Management of Monoamniotic Twins
Vagisha Pruthi, Shiri Shinar, Johannes Keunen, Greg Ryan and Tim van Mieghem
The Facts
Definition and Epidemiology
In monochorionic-monoamniotic twin pregnancies, two fetuses share a single placenta and a single amniotic cavity.
This specific anatomic configuration is rare (8 per 100,000 pregnancies) and is the result of the late splitting of a single embryo between 8 and 13 days after fertilisation.1 As such, monoamniotic twins are always monozygotic. Conjoined twins are a specific subtype of monoamniotic twins in whom the splitting of the embryos occurs even later in pregnancy. Monochorionic and monoamniotic twins are more common after assisted reproduction. The reason for this is unclear, but some think assisted hatching and embryo manipulation play a role.2 Occasionally, monoamniotic twins can be the result of spontaneous or iatrogenic (amniocentesis, fetal surgery) tearing of the inter-twin amniotic membrane in diamniotic twins.Diagnosis
It is important to determine chorionicity and amnionicity in the first trimester of pregnancy as this is the most accurate time period in which to do so. Moreover, correct determination of the number of placentas and inter-twin membranes in the first trimester is critical to counsel parents about possible pregnancy complications and to outline a plan for pregnancy surveillance. Monoamniotic twins are at significantly higher risk of adverse pregnancy outcomes than monochorionic-diamniotic or dichorionic twins. Monoamnionicity is diagnosed when no intervening membranes between two fetuses can be visualised with ultrasound (Figure 17.1). Amnionicity can be difficult to determine before 10 weeks as the inter-twin membrane in monochorionic-diamniotic twins is often very thin at that time. Transvaginal ultrasound with a high-frequency probe can help in that situation.
Other ultrasound findings that may be helpful in determining amnionicity include the presence of cord entanglement, which is pathognomonic for monoamniotic twins, and the number of yolk sacs. Of note, however, is that only 68% of monoamniotic twins will have a single yolk sac and 32% will have two sacs.3 If chorionicity and amnionicity cannot be determined by 12 weeks of gestation, referral to an expert centre is recommended.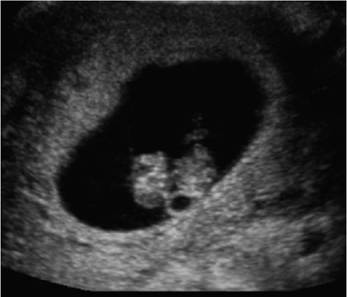
Figure 17.1 Ultrasound image of monoamniotic twin pregnancy at 7 weeks of gestation. Note the single yolk sac and the lack of intervening membrane.
Complications
Congenital Anomalies
In monoamniotic twins, the risk of birth defects is as high as 15-25%.4,5 Usually, only one fetus is affected, and if both fetuses are affected, anomalies are often discordant. The high incidence of structural anomalies is explained by the delayed cleavage of the embryo and likely also by important blood volume shifts through large artery-to-artery anastomoses at the level of the placenta.6 As a consequence, heart defects are the most common anomaly in monoamniotic twins (up to 30% of all anomalies). Acardiac twinning, also called twin- reversed arterial perfusion (TRAP) sequence, is a type of cardiac anomaly specific to monochorionic twins and can also occur in monoamniotic pregnancies. In this condition, which is described in more detail in Chapter 15, the acardiac mass does not have a circulation of its own and is perfused by the pump twin through placental anastomoses. The acardiac mass is never viable and compromises the healthy co-twin through cardiac failure (polyhydramnios, hydrops, fetal death) and mass effect (preterm birth). Only 4% of structural defects in monoamniotic twins have an underlying genetic aetiology, which is much less than in monochorionic-diamniotic twins (15%) or dichorionic twins (25%).
Birth defects and pregnancy terminations as a consequence of birth defects explain about half of the mortalities observed in monoamniotic twins.
The management of discordant anomalies is similar to that in monochorionic-diamniotic twins except that, in case of selective reduction, cord transection should be performed after the cord flow is interrupted to prevent further cord accidents. Given the frequency and impact of birth defects in this population, we perform earlier anatomy assessment and echocardiography in these pregnancies.Twin-Twin Transfusion Syndrome
Twin-twin transfusion syndrome (TTTS), which complicates 10-15% of monochorionic- diamniotic twins, is only seen in 2-4% of monoamniotic pregnancies.1 This lower incidence is explained by the proximate cord insertions and large bidirectional artery-to-artery anastomoses which compensate for unidirectional flow through arterio-venous anastomoses.6 As there is no inter-twin membrane to delineate the fetus with oligohydramnios from the fetus with polyhydramnios, TTTS is harder to diagnose in monoamniotic twins and stage I TTTS (amniotic fluid discordance) cannot be diagnosed. More advanced stages of TTTS are suspected if polyuric polyhydramnios (large bladder in one twin) is noted in combination with an empty bladder in the other twin and/or Doppler changes characteristic of TTTS. Despite the rarity of TTTS, we follow these pregnancies with biweekly ultrasounds from 16 weeks of gestation onwards.
A recent systematic review and meta-analysis documents the outcomes of TTTS in monoamniotic twins.7 Among 890 monoamniotic twin pregnancies, only 46 developed TTTS. Expectantly managed cases miscarried in 10.7% of cases. The incidence of intrauterine, neonatal and perinatal deaths was 24.3%, 13.5% and 32.4%, respectively. Fetoscopic laser ablation of placental anastomoses did not seem to improve outcomes significantly, and this is likely due to the fact that occlusion of large inter-twin anastomoses in the presence of proximate cord insertions is often lethal for both fetuses. Although the number of cases reviewed in the paper was too low to provide strong evidence regarding the outcomes of selective cord occlusion, this strategy seemed to be associated with the best survival rates.
Of note, after cord occlusion in monoamniotic twins, one should transect the cord of the dead fetus to prevent further cord accidents.Selective Fetal Growth Restriction
Growth restriction is three times more common in monoamniotic twins than in singletons. Almost 40% of cases are born with a birthweight below the 10th centile10 and 10% weigh less than the 3rd centile.5 The incidence of selective fetal growth restriction, where only one fetus is small, is lower than in monochorionic-diamniotic twin pregnancies due to the proximate cord insertions and large placental vascular anastomoses. The average birthweight discordance in monoamniotic twins is 10%5 compared with ~15% in diamniotic twins, and a birthweight difference of more than 25% is only seen in 3% of cases.8 Important intertwin weight differences increase the risk of fetal death in monoamniotic twins.
Intrauterine Fetal Death
Although the perinatal mortality of monoamniotic twins has decreased over the past three decades, still only 62-70% of monoamniotic twins diagnosed in the first trimester of pregnancy survive.9,10 As discussed earlier, about half of the fetal losses are explained by congenital anomalies or pregnancy termination. The remaining fetal deaths are explained by cord accidents (tight entanglement) (Figure 17.2) and/or rapid inter-twin transfusion imbalances. Prevention by maternal administration of Sulindac, which reduces the fetal urinary output, the amniotic fluid volume and fetal movements, has never found widespread uptake.
The Issues
Once monoamniotic fetuses have reached a gestational age at which delivery becomes an option, prevention of stillbirth could be initiated by urgent delivery if signs of fetal distress are noted. Most centres will therefore initiate close surveillance after viability. Unfortunately, level 1 evidence on the best method, frequency and setting of surveillance is still lacking. Moreover, experts still disagree on the timing of delivery and to a lesser extent on mode of delivery.
The controversy is mainly due to the rarity of these pregnancies, precluding large trials. The evidence and guidance presented in the next section mainly relies on outcomes reported in retrospective (multicentre) observational studies. Despite
Figure 17.2 Proximate cord insertions and cord entanglement in a monoamniotic twin pregnancy (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
the fact that interventional and prospective trials are lacking, more recent studies present better outcomes than older studies, suggesting that current surveillance strategies, in combination with advances in neonatal care, have made a positive difference for these pregnancies. Additionally, a few observational studies seem to show that monoamniotic pregnancies undergoing close surveillance have better outcomes than those that do not.
The Management Options
Method of Surveillance
At our centre, we intensify fetal surveillance after ‘viability’. We îffer a consultation with our neonatology team to all couples expecting monoamniotic twins around 24 weeks of gestation to discuss the outcomes of preterm birth. After this discussion, the timing of variability is set, typically between 24 and 28 weeks, depending on patient preferences. At ‘viability’, steroids are administered for fetal pulmonary maturation. The best surveillance method for monitoring monoamniotic twin pregnancies is still unclear. Most centres initiate both ultrasound surveillance (to assess long-term well-being by assessing growth and amniotic fluid volume) in combination with fetal heart rate monitoring (to assess short-term well-being by looking for heart rate decelerations or prolonged episodes of fetal tachycardia). On Doppler ultrasound, diastolic notching in the umbilical artery or absent and reversed end-diastolic flow suggest the presence of cord compression, but these flow patterns are extremely common and often transient.
As such, we don’t use these indicators as triggers for delivery. Management of monoamniotic twins in expert centres is recommended given that clinician experience plays an important role in recognising triggers for delivery, but also to avoid unwarranted preterm delivery based on benign findings.Frequency and Setting of Surveillance
Evidence is lacking on the optimal frequency of surveillance after viability, but most will recommend daily to alternate day fetal heart rate monitoring in combination with ultrasound one to three times per week.5,11,12 Continuous fetal heart rate monitoring is impractical and only feasible in about 50% of cases and is therefore not recommended. Even with very close surveillance, fetal deaths have been reported just hours after a reassuring test, suggesting that fetal deaths are not all preventable and most large centres report fetal death rates of 2-5%, despite close surveillance.
Specialists still disagree on the optimal setting of surveillance (inpatient vs outpatient), and this has been the topic of heated debates. Unfortunately, when critically analysing the literature, most studies are confounded by the fact that location of surveillance (inpatient vs outpatient) is often linked with method and frequency of surveillance with less or no surveillance going on in outpatients and surveillance starting later in pregnancy.10,11,12 Careful analysis of all studies, however, suggests that the risk of fetal death becomes very low once surveillance is initiated, be it in an inpatient or outpatient setting (< 5%).5,8,10,13 At our centre, we therefore offer patients the choice, taking all risks and benefits into consideration. Of note, we discuss the risks of inpatient surveillance including an increased risk of venous thromboembolism, the economic and societal costs, the disruption to family life and an increased risk of psychiatric distress with higher rates of hopelessness and despair (42% vs 24%), thoughts of self-harm or suicide (4% vs 0%) and post-partum depression (12% vs 4%) in inpatients.14 This should obviously be balanced with access to care and geographic constraints.
Timing of Birth
As mentioned earlier, some fetal deaths remain unpredictable, despite close surveillance. Therefore, most experts will recommend delivery when the risk of pregnancy continuation outweighs neonatal risks. A retrospective multicentre study of nearly 200 mono- amniotic twin pairs showed that this balance was reached around between 32 and 33 weeks of gestation.5 At that point, the risk of a severe, non-respiratory neonatal complication (death before discharge from the NICU, culture-proven sepsis, necrotising enterocolitis, retinopathy of prematurity more than grade II, intraventricular haemorrhage more than grade I or cystic periventricular leukomalacia) is lower than the prospective risk of fetal death (3.1%).5 At our centre, we therefore deliver uncomplicated monoamniotic twins from 33 weeks of gestation, even though in some units, longer expectant management is offered.15
Mode of Delivery
Most experts will deliver monoamniotic twins by elective caesarean section given the risk of acute occlusion of cord knots during labour and delivery. Moreover, there is a risk of entanglement of the first twin in the umbilical cord of the second twin, mandating transection of that cord to allow for delivery of the first twin. This scenario creates an acute emergency and possible asphyxia of the second twin. Despite this, it is important to mention that some obstetricians still advocate for vaginal delivery of monoamniotic twins.15
Key Points
• Adverse pregnancy outcomes are increased in MCMA twin pregnancies.
• Highest risk of pregnancy loss is before 20 weeks' gestation.
• Increased fetal surveillance is advocated in all MCMA twins after 24 weeks' gestation - in either the inpatient or the outpatient setting.
• Elective birth is advocated from 33 weeks' gestation.
Video 17.1 Dating ultrasound at 9 weeks of gestation. Transabdominalultrasound showing a monoamniotic twin gestation with a single yolk sac and a single amniotic cavity.
Video 17.2 First-trimester ultrasound at 12 weeks of gestation. Transabdominalultrasound showing a monoamniotic twin gestation. Note the presence ofcord entanglement and the absence of a dividing inter-twin membrane.
References
1. Glinianaia SV, Rankin J, Khalil A et al. Prevalence, antenatal management and perinatal outcome of monochorionic monoamniotic twin pregnancy:
a collaborative multicenter study in England, 2000-2013. Ultrasound Obstet Gynecol 2019;53:184-92.
2. Knopman JM, Krey LC, Oh C, Lee J, McCaffrey C, Noyes N. What makes them split? Identifying risk factors that lead to monozygotic twins after in vitro fertilization. Fertil Steril 2014 Jul;102(1):82-9.
3. Fenton C, Reidy K, Demyanenko M, Palma- Dias R, Cole S, Umstad MP. The significance of yolk sac number in monoamniotic twins. Fetal Diagn Ther 2019;46(3):193-9.
4. Allen VM, Windrim R, Barrett J, Ohlsson A. Management of monoamniotic twin pregnancies: a case series and systematic review of the literature. BJOG 2001 Sep; 108 (9):931-6.
5. Van Mieghem T, De Heus R, Lewi L et al. Prenatal management of monoamniotic twin pregnancies. Obstet Gynecol 2014 Sep;124(3):498-506.
6. Hack KE, Van Gemert MJ, Lopriore E et al. Placental characteristics of monoamniotic twin pregnancies in relation to perinatal outcome. Placenta 2009 Jan;30(1):62-5.
7. Murgano D, Khalil A, Prefumo F et al. Outcome of twin-to-twin transfusion syndrome in monochorionic monoamniotic twin pregnancies: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2019 Oct 8. https://doi.org/10.1002/uog.21889
8. Saccone G, Khalil A, Thilaganathan B et al. Weight discordance and perinatal mortality in monoamniotic twin pregnancies: analysis of the MONOMONO, NorSTAMP and STORK multiple pregnancy cohorts. Ultrasound Obstet Gynecol 2020
March 27;55(3):332-8.
9. Litwinska E, Syngelaki A, Cimpoca B, Frei L, Nicolaides KH. Outcome of twin pregnancies with two live fetuses at 11-13 weeks' gestation. Ultrasound Obstet Gynecol 2019 Oct 15. https://doi.org/10.1002∕uog.21892
10. Madsen C, S0gaard K, Zingenberg H et al. Outcomes of monoamniotic twin pregnancies managed primarily in outpatient care: a Danish multicenter study. Acta Obstet Gynecol Scand 2019 Apr;98(4):479-86. https://doi.org/10.1111/ aogs.13509
11. Heyborne KD, Porreco RP, Garite TJ, Phair K, Abril D, Obstetrix/Pediatrix Research Study Group. Improved perinatal survival of monoamniotic twins with intensive inpatient monitoring. Am
J Obstet Gynecol 2005;192:96-101.
12. MONOMONO Working Group. Inpatient vs outpatient management and timing of delivery of uncomplicated monochorionic monoamniotic twin pregnancy: the MONOMONO study. Ultrasound Obstet Gynecol 2019 Feb;53(2):175-83.
13. Van Mieghem T, Shub A. Management of monoamniotic twins: the question is not ‘where?', but ‘how?' Ultrasound Obstet Gynecol 2019 Feb;53(2):151-2.
14.
Winkler SS, Mustian MN, Mertz HL. The psychosocial impact of inpatient management of monoamniotic twin gestations. J Matern Fetal Neonatal Med 2016;29:1877-80.
15. Anselem O, Mephon A, Le Ray C, Marcellin L, Cabrol D, Goffinet F. Continued pregnancy and vaginal delivery after 32 weeks of gestation for monoamniotic twins. Eur J Obstet Gynecol Reprod Biol 2015 Nov;194:194-8.