedure was performed before 13 weeks of gestation.11 Risk of maternal morbidity associated with the procedure is low.
This procedure can be performed in an office/outpatient setting. The most important issue is to complete a structured review of the pregnancy and to clearly identify both the normal and the abnormal twin prior to commencing the procedure and to confirm these findings with a second, independent, experienced sonologist. Inadvertent reduction of the normal rather than the anomalous twin has been reported on a number of occasions.
Several contemporaneous studies have reported similar or lower loss rates for twin reduction and suggest that loss rates are not as dependent on gestation as was originally thought. Indeed, some authors promote delaying the procedure to a later gestation to remove the risk of miscarriage, although this comes with its own potential legal, ethical and psychosocial complications.
Monochorionic Twins
Many of the specific risks of a fetal anomaly will be similar for dichorionic and monochor- ionic twins. There are some significant differences in monochorionic pregnancies, though. From an aneuploidy perspective, although monochorionic twins are monozygotic and will in most circumstances have the same karyotype, there are a number of reports of hetero- karyotypia and if one fetus is anomalous and the other is apparently normal, double amniocentesis may be preferred to karyotype the pregnancy rather than chorionic villus sampling from the single placenta.12
A significant number of monochorionic twins will be impacted by twin-twin transfusion syndrome and/or selective intrauterine fetal growth restriction and there is a risk that the pregnancy may be impacted by two different pathologies. Similarly, almost all mono- chorionic pregnancies have vascular anastomoses and if a fetal anomaly is associated with an increased risk of intrauterine fetal death, this increases risk to the whole pregnancy.
Selectively reducing an anomalous twin within a monochorionic pair is technically more challenging as death of a monochorionic twin can result in secondary exsanguination of the co-twin, which has been shown to be associated with a significant risk of death (25%) or neurodevelopmental handicap (20%) in survivors.
Consequently, a procedure aiming to effect selective termination in a monochorionic twin pregnancy needs to occlude the circulation of this twin so that subsequently there can be no retrograde flow. A number of different approaches have been used for this, but three common therapies in contemporary use are bipolar cord occlusion, interstitial laser ablation and radiofrequency ablation. Each method has advantages and disadvantages.
Bipolar cord occlusion requires introduction of a single 3 mm ‘vascular catheter' port into the uterus.13 Port insertion was initially used for endoscopic laser ablation of twin-twin transfusion - in that circumstance, the port is introduced into a tense uterus with polyhydramnios. Care has to be taken when the myometrium is typically thicker and softer; port insertion is most safely achieved using a ‘Seldinger' technique and infusion of additional saline into the uterus to make room for the procedure.
Once the port is inserted, a bipolar forceps can be introduced into the uterus and, under ultrasound guidance, used to grasp the cord and apply diathermy to seal the umbilical arteries and vein. The process is normally repeated to ensure the circulation is occluded. Fetal bradycardia, cardiac asystole and death will follow over the course of several minutes.
The procedure has the advantage that it is straightforward and the equipment is cheap and readily available. Obstetricians/gynaecologists who have trained in both ultrasound and laparoscopic surgery have the skill set to complete the procedure under ultrasound guidance. The disadvantage to the procedure is that the port is relatively large (with risk of miscarriage and PPRoM) and the jaws of the instrument are limited to grasp the whole cord, making this technically challenging at more advanced gestations.
The energy for an interstitial laser is typically passed through a fine (400 um) optic fibre which can be inserted into an 18 G needle; this has the advantage of a small cross-sectional profile and can be advanced into the uterus more safely.14 The fibre is used to heat and coagulate interstitial vessels. One disadvantage of this technique is cost - it requires access to a NdYAG/diode laser with fibres that can be used with tissue contact.
Radiofrequency ablation also requires more costly equipment, but the probes also have a smaller cross-sectional profile than bipolar forceps (Figure 11.4) and the procedure can more readily be performed under local anaesthesia.15 We use a 17 G (1.4 mm diameter) Starburst SDE (Angiodynamics Inc., Queensbury, NY, USA) multi-tine electrode. Once the probe is inserted and the tines are advanced, a sinusoidal current is generated that agitates tissue ions, creating frictional heat and causing coagulation of the tissue. Energy levels and time of delivery are set (typically 40-60 W for 3-5 minutes to reach a target temperature of ~120°C). The probe provides temperature feedback that improves consistency of coagulation and theoretically reduces the risk of failing to occlude vessels within the ‘burn radius' - which is several centimetres for most probes. Multiple cycles may be required before the desired result is achieved. As a consequence, this technique can be used for more advanced pregnancies where bipolar cord occlusion is not possible. Ultrasound assessment is used to confirm fetal cardiac asystole in the anomalous twin prior to withdrawal of the needle.
The completeness of radiofrequency or interstitial laser procedures is difficult to quantify by use of colour Doppler flow estimates, unlike post-bipolar cord occlusion, where this is quite a simple exercise. Mid-cerebral artery Doppler waveforms and cardiac filling are assessed in the surviving twin to screen for fetal anaemia consequent to ongoing haemorrhage into the dead twin.
There is also a risk heat may damage neighbouring structures using the interstitial technique - one of the proposed mechanisms for preterm rupture of membranes after these procedures. Individual circumstances may also affect choice of procedure; the length of the radiofrequency electrode limits its use in women with higher body mass index, and
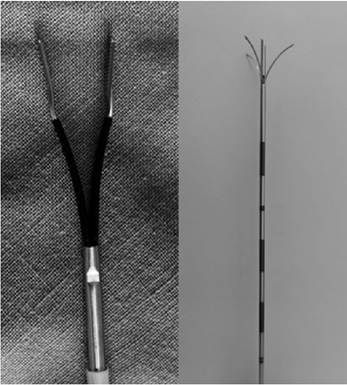
Figure 11.4 The tips of bipolar forceps (left panel) and the radiofrequency ablation (RFA) probe (right panel).
The bipolar instrument is a wider diameter (3.5 mm) and the tongs open to 12 mm diameter. The RFA probe is narrower (1.5 mm) and opens to deploy multiple tines to a diameter of 2-3 cm.
bipolar cord occlusion is technically more challenging with oligohydramnios or a short cord (as is frequently seen in acardiac twin pregnancies).
Success rates vary by publication, but broadly speaking, they appear to be comparable for the two procedure types. A systematic review comparing the techniques observed that bipolar cord occlusion was preferred to radiofrequency at later gestations (21.1 vs 18.8 weeks), was associated with fewer deaths of co-twins than radiofrequency ablation (10.6% vs 14.7%), and resulted in higher live birth rates (86.7% vs 81.3%), but tended to have earlier birth in survivors (34.7 vs 35.1 weeks of gestation) and a greater PPROM risk (28.2% vs 17.7%).16 Although there are small differences between these procedures, management of a specific pregnancy is likely best defined at the discretion of the caring clinician and will be determined by the type of anomaly, gestation, geographic features of the pregnancy and maternal body habitus.
Exceptional Circumstances
Monoamniotic Twins
The majority of monochorionic twins are diamniotic, but in the circumstance of mono- amnionicity, there is an additional post-procedural risk of cord entanglement (Figure 11.5). Post procedure, as the cord of the dead twin becomes more fibrous and the weight of the fetus pulls it taut, it is likely to be less forgiving and this can easily lead to delayed unanticipated intrauterine death of the co-twin. Transection of the cord after ablation has been proposed and several methods have been described to achieve this, including use of a contact LASER or use of endoscopic shears or a harmonic scalpel (through a second 5 mm port). Valsky et al. reported a series of 17 monoamniotic twins who underwent selective reduction plus cord transection and compared their outcomes to a cohort of 72 monochor- ionic-diamniotic twins who also underwent selective termination.17 They observed a nonsignificant difference in PPROM risk (35.3% vs 20.8% before 32 weeks), preterm delivery under 32 weeks of gestation (41.2% vs 28.2%), fetal death in utero and neonatal morbidity
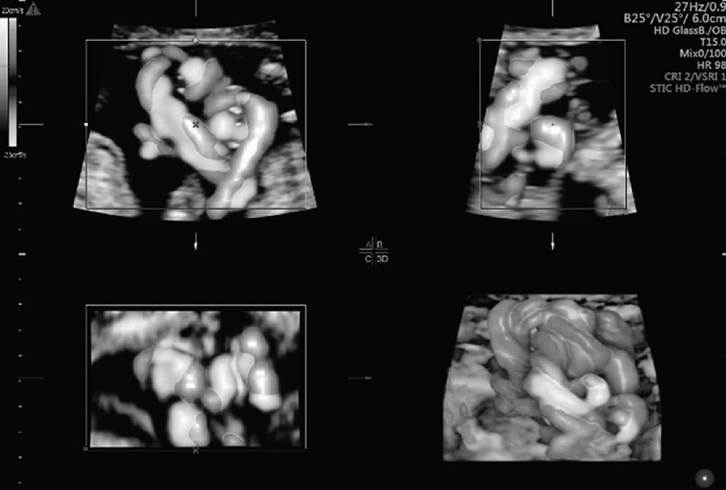
Figure 11.5 3-D multiplanar image showing cord entanglement in MCMA twins at 18 weeks of gestation (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
risk, and it is necessary to recognise that the study was likely underpowered for these outcomes. The median gestational age at delivery was 35 weeks in the monoamniotic cohort (that had cord transection) and 37+1 weeks in the diamniotic cohort.
Twin-Reversed Arterial Perfusion Sequence (TRAP)
Another anomaly unique to monochorionicity is twin-reversed arterial perfusion (TRAP), involving a normal ‘pump’ twin that also, through placental anastomoses, perfuses a parasitic tissue mass. The tissue mass represents a significantly malformed co-twin that, likely due to disrupted vascular perfusion, sustained significant errors in embryological development. Many of these masses are anencephalic as well as acardiac. Untreated, mortality in the pump twin may exceed 50% as this infant is prone to unanticipated intrauterine death during early pregnancy and later developing high-output cardiac failure and hydrops. There is also a significant risk of preterm delivery due to maternal mirror syndrome or following spontaneous onset of labour related to polyhydramnios. As first- trimester ultrasound has become more prevalent, TRAP is typically diagnosed at an early stage of pregnancy, and this provides a dilemma for management. An early intervention potentially reduces the risk of unanticipated loss of the pump twin, but intervention with substantive instrumentation (e.g. using radiofrequency ablation) has a higher risk of loss at an earlier gestation.18 A wide range of approaches for therapeutic intervention have been reported with varying rates of success over the past 20 years. In most cases, the cord of the acardiac twin is extremely short and this fetus is held close to the placenta, making access for bipolar cord occlusion difficult. At this point in time, the two most common approaches used for treatment involve interstitial laser (particularly popular amongst those that promote an early intervention) and radiofrequency ablation.19,20 Survival rates of the pump twin are estimated around 80%.
Higher-Order Multiples
Higher-order multiples are less common and there is little literature describing management of discordant anomalies in these pregnancies. The intervention will depend on the anomaly, gestation and pattern of chorionicity. As risks of preterm birth are inherently higher in higher-order multiples, the procedural risk and impact may be lower than that seen in twins. One systematic review, including a variety of indications for reduction, noted a reduction in preterm births from 33.3% in triplets managed conservatively to 5.5% when the pregnancy was reduced to a singleton, and 11.8-17.6% when reduced to twins.21
Key Points
• More than 3% of twin pregnancies will be discordant for fetal abnormality.
• Whilst anomaly rates are similar in dichorionic twins, they are three to five times more common in monochorionic twins.
• The central nervous, facial, cardiac and gastrointestinal systems are most prevalent.
• Accurate determination of chorionicity is central to management.
• Management decisions need to be made according to balance of benefits and harms and should be shared with the patient.
References
1. Boyle B, McConkey R, Garne E et al. Trends in the prevalence, risk and pregnancy outcome of multiple births with congenital anomaly: a registry-based study in 14 European countries 1984-2007. BJOG 2013;120:707-16.
2. Weber MA, Sebire NJ. Genetics and developmental pathology of twinning. Semin Fetal Neonatal Med 2010;15:313-18.
3. Silva S, Martins Y, Matias A, Blickstein I. Why are monozygotic twins different?
J. Perinat Med 2011;39:195-202.
4. Cuckle H, Benn P. Review of epidemiological factors (other than maternal age) that determine the prevalence of common autosomal trisomies. Prenat Diagn 2020; 41(5):536-44. Portico. https:// doi.org/10.1002/pd.5822
5. D'Antonio F, Familiari A, Thilaganathan B et al. Sensitivity of first-trimester ultrasound in the detection of congenital anomalies in twin pregnancies: population study and systematic review. Acta Obstet Gynecol Scand 2016 Dec;95(12):1359-67.
6. Phillips T, Moore B, Posma E, Gillam L, Cuzzilla R, Cole S. Ethical considerations in multiple pregnancy: preterm delivery in the setting of discordant fetal anomaly. Twin Res Hum Genet 2019;22:120-3.
7. Vandecruys H, Avgidou K, Surerus E, Flack N, Nicolaides KH. Dilemmas in the management of twins discordant for anencephaly diagnosed at 11+0 to 13+6 weeks of gestation. Ultrasound Obstet Gynecol 2006;28:653-8.
8. Lust A, De Catte L, Lewi L, Deprest J, Loquet P, Devlieger R. Monochorionic and dichorionic twin pregnancies discordant for fetal anencephaly: a systematic review of prenatal management options. Prenat Diagn 2008;28:275-9.
9. Algeri P, Russo FM, Incerti M et al. Expectant management in dichorionic pregnancies complicated by discordant anomalous twin. J. Perinat Med 2018;46:721-7.
10. Nassar AH, Adra AM, Gomez-Marin O, O’Sullivan MJ. Perinatal outcome of twin pregnancies with one structurally affected fetus: a case-controlled study. J Perinatol 2000;20:82-6.
11. Evans MI, Goldberg JD, Horenstein J et al. Selective termination for structural, chromosomal and Mendelian anomalies: international experience. AJOG 1999;181:893-7.
12. Egan E, Reidy K, O’Brien L, Erwin R, Umstad M. The outcome of twin pregnancies discordant for trisomy 21. Twin Res Hum Genet 2014 Feb;17(1):38-44.
13. Lanna MM, Rustico MA, Dell’Avanzo M et al. Bipolar cord coagulation for selective feticide in complicated monochorionic twin pregnancies: 118 consecutive cases at a single center. Ultrasound Obstet Gynecol 2012;39:407-13.
14. O’Donoghue K, Barigye O, Pasquini L, Chappell L, Wimalasundera RC, Fisk NM. Interstitial laser therapy for fetal reduction in monochorionic multiple pregnancy: loss rate and association with aplasia cutis congenita. Prenat Diagn 2008;28:535-43.
15. Paramasivam G, Wimalasundera R, Wiechec M, Zhang E, Saeed F, Kumar S. Radiofrequency ablation for selective reduction in complex monochorionic pregnancies. BJOG 2010;117:1294-8.
16. Gaerty K, Greer RM, Kumar S. Systematic review and meta-analysis of perinatal outcomes after radiofrequency ablation and bipolar cord occlusion in monochorionic pregnancies. Am J Obstet Gynecol 2015;213:637-43.
17. Valsky DV, Martinez-Serrano MJ, Sanz M et al. Cord occlusion followed by LASER cord transection in monochorionic monoamniotic discordant twins. Ultrasound Obstet Gynecol 2011;37:684-8.
18. Chaveeva P, Poon LC, Sotiriadis A, Kosinski P, Nicolaides KH. Optimal method and timing of intrauterine intervention in twin reversed arterial perfusion sequence: case study and meta-analysis. Eur J Obstet Gynecol Reprod Biol 2013;166:127-32.
19. Pagani G, D’Antonio F, Khalil A, Papageorghiou A, Bhide A, Thilaganathan B. Intrafetal laser treatment for twin reversed arterial perfusion sequence: cohort study and meta-analysis. Ultrasound Obstet Gynecol 2013;42:6-14.
20. Lee H, Bebbington M, Crombleholme TM. The North American Fetal Therapy Network registry data on outcomes of radiofrequency ablation for twin-reversed arterial perfusion sequence. Fetal Diagn Ther 2013;33:224-9.
21. Morlando M, Ferrara L, D’Antonio F et al. Dichorionic triplet pregnancies: risk of miscarriage and severe preterm delivery with fetal reduction versus expectant management. Outcome of a cohort study and systematic review. BJOG 2015;122:1053-60.