Gestational Dating in Multiple Pregnancy
Pierre Mace, Houman Mahallati and Laurent J. Salomon
Introduction
In addition to determining chorionicity and amnionicity, screening for aneuploidies and structural defects, dating of the pregnancy is one of the important goals of ultrasound in twin pregnancies, especially when exams are done in the first trimester.
The primary purpose of dating in twin pregnancies is not entirely the same as in singleton pregnancies in that the estimation of a due date is not as relevant in the context of multiple pregnancies. Most deliveries take place before 40 weeks of gestation, either spontaneously or due to a medical indication. The main objective of dating in multiple pregnancies is to make subsequent ultrasound examinations at later term more effective in the screening and management of complications either specific to twin pregnancies (twin-twin transfusion syndrome (TTTS) or selective fetal growth restriction (FGR)) or more frequent in these pregnancies (preterm birth, structural defects, aneuploidies). One of the recurrent questions is the choice of the fetus upon which to base dating, especially when there is a significant difference between the size of the two twins. This must be done in a manner that does not ignore potential complications and that at the same time does not generate unnecessary parental anxiety or result in further unnecessary investigations.The Issues
When and How?
Routine dating of a singleton pregnancy from a measurement of the crown-rump length (CRL) at the time of first-trimester ultrasound has been shown to be superior to the use of menstrual dates or dating after 14 weeks of gestational age.12 It is likely that the same should apply in twins, although there have been no specific studies demonstrating that it performs better than the last menstrual period. The question is therefore whether the CRL reference charts used in singleton pregnancies can also be used in twin pregnancies.
In cases where the patient presents after 14 weeks of gestation or the CRL measurement is greater than 84 mm, one must use the biometric measurements producing the most accurate prediction of gestational age. Dating options in cases where pregnancies are conceived via assisted reproductive technologies (ART) are discussed later in this chapter.Which Twin?
While it is likely that dating in the first trimester is desirable, there is less consensus on whether pregnancy should be dated on measurements taken on the smallest twin, the largest twin or the mean measurements of the two twins.3 Theoretically, the choice of the smallest 48 twin has the advantage of not creating unnecessary parental anxiety about possible growth restriction as early as the first trimester. The exception to this would be cases with significant and obviously pathological CRL discordances (see later in this chapter). There are three potential disadvantages to this strategy: (1) ignoring growth restriction in the smaller fetus; (2) the potential to incorrectly assume there is fetal macrosomia of the larger twin at a later term; and (3) the risk of neglecting a post-term twin pregnancy. These risks and the relative infrequency of large-for-gestational-age fetuses in twin pregnancies explain the common practice of dating the pregnancy based on the larger twin. In this situation, the choice is effectively that of increasing the sensitivity of screening for selective FGR whilst recognising the increased risk of a higher number of false positives and potentially unnecessary additional testing and increasing parental anxiety. The choice should therefore be based on the most accurate measurement in this context, but unfortunately the literature is inconsistent as to what constitutes the most accurate measurement, with several authors finding a higher performance of either the smallest CRL,3,7 or the mean of the two measurements,4 while the largest CRL often leads to the greatest difference with the assumed date of pregnancy by in-vitro fertilisation timing.
Putting this into perspective, given that CRL discordance in twin pregnancies is rare (less than 10% of twins have a discordance of more than 10%), the mean discrepancy between twins at the time of first-trimester ultrasound would be expected to be very low.3,8
In a prospective study including 182 twin pregnancies, Salomon et al.3 showed that the mean difference in the CRL measurement between the two twins was 3.4 mm or 1.2 days. This was supported in a large retrospective study on 6,225 twin pregnancies which stated that the mean difference in CRL measurement was 3.2 mm in dichorionic pregnancies and 3.6 mm in monochorionic-diamniotic pregnancies.8 In this sense, using the formula reported by Robinson et al., a 3 mm difference in CRL measurement is at most equivalent to a difference of 2 days of gestational age.9 As mentioned later, this difference may simply reflect different growth patterns and/or measurement errors of two normal fetuses and is well below the measurement error reported for CRL assessment. It is therefore unlikely to have a significant impact on subsequent pregnancy follow-up.
The situation is different in the presence of a major discrepancy between CRL measurements. Several different cut-offs of significant CRL discrepancy have been proposed, which is itself a concern as the association between CRL discordance and adverse outcomes is highly dependent on the threshold adopted. It is therefore important to set a threshold to define a significant discrepancy that could impact the pregnancy outcome. The ≥10mm or 15% CRL discordance are the most commonly used thresholds to represent the higher centiles of discordance, and the 95th percentile for CRL discrepancy seems to be around 10 mm, which is a 14% difference in CRL measurement or 3.6 days of gestational age.3 Again, according to Robinson et al., a 10 mm difference is equivalent to a difference of between 4 and 6 days depending on the gestation at the time of measurement.9
Above these limits, the dating of the pregnancy should be based on the larger twin's CRL, as this major discrepancy probably indicates a very early-onset growth restriction of the smallest twin, which may have the same significance as in a singleton pregnancy and reveal a chromosomal defect or structural abnormalities.3 However, it is to be noted that the role of CRL discordance in screening for aneuploidy is probably limited with the introduction of non-invasive prenatal testing.
A significant CRL discordance has also been reported as an early predictor of adverse pregnancy outcomes such as significant birthweight discrepancy10, selective intrauterine growth restriction (IUGR), fetal loss before 20 or 24 weeks of gestation, preterm birth,8,11 fetal loss after 24 weeks of gestation11 or TTTS in monochorionic twins 8,12-14 - with a moderate strength of association and too poor prediction accuracy to form a clinically relevant screening test for these adverse outcomes.8,11The Management Option
When and How?
The dating of twin pregnancies should ideally be based on that of singletons and should be performed when the CRL measurement is between 45 and 84 mm (i.e. 11+0 to 13+6 weeks of gestation), using the same singleton reference chart used at the time of the routine first- trimester examination.4,5
Dias et al.4 compared the dating of twin and singleton pregnancies (controls) conceived following ART by measuring the CRL (Robinson charts9) and compared CRL-based dates with the known date of conception. They showed that the variation in CRL between singletons and twins was unlikely to be clinically relevant, with a maximum variation of about 2 mm or 1 day, well within the first-trimester ultrasound accuracy range for dating pregnancy, and probably consistent with normal physiological variation. If the woman presents after 14 weeks of gestational age and with a CRL measurement above 84 mm, the dating of pregnancy should be based on measurement of the head circumference,2,5 which appears to produce the most reliable prediction.15
As is the case for singleton pregnancies, twin pregnancies conceived via ART should be dated using the oocyte retrieval date or the embryonic age from fertilisation.5 In the case of pregnancies conceived either spontaneously or via ART, significant discrepancy between the two twins (>10 mm, >15%) should lead to consideration of additional investigations of the smallest twin, which is the twin at higher risk of aneuploidy or FGR, and closer followup of the pregnancy should be instituted.
This is despite the poor screening performance for adverse pregnancy outcomes as stated earlier in this chapter. An additional earlier scan at 14 weeks for monochorionic pregnancies and 16 weeks of gestational age for dichorionic pregnancies should still be offered. With regards to the risk of aneuploidy, future research should investigate the relevance of major CRL discrepancy in the era of cfDNA testing.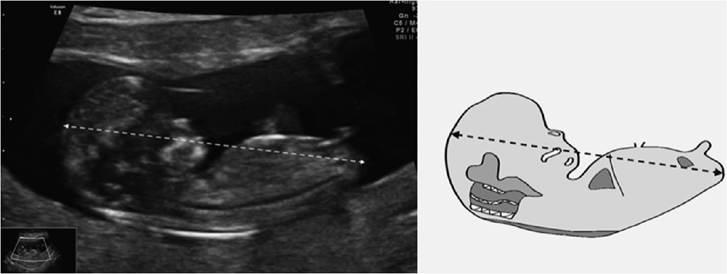
Figure 5.1 Crown-rump length measurement, left: ultrasound view, right: schematic view
Which Twin?
In the vast majority of twin pregnancies for which the discordance is less than 15% (i.e. in practice less than 7-12 mm), the question of which twin to use for dating remains debatable.
While the smaller twin, which appears closer to the actual age in ART-conceived pregnancies, could be used for dating, this will decrease the FGR detection rate later in pregnancy.3,7 The use of the average CRL will reduce the random error of the measurements. Finally, the use of the larger twin allows for a simple and consistent practice since it applies even in the case of a major discrepancy related to aneuploidy or structural defects of the smaller one and increases the sensitivity of subsequent selective FGR screening. This recommendation has also recently been stated in the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) guidelines on the role of ultrasound in twin pregnancies and is likely to ensure, through its simplicity, a much-needed standardisation of practices.5 To add emphasis, such a recommendation can be applied in all cases regardless of the discrepancy in CRL between the twins. If the woman presents after 14 weeks of gestational age, the larger head circumference should be used for dating pregnancy. The following flow chart summarises the management options for the dating of twin pregnancies.
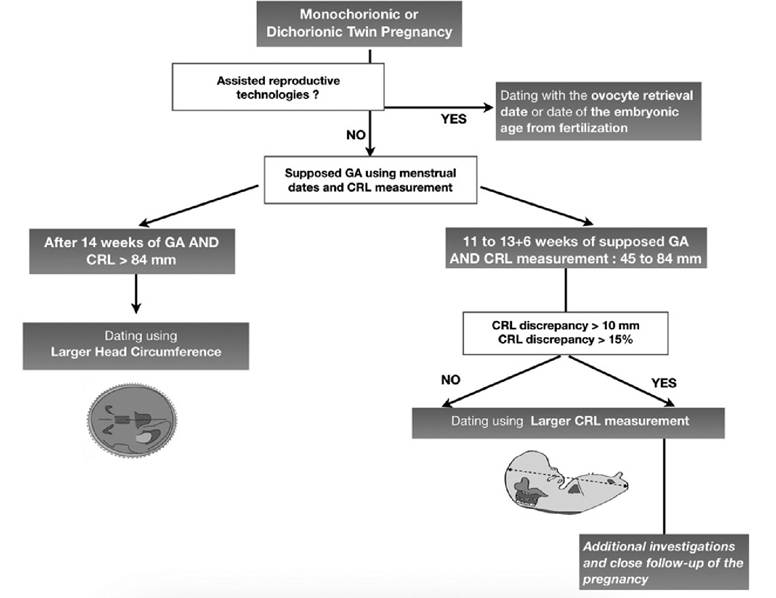
Figure 5.2 Management flow chart for dating of twin pregnancies
Key Points
• Dating of the pregnancy is one of the main objectives of first-trimester ultrasound in twin pregnancies.
• Unlike singleton pregnancies where dating establishes term, due to frequent earlier delivery dates, the main objective of dating twin pregnancies is to improve the screening and management of twin pregnancy complications, especially selective IUGR.
• Twin pregnancies conceived via ART should be dated using the oocyte retrieval date or the embryonic age from fertilisation.
• The dating of twin pregnancies should be based on CRL measurements between 45 and 84 mm (i.e. 11+0 to 13+6 weeks of gestation) using the same reference charts used for singleton pregnancies.
• The mean discrepancy between twins at the time of the first-trimester ultrasound appears to be clinically irrelevant and is unlikely to have a significant impact on subsequent pregnancy follow-up.
• Dating of twin pregnancies using the largest CRL measurement, as advised by the ISUOG guidelines, is the simplest and the most common practice and allows high sensitivity for the screening of selective IUGR.
• Ifthe CRL measurement discrepancy is >10 mm or >15%, additional investigations should be considered for the smaller twin, which is at higher risk of aneuploidy or FGR despite the poor prediction accuracy of CRL discrepancy for adverse pregnancy outcomes.
• After 14 weeks of gestational age or if the CRL measurement is above 84 mm, the larger head circumference should be used for dating pregnancy.
References
1. Whitworth M, Bricker L, Mullan C. Ultrasound for fetal assessment in early pregnancy. Cochrane Pregnancy and Childbirth Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2015 Jul 14 [cited 2019 Apr 11]. http://doi.wiley.com/10.1002/14651858.CD007058.pub3
2. ISUOG Practice Guidelines: performance of first-trimester fetal ultrasound scan. Ultrasound in Obstetrics & Gynecology 2013 Jan;41(1):102-13.
3. Salomon LJ, Cavicchioni O, Bernard JP, Duyme M, Ville Y. Growth discrepancy in twins in the first trimester of pregnancy. Ultrasound in Obstetrics & Gynecology 2005;26(5):512-26.
4. Dias T, Mahsud-Dornan S, Thilaganathan B, Papageorghiou A, Bhide A. First-trimester ultrasound dating of twin pregnancy: are singleton charts reliable? BJOG 2010;117(8):979-84.
5. Khalil A, Rodgers M, Baschat A, Bhide A, Gratacos E, Hecher K et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound in Obstetrics & Gynecology 2016;47(2):247-63.
6. Sebire NJ, D'Ercole C, Soares W, Nayar R, Nicolaides KH. Intertwin disparity in fetal size in monochorionic and dichorionic pregnancies. Obstet Gynecol 1998 Jan;91 (1):82-5.
7. Chaudhuri K, Su L-L, Wong P-C, Chan Y-H, Choolani MA, Chia D et al. Determination of gestational age in twin pregnancy: which fetal crown-rump length should be used? Gestational dating in twins. Journal of Obstetrics and Gynaecology Research 2013 Apr;39(4):761-5.
8. Litwinska E, Syngelaki A, Cimpoca B, Sapantzoglou I, Nicolaides KH. Intertwin discordance in fetal size at 11-13 weeks' gestation and pregnancy outcome. Ultrasound in Obstetrics & Gynecology
2020 Feb;55 (2):189-97. https://obgyn- onlinelibrary-wiley-com.lama.univ-amu.fr∕doi∕10.1002∕uog.21923
9. Robinson HP, Fleming JEE. A critical evaluation of sonar ‘crown-rump length' measurements. Br J Obstet Gynaecol 1975 Sep;82(9):702-10.
10. Kalish RB, Chasen ST, Gupta M, Sharma G, Perni SC, Chervenak FA. First trimester prediction of growth discordance in twin gestations. Am J Obstet Gynecol 2003 Sep;189(3):706-9.
11. D'Antonio F, Khalil A, Pagani G, Papageorghiou AT, Bhide A, Thilaganathan B. Crown-rump length discordance and adverse perinatal outcome in twin pregnancies: systematic review and meta-analysis. Ultrasound in Obstetrics & Gynecology 2014;44(2):138-46.
12. Mackie FL, Hall MJ, Morris RK, Kilby MD. Early prognostic factors of outcomes in monochorionic twin pregnancy: systematic review and meta-analysis. American Journal of Obstetrics and Gynecology 2018 Nov;219(5):436-46.
13. Stagnati V, Zanardini C, Fichera A, Pagani G, Quintero RA, Bellocco R et al. Early prediction of twin-to-twin transfusion syndrome: systematic review and meta-analysis. Ultrasound in Obstetrics & Gynecology 2017 May;49 (5):573-82.
14. Memmo A, Dias T, Mahsud-Dornan S, Papageorghiou AT, Bhide A, Thilaganathan B. Prediction of selective fetal growth restriction and twin-to- twin transfusion syndrome in monochorionic twins.BJOG 2012; 119 (4):417-21.
15. Papageorghiou AT, Kemp B, Stones W, Ohuma EO, Kennedy SH, Purwar M et al. Ultrasound-based gestational-age estimation in late pregnancy. Ultrasound Obstet Gynecol 2016 Dec 1;48(6):719-26.