Screening for Fetal Aneuploidy in Multiple Pregnancy
Maria del Mar Gil and Kypros Nicolaides
The Facts
Aneuploidies, particularly trisomies 21, 18 and 13, are common and major causes of perinatal death and childhood handicap and their prenatal detection has been one of the main goals of fetal medicine.
Diagnosis of fetal aneuploidies necessitates invasive testing by amniocentesis or chorionic villus sampling (CVS) and karyotyping of amniotic fluid and chorionic tissue, respectively. However, these procedures are associated with an increased risk of miscarriage and therefore these tests are carried out only in pregnancies considered at high risk for aneuploidies. Consequently, strategies have focused on the development of effective methods of screening to define the group in need of such invasive testing.The primary aim of screening was always prenatal detection of trisomy 21; however, a beneficial consequence of such screening was the detection of trisomies 18 and 13, Turner syndrome, triploidy and some other rare chromosomal defects.1 In the past 50 years, screening for aneuploidies in singleton pregnancies has evolved from maternal age in the 1970s with detection rate (DR) for Down syndrome of 30% and false positive rate (FPR) of 5%, to second-trimester serum biochemical testing in the 1980s with DR of 50-70% at FPR of 5%, to the first-trimester combined test with maternal age, fetal nuchal translucency (NT) and maternal serum pregnancy-associated plasma protein A (PAPP-A) and free β-human chorionic gonadotrophin (β-hCG) in the 1990s, with DR of 90% at FPR of 5%. Finally, in the past 10 years, several externally blinded validation and implementation studies have shown that it is possible through analysis of cell-free (cf) DNA in maternal blood to detect 99.7%, 97.9% and 99.0% of cases of trisomy 21, trisomy 18 and trisomy 13, respectively, with FPR of about 0.4%, 0.4% and 0.4%, respectively.2
Overall, dizygotic twin pregnancies are at higher risk for aneuploidy than singleton pregnancies because either of the two fetuses could be affected and also because women with such pregnancies are usually older than women with singleton pregnancies.
Consequently, the proportion of these pregnancies that are positive by the traditional methods of screening is considerably higher than in singleton pregnancies. However, prenatal screening and diagnosis for aneuploidy in multiple pregnancies is limited by significant clinical, technical and ethical issues.The Issues
In multiple pregnancies, compared with singleton pregnancies, prenatal diagnosis is complicated because, first, the techniques of invasive testing may provide uncertain results or may be associated with higher risks of miscarriage; second, the fetuses may be discordant for the abnormality; third, the different methods of screening described for singletons need specific corrections and their performance may be lower; fourth, the number of affected cases studied in multiple pregnancies is much lower than in singleton pregnancies; therefore, estimates of test performance will always be less precise.
Monozygotic pregnancies are genetically identical in the vast majority of cases (with very rare exceptions due to post-zygotic changes) and therefore all fetuses are either affected or unaffected, whereas dizygotic (or higher order) pregnancies are genetically different and therefore most likely discordant for the aneuploidy, with one fetus affected and the other(s) not. When screening monozygotic pregnancies, an overall risk assessment is provided for the entire pregnancy, while pregnancies of higher zygosity order will be provided a specific risk for each fetus, being the risk of aneuploidy for each fetus more or less independent of the risk for the other (although NT measurements in both fetuses may be somehow correlated). However, zygosity can only be determined by DNA fingerprinting, which requires amniocentesis, CVS or cordocentesis. Thus, chorionicity, which can be indirectly determined by ultrasound, is used as a proxy for zygosity in prenatal diagnosis: all mono- chorionic twins are monozygotic and about 85% of dichorionic twins are dizygotic.
Conversely, all dizygotic twins are dichorionic whereas two-thirds of monozygotic twins are monochorionic and one-third are dichorionic, depending on the timing of embryo splitting.Monochorionic twins carry a higher risk of structural abnormalities, but the risk of aneuploidy appears similar to the risk in singletons. On the other hand, in dizygotic pregnancies, the maternal age-related risk for chromosomal abnormalities for each twin is the same as in singleton pregnancies and therefore the chance that at least one fetus is affected by a chromosomal defect is about twice as high as in singleton pregnancies.
In multiple pregnancies, effective screening for trisomies can be provided by a combination of maternal age and fetal NT thickness. However, in monochorionic pregnancies, the false positive rate of NT screening is higher than in singletons due to an early manifestation of a twin-twin transfusion syndrome seen as discordant NT thickness among fetuses.3
Serum biochemical marker concentrations used for risk assessment in the first or second trimester in twin pregnancies reflect the presence of two fetuses rather than one and are also different according to chorionicity - that is, around gestational weeks 11-13, maternal serum concentrations in twins are approximately double than those found in singletons.4-6 For this reason, risk assessment for twin pregnancies by the first-trimester combined test or by the second-trimester triple or quadruple test needs adjustment by chorionicity and it is not possible in multiple pregnancies of higher order. Additionally, biochemical markers are not fetus-specific, and therefore the abnormality from one fetus may be masked by the normal fetus and vice versa.
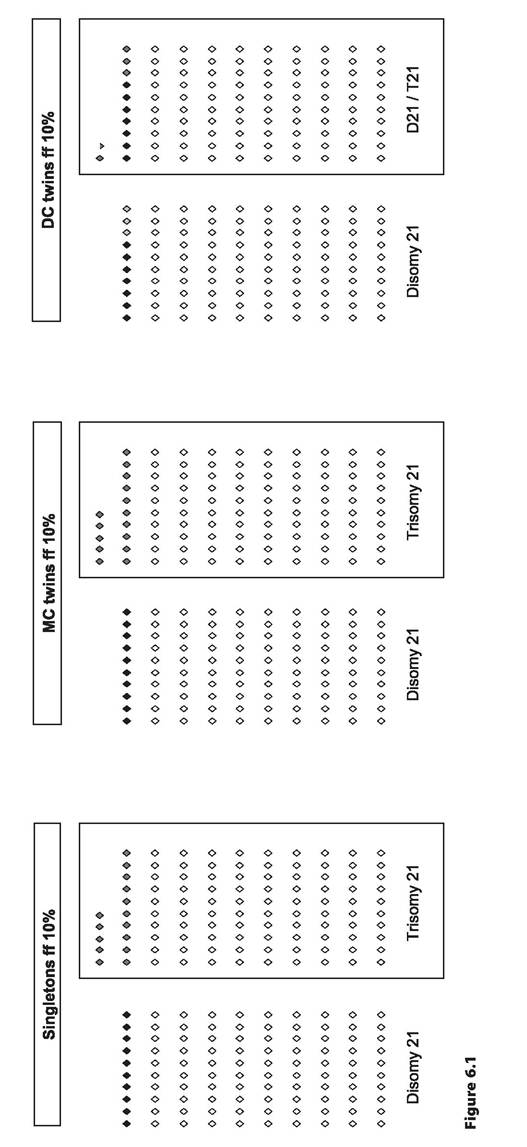
In cfDNA testing, the ability to detect a small increase in the amount of a given chromosome in maternal plasma in a trisomic compared to a disomic pregnancy is directly related to the proportion of the fetal to maternal origin of the cfDNA.
This proportion of cfDNA from the fetus in the mother's bloodstream is known as fetal fraction. When the fetal fraction is low, it is more difficult to discriminate between aneuploid and euploid pregnancies. In twin pregnancies, cfDNA testing is more complex than in singleton pregnancies because the two fetuses could be either monozygotic, which are therefore genetically identical, or dizygotic, in which case only one fetus is likely to have the aneuploidy when present. When performing analysis of cfDNA in maternal blood in dizygotic twins, each fetus contributes different amounts of cfDNA into the maternal circulation, which could vary by nearly twofold.7 It is therefore possible that in a dizygotic twin pregnancy discordant for aneuploidy, the fetal fraction of the affected fetus is below the minimal threshold (normally about 4%) required for successful testing. This could lead to an erroneous result of low risk for aneuploidy because a high contribution from the disomic co-twin could result in a satisfactory total fetal fraction (Figure 6.1). This phenomenon would happen more frequently in multiple pregnancies of increasing order. To avoid this potential error, two strategies have been proposed: first, to determine the fetal fraction for each twin and to use the lowest of the two for risk estimation, and, second, to increase the fetal fraction threshold for reporting a result - that is, from 4% to 8%. However, these approaches will inevitably lead to a higher proportion of tests that will not yield a result. Although the number of affected cases evaluated is significantly lower than that for singletons, performance of cfDNA testing for trisomy 21 in twin pregnancies is similar to that in singletons.7 However, there are insufficient data to accurately report the performance of the test for conditions other than trisomy 21 or for multiple pregnancies of order three or higher.The Management Options
A summary of screening performance for trisomy 21 of each screening method in twin pregnancies is provided in Table 6.1.
Screening by Maternal Age
When defining a risk cut-off for screening of aneuploidies, we must always state when that probability refers to. Since the rate of fetal death between 12 weeks of gestation and term is about 30% for trisomy 21, 80% for trisomies 18 and 13 and only 1-2% for euploid fetuses, the risk for trisomies decreases with gestation and the risk cut-off will vary depending on when the risk assessment is performed.8 For example, in screening for aneuploidies by maternal age, the estimated risks for fetal trisomies 21, 18 and 13 for a woman aged 20 years at 12 weeks of gestation are about 1 in 1,000,1 in 2,500 and 1 in 8,000, respectively, whereas the risks of such woman delivering an affected baby at term are 1 in 1,500,1 in 18,000 and 1 in 42,000, respectively. Conversely, the respective risks for these aneuploidies for a 35-year- old woman at 12 weeks of gestation are about 1 in 250,1 in 600 and 1 in 1,800, and the risks of delivering an affected baby at term are 1 in 350, 1 in 4,000 and 1 in 10,000. Monosomy X (45,X) has a prevalence of about 1 in 1,500 at 12 weeks and 1 in 4,000 at 40 weeks and is not related to maternal age. Other sex chromosome aneuploidies (47,XXX, 47,XXY and 47,
Table 6.1 Performance of different methods of screening for trisomy 21
| Method of screening | Detection rate | False positive rate |
| Maternal age | 40 | 65 |
| Maternal age + fetal NT | 75-80 | 8 |
| First-trimester combined test | 90 | 6 (DC), 9 (MC) |
| Quadruple test | 45 | 5 |
| Cell free DNA test | > 99 | 0.05 |
NT: nuchaltranslucency; DC: dichorionic; MC: monochorionic
https://doi.org/10.1017/9781108915038.006 Published online by Cambridge University Press
XYY) have the same rate of fetal death as euploid fetuses and therefore their overall prevalence (about 1 in 500) does not decrease with gestation and also it does not significantly change with maternal age.
Finally, triploidy is unrelated to maternal age and has a prevalence of about 1 in 2,000 but, because most of the affected fetuses die by 20 weeks, it is rarely seen in live births.Unlike with singletons, there is little direct information on the prior maternal agespecific risk in twins and almost non-existent information in multiple pregnancies of higher order. If the risk of trisomy 21 for each fetus was completely independent of the risk of the other(s), the risk that at least one fetus is affected in a twin pregnancy would be double than in a singleton pregnancy. Actually, the risk is somewhat less than double (about 1.6) for two reasons: first, monozygotic pregnancies are concordant for the aneuploidy, and second, because NT measurements in euploid twins are somehow correlated even after accounting for the sonographer.9
In monochorionic pregnancies where both fetuses are assumed to be genetically identical, the prior risk for aneuploidies for the whole pregnancy according to maternal age is the same as in singleton pregnancies. In dichorionic twins, it has been estimated by modelling charts that the traditional threshold of 35 years used to define the high-risk group by maternal age alone (risk cut-off: 1 in 250 at 12 weeks of gestation) in singleton pregnancies corresponds to 31-33-year-olds in a dichorionic twin pregnancy (Table 6.2). The same rationale applies to multiple pregnancies of higher order.
However, screening for aneuploidies based on maternal age alone in multiple pregnancies should be discouraged for several reasons: first, lowering the cut-off to define the high- risk group in addition to a higher proportion of elderly women in this group of patients would inevitably lead to a disproportionally increased screened positive rate of about 65%. Second, there is a higher miscarriage rate related to invasive diagnostic procedures in these pregnancies, and therefore the aim should be to reduce the screen positive rate. Third, the observed incidence of trisomy 21 in twin pregnancies is lower than that predicted by theoretical models, and therefore it is likely that these figures are overestimating the risk.10
Screening by Nuchal Translucency
Chorionic villus sampling for fetal karyotyping is the preferred method for prenatal diagnosis in singleton pregnancies due to the advantages of early diagnosis and early selective termination of pregnancy as an option. However, although the risk of miscarriage following CVS in twin pregnancies is not higher than that of amniocentesis, in about 5% of cases, it may be unclear whether the same placenta has been sampled and hence it may be argued that the best method for fetal karyotyping is amniocentesis. However, it must be kept in mind that cytogenetic results from amniocentesis may not be available until 18-20 weeks, when the risk of miscarriage of performing a selective feticide is about three times higher than if it is performed before 16 weeks. Therefore, there must be a proper and early risk assessment to help select the most appropriate invasive diagnostic procedure according to the likelihood of ending requiring a selective termination of pregnancy. In this respect, screening by fetal nuchal translucency in the first trimester provided a major step in the management of fetal aneuploidies in multiple pregnancies.
In multiple pregnancies, effective screening for chromosomal abnormalities is provided by a combination of maternal age and fetal NT thickness. The optimal time for measuring NT thickness is between 11+0 and 13+6 weeks of gestation, when the fetal crown-rump
Table 6.2 Riskfor trisomy 21 in singleton pregnancies at 12 weeks of gestation and risk estimates of the same risk for both, monochorionic and dichorionic twin pregnancies
| Maternal age (years) | Risk for trisomy 21 in singletons and MC twins (1 in X) | Risk for trisomy 21 in DC twins (1 in X) |
| 20 | 1,068 | 534 |
| 25 | 946 | 483 |
| 30 | 626 | 313 |
| 31 | 544 | 272 |
| 32 | 460 | 230 |
| 33 | 380 | 190 |
| 34 | 312 | 156 |
| 35 | 250 | 125 |
| 36 | 200 | 100 |
| 37 | 150 | 75 |
| 38 | 118 | 59 |
| 39 | 90 | 45 |
| 40 | 68 | 34 |
| 41 | 50 | 25 |
| 42 | 38 | bgcolor=white>19|
| 43 | 30 | 15 |
| 44 | 20 | 10 |
| 45 | 16 | 8 |
DC: dichorionic; MC: monochorionic
length ranges from 45 to 84 mm. Fetal NT thickness increases with crown-rump length and a measurement above the 95th centile detects about 75-80% of trisomy 21 fetuses in both singleton and multiple pregnancies.3,8 Furthermore, NT thickness is independent of maternal age; therefore, data from these two parameters can be combined, increasing DR of trisomy 21 to 80-85% at an FPR of 5% in singletons, while the same DR can be achieved in twins at the expense of a higher FPR of about 8%, likely as a consequence of fetal heart failure of the recipient in monochorionic pregnancies complicated by early twin-twin transfusion syndrome.3,6,8 Because neither serum biomarkers nor cfDNA testing can be used in multiple pregnancies of order three or higher, screening by a combination of fetal NT thickness and maternal age is the preferred method for screening of trisomy 21 in these pregnancies.
Screening by First-Trimester Combined Test
Performance of screening by fetal NT thickness and maternal age in the first trimester can be improved by the addition of maternal serum biochemistry when appropriate adjustments for chorionicity are performed. At 11+0 to 13+6 weeks, the levels of maternal serum-free β- hCG and PAPP-A in dichorionic pregnancies are twice as high as in singleton pregnancies.4-6 In monochorionic twins, these levels are also higher than in singletons but lower than in dichorionic twins.4-6 The use of serum biomarkers has not been validated in multiple pregnancies of order three or higher.
The addition of likelihood ratios for PAPP-A and free β-hCG to risk assessment by maternal age and fetal NT in dichorionic twins increases the DR for fetal trisomy 21 up to 90% and decreases the FPR from approximately 8% to 6%, which is similar than the screening performance of the first-trimester combined test in singletons.6,11 However, there appears to be no improvement in the DR of fetal aneuploidy in monochorionic twins, which is about 85-90% for trisomy 21, nor in the FPR, which remains around 9%, by the addition of biochemical markers.6
In monochorionic twins, risks for trisomy 21 are calculated for each fetus using maternal age, fetal NT thickness and crown-rump length and serum levels of free β-hCG and PAPP- A corrected by chorionicity. Then the average of the two risks is calculated to estimate the overall pregnancy risk. However, in dichorionic twins, risks for trisomy 21 are calculated in the same way but provided for each fetus separately. It can be assumed that the two fetuses are independent or, alternatively, the correlation in NT measurements between fetuses can be taken into account for the risk calculation.8,9 This measure may not have a significant impact on the overall performance of screening, but it does have a substantial impact on the estimated patient-specific risk.9
Screening by Second-Trimester Serum Biomarkers
Several second-trimester serum biomarkers have been incorporated to improve DR of screening for trisomy 21 by maternal age alone from 14 weeks of gestation onwards. In singleton pregnancies, at a fixed FPR of 5%, the DR by combining maternal age with serum alpha fetoprotein and free β-hCG (double test) is about 60-65%. With the addition of unconjugated estriol (triple test), it is about 65-70%, and with the addition of inhibin A (quadruple test), it is about 70-75%. However, in twin pregnancies, the maximum DR that can be achieved by this method is only about 45-50% at the same FPR of 5%.12
One limitation of screening for trisomy 21 by serum biomarkers alone in twins is that the pregnancy is classified as high risk as a whole without any indication of which fetus may be the affected one, unlike ultrasound markers, which are fetus-specific. This method is not validated for pregnancies of order three or higher, and for twin pregnancies, it would only be recommended when other screening methods with higher performance are not available.
Screening by Cell-Free DNA Testing
Analysis of cfDNA testing in maternal blood for screening of aneuploidies should not be performed before 10 weeks of gestation to ensure accurate results, without an upper limit for testing. Several clinical validation and implementation studies have been published, and this method is currently recommended either as first-line screening or as contingent screening following the results from a previously performed screening method.
Performance of cfDNA testing for trisomy 21 in twin pregnancies is similar to that reported in singleton pregnancies, showing a DR of about 98% and an FPR of 0.05%.7 Although the number of cases reported in the literature is still insufficient to properly evaluate performance of cfDNA screening for trisomy 18, DR and FPR are about 90% and 0.03%, respectively.7 The use of cfDNA testing for screening of other aneuploidies or genetic conditions is currently not validated and therefore not recommended.
Despite its good performance, cfDNA testing remains as a screening test, which means that a high-risk result requires confirmation by invasive testing and that a negative result, although reassuring, does not mean that the pregnancy is certainly not affected.
The two main concerns when screening for trisomy 21 by cfDNA testing in twin pregnancies relate to, first, the limited available data and, second, to the increased rate of tests that do not yield a result (no-result rate) in dichorionic twins as compared to singletons (5% versus 1% after second testing).13 One of the main reasons for this increased no-result rate in dichorionic twins is directly related to twinning and the necessity of being very conservative with the minimal fetal fraction required in order to ensure accurate results. However, another risk factor for an increased no-result rate that has been repeatedly associated with a lower fetal fraction and therefore to an increased no-result rate is the use of assisted reproductive techniques for pregnancy conception, something which is far more frequent in twin than in singleton pregnancies.13 Other risk factors for not obtaining a result after testing are increasing maternal weight, nulliparity, certain ethnic origins, like Afro-Caribbean or South Asian, and factors related to a smaller placental size, like earlier gestational age or low serum levels of free β-hCG and PAPP-A.13 Likewise, aneuploidies related to a small placenta, such as trisomies 18 and 13 and digynic triploidy but not trisomy 21, have a lower fetal fraction, and therefore they are also associated with an increased noresult rate. Therefore, when a result is not obtained from cfDNA testing, careful ultrasound assessment of the fetal anatomy must be carried out in order to rule out the presence of any structural defects related to any of the aforementioned conditions; if those are excluded, repeating the test is a sensible management option, and a result will be obtained in the second draw in about 50% of cases.13 In those cases where a result is not reported after second testing, other risk factors or screening tests must be considered to help decide if an invasive diagnostic testing is advisable (Figure 6.2). Therefore, pretest counselling should not only include DR and FPR but also the no-result rate since it is a component of the test screening performance.
“No result" from cf DNA test at first sampling
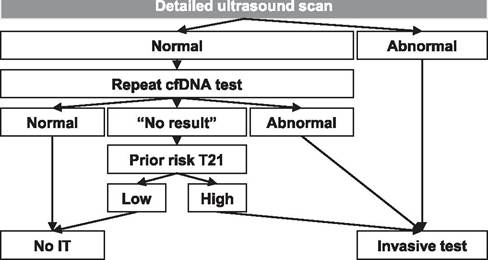
Figure 6.2 Management algorithm if cfDNA test yields 'no-result'
Although it has been tested in triplets, cfDNA screening has not been validated for pregnancies of order three or higher. As for serum biomarkers, it has the disadvantage of not being fetusspecific, and therefore, the results are provided for the whole pregnancy without any information on which can be the affected fetus. Consequently, it is recommended that cfDNA testing is always accompanied by a comprehensive ultrasound assessment.
Screening of Aneuploidies in the Presence of a Vanishing Twin
The presence of a vanishing twin may complicate screening using maternal serum biomarkers or cfDNA testing since placental products from the interrupted pregnancy are present in the maternal bloodstream for several weeks.
Although it was generally recommended not to use serum biomarkers when there is a measurable fetal pole,14 it has been recently reported that, unlike PAPP-A levels, which are always increased in vanishing twin pregnancies even if only an empty sac is visible, free β-hCG levels are not significantly different from those in normal singleton pregnancies, regardless of when the fetal demise occurred.15 This knowledge may allow performing first- trimester screening by combining maternal age, fetal NT thickness and free β-hCG in these pregnancies, increasing DR from 80% to 85% as compared to screening by maternal age and NT alone, both at 5% FPR.15
The cfDNA testing should not be performed in vanishing twin pregnancies because of flooding of cfDNA into the maternal plasma from the necrotic cytotrophoblasts, which may persist for at least 15 weeks after fetal demise. This persisting cfDNA from the vanishing twin in the maternal circulation may reduce DR and increase false positive and no-result rates.
Key Points
• For monochorionic pregnancies, an overall risk assessment is provided for the entire pregnancy, while for dichorionic (or higher chorionicity order) a specific risk is provided for each fetus.
• In monochorionic pregnancies, the risk of aneuploidy appears similar to the risk in singleton pregnancies; in dizygotic pregnancies, the chance that at least one fetus is affected by a chromosomal defect is about twice as high as in singleton pregnancies.
• Screening by a combination of maternal age and fetal NT thickness in multiple pregnancies shows a similar DR to that in singleton pregnancies, of about 80-85%, but at a higher FPR with higher number of fetuses. This is the recommended method for multiple pregnancies of order three or higher.
• First-trimester combined tests in twins show a similar detection rate to singletons of about 90%, but at a higher FPR, of 6% for dichorionic twins and 9% for monochorionic twins. It is not possible to screen multiple pregnancies of order three or higher by this method.
• Screening for trisomy 21 in twins by the second-trimester quadruple test will only achieve a DR of about 45% at a 5% false positive rate. It is not possible to screen multiple pregnancies of order three or higher by this method.
• Analysis of cfDNA in maternal blood for screening of trisomy 21 in twin pregnancies achieves similar performance to singleton pregnancies, showing a DR of 98% at FPR of 0.05%. Data are limited for other aneuploidies and genetic conditions as well as for multiple pregnancies of order three or higher.
• In the presence of a vanishing twin with a measurable fetal pole it is recommended to screen by maternal age and fetal NT thickness (+/- free β-hCG) since contamination of maternal blood by placental products from the interrupted pregnancy may affect serum biomarkers levels and cfDNA analysis.
References
1. Santorum M, Wright D, Syngelaki A, Karagioti N, Nicolaides KH. Accuracy of first-trimester combined test in screening for trisomies 21, 18 and 13. Ultrasound Obstet Gynecol 2017;49:714-20.
2. Gil MM, Accurti V, Santacruz B, Plana MN, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: updated meta-analysis. Ultrasound Obstet Gynecol 2017;50:302-14.
3. Sebire NJ, Snijders RJ, Hughes K, Sepulveda W, Nicolaides KH. Screening for trisomy 21 in twin pregnancies by maternal age and fetal nuchal translucency thickness at 10-14 weeks of gestation. Br J Obstet Gynaecol 1996;103:999-1003.
4. Spencer K. Screening for trisomy 21 in twin pregnancies in the first trimester using free beta-hCG and PAPP-A combined with fetal nuchal translucency thickness. Prenat Diagn 2000;20:91-5.
5. Spencer K, Kagan KO, Nicolaides KH. Screening for trisomy 21 in twin pregnancies in the first trimester: an update of the impact of chorionicity on maternal serum markers. Prenat Diagn 2008;28:49-52.
6. Madsen HN, Ball S, Wright D et al.
A reassessment of biochemical marker distributions in trisomy 21-affected and unaffected twin pregnancies in the first trimester. Ultrasound Obstet Gynecol 2011;37:38-47.
7. Gil MM, Galeva S, Jani J et al. Screening for trisomies by cfDNA testing of maternal blood in twin pregnancy: update of the Fetal Medicine Foundation results and meta-analysis. Ultrasound Obstet Gynecol 2019;53:734-42.
8. Nicolaides KH. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat Diagn 2011;31:7-15.
9. Wright D, Syngelaki A, Staboulidou I, Cruz J, Nicolaides KH. Screening for
trisomies in dichorionic twins by measurement of fetal nuchal translucency thickness according to the mixture model. Prenat Diagn 2011;31:16-21.
10. Audibert F, Gagnon A, Genetics Committee of the Society of Obstetricians and Gynaecologists of Canada, Prenatal Diagnosis Committee of the Canadian College of Medical Geneticists. Prenatal screening for and diagnosis of aneuploidy in twin pregnancies. J Obstet Gynaecol Can 2011;33:754-67.
11. Prats P, Rodriguez I, Comas C, Puerto B. Systematic review of screening for trisomy 21 in twin pregnancies in first trimester combining nuchal translucency and biochemical markers: a meta-analysis. Prenat Diagn 2014;34:1077-83.
12. Cuckle H. Down's syndrome screening in twins. J Med Screen. 1998;5:3-4.
13. Galeva S, Gil MM, Konstantinidou L, Akolekar R, Nicolaides KH. First- trimester screening for trisomies by cfDNA testing of maternal blood in singleton and twin pregnancies: factors affecting test failure. Ultrasound Obstet Gynecol 2019;53:804-9.
14. Khalil A, Rodgers M, Baschat A et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol. 2016 Feb;47(2):247-63. doi: 10.1002/ uog.15821. Erratum in Ultrasound Obstet Gynecol. 2018 Jul;52(1):140. PMID: 26577371.
15. Chaveeva P, Wright A, Syngelaki A, Konstantinidou L, Wright D, Nicolaides KH. First-trimester screening for trisomies in pregnancies with vanishing twin.Ultrasound Obstet Gynecol. 2020 Mar;55(3):326-31. doi: 10.1002∕uog.21922. Epub 2020 Feb 13. PMID: 31710734.