Managing the obstetric aspects of stillbirth
The acute presentation, including the diagnosis of stillbirth
Stillbirth presents in many ways but in each case the obstetric management must be compassionate and the multiprofessional team involved should be cognisant of the extreme impact of the diagnosis and the emotional well-being of the woman and her family.
A common presentation in the third trimester will be associated with reduced or absent fetal movements, and then an inability to detect the fetal heart using a hand-held Doppler or cardiotocography (CTG) machine. It is important that confirmation of the diagnosis is made with ultrasonography as soon as possible, and that there is senior obstetric and midwifery input at the time. It is essential to avoid any uncertainty. The statement ‘I don't think there is a fetal heart present' leaves open the possibility that this could be wrong and can compound the grief reaction when it is finally confirmed. Another common scenario is when an ultrasound examination is being performed, either as part of routine screening or if there is a reduced fundal height, and in this case the sonographer may be the first person to make the diagnosis. Once again, senior input from maternity caregivers is essential, as this is an emotional emergency and how it is handled can impact the grief reaction for many months afterwards. There is no place for delaying the formal diagnosis by ultrasonography until a later, more convenient time.One particularly difficult situation is when it is discovered that one of twins or triplets has died. For di- or trichorionic pregnancies this will not normally lead to a decision to intervene by delivering the remaining twin or triplets. In the situation of monochorionic twins, especially at more advanced gestations, consideration may need to be given to immediate delivery of the surviving twin to avoid neurological sequelae, although this will depend on the gestational age and the length of time since fetal death occurred.
Delivery care: induction of labour and other obstetric aspects including complications
In many respects, the birth of a stillborn baby is not especially different from that of a live-born baby. Methods of induction of labour are generally going to be the same, although with very early gestations (up to about 30 weeks) other drug combinations such as mifepristone and misoprostol may be used. Local protocols should be consulted but generally a combination of prostaglandins and then artificial rupture of membranes/Syntocinon is used in the third trimester, sometimes with the addition of a cervical catheter to ripen the cervix if very unfavourable.
It is relatively common for women (and their families) to request ‘an immediate caesarean section' after fetal death been diagnosed, especially if this is late in the third trimester. This request should be managed respectfully, but it should also be considered to be a natural part of the immediate grief reaction. The desire to deliver the baby by the quickest method possible may be driven by the need to see and hold the baby and protect it from any further harm. While there is no rigorous evidence to support either approach, the experience of many involved in stillbirth care is that careful and expert counselling will lead to a decision to deliver the baby using the method that was originally planned, had the baby survived. It is clearly difficult to raise the issue of the next pregnancy at such a difficult time for parents but avoiding an unnecessary caesarean section may improve outcomes next time, and make management of that pregnancy much easier.
Obstetric complications associated with stillbirth are many, and these need to be explained to the woman before commencing induction of labour. It can be quite unpredictable how long the induction process may take, especially if the pregnancy is still in the second trimester. Stillbirth is more commonly encountered with both FGR and macrosomia, as well as with both oligo- and polyhydramnios, so unstable lie and malpresentations are more common.
After the birth it is not unusual to have a retained placenta, and postpartum haemorrhage is also more common as the fetal death may be associated with abnormalities of placentation including abruption. Management of the third stage should be active and the team should be ready to deal with any third-stage complication.Investigation after stillbirth including postmortem and placental histopathology
In most developed countries there exist protocols for investigation after stillbirth, although there are a number of studies being conducted worldwide into the efficacy and cost-effectiveness of a range of investigations. The purpose of investigations is to try to identify, as far as is possible, a cause of the stillbirth, which should then facilitate discussions about recurrence risks. Investigations are expensive, and all may not be available in every context in which stillbirth occurs. Generally investigations can be discussed under four headings:
Fetal and placental examination (including postmortem (autopsy) and imaging)
The autopsy should be considered the ‘gold standard' of the investigations, but there are many considerations around autopsy consent, and availability of expert perinatal pathologists to both perform the autopsy and interpret the results. Many parents will not consent to autopsy as they consider it is highly invasive and in some cases may be against their spiritual or cultural beliefs. This requires careful discussion and senior counselling intervention as the lack of an autopsy will often impede the final diagnosis and classification of the cause, as well as an understanding of any contributory factors. If autopsy is not agreed to, or not available, there are a number of alternatives, which range from external examination by a paediatrician or geneticist to try to identify dysmorphic features, imaging such as radiography or other more complex tests such as computed tomography or magnetic resonance imaging. In some cases, women may consent to a limited autopsy if it is thought that a particular organ system might be involved. It has been recommended that the target autopsy rate should be at least 50% of all stillbirths, but there is some argument for the selective use of this expensive investigation, especially if there is likely to be a low yield or if the cause of the fetal death is obvious.
Even if there is no fetal examination performed, placental histopathology should also be done as there is a strong association between various placental pathologies and stillbirth (Figure 34.3). The placenta should always be sent to the pathology laboratory fresh, and not placed in formalin.Microbiological studies
Infection is a relatively common cause of stillbirth but interpretation of microbiological results can be difficult as bacteria will often be present as contaminants, especially if fetal death has been present for some time. Swabs should be taken from the lower genital tract, the fetal membranes and placenta, and also from the fetal skin and internal organs. Generally, to attribute fetal death to bacterial infection it is important to see that the same bacteria is found in multiple sites, that it is considered to be pathogenic, and that there is evidence of some maternal and/or fetal response to the bacteria by eliciting signs of inflammation with histopathology. In some cases not all of these features are present and the conclusion must be drawn that ‘infection may have been the cause but it cannot be confirmed'.
Maternal blood tests
In general, the yield from maternal blood tests is quite low. These investigations are aimed at diagnosing a range of maternal medical conditions, such as diabetes, cholestasis, or thyroid disease, and in modern antenatal care it is unusual for these conditions to have been
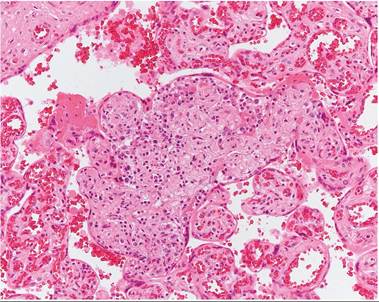
Figure 34.3 Placental histopathology slide showing evidence of chronic villitis, which is strongly associated with fetal growth restriction and stillbirth.
Courtesy of Professor Jane Dahlstrom.
missed prior to the stillbirth. ‘TORCH’ titres and thrombophilia screens are often part of stillbirth investigation protocols but interpretation of results needs some expertise as they can be misleading. For example, factor V Leiden heterozygosity is found in about 5% of the population and if seen without any evidence of placental infarction it is unlikely to be of significance.
Chromosomal and genetic studies
In the past, a fetal karyotype was always recommended, and this would be done by either taking a skin sample, or else some knee cartilage. Unfortunately, the growth of cells obtained from these sites is often overrun by bacterial growth. More modern molecular techniques are being introduced into practice and there is now some evidence to support the use of microarray technology in stillbirth samples as a range of unusual genetic deletions and duplications have been described in association with third-trimester stillbirth. Recent research with whole genome sequencing is also showing promise as a tool that might reveal previously hidden causes of unexplained stillbirth.
These investigations take time to complete, especially autopsy finalization, and women should be told that there may be a wait of 6-12 weeks to provide results, especially if there is a shortage of expert perinatal pathologists. For this reason, the follow-up from a physical and emotional perspective should be staged, with early appointments scheduled for specific reasons. There must be a clear understanding of when the final results will be available and it is important to avoid giving women and their family results piece by piece. Putting the whole story together requires all the results to be available, for these to be considered in the context of the history, and for an expert in interpretation to be available for the scheduled appointment. This is a highly specialized field and needs to be seen as a tertiary service.
Care in the next pregnancy: recurrence risk, monitoring, timing, and mode of birth
For many women there is a subsequent pregnancy after stillbirth, so care in the next pregnancy is very important although there is little evidence to support the various practices used by clinicians. Surveys of obstetricians show a very high proportion would offer much more intensive fetal monitoring with both ultrasonography and CTG, and many would offer early delivery for women whose previous pregnancy ended in late gestation stillbirth (12).
When managing the next pregnancy, an understanding of the cause of the previous stillbirth is essential to guide clinical decisionmaking. Early booking, or even pre-pregnancy counselling is helpful in making a comprehensive plan for antenatal care and birth. This plan is inevitably a compromise of both medical and emotional indications for various actions. For some women, normalizing the next pregnancy is important as this helps to reduce their anxiety around recurrence. For others, very intensive monitoring may be welcomed and getting the balance right is essential, as both under- and overmonitoring may fuel anxiety.
The timing and mode of birth are significant variables that both need to be included in the birth plan. Timing will often be influenced by the gestational age at which fetal death occurred previously, although if there is believed to be no or little risk of recurrence it makes no sense to cause iatrogenic prematurity without a good medical indication. Similarly, the view that caesarean section is indicated just because the previous pregnancy resulted in stillbirth is somewhat contentious. The view of these authors is that a request for planned elective caesarean section really should be considered in the same way that this request is considered in any other pregnancy. The option of planned, early induction of labour with close fetal monitoring is a reasonable alternative for the woman who wants to be in control of the timing and circumstances of birth, without the need for planned caesarean section.