Single and Double Fetal Loss in Twin Pregnancy
Mark D. Kilby, Leo Gurney, Janice L. Gibson and R. Katie Morris
The Facts
First-Trimester Single Fetal Demise
Loss of a twin before 12 weeks of gestation maybe referred to as ‘vanishing twin syndrome'.
Due to the non-viable embryo becoming incorporated into placental membranes, a proportion of such pregnancies will be unrecognised and misclassified as singleton gestations. Determining the rate of first-trimester twin loss is therefore difficult. When diagnosed, early co-twin loss does not seem to be associated with subsequent morbidity in surviving infants; however, it has an important implication for the interpretation of non- invasive prenatal chromosome anomaly screening and may contribute to an increased risk of ‘false positive' results.1Spontaneous Second- or Third-Trimester Fetal Loss
A single twin demise in the second or third trimester of a pregnancy (in either monochor- ionic (MC) twins or dichorionic twins (DC) twins) should be considered differently to earlier loss as it is associated with increased risk of late miscarriage, stillbirth, preterm birth and morbidity for the surviving twin.2
Rates of Second- or Third-Trimester Fetal Loss in Twin Pregnancy
Within the UK, twin stillbirth (after 24 weeks) and infant death surveillance data are presented annually within UK-MBRRACE perinatal mortality reports. The most recent publication assessed pregnancy losses in 2017 and demonstrated a stillbirth rate of twin fetuses of 6.99 per 1,000 live-born twin infants.3 This is more than double the stillbirth rate of singleton fetuses (3 per 1,000 live-born singletons). There has, however, been a progressive reduction in UK twin stillbirth rates, with an apparent drop from 11.07 per 1,000 live twin births since 2014 documented in UK-MBRRACE reports and over the longer term from 16.7 per 1,000 live twin births in 2000 documented in preceding national perinatal surveillance programmes.4 This provides encouragement that a number of national and international guidelines published during these time frames have had some positive effect on the outcomes of these high-risk pregnancies through the promotion of specialist and structured management.
The chorionicity of a twin pregnancy has an important influence on risk of fetal loss. National data on the rate of stillbirths in twins divided by chorionicity are difficult to obtain and are still not reported universally in multiple pregnancy research. Surveillance data of twin pregnancy outcomes collected through MBRRACE-UK now record the chorionicity of demised fetuses in more than 95% of cases. Calculations of rates of loss are hindered by the lack of linked national denominator data (live-born twins subdivided by chorionicity). However, applying an assumption that 80% of live-born twins are dichorionic to the MBRRACE-UK loss data collected between 2016 and 2018, it can be estimated that stillbirth rates fell from 27 to 19 per 1,000 live twin births in MC twins, and from 5 to 3 per 1,000 live twin births in DC twins.4
The reports do not calculate the rates of single compared to double in utero loss in twin pregnancies, however the majority appear to be single fetal losses.3 The importance of more detailed data in twin pregnancies is recognised and forms the basis of a current case-based audit by UK-MBRRACE. An additional consideration when using national data to inform fetal loss rates is that although these national reports also include a separate data set on fetal losses from 22 to 24 weeks of pregnancy, complications of MC twin pregnancies, such as twin-twin transfusion syndrome (TTTS) and severe selective growth restriction (sGR), may present early in the second trimester and be associated with fetal demise at gestations earlier than 22 weeks and therefore remain hidden from national statistics.4
Aetiology of Fetal Loss in Twin Pregnancy
Maternal Causes of Fetal Loss
Compared to singletons, a higher incidence of pregnancy-related maternal conditions is associated with an increased risk of stillbirth, such as hypertensive disorders and gestational diabetes. Additionally, pre-existing maternal autoimmune, cardiac and renal disease can predispose to fetal loss, with such risks increased in multiple pregnancy.
Fetal Causes of Loss
Most DC twin pregnancies are dizygotic and therefore, as each embryo is associated with its own aneuploidy risk, the overall per-pregnancy aneuploidy risk is nearly twofold that of singletons. In contrast, except in rare cases of discordant chromosome anomalies (heterokaryotypic monozygotism), MC twin pregnancies have a similar per-pregnancy aneuploidy risk to singleton pregnancies (albeit with both fetuses affected). In addition to an aneuploidy causing fetal loss, a risk of loss accompanies the screening programme for such fetal chromosome anomalies. Twin pregnancies that undergo first-trimester screening for aneuploidy (by nuchal measurement, serum biochemistry or free fetal DNA) are subject to a greater false positive rate compared with singleton pregnancies, which may lead to an increased likelihood of being offered prenatal invasive testing. The risks of pregnancy loss following invasive testing are increased, with a loss rate up to 3.8% following chorionic villus sampling and 3.1% following amniocentesis, compared with rates of 0.5-1% for singletons.5
Monozygotic twins (all MC twins and approximately 20% of DC twins) are at increased risk of structural anomalies. The pathology reflects problems that can occur during embryonic cleavage with complex midline structures at particular risk, giving an increased risk of cardiac and neural tube abnormalities.6 Structural anomalies may place the affected fetus and the co-twin at risk of in utero demise, with additional iatrogenic risk if selective termination of pregnancy is opted for.
Placental and Membrane Causes of Fetal Loss
Utero-placental dysfunction occurs more commonly in twin pregnancies, predisposing fetuses to intrauterine growth restriction. Although both fetuses may be affected, it is frequently selective, affecting one of the pair. Selective growth restriction is defined as a condition whereby one fetus is growth restricted, defined as < 10th centile for estimated fetal weight (EFW), alongside an inter-twin growth discordance of > 25%.
At these thresholds there is a significant risk of in utero demise of the growth-restricted fetus. Management of sGR is more complex than that of growth restriction complicating a singleton pregnancy as the risks of interventions to both fetuses must be considered.In DC twin pregnancies, if sGR is diagnosed at early viable gestations, then iatrogenic early delivery will remove the risk of in utero demise of a compromised twin, but may be associated with unacceptable risks of neonatal mortality and morbidity due to prematurity. In such a situation, a conservative approach in the interests of the appropriately grown twin may be justified. In MC twin pregnancies, the management is even more complex as in utero loss rates of individual fetuses are less independent because of the shared fetal circulations within the single placenta. Selective termination of pregnancy by vascular occlusive methods at pre-viable gestations or an earlier gestational threshold for premature delivery are options to try to reduce the risks of double fetal loss.
As well as increasing the incidence and complicating the management of severe sGR, the shared placenta of monochorionic twins places these fetuses at risk of the specific complications of TTTS, twin anaemia polycythaemia sequence (TAPS) and monoamnionicity. Twin-twin transfusion syndrome occurs in up to 15% of MCDA twin pregnancies and without interventional therapy, the risk of death for both twins is high (80-90%).
Treatments for TTTS such as fetoscopic laser ablation (FLA) (or more rarely serial amnioreduction) offer the possibility of improved survival for one or both affected twins. Fetoscopic laser ablation is associated with an improvement in survival without neurological impairment and is the recommended treatment of TTTS where available.7 Equatorial laser ‘dichorionisation’ (the Solomon technique) can reduce the risk of TTTS recurrence or subsequent TAPS compared to selective ablation of anastomosis.8 Internationally, FLA offers up to 75% overall survival rate for MC pregnancies complicated by TTTS.9 Thus, although TTTS outcomes are greatly improved with treatment, a chance remains of single (20-25%) or double (10-15%) fetal loss from which, given the invasive nature of the procedure, there may be an iatrogenic contribution.7
Twin anaemia polycythaemia sequence is defined by a significant discordance in haemoglobin levels between twins without substantial differences in amniotic fluid volume.
It is thought to occur from a chronic transfusion of blood from a donor to recipient fetus via miniscule (< 1 mm) artery-vein anastomoses. It affects 2% of MCDA pregnancies spontaneously, but this may increase to 13% following FLA if the Solomon technique is not utilised.7 Twin pregnancies with this condition will be at increased risk of miscarriage and stillbirth; however, there is little evidence from prospective cohort studies regarding outcomes and optimal clinical management of this pathology.Monochorionic-monoamniotic (MCMA) twin pregnancies are rare, constituting 5% of all monochorionic pregnancies but < 1% of all twin pregnancies.10 They have a very high fetal and perinatal loss rate of 50% prior to 16 weeks of gestation, secondary to fetal abnormality or spontaneous miscarriage. Loss rates at later gestations have fallen from 40% to 10-15%, largely due to the management of such cases in specialist centres and delivery at an optimal preterm gestation. Monochorionic-monoamniotic twins are at increased risk of fetal loss from 34 weeks of gestation and therefore delivery via caesarean section is indicated between 32 and 33+6 weeks of pregnancy.
A reported rate of preterm, pre-labour rupture of the membranes (PPROM) in twin pregnancies of 11% versus a singleton rate of 3-4% can expose the pregnancy to ascending bacterial infection with the potential to place either twin at risk of preterm birth, stillbirth or early neonatal death. As with singletons, transplacental infections such as cytomegalovirus or parvovirus B19 are recognised causes of stillbirth for twins.
Iatrogenic Fetal Loss
The main iatrogenic cause of fetal loss in twin pregnancies is selective feticide. This may be performed in cases of discordant fetal chromosomes or structural anomaly in any twin pregnancy, or if there is evidence of severe single fetal compromise in a monochorionic twin pregnancy, such as severe early-onset sGR. The method of feticide will depend on the chorionicity of the pregnancy.
Ultrasound-guided injection of an abortifactant into the fetal circulation of the affected twin is only appropriate for DC pregnancies (with discordant fetal circulations) and is associated with an incidence of overall pregnancy loss of 7% and a preterm birth risk of 14% before 32 weeks. In monochorionic twins, due to the shared fetoplacental circulation, vascular occlusive procedures including ultrasound-guided intra-fetal laser (IL), usually < 16 weeks; radiofrequency ablation (RFA) up to 22 weeks; or bipolar cord occlusion (BCO) are required for selective feticide to minimise risks to the surviving cotwin. Case series have demonstrated variation in risk of further fetal loss from 12.5% to 7.7% with RFA associated with the lowest co-twin loss rate and risk of amniorrhexis.11Pregnancy-Associated Risks following Spontaneous Single Intrauterine Fetal Death
The prognosis of the co-twin after spontaneous single intrauterine fetal death (sIUFD) has been analysed in systematic reviews and meta-analysis of the literature, the most recent published in 2019.2 In this review, pregnancies were stratified to allow for separate analysis according to chorionicity of pregnancy.
As can be seen in the results summary in Table 12.1, these data indicate an approximately twofold increased risk for co-twin death in MC (41%) compared to DC pregnancy (22.4%) following a single intrauterine twin death, with rates of neonatal deaths also increased for MC pregnancies (27.8% vs 21.2%). For MC twins, when sIUFD occurred at less than 28 weeks, there was a significantly increased rate of co-twin fetal intrauterine death (OR 2.31, 95% C1 1.02-5.25) or neonatal death (OR 2.84, 95% CI 1.14-20.47) compared to twin gestations where the initial sIUFD occurred after 28 weeks of gestation.2
Co-twin survivors of sIUFD are also at significantly increased risk of neurodevelop- mental abnormalities when compared to viable twin pregnancy controls. In cases of sIUFD, surviving co-twins are at greater risk of subsequent cerebral palsy (CP) than pregnancies where both twins survive (OR 6.3; 95% CI: 3.1-12.8)2 and chorionicity again appears to be a key determinant of risk: epidemiological studies reviewing the rates of CP for survivors in pregnancies affected by single twin demise, using same- or different-sex twins as a surrogate means of determining chorionicity, found a rate of CP of 106 per 1,000 for same-sex twins, compared with 26 per 1,000 for different-sex twins.12 Data from
Table 12.1 Adverse outcomes affecting surviving co-twin following single intrauterine fetaldeath. Adapted from Mackieet al.2 Table includes the monochorionic and dichorionicevent rates and comparative odds ratios for the following outcomes: co-twin death, preterm birth (less than 34 weeks), abnormalfetalbrain MRI, other abnormalfetalbrain imaging, neurodevelopmentalmorbidity and neonataldeath.
| Adverse co-twin event | Monochorionic event rate (number of studied pregnancies) | Dichorionic event rate (number of studied pregnancies) |
| Intrauterine fetal death | 41% (379) | 22% (255) |
| Abnormal antenatal brain fMRI | 20% (116) | |
| Preterm birth (24+0 to 34+0 weeks of gestation) | 58% (202) | 54% (107) |
| Neonatal death | 28% (206) | 21% (130) |
| Neurodevelopmental morbidity | 28% (103) | 10% (62) |
| Abnormal postnatal | 43% (140) | 21% (75) |
brain imaging (CT, MRI or USS)
systematic reviews report event rates for neurodevelopmental abnormality of 28.5% for monochorionic twins and 10% for dichorionic twins after sIUFD.2 However, such figures must be viewed in the context of the high risk of premature birth for twin pregnancies in general and following IUFD as prematurity can predispose towards or cause secondary neurological disability.
For both MC and DC pregnancies, there is an increased risk of preterm birth following sIUFD, with systematic reviews finding an increased risk of preterm birth between 24+0 and 34+0 weeks gestation for the remaining co-twin of 58.5% for MC and 53.7% for DC pregnancies. The limited data available suggest that iatrogenic preterm birth occurs more commonly in MC pregnancies, possibly indicating a lower threshold for clinical intervention due to the increased risks faced by these pregnancies.6
An increase in maternal hypertensive disorders in twin pregnancies following sIUFD has been observed when compared to viable twin pregnancy controls; however, there is no published evidence to date suggesting an increased risk of maternal coagulopathy or sepsis for a mother of a twin pregnancy complicated by a single fetal loss.
The Issues
Can Spontaneous Intrauterine Fetal Death Be Avoided?
As described earlier in this chapter, there are a broad range of predisposing factors to sIUFD, including maternal risks, fetal risks and those specifically relating to chorionicity. National guidance should be followed wherever possible and twin pregnancies should be managed within multidisciplinary teams with a specialist interest in such pregnancies. Given the potentially very high risks of stillbirth, MCMA pregnancies should be managed in fetal medicine centres with specialist expertise.
Any pre-existing maternal illness which may confer additional risk to the pregnancy (e.g. anti-phospholipid syndrome, diabetes mellitus, other autoimmune or maternal renal or cardiac disease) should be identified and management optimised prior to and during the pregnancy in specialised maternal medicine clinics. Additionally, the pregnancy-associated conditions of gestational diabetes and hypertensive disorders of pregnancy should be appropriately screened for and managed if they arise. Careful discussion and counselling regarding the dilemmas associated with twin aneuploidy and anomaly screening, including the iatrogenic risks of invasive investigations or feticide, should be fully discussed with parents prior to testing.
For all twin pregnancies, regular ultrasonographic assessment of fetal biometry, liquor volume and umbilical artery Doppler velocimetry is advised. In DC pregnancy, this can be performed every three to four weeks from 20 weeks of gestation onwards, although this may need to be more frequent and include more advanced Doppler assessments should there be concerns regarding fetal growth or well-being. Fortnightly screening for TTTS and sGR in MC pregnancies should begin at 16 weeks and continue throughout the pregnancy, to include ultrasonographic assessment of fetal biometry, liquor volume and umbilical artery Doppler velocimetry. When diagnosed using ultrasound, TTTS should be clinically staged using the Quintero system (with assessment of twin fetal cardiac function) and referred to specialist fetal medicine centres for assessment. Although routine screening for TAPS has not been recommended nationally in the UK in uncomplicated MC twins, for high-risk cases (those with TTTS or who have undergone FLA), serial middle cerebral artery peak systolic velocity (MCA-PSV) measurements should be performed on both twins.13
Data from systematic reviews evaluating risk of stillbirth in twins demonstrated that risk of stillbirth increases progressively with later gestations and the risk of neonatal complications diminishes to favour delivery at 36-37 weeks in uncomplicated MC pregnancies and delivery at 37-38 weeks in uncomplicated DC pregnancies.14
What Monitoring Should Take Place after Spontaneous Intrauterine Fetal Death?
Following sIUFD in DC pregnancy, although there is no increased risk of antenatal neurological co-twin damage, there is a twofold increased risk of co-twin death and a risk of preterm birth before 34 weeks of 53.7%.2 There is no clear evidence base to guide clinicians on the best means of avoiding these outcomes, and therefore individuals should be managed on a case-by-case basis. Regular ultrasound surveillance of the remaining cotwin should occur to assess fetal growth, liquor volume and umbilical artery Doppler velocimetry, the timing of which can be tailored according to current fetal status and to support maternal psychological well-being. Surveillance for preterm birth should be limited to patient education regarding the risks, any signs and symptoms and an awareness of the importance of early presentation to a unit with appropriate neonatal facilities. In situations where preterm labour is suspected or preterm delivery is planned, interventions such as antenatal steroids to aid fetal lung maturity or magnesium sulphate for fetal neuroprotection should be considered based on a critical assessment of optimal benefit according to fetal gestation.
The increased risk of stillbirth and neurological morbidity for MC co-twin survivors has been explained by a ‘transfusional hypothesis’ whereby a single twin demise leads to a comparative fall in the vascular pressure for the chorionic unit supplying the demised twin, compared to the area supplying the surviving twin, and thus leads to an acute transfusion from the survivor to the demised twin. Evidence for this theory derives from a study examining the results of fetal blood sampling following a single twin death in a series of eight twins: samples taken from surviving twins following loss of the co-twin demonstrated significant new-onset anaemia.15
In MC pregnancies complicated by sIUFD, MCA-PSV Doppler studies performed on cotwin survivors before and after in utero fetal blood sampling and intrauterine transfusion (IUT) have demonstrated good correlation between MCA-PSV and pre- and post-transfusion haemoglobin concentration. Thus, surveillance of MCA PSV can be recommended from within 24 hours for surviving co-twins of monochorionic pregnancies complicated by sIUFD, and it may be suitable to continue this surveillance through the pregnancy according to an individualised plan (Figure 12.1).
Following sIUFD in MC twin pregnancies as described for DC pregnancies, regular ongoing ultrasound assessment of fetal well-being should be performed. Without evidence to guide the frequency of these ultrasound assessments, weekly assessments of liquor volume, comprehensive Doppler studies and brain structure are suggested by the authors for four weeks (with biometry performed fortnightly) following sIUFD. If reassuring, these may be spaced to fortnightly intervals with maternal anxieties taken into consideration.
Although fetal brain lesions in up to 4.9% of MC co-twin survivors may be identified by ultrasound within a week of sIUFD, in utero MRI (iuMRI) can improve this detection rate by 33%. The largest multicentre study examining antenatal iuMRI fetal brain changes in surviving MC co-twins demonstrated ventriculomegaly as the only intracranial finding in 3.4%, and other abnormalities in 9.7% of surviving twins. The pattern of neurologic acquired anomaly may range from focal ischaemic lesions (with or without reparative polymicrogyria) to global ischaemic or haemorrhagic abnormalities.16,17 An iuMRI image demonstrating an example of reparative polymicrogyria in a surviving MC co-twin is displayed in Figure 12.2. Recent evidence supports that, where available, an assessment of brain damage can be performed with higher resolution single-shot fast-spin-echo T2- weighted MRI sequences from seven days after fetal demise.16
If an iuMRI for a surviving MC co-twin is performed prior to 28 weeks and is normal, then further iuMRI later in pregnancy may be considered to pick up neuronal migration disorders that may have been acquired. If a brain lesion associated with neurodevelop- mental morbidity is confirmed radiologically, the option of terminating the pregnancy should be discussed with the parents in a non-judgmental fashion.
Can Co-twin Sequelae following Spontaneous Intrauterine Fetal Death Be Avoided?
Additional to the risks of preterm delivery, surviving co-twins of an MC pregnancy complicated by sIUFD are at increased risk of stillbirth and neurological insult. Due to the complex nature of decision-making involving such pregnancies, referral to a specialist centre for further management is recommended.
In a case series reporting on pregnancy outcomes following intrauterine transfusion (IUT) for MC co-twin survivors, all non-anaemic babies achieved normal outcomes. Anaemic babies receiving intrauterine transfusion demonstrated improved survival, but up to 30% of these babies had subsequent neurological abnormalities.18 Therefore, fetal blood sampling and IUT can be offered in cases where fetal anaemia of the remaining co-twin is suspected on
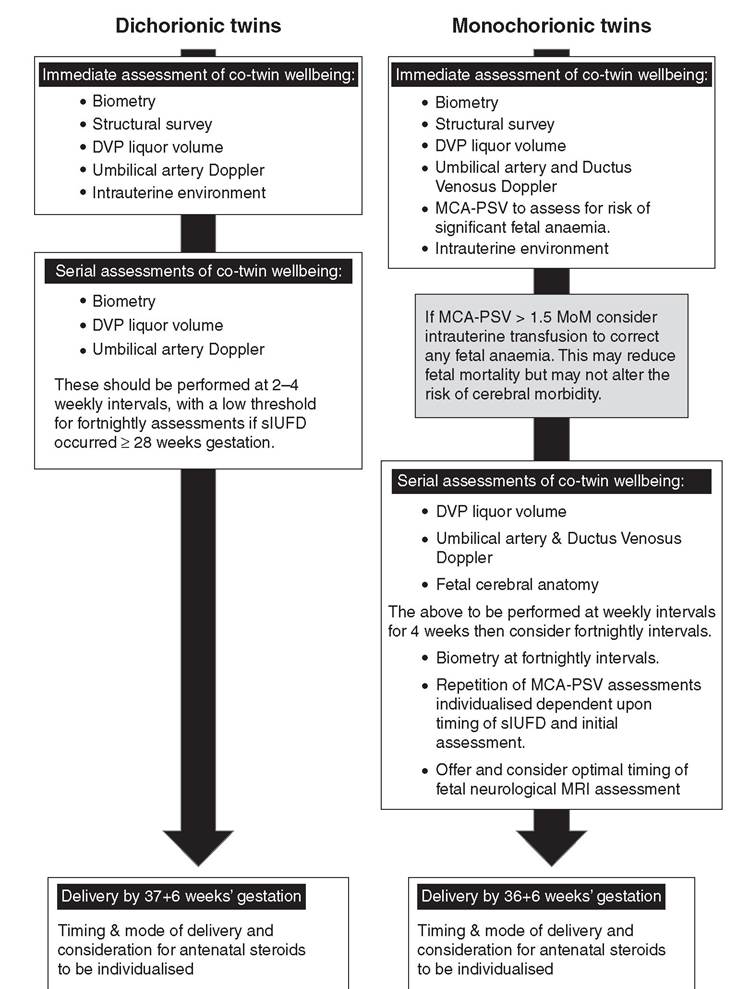
Figure 12.1 Authors' suggested management approach for co-twin survivors in cases of single in utero fetal demise for both dichorionic and monochorionic pregnancies
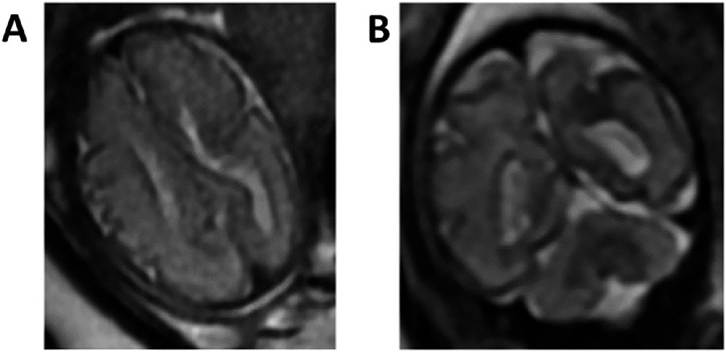
Figure 12.2 Example of reparative polymicrogyria in surviving MC co-twin. Adapted from Griffiths et al.17 Exact time of single intrauterine demise is unknown but is after 27 weeks of gestation. The iuMRIperformed here at 32 weeks shows an abnormalcleft in the left paracentral lobe lined by abnormalcortex (A axialand B coronalsingleshot, fast-spin echo images). This can be interpreted as a site of previous infarct and reparative polymicrogyria.
the basis of abnormal MCA-PSV; however, parents should be aware that although the evidence supports improved survival, it may not alter the neurological prognosis.
Iatrogenic considerations can influence the subsequent prognosis of surviving co-twins following sIUFD. For dichorionic pregnancies undergoing selective feticide for fetal anomaly, it is an option to delay the procedure until advanced gestations (32-34 weeks) due to procedure-related complications (i.e. amniorrhexis) increasing risks of preterm birth. However, it should be taken into account that the anomalous twin itself may increase the risk of a preterm birth occurring and therefore the possible window for performing selective termination may be lost.
Selective feticide procedures for MC pregnancies may carry a risk to the co-twin dependent on the type of procedure with procedure-related co-twin death appearing to be higher with interstitial laser (12.5%) than with the use of bipolar cord occlusion (9.1%) or radiofrequency ablation techniques (7.5%).11 The incidence of neurodevelopmental impairment in MC co-twin survivors following selective feticide has been reported in long-term follow-up data as 6.8%, which compares favourably with a rate of 28.5% for MC co-twin survivors of spontaneous sIUFD.19
Studies examining neurological outcome from MC twins following FLA for TTTS do not demonstrate differences between pregnancies where subsequent fetal loss occurs, compared to those where both twins survive. This may suggest that ablation of inter-twin placental anastomosis confers a protective effect on surviving co-twins in the event of sIUFD. Technique of ablation does not directly appear to affect risk of neurological morbidity, with data from randomised controlled trials comparing the Solomon technique with standard anastomotic ablation reporting similar subsequent rates of severe cerebral injury (5% and 6% respectively).8 Despite this, the Solomon technique is shown to reduce rates of recurrent TTTS and post-laser TAPS and theoretically this should have a neuroprotective benefit for surviving co-twins.
How and When Should Delivery Take Place after Spontaneous Intrauterine Fetal Death?
Dichorionic twins do not share a circulation and there is not an increased risk of antenatal neurological damage to the surviving co-twin following sIUFD, and therefore preterm birth is the most prominent risk faced by such pregnancies. Although limited outcome data are available for preterm twin pregnancies, it is recognised that for singleton pregnancies, moderate to late preterm deliveries (32-36 weeks) can exhibit mild developmental delay at two years of age when compared to full-term controls. Therefore, in the absence of evidence of maternal or fetal compromise, aiming to prolong the pregnancy towards 37 weeks of gestation is advisable.
For MC pregnancies complicated by sIUFD, the initial management dilemma is whether to choose conservative surveillance of the pregnancy in order to advance fetal gestation or opt for immediate delivery. There is little evidence to guide the obstetrician as to whether immediate delivery is of benefit or harm. Several considerations must be balanced: co-twin demise appears more likely within seven days of sIUFD, large placental vascular anastomoses predispose to adverse outcome and detailed ultrasound assessment of the surviving co-twin is the primary indicator as to whether the fetus is at imminent risk of loss. The exact timing of neurological insult in MC surviving co-twins following sIUFD is unknown and it is possible that such damage may occur immediately. Therefore, immediate delivery may not be of value in reducing the risk of neurodevelopmental delay in surviving co-twins, even at advanced gestations.
For MC twins, therefore, any decision regarding immediate delivery upon diagnosis of sIUFD will depend upon the current gestational age, available information concerning the surviving fetal condition or maternal well-being, and a weighing up of the ongoing risk of in utero demise compared to the iatrogenic preterm delivery risks of neonatal mortality and morbidity. Where conservative management is implemented, then delivery is likely to be justified earlier than 36-37 weeks with precise timing individualised by the complex interplay of obstetric and maternal concerns.
Vaginal delivery may be considered in twin pregnancies where sIUFD has occurred and decisions regarding mode of delivery can be individualised in discussion with the woman. If the demised twin is presenting, then there is the potential for intra-partum dystocia or obstruction and delivery by caesarean section is typically preferred. For MC pregnancies, there is an increased risk of planned delivery between 34 and 36 weeks of gestation and therefore such pregnancies are more likely to be delivered by caesarean section.
Pregnancy Management following Spontaneous Intrauterine Fetal Death
As with prognosis, the management of sIUFD is highly dependent on chorionicity and gestation. There remains a lack of a strong evidence base for management in cases of sIUFD in multiple pregnancy, with recommendations largely based on case reports, case studies and expert opinion. A suggested approach to the management of such pregnancies is outlined in Figure 12.1. For multiple pregnancies complicated by sIUFD in the first trimester, there is minimal ongoing risk to the remaining co-twin in MC or DC pregnancies other than an increased risk of miscarriage to the whole pregnancy; therefore, a conservative approach throughout the remaining pregnancy is warranted.
Once sIUFD has been confirmed, rhesus-negative mothers should have a Keilhauer test and an appropriate volume of anti-D should be administered to minimise risk of alloimmunisation. The mother should have close surveillance for hypertensive disorders of pregnancy and should be educated about signs and symptoms of preterm labour with advice to present early for assessment if she has any concerns. Ideally, the ongoing monitoring of her pregnancy should be provided though a named multidisciplinary team to whom she can promptly self-refer.
Following delivery, parents should be encouraged to consider the benefits of postmortem and placental histology to investigate or help confirm the cause of single or double in utero death. Surviving neonates should be assessed for the need of neonatal and paediatric follow-up. Infants delivered preterm and those with known abnormal antenatal neurological findings should have specialised neurodevelopmental follow-up.
Parents should be offered postnatal follow-up with a senior obstetrician, ideally the clinician managing their case prenatally. This discussion should cover what occurred during the pregnancy, review the results of any investigations, talk about any implications for future pregnancies and ensure that parents are managing emotionally and have multidisciplinary support. Loss of a twin is a devastating emotional experience for parents. Educating parents about support and counselling services is important, and referral to perinatal mental health services should be considered if there are risk factors for or evidence of postnatal depression.
Key Points
• Defining rates of single and double twin stillbirth in national surveillance reports is challenging; however, there appears to be an overall trend towards twin stillbirth reduction from UK reported data.
• The causes of twin single or double fetal loss can be considered as maternal causes, fetal causes, causes related to the chorionic and amniotic status of the pregnancy and iatrogenic causes.
• The key determinants of risk posed to the surviving co-twin are chorionicity and gestation.
• Risk of preterm birth is increased following sIUFD for both DC and MC co-twin survivors.
• Monochorionic co-twin survivors are at additional risk of stillbirth, neonatal death and neurological morbidity.
• Management should be tailored to individual pregnancies with chorionicity and gestation at sIUFD key factors in determining approach.
• Post-delivery investigations including full post-mortem should be offered.
• Postnatal follow-up is essential with emotional and bereavement support for parents a vital component of this.
References
1. Van der Meij KRM, Sistermans EA, Macville MVE et al. TRIDENT-2: national implementation of genome-wide non-invasive prenatal testing as a first-tier screening test in the Netherlands. AmJHum Genet 2019 Dec 5;105(6):1091-1101.
2. Mackie FL, Rigby A, Morris RK, Kilby MD. Prognosis of the co-twin following spontaneous single intrauterine fetal death in twin pregnancies: a systematic review and meta-analysis. BJOG 2019 Apr;126 (5):569-78.
3. MBBRACE-UK. Perinatal Mortality Surveillance Report. 2019. www.npeu.ox.ac.uk/mbrrace-uk/reports
4. Kilby MD, Gibson JL, Ville Y. Falling perinatal mortality in twins in the UK: organisational success or chance? BJOG 2019 Feb;126(3):341-7.
5. Agarwal K, Alfirevic Z. Pregnancy loss after chorionic villus sampling and genetic amniocentesis in twin pregnancies:
a systematic review. Ultrasound Obstet Gynecol 2012 Aug;40(2):128-34.
6. Glinianaia SV, Rankin J, Wright C. Congenital anomalies in twins: a register-based study. Hum Reprod 2008 Jun;23 (6):1306-11.
7. Roberts D, Neilson JP, Kilby MD, Gates S. Interventions for the treatment of twin-twin transfusion syndrome. Cochrane Database Syst Rev. 2014 Jan 30;(1): CD002073. https//:doi.org/10.1002/146518 58.CD002073.pub3. PMID: 24482008.
8. Slaghekke F, Lopriore E, Lewi L et al. Fetoscopic laser coagulation of the vascular equator versus selective coagulation for twin-to-twin transfusion syndrome: an open-label randomised controlled trial. Lancet 2014;383(9935):214-51.
9. Mullers SM, McAuliffe FM, Kent E et al. Outcome following selective fetoscopic laser ablation for twin to twin transfusion syndrome: an 8 year national collaborative experience. Eur J Obstet Gynecol Reprod Biol 2015;191:125-9.
10. Litwinska E, Syngelaki A, Cimpoca B, Frei L, Nicolaides KH. Outcome of twin pregnancy with two live fetuses at 11-13 weeks' gestation. Ultrasound Obstet Gynecol 2020;55(1):32-8.
11. Nobili E, Paramasivam G, Kumar S. Outcome following selective fetal reduction in monochorionic and dichorionic twin pregnancies discordant for structural, chromosomal and genetic disorders. Aust NZ J Obstet Gynaecol 2013;53(2):114-18.
12. Pharoah PO, Adi Y. Consequences of in-utero death in a twin pregnancy. Lancet 2000 May 6;355(9215):1597-1602.
13. RCOG. Management of monochorionic twin pregnancy: Green-Top Guideline No. 51. BJOG 2017 Jan;124(1):e1-e45.
14. Cheong-See F, Schuit E, Arroyo-Manzano D et al. Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis. BMJ 2016;354:i4353.
15. Nicolini U, Pisoni MP, Cela E, Roberts A. Fetal blood sampling immediately before and within 24 hours of death in monochorionic twin pregnancies complicated by single intrauterine death. Am J Obstet Gynecol 1998 Sep; 179(3 Pt 1):800-3.
16. Conte G, Righini A, Griffiths PD et al. Brain-injured survivors of monochorionic twin pregnancies complicated by single intrauterine death: MR findings in
a multicenter study. Radiology 2018 Aug;288(2):582-90.
17. Griffiths PD, Sharrack S, Chan KL, Bamfo J, Williams F, Kilby MD. Fetal brain injury in survivors of twin pregnancies complicated by demise of one twin as assessed by in utero MR imaging. Prenat Diagn 2015 Jun;35(6):583-91.
18. Tanawattanacharoen S, Taylor MJ, Letsky EA, Cox PM, Cowan FM, Fisk NM. Intrauterine rescue transfusion in monochorionic multiple pregnancies with recent single intrauterine death. Prenat Diagn 2001 Apr;21 (4):274-8.
19. Van Klink J, Koopman H, Middeldorp J et al. Long-term neurodevelopmental outcome after selective feticide in monochorionic pregnancies. BJOG 2015;122(11):1517-24.
Chapter
More on the topic Single and Double Fetal Loss in Twin Pregnancy:
- Invasive Prenatal Diagnosis in Multiple Pregnancy
- Contents
- Multifetal Pregnancy Reduction
- Risk Assessment and Screening for Preterm Birth in Multiple Pregnancy
- New Frontiers in Multiple Pregnancy Management
- Management of Twin-Reversed Arterial Perfusion (TRAP) Sequence
- Gestational Dating in Multiple Pregnancy
- Obstetric Anaesthesia in Multiple Pregnancy
- Multiple Pregnancy Resources for Professionals and the Public
- Epidemiology of stillbirth