Management of Twin-Reversed Arterial Perfusion (TRAP) Sequence
Werner Diehl
The Facts (What We Know)
Twin-reversed arterial perfusion (TRAP) sequence is a rare complication of monochorionic twinning characterised by reverse (retrograde) perfusion of one of the twins via abnormal placental arterio-arterial anastomoses, with the consequence of completely disrupted and malformed fetal development.
Typically, the affected fetus has an absent or rudimentary heart and is therefore referred to as the ‘acardiac twin' and the unaffected twin is known as the ‘pump twin' since it haemodynamically supplies the acardiac twin completely. As a consequence of this burden, there is a high risk of heart failure and intrauterine death of the pump twin, as well as development of polyhydramnios, preterm birth and neonatal death. As a result, the survival rate of the pump twin is approximately only 50-60%. Twin- reversed arterial perfusion can also occur in monochorionic triplets or higher-order mono- chorionic pregnancies.Historically, the incidence of TRAP sequence has been reported as a very rare abnormality affecting 1 in 35,000 pregnancies or 1% of monochorionic twins. However, a recent study concluded that the incidence is higher at around 1 in 10,000 pregnancies or 2.6% of monochorionic twins.1 The study found that when taking into account recent more robust statistics and the effect of assisted reproductive therapy on the increased rate of multiple pregnancies seen in recent decades in general, and the increased proportion of monochor- ionic twins in particular, this diagnosis can be expected more frequently than previously assumed.
Furthermore, among the fundamental conditions believed to be required for an acardiac twin pregnancy to occur, one is the existence of at least a set of one arterio-arterial (AA) and one veno-venous (VV) placental anastomoses, as further discussed later in this chapter.
When seen from the embryological perspective of placental vascular development, one in eight monochorionic twins with a placenta with this particular configuration of anastomoses could be affected by TRAP sequence. However, early spontaneous cessation of retrograde perfusion to the acardiac twin or demise of the pump twin and pregnancy loss may contribute to the reported lower incidence of 2.6%.The precise mechanisms involved in the development of acardiac twin malformation are not well known, as only snapshot observations of early embryonic and fetal pathology specimens are available. However, as mentioned earlier, some fundamental prerequisites appear to be required for the occurrence of an acardiac twin. Before going into these prerequisites, it is important to look at the timeline of post-zygotic twinning and the point in time at which a splitting occurs, since in monozygotic twins this is of key importance in the understanding of different types of chorionicity and amnionicity.
It is generally accepted that splitting of the fertilised oocyte leads to monozygotic (MZ) ‘identical’ twins and that if cleavage occurs as early as within the first three days post conception (i.e. before differentiation of cells that will contribute to the placenta), two separate placentae with two separate amniotic sacs will develop, leading to monozygotic dichorionic (DC) diamniotic (DA) twins. Around 20-30% of MZ twins are believed to have this origin. In contrast, if splitting occurs between day 3 and day 9 (after differentiation of chorionic precursor cells, but before development of amnion precursor cells), one common placenta with two separate amniotic cavities will be the result. This gives rise to mono- chorionic (MC) diamniotic (DA) twins, and 70-80% of MZ twins have this origin. If splitting occurs between days 9 and 12 (after differentiation of amnion cells), separation into two amniotic sacs then is no longer possible and the result will be monoamniotic (MA) twins.2 Around 5% of MZ twins will have this origin.
Although the exact point in time and mechanism of origin in conjoined twins is controversial, it is hypothesised that an even later splitting after 12 days may be involved in their origins, if following the fission theory (incomplete separation of embryonic structures). However, due to the different anatomical sites of non-separation observed in conjoined twins, fusion processes in monoamniotic embryos seem plausible as well (fusion theory). Conjoined twinning and other forms of aberrant twinning (e.g. extra-parasitic twins, endo-parasitic twins) are beyond the scope of this chapter but are in general most likely related to intrinsic embryonic developmental disorders. Although the majority of acardiac twins are diamniotic, a number of them prove to be monoamniotic and therefore other factors different than the timing of their splitting process are most likely involved in their genesis.It is increasingly accepted that the process of MZ twinning rather rarely results in an equal splitting of the inner cell mass in the stage of the blastocyst. Presumably due to intrinsic genetic, epigenetic and intercellular processes not all yet elucidated, it is more likely that if a splitting is to occur, the majority of events will result in unequal number of cells that will thereafter be available to develop the corresponding future embryos.3 This fact, apart from contributing to the general observation that MZ twins rarely are ‘truly’ identical, may have the consequence that one of the future embryos, although initially having the potential to develop normally, would display a slightly more ‘retarded’ evolution. This may result in significant differences in vascularisation, cardiac development and perfusion that may underlie the spectrum of complications typical to MC twins, ranging from twin-twin transfusion syndrome (TTTS) to selective fetal growth restriction (sIUGR). But in the case of acardiac twinning, an unequal number of cells as embryonic precursors may lead to either intrinsic cardiac abnormalities in the affected embryo or the development of aberrant placental vascular anastomoses, or even both.
Furthermore, it is possible that an unequal inner cell mass segregation may also affect development of the corresponding chorionic vascular territories, later resulting in unequal placental sharing (as underlying cause of selective growth restriction and as contributing cause in TTTS).Another prerequisite is the coexistence of a haemodynamically dominant set of one AA and one VV anastomoses (see earlier in this chapter) on the placenta, and it is then the combination of all these factors that may lead to a progressive retrograde perfusion of the smaller embryo. Favoured by a lower resistance, transfusion of deoxygenated blood via the AA anastomosis from the dominant pump twin to the smaller embryo in a reversed fashion is the most likely cause for major structural abnormalities in the affected twin. As a consequence, typically the acardiac twin shows some normal development of lower extremities but severe and bizarre malformations of the upper body (missing/abnormal upper limbs and acrania). After arterial retrograde perfusion of the acardiac mass, further desaturated blood returns to the pump twin via the VV anastomosis, bypassing the placenta and increasing its cardiac preload. This hemodynamic burden results in chronic hyperdynamic heart failure in the pump twin, causing hydrops and intrauterine death, polyhydramnios and preterm birth.
In some cases, perhaps due to increasing oedema and increasing vascular resistance within the acardiac mass, spontaneous cessation of retrograde flow can occur. In a series of 24 cases of TRAP, it was found that after diagnosis during first trimester and subsequent reevaluation at 16 to 18 weeks, in 21%, there was spontaneous arrest of flow to the acardiac twin.4 However, during this period of time, there was demise of the pump twin in 33% of cases and persistent flow to the acardiac twin in 46% of cases. This important observation has strengthened the rationale for intervention in the first trimester.
Advances in ultrasound technology and high-resolution imaging have allowed a shift in the diagnosis of TRAP sequence from the second to the first trimester.
But irrespective of gestational age, the ultrasound diagnosis of TRAP sequence can be established when in a monochorionic twin pregnancy besides a structurally normal co-twin, a hydropic mass of tissue with some skeletal structures (in particular vertebral structures, pelvis and lower limbs) and colour Doppler evidence of retrograde blood flow is visualised. Although in some cases, an inter-twin membrane maybe absent due to monoamnionicity, amniotic fluid can be reduced in the sac of the acardiac twin in a diamniotic setting and the inter-twin membrane may be difficult to identify. However, careful identification of the inter-twin membrane is important, as this does have major implications for therapeutic options. Additional typical findings include that the umbilical cord of the acardiac twin is frequently thinner and shorter than that of the pump twin and contains only two vessels in the majority of cases. However, if gestational age is more advanced, the cord can be thickened by hydropic changes and this too may have implications for therapeutic options. A more detailed examination of the placental topography will reveal in most of the cases one AA and one VV anastomosis between both cord insertions. Cord insertions frequently are close to each other, although in more rare cases, the cord of the acardiac inserts laterally onto the cord of the pump twin.Although the use of colour Doppler in the first trimester should be limited to the minimum necessary, in the presence of an intra-amniotic hydropic tissue mass aside of a normal co-twin, its use is key for the diagnosis of TRAP sequence since it will demonstrate retrograde perfusion of the acardiac twin. Key ultrasound diagnostic features, signs of poor prognosis and their descriptions are summarised in Tables 15.1 and 15.2 respectively.
The Issues (What We Do Not Know)
Our current understanding of the origin of the acardiac twinning process is still incomplete. As discussed earlier in this chapter and inherent to the limited possibilities of accurate observation of early human development, the process of monochorionic splitting and distribution of inner cell masses of the future embryos and their placental sharing escapes our capabilities.
However, multiple factors certainly are involved when the outcome of the splitting process is adverse as in acardiac twinning. Not only the point in time of splitting, but also an unequal number of cells splitting off in the inner mass and destined to develop into future embryos, as well as development and coexistence of AA and VV anastomoses inhttps://doi.org/10.1017/9781108915038.015 Published online by Cambridge University Press
Table 15.1 Key ultrasound signs for diagnosis of twin-reversed arterialperfusion sequence
| Diagnostic signs of TRAP sequence | Description |
| MC placenta (MC twin pregnancy) Presence of hydropic tissue mass AND (normal) co-twin | Presence of a single placenta Besides a structurally normal co-twin, a hydropic mass of tissue with some skeletal structures can be seen (vertebrae, pelvic bones, lower limbs) with absence of a heartbeat (caveat: rudimentary cardiac structures are possible) and absence of a cranial vault (hence the term 'acardius acranius,). |
| Retrograde perfusion of acardiac twin (colour Doppler) | Colour Doppler demonstrates retrograde perfusion of acardiac twin: Typically blood flow is seen entering the acardiac tissue mass at the abdominal region and ascending along the abdominal aorta to reach the thoracic area. In some cases, intrinsic pulsations of rudimentary heart structures can be seen. Blood flow then is seen to return via a former intra-fetal umbilical vein to the cord of this acardiac twin. Some cases may present already without any demonstrable blood flow in the acardiac twin (spontaneous cessation of retrograde perfusion). |
| Close cord insertions | Cord insertions of the pump twin and the acardiac twin are topographically close together in most cases. In rare cases, cord insertion of the acardiac twin may even arise directly from cord insertion of pump twin in a lateral fashion. |
| Placental AA and VV anastomoses | Detailed assessment of the chorionic plate between both cord insertions using colour Doppler may reveal the presence of at least one AA and one VV anastomoses. |
| Thin umbilical cord with two vessels | The umbilical cord of the acardiac twin can be thinner as compared to the pump twin. However, if the acardiac twin is hydropic, its umbilical cord may be thick and hydropic as well. |
Table 15.2 Signs of poor prognosis in twin-reversed arterialperfusion sequence
| Signs of poor prognosis | Description |
| Large acardiac twin | The acardiac twin's largest diameters can be used to compare its estimate weight with the pump twin's weight. Ifit is more than 50% of the weight of the pump twin, its haemodynamic effect is most likely to negatively impact the pump twin. |
| Signs of cardiac decompensation of pump twin (abnormal ductus venosus flow, tricuspid regurgitation, hydrops) | The presence of reverse flow (reversed a-wave) in the ductus venosus (DV) in the pump twin may be interpreted as a sign of cardiac distress in the context of TRAP sequence. Cardiac decompensation is even more likely if the pump twin shows signs of hydrops (ascites, pericardial or pleural effusions, skin oedema) or abnormal umbilical Doppler flow. |
| Monoamniotic pregnancy | Cord entanglement is known to be present in almost all monoamniotic twins as early as the first trimester. As in all monoamniotic twins, cord complications most likely accounts for the majority of fetal losses in acardiac twins. |
| Low resistance in umbilical artery of acardiac twin | Low-resistance umbilical blood flow in the acardiac twin or within its tissue mass (i.e. increased end-diastolic flow) makes spontaneous cessation of flow less likely and confirms haemodynamic burden of the pump twin's circulation. |
the future chorionic plate, most likely need to coincide with and contribute to this abnormal phenomenon.
Although the study mentioned before points to the rationale for early intervention, we don't exactly know when and how this should be undertaken.4 Heterogeneity of existing studies and paucity of robust statistics with limited number of cases do not allow a conclusive management strategy.
A case series and meta-analysis on optimal method and timing of interventions for TRAP found that when the diagnosis is established in the first trimester and intervention delayed until the second trimester, there is 60% spontaneous cessation of blood flow to the acardiac twin. However, in these cases, there is death of the pump twin or brain damage thereafter in up to 61%. Along with the lack of predictive ultrasound signs for subsequent fetal demise if expectantly managed, and the lack of benefit of delaying an intervention in terms of improved survival rates, elective intervention at 12-14 weeks appears to be indicated in TRAP.5 Addressing the method of choice, the study concludes that intra-fetal laser appears to be the technique most likely to prevail.
In an attempt to definitively shed light on the best time for intervention, an international multicentre randomised trial is underway and will recruit women with a first-trimester diagnosis of TRAP and compare early intervention between 12 and 14 weeks (intra-fetal coagulation) versus late intervention between 16 and 19 weeks (intra-fetal or fetoscopic coagulation) (TRAPIST = TRAP Intervention Study).6 To optimise outcomes and reproducibility, the procedures will be undertaken by experienced operators and the techniques standardised.
Long-term neurodevelopmental outcomes after TRAP sequence also need further investigation, taking into account if managed with early or late intervention, and as compared to expectant management. Again here, standardisation not only of procedure type and timing is of key importance, but also of neurodevelopmental tests to allow definitive conclusions.
Management Options
A variety of intrauterine interventions have been used in the treatment of TRAP. Historically, second-trimester ultrasound guided interventions and posteriorly fetoscopic approaches have been implemented with the aim of coagulation of the umbilical cord of the acardiac twin. Intra-fetal techniques targeting vessels within the body of the acardiac have successfully been used as well. However, in recent years, the tendency to earlier and less invasive techniques has become stronger, mostly involving ultrasound guided intra-fetal laser or radiofrequency coagulation of vessels within the acardiac twin. However, it is the gestational age at which the diagnosis of TRAP is established in a particular case that will define the treatment options available.
Expectant Management
Gestational age at diagnosis plays a key role in the management of TRAP sequence. When diagnosed during the first trimester (11-13+6 weeks), in around one-third of cases, demise of the pump twin will occur if managed expectantly.4 This observation has led to the implementation of earlier and less invasive therapeutic options than fetoscopy, and a number of recent studies have shown that early intervention may result in improved survival rates and perinatal outcomes.
However, in selected cases, expectant management may achieve satisfactory outcomes. In particular, a small size of the acardiac twin at diagnosis has been used as criteria for this option.7 For instance, a survival rate of 88% was reported if the calculated weight of the acardiac twin was less than 50% the weight of the pump twin. However, the numbers in these series were very small and no definitive conclusion can be drawn from these findings. Spontaneous flow arrest may be likely in these cases and invasive interventions with their inherent risks could be avoided, but spontaneous demise of pump twins with small acardiac twins has also been reported. However, if a small-sized acardiac twin presents in combination with high-resistance umbilical flow or intra-fetal blood flow shows low peak velocities, expectant management may be justified since spontaneous cessation of retrograde perfusion is likely. Close surveillance to detect deterioration of the pump twin or increasing retrograde perfusion to the acardiac twin may, however, indicate the need for intervention, as does rapid growth of the acardiac mass. Regardless of gestational age at diagnosis, and especially in the presence of signs of poor prognosis (Table 15.2), most parents may opt for intervention, more so if the diagnosis is established during the first trimester.
If no retrograde flow to the acardiac twin is detected by colour Doppler (at diagnosis or after spontaneous cessation in a follow-up review), expectant management is indicated as the goal of any invasive treatment - that is, the interruption of flow to the acardiac twin - has spontaneously occurred. Perinatal outcomes are very good with survival rates reaching 100% and gestational age at delivery beyond 36 weeks.7 However, the patient needs to be aware that sudden demise of the pump twin may still occur, especially in monoamniotic TRAP. Invasive cord transection in monoamniotic acardiac twins, even with arrested flow to the acardiac at presentation or during follow-up should be discussed with the parents, since there is persistent risk of tightening of cord entanglement due to retraction of necrotising cord tissues.8 In monoamniotic TRAP, with active retrograde perfusion of the acardiac at diagnosis during the first trimester, expectant management is not recommended, but the intervention should be delayed until beyond 16 weeks, when fetoscopy with cord coagulation and cord transection becomes feasible. When compared to cord occlusion in monoamniotic discordant twins, additional cord transection appears not to have a significant impact on outcomes apart from a longer operative time.9
Early Intervention (12-14 Weeks)
The aim of this minimally invasive procedure is to coagulate and stop blood flow in the acardiac twin by means of laser or radiofrequency energy, with the use of a needle which is much thinner than a fetoscope. In order to achieve this, usually a 17G or 18G needle is percutaneously inserted under ultrasound guidance, using maternal local anaesthesia, into the body of the acardiac twin (intra-fetal) at the level of its abdominal cord insertion and pelvic area. This is undertaken in tertiary centres with appropriate equipment and expertise. Although a transamniotic approach is preferred, leaving the sac of the pump twin intact, sometimes an extensive anterior placenta cannot be avoided, resulting in transplacental access to the acardiac fetus. Since it is unclear whether the latter has an impact on outcomes in this procedure, maternal safety and a clear needle path and target entry justify this approach. Once the needle tip is in close proximity of the target vessels, a 400 nm laser fibre or radiofrequency (RF) device is passed through and activated. Colour Doppler is used to determine and confirm retrograde blood flow arrest before retrieving the laser fibre or RF device. After needle extraction, fetal heart rate in the pump twin should be documented and again cessation of retrograde flow to the acardiac twin should be confirmed. Although incomplete coagulation with persistence of flow may require a repeated procedure, this is unlikely in expert hands.
Most centres using early intra-fetal laser coagulation (between 12 and 14 weeks) have reported an overall survival rate of 80-90%. A recent small retrospective series reported survival rates of up to 91.7% with the majority of pregnancies reaching 39 weeks at delivery.10 When compared with late intervention, another study found a reduced rate of premature rupture of membranes, a lower incidence of delivery before 34 weeks and significantly higher birthweight, at comparable survival rates and rate of demise of the pump twin.11 Although with statistically limited power, these outcomes are adding evidence in favour of early intervention as compared to second-trimester intervention. A recent review on current treatment options also comes to the conclusion in favour of early intervention.12
Late Intervention (after 16 Weeks)
If after early diagnosis expectant management until a second-trimester intervention is chosen, or if first establishment of the diagnosis of TRAP is during the second trimester, most commonly an intra-fetal radiofrequency ablation or fetoscopic laser coagulation is offered. Although a number of different techniques have been used, these two approaches have become the most frequently used. Although intra-fetal laser coagulation may also be used in second-trimester intervention, it rather is preferred for first-trimester treatment. However, the use of intra-fetal radiofrequency ablation at this gestational age has reported survival rates of 80% and gestational ages at delivery beyond 36 weeks.13 Ultrasound-guided or fetoscopic bipolar coagulation also represents a common alternative, especially for cases where advanced hydrops of the acardiac and its cord anticipate limitations of laser coagulation.
Inherent to the procedure, fetoscopy is more invasive than intra-fetal coagulation as it involves insertion of fetoscopes of 2-2.8 mm in diameter with a working channel for a laser fibre, similarly as used for the management of severe mid-trimester TTTS. Preoperative evaluation of amnionicity and placental topography are key to a successful procedure. Once vascular anastomoses (AA and VV) on the chorionic plate have been visualised at fetoscopy, laser coagulation is undertaken to stop retrograde perfusion to the acardiac fetus. This is confirmed intraoperatively with the use of colour Doppler. However, if fetoscopic access to the anastomosis is impaired or the cord to the acardiac directly arises from the cord of the pumping twin, cord coagulation is undertaken. This may be more difficult to achieve as the cord to the acardiac may be thick or hydropic or the flow is high due to advanced gestational age. In this situation, bipolar coagulation may be used primarily (if technical complications are anticipated at the time of diagnosis), or secondarily (during fetoscopy). If so, a second entry trocar may be inserted to pass the bipolar forceps. It is used either to electro-coagulate the cord or just to compress it to reduce flow and then use laser energy to coagulate cord vessels. A second entry may not significantly increase the rate of premature rupture of membranes or miscarriage, as shown in a series and the likelihood of its necessity was reported to be 15% if the procedure was undertaken after 18 weeks.14
As previously discussed, in monoamniotic acardiac twins the aim of intervention is not only to stop retrograde perfusion, but additionally to address the risk of cord complications. Therefore, after coagulation of two segments of the cord of the acardiac twin (usually close to its abdominal insertion to ensure identification), cord transection between these segments is undertaken using laser energy. Thereafter, cord disentanglement should be undertaken to minimise the risk of tightening of true knots or twists by retraction of necrotic cord tissues.8
When looking at data from the largest series and meta-analysis, in general, survival rates of fetoscopy range from 76% to 83% with the majority of pregnancies delivering after 36 weeks. The rate of procedure-related premature rupture of membranes can be estimated at around 7% and the rate of severe preterm birth (before 32 weeks) at around 7-20%.5,14,15
Management Options Conclusion
Although there is large heterogeneity in the available data and therefore only ranges of survival rates can be used for counselling patients, what we can say is that intervention has changed the natural course of these pregnancies, which otherwise would have a high risk of poor outcome. Current thinking is in favour of early intervention, but this has not been proven definitively. See Figure 15.1, which illustrates a common management approach.
https://doi.org/10.1017/9781108915038.015 Published online by Cambridge University Press
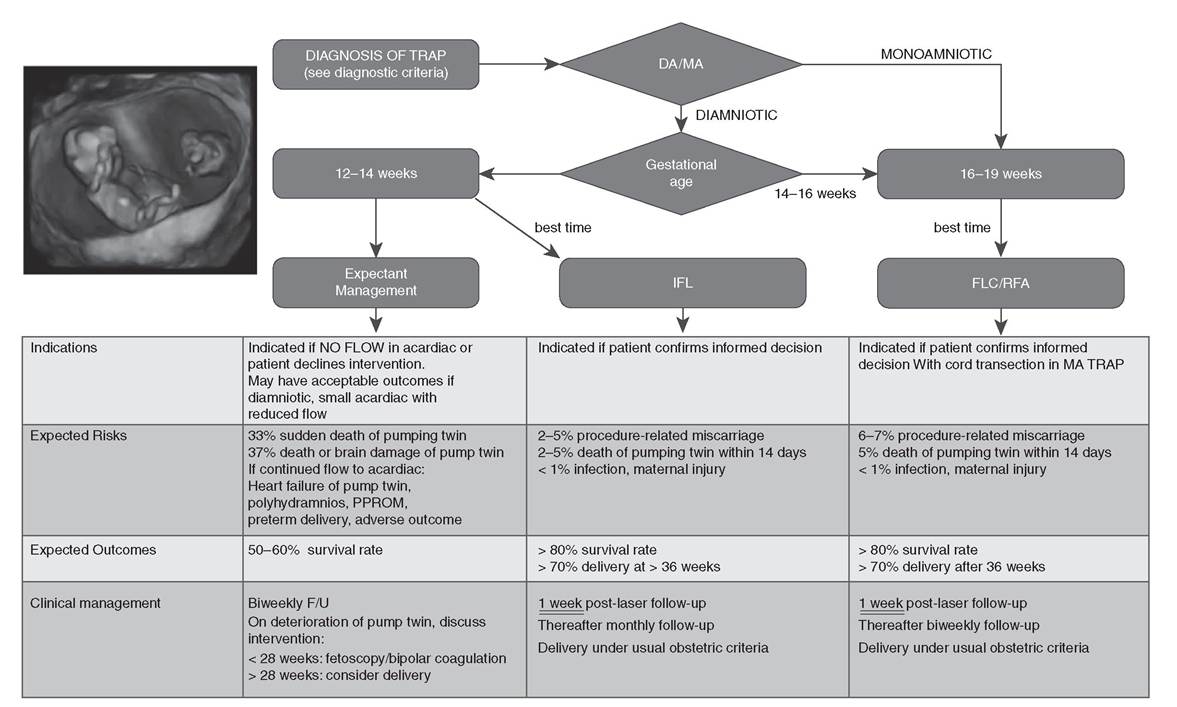
Figure 15.1 Management of TRAP sequence: once diagnosis has been established, amnionicity and gestational age at diagnosis play an important role in Clinicalmanagement. Monoamniotic (MA)TRAPshould be offered fetoscopic laser coagulation and cord transection at 16-19 weeks. In diamniotic (DA)TRAP, if diagnosis is early, intra-fetal laser (IFL) coagulation at 12-14 weeks most likely represents the best treatment option. Ifdiagnosis is made later, fetoscopic laser coagulation (FLC) of placentalanastomosesor cord coagulation can be offered. Intra- fetal radiofrequency ablation (RFA) represents an alternative with comparable outcomes as well. Ifdiagnosis is established between 14 and 16 weeks, expectant management untilsafer FLC or RFA can be undertaken is indicated, as higher rates of procedure-related rupture of membranes and miscarriage are observed.
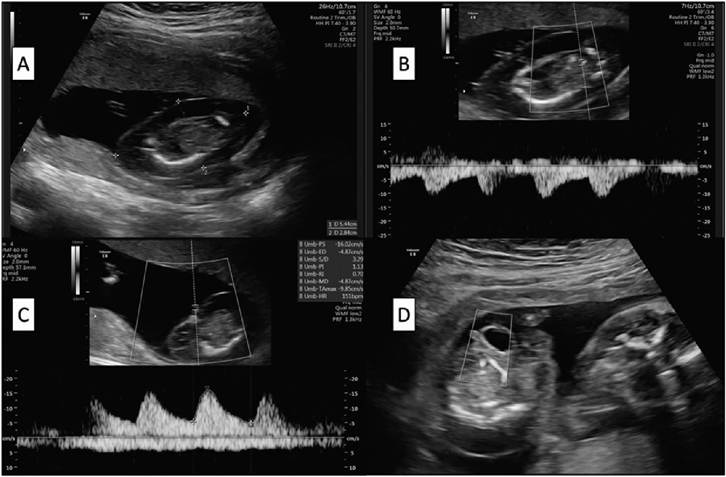
Figure 15.2 Ultrasound images of TRAP sequence: an acardiac twin with marked hydrops is seen (A). Low- resistance retrograde perfusion within the body of the acardiac is clearly seen in (B) in colour Doppler. Retrograde perfusion at the abdominal cord insertion can be detected in (C). Optimaltarget for interstitiallaser coagulation is the abdominal area of the acardiac due to confluence of vessels (D).
Key Points
• Twin-reversed arterial perfusion sequence is a complication of monochorionic twinning that occurs more frequently than previously thought.
• With increasing awareness, first-trimester diagnosis should be aimed for, as the latter is of key importance in its management.
• Intervention is associated with better outcomes compared with expectant management.
• Even if the acardiac twin is small, there is a lack of reassuring predictive factors and intervention is advocated in view of the risk of death or brain damage of the pump twin.
• Although still unclear whether early intervention (i.e. in the first trimester) leads to better perinatal outcomes, recent data support this management.
• First-trimester intra-fetal laser coagulation is likely to become treatment of choice supported by its minimal invasiveness (18G needle technique, short operative time, outpatient/day-surgery setting) and acceptable survival rates.
• If diagnosis is late or there is deterioration during expectant management, intervention with fetoscopic laser coagulation of placental anastomoses or acardiac fetus cord coagulation or intra-fetal radiofrequency ablation can be offered with comparable outcomes, and the choice will depend on the clinician’s preference and expertise.
• The TRAPIST trial of early versus late intervention is expected to definitively answer the question about the best timing for intervention.
• In monoamnionicity, intervention can only be late as in addition to cord coagulation, cord transection is required.
References
1. Van Gemert MJ, Van den Wijngaard JP, Vandenbussche FP. Twin reversed arterial perfusion sequence is more frequent than generally accepted. Birth Defects Res A Clin Mol Teratol 2015;103(7):641-3.
2. Benirschke K. The monozygotic twinning process, the twin-twin transfusion syndrome and acardiac twins. Placenta 2009;30(11):923-8.
3. Machin G. Non-identical monozygotic twins, intermediate twin types, zygosity testing, and the non-random nature of monozygotic twinning: s review. Am J Med Genet Part C Semin Med Genet 2009;151C:110-27.
4. Lewi L, Valencia C, Gonzalez E, et al. The outcome of twin reversed arterial perfusion sequence diagnosed in the first trimester. Am J Obstet Gynecol 2010;203:213.e1-e4.
5. Chaveeva P, Poon LC, Sotiriadis A, Kosinski P, Nicolaides KH. Optimal method and timing of intrauterine intervention in twin reversed arterial perfusion sequence: case study and meta-analysis. Fetal Diagn Ther 2014;35:267-79.
6. TRAP Intervention STudy (TRAPIST). ClinincalTrials.gov: NCT02621645.
7. Jelin E, Hirose S, Rand L et al. Perinatal outcome of conservative management versus fetal intervention for twin reversed arterial perfusion sequence with a small acardiac twin. Fetal Diagn Ther 2010;27:138-41.
8. Berg C, Koenninger A, Gembruch U, Geipel A. Twin arterial reversed arterial perfusion (TRAP) sequence: does monoamnionicity preclude early intervention? Ultrasound Obstet Gynecol 2014;44:241-2.
9. Valsky DV, Martinez-Serrano MJ, Sanz M et al. Cord occlusion followed by laser cord transection in monochorionic monoamniotic discordant twins.
Ultrasound Obstet Gynecol 2011;37:684-8.
10. Tavares de Sousa M, Glosemeyer P, Diemert A, Bamberg C, Hecher
K. First-trimester intervention in twin reversed arterial perfusion sequence. Ultrasound Obstet Gynecol 2020;55:47-9.
11. Berg C, Holst D, Mallmann MR, Gottschalk I, Gembruch U, Geipel A. Early vs late intervention in twin reversed arterial perfusion sequence. Ultrasound Obstet Gynecol 2014;43:60-4.
12. Vitucci A, Fichera A, Fratelli N, Sartori E, Prefumo F. Twin reversed arterial perfusion sequence: current treatment options. Int J Womens Health 2020;12:435-43.
13. Lee H, Bebbington M, Crombelholme TM, North American Fetal Therapy Network. The North American Fetal Therapy Network Registry data on outcomes of radiofrequency ablation for twin-reversed arterial perfusion sequence. Fetal Diagn Ther 2013;33(4):224-9.
14. Diehl W, Hecher K. Selective cord coagulation in acardiac twins. Semin Fetal Neonatal Med 2007;12(6):458-63.
15. Pagani G, D'Antonio F, Khalil A, Papageorghiou A, Bhide A, Thilaganathan B. Intrafetal laser treatment for twin reversed arterial perfusion sequence: cohort study and meta-analysis. Ultrasound Obstet Gynecol 2013 Jul;42 (1):6-14. https://doi.org/10.1002/uog.12495