Epidemiology of stillbirth
Definitions
Stillbirth is defined by the World Health Organization as ‘death prior to the complete expulsion or extraction from its mother of a product of conception... the fetus does not breathe or show any other evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles’.
While the term fetal death is most accurate, the word stillbirth is preferred by parents and the community (1, 2). The International Classification of Diseases 10th revision (ICD-10) definitions are as follows:• Late fetal death: 1000 g or more or 28 weeks or more or 35 cm or more.
• Early fetal death: 500 g or more or 22 weeks or more or 25 cm or more.
• Miscarriage is a pregnancy loss before 22 completed weeks of gestational age (birthweight is given priority over gestational age).
For international comparisons, the World Health Organization recommends reporting of late gestation stillbirths (>28 weeks). The stillbirth rate is commonly expressed as the number of stillbirths per 1000 births. Many high-income countries (HICs) use a lower gestational age and birthweight threshold. For example, the United States, Canada, and Australia use 20 weeks’ gestation or 400 g. Different practices for inclusion of medical terminations of pregnancy also result in variations in reported stillbirth rates (3).
Rates and trends in stillbirth rates
Around 2.6 million late gestation stillbirths occur globally each year. The majority (98%) occur in low- and middle-income countries (LMIC) (Figure 34.1) (4) with around half during labour or intrapartum (Figure 34.2). Applying the lower gestational cut-off definition used across many HICs, the number of stillbirths could be up to 50% higher. A wide variation in stillbirth rates is evident, ranging from 28.7 (sub-Saharan Africa) to 3.4 per 1000 births (developed regions).
Reduction in global stillbirth rates has been slow, estimated at 1.4% per year from 2000 to 2015, which is around half that seen for maternal and newborn deaths (5).While absolute stillbirth rates in HICs are relatively low, variation in rates suggests that further reduction is possible. In the United States and Australia (using similar definitions of 20 weeks’ gestation or 400 g), stillbirth rates are 6.1 and 7.8/1000 births respectively and make up around 70% of total perinatal mortality, with the majority occurring in the antepartum period (3). Overall, around 1 in 140 women who reach 20 weeks’ gestation will have a stillborn baby. Using the number of ongoing pregnancies as the denominator, there is a U-shaped risk of stillbirth which is higher in the 20-24 weeks period, falls and then increases from 1 in 2000 at 37 weeks to 1 in 500 at 42 weeks (6).
Risk factors
Two recently reported systematic reviews on risk factors for stillbirth (5, 7) are summarized here with the major factors presented in Table 34.1.
Maternal sociodemographic factors
Advanced maternal age (>35 years), overweight (body mass index (BMI) 25-30 kg/m2), and obesity (BMI >30 kg/m2) and smoking are the three largest potentially modifiable contributors to stillbirth across HICs. These risk factors also make an important contribution to stillbirth globally (5). Women of 35 years or older have a 70% increased risk in stillbirth accounting for around 7% of stillbirths globally (7). Women over the age of 40 years have a doubling of the risk of stillbirth. Maternal overweight and obesity has become a global health problem, which also carries an increased risk of stillbirth (20% and 60% respectively). Women with a very high BMI (>40 kg/ m2) have a more than twofold increase in the risk (7). The contribution to stillbirth of maternal overweight and obesity globally is estimated at 10% (5) and may be twice that in some disadvantaged groups with higher rates of overweight and obesity (7).
Maternal obesity also increases the risk of diabetes and hypertension, which further places women at increased risk of stillbirth. Data from HICs show that while the overall contribution of pre-existing diabetes to stillbirths is small at the population level, it is one of the maternal medical conditions most strongly associated with stillbirth. Despite modern obstetric care, pre-existing diabetes is associated with a threefold increase in stillbirth (7). Chronic/pre-existing hypertension remains an important contributor to adverse pregnancy outcome with almost three times the risk in HICs (7).The risk of stillbirth for women having their first child is around 40% higher than women who have had a previous birth. In HICs,
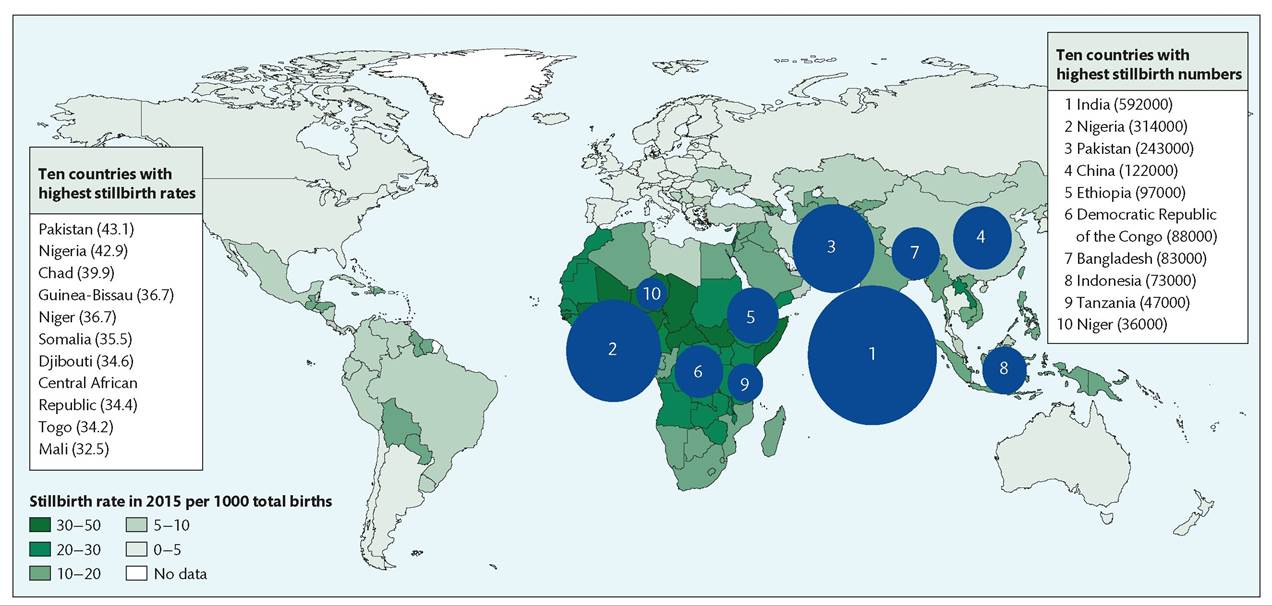
Figure 34.1 Variation between countries in stillbirth rates in 2015 Showingthe ten Countrieswith the highest rates, and those with the largest numbers.
Reproduced from Blencowe H1 et al. (2016). National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. The Lancet G∕oha∕ Health 4(2): e98-e108 with permission from Elsevier.
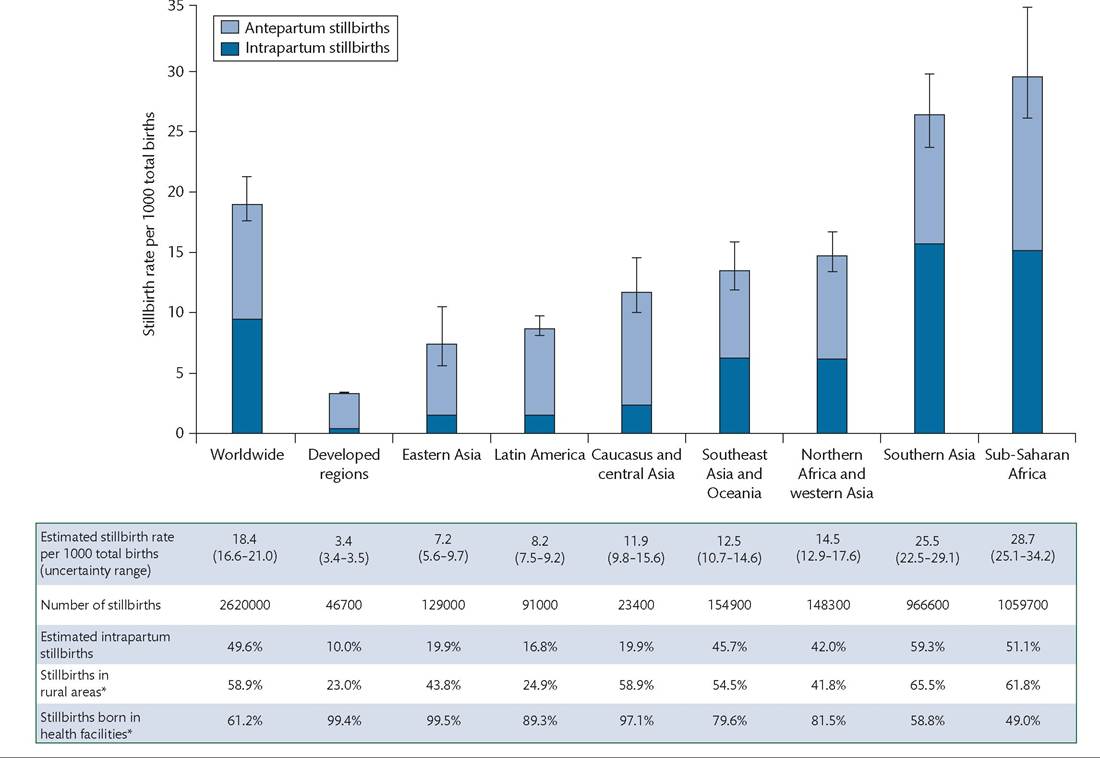
Figure 34.2 Regional variation in estimated stillbirth rates, showing uncertainty ranges, and the proportion of intrapartum stillbirths for 2015. *Based on urban and rural birth cohorts with national stillbirth rates so the values might underestimate rural stillbirth rates, which are expected to be higher than urban rates. Facility and home stillbirth rates are differential, the direction of increased stillbirth rates is unpredictable because the values might be lower at home if high-risk cases are in facilities, or higher at home if very low access to care.
Reproduced from Lawn JE, Blencowe H, Waiswa P, et al. Stillbirths: rates, risk factors and potential for progress towards 2030.
Lancet 2016; 387: 587-603 with permission from Elsevier.primiparity is an important contributor accounting for around 15% of stillbirths. Combining risk factors is also important and the stillbirth risk in older primiparous women (i.e. ≥35 years) may be two- to fourfold higher than their counterparts. In HICs particularly, with more women delaying childbearing, the higher rates of primiparous women of advanced age combined with increasing rates of overweight and obesity, sets a real challenge for stillbirth prevention. While rare in many settings, multiparity of five or more births carries increased risk of stillbirth and other adverse pregnancy outcomes (7).
Smoking has a tremendous global impact on health and smoking in pregnancy is causally related to placental pathology and increased risk of stillbirth (around 40%). Heavy smoking (ten or more cigarettes per day) carries a doubling of the risk. Women who are disadvantaged (lower socioeconomic status, poor education, by race/ethnic background, lack of access to quality culturally appropriate care), even in HIC settings, have approximately double or more the risk of stillbirth (7). Higher smoking rates, and poor antenatal care (which itself is associated with a threefold increase risk) and maternal medical conditions are important contributors in disadvantaged populations (3). Other factors contributing to this excess includes alcohol consumption (binge drinking) in the first trimester, illicit drugs use in pregnancy, indoor pollution, young maternal age, domestic violence, and possibly short interpregnancy interval. Consanguinity is a risk factor for stillbirth in some regions and cultures. While the adverse effects of alcohol consumption on the developing fetus are well accepted, there is a paucity of high-quality data to assess its true impact. Studies in HICs show a small (around 10%) increase in stillbirth for low intake (one to three drinks per week). One large study in the United States showed the association was stronger for stillbirth at less than 28 weeks' gestation (80% increase).
However, the risk was isolated to women with more than five drinks per week. Based on a prevalence of 50% and a 40% increased risk, alcohol intake in pregnancy could account for up to 17% of stillbirth in HIC settings.Table 34.1 Risk factors for stillbirth
| Factor | High-income countries’ | Globallyb | ||
| aOR (95% CI)c | PAR (%)d | aOR range | PAR (%)d | |
| Demographic and fertility | ||||
| Maternal age (years)® | ||||
| 35-39 | 1.5 (1.2-1.7) | - | - | - |
| 40-44 | 1.8(1.4-2.3) | - | - | - |
| ≥45 | 2.9(1.9-4.4) | - | - | - |
| >35 | 1.7(1.6-1.7) | 12 | 1.7(1.6-1.7)a | 6.7 |
| Low education | 1.7(1.4-2.0) | 4.9 | - | - |
| Low socioeconomic status | 1.2(1.0-1.4) | 9.0 | - | - |
| No antenatal care | 3.3 (3.1-3.6) | 0.7 | - | - |
| Assisted reproductive technology (singleton pregnancy) | 2.7(1.6-4.7) | 3.1 | - | - |
| Primiparity | 1.4 (1.4-1.3) | 15 | - | - |
| Previous stillbirth | 3.4 (2.6-4.4)f | 1f | ||
| Non-communicable disease and obesity | ||||
| BMI (kg∕m2)g | ||||
| 25-30 | 1.2(1.1-1.4) | - | 1.2 (1.1-1.4)a | - |
| >30 | 1.6(1.4-2.0) | - | 1.6 (1.4-2.0)a | - |
| >25 | 8-18 | 10 | ||
| Pre-existing diabetes | 2.9(2.1-4.1) | 2-3 | 2.9(2.1-4.1)a | 7.6 |
| Pre-existing hypertension | 2.6(2.1-3.1) | 5-10 | 2.6(2.1-3.1)a | 10.4 |
| Pre-eclampsia | 1.6(1.1-2.2) | 3.1 | 1.6(1.1-2.2)a | 2.6 |
| Eclampsia | 2.2(1.5-3.2) | 0.1 | 2.2 (1.5-3.2)a | 2.1 |
| Fetal factors | ||||
| SGA (increases the risk of stillbirth in a subsequent pregnancy by three to five times (7). Previous caesarean section may be associated with an increased risk of stillbirth which is thought to be due to abnormal placentation, however further research is needed (7). Suboptimal fetal growth is strongly linked with stillbirth. In an analysis of studies across HICs, SGA (less than the tenth centile for gestational age), was independently associated with a fourfold increased risk of stillbirth contributing to 23% of stillbirths (7). This finding points to the important contribution of placental patholo- gies/insufficiencies in stillbirth in HIC settings. Post- term pregnancy (≥42 weeks' gestation) is a risk factor for adverse pregnancy outcome estimated to contribute to 14% of stillbirths globally (5). With induction of labour policies before 42 weeks in many developed regions, the contribution to stillbirth of post-term pregnancy in these settings is usually quite small (7). Multiple pregnancy carries up to a sixfold increase in the odds of stillbirth when controlled for other factors (7). The currently available data suggest that women conceiving using assisted reproductive technology are likely to be at increased risk of neonatal deaths through SGA and preterm birth. While the association between assisted reproductive technologies and stillbirth is unclear, in vitro fertilization is definitely associated with an increased risk for singleton pregnancies (7). Male sex is associated with a small increase in the odds of stillbirth which may be through X-linked conditions, increased risk of preterm birth, and poor fetal growth (5). Causes of stillbirth Accurate and consistently classified data on the global causes of stillbirth are limited, particularly in LMIC. This is partly due to the difficulty in assigning causation due to the multifactorial circumstances of many stillbirths, underinvestigation, and the use of various, disparate classification systems for assigning cause of death (3). Globally, less than 10% of stillbirths are attributed to congenital abnormality (5) indicating that there is a high degree of potential preventability for cases due to other causes. Even for stillbirth with major abnormalities the potential for primary prevention exists (e.g. folic acid supplementation for neural tube defects). Causes of stillbirth vary with rates, with high-burden settings often reporting much higher proportions of intrapartum-related stillbirths. Low- and middle-income countries While data are sparse and vary widely by region across LMIC, the main reported causes of stillbirth include placental abruption accounting for up to one-quarter of stillbirths, pre-eclampsia and eclampsia, infection with malaria and syphilis which is a major problem in some regions, maternal conditions such as pre-existing diabetes and hypertension, and intrapartum complications accounting for up to 40% in some regions (9). High-income countries While a global picture of causes of stillbirth across HICs is difficult due to factors previously mentioned, recent population-based data show the most consistently reported categories of causes (3): placental pathology ranging from 13% to 39% (including largely placental abruption and insufficiency), fetomaternal haemorrhage around 2%, infection 5-15%, congenital anomalies 9-27%, maternal hypertensive disorders 3-9%, maternal diabetes 1-3%, cord complications 9%, and intrapartum complications around 3%. Complications of multiple gestation are not well reported but appear to account for around 6% of stillbirths (of which twin-twin transfusion syndrome contributes about 1-3%). Fetal growth restriction (FGR) or SGA, while not strictly a cause of stillbirth, is captured in most stillbirth classification systems with reported proportions ranging widely (3-38%) depending on whether conditions leading to poor fetal growth are classified preferentially. In systems where the scenarios of preterm labour and preterm prelabour rupture of membranes (often in combination with chorioamnionitis) are captured, from 3% to 15% of stillbirths are attributed to these scenarios and up to 40% of stillbirths at less than 28 weeks' gestation. Unexplained stillbirth ranges from 11% to 31% with adequacy of investigation and the system used being important influencing factors (3). Using a system which takes into account the quality of investigations for stillbirth, one study reported a low proportion of unexplained with thorough investigation (11%), classifying a further 19% as unknown due to insufficient investigation (6). Quality of care and stillbirth The stillbirth rate is a key indicator of the health of women in general and the quality of healthcare during pregnancy and childbirth. While the stillbirth rate itself is a valuable indicator (particularly in LMIC settings), to ensure policy and practice change a systematic approach to perinatal outcome audit with feedback to clinicians is needed (10). Perinatal outcome audit has been defined as ‘the process of capturing information on the number and causes of all stillbirths and neonatal deaths, or near-misses where applicable, with an aim towards identifying specific cases for systematic, critical analysis of the quality of perinatal care received in a no-blame, interdisciplinary setting in order to improve the care provided to all mothers and babies' (10). Perinatal mortality audits have consistently shown that suboptimal antenatal and obstetric care are frequently associated with stillbirths and neonatal deaths, ranging from 10% to 60% of cases. The main reported factors relate to delayed recognition of emerging clinical disorders, and inadequate or delayed response (most notably around maternal concern of decreased fetal movements (DFMs) and FGR). Other factors include failure to update and use best practice protocols, poor communication between staff, inadequate antenatal care, poor diabetes management, and maternal smoking. In the South African audit programme (Perinatal Problem Identification Programme), almost half of the deaths due to intrapartum asphyxia were found to be probably preventable with better fetal monitoring, use of the partogram, and optimal care in the second stage of labour (11). Although intrapartum stillbirths now make up a small proportion of late gestation stillbirths in HICs, concerns have been raised regarding the contribution of suboptimal care in these cases. In LMIC, high fertility rates coupled with low coverage of care and access to family planning are major contributors to stillbirth and neonatal death. Perinatal mortality audit, when combined with an approach to ensure practice change, can reduce avoidable stillbirth and neonatal deaths and is an essential part of good obstetric practice (10).
More medical literature on Medic.Studio
More on the topic Epidemiology of stillbirth:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
| ||||