Obstetric Anaesthesia in Multiple Pregnancy
Tarek Ansari
Introduction
Multiple pregnancy is associated with an increased risk of maternal and fetal morbidity and mortality. A successful outcome requires a multidisciplinary approach involving obstetricians, neonatologists, obstetric anaesthetists and midwives.
The obstetric anaesthetist may be involved in antenatal assessment, care planning and counselling of parturients with multiple gestation. This is particularly important in pregnant women with medical comorbidities associated with special care needs and increased risk of perinatal complications or adverse outcomes. In twin vaginal delivery, effective epidural in labour is crucial for adequate analgesia, but it may also increase the chances of successful delivery of the second twin. Providing safe and effective spinal anaesthesia, or general anaesthesia when indicated, for caesarean delivery is essential. A multimodal approach to postoperative analgesia enables enhanced recovery and early discharge after caesarean section. The role of the anaesthetist is crucial in managing critically ill pregnant women including those with pre-eclampsia and its complications. This chapter covers the anaesthetist’s role in the context of multiple pregnancy.Maternal Physiological Changes in Multiple Gestation
The maternal physiological adaptation to multiple gestation is far more exaggerated than that of singleton pregnancies. Twin gestation is associated with significantly higher cardiac output than singleton pregnancy due to the increase in both stroke volume and heart rate. By 20 weeks of gestation the blood volume in twin pregnancy increases by 50-70% compared to 20% in singleton pregnancy. This is reflected in increased left atrial diameter and left ventricular end-diastolic diameter, indicating a rise in the cardiac preload in twin pregnancy. In contrast to the increase in blood volume, twin pregnancy is associated with only a 25% increase in erythrocyte volume, which leads to haemodilution anaemia, a decrease in albumin and water-soluble vitamin concentration.
Increased uterine size in multiple gestation, particularly in the third trimester, leads to reduction in total lung capacity and functional residual capacity. This predisposes to a more rapid development of hypoxemia after a brief period of apnoea. After 30 weeks of gestation, women with multiple pregnancies have an increased tendency for weight gain. The large size of the uterus displaces the stomach and reduces the competency of the lower oesophageal sphincter, increasing the risk of passive regurgitation of stomach contents. These changes combine to significantly increase the risk of difficult intubation and pulmonary aspiration during general anaesthesia for women with multiple gestation.
Risk of Maternal Morbidity and Mortality in Multiple Gestation The risk of severe maternal morbidity in multiple pregnancies is 28 per 1,000 deliveries, while that of singleton pregnancies is 6.5 in 100,000 deliveries. Higher-order gestation further increases the risk. The relative risk of severe maternal morbidity compared to singleton pregnancy is 4.3 in twins and 6.2 in triplets. The risk of morbidity increases with a maternal age of more than 40 years, the use of assisted reproductive technology and non-spontaneous onset of labour.1 This increased risk necessitates the involvement of the obstetric anaesthetist as part of the multidisciplinary team, including where high- dependency or intensive care is required, to optimise outcome.
Pre-eclampsia
Pre-eclampsia remains a leading cause of maternal morbidity and mortality. Twin pregnancy doubles the risk of pre-eclampsia compared to singleton pregnancy. The larger placental volume in multiple gestation may be partly responsible for this association. Multiple gestation resulting from assisted reproductive technology carries twice the risk of pre-eclampsia compared to spontaneous twin conception. Pre-eclampsia develops earlier in multiple gestation and is often more severe. The risk of developing haemolysis, elevated liver enzymes and low platelets (HELLP) syndrome is four times higher than in singleton pregnancy.2
The anaesthetic management of pre-eclampsia may include neuraxial block for vaginal delivery or caesarean section.
Severe generalised oedema over the lower back may increase the technical difficulty of spinal or epidural anaesthesia. If general anaesthesia is required for caesarean section, airway oedema may significantly increase the risk of difficult intubation. Uncontrolled hypertension may predispose to the increased risk of cerebrovascular accidents during general anaesthesia and endotracheal intubation. The role of the anaesthetist is crucial in the critical care management of parturients with fulminating pre-eclampsia. This may include invasive monitoring, control of hypertension and the management of cardiorespiratory, cerebral and renal complications.3Post-partum Haemorrhage
The risk of post-partum haemorrhage in multiple gestation is two to four times that of singleton pregnancy. Contributing factors may include greater uterine distension that predisposes to uterine atony, increased maternal blood volume and uterine blood flow. The use of tocolytic agents during vaginal twin delivery, placenta praevia and placental abruption further increase the risk.
Women with multiple gestation are more likely to suffer from iron-deficiency anaemia and are at greater risk of requiring blood transfusion. A multivariable logistic regression model identified a low platelet count (< 100,000/ microliter), haematocrit < 30% and general anaesthesia as predictors of post-partum haemorrhage requiring blood transfusion in women with twin pregnancies.4 The anaesthetist is fundamental during the management of post-partum haemorrhage, taking the lead in cardiovascular resuscitation and replacement of blood products.
Risk of Fetal Complications
Multiple gestation is associated with a significant increase in the risk of perinatal morbidity and mortality. The perinatal mortality rate is two and a half times higher in twin pregnancy, while that of triplet pregnancy is five times higher than that of singleton pregnancy.
In all dizygotic twins (two separate fertilised ova) the placenta is dichorionic and diamniotic, while in monozygotic twins (single fertilised ovum, dividing into two distinct individuals) the placenta can be monochorionic or dichorionic, depending on the time of embryonic cleavage.
Seventy-five per cent of monozygotic twins are monochorionic and diamniotic. Vascular communications occur in almost all monochorionic placentas and may result in fetal complications such as twin-twin transfusion syndrome and intrauterine fetal death (IUFD). Other fetal complications associated with multiple gestation include preterm labour, congenital anomalies, polyhydramnios, fetal growth restriction and multiple presentation.Twin-Twin Transfusion
Monochorionic twins with deep arterio-venous vascular anastomosis may suffer from twintwin transfusion. The donor twin will be at risk of fetal growth restriction and anaemia, while the recipient twin will be at risk of polycythaemia, polyuria, polyhydramnios, fetal hydrops and hypertrophic cardiomyopathy. Twin-twin transfusion can be managed by amnioreduction, amniotic septostomy or selective fetoscopic laser photocoagulation (SFLP). Selective fetoscopic laser photocoagulation is associated with the highest birth survival rate, with 62% mean survival rate for both twins and 88% for at least one twin.
Anaesthesia for SFLP procedures can be provided by local anaesthetic infiltration of the anterior abdominal wall. This is usually sufficient to reduce maternal discomfort; however, supplemental analgesia or sedation can be provided using a short-term opioid such as fentanyl or a hypnotic such as midazolam. A low-dose propofol infusion can also be used for sedation. Neuraxial block is occasionally used but general anaesthesia is rarely needed. When providing neuraxial block it in this clinical scenario, it is essential to avoid maternal hypotension as the compromised fetuses are cardiovascularly unstable and very sensitive to placental hypoperfusion, which may result in fetal death. General anaesthesia where the woman is intubated and ventilated is not ideal because the deep breathing movement results in exaggerated movement of the uterus and placenta and makes accurate visualisation of anastomoses and laser coagulation technically difficult.
As with other anaesthesia for non- obstetric surgery, the anaesthetist should perform a full preoperative anaesthetic assessment and decide with the mother and the surgeon on the most appropriate anaesthetic technique.Fetal hydrops secondary to twin-twin transfusion may be associated with a rare but potentially life-threatening maternal complication. Mirror syndrome is diagnosed when maternal and placental oedema develop secondary to fetal hydrops. Other causes of mirror syndrome include Rh-isoimmunisation, intrauterine infection or placental tumours. Patients with mirror syndrome will present with severe generalised oedema, ascites and pulmonary oedema. It can be associated with elevation of blood pressure and proteinuria, mimicking pre-eclampsia. The definitive treatment of mirror syndrome is the delivery of the fetus and placenta. In cases of twin-twin transfusion syndrome, resolution of the maternal signs and symptoms can be achieved by artificial feticide or fetoscopic laser photocoagulation. The anaesthetic management of mirror syndrome is similar to that of severe pre- eclampsia.3
Delivery of Women with Multiple Gestation
The overall rate of caesarean section for twin delivery is 75%, while the caesarean delivery rate for twins with a cephalic presenting first twin is 68%. The term breech trial published in 2000 concluded that planned caesarean section for breech presentation in singleton pregnancy reduces the risk of perinatal mortality and serious morbidity by threefold.5 This study had a profound impact on obstetric practice. The almost unanimous and universal acceptance of its results meant most obstetricians completely abandoned planned vaginal breech delivery in favour of caesarean section. This also resulted in a general consensus that twin pregnancies where the first twin's presentation is breech should be delivered by caesarean section. However, the extrapolation of the term breech trial findings to twin pregnancies with a cephalic presenting first twin and a non-vertex presenting second twin led to a progressive increase in caesarean section rate for all twin deliveries.
In 2013 the first large randomised controlled multicentre study on the mode of delivery for twin pregnancy with a cephalic presenting first twin (Twin Birth Study) was published. The study found that in twin pregnancies between 32 and 38+6 weeks of gestation there was no significant difference in fetal or neonatal outcome between planned vaginal delivery and planned caesarean section.6The recent guidelines from the National Institute for Health and Care Excellence (NICE) recommend that planned vaginal delivery should be offered to women with uncomplicated dichorionic-diamniotic or monochorionic-diamniotic twin pregnancies if the presentation of the first twin is cephalic and there is no significant size discordance between the twins.7 Planned caesarean section is indicated for the following: monoamniotic twin pregnancies, non-cephalic presentation of the first twin at the time of planned birth, triplets and higher- order pregnancies
Planned Vaginal Delivery
Women with a twin pregnancy are at increased risk of intervention in labour, particularly for the delivery of the second twin. This may include external cephalic version, internal podalic version and total breech extraction, instrumental vaginal cephalic delivery or emergency caesarean section.
In the Twin Birth Study 43.8% of women in the planned vaginal delivery group had emergency caesarean sections during labour and 4.2% had an emergency section for delivery of the second twin.6 Only 30% of women in the planned vaginal delivery group had epidural analgesia in labour.
In a retrospective cohort study comparing outcomes of twin pregnancies with planned vaginal delivery and active second-stage management to the outcomes of planned caesarean delivery, all women in the planned vaginal delivery group had epidural analgesia: 15.4 % had emergency caesarean sections for both twins, while 84.6% delivered both twins vaginally. None of the women had emergency caesarean sections for the delivery of the second twin. All deliveries took place in the operating theatre with the anaesthesiologist in attendance.8
Despite the paucity of evidence on the effect of epidural analgesia on the outcome of vaginal twin delivery, the consensus is that effective labour analgesia would facilitate prompt delivery of the second twin in an emergency, reducing the risk of fetal or neonatal morbidity and mortality. The recent NICE guidelines recommended offering epidural analgesia to all women with a twin or triplet pregnancy who choose to have a vaginal birth. By providing better analgesia and relaxation of the abdominal wall and pelvic floor muscles, an effective epidural increases the chances of success for internal podalic version and total breech extraction of the second twin. If further uterine relaxation is required to facilitate the delivery of the second twin, a tocolytic agent such as nitroglycerine can be given intravenously in a dose of 150-250 micrograms.
A combination of excessive weight gain and large uterine size in multiple gestation might lead to difficulty in identifying anatomical landmarks and in positioning the mother for epidural catheter placement. The use of a pre-procedure ultrasound to guide epidural catheter insertion was shown to double the first attempt success rate compared to the traditional landmark technique in obese patients or those with difficult backs. It is postulated that identifying the depth of the dura using ultrasound may reduce the risk of accidental dural puncture and post-dural puncture headache. Applying a low-frequency curvilinear ultrasound probe using the longitudinal paramedian sagittal approach, followed by the transverse midline interspinous approach, provides information that allows the anaesthetist to determine the level of the desired intervertebral space and the optimum puncture site. It also helps to determine the depth of the dura and the best angle for the needle approach.9 See Figures 31.1 and 31.2.
Successful management of vaginal twin delivery relies on the presence of an experienced obstetrician skilled and comfortable with the active management of the second stage of labour. This may include internal podalic version and total breech extraction. Other essential elements include continuous fetal monitoring and routine epidural analgesia. Performing twin vaginal delivery in the operating theatre with the anaesthesiologist in attendance is routine in some centres but not a universal practice. The anaesthesiolo- gist should ensure that the epidural catheter is working effectively, and in case of any doubt, should have a low threshold for re-siting the catheter. The combination of a low- dose local anaesthetic and a lipophilic narcotic (such as ropivacaine 0.1% plus fentanyl 0.2%) is routinely used to provide effective epidural analgesia with minimal motor block. Prompt conversion of epidural analgesia into surgical anaesthesia is an essential skill to reduce the need for general anaesthesia in case of emergency caesarean section. This can be achieved using 15-20 mls of lidocaine 2% with epinephrine 1/200,000 to extend the surgical sensory block up to T4 dermatome. Every effort should be made to ensure that
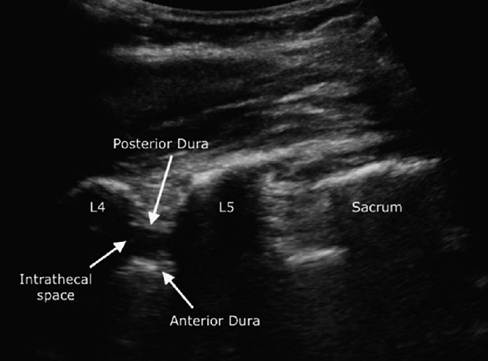
Figure 31.1 Ultrasound-guided neuraxialscan. Paramedian Sagittaloblique approach
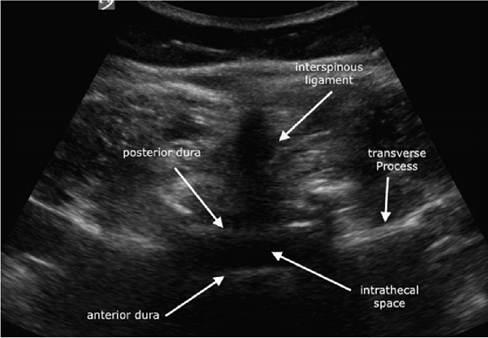
Figure 31.2 Ultrasoundguided neuraxialscan. Transverse interspinous approach
the epidural top-up produces adequate surgical anaesthesia before the start of surgery. If the epidural top-up fails, a spinal or a general anaesthetic can be administered depending on the urgency of the caesarean section. Predictors for failed conversion of epidural analgesia to epidural anaesthesia include the degree of urgency of caesarean section, the need for frequent epidural top-ups during labour and the experience of the anaesthesi- ologist. Effective team communication between obstetricians, anaesthesiologists and midwives can help in anticipating the need for intra-partum caesarean delivery, allowing sufficient time to achieve epidural anaesthesia. A retrospective study found that 44% of general anaesthesia for caesarean section can be avoided and that a low hospital use of labour epidural analgesia is a strong predictor of potentially avoidable use of general anaesthesia for caesarean section.10
General anaesthesia for emergency caesarean section is associated with increased risk of maternal complications such as difficult intubation, regurgitation and pulmonary aspiration of gastric contents and intraoperative awareness. It is also associated with an increased risk for post-partum haemorrhage, surgical site infection and deep vein thrombosis. On the other hand, neuraxial anaesthesia-induced sympathetic blockade leads to attenuation of the inflammatory response to surgery. The associated peripheral vasodilatation improves tissue perfusion and oxygenation, reducing the risk of infection and thromboembolism.
The use of interdisciplinary simulation of vaginal twin delivery is essential in reducing maternal and neonatal risk and ensuring an optimum outcome. Team training in internal podalic version, breech extraction and emergency caesarean section may help optimise team dynamics and enhance timely and effective communication between obstetricians, midwives and anaesthesiologists in a challenging and time-sensitive scenario. This may lead to a reduction in avoidable intra-partum caesarean section and general anaesthesia.11
Anaesthesia for Caesarean Delivery
Forty years ago the risk of maternal mortality from general anaesthesia for caesarean section was 17 times greater than that from neuraxial anaesthesia. Nowadays the case fatality rates of general and neuraxial anaesthesia in obstetrics have converged to become statistically indistinguishable. However, it was shown that in the first post-operative week after caesarean section patients who had neuraxial anaesthesia had less pain, gastrointestinal stasis, coughing and fever than patients who received general anaesthesia. Women were also able to ambulate earlier and were less likely to experience breastfeeding difficulties. It was recently shown that general anaesthesia for caesarean section increases the odds of postpartum depression by 54%.
In the absence of contraindications, neuraxial anaesthesia, in particular single-shot spinal anaesthesia, is currently the default technique for caesarean section. It is estimated that on average only 5% of elective caesarean sections and 15% of emergency caesarean sections are performed under general anaesthesia. Spinal anaesthesia is achieved using a combination of hyperbaric bupivacaine 0.5% and a lipid-soluble opioid such as fentanyl 20 micrograms. It was believed that women with multiple gestation were more susceptible to spinal-induced hypotension than women with singleton gestation due to the larger uterine size. Similarly, it was thought that they were more likely to have a higher cephalad spread of sensory and motor blockade with spinal anaesthesia. However, several studies concluded that there is no difference in the effect of spinal anaesthesia in both groups of women. Spinal-induced hypotension, secondary to sympathetic blockade, can be successfully prevented using a combination of an infusion of a directly acting vasopressor (phenylephrine) and a rapid intravenous administration of Lactated Ringer's solution immediately after the spinal injection (co-loading).12 The phenylephrine infusion can be titrated in order to maintain baseline blood pressure. Compared to the indirectly acting sympathomimetic ephedrine, phenylephrine is associated with lower incidence of maternal nausea, vomiting and tachycardia, and with better neonatal umbilical artery pH and base excess.
Managing Haemorrhage
Multiple gestation is associated with an increased risk of antepartum and post-partum haemorrhage. The rate of placental abruption is two to three times that of singleton pregnancy, while the rate of placenta praevia is 40% higher in twins than in singletons. An over-distended uterus doubles the rate of post-partum haemorrhage secondary to uterine atony. In the Twin Birth Study 6.9% had post-partum haemorrhage, 2.1% with blood loss >/= 1,500 mL, and 5% required blood transfusion (no significant difference between planned vaginal versus planned caesarean birth).6
Adopting an evidence-based massive haemorrhage protocol has been shown to improve maternal outcome. This should include a uterotonic drug cascade with a low threshold to move to the next drug in case of failure to achieve an adequate response. Intravenous oxytocin or carbetocin is usually the default uterotonic. In the absence of contraindications, this is followed by intramuscular methylergometrine and carboprost, then rectal or vaginal misoprostol.
In major obstetric haemorrhage the fibrinogen level was the parameter best correlating with the volume of blood loss. Fibrinogen concentration of less than 2 g/l was found to have a positive predictive value of 100% for severe post-partum haemorrhage, while a level of more than 4 g/l had a negative predictive value of 79%.13 Compared to a fibrinogen level of more than 3 g/l, a fibrinogen level of between 2 and 3 grams, which is usually considered normal, doubles the risk of severe haemorrhage. In the setting of post-partum haemorrhage the anaesthesiologist should assess the fibrinogen level early and initiate its replacement aggressively. Fibrinogen concentrate provides a safe, effective and readily available source of fibrinogen. The use of a point-of-care coagulation monitor such as thromboelastometry can provide valuable information on clot initiation, propagation, clot firmness and stability and fibrinogen function. A thromboelastometry-guided algorithm for post-partum haemorrhage may reduce bleeding and the need for blood and blood-component transfusion.
A large, international, randomised, double-blind, placebo-controlled trial concluded that the early use of tranexamic acid can reduce maternal mortality from post-partum haemorrhage by more than 30% in cases of uterine atony or trauma.14
Historic concerns over the risk of amniotic fluid embolism prevented the use of cell saver in obstetrics. It is now believed that the use of cell saver in obstetrics is safe and can lead to a reduction in the use of allogeneic blood and in the overall number of patients who receive blood or blood-component transfusions. Routine cell saver use for all caesarean section patients is not recommended due to concerns over its cost-effectiveness. However, its use in high-risk obstetrics including multiple gestation is recommended by the American College of Obstetricians and Gynaecologists and the Association of Anaesthetists of Great Britain and Ireland.
Post-caesarean Analgesia
Effective analgesia after caesarean delivery improves patient satisfaction and is an essential element of enhanced recovery. It enables early ambulation, reduces the risk of venous thromboembolism and facilitates breastfeeding. It may also reduce the risk of developing chronic post-operative pain.
The gold standard for post-caesarean section analgesia is a multimodal approach. Multimodal techniques provide efficient analgesia by acting on different levels of the pain pathways to maximise analgesia while limiting side effects. At the centre of this approach lies the use of intrathecal morphine, a lipophilic long-acting opioid. Intrathecal morphine in a dose of 50-100 micrograms provides effective, long-acting analgesia. Side effects include pruritus, nausea and vomiting, urinary retention and rarely respiratory depression. Other components of the multimodel approach are regular or scheduled paracetamol and nonsteroidal anti-inflammatory drugs (NSAID) such as diclofenac or ibuprofen. Both groups of drugs have an opioid-sparing effect of 20% and 50%, respectively. Intramuscular morphine may be used for breakthrough pain.
Abdominal Fascial Plane Blocks
Ultrasound-guided abdominal fascial plane blocks are a relatively recent addition to the elements of multimodal post-operative analgesia for abdominal surgeries including cesarean sections. The most commonly used techniques are transversus abdominis plane block (TAP) and quadratus lumborum block (QLB).
In TAP the local anaesthetic is injected in a fascial plane between the internal oblique and transversus abdominis muscles, blocking the somatic fibres supplying the lower abdominal wall. Although intrathecal morphine provides superior analgesia, TAP block may be used as part of a multimodal post-operative analgesic approach if caesarean delivery is done under general anaesthesia, or when intrathecal morphine is contraindicated.
Quadratus lumborum block is a posterior abdominal wall block that is a modification of TAP block. While the patient is in the supine position with a lateral tilt, a curvilinear ultrasound probe is placed transversely at the midaxillary line above the iliac crest at the
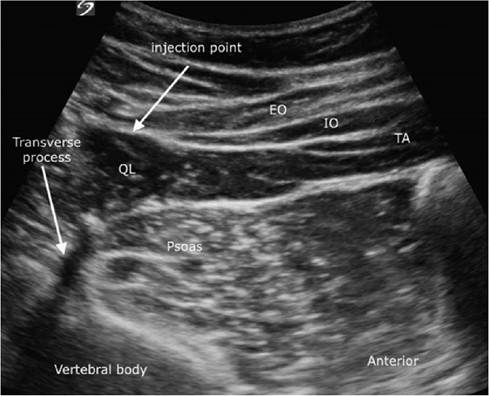
Figure 31.3 Quadratus
Iumborum block. TA: transversus abdominis muscle; IO: internal oblique muscle; EO: external oblique muscle; QL: quadratus lumborum muscle
level of the umbilicus. The quadratus Iumborum muscle (QL) is identified as a hypoechoic muscle posterolateral to the anterior abdominal muscles (external oblique, internal oblique and transversus abdominis) and anteromedial to the psoas major muscle at the tip of the lumbar transverse process. The local anaesthetic is injected under ultrasound guidance at the posterior border of the QL. Although several injection points are proposed for QLB, the posterior approach is the default technique in our institution. We routinely use bupivacaine 0.125% in a dose of 0.4 ml/kg on both sides. After injection the local anaesthetic spreads posteriorly along the thoracolumbar fascia with its network of sympathetic fibres, blocking both somatic and visceral pain. Further spread into the paravertebral space may explain its longer-lasting analgesia effect. Quadratus lumborum block is considered a safer technique than TAP block as the tip of the needle is separated from the peritoneum by the QL, thus reducing the risk of intraperitoneal injection and bowel injury. Compared to TAP block, and as one component of a multimodal approach, QLB seems to offer superior postoperative analgesia with significant reductions in morphine consumption and pain scores. This effect lasts for up to 48 hours after the caesarean section.15 See Figure 31.3.
Key Points
• The rate of multiple gestation is rising exponentially due to increased use of assisted reproductive technology and older maternal age.
• Multiple gestation exaggerates the physiological changes of pregnancy compared to singleton gestation.
• Women with twins and higher-order gestation are at increased risk of maternal and fetal complications such as pre-eclampsia, post-partum haemorrhage, fetal pathology particularly if monochorionic, and intrauterine fetal death.
• Good-quality evidence suggests that in twin pregnancies with a cephalic presenting first twin and a non-vertex presenting second twin there is no significant difference in maternal and neonatal outcome between planned vaginal delivery and planned caesarean delivery.
• Despite the lack of evidence, the general consensus is that epidural analgesia in twin vaginal delivery may facilitate the active management of the second stage of labour and reduce the risk of avoidable general anaesthesia for emergency caesarean section.
• Single-shot spinal anaesthesia remains the preferred technique for caesarean delivery in multiple pregnancy. It is associated with better maternal and neonatal outcomes and reduction of perioperative complications such as post-partum haemorrhage, deep vein thrombosis and surgical site infection.
• An effective multimodal post-caesarean pain management approach should include intrathecal morphine or an abdominal fascial plane block at its core. This enables smooth recovery after caesarean section and facilitates early ambulation and successful breastfeeding.
References
1. Witteveen T, Van den Akker T, Zwart JJ et al. Severe acute maternal morbidity in multiple pregnancies: a nationwide cohort study. Am J Obstet Gynecol 2016;214:641. e1-641.e10.
2. Day MC, Barton JR, O'Brien JM et al. The effect of fetal number on the development of hypertensive conditions of pregnancy. Obstet Gynecol 2005;106:927-31.
3. Xu W, Smith C, Binstock A, Lim G. Maternal mirror syndrome masquerading as congestive heart failure: a case report.
A A Pract 2019;12(11):447-51.
4. Blitz M, Yukhayev A, Patchman S et al. Twin pregnancy and risk of postpartum hemorrhage. J Matern Fetal Neonatal Med 2020. Nov;33(22):3740-5. https://doi.org/ 10.1080/14767058.2019.1583736.Epub 2019 Mar 5.PMID:30836810
5. Hannah ME, Hannah WJ, Hewson S et al. for the Term Breech Trial Collaborative Group. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial.Lancet 2000;356:1375-83.
6. Barrett JF, Hannah ME, Hutton EK et al. for the Twin Birth Study Collaborative Group. A randomized trial of planned cesarean or vaginal birth for twin pregnancies. N Engl
J Med 2013;369:1295-1305.
7. National Institute for Health and Care Excellence. 2019 Twin and triplet pregnancy (NICE guideline 137). Available at www.nice.org.uk/guidance/ng137
8. Fox NS, Silverstein M, Bender S, Klauser CK, Saltzman DH, Rebarber A. Active second-stage management in twin pregnancies undergoing planned vaginal delivery in a U.S. population. Obstet Gynecol 2010;115(2 Pt 1):229-33.
9. Chin KJ, Perlas A. Ultrasonography of the lumbar spine for neuraxial and lumbar plexus blocks. Curr Opin Anaesthesiol 2011 Oct;24(5):567-72.
10. Guglielminotti J, Landau R, Li G. Adverse events and factors associated with potentially avoidable use of general anesthesia in cesarean deliveries. Anesthesiology 2019;130:912-22.
11. Lepage J, Ceccaldi PF, Remini SA, Plaisance P, Voulgaropoulos A, Luton D. Twin vaginal delivery: to maintain skill simulation is required. Eur J Obstet Gynecol Reprod Biol 2019 Mar;234:195-9.
12. Ngan Kee WD. The use of vasopressors during spinal anaesthesia for caesarean section. Curr Opin Anaesthesiol 2017 Jun;30(3):319-25. https://doi.org/10.1097/ ACO.0000000000000453. PMID: 28277383.
13. Charbit B, Mandelbrot L, Samain E et al. The decrease of fibrinogen is an early predictor of the severity of postpartum hemorrhage. J Thromb Haemost 2007;5:266-73.
14. Woman Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet 2017;389:2105-16.
15. Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med 2016;41:757-62.