Index
Note: Page numbers followed by f indicate a figure on the corresponding page. Page numbers followed by t indicate a table on the corresponding page.
abnormal fetal growth, 271-3 abnormal fetal heart rate, 252-3 acardiac twin pregnancy.
see twin-reversed arterial perfusion syndrome active delivery approach, 262 activity and exercise during pregnancy facts of, 286 issues with, 286 lifestyle considerations, 286-7 management options, 286 adjustment to parenting, 306-7 Advanced Dynamic Flow (ADF), 320 air travel during pregnancy, 287 American College of Obstetricians and Gynecologists (ACOG), 6-8, 72, 253-4, 259 American Institute ofUltrasound in Medicine (AIUM), 72
American Society for Reproductive Medicine (ASRM), 6, 7-8 amniocentesis
DNA fingerprinting with, 55 invasive prenatal diagnosis with, 54, 74, 92, 93, 94-5, 320 process of, 95 timing of, 97 amnionicity. see also monochorionic diamniotic (MCDA) pregnancies
defined, 31 diagnosis of, 181, 182f diamniotic twins, 32, 33-4f dichorionic diamniotic twins, 32, 33-4f, 43-4,
202- 3, 241
fetal growth restriction risks,
168- 9 in higher-order multiple pregnancies, 35-6, 37f introduction to, 18-20, 19f monoamniotic twins, 32-4, 35f, 36f
overview of, 31-2 prenatal determination of, 32-4
pseudoamnionicity, 34 ultrasound findings, 181 amniotic fluid (AF)
amniocentesis and, 95 bipolar coagulation and, 42 in cephalic twins, 262-3, 266 embolism, 347
evaluation of, 135, 184, 245-6, 262
fetoscopy and, 138 prenatal echocardiogram and, 102
preterm birth risk and, 206 reduction of, 159 sampling of, 235
TAPS and, 139, 148-9, 153
TTTS and, 137, 141, 142-3, 148-9, 182-3, 274 anaemia, 39, 93, 128-31, 226, 236, 340, 341. see also twin anemia polycythemia syndrome analgesia use during vaginal delivery, 260 aneuploidy screening, 114, 222, 223t, 237 angiography imaging, 105 anovulatory infertility, 11-13 antenatal care
consultation for, 276-7 corticosteroids use, 227-8 in early pregnancy, 221-2 education classes, 297-8 existing guidelines, 221 fetal growth pathology, 224, 225t
how/when to deliver, 228-9, 230-1t
informational and emotional support, 228
introduction to, 221 maternal complications, 226-7
monochorionicity complications, 225-6 nutritional supplements, diet, lifestyle, 228
planning and purpose of, 228 for preterm labour, 227 referral to tertiary fetal services, 229
screening for fetal complications, 222-6
screening for structural abnormalities, 223-4 antenatal ultrasound, 70, 71 antibiotic use, 43, 278 apparent diffusion coefficient (ADC), 324 appropriate-for-gestational age (AGA), 271-3 arterio-arterial (A-A)
anastomosis, 78-9, 158-9, 320, 322
arterio-venous (A-V) anastomosis, 78-9, 320, 322 artery-to-vein anastomoses, 273-5
assisted conception
for anovulatory infertility, 11-13
facts on, 11
for IVF, 13-14
for unexplained infertility, 13 assisted hatching, 202 assisted reproductive technologies (ART)
avoidance of multiple pregnancy, 201-2
DZ twins from, 5
gestational dating and, 50, 52 higher-order pregnancies from, 233
(ART) (cont.) methodology of, 7 modifying risk factors, 6 multiple pregnancies from,
1, 2f, 3, 8, 233
MZ twins from, 3-4 placental pathophysiology and, 189
assisted ventilation, 277
Association for Improvements in the Maternity Services (AIMS), 293
atypical twinning, 3
bacterial vaginosis screening, 207t, 207
bed rest, 210, 286 bereavement support, 304, 334 bipolar cord occlusion (BCO), 41-2, 118, 126, 177
body mass index (BMI), 5, 282-4, 285
BOLD-MRI, 324
Bracht manoeuvre, 265 Braxton Hicks, John, 263-4 breastfeeding
challenges with multiples, 198, 307-8
overview, 278-9
resources for parents, 336 support for, 276 breech-presenting twin, 253, 263-6, 343
British Fertility Society, 14
cardiac examination of conjoined twins, 105-6 cardiotocograph (CTG) shortterm variation, 174-5
cardiovascular disease, maternal, 197
cardiovascular outcomes after fetoscopic laser surgery, 140
cell-free DNA (cfDNA) testing, 55-6, 60-3, 222
Centers for Disease Control and Prevention (CDC), 6, 191 cephalic/breech twins delivery, 263
cephalic/cephalic twins delivery, 261-3
cephalic/non-cephalic twins delivery, 263
cephalic/oblique or transverse, 266 cephalopagus twins, 99-100 cerebral palsy (CP), 126, 221, 275, 276
cervical cerclage
controversy over, 211 history-indicated use, 211 management options, 213 meta-analysis/systemic review of, 212-13
for multiples only, 211 physical exam-indicated use, 212
in preterm birth (PB) prevention, 211-13 rescue cerclage, 212 ultrasound-indicated use, 212,217
cervical examination and preterm birth, 206
cervical pessary
definition and usage, 213-14 management options, 214 meta-analyses/systematic review, 214
for preterm birth prevention, 213-14
caesarean delivery management of MOMO pregnancies, 246 maternal morbidity and, 39, 196
neonatal mortality and, 251 obstetric anaesthesia during,
345- 6
planned caesarean delivery, 196, 251-5, 349
post-caesarean analgesia, 347-8, 348f
in singleton pregnancy, 249-51
trial of labour after
a previous caesarean, 255 child abuse, 7
‘Choosing Wisely' programme, 212
chorioamnionicity, 18 chorionic villus
sampling (CVS)
fetal aneuploidies diagnosis with, 54
in higher-order pregnancies, 235
invasive prenatal diagnosis with, 92, 93, 94, 320
for nuchal translucency screening, 58-9
timing of, 97
zygosity determination, 55 chorionicity
assessment importance, 97 defined, 21 dichorionicity, 23, 24f, 27f, 28-9
early first trimester, 23-5, 24f, 26f
establishing, 78 fetal abnormality risks and, 64-5f, 67-8f
fetal growth restriction risks, 168-9
in higher-order multiple pregnancies, 35-6, 37f
in higher-order pregnancies, 234 impact on preterm birth, 202-3
introduction to, 18-20, 19f late first trimester, 25, 27f MFPR with separate chorionicities, 44-6 monochorionic twin pregnancy, 23-5,28-9f, 32 overview of, 21-2
PAPP-A in dichorionic pregnancies, 59-60, 61 prenatal determination of, 22-3
second and third trimesters, 25, 30f, 31f
stillbirth and, 241, 242f chromosomal abnormalities/ defects, 54, 58-9, 94 chronic inter-twin transfusion imbalance, 149 clomiphene citrate (CC), 11, 12 co-bedding twins, 303 combined delivery, 252 complete moles, 3 computed tomography angiogram (CTA), 105 computed tomography (CT), 104-5
congenital abnormalities/ anomalies, 182, 270, 273 conjoined twinning anatomic classification, 108t cephalopagus twins, 99-100 craniopagus twins, 101 dorsal unions, 101 embryology of, 99 emergency separation, 107 facts of, 99 intrapartum management, 103 ischiopagus twins, 100 lateral unions, 100 management of, 101-7,
108-11f omphalopagus twins, 100 parapagus twins, 100 postnatal imaging, 104-6 prenatal imaging, 101-3 pygopagus twins, 101 rachipagus twins, 101 surgical simulation role in, 107-9
survival rates, 99 theories of, 273 thoracopagus twins, 100 ventral unions, 99-100 continuity of care, 329-30 continuous electronic monitoring, 256 cord complications, 275 cord entanglement, 103, 119-20, 120f, 181 cordocentesis, 55, 154 corticosteroids use, 227-8 cotyledonary flows, 322-4 craniopagus twins, 101 Crede’s manoeuvre, 265-6 crown-rump length (CRL), 48-51, 50f, 52, 66-9, 69f, 78 cryopreservation, 14 cytogenetic testing, 95-6
Data Safety Monitoring Board, 212
Dear Orla (UK), 291
Dekker, Rebecca, 300 delivery mode breech-presenting twin, 253 combined delivery, 252 facts of, 249-51 higher-order multiple pregnancies, 255 issues with, 251-5 management recommendations, 255-6 monochorionic diamniotic pregnancies, 254 monochorionic
monoamniotic pregnancies, 253-4 non-cephalic second twin and, 251-2 preterm birth and, 254-5
time interval between, 252-3 delivery room management, 277 delivery timing
dichorionic twin pregnancy, 242-3, 244t, 245t, 246f facts of, 241-2 higher-order multiple pregnancies, 245
importance of dating, 241 issues with, 242-5 management options, 245-6 monochorionic- monoamniotic twin pregnancies, 244-5, 247f monochorionic twin pregnancy, 242-3, 244t, 245t, 246f
neonatal mortality, rate versus risk, 241-2 stillbirth, rate versus risk, 241, 242f
triplet pregnancy and, 245 Delphi process, 84 diastolic notching, 184 dichorionic-diamniotic
(DCDA) twin pregnancies, 32, 33-4f, 43-4, 202-3, 241 dichorionic-triamniotic
(DCTA) pregnancies,
201- 2, 238 dichorionic-triamniotic (DT) triplet pregnancies, 40f, 43, 142-3, 202, 245 dichorionic twin pregnancy delivery timing and, 242-3,
244t, 245t, 246f
detection of, 23, 24f, 27f, 28-9
discordant fetal anomaly, 115-17, 116f
Down syndrome risk, 222 euploid dichorionic twins, 67 fetal growth restriction and, 168, 171, 172-5, 176t nuchal translucency measurement, 69 diet factors in DZ twin births, 5 dietary care, 228 diffusion-weighted imaging (DWI), 102, 324 discharge home and follow-up, 278 discordant fetal anomaly
defined, 112, 271-3
in dichorionic twins, 115-17, 116f
exceptional circumstances with, 119-21
introduction to, 112 management of, 114-19 in monochorionic twins,
117, 119f prenatal detection of, 114 prevalence of, 112, 113f selective termination
and, 117 dividing membrane
measurements, 31 dizygous (non-identical) twins defined, 1, 2f, 18, 19f, 20, 37 diamnionicity, 32, 33-4f dichorionicity, 23, 24f, 27f establishment of, 20-1 fetal abnormalities risk, 65 fetal aneuploidy risks, 54, 58 fetal causes of fetal loss/
mortality, 124 placentas of, 22-3 rates of, 8 risk factors for, 4-5 DNA fingerprinting, 55 Doppler ultrasound diastolic notching on, 184 in fetal growth restriction, 172, 174-5, 176-7 in placental vasculature and
function, 320-4, 321f, 323f dorsal unions in conjoined
twinning, 101
Down syndrome, 54, 222, 223t
echocardiography, 81, 102, 105,
107, 182, 197, 224 echoplanar imaging (EPI), 102 egg donation, 15 elective birth, 155, 241, 243 elective single embryo
transfer, 14 electrocardiographic (ECG)
imaging, 104, 105 emergency separation of
conjoined twins, 107 emotional and mental well-being antenatal considerations,
289-98
antenatal education classes,
297-8 bereavement support, 304 consequences of physical
challenges, 297 emotional and mental (cont.) external strains and stressors, 304-5 family-integrated care, 302-3 impact of contested interventions, 295-7 introduction to, 289 mental health support, 301-2 NICU and special care environment, 301-5 parent-centred birth experience, 298-301 patient vignettes, 292, 293, 294, 299, 308 postpartum well-being, 306-11 psychological impact of high-risk label, 292-3, 293, 294 psychosocial factors of patient, 291-2 recognition and empathy, 289-90
referrals for support, 290-1 twinship and individuality, 303-4
emotional antenatal support, 228 epidemiology of multiple pregnancy facts on, 1-6 management options, 6-8 modifying risk factors, 6 multifetal pregnancy reduction, 7, 8t overall incidences, 1, 2f, 3 epidural analgesia, 260, 343-5 ESPRiT study cohort, 169 estimated date of delivery (EDD), 88, 89 estimated fetal weight (EFW), 81, 125 euploid dichorionic twins, 67 European IVF Monitoring (EIM) Consortium, 238 ex utero intrapartum treatment (EXIT), 107 exchange transfusion, 84, 148, 154, 156, 226, 274 exogenous surfactant, 271, 277 external cephalic version (ECV) delivery, 251, 263
Family Crisis Support service, 335
family history and DZ twins, 4 family-integrated care, 302-3 family well-being during pregnancy.
see emotional and mental well-being feeding resources for parents, 336Fertility Clinic Success Rate and Certification Act (1992), 6 fetal abnormality screening chorionicity and, 64-5f, 67-8f
crown-rump length (CRL) measurement, 66-9, 69f facts of, 64-70 issues with, 70-4 labelling twins, 70f, 71f, 74 management of pregnancy, 73-4 nuchal translucency measurement, 69-70
role of ultrasound in, 72-3 fetal aneuploidy screening cell-free DNA testing, 55-6, 60-3
facts of, 54
by first-trimester combined test, 59-60, 62
issues with, 54-6 management options, 56t, 62 by maternal age, 56-8,
59t, 62
by nuchal translucency, 58-9 in presence of a vanishing twin, 62, 63
by second-trimester serum biomarkers, 60 fetal blood sampling (FBS), 93 fetal causes of fetal loss/ mortality, 124 fetal complications
abnormal fetal heart rate, 252-3
antenatal care screening, 222-6
as cause of preterm birth,
203- 4
obstetric anaesthesia risk of, 341-2 fetal echocardiogram screening, 81 fetal fibronectin (fFN) screening, 44, 207 fetal growth restriction (FGR)
antenatal care for, 224, 225t aetiology of, 168-9
fetoscopic laser surgery and, 177-8
inter-twin biometry discordance, 169 introduction to, 168, 271-3 management dilemma,
169- 70
management options,
170- 1f, 172, 173f, 175t prediction of, 178 prevalence of, 168, 169-74t role of intrauterine fetal
intervention, 177-8 selective growth restriction, 168, 170, 171-2, 174t, 177-8, 179
selective termination and, 177
summary of, 178 timing delivery of DC twins, 172-5, 176t
timing delivery of MC twins, 175-7
fetal hydrops, 342
fetal loss/mortality. see also intrauterine fetal death; neonatal mortality; single intrauterine fetal death aetiology of, 124-7 bereavement support, 304 facts of, 123-4 fetal causes of, 124 first trimester, 123 hemodynamic changes, 41-3 in higher-order pregnancies, 237 iatrogenic fetal loss, 126 intrauterine donor death, 139
maternal causes of, 124 in monochorionic- monoamniotic twins, 183, 184f
perinatal mortality, 271, 318
placental/membrane causes of, 125-6
second trimester, 123-4, 318-19
single fetal demise, 86, 123 single intrauterine death, 203-4
stillbirth, 39, 128-9, 169-70, 221, 241, 242f strangulation due to cord entanglement, 103
surviving twin with fetal demise, 275
third trimester, 123-4 with trisomies, 56-8 with TTTS, 125, 128, 276, 318-19
fetal mapping, 74, 94 fetal monitoring, 83, 238, 260, 267, 344
fetal pulmonary
maturation, 184 fetoscopic laser surgery for
TTTS cardiovascular outcomes after, 140 coagulation of the anastomoses cures
TTTS, 153 of connecting vessels, 177-8 fetal complications, 139 introduction to, 137-8 maternal complications, 139 neurodevelopmental impairment after, 140 optimal technique for, 142 outcomes after, 140 overview, 137-40 perinatal survival after, 140 of placental
anastomoses, 183 TAPS occurrence after, 147,
149-51, 152f, 156 technique of, 138 timing and mode of delivery after, 143 fetus infetu, 3 first trimester
detrimental effect of elective cerclage, 211 early first-trimester chorionicity, 23-5, 24f, 26f fetal aneuploidy screening,
59-60, 62 interventions for TRAP, 162,
163, 166 labelling twins in, 71, 74 late first-trimester chorionicity, 25, 27f maternal complications
in, 192
prediction of twin-to-twin transfusion syndrome, 136 screening for twin-to-twin transfusion syndrome, 80 single fetal demise, 123 ultrasound role in, 72 fission theory, 273 fluoroscopy of conjoined twins, 104 follicle-stimulating hormone (FSH), 4-5, 11-12 fragile X mental retardation 1 (FMR1) gene, 5 free β-hCG risk assessment, 59-60, 61, 62 frozen embryo replacements (FET), 11 fusion theory, 99, 273 gamete intrafallopian transfer (GIFT), 5 general anaesthesia, 345 genetic factors and DZ twins, 4-5 genetic screening
in low-risk pregnancy, 72 multifetal pregnancy reduction and, 41, 44-5, 46
nuchal translucency measurement and, 69 preimplantation genetic screening, 5
reviewing options for, 88 zygosity and, 64 gestational dating
choosing fetus for, 48-50, 51f
crown-rump length measurements, 48-51, 50f, 52
importance of, 241 introduction to, 48 issues with, 48-50 management of, 50-1, 51f when and how, 48, 50f gestational diabetes mellitus (GDM), 39, 193, 226, 236 gonadotrophin-releasing hormone (GnRH), 4, 11 Gratacos classification of sFGR, 179 Green-Top guideline number 51 on the management of monochorionic pregnancy, 329 growth differentiation factor 9 (GDF9) gene, 4 Growth Restriction
Intervention Trial (GRIT), 174 hearing deficit, 278 haemorrhage intraventricular
haemorrhage, 185, 254, 275, 278
as maternal complications,
39, 197, 236, 341 obstetric anaesthesia and,
346- 7 postpartum haemorrhage,
88, 103, 196-7, 255, 341, 348, 349 heterokaryotypic twins, 20, 28,
96, 117 heterotopic pregnancies, 3 Higgins Nutritional
Intervention Program, 284 High-intensity focused
ultrasound (HIFU), 325-6 higher-order multiple (HOM) pregnancies.
see also triplet pregnancy assisted reproductivetechnologies and, 201-2 defined, 35 delivery mode, 255 delivery timing, 245 determination of
chorionicity and amnionicity, 35-6, 37f discordant fetal
anomaly, 121 facts on, 233, 234t invasive prenatal diagnosis, 96 issues with, 234-6 management options, 237 medical complications, 236 miscarriage risks, 235 prenatal care of, 234-5 prenatal diagnosis of, 235 prenatal imaging/
screening, 235 preterm birth
prevention, 217 risk factors, 6, 23 risks with, 235-6 spontaneous preterm birth, 227, 236 vaginal delivery of, 267-8 Home-Start website, 335 home uterine activity monitor
(HUAM), 206-7 Human Fertilisation and
Embryology Authority (HFEA), 6, 7, 14 hyperbilirubinemia, 274, 278 hyperemesis gravidarum,
39, 236 hypertension/hypertensive disorders, 39,226,236, 341 hypogonadotrophic hypogonadism anovulatory infertility, 11-13
iatrogenic fetal loss, 126 ICOMBO (International
Council of Multiple Birth Organisations), 290 identical twins. see
monozygous (identical) twins
immunization administration, 278 in utero magnetic resonance imaging (iuMRI), 129 in vitro fertilization (IVF) avoidance of multiple pregnancy, 201-2
data and statistics on, 6 dizygous (non-identical) twins from, 1 multiple pregnancy rates with, 11, 13-14, 201-2 ovarian induction for, 13-14 preterm birth and, 205 informational antenatal
support, 228 Institute of Medicine
(IOM), 192 inter-twin biometry discordance, 169 inter-twin delivery interval, 252-3, 256 internal podalic version and breech delivery, 263-6, 264-5f
International Society of Ultrasound in Obstetrics & Gynecology (ISUOG), 72, 246
interstitial laser technique, 118, 120-1, 131, 165-6f intracytoplasmic sperm injection (ICSI), 202, 205 intrafetal laser coagulation, 163, 166
intrapartum management in conjoined twinning, 103 intrauterine donor death, 139 intrauterine fetal death. see also fetal loss/mortality; single intrauterine fetal death fetal anomaly and, 117 monochorionic monoamniotic twins and, 244-5
overview of, 183, 184f rates in smaller twin, 82 rates with multiples, 233 selective demise, 43 TTTS and, 137, 139, 342 intrauterine growth restriction (IUGR), 22, 44, 45-6, 125, 271-3.
see also selective intrauterine growth restrictionintrauterine insemination (IUI), 8, 11-13
intrauterine transfusion (IUT), 129, 154
intraventricular haemorrhage, 185, 254, 275, 278
invasive prenatal diagnosis amniocentesis, 92, 93, 94-5, 320
chorionic villus sampling, 92, 93, 94, 320
delayed cytogenetic testing, 95-6 facts of, 92-3 fetal blood sampling, 93 introduction to, 92 issues with, 94-6 management of procedures, 96-7 pregnancy loss with, 95, 97 special considerations, 95-6 technical
considerations, 94-5 ischiopagus twins, 100 ISUOG Practice Guidelines on the role of ultrasound in twin pregnancy, 329
JUmeaux MODe d'Accouchement (JUMODA) study, 251
labelling twins, 70f, 71f, 74, 78 lambda sign, 29, 30f, 64 language barriers to care, 291 laparoscopic ovarian diathermy, 12
large-for-gestational age (LGA), 271-3 laser coagulation in umbilical cord occlusion, 41-2 lateral unions in conjoined twinning, 100
Levret, Andre, 266 lifestyle care/considerations activity and exercise during pregnancy, 286-7 introduction to, 282 nutrition and weight gain during pregnancy, 282-6 nutritional supplements, 228 travel during pregnancy, 287-8
long-term outcomes, 43, 275-6 Lovset's manoeuvre, 265 low birthweight
after egg donation, 15 cervical cerclage and,211-12 delivery mode and, 254-5, 256
description of, 271-3 in dichorionic twin pregnancies, 11, 205 hospitalization risks, 276 in multiples, 249, 307 reduced risks of, 238, 284 Luke, Barbara, 284 Lullaby Trust, 337 luteinizing hormone (LH), 4, 11-12
magnetic resonance cholangiopan creatography (MRCP), 105 magnetic resonance imaging (MRI), 102, 104, 105, 129, 320, 325
maternal age
chromosomal abnormality risks, 114
delivery modes and, 250
DZ twins and, 4, 8, 65 fetal aneuploidy screening by, 54, 55, 56-8, 59t, 62, 92, 235
morbidity risks and, 341 NT screening and, 58-60, 63, 222
optimizing delivery outcomes, 197
preterm births and, 11 screening by serum markers, 60
triplets and higher-order multiples, 6, 92, 233 maternal body composition, 5 maternal complications addressing risks of, 191 anaemia, 39,93,128-31,226, 236, 340, 341
antenatal care for, 226-7 cardiovascular disease, maternal, 197
causes of fetal loss, 124 depression, 7 facts on, 188-91 in first trimester, 192 gestational diabetes mellitus, 39, 193, 226, 236 haemorrhage concerns, 39, 197, 236, 341 hypertension/hypertensive disorders, 39, 226, 236 issues of, 191-3 management options, 193-9 maternal morbidity, 188, 189f
mirror syndrome, 106, 120, 342
mitigating risk at delivery, 196-8, 197t
neonatal outcomes versus, 193, 195f, 199 patient-level pathophysiology, 188-90, 190t
placenta and, 189 population-level data on, 190-1
postpartum maternal care, 198f, 199
pre-eclampsia, 195,
204- 5, 341
smoking during pregnancy, 204 in third trimester, 192-3, 194t
vaginal birth safety, 196, 199 venous
thromboembolism, 193 maternal fetal medicine specialist, 72, 73 maternal morbidity maternal age and, 341 multifetal pregnancy reduction and, 39, 46 with multiple
pregnancies, 221 obstetric anaesthesia risk, 341 overview of complications, 188, 189f
maternal serum genetic screening, 69-70
Mauriceau, Francois, 266 maximum fecundity, 6 medical complications of
HOM pregnancies, 236 mental health support,
301- 2, 337 mental well-being.
see emotional and mental well-beingMichigan Multiples Clinic, 284 middle cerebral artery peak systolic velocity (MCA- PSV), 84, 85f, 128, 129, 147, 148f, 149, 151, 155 mirror syndrome, 106,120, 342 miscarriage rates/risks after sIUFD, 132-3 amniocentesis and, 93, 95 bipolar cord occlusion and, 118
cytogenetic testing and, 96 embryo versus fetal reduction, 40-1, 44 fetal reduction and, 237-8 invasive prenatal diagnosis and, 95, 97
invasive tests and, 54, 58 of monochorionic pregnancies, 125-6, 320 progesterone administration and, 216
second entry trocar, 164 selective termination and, 58, 116, 117, 202 single twin fetal loss and, 123 TAPS and, 125 triplets and higher-order multiples, 235
TTTS and, 243 monochorionic-diamniotic (MCDA) pregnancies defined, 78, 158 delivery mode and, 254 preterm birth risk and,
202- 3
stillbirth and, 241 twin-to-twin transfusion syndrome and, 203 monochorionic-monoamniotic (MCMA) twin pregnancies. see also twin to twin transfusion syndrome complications, 182-3, 275 congenital abnormalities, 182
defined, 78, 158, 181 delivery mode, 253-4 delivery timing of, 244-5, 247f
diagnosis of, 101, 181, 182f discordant fetal anomaly, 119-20, 120f
facts on, 181-3 fetal abnormalities risk, 64 fetal loss and, 125-6, 127 frequency and setting of surveillance, 184-5 intrauterine fetal death, 183, 184f
introduction to, 32-4, 35f, 36f, 38
issues with, 183-4 management options, 184-5 methods of surveillance, 184 MFPR not recommended for, 43
mode of delivery, 185 rate of congenital anomalies, 88
screening and diagnosis of, 86-8, 87f
selective growth restriction with, 78, 183
timing of birth, 185
TTTS in, 136 twin-to-twin transfusion syndrome in, 182-3 monochorionic twin
pregnancy
after in vitro fertilization, 202 complications with, 78, 225-6
delivery timing and, 242-3, 244t, 245t, 246f discordant fetal anomaly, 117, 119f
Down syndrome risk, 222 facts of, 77t, 78 fetal aneuploidy risks, 58, 60, 62
fetal growth restriction and, 168, 171-2, 175-7
invasive prenatal diagnosis, 96
issues with, 78-88 management of, 88-9 multifetal pregnancy reduction and, 41-3 monochorionic twin (cont.) nuchal translucency measurement, 69-70 overview of, 23-5, 28-9f, 32, 37
perinatal mortality, 271, 318 placental disease understanding, 319
preterm birth risk assessment, 88
screening and diagnosis techniques, 86-8
selective termination
in, 45-6
single intrauterine death,
203- 4
structural anomalies, 88 vascular anastomoses, 78-9, 318-19
MONOMONO study, 88 monosomy X screening, 56-8 monozygous (identical) twins.
see also conjoined twinning
after in vitro fertilization, 202
defined, 1-3, 18, 19f, 20,
37, 158
discordant fetal anomaly risk, 112
fetal abnormalities risk, 65-6
fetal aneuploidy risks, 55, 58 fetal causes of fetal loss/ mortality, 124
monoamniotic twins, 32-4, 35f, 36f
monochorionic twin pregnancy, 23-5, 28-9f, 32
placenta of, 22
rates of, 8
risk factors for, 3-4, 14
TTTS in, 158
multifetal pregnancy reduction (MFPR)
facts of, 39-41, 40f
genetic screening and, 41, 46 in higher-order multiple pregnancies, 237-8 introduction to, 7, 8t, 15 loss rates, 39
management of pregnancies after, 44
post-reduction pregnancy management, 45, 46 pre-pregnancy counselling and, 44-5
preterm birth risk and, 202 protocol for, 45 with separate chorionicities, 44-6 timing of, 40-1 in twin and triplet pregnancies, 43-4 multinomial logistic regression analysis, 205
National Academy of Medicine, 282
National Institute for Health and Care Excellence (NICE) (UK) care pathway and parents' proforma endorsement, 331 cephalic presentation of presenting fetus, 259 on caesarean delivery, 253-4 drop in multiple live birth rates and, 14
Guideline 137 for Twin and Triplet Pregnancy, 329 Hypertension in Pregnancy guidelines, 226
multiple pregnancy guidelines, 221, 229 preterm labour predictions, 227
Quality Standard 46 for Twin and Triplet Pregnancy, 329, 330f, 331 neonatal care
abnormal fetal growth, 271-3
adverse outcomes, 270-1 antenatal consultation, 276-7
breastfeeding, 198, 276, 278-9
congenital abnormalities/ anomalies, 182, 270, 273 cord complications, 275 delivery room management, 277 discharge home and followup, 278
issues with, 270 long-term outcomes, 275-6 management of multiple pregnancy deliveries, 276-9
neonatal intensive care unit, 252, 270, 277-8, 279
non-presenting newborns, 275
parental support, 279 perinatal depression, 275 perinatal morbidity, 270 perinatal mortality, 271 placental vascular anastomoses and, 273-5 prematurity, 271, 272f resources for parents, 334 respiratory distress, 275 surviving twin with fetal demise, 275
neonatal intensive care unit (NICU), 252, 270, 277-8, 279 bereavement support, 304 emotional and mental wellbeing of, 301-5 external strains and stressors, 304-5 family-integrated care,
302- 3
mental health support in, 301-2
support frameworks and self confidence, 309-10 twinship and individuality,
303- 4
neonatal mortality. see also fetal loss/mortality antenatal care and, 229 in breech-presenting twins, 253 cervical cerclage and, 211 caesarean delivery and, 251
iatrogenic preterm delivery risk and, 125, 132
with multifetal
gestations, 210 NICE guidelines on, 221 preterm delivery and, 216, 243
rates of risk, 241-2, 267 risk with multiples, 39 selective growth restriction and, 125
stillbirth risks, 241
TAPS and, 148 twin TOLAC and, 255 neurodevelopmental impairment, 140, 171, 275-6, 319 neurological morbidity in fetus, 41-3
NICHD Human Placenta
Project, 319 non-cephalic second twin delivery, 251-2 non-invasive intrauterine
treatments, 325-6 non-invasive prenatal diagnosis (NIPD), 325 non-invasive prenatal testing (NIPT), 222, 325 non-presenting newborns, 275 non-vertex-presenting twin, 266-7
North American Fetal Therapy Network (NafTNET), 72 nuchal translucency measurement, 58-9, 69-70, 114 nutrition and weight gain during pregnancy
body mass index, 282-4, 285 facts of, 282-4t issues with, 285 lifestyle considerations, 282-6
management options, 285-6 nutritional supplements, 228
obesity epidemic, 5 obstetric anaesthesia
for caesarean delivery, 345-6 during delivery, 342-6 epidural analgesia, 343-5 fetal complications risk, 341-2
general anaesthesia, 345 haemorrhage and, 341,
346- 7
introduction to, 340
maternal morbidity risk, 341 maternal physiological changes and, 340
planned vaginal delivery and, 343-5, 344f post-caesarean analgesia,
347- 8, 348f
pre-eclampsia and, 341 twin-to-twin transfusion syndrome and, 342 omphalopagus twins, 100 ovarian hyper-stimulation syndrome (OHSS), 5, 7, 14, 202 ovarian induction (OI)
for anovulatory infertility, 11-13
for IVF, 13-14
risk of multifetal gestation, 8 for unexplained infertility, 13 ovarian reserve, 4 overt systolic failure, 197 oxygen therapy, 277 oxytocin use, 256
PAPP-A in dichorionic
pregnancies, 59-60, 61 parapagus twins, 100 Pare, Ambroise, 263-4 Pare technique, 264-5 parent-centred birth
experience
changing language around birth, 300
emotional and mental wellbeing of, 298-301
environment of, 300-1 mode of birth, 298 support for, 300 parent resources
on bereavement, 334
on feeding, 336
on mental health, 337 for multiple pregnancies, 333-7, 338f
on neonatal care, 334
on practical challenges, 335, 336f
on pregnancy, 333
on sleep, 336 summary and further support, 337 parental support, 279 parents of multiples (PoMs), 289, 290, 297-8 parity increase and DZ twins, 4 passive delivery approach, 262 patent ductus arteriosus, 278 patient-level pathophysiology, 188-90,190t peer support, 297 perinatal depression, 275 perinatal morbidity, 46, 64, 168, 201,210,217, 233, 270, 275, 341 perinatal mortality
antenatal care and, 318 cerclage in twin gestation, 212
caesarean delivery and, 253 of conjoined twins, 99, 110 of MCMA twins, 87
modes of conception
and, 205
in MOMO twin
pregnancies, 244 of monoamniotic twins, 183 in monochorionic twins, 168 overview of, 271 TTTSand, 137, 141 UK-MBRRACE reports, 123 perinatal switch, 71 periventricular
leukomalacia, 275 physical exam-indicated
cervical cerclage
(PEIC), 212
Pinard manoeuvre, 265 placental angiogenesis, 135 placental disease understanding, 319 placental/membrane causes of
fetal loss, 125-6 placental vascular anastomoses, 273-5 placental vasculature and function assessment, 320-4, 321f, 323f planned caesarean delivery,
196, 251-5, 349 planned vaginal delivery (VD), 250-1, 252, 253, 343-5, 344f polycystic ovary syndrome
(PCOS) anovulatory infertility, 11-13 post caesarean analgesia,
347-8, 348f postnatal imaging in conjoined
twinning, 104-6 postnatal support resources,
333f, 332 postpartum depression, 39,
185, 236, 306-7, 337 postpartum haemorrhage, 88,
103, 196-7, 255, 341,
348, 349 postpartum maternal care,
198f, 199 postpartum well-being breastfeeding multiples,
307-8
life with multiples, 310-11 overview of, 306-11 recovery and adjustment to
parenting, 306-7 support frameworks and self
confidence, 309-10 practical challenges resources for parents, 335, 336f Practical Preparing for Parenthood course, 335
Prague manoeuvre, 266 pre-pregnancy counselling, 44-5, 46, 106 pre-eclampsia, 195, 204-5, 341 pregnancy loss. see miscarriage rates/risks
pregnancy management with multiples
facts of, 318
issues with, 318-20 placental vasculature and function assessment, 320-4, 321f, 323f research avenues, 320-6 pregnancy resources for parents, 333 preimplantation genetic screening (PGS), 5 premature cervical shortening in TTTS, 141 prematurity, 271, 272f prenatal care of higher-order multiple pregnancies, 234-5
prenatal determination/ diagnosis, 22-3, 32-4, 235. see also invasive prenatal diagnosis
preterm birth (PTB), 39
after multifetal pregnancy reduction, 44
amniotic fluid and, 206 avoidance of multiple pregnancies, 201-2
bacterial vaginosis screening and, 207t, 207
cervical examination
and, 206
chorionicity impact on,
202- 3
of conjoined twins, 103 contraception mode impact on, 205
delivery mode, 254-5 fetal complications as cause,
203- 4
fetal fibronectin and, 207 home uterine activity monitor and, 206-7
introduction, 201 maternal indications for,
204- 5 multifetal pregnancy reduction and, 202 pathophysiology, 201 pre-eclampsia and, 204-5 prematurity, 271, 272f preterm labour care, 227 prevention of multiple pregnancies, 201-2 previous history of, 204 race/ethnicity impact on, 205 risk assessment, 88 risks of, 221 single intrauterine death, 203-4
smoking during pregnancy, 204 spontaneous preterm birth, 227, 236
transvaginal ultrasound cervical length and, 205-6 twin-to-twin transfusion syndrome and, 203 preterm birth (PTB) prevention
cervical cerclage, 211-13 cervical pessary, 213-14 hospitalization and bed rest, 210
introduction to, 210 management of, 218t progesterone supplementation, 214-17 in triplets and higher-order pregnancies, 217 preterm delivery (PTD), 270-1, 272f preterm premature rupture of the membranes (PPROM), 103, 126, 139, 203, 270 progesterone supplementation management options, 216-17
meta-analyses of, 216
in preterm birth prevention,
214- 17
17-alpha- hydroxyprogesterone caproate (17-OHPC),
215- 16, 217
twins with short cervix, 215-16
unselected twins and, 215 vaginal-micronized progesterone, 215, 216,217 prophylactic tocolytes, 210 pseudoamnionicity, 34 psychological impact of high- risk label, 292-3, 293, 294
psychosocial factors of patient, 291-2
pygopagus twins, 101
Quadratus lumborum block (QLB), 347-8 quantitative fluorescent polymerase chain reaction (QF-PCR) analysis, 93, 96 Quintero staging criteria, 136, 137t
race/ethnicity factors, 4, 205 rachipagus twins, 101 radiofrequency ablation (RFA) in fetal growth restriction, 171-2, 177
iatrogenic cause of fetal loss, 126
intrauterine fetal therapy, 171-2
selective termination with, 118,318
TRAP and, 164, 165-6f, 210 in umbilical cord occlusion, 41-2, 118, 119f, 131, 177 radiograph use in conjoined twinning, 104 randomised controlled trials (RCTs), 12, 13, 142, 213, 215, 229, 249, 253, 347 receiver operating characteristic (ROC) curve, 205 recovery and adjustment to parenting, 306-7 rescue cerclage, 212 resources for multiple pregnancies
care in practice guidelines, 329-30, 331f
outcome guidelines and policies, 329, 330f
for parents, 333-7, 338f
for postnatal support,
333f, 332
support for health professionals, 330-3
Twins Trust's Maternity Engagement Quality Improvement project, 329, 331, 332f respiratory distress, 151, 211-12,215,216, 233, 244-5, 270, 274, 275 retinopathy of prematurity, 278 routine hospitalization, 210 Royal College of Obstetricians and Gynaecologists (RCOG), 175
SANDS (UK), 291 seasonal variation in DZ twin births, 5
second trimester
fetal aneuploidy screening, 60
fetal loss, 123-4 interventions for TRAP, 164 screening for twin-to-twin transfusion syndrome, 80 ultrasound role in, 72 selective fetoscopic laser photocoagulation (SFLP), 342
selective growth restriction (sFGR)
antenatal care, 224, 225t fetal growth restriction and, 168, 170, 171-2, 174t, 177-8, 179
higher-order multiple pregnancies, 236 in monoamniotic twins,
78, 183
selective growth restriction (sGR), 125
selective intrauterine growth restriction (sIUGR), 64, 78, 81-4, 82f, 82t, 83f, 147, 203
selective termination (ST) defined, 39 discordant fetal anomaly and, 117
fetal abnormality and, 73 fetal growth restriction and, 177
management of pregnancies after, 44
miscarriage rates/risks, 58, 116, 117, 202
in monochorionic twin pregnancy, 45-6
protocol for, 45 psychological impact of, 294 with radiofrequency ablation, 318
radiofrequency ablation and, 118, 318
reducing preterm birth risk, 202
in separate chorionicities, 44-6 timing of MFPR, 40-1 twin anaemia polycythemia syndrome and, 154-5 17-alpha-hydroxyprogesterone caproate (17-OHPC), 215-16,217
sex determination of fetus, 28 sexual activity during pregnancy, 286
single fetal demise, 86, 123 single intrauterine fetal death (sIUFD)
avoidance of, 127-8 avoiding co-twin sequelae following, 129-31 co-twin survivors of, 126 delivery after, 132 issues with, 127-33 monitoring after, 128-9, 130f, 131f pregnancy-associated risks, 126, 127t
pregnancy management after, 132-3
in twin and preterm birth, 203-4
single-nucleotide polymorphisms, 21 single-shot fast spin echo
(SSFSE), 102
Sleep Expectations factsheet, 337
sleep resources for parents, 336 Sleep Top Tips for Multiples factsheet, 337 small-for-gestational age (SGA), 271-3
Smellie, William, 266 smoking during pregnancy, 204
Society for Reproductive Technology (SART), 6
Society of Maternal Fetal Medicine (SMFM), 259
Society of Obstetricians and Gynaecologists of Canada (SOGC), 253-4 spontaneous preterm birth (SPTB), 227, 236. see also preterm birth
stillbirth, 128-9, 169-70, 221, 241, 242f
STOPPIT2 trial, 214 strangulation due to cord entanglement, 103 sudden infant death syndrome (SIDS), 337
superb microvascular imaging (SMI), 320
superfetation, defined, 3 superovulation, 7, 11, 13-14, 233
surviving twin with fetal demise, 275
suture ligation in umbilical cord occlusion, 41-2
swallowing anomalies, 117
T-sign, 64
T1-weight gradient echo (GRE), 102
T2-weighted single-shot fast spin echo (SSFSE), 102
TBS study, 249-50
Term Breech Trial, 253 termination of pregnancy in conjoined twinning, 106 thermal-neutral
environments, 277
third trimester, 123-4, 192-3, 194t
thoracopagus twins, 100 thromboelastometry, 347 thrombosis risks, 287 tocolytic agents, 210 tomographic ultrasound imaging (TUI), 320 total vascular resistance
(TVR), 190
transvaginal ultrasound, 12, 66, 73
transvaginal ultrasound cervical length (TVUCL),
205- 6
transversus abdominis plane block (TAP), 347-8 travel during pregnancy
facts of, 287
issues with, 287 lifestyle considerations, 287-8
management options, 287-8
trial of labour after a previous caesarean (TOLAC), 255 trichorionic triamniotic (TCTA) pregnancies, 43-4, 202
triplet pregnancy. see also higher-order multiple (HOM) pregnancies delivery timing and, 245 dichorionic-triamniotic triplets, 40f, 43, 142-3, 202, 245
dichorionicity, 23 multifetal pregnancy reduction in, 43-4
preterm birth prevention, 217 twin-to-twin transfusion syndrome in, 142-3 vaginal delivery of, 267-8 trisomy 13 screening, 54, 55, 56-8, 115, 222-3 trisomy 18 screening, 54, 55, 56-8, 115, 222-3 trisomy 21 screening, 56-8, 59, 62, 114, 115, 222-3 TRUFFLE trial (Trial of Umbilical and Fetal Flow in Europe), 174 twin anaemia polycythemia syndrome (TAPS) after fetoscopic laser surgery, 139
after fetoscopic laser surgery for TTTS, 147, 149-51, 152f, 156
amniotic fluid and, 139, 148-9, 153
characterization of, 148-9, 155
as chronic inter-twin transfusion imbalance, 149
clinical outcomes, 273-4 defined, 125, 147, 151 detection with MCA-PSV, 147, 148f, 149, 151, 155
elective birth and, 155 expectant management of, 152
facts of, 147-9, 148t, 150- 1f fetoscopic laser coagulation of anastomoses for, 153 in higher-order multiple pregnancies, 236 intrauterine transfusion of donor with exchange transfusion, 154 issues with, 78, 149-51, 152f management options, 152-5,
153- 4f
miscarriage rates/risks, 125 neonatal mortality, 148 occurrence after fetoscopic laser surgery, 147, 149-51, 152f, 156
overview, 84, 85f, 85t, 225-6 preterm birth and, 203 selective termination and,
154- 5
Twin Birth Study (TBS), 249, 343, 346
twin pregnancies. see also conjoined twinning; specific twin pregnancies after egg donation, 15 atypical twinning, 3 birth rates, 1 heterokaryotypic twins, 20 incidence of, 1-3, 2f inter-twin biometry discordance, 169 labelling twins, 70f, 71f, 78 multifetal pregnancy reduction in, 43-4 omphalopagus twins, 100 parapagus twins, 100 rachipagus twins, 101 surviving twin with fetal demise, 275 thoracopagus twins, 100 vanishing twin pregnancy, 3, 62, 63, 237 twin-reversed arterial perfusion syndrome (TRAP)
acardiac twin pregnancy in, 157-8
complications with, 78 defined, 157, 166, 182, 274-5 early intervention, 162, 163 expectant management, 162-3
facts of, 157-9, 160-1t first-trimester diagnosis,
162, 163, 166 incidence of, 157 intrafetal laser coagulation,
163, 166
issues in, 159-62 late intervention, 164, 166-7 management options, 43, 162-4, 165-6f
overview of, 84-6, 86f, 120-1 radiofrequency ablation and, 164, 165-6f, 210 second-trimester
interventions, 164 ultrasound monitoring and, 159
twin-to-twin transfusion syndrome (TTTS). see also fetoscopic laser surgery for TTTS
amniotic fluid and, 137, 141, 142-3, 148-9, 182-3, 274
anastomoses with, 79f, 79 clinical outcomes, 273-4 complications with, 64-6, 78 diagnosis of, 81, 135-6 Doppler ultrasound changes characteristic of, 183 fetal demise with, 276 fetal growth differences, 169 fetal loss/mortality, 125, 128, 276, 318-19
fetal loss with, 125, 128, 276, 318-19
fetoscopic laser surgery, 137-40, 153
first-trimester screening for, 80
incidence in MCMA twins, 87, 182-3
intrauterine fetal death, 137, 139, 342
introduction to, 79, 80t,
135
management of Stage
I TTTS, 141 miscarriage rates/risks, 243
in monochorionic- monoamniotic twins, 87, 182-3
monozygous (identical) twins, 158
nuchal translucency thickness and, 69-70 obstetric anaesthesia management of, 342 overview of, 79-81, 225 perinatal mortality, 137, 141
placental vasculature and function assessment, 321-4, 323f
prediction in first trimester, 136 premature cervical shortening, 141 preterm birth and, 203 screening with fetal echocardiogram, 81 second-trimester screening for, 80
summary of, 143
TAPS after fetoscopic laser surgery for, 147, 149-51, 152f, 156
treatment of, 137-8 in triplets, 142-3 ultrasound staging systems, 136, 137t
vascular anastomoses, 78, 79f Twins Trust's BeCOME survey, 329, 333f, 332
Twins Trust's CPD website, 332
Twins Trust's Maternity Engagement Quality Improvement project, 329, 331, 332f
UK-MBRRACE perinatal mortality reports, 123-4 ultrasound monitoring. see also Doppler ultrasound after single intrauterine fetal death, 128
in amnionicity diagnosis, 181
of conjoined twins, 102, 103, 104
delivery mode and, 255 dividing membrane measurements, 31
fetal growth restriction and, 170, 172
gestational dating, 48 high-intensity focused ultrasound, 325-6
in higher-order pregnancies, 234 iatrogenic fetal loss, 126 for intrauterine growth restriction, 45-6
introduction to, 12 mapping of fetuses, 45 of monochorionic pregnancies, 89
role in fetal abnormality screening, 72-3
as screening for structural abnormalities, 223 staging systems for twin-to- twin transfusion syndrome, 136, 137t tomographic ultrasound imaging, 320 twin-reversed arterial perfusion syndrome and, 159
use in cerclage, 212, 217 umbilical artery Doppler velocimetry, 128 umbilical cord occlusion, 41-2, 118-19
uterine incision, 268
vaginal delivery (VD) active approach, 262 analgesia use, 260 birth safety, 196, 199 cephalic/breech twins, 263 cephalic/cephalic twins, 261-3
cephalic/non-cephalic twins, 263
cephalic/oblique or transverse, 266
external cephalic version, 251,263
facts of, 259-68 fetal monitoring, 260 of higher-order multiples, 267-8
internal podalic version and breech delivery, 263-6, 264-5f
issues with, 268 labour during, 260 labour patterns in twins, 260 methodology of, 261-7 non-vertex-presenting, 266-7
passive approach, 262 planning of, 261 preparation for, 259-60 of triplets, 267-8 of twins, 259-67
uterine incision, 268 vaginal-micronized
progesterone, 215,
216,217 vanishing twin pregnancy, 3,
62, 63, 237 vascular anastomoses,
78-9, 164 vascular disruption sequence,
274-5
Veit, Gustave, 266
Veit, Mauriceau
Smellie, 265-6 veno-venous (V-V)
anastomosis, 78-9, 158-9 venous thromboembolism
(VTE), 193 ventral unions in conjoined
twinning, 99-100 virtual fetoscopy
technique, 322 voiding cystoureterogram
(VCUG), 104 vulnerable child syndrome, 309
well-being during pregnancy.
see emotional and mental well-being work restrictions during
pregnancy, 286
World Health
Organization, 191
zygosity
chorionic villus sampling and, 55
defined, 20
dizygosity, 20-1 genetic screening
and, 64 introduction to, 18-20, 19f overview, 20, 21f testing for, 290 zygote intrafallopian transfer
(ZIFT), 5
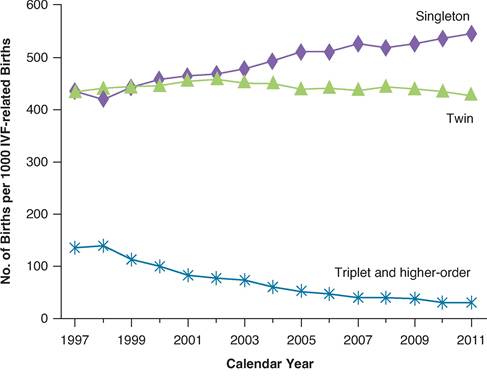
Figure 1.1 Changing incidence of multiple pregnancies
(Kulkarni AD, Jamieson DJ, Jones HWJr, Kissin DM, Gallo MF, Macaluso M, Adashi EY. Fertility treatments and multiple births in the United States. NEnglJMed 2013; 369(23):2218-25. doi: 10.1056/NEJMoa1301467)
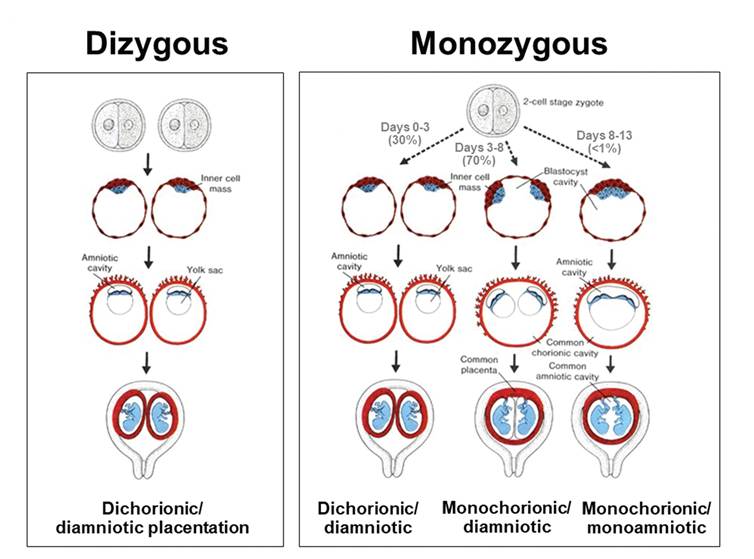
Figure 1.2 Zygosity and chorionicity of twin pregnancies
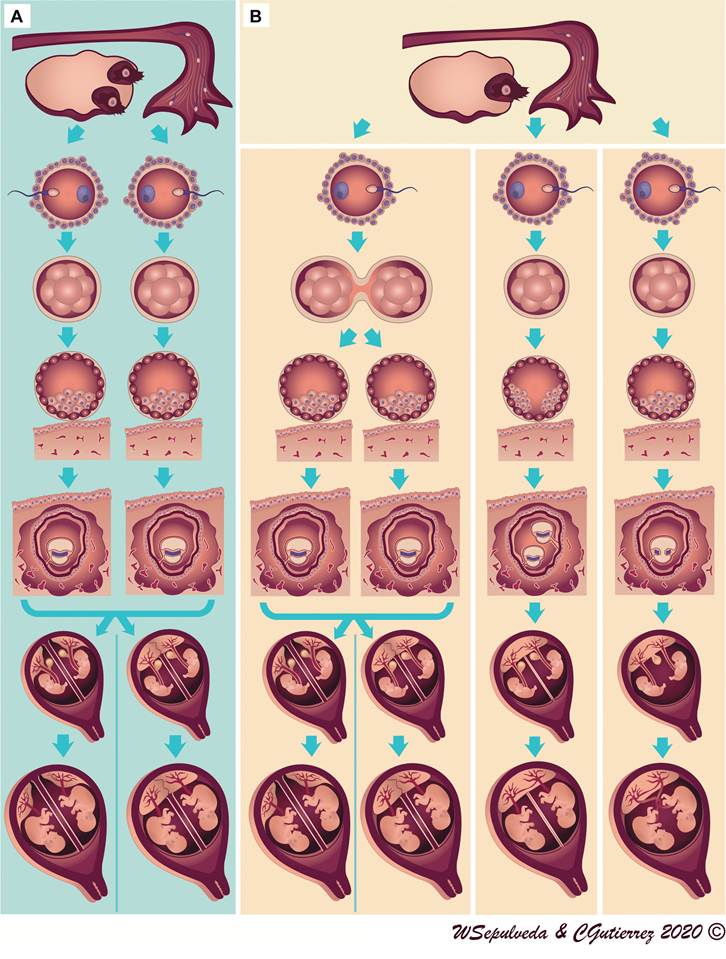
Figure 3.1 Classical representation of the three types of placentation in twin pregnancies according to zygosity. (A) Dizygotic twins develop from two separate eggs that are fertilised by two sperm; all have dichorionic-diamniotic placentation. (B) Monozygotic twins develop from a single zygote that subsequently splits and forms two embryos. Depending on the timing of splitting, they can be dichorionic-diamniotic, monochorionic-diamniotic or monochorionic-monoamniotic.
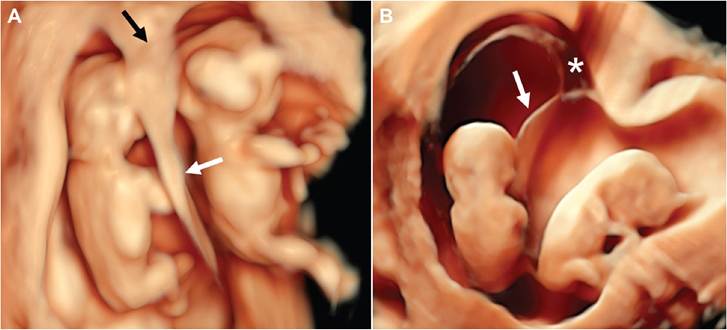
Figure 3.8 Surface-rendering three-dimensional ultrasound views of first-trimester twin pregnancies show the differences between dichorionic-diamniotic and monochorionic-diamniotic twins at the level of the dividing membrane (white arrows). (A) In dichorionic twins, the dividing membrane is thicker than in monochorionic- diamniotic twins and the 'lambda' sign is clearly seen at the inter-twin membrane-placental junction (black arrow). (B) In monochorionic-diamniotic twins, the dividing membrane is thin and is devoid of interposing chorion, which is also reflected at the level of the chorionic cavity (asterisk).
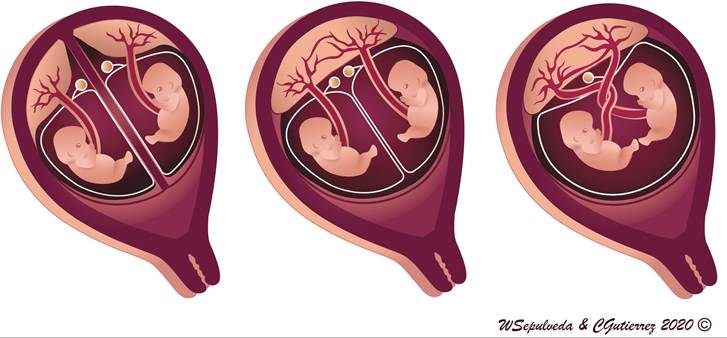
Figure 3.12 Schematic representation of the relation between yolk sac number and amnionicity in early pregnancy. In all dichorionic-diamniotic twin pregnancies, the yolk sacs are separated by chorionic tissue (left panel). In monochorionic-diamniotic twin pregnancies, two yolk sacs are present in the single chorionic cavity (middle panel). In monochorionic-monoamniotic twin pregnancies, only one yolk sac is usually identified (right panel).
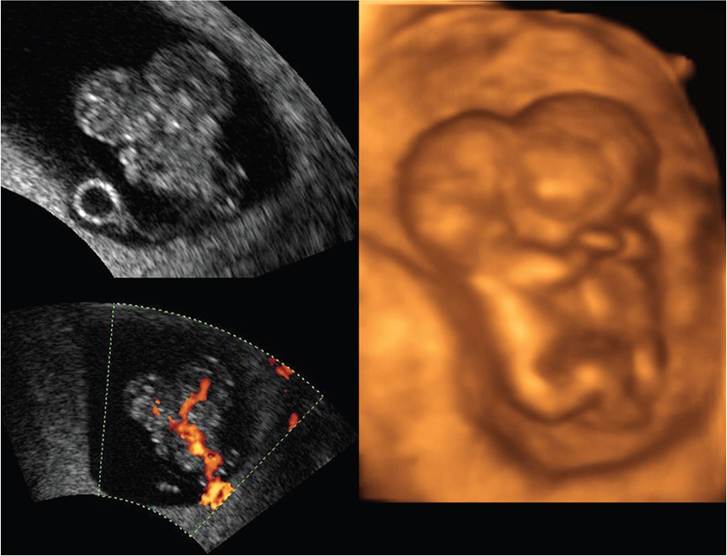
Figure 3.14 Amnionicity in early first-trimester monochorionic-monoamniotic twins. In this set of monochorionic- monoamniotic conjoined twins (thoracopagus type), there is only one yolk sac in the common chorionic cavity.
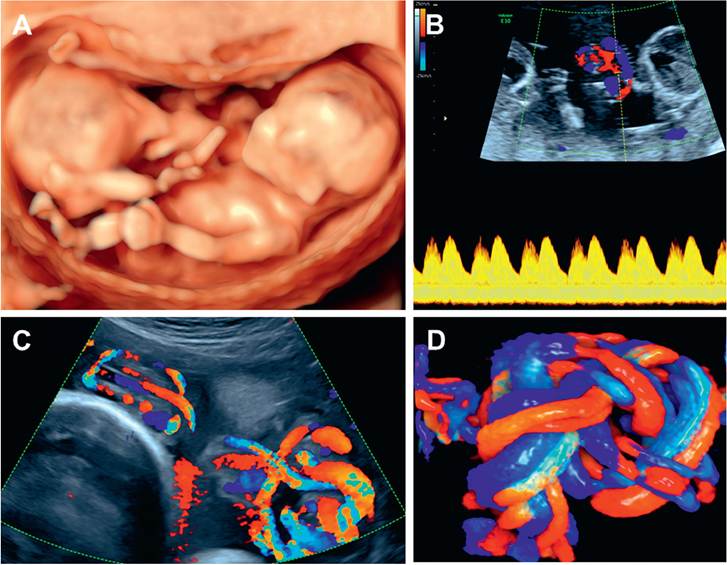
Figure 3.15 Monochorionic-monoamniotic twin pregnancy at 12 weeks 6 days. (A) Three-dimensional ultrasound shows two fetuses lying close together. The amniotic membrane was not identified. (B) Entanglement of the umbilical cords confirmed monoamnionicity. Spectral Doppler ultrasound demonstrates the two cardiac beats in the area of entanglement of the umbilical cords. (C) At 30 weeks, entanglement of the umbilical cords is evident as visualised with colour flow mapping. D, Three-dimensional HD live flow mapping demonstrates entanglement of the umbilical cords.
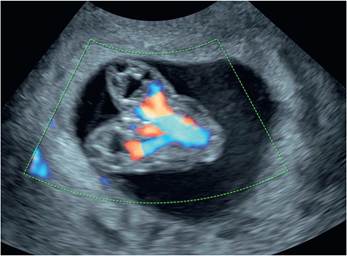
Figure 7.8 These images represent conjoined monochorionic-monoamniotic at 9 weeks. Colour Doppler is used to clarify the anatomy and identification of the conjoined twins which are thoracopagus (fusion from thorax to umbilicus).
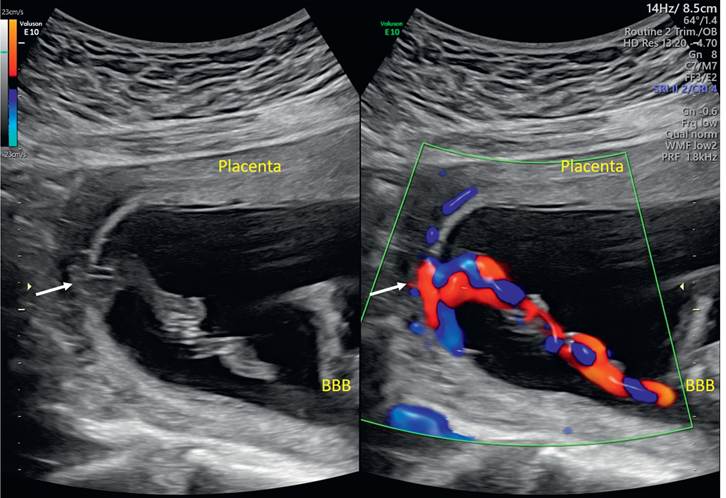
Figure 8.2 Split-screen ultrasound demonstrating a velamentous PCI (arrows) by two-dimensional (left) and colour flow (right) imaging with the anterior placenta several centimetres from the cord insertion.
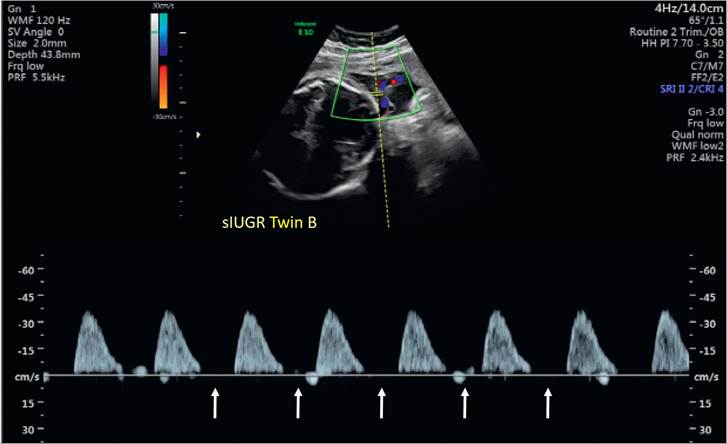
Figure 8.3 Doppler velocimetry of an MCDA twin with sIUGR demonstrating persistent absent end-diastolic flow (arrows)
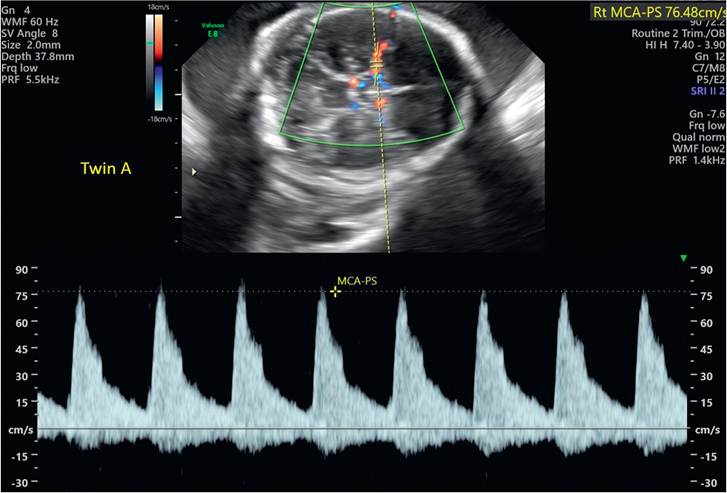
Figure 8.4 Elevated MCA-PSVinan MCDAtwin pregnancy complicated by TAPS at 29 weeks after laser therapy for stage III TTTS at 21 weeks of gestation.
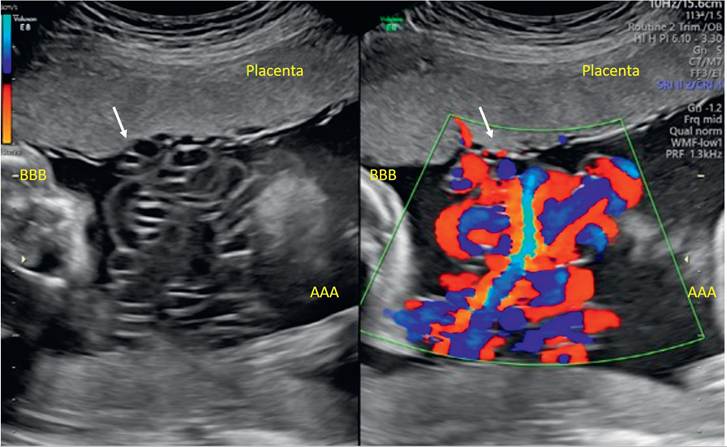
Figure 8.6 Split-screen ultrasound demonstrating umbilical cord entanglement (arrows) by two-dimensional (left) and colour flow (right) imaging in monoamniotic twins.

Figure 10.5 Three-dimensional ultrasound of dicephalic parapagus conjoined twins at 19 weeks of gestational age.
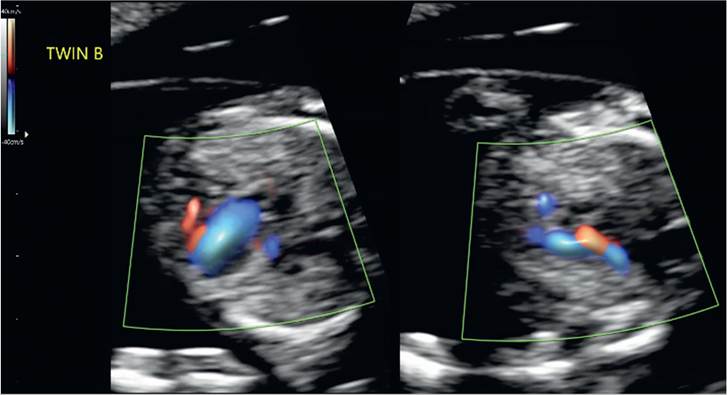
Figure 11.1 Hypoplastic left heart syndrome demonstrated in an MCDAtwin at 13 weeks of gestation. The lefthand image of the four-chamber view shows univentricular filling and the right-hand image of the three-vessel view shows reversed flow in the ascending aorta.
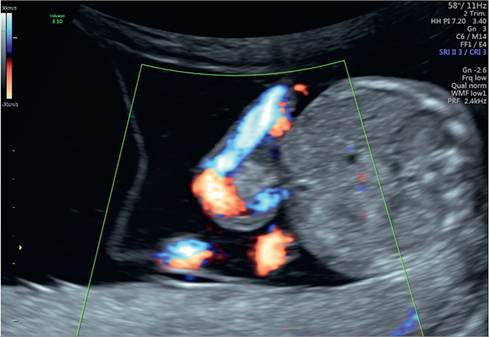
Figure 11.2 A small exomphalos seen in this MCDA twin at 14 weeks of gestation. The inter-twin membrane can be seen inserting into the monochorionic placenta.
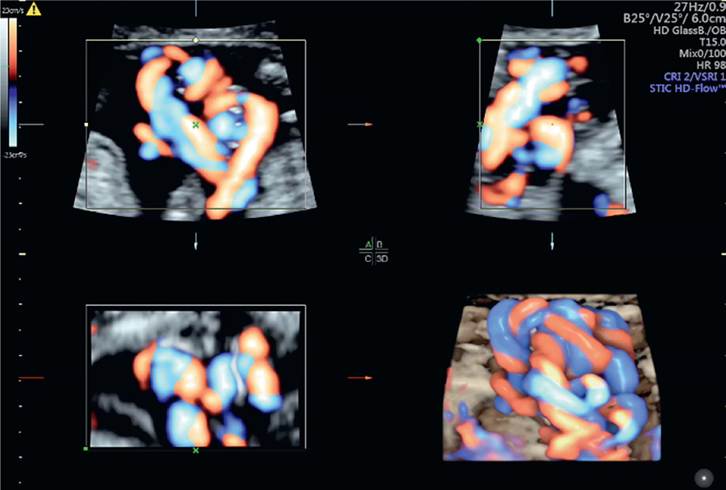
Figure 11.5 3-D multiplanar image showing cord entanglement in MCMA twins at 18 weeks of gestation
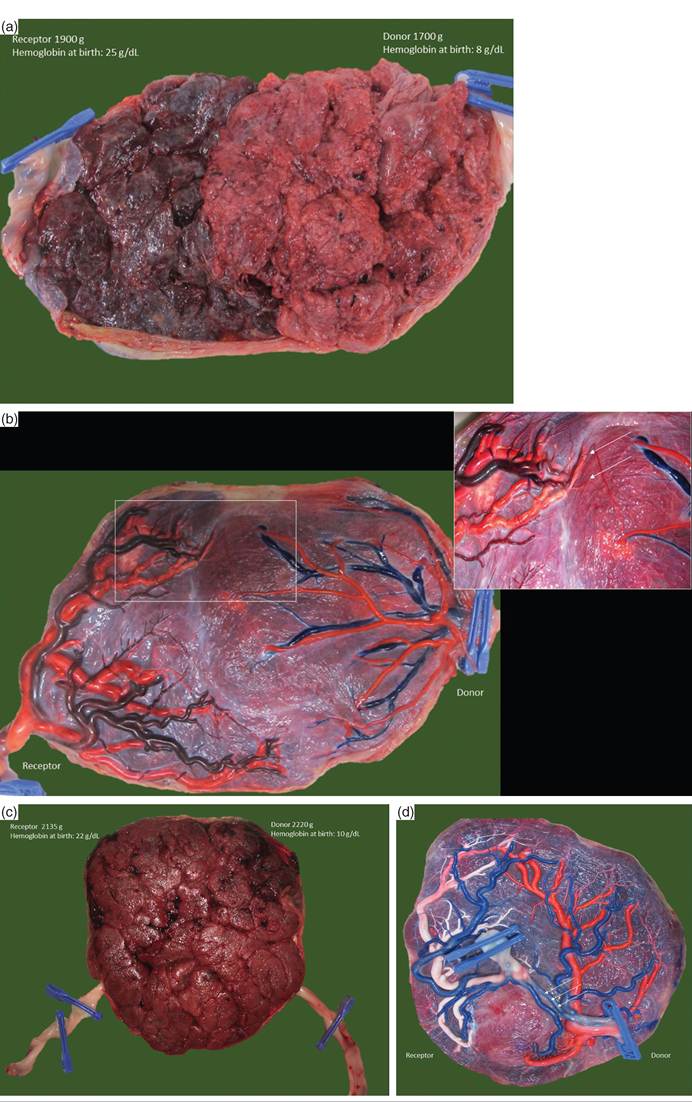
Figure 14.2 (a) Image of the maternal side from a monochorionic placenta of a spontaneous TAPS diagnosed at 30 weeks of gestation. This patient received one intrauterine transfusion at 31 weeks and was delivered electively at 32 weeks. There is a striking colour difference between the two parts. Also, the larger receptor had the smaller part of the placenta, indicating that TAPS influences fetal growth. (b) Image of the fetal side after colour injection. There were tiny artery-to-vein anastomoses (arrows). (c) Image of the maternal side from a monochorionic placenta of an acute peri-partum inter-twin transfusion. The babies were born vaginally at 34 weeks. There is no colour difference between the placental shares. (d) Placental injection showed a large artery-to-artery anastomoses (arrow), confirming an acute intra-partum transfusion as the cause of the haemoglobin difference.
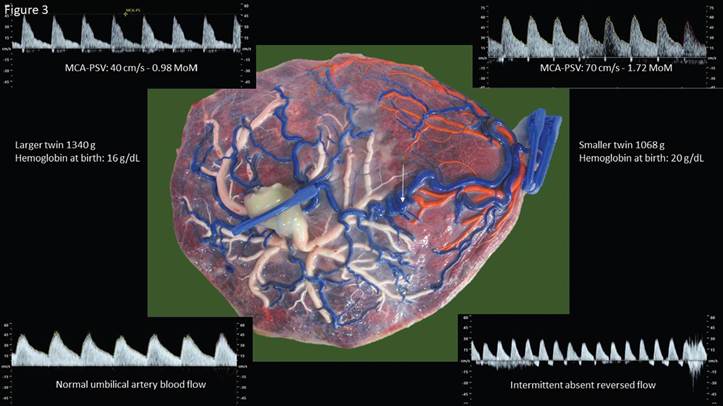
Figure 14.3 Monochorionic twin pair with type 3 selective growth restriction at 30 weeks of gestational age. Because of brain sparing, the MCA-PSV was increased in the smaller twin and normal in the larger twin. The typical intermittent absent or reversed end-diastolic flow pattern in the umbilical artery of the smaller twin indicates the presence of a large artery-to-artery anastomosis, which precludes the diagnosis of TAPS. The placenta showed the typical features of a type 3 growth restriction with a large artery-to-artery anastomosis (arrows) and little individual territory for the smaller twin with the marginal insertion.
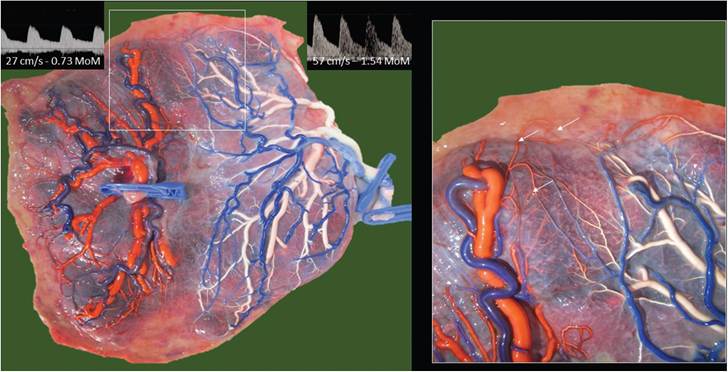
Figure 14.4 Images of a monochorionic pair with TTTS and coexistent TAPS at 28 weeks. The deepest vertical pocket was 11 cm in the receptor and 1.3 cm in the donor. At 28 weeks, we coagulated a visible artery-to-vein anastomosis and three tiny, unspecified anastomoses. We could not draw a Solomon line on the placenta because of intra-amniotic bleeding. After the surgery, TTTS disappeared but TAPS persisted. At 29 weeks, we gave an intrauterine transfusion to the donor for a haemoglobin of 6 g/dL and a partial exchange transfusion of the recipient for a haemoglobin of 21 g/dL. She was delivered electively at 32 weeks. The placenta showed minuscule, residual artery- to-vein anastomoses from the donor (2 clamps) to the receptor (1 clamp).
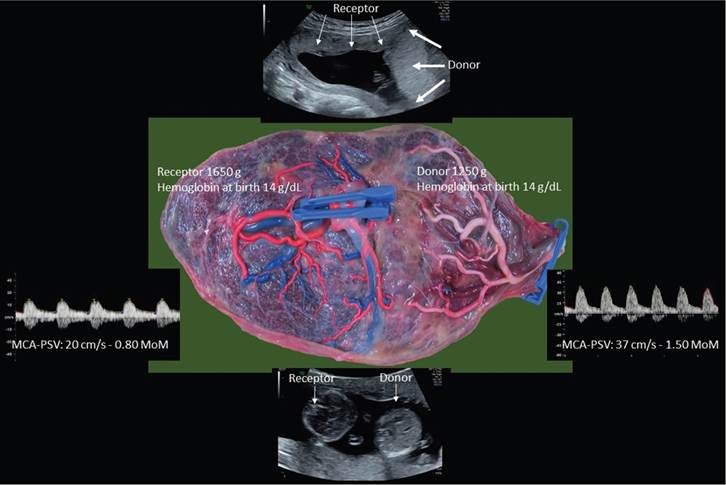
Figure 14.6 Ultrasound image of twin anemia-polycythemia at 15 weeks. The donor had the thick white part of the placenta, whereas the receptor had the thin, dark part. The receptor had a starry sky aspect of the liver. The pregnancy was managed expectantly. The MCA-PSV discordance improved spontaneously, and by 20 weeks, the MCA-PSV was concordant. She delivered at 31 weeks after spontaneous rupture of the membranes. The placenta did not show any anastomoses, as if we had performed a laser coagulation of all the anastomoses.
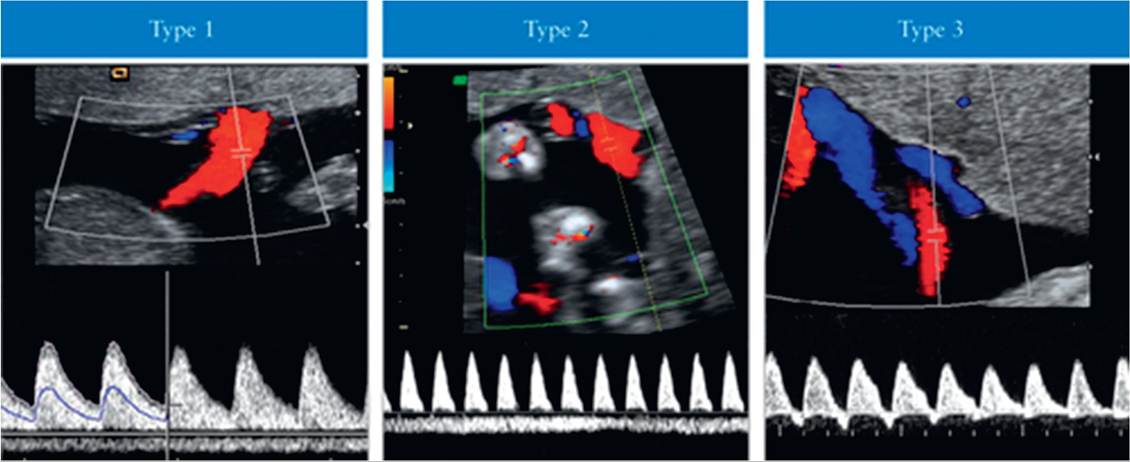
Figure 16.3 Gratacos et al. classification system for sFGR in twin pregnancies. In type I, the umbilical artery Doppler waveform has positive end-diastolic flow, while in type II, there is absent or reversed end-diastolic flow (AREDF). In type III, there is a cyclical/intermittent pattern of AREDF.7
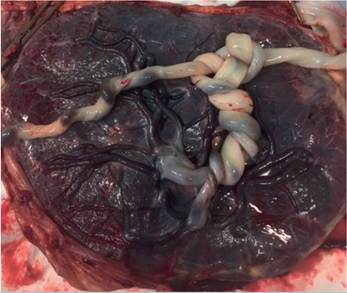
Figure 17.2 Proximate cord insertions and cord entanglement in a monoamniotic twin pregnancy
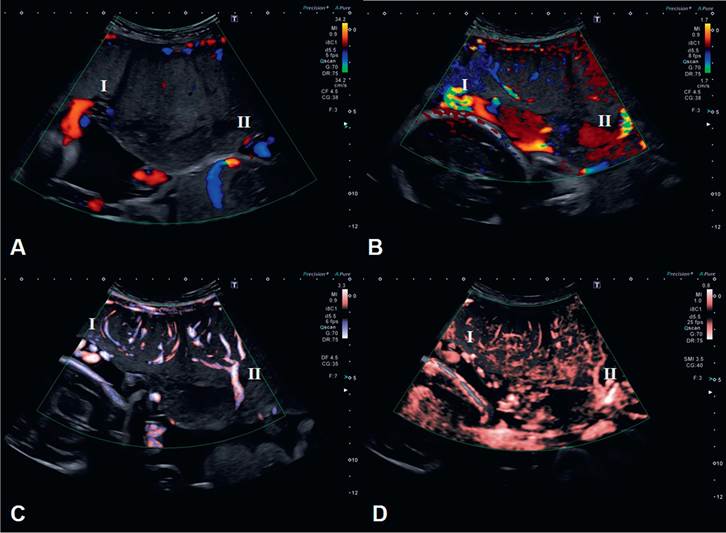
Figure 29.1 Comparison of colour Doppler imaging modalities to identify placental vasculature
The ultrasound images were taken from a monochorionic twin pregnancy with no features of twin-twin transfusion syndrome at 25+6 weeks' gestational age using:
(A) conventional colour Dopplerwith default obstetric mode settings (scale -34.2-34.2 cm.s-1). Herethe umbilical cord insertions (denoted as I and II) can be seen at the placental-amniotic interface; however, little colour signal is visible within the placental tissue.
(B) conventional colour Doppler with scale reduced to capture low flow (scale -1.7-1.7 cm.s-1). In this image there is aliasing at the sites of the umbilical cord insertion into the placenta (denoted as I and II) and more vessels are seen within the placental tissue. However, the quality of the image is greatly reduced by motion artefact and signal noise and detail of the placental angio-architecture cannot be ascertained.
(C) Advanced dynamic flow with default settings (scale -3.3-3.3 cm.s-1). Here the umbilical cord insertions are again seen at the placental-amniotic interface (denoted as I and II). However, in this image the branching vessels within the placenta can be seen in continuity from the cord insertions towards the materno-fetal interface, with minimal motion artefact or signal noise.
(D) Superb microvascular imaging with default settings (scale -0.8-0.8 cm.s-1). Here the umbilical cord insertions can again be defined by colour signal intensity (denoted I and II) and there is an appearance of branching vessels from the cord insertions towards the materno-fetal interface, with many more and smaller vessels seen compared to ADF. In this instance there is significant motion artefact despite the relatively high frame rate.
Ultrasound images were obtained using a 1.8-6.2 MHz convex probe (i8C1, Aplio i900, Canon Medical Systems) and are reproduced here with written consent from the patient.
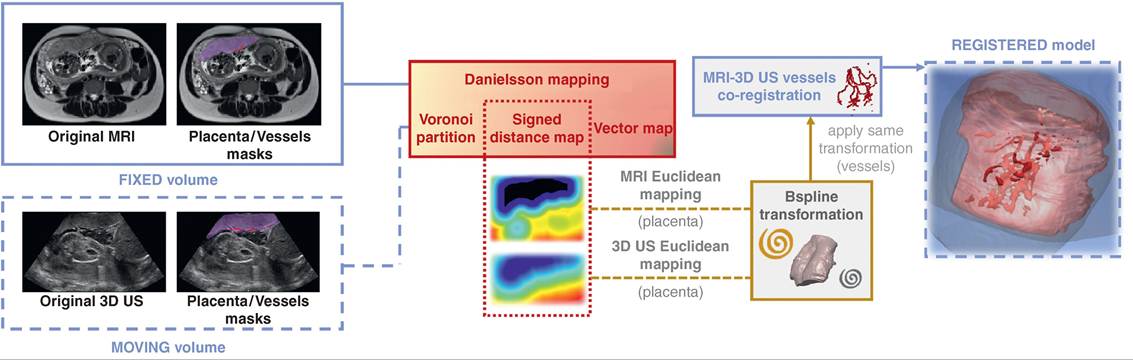
Figure 29.2 Schematic overview of the proposed MRI - 3D US registration methodology
Source: Torrents-Barrena et al. 2019 (13). TTTS-GPS: Patient-specific preoperative planning and simulation platform fortwin-to-twin transfusion syndrome fetal surgery. Computer Methods and Programs in Biomedicine, 179, 104993 (Reuse licence 4784840550036)