New Frontiers in Multiple Pregnancy Management
Caroline J. Shaw and Christoph C. Lees
The Facts
Multiple pregnancy is widely understood to carry higher risks - that increase with the number of fetuses - of adverse perinatal outcome when compared to singleton pregnancy.
While this is due to higher rates of premature delivery, fetal growth restriction and congenital malformations, it is also important not to underestimate the impact of complications uniquely associated with monochorionic placentation irrespective of fetal number. Even in the context of current assisted reproductive technology, about one-fifth of twins are monochorionic. The fall in overall twin pregnancy perinatal mortality in the UK following the introduction of evidence-based, chorionicity-specific national standards for antenatal care is an important achievement. However, it clearly demonstrates the burden of mono- chorionicity, and this may explain why research in multiple pregnancy appears dispropor- tionally focused on the development of diagnostic and treatment modalities for monochorionic twins or dichorionic triplets when compared to dichorionic twins or even trichorionic triplets. Although the ‘hidden mortality of monochorionic twins' was a phrase coined more than two decades ago, its message holds true.The excess mortality of monochorionic multiple pregnancy is attributable to complications of a shared placental circulation; anastomoses between the vessels of what ideally should be separate circulations are found in up to 90% of monochorionic placentae. They may form artery to artery (AAA), artery to vein (AVA) or vein to vein (VVA), and have been found both superficially and deep within the placental cotyledon.1 The consequences of a shared placentation and the presence of placental vascular anastomoses include twin-twin transfusion syndrome (TTTS), twin anaemia-polycythaemia sequence (TAPS), twin- reversed arterial perfusion (TRAP) sequence, selective intrauterine growth restriction (sIGUR) and a risk of co-twin death or ischaemic-hypoxic brain or organ injury in the event of a single intrauterine fetal death (sIUFD).
Of these, TTTS is the leading cause of perinatal mortality in all twins.The Issues
The disparity in second-trimester fetal loss between monochorionic and dichorionic twins - or mono/dichorionic and trichorionic triplets - is acknowledged to be primarily due to TTTS, a disease which currently cannot be screened for, nor can patient risk stratification be performed. Management strategies are based on regular review to detect early disease stages by ultrasound examination and timely intervention where indicated. Fetoscopic laser has emerged as the leading intervention, rather than amnioreduction or selective termination of one fetus with radiofrequency ablation (RFA) or bipolar cord occlusion. This is despite a 2013 Cochrane review demonstrating neither a survival advantage nor a reduction in major neurological abnormality at the age of six years when treatment with fetoscopic laser is compared to amnioreduction.2 Fetoscopic laser treatment of TTTS continues to be recommended as it reduces the rate of minor neurological abnormalities at the age of six years.
A current Cochrane review identifies that further research is needed in the appropriate treatment for less severe disease (stages I-II); this is an advance from the previous version, which concluded that further research was needed only for the appropriate treatment of stage I disease. These conclusions infer a more basic lack of medical and scientific knowledge: the natural history of TTTS remains unclear. While the Quintero stage at diagnosis is prognostic of perinatal outcome, a nearly equal chance remains that stage I disease will remain stable, regress or progress once diagnosed. Hence, for any particular family, specific - or customised - outcomes remain difficult to approximate, making the burden of choosing between the risks of expectant management and intervention a heavy one. Similarly, in pregnancies diagnosed with TRAP sequence, a one-third chance remains of spontaneous resolution with invasive treatment, but determinants on which families can choose to safely pursue expectant management remain uncharacterised.
So too, in the management of selective growth restriction, where termination of the growth-restricted fetus can be considered to prevent the potential consequences of sIUFD to the appropriately grown surviving twin, there is little understanding of why some co-twins suffer hypoxic- ischaemic injury, but the majority do not.These questions shine a light on perhaps the least understood area of monochorionic pregnancies: the function of the placental vasculature within the shared placental portion. Histological and dye injection studies have demonstrated the anatomical structure of the monochorionic placenta with its multiple anastomotic connections; however, there is very limited functional assessment of the placenta in vivo. How a vessel that is histologically a vein functions when connected to another vein may, for example, be different to how it functions when it is anastomosed to an artery. Veins used as conduits for arterial flow have been shown to have greater incidence of endothelial injury due to haemodynamic stresses when compared to arteries, as well as poor elastic recoil, increased stiffness and turbulent flow beyond the point of anastomosis with a reduction in the mean blood flow velocity, yet none of these features have been described in placental AVAs to date.
Here, then, is our first frontier: a better understanding of the pathophysiology of disease in monochorionic placentae is needed. For this, a better understanding of normal and abnormal function of the shared circulation in the monochorionic placenta is a prerequisite. The lack of a preclinical model for the monochorionic placenta which mimics the gross shape, the haemochorial nature of the materno-fetal interface and the anatomy of shared placental portion has limited the amount of basic scientific research in this field.3 However, the National Institute of Child Health and Human Development (NICHD) Human Placenta Project, which aspires in part to develop new technologies for real-time assessment of placental development across normal and abnormal pregnancies, has regenerated a timely interest in technologies for both ex vivo models and in vivo assessment of the human placenta, which may be applicable to the monochorionic placenta.4 Only with better understanding of the pathophysiology of monochorionic placental disease can we move from observational, population-based statistics to individualised assessment of likely outcomes.
Closely related is our second frontier: how to ease the burden of decision-making on families with multiple pregnancies. Even if supplied with customised prognostications of disease outcome, many of the available interventions intended to further inform or reduce the risks associated with multiple pregnancy involve invasion into the intrauterine space, requiring the acceptance of the risk of associated iatrogenic miscarriage or pregnancy loss if they are chosen over expectant management. As the research revealing high levels of support among women for non-invasive prenatal testing for chromosomal anomaly compared to chorionic villous sampling (CVS) or amniocentesis has shown, concerns related to miscarriage are a key motivator in rejecting invasive procedures. Given that CVS, amniocentesis, fetoscopic laser, radio-frequency ablation and in utero transfusion are already minimally invasive procedures and remain associated with iatrogenic pregnancy loss, this suggests the focus should be on non-invasive therapies or techniques to mitigate the damage caused by intrauterine invasion. While decisions regarding individual fetuses within a multiple pregnancy have additional complexities of bereavement reactions despite ongoing pregnancy, reducing the risk of procedure-related pregnancy loss can only be a benefit.
Research Avenues
Assessment of Multiple-Pregnancy Placental Vasculature and Function Using Diagnostic Imaging
In a research setting the structure and, to a lesser degree, the function of placental anastomoses within the shared region of the monochorionic placenta have been investigated using both Doppler ultrasound and MR angiography. Additionally, the function of the materno- fetal interface in both monochorionic and dichorionic twin pregnancy has been assessed using MRI.
Standard 2D colour and pulse-wave Doppler techniques can be used to identify both AAAs and AVAs.5-7 The AAAs appear easier to locate with a sensitivity of 85% and specificity of 97% compared to placental injection studies,5 while AVAs have a lower sensitivity of 50% but retain a reported specificity of 93-97%.6,7 Recently the use of 3D high- definition flow between the cord insertions of the twins co-registered with tomographic ultrasound imaging (TUI) has improved the sensitivity for AVAs to 88% while maintaining a high sensitivity.8 Tomographic ultrasound imaging combines spatial tracking of the ultrasound probe (typically using spatial sensors attached to the probe) with the diagnostic imaging obtained during the probe movements.
This offers the possibility of ultrasound post-processing, as in this application, to display multiple parallel sections of the placenta, allowing identification of both superficial and deep anastomoses.Innovation in colour Doppler imaging may also have a role to play in this field. Conventional colour Doppler imaging within obstetrics employs a wall filter to reduce motion artefacts and remove low-flow ‘noise’ that could contaminate the ultrasound signals so as to optimise identification of high-flow vessels within the fetal circulation and umbilical cord. However, the loss of the low-flow signal compromises the imaging capabilities for microvascular circulations such as placental vessels and anastomoses. Colour Doppler applications such as superb microvascular imaging (SMI) or advanced dynamic flow (ADF) focus on flow distribution in the region of interest using a high-density ultrasound system architecture.9,10 This enables the processed ultrasound image to identify and remove
global motion signals while preserving very low-flow (SMI < 1 cm.s-1) and low-flow components (ADF < 10 cm.s-1), hence enabling visualisation of placental microvasculature with a much greater degree of clarity than simply reducing the scale of conventional colour Doppler (Figure 29.1).11
In all these studies, sensitivity and specificity values were determined by comparison of the number and type of anastomoses detected on postnatal dye injection studies - which
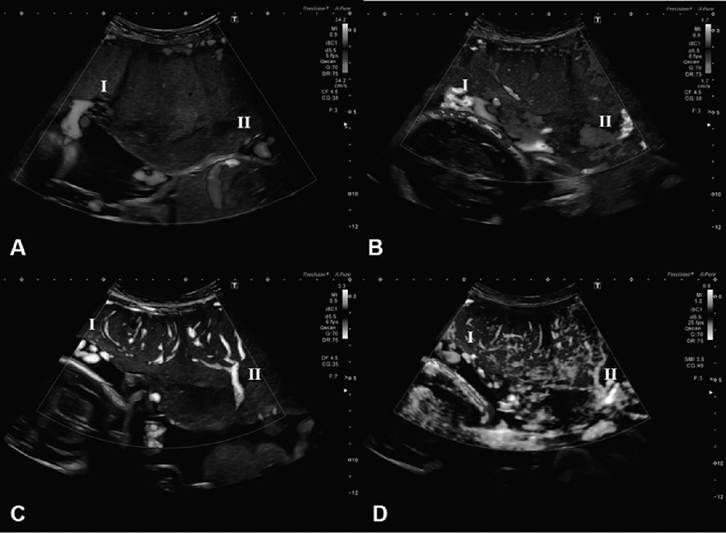
Figure 29.1 Comparison of colour Doppler imaging modalities to identify placentalvasculature (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
The ultrasound images were taken from a monochorionic twin pregnancy with no features of twin-twin transfusion syndrome at 25+6 weeks' gestationalage using:
(A) conventionalcolour Dopplerwith default obstetric mode settings (scale -34.2-34.2 cm.s-1).
Herethe umbilical cord insertions (denoted as I and II) can be seen at the placental-amniotic interface; however, little colour signalis visible within the placentaltissue.(B) conventionalcolour Dopplerwith scale reduced to capture low flow (scale-1.7-1.7 cm.s-lJ. In this image there is aliasing at the sites of the umbilicalcord insertion into the placenta (denoted as I and II) and more vessels are seen within the placentaltissue. However, the quality of the image is greatly reduced by motion artefact and signalnoise and detailof the placental angio-architecture cannot be ascertained.
(C) Advanced dynamic flow with default settings (scale -3.3-3.3 cm.s-1). Here the umbilicalcord insertions are again seen at the placental-amniotic interface (denoted as I and II). However, in this image the branching vessels within the placenta can be seen in continuity from the cord insertions towards the materno-fetalinterface, with minimalmotion artefact or signal noise.
(D) Superb microvascular imaging with default settings (scale -0.8-0.8 cm.s-1). Here the umbilicalcord insertions can again be defined by colour signal intensity (denoted I and II) and there is an appearance of branching vessels from the cord insertions towards the materno-fetalinterface, with many more and smaller vessels seen compared to ADF. In this instance there is significant motion artefact despite the relatively high frame rate.
Ultrasound images were obtained using a 1.8-6.2 MHz convex probe (i8C1, Aplio i900, Canon MedicalSystems) and are reproduced here with written consent from the patient. showed only superficial anastomoses - to the number and type predicted based on previous ultrasound assessments, which should have identified both superficial and deep anastomoses. These studies also did not provide any functional assessment of the in vivo direction or nature of flow through the anastomoses, nor their contribution to the disease processes (sIUGR, TTTS, TAPS) within the population studied. None of these studies have determined whether the structure of a placental vessels - be it arterial or venous - within the monochorionic placenta corresponds absolutely to either the direction or pattern of the blood flow within it in utero. This is a major and frequently overlooked fact. Hence we are able to conclude from these important studies that it is possible to see opposing arterial- arterial and arterial-venous flow as vessels of the two fetal circulations meet. They do not, however, elucidate why the proportion of monochorionic placentae with AVAs far exceeds those that will develop TTTS. Nor do they explain why hypoxic-ischaemic injury following sIUFD is fivefold more likely in pregnancies affected by TTTS than sIUGR.
While rarely challenged, it should be recalled that the role of AAAs, AVAs and VVAs in the development of disease in monochorionic twins has not been demonstrated in vivo and remains speculative to an extent. For example, a study in which intra-amniotic Doppler was performed in a series of three patients affected by TTTS showed that the net direction of blood flow in TTTS was from the recipient to the donor, contrary to received wisdom.12 Why, for example, could a ‘recipient’ twin not maintain the blood supply of a donor with a poor share of the placenta - the latter explaining its inability to grow or produce urine?
While this novel application of Doppler remains unvalidated, and the findings may be affected by fluctuations in flow or skewed by AVAs not identified on fetoscopy, it remains an intriguing counterpoint to received wisdom regarding the pathogenesis of TTTS. In fact, while reasonable correlations based on that same received wisdom have been drawn between the findings of Doppler ultrasound antenatally and superficial dye injection studies postnatally, the ability to ascribe a specific Doppler waveform recorded antenatally to a particular vessel within a post-delivery placenta is limited unless that vessel is described relative to a landmark such as the cord insertion. This truly would be an important next step in understanding the function of placental anastomoses.
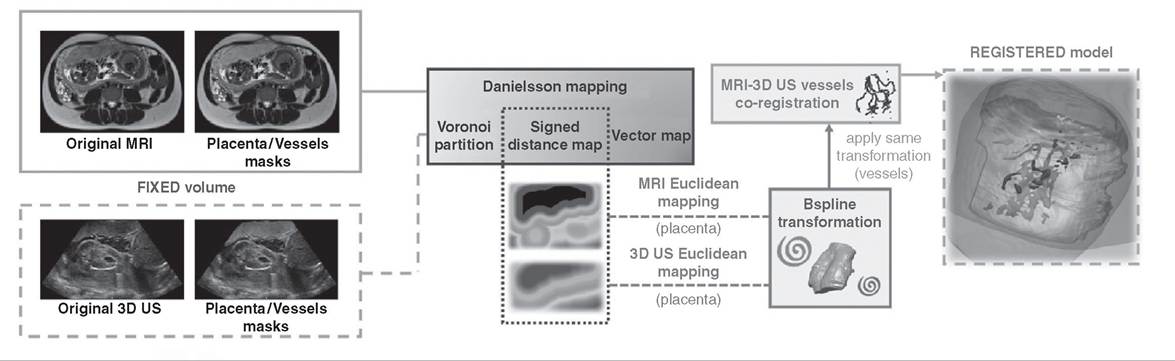
Such a technology remains elusive, but the advances in co-registration techniques suggest it may be possible. A novel simulator showing a fetoscopic view of the placental surface has been described using MRI-derived imaging of the placenta co-registered with 3D ultrasound imaging overlaid (Figure 29.2).13 While this system, by design, focuses on showing the position of surface placental vessels within the body of the uterus for the purpose of treatment planning and training of fetoscopic laser techniques, there is potential for it to be adapted. It is a significant advance on the 3D representations of the monochor- ionic placenta previously produced, using software modelling of overlapping image layers. This ‘virtual fetoscopy’ technique was reported to allow identification of the umbilical cord insertions and placental equator, but was unable to characterise the nature of the anastomoses seen, as blood flow within the vessels could not be assessed to be arterial or venous.14
Such co-registration techniques, between Doppler ultrasound, which assesses the direction and characteristics of anastomotic blood flow, and B-mode or MRI to show the structure of placental tissues and the uterus raise the possibility of a meaningful study of the in vivo assessment of placental anastomotic function, although quantification of blood flow remains problematic. A study quantified blood flow through AVAs and both shared and non-shared cotyledons in MCDA placentas, and then correlated the ultrasound findings with histological examination of the placenta.7 However, both vessel size (a circular
https://doi.org/10.1017/9781108915038.029 Published online by Cambridge University Press
MOVING volume
Figure 29.2 Schematic overview of the proposed MRI- 3D US registration methodology (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
Source: Torrents-Barrena et al. 2019 (13). TTTS-GPS: Patient-specific preoperative planning and simulation platform for twin-to-twin transfusion syndrome fetalsurgery. Computer Methods and Programs in Biomedicine, 179, 104993 (Reuse licence 4784840550036)
vessel was assumed and calculated from the radius) and velocity (not angle corrected, measured with Doppler optimised for higher flows than observed) calculations involved assumptions. These were appropriate methodologies employed to overcome the technical limitations of Doppler at the time, but potentially explain why the flow velocities recorded were inconsistent with previous studies where cotyledonary flows are typically reported around 3 ml/min, compared to the authors' findings of around 31 ml/min in this study, which appear supra-physiological. To date, there remains no accepted quantification of the flow through placental anastomoses or between monochorionic twins in complicated or uncomplicated pregnancies.
As a body of evidence, therefore, these studies remain a proof of principle that anastomoses can be identified but do not suggest a standard procedure to identify, type and record the presence of placental anastomoses - the basis of making an ultrasound ‘map' of the placenta for use as a reproducible screening tool. Without this the value of such studies as prognostic indicators of pregnancy outcomes cannot be inferred.
While MRI has not been the leading technology in assessment of placental anastomoses, both diffusion-weighted (DWI-MRI) and blood-oxygenation-level-dependant (BOLD- MRI) imaging have been used to investigate the function of the materno-fetal interface in multiple as well as singleton pregnancies.
The DWI-MRI is a measure of tissue integrity; this can be assessed quantitatively as the apparent diffusion coefficient (ADC), where the impedance of water molecules due to tissue cellularity and the presence of intact cell membranes is calculated. The ADC is not thought to change during placental maturation despite progressive structural changes, increase in parenchyma and angiogenesis during gestation in singleton pregnancies. Neither is ADC affected by uncomplicated twin pregnancy, in either monochorionic or dichorionic twin pregnancy.16 However, ADC is different between the recipient and donor portions of a monochorionic placenta affected by TTTS, a disparity not seen in uncomplicated monochorionic pregnancy. The ADC is also different in the donor portion of the placenta, but not the recipient portion, when compared to uncomplicated MCDA placentae, which suggests an accumulation of tissue damage within the donor portion of the placenta.17
Independent assessment of placental damage may be a useful adjunct in understanding whether TTTS is likely to progress, remain stable or spontaneously improve, although there is currently no evidence to support this. Multiple groups investigating the cardiovascular function of twins affected by TTTS have reported that placental impedance has a role to play in cardiac remodelling, acquired right ventricular outflow tract abnormalities and the risk of fetal demise following intrauterine procedures or the death of a cotwin. Placental damage such as that suggested by ADC could feasibly account for such acquired placental impedance; however, this remains speculative in the absence of further evidence.
The BOLD-MRI is a tool for visualising tissue and placental oxygenation, exploiting the differences in T2* weighted signal of deoxy- and oxyhaemoglobin in blood. As such, it provides an alternative to gadolinium-enhanced MRI, given the associated risk of adverse pregnancy and neonatal outcomes associated with gadolinium usage. In both monochor- ionic and dichorionic twins, inter-twin differences in placental oxygen time-to-plateau maps were independent predictors of sIUGR and enhanced the sensitivity and specificity of ultrasound-based estimation of discrepancy in estimated fetal weight alone.18,19 The use of BOLD-MRI has not been reported in TTTS at the time of writing.
Non-invasive Diagnosis of Chromosomal Abnormality and Genetic Disease
Non-invasive prenatal testing for chromosomal abnormalities and non-invasive prenatal diagnosis (NIPD) are the most obvious non-invasive fields in which multiple pregnancy management lags behind that of singleton pregnancy. Non-invasive prenatal testing is currently recommended with caution in twin pregnancies as it has poorer sensitivity and specificity than in singleton pregnancy, but it is still superior to other available screening modalities.
Existing NIPT providers use a variety of platforms to perform screening: nextgeneration targeted SNP-based, targeted and massively parallel shotgun sequencing methods have all been reported by companies, each used with its own proprietary algorithms to interpret the results. Research groups have reported that SNP-based NIPT techniques appear to have high specificity for trisomies 21,18 and 13 in addition to zygosity and fetal sex in both monochorionic and dichorionic twins.20 There is potentially a limited role for assessment of zygosity using NIPD. As previously discussed chorionicity is the most important predictor of outcome in multiple pregnancy and therefore dictates the intensity of antenatal screening. In situations where it is not possible to assign chorionicity with ultrasound such a technique could provide additional information.
A key issue when understanding NIPT usage in multiple pregnancy is that while maternal serum has an overall higher fetal fraction when compared to singleton pregnancy, there is a smaller contribution per fetus, making failure more likely. It may be possible to overcome this limitation using low-coverage, paired-end, whole-genome sequencing of maternal plasma: in one study a sufficient fetal fraction was obtained for screening of triplet, quadruplets, sextuplets and octuplets in addition to twins as a proof of principle. It is therefore possible to envisage a situation in which NIPT could play a larger role in diagnosis of aneuploidy and genetic conditions in multiple pregnancies.
Non-invasive Intrauterine Treatments
In the past decade high-intensity focused ultrasound (HIFU) has been proposed as a non- invasive treatment which may be suited for use in fetal and placental therapies. It is an established non-invasive method of ablating soft tissue and occluding blood vessels which has been in clinical usage since the 1990s. It uses ultrasound waves generated by an externally placed ultrasound transducer to produce localised tissue necrosis at depth due to a combination of thermal and/or mechanical effects. The ultrasound energy ideally passes through overlying tissue without causing damage to converge in a small region (the focus) where the increase in temperature or changes in pressure is sufficient to ablate tissue or occlude vessels. As such, HIFU technology is reliant on diagnostic imaging modalities such as ultrasound or MRI to direct the HIFU focus to the target tissue.
In obstetrics and gynaecology HIFU has been used for the treatment of uterine fibroids, endometriosis, adenomyosis and caesarean scar pregnancy, using MRI guidance, with a low rate of complications.21 In a research setting ultrasound-guided HIFU has been reported as the treatment for monochorionic twins with TRAP sequence: in about half of these cases blood flow to the acardiac twin was successfully occluded and no significant maternal or fetal adverse outcomes were reported.22 In this application researchers used HIFU to target the soft tissues surrounding the cord insertion of the acardiac twin to effect cord occlusion. This ultrasound-guided HIFU technique could be adapted to perform selective fetal reduction when indicated.
High-intensity focused ultrasound has also been suggested as a non-invasive method of treating fetal conditions such as TTTS, where access to blood vessels is restricted or associated with the risks of iatrogenic pregnancy loss.23,24 Recently preclinical studies have been used to demonstrate the feasibility, high efficacy and materno-fetal safety of using ultrasound-guided HIFU to selectively occlude placental blood vessels in an animal model.25,26,27 In these studies colour Doppler was used to identify placental vessels and direct the HIFU focus in order to occlude them through intact maternal abdominal skin. High rates of successful selective occlusion (93-100%) of targeted placental vessels were reported without excessive destruction of placental tissue. In later studies persistent vascular occlusion of placental vessels for up to 21 days was also demonstrated histologically. A combination of invasive and non-invasive techniques was employed to monitor maternal and fetal cardiovascular, metabolic, acid-base, stress responses and fetal growth and development patterns both during and following HIFU medicated placental vascular occlusion. The overall conclusion of this work was that HIFU mediated selective placental vascular occlusion appeared to be well tolerated in the mother and fetus in both the short and long term with no discernible adverse effects. However, as in the treatments for TRAP sequence, maternal abdominal skin erythema did result in a proportion of exposed subjects.22
Based on this research the clinical applications are clear and could in addition to HIFU include non-invasive treatment for TRAP and selective reduction in monochorionic pregnancy. A phase 1a clinical trial is currently being designed for the non-invasive treatment of TTTS using HIFU in human pregnancy.28 The intention is to target the HIFU focus using colour Doppler modalities optimised to the low-flow placental vessels. If non-invasive ablation of blood vessels using ultrasound-guided HIFU was successful, this would represent a paradigm shift in the treatment of the condition. As previously discussed, fetoscopic laser has not been shown to confer a survival advantage when compared to amniodrainage, in part due to the associated risk of procedure-related pregnancy loss.[3] [4] Hence a treatment which is able to occlude placental anastomoses without breaching the intrauterine space would have the potential to deliver the therapeutic benefit of anastomotic occlusion without the associated risks of invasive fetoscopy itself. Such a treatment also lends itself better to retreatment of recurrent disease. Furthermore, following fetoscopic laser, 5-35% of mono- chorionic placental retain residual anastomoses deep within the placenta,29 and up to 16% of cases have recurrent disease due to this, which has been shown to have a worse prognosis.30 Given that laser as a technology has a limited depth to which it can ablate tissue, there is again a case for a technology such as HIFU which can occlude vessels at any depth within the placental tissue.
References
transfusion syndrome. Cochrane Database
Syst Rev 2014;1:CD002073.
3. Grigsby PL. Animal models to study placental development and function throughout normal and dysfunctional human pregnancy. Semin Reprod Med 2016;34(1):11-16.
4. Kaiser J. Reproductive biology. Gearing up for a closer look at the human placenta. Science 2014;344(6188):1073.
5. Taylor MJ, Denbow ML, Tanawattanacharoen S, Gannon C, Cox PM, Fisk NM. Doppler detection of arterio-arterial anastomoses in monochorionic twins: feasibility and clinical application. Hum Reprod 2000; 15 (7):1632-6.
6. Machin GA, Feldstein VA, Van Gemert MJ, Keith LG, Hecher K. Doppler sonographic demonstration of arterio-venous anastomosis in monochorionic twin gestation. Ultrasound Obstet Gynecol 2000;16(3):214-17.
7. Wee LY, Sullivan M, Humphries K, Fisk NM. Longitudinal blood flow in shared (arteriovenous anastomoses) and non-shared cotyledons in monochorionic placentae. Placenta 2007;28(5-6):516-22.
8. Sun W, Cai A. OP12.03: 3D high-definition flow combined with tomographic ultrasound imaging in observation of placental vascular anastomoses in monochorionic twins. Ultrasound Obstet Gynecol 2019;54(S1):124-.
9. Sato T. Technological description of advanced dynamic flow in the aplio diagnostic ultrasound system. eMedical Review, Toshiba Corporation, 2003.
10. Mack LM, Mastrobattista JM, Gandhi R, Castro EC, Burgess APH, Lee W. Characterization of placental microvasculature using superb microvascular imaging. J Ultrasound Med 2019;38(9):2485-91.
11. Girardelli S, Shaw C, Lees C. OP12.02: Mapping of the placental angioarchitecture in monochorionic twin pregnancies using different colour Doppler filters. Ultrasound Obstet Gynecol 2019;54(S1):123.
12. Nakata M, Martinez JM, Diaz C, Chmait R, Quintero RA. Intra-amniotic Doppler measurement of blood flow in placental vascular anastomoses in twin-twin transfusion syndrome. Ultrasound Obstet Gynecol 2004;24(1):102-3.
13. Torrents-Barrena J, Lopez-Velazco R, Piella G et al. TTTS-GPS: patient-specific preoperative planning and simulation platform for twin-to-twin transfusion syndrome fetal surgery. Comput Methods Programs Biomed 2019;179:104993.
14. Werner H, Dos Santos JL, Sa RA et al. Visualisation of the vascular equator in twin-to-twin transfusion syndrome by virtual fetoscopy. Arch Gynecol Obstet 2015;292(6):1183-4.
15. Denbow ML, Taylor M, Cox P, Fisk NM. Derivation of rate of arterio-arterial anastomotic transfusion between monochorionic twin fetuses by Doppler waveform analysis. Placenta 2004;25 (7):664-70.
16. Shapira-Zaltsberg G, Grynspan D, Reddy D, Miller E. Apparent diffusion coefficient of the placenta in twin versus singleton pregnancies. Fetal Diagn Ther 2018;44(2):129-34.
17. Fu L, Zhang J, Xiong S, Sun M. Decreased apparent diffusion coefficient in the placentas of monochorionic twins with selective intrauterine growth restriction. Placenta 2018;69:26-31.
18. Poulsen SS, Sinding M, Hansen DN, Peters DA, Frokjaer JB, Sorensen A. Placental T2* estimated by magnetic resonance imaging and fetal weight estimated by ultrasound in the prediction of birthweight differences in dichorionic twin pairs. Placenta 2019;78:18-22.
19. Luo J, Abaci Turk E, Bibbo C et al. In vivo quantification of placental insufficiency by BOLD MRI: a human study. Sci Rep 2017;7 (1):3713.
20. Norwitz ER, McNeill G, Kalyan A et al. Validation of a single-nucleotide polymorphism-based non-invasive prenatal test in twin gestations: determination of zygosity, individual fetal sex, and fetal aneuploidy. J Clin Med 2019;8(7).
21. Chen J, Chen W, Zhang L et al. Safety of ultrasound-guided ultrasound ablation for uterine fibroids and adenomyosis: a review of 9988 cases. Ultrason Sonochem 2015;27:671-6.
22. Seo K, Ichizuka K, Okai T et al. Treatment of twin-reversed arterial perfusion sequence using high-intensity focused ultrasound. Ultrasound Obstet Gynecol 2019 Jul;54(1):128-34.
23. Shaw CJ, Ter Haar GR, Rivens IH, Giussani DA, Lees CC. Pathophysiological mechanisms of high-intensity focused ultrasound-mediated vascular occlusion and relevance to non-invasive fetal surgery. J R Soc Interface 2014; 11 (95):20140029.
24. Caloone J, Huissoud C, Vincenot J et al. High-intensity focused ultrasound applied to the placenta using a toroidal transducer: a preliminary ex-vivo study. Ultrasound Obstet Gynecol 2015;45 (3):313-19.
25. Shaw CJ, Civale J, Botting KJ et al. Noninvasive high-intensity focused ultrasound treatment of twin-twin transfusion syndrome: A preliminary in vivo study. Sci Transl Med 2016;8 (347):347ra95.
26. Shaw CJ, Rivens I, Civale J et al. Transabdominal in vivo placental vessel occlusion using high intensity focused ultrasound. Sci Rep 2018;8(1):13631.
27. Shaw CJ, Rivens I, Civale J et al. Maternal and fetal cardiometabolic recovery following ultrasound-guided high-intensity focused ultrasound placental vascular occlusion. J R Soc Interface 2019;16(154):20190013.
28. ISTCRN registry. Developing a non- invasive treatment for twin-twin transfusion syndrome. https://doi.org/10.1186/ISRCTN33458649
29. Chmait RH, Assaf SA, Benirschke K. Residual vascular communications in twin-twin transfusion syndrome treated with sequential laser surgery: frequency and clinical implications. Placenta 2010;31 (7):611-14.
30. Walsh CA, McAuliffe FM. Recurrent twintwin transfusion syndrome after selective fetoscopic laser photocoagulation:
a systematic review of the literature. Ultrasound Obstet Gynecol 2012;40 (5):506-12.
More on the topic New Frontiers in Multiple Pregnancy Management:
- Single and Double Fetal Loss in Twin Pregnancy
- CHAPTER FOUR Town and Country Urban devotions and rural rituals