Management of Fetal Growth Pathology in Multiple Pregnancy
Nikolaos Antonakopoulos and Asma Khalil
Introduction
The advances in assisted reproductive techniques combined with the advanced age of women trying to conceive has led to increased implementation of these techniques in order to overcome fertility barriers.
An inevitable consequence of assisted reproduction is the raised incidence of multiple pregnancies, mainly twin pregnancies.1Twin pregnancies are known to have significantly higher rates of perinatal morbidity and mortality than singleton pregnancies. This is related not only to the high rate of preterm delivery of these pregnancies, but also to the high risk of fetal growth disturbances. It is well established that twin pregnancies with evident growth discordance have poorer perinatal outcomes, independently of gestational age at delivery.2
Prevalence
The prevalence of fetal growth restriction (FGR) in twins depends on the definition used. The incidence is 48%, 27% or 16% if the definition denotes at least one twin with birthweight < 10th centile, < 5th centile or a birthweight discrepancy ≥ 20%, respectively. In recent years, the diagnostic convention for selective fetal growth restriction (sFGR) has become an estimated fetal weight < 10th centile in one twin with an inter-twin discordance of ≥ 25%.
Monochorionic (MC) twin pregnancies are more likely to be complicated by growth restriction than dichorionic (DC) twin pregnancies, with nearly twice the rate of FGR at 19.7% compared to 10.5% and a higher incidence of associated perinatal mortality with a rate of 7.5% compared to 3.3%.3 Selective growth restriction may have similar prevalence between MC and DC twins, but neurological complications and morbidity in the co-twin are more common in affected MC pregnancies than in DC pregnancies.3 In an attempt to standardise the management of sFGR in MC pregnancies, a consensus was recently published on the diagnostic criteria of sFGR in DC and MC twin pregnancies.
The diagnosis of sFGR is made if the estimated fetal weight (EFW) of the small twin is less than the 3rd centile or if two of the following criteria are met: EFW of one twin < 10th centile, AC of one twin < 10th centile, EFW discordance ≥ 25% or umbilical artery pulsatility index (PI) of the smaller twin > 95th centile (Table 16.1).4,5Aetiology
Although FGR is usually thought to be placental in origin, it is important to rule out intrauterine infection (cytomegalovirus, toxoplasmosis and rubella) and discordance due to chromosomal or congenital anomalies. The incidence of discordant anomalies is around 4% in DC twin pregnancies compared to 6.7% in MC twin pregnancies.3
168
Table 16.1 Diagnostic criteria for selective fetalgrowth restriction in twin pregnancy as determined by experts4
| Monochorionic twin pregnancy | Dichorionic twin pregnancy | |
| Solitary | EFW of one twin < 3rd centile | EFW of one twin < 3rd centile |
| Contributory | Two out of four of the following contributory parameters are required (irrespective of which parameter) EFW of one twin < 10th centile | Two out of three of the following contributory parameters are required (irrespective of which parameter) EFW of one twin < 10th centile |
| AC of one twin < 10th centile | EFW discordance ≥ 25% | |
| EFW discordance ≥ 25% | UA-PI of smaller twin > 95th Centile | |
| UA-PI of smaller twin > 95th centile |
AC, abdominal circumferences; EFW, estimated fetalweight; PI, pulsatility index; UA, Umbilicalartery
Chorionicity and amnionicity also determine the aetiology of fetal growth discordance in twins to a large extent.
In MC twins, differences are largely attributed to twin-to-twin transfusion syndrome (TTTS) or to unequal share of placental mass between the fetuses. There is also evidence from the ESPRiT study cohort relating to the cord insertion site and its relation to both birthweight discordance and small-for-gestational age (SGA) status in MC twins.2On the other hand, in DC twins, differences may be attributed to different genetic growth potential, but underlying pathology may also be present, leading to adverse neonatal outcomes, similar to singleton cases. In DC twins, in contrast to MC twins, both discordant birthweight and SGA status are associated with underlying placental histological abnormalities. For DC twins, growth discordance can be related to underlying placental insufficiency selectively affecting one twin.2
Fetal Biometry in Twin Pregnancies
The inter-twin biometry discordance, as well as the difference in size between twin and singleton pregnancies, is more pronounced in the third trimester and is seen earlier in MC pregnancies. A problematic common practice is to plot the growth of twin fetuses on growth charts created from data of uncomplicated singleton pregnancies. The issue is whether the observed differences in growth between twins and singletons represent physiological adaptation to the intrauterine environment or growth restriction to less than optimal growth. Thus, if twins are physiologically adapted, then comparing them to singletons may increase unnecessary interventions and prematurity for suspected fetal compromise without actual benefit.3
Management Dilemma
The management of FGR in multiple pregnancy, particularly where only one fetus is affected, is complicated by the need to consider the interests of both twins. A policy which relies on the fetal size alone to identify fetuses at risk is unlikely to be very effective in preventing stillbirth at term. There is a need for better markers to identify fetuses at risk of adverse perinatal outcome among those which are SGA, as the majority of small fetuses have normal outcome.
Equally important, a more challenging task is to identify the fetuses at risk of adverse perinatal outcome among those which are presumed to be at low risk, simply due to the fact that their size is within normal range. It may be the case that in both singleton and twin pregnancies, the addition of Doppler parameters is of benefit in distinguishing the growth- restricted fetus from the ‘normally’ small baby.3
Selective FGR represents a management dilemma which is unique to twin pregnancies, where one twin appears to be compromised while the other is growing normally. The best interests of the twins may diverge, but the management chosen, whether intervention or conservative, will affect both.
Management Options
Regular ultrasound monitoring of fetal growth is an essential part of antenatal care in
multiple pregnancies and the frequency
(Figures 16.1 and 16.2).6
of monitoring depends on chorionicity
Monochorionic twin pregnancy
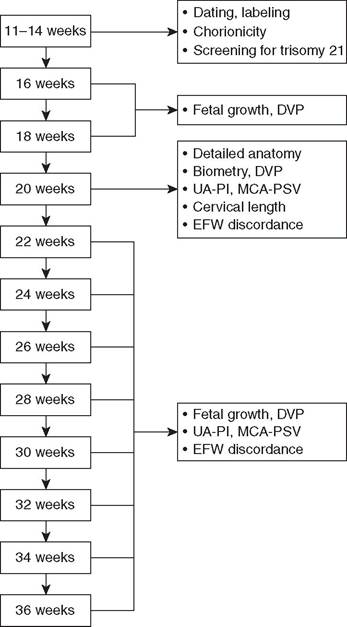
Figure 16.1 Sonographic monitoring of fetalgrowth and well-being in monochorionic twin pregnancies6
Dichorionic twin pregnancy
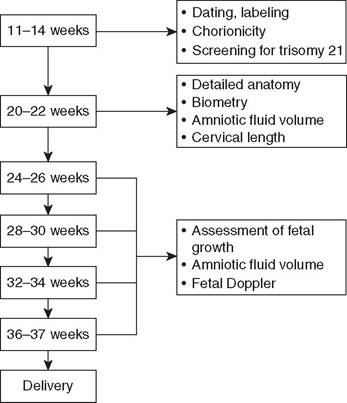
Figure 16.2 Sonographic monitoring of fetalgrowth and well-being in dichorionic twin pregnancies6
The management of the growth-restricted dichorionic twin is similar to that of a growth- restricted singleton, with the added factor of aiming to continue the pregnancy as long as possible in the interests of the appropriately grown co-twin. In same-sex twins, greater discordance is associated with increased risk of intrauterine death for both the smaller and the larger twin, while intrauterine death and the prognosis of the larger twin are unrelated to discordance when the twins are of different sexes.7
In certain highly selected cases, selective reduction can be the most appropriate management in a DC twin pregnancy.
For example, early-onset severe pre-eclampsia may be associated with severe growth restriction in one of the twins. Selective reduction of the affected twin maybe associated with resolution of the pre-eclampsia and can allow continuation of the pregnancy to achieve improved outcomes in the appropriately grown twin. In DC pregnancies, the death of the affected twin introduces a low risk of harm to the co-twin, mainly the risk of preterm delivery; therefore, expectant management is usually preferred.3The management of sFGR in MC twins is based on the MC placental structure and interdependent fetal circulations. There is only scant evidence on how best to manage this condition, based on observational studies, and current practice varies among centres and clinicians. In MC pregnancies, the connected placental circulations put the healthy co-twin at risk of death and serious neurological impairment in addition to the risk of preterm delivery. Demise of one twin is associated with a 15% risk of death and 25% risk of neurodevelopmental impairment in the co-twin due to the acute feto-fetal transfusion that can result from the sudden fall in vascular resistance in the circulation of the demised twin. Any intervention should precede the fetal demise in order to prevent these consequences. Selective reduction is technically challenging as the vascular communications preclude the use of potassium chloride. Intrauterine fetal therapy has introduced a range of potential interventions for the antenatal management of these cases, including cord occlusion of the affected twin, intra-fetal laser ablation or radiofrequency ablation (RFA) of communicating vessels. With either of the latter techniques, the outcome for the co-twin looks similar, so the choice depends on operator preference and expertise.3
Doppler assessment seems to offer reliable information to determine the management type and timing. In DC pregnancies, similar to singletons, Dopplers are expected to follow a pattern of deterioration that can be used to guide the timing of intervention, but in MC pregnancies, the typical pattern of deterioration may not be observed.
The compensatory effect of the co-twin’s circulation may delay or even fully obscure the deterioration of the affected twin.3In MC pregnancies, the presence or absence of umbilical artery Doppler end-diastolic flow in the affected twin at the time of diagnosis forms the basis of the classification system by Gratacos et al. (Figure 16.3).8 Positive end-diastolic flow is reassuring (type I) whereas absent or reversed end-diastolic flow is a poor prognostic indicator (type II). The third category of intermittent absent or reversed end-diastolic flow (type III) is unique to MC pregnancies. In this group, the presence of large-diameter arterio-arterial anastomoses permits a compensatory flow from the normal twin, promoting longer survival of the growth-restricted twin. Unfortunately this is also the cause of acute transfusion events that is unpredictable and can lead to unexpected intrauterine death or neurological damage in both the growth-restricted and normally grown twin. It must be noted that this Doppler pattern is most likely to be close to the placental cord insertion site of the umbilical cord and can be missed unless low-sweep-speed pulsed Doppler is used.
The outcome of sFGR in MC twin pregnancies is dependant on the type. Type I sFGR has a good prognosis and elective delivery at around 34 weeks, and sometimes even up to 36 weeks is possible. A proportion of these cases can progress, underlining the importance of regular ultrasound surveillance. Types II and III have a poorer prognosis and are more likely to require intervention. Type II tends to progress in about 60% of cases, necessitating earlier delivery at 30-32 weeks, and has a worse prognosis compared with types I and III, particularly for the smaller fetus. In type III, deterioration of fetal status occurs in about 10% of cases, necessitating delivery at 31-33 weeks, and the larger fetus can have abnormal brain imaging and periventricular leukomalacia in up to 20% of cases due to the unpredictable acute transfusion events mentioned earlier. See Tables 16.2 and 16.3 for more detailed outcome data for each type derived from a systematic review and meta-analysis of 13 studies.9
Timing of Delivery in Dichorionic Twins with Selective Fetal Growth Restriction
There is little consensus about the optimal time of delivery. Early delivery carries the risks associated with prematurity, but delay may increase hypoxic damage.10 In very early-onset severe FGR (< 28 weeks), particularly where the estimated weight of the growth-restricted fetus is not viable or is borderline viable (< 500-600 g), one option is no intervention, accepting that the growth-restricted fetus may die in utero but optimising gestation and hence outcome for the normal fetus. Where the growth-restricted fetus is viable and live birth is desirable, management decisions follow the same principle as for singleton FGR, but given that it is generally advised that uncomplicated dichorionic twins are delivered at 3738 weeks of gestation and this is considered ‘term’, for late-onset growth pathology, an earlier gestational threshold is advised - that is, 35-36 weeks.
https://doi.org/10.1017/9781108915038.016 Published online by Cambridge University Press
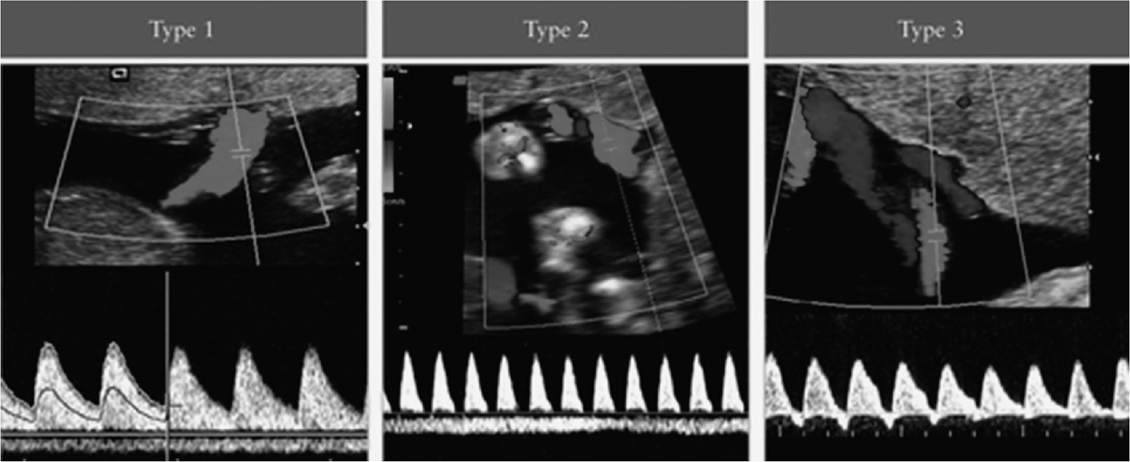
Figure 16.3 Gratacos et al. classification system for sFGR in twin pregnancies. In type I, the Umbilicalartery Doppler waveform has positive end-diastolic flow, while in type II, there is absent or reversed end-diastolic flow (AREDF). In type III, there is a cyclical/intermittent pattern of AREDF.7 (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
Table 16.2 Outcomes in monochorionic twin pregnancies with selective fetalgrowth restriction (sFGR according to type of sFGR) (adapted from systematic review and meta-analysis Buca et al. 2017)9
| Type I sFGR | Type II sFGR | Type III sFGR | |
| Deterioration of fetal status | 16.2% | 58.9% | 10.1% |
| Mean gestational age at delivery in | 33.7 | 30.9 | 32.0 |
| weeks (95% CI) | (33.0-34.3) | (30.0-31.8) | (31.3-32.8) |
| % Birthweight discordance (95% CI) | 23% | 44.3% | 32.5% |
| (14.7-31.4) | (36.8-51.8) | (28.5-36.6) | |
| Fetal outcomes (%) | |||
| Perinatal mortality | 6.3 | 21 | 11 |
| Intrauterine death | 2.5 | 13.2 | 8.9 |
| Neonatal death | 3.1 | 9.2 | 2.7 |
| Double fetal loss | 1 | 7.8 | 3.4 |
| Abnormal brain imaging | 2.5 | 13.8 | 12 |
| IVH | 0 | 8.2 | 4.9 |
| PVL | 2.1 | 13.9 | 11.7 |
| Admission to NICU | 38 | 93.4 | 58.3 |
| RDS | 30.1 | 45.7 | 91.7 |
| Composite adverse outcome* | 4.8 | 26.3 | 18.6 |
Composite adverse outcome defined as presence of any mortality or abnormalbrain findings
IVH = intraventricular haemorrhage; PVL = periventricular leukomalacia; RDS = respiratory distress syndrome; NICU = neonatal intensive care unit
For early-onset FGR, a few prospective multicentre studies have addressed the timing of delivery issue based on Doppler flow parameters. The Growth Restriction Intervention Trial (GRIT) investigated the timing of delivery for FGR in singleton pregnancy.11 Pregnant women between 24 and 36 weeks of gestation with FGR were randomly assigned to immediate or delayed delivery if the obstetrician was uncertain about when the FGR fetus should be delivered based on umbilical artery Doppler parameters. There was no difference in overall mortality between the two groups. Although the GRIT study could not provide standard criteria for determining the timing of delivery, the lack of a difference in overall mortality between immediate and delayed delivery suggests that it may be important for parents or obstetricians to consider prolonging the time in utero for the normal twin of DC twins with sFGR, even for a short period. This is further supported by the fact that in a subgroup analysis of those delivered before 31 weeks, delayed delivery was associated with less neurodevelopmental morbidity and disability at age two.12 Since publication of the GRIT study, the Trial of Umbilical and Fetal Flow in Europe (TRUFFLE) investigated in singleton pregnancy which method of fetal assessment should be used to trigger delivery in preterm fetal growth restriction - early or late changes in the fetal ductus venosus Doppler
Table 16.3 Outcomes in monochorionic twin pregnancies with selective intrauterine growth restriction (sFGR) according to type of sFGR, for smaller and larger fetus (adapted from systematic review and meta-analysis Buca etal. 2017)9
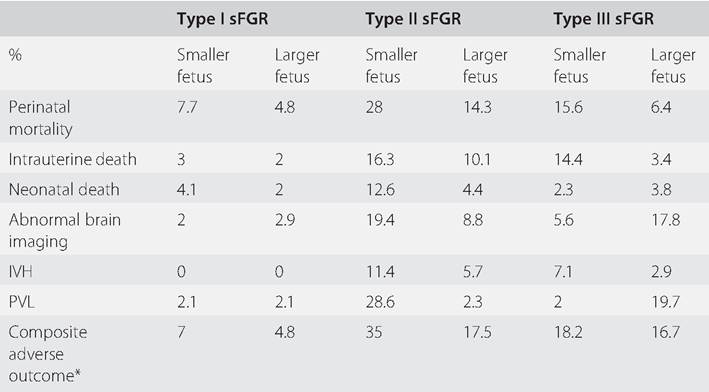
* Composite adverse outcome is defined as the presence of any mortality or abnormalbrain findings. IVH = intraventricular haemorrhage; PVL= periventricular leukomalacia
waveform or Cardiotocograph (CTG) short-term variation.13 There was no difference in the primary outcome of the trial or the proportion of children free from neurological impairment at two years old, but the findings suggested that waiting for late ductus venosus changes (or severe CTG changes, which were used as safety net indication for delivery) was associated with more favourable developmental outcomes at two years of age. Current guidance is that a combination of sonographically evaluating growth velocity and Doppler flow parameters in umbilical artery, middle cerebral artery and the ductus venosus, using biophysical profile and/or computerised CTG should trigger gestational cut-offs to consider delivery.14 See Tables 16.4 and 16.5.
Timing of Delivery in Monochorionic Twins with Selective Fetal Growth Restriction
The most recent guidelines on twin pregnancy have highlighted the lack of evidence. The ISUOG guidance states that ‘there is limited evidence to guide the management of MC twins affected by sFGR',6 while the Royal College of Obstetricians and Gynaecologists (RCOG) guidance on twin pregnancy states that ‘due to a lack of available high quality evidence, there is no clear guidance on how to manage sFGR in twin pregnancies'.15
Based on expert opinion, these pregnancies should have follow-up ultrasound examinations at least weekly. In cases in which ductus venosus Doppler shows absent or reversed a-wave before 26 weeks of gestation, indicating a substantial risk of fetal demise of the
Table 16.4 Thresholds for timing of delivery in fetalgrowth restriction in dichorionic twins
| Threshold for delivery | Parameters |
| < 30 weeks | Expectant management |
| 30 weeks | DV absent or reversed 'a' wave |
| 30-32 weeks | UA REDF |
| 32-34 weeks | UAAEDF |
| > 34 weeks | MCA low PI |
| 34-36 weeks | UA high PI |
| Triggers for considering earlier delivery at any gestation when EFW of FGR fetus > 500-600g | Static growth in a 2 week period, repeated persistent unprovoked decelerations on CTG or abnormal STV on cCTG, maternal indication eg. severe fulminating pre-eclampsia |
DV = ductus venosus, UA= Umbilicalartery, REDF = reversed end diastolic flow, AEDF = absent end diastolic flow, MCA = middle cerebral artery, PI = pulsitility index, STV = short term variation, CTG = cardiotocograph, cCTG = computerized CTG
Table 16.5 Computerised cardiotocograph short-term variation (STV) thresholds (adapted from ISUOG Practice Guidelines)12
| Gestation | STV (ms) |
| 26-28+6 weeks | < 2.6 |
| 29-31+6 weeks | < 3.0 |
| 32-33+6 weeks | < 3.5 |
| >/= 34 weeks | and the growth-restricted twin is not stuck - that is, may have oligohydramnios but not anhydramnios, which makes it more difficult to visualise the placental vascular equator. In one study of laser photocoagulation of connecting placental vessels for type III sFGR, only 88.9% of procedures were completed because of technical difficulties and 12.5% of them required a second procedure.18 The procedure carries a risk of preterm premature rupture of the membranes (PPROM), preterm labour and chorioam- nionitis. Furthermore, perforation of the inter-twin membrane may occur either deliberately to facilitate access to the vascular equator or incidentally during the procedure, and cases of iatrogenic monoamniotic pregnancies have been reported.18 Chorioamniotic separation may occur in up to 20% of cases treated fetoscopically and is associated with worse pregnancy outcomes. Type II sFGR has the worst clinical prognosis and pregnancies with it comprised the first target group for trials of laser therapy. The survival of the larger twin seems to be less than after laser therapy (67.6-73.9%), but 30.4-38.7% of the smaller twins survive, contributing to a slight increase in overall survival compared to cord occlusion. The sFGR pregnancies most at risk of acute feto-fetal transfusion events are type III cases where large AA anastomoses render each twin vulnerable to ischaemic brain damage during even short periods of bradycardia and hypotension in their co-twin. Although the overall survival rate is higher than in type II, the difficulty in predicting deterioration in this group means they might be expected to benefit most from the ‘dichorionisation’ effect of laser treatment.3 Prediction of Growth Restriction In terms of prediction, discordance in the crown-rump length is associated with the development of growth discordance and sFGR later in pregnancy. Crown-rump length discordance in the first trimester is also associated with a number of adverse pregnancy outcomes, including preterm delivery and pregnancy loss, thus pregnancies affected by a CRL discordance of > 20% should be discussed with a fetal medicine expert for consideration of additional monitoring. Recent studies have reported that the predictive accuracy is poor, however. In the second trimester, if the EFWs are concordant, it is highly unlikely that sFGR will develop, and this finding can be used to guide frequency of monitoring in later pregnancy. The presence of discordance at 21-24 weeks has been shown to be a poor predictor of the development of growth discordance and sFGR later in pregnancy.3 Conclusion As twin pregnancies increase in frequency, general obstetricians need to develop a detailed appreciation of the physiological differences and subsequent challenges of managing FGR in twin pregnancies. Increased antenatal surveillance in twins is necessary to identify growth impairment early and to facilitate timely intervention. Concerning MC twins, despite the widespread use of fetoscopic intervention for TTTS, the therapeutic value of fetal intervention for sFGR is yet to be established. No randomised controlled trials have yet been reported, and there is therefore a lack of clarity on where the balance of risk and benefit lies when considering intervention in this group. Current best evidence suggests that selective reduction and fetoscopic laser therapy offer similar overall survival chances but laser therapy carries a higher risk of mortality and lower risk of morbidity. Key Points • At every ultrasound assessment of a twin pregnancy beyond 20 weeks of gestation, the EFW discordance should be calculated. • Regular monitoring of fetal growth is fundamental. • Chorionicity determines the aetiology of fetal growth discordance in multiple pregnancy. • Selective fetal growth restriction in MC twins is related to placental share or TTTS. • Selective FGR in DC twins is attributed to different genetic growth potential or underlying placental pathology, similar to singleton cases. • Management of growth restriction in twin pregnancy needs to balance the competing interests of the larger and smaller fetuses. • The Gratacos classification of sFGR in MC twin pregnancies is strongly correlated to the adverse perinatal outcomes. • The management of the growth-restricted DC twin is similar to that of a growth- restricted singleton, with the added factor of aiming to continue the pregnancy as long as possible in the interests of the appropriately grown co-twin. • The management of sFGR in MC pregnancies is complex and depends on type and severity of sFGR. • In MC pregnancies, the typical pattern of Doppler deterioration may not be observed. • Fetoscopic laser coagulation for sFGR is technically challenging and its therapeutic value is yet to be established. • Twin pregnancies presenting with a CRL discordance of > 20% in the first trimester should be discussed with a fetal medicine specialist. References 1. Kulkarni AD, Jamieson DJ, Jones HW Jr et al. Fertility treatments and multiple births in the United States. N Engl J Med 2013;369 (23):2218-25. 2. Kent EM, Breathnach FM, Gillan JE et al. Placental pathology, birthweight discordance, and growth restriction in twin pregnancy: results of the ESPRiT Study. Am J Obstet Gynecol 2012;207 (220):e1-e5. 3. Townsend R, Khalil A. Fetal growth restriction in twins. Best Pract Res Clin Obstet Gynaecol 2018;49:79-88. 4. Khalil A, Beune I, Hecher K et al. Consensus definition and essential reporting parameters of selective fetal growth restriction in twin pregnancy: a Delphi procedure. Ultrasound Obstet Gynecol 2019;53:47-54. 5. Khalil A, Thilaganathan B. Selective fetal growth restriction in monochorionic twin pregnancy: a dilemma for clinicians and a challenge for researchers. Ultrasound Obstet Gynecol 2019;53:23-5. 6. Khalil A, Rodgers M, Baschat A et al. ISUOG practice guidelines: the role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol 2016;48:669-70. 7. Demissie K, Ananth CV, Martin J et al. Fetal and neonatal mortality among twin gestations in the United States: the role of intrapair birth weight discordance. Obstet Gynecol 2002;100(3):474-80. 8. Gratacos E, Lewi L, Munoz B et al. A classification system for selective intrauterine growth restriction in monochorionic pregnancies according to umbilical artery Doppler flow in the smaller twin. Ultrasound Obstet Gynecol 2007;30:28-34. 9. Buca D, Pagani G, Rizzo G, et al. Outcome in monochorionic twin pregnancies with selective intrauterine growth restriction according to the umbilical artery Doppler pattern of the smaller twin: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017;50:559-68. 10. Kaku S, Kimura F, Murakami T. Management of fetal growth arrest in one of dichorionic twins: three cases and a literature review. Obstet Gynecol Int 2015;2015:289875. 11. GRIT Study Group. A randomised trial of timed delivery for the compromised preterm fetus: short term outcomes and Bayesian interpretation. BJOG 2003;110 (1):27-32. 12 Thornton JG, Hornbuckle J, Vail A, Spiegelhalter DJ, Levene M. GRIT Study Group. Infant wellbeing at 2 years of age in the Growth Restriction Intervention Trial (GRIT): multicentred randomised controlled trial. Lancet 2004 7-13 Aug;364 (9433):513-20. https://doi.org/10.1016/S01 40-6736(04)16809-8. PMID: 15302194. 13. Lees CC, Marlow N, Van Wassenaer- Leemhuis A et al. 2 year neurodevelopmental and intermediate perinatal outcomes in infants with very preterm fetal growth restriction (TRUFFLE): a randomised trial. Lancet 2015;385(9983):2162-72. https://doi.org/ 10.1016/S0140-6736(14)62049-3 14. Khalil A, Rodgers M, Baschat A et al. ISUOG practice guidelines: diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet Gynecol 2020;56:298-312. Published online in Wiley Online Library (wileyonlinelibrary. com). https://doi.org/10.1002/uog.22134 15. Royal College of Obstetricians and Gynaecologists (RCOG). Management of monochorionic twin pregnancy. Green-top Guideline No. 51. RCOG: London, 2016. www.rcog.org.uk/en/guidelines-research- services/guidelines/gtg51 16. Bebbington MW, Danzer E, Moldenhauer J, Khalek N, Johnson MP. Radiofrequency ablation vs bipolar umbilical cord coagulation in the management of complicated monochorionic pregnancies. Ultrasound Obstet Gynecol 2012;40(3):319-24. 17. Parra-Cordero M, Bennasar M, Martinez JM, Eixarch E, Torres X, Gratacos E. Cord occlusion in monochorionic twins with early selective intrauterine growth restriction and abnormal umbilical artery Doppler: a consecutive series of 90 cases. Fetal Diagn Ther 2016 Jan;39 (3):186-91. 18. Gratacos E, Antolin E, Lewi L, et al. Monochorionic twins with selective intrauterine growth restriction and intermittent absent or reversed end-diastolic flow (Type III): feasibility and perinatal outcome of fetoscopic placental laser coagulation. Ultrasound Obstet Gynecol 2008;31(6):669-75.
More medical literature on Medic.Studio
More on the topic Management of Fetal Growth Pathology in Multiple Pregnancy:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|