Maternal Complications in Multiple Pregnancy
Sarah Rae Easter and Mike Foley
The Facts
Maternal Morbidity in Multiple Pregnancy
Considering the prevalence of fetal and prematurity-associated complications in multifetal gestations, clinicians dedicate a tremendous amount of resources to optimise neonatal outcomes in these high-risk pregnancies.
From use of ultrasound to screen for placental complications to assessments for risk of preterm birth, the majority of guidelines in the management of twin and higher-order multiple pregnancies centre on the fetus.1 A well- known but less overtly considered set of complications of multifetal pregnancies are those related to maternal health. The increased association between multifetal pregnancies and adverse maternal outcomes relative to singleton pregnancies is not only intuitive, but is also well described in the literature. Yet we lack specific guidelines or screening protocols to monitor for the well-known maternal complications of multifetal pregnancies.The complexity of addressing maternal complications of multifetal pregnancies is underscored by evolutionary and societal imperative - the unspoken acknowledgement that mothers of multiples assume more risk for the potential reward of more offspring. This biologic truth coupled with the confounded epidemiology of multifetal pregnancy in the era of assisted reproductive technology (ART) challenges any attempt to systematically improve maternal outcomes in this population.2 The exclusion of multifetal pregnancies in many clinical trials coupled with the knowledge of differential impact of obstetric interventions in twin compared to singleton populations can further challenge the development of an evidence-based strategy. In the absence of evidence-based guidelines, the obstetric care provider must adopt a uniform approach to prevention and management of maternal complications of multifetal pregnancies characterised by a high index of suspicion rooted in an understanding of epidemiology and pathophysiology.
The tenets of this strategy include universal maternal risk assessment to provide risk-appropriate antenatal care, avoidance of severe maternal morbidity (SMM) at the time of delivery and comprehensive post-partum follow-up aimed at early detection and prevention (Figure 18.1).Patient-Level Pathophysiology
Multifetal pregnancies carry an increased risk of a range of maternal complications. The clinical impact of some complications such as hyperemesis, gestational diabetes or anaemia may be minimal in the context of an otherwise high-risk pregnancy. Other diagnoses such as hypertension, haemorrhage and caesarean delivery may be causal on the pathway to SMM. Though the severity of these maternal complications may vary, their increased prevalence in
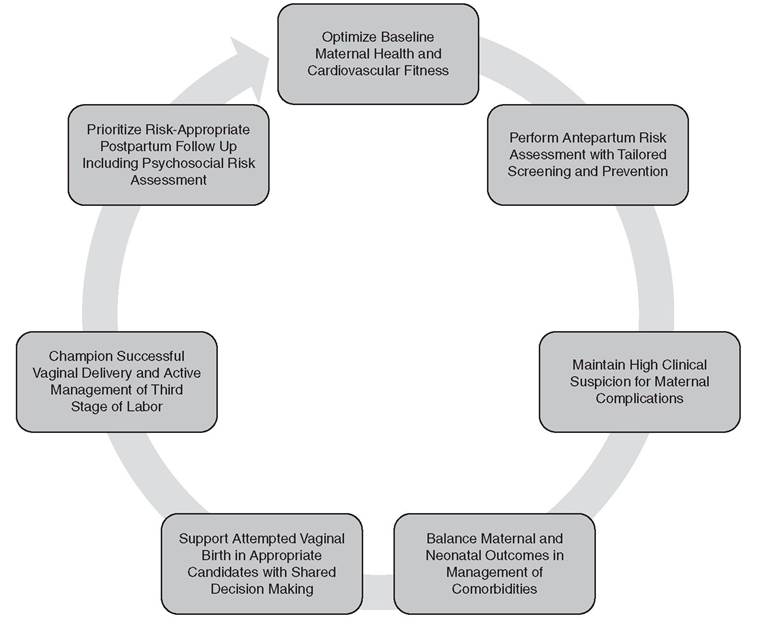
Figure 18.1 Frameworkfor standardised approach to optimising maternaloutcomes in multifetalgestations
multifetal pregnancies relative to singleton pregnancies underscores the extreme aberrations in physiology required to support two or more fetuses and their accompanying placentas.
The role of the placenta in hallmark diseases of pregnancy such as pre-eclampsia, gestational diabetes and hyperemesis is well described. Reason coupled with evidence suggests that the increase in placental mass accompanying multifetal pregnancies would increase the risk of these complications arising from the placental milieu. Observational data demonstrating a 6.5% prevalence of pre-eclampsia in singleton pregnancies and a rate of 12.7% in twins and 20.0% in triplets lend support to this notion. The known association between ART, pre-eclampsia and twins and higher-order multiples further confounds the relationship between placental pathophysiology and multifetal gestations. A review of cardiovascular physiology highlights the contribution of maternal haemodynamics to the hallmark diseases affecting multifetal pregnancies and may help explain the increased prevalence of more severe maternal outcomes in this population.
Contemporary studies underscore the importance of the maternal cardiovascular adaptation to pregnancy in the pathogenesis of comorbidities thought to arise from the placenta, including pre-eclampsia or fetal growth restriction. If an increase in cardiac output (CO) is the hallmark physiologic adaptation of pregnancy, clinical intuition would suggest the increase in this parameter is more dramatic in multiple pregnancies. Echocardiographic studies support this increase in CO accompanied by a decrease in total vascular resistance (TVR).3 Longitudinal data demonstrate that patients with twin pregnancies complicated by placental insufficiency or pre-eclampsia show a decrease in CO and an increase in TVR compared to those without complication (Table 18.1).4 These studies parallel findings from the singleton literature supporting the association between aberrant maternal haemodynamics and adverse fetal and obstetric outcomes (Table 18.1).
Echocardiographic assessment of cardiac function during twin pregnancies highlights the importance of diastolic function. Diastolic function refers to the ability of the heart to relax during ventricular filling and, in the context of pregnancy, accommodate the increased plasma volume requisite to increase stroke volume and CO. Echocardiographic studies of uncomplicated twin pregnancies demonstrate a progressive decrease in diastolic function across trimesters supporting the toll of this subacute state of volume overload on the maternal heart. Post-partum assessment of diastolic function demonstrates impaired ventricular relaxation relative to first trimester values. Physiologically these findings can be considered evidence of the early adaptations in diastolic function in twin pregnancies or support the longterm impact of this exaggerated cardiovascular demand. The aforementioned changes in both systolic and diastolic function in twin pregnancies highlight the extreme adaptation required to support a multifetal pregnancy and perfuse the associated placentas.
Population-Level Data
A deeper understanding of the hallmark cardiovascular adaptations to pregnancy helps underscore some of the pathophysiology of pregnancy-associated comorbidities, like pre-eclampsia,
Table 18.1 Changes in haemodynamic parameters in uncomplicated twin compared to other pregnancies
| Parameter | Change across Uncomplicated Twin Pregnancy | Twin vs Singleton Pregnancy | Complicated* vs Uncomplicated Twin Pregnancy | Change across Complicated* Twin Pregnancy |
| Heart Rate | Increase | None | None | None |
| Stroke Volume | None | Higher | Higher | None |
| Cardiac Output | Increase | Higher | Lower | None |
| Systolic Blood Pressure | Increase | None | None | None |
| Diastolic Blood Pressure | Increase | None | None | None |
| Mean Arterial Pressure | Increase | None | None | None |
| Total Vascular | Decrease | Lower | Lower | None |
Resistance
* Complicated twin pregnancy is defined as pre-eclampsia or gestationalhypertension or birthweight of one or both twins less than the 5th percentile for gestationalage.
found in multifetal pregnancies. At the other end of the scientific spectrum, changes in haemodynamics can also inform the interpretation of studies exploring the epidemiology of extreme adverse outcomes including severe maternal morbidity or mortality. Studies from the Centers for Disease Control and World Health Organization independently report a threefold increase in the risk of all causes of maternal mortality for multifetal pregnancies compared to singleton pregnancies.2 These epidemiologic associations between multifetal pregnancy and SMM are remarkably consistent across a large time span in a variety of practice settings. The relative contribution of maternal comorbidities and available resources to improve maternal outcomes undoubtedly varies according to clinical environment. But the relative stability of the risk factors and their magnitude of effect underscores the obvious - there is something fundamentally different about multifetal pregnancy compared to singleton pregnancies.
For the physiologist, the aforementioned findings offer fascinating insight into the maternal cardiovascular adaptation to twin pregnancy. For the epidemiologist, the adverse maternal outcomes suggest potential public health interventions to improve outcomes. For the clinician, these physiologic and epidemiology studies considered in tandem offer important background to help contextualise the downstream maternal complications associated with multifetal gestations. Cardiovascular maladaptation may be a risk factor for developing pregnancy-specific comorbidities, but it also contributes to the maternal response to the physiologic challenge of pregnancy, labour and delivery.
The Issues
Addressing Maternal Risk
Simply stating a patient is at an increased risk of adverse outcomes relative to a singleton pregnancy without identifying a modifiable risk factor or intervention is of little use to the clinician charged with managing the patient at the bedside. Conversely, an understanding of the increased maternal risks associated with multifetal pregnancy compared to singleton pregnancy is helpful to both raise clinical suspicion for adverse maternal outcomes and offer background context on the limited physiologic reserve that may accompany this extreme haemodynamic state.
A broad overview of the maternal risks associated with multifetal pregnancy is a key part of counselling to encourage awareness of symptoms. National guidelines support offering nondirective patient counselling about the risks associated with higher-order multifetal pregnancies including the option of multifetal pregnancy reduction of one or more fetuses. The majority of evidence on multifetal pregnancy reduction centres on optimising neonatal outcomes but patient counselling should incorporate the maternal medical risks of multifetal pregnancy situated in the context of pre-existing maternal comorbidities.Quantifying an individual’s risk of severe maternal morbidity is challenging, but evidencebased scoring systems or algorithms exist. Using data from a French multicentre study of twin pregnancies, Korb and colleagues developed two algorithms to quantify maternal risk incorporating characteristics known at the onset of pregnancy and developing across the course of gestation.5 Key early risk factors for severe maternal morbidity included a pregnancy conceived by in vitro fertilisation (IVF), nulliparity and maternal country of birth. These risk factors evolved later in pregnancy to include the presence of pre-eclampsia, placenta praevia and fetal macrosomia. This type of individualised risk assessment presented to patients as absolute and not relative risk is more clinically useful than the aforementioned studies comparing women with multifetal gestations to women with singleton gestations.
First-Trimester Clinical Complaints
After appropriate counselling, attention should be directed towards available strategies for maternal risk reduction. National guidelines support the use of low-dose aspirin beginning at 12 weeks for all patients with multifetal pregnancies to reduce the risk of pre-eclampsia. Contemporary meta-analyses demonstrate a relative risk for preterm pre-eclampsia of 0.62 (95% CI 0.45-0.87).6 Subsequent stratified analyses demonstrate this reduction in preterm pre-eclampsia was confined to trials where aspirin was initiated prior to 16 weeks at a dose at or above 100 mg. The inclusion of twin and multifetal pregnancies in studies examining the impact of aspirin on pre-eclampsia is variable. Most guidelines continue to endorse administration of 81 mg of aspirin. The evidence supporting the efficacy of a slightly higher dose coupled with the increased volume of distribution and clearance in multifetal pregnancy could support a role for higher doses of 100-150 mg in this population.
Management of other first-trimester maternal issues such as nausea and vomiting of pregnancy or hyperemesis gravidarum parallels recommendations for singleton pregnancies. Multifetal pregnancies carry with them an increased metabolic demand warranting dedicated anticipatory guidance and tailored consideration in addressing complications. The Institute of Medicine (IOM) recommends a gestational weight gain of 37-54 pounds for women of normal weight, 31-50 pounds for overweight women and 25-42 pounds for those with comorbid obesity. 7 The increased metabolic demand and higher nutritional requirement of multifetal pregnancies may lower the threshold for initiation of supplemental nutrition. The reported tolerance of enteral nutrition coupled with known complications of total parenteral nutrition including line-associated sepsis and thromboembolic disease make enteral nutrition via nasogastric tube the preferred approach. The IOM recommendations are derived from studies demonstrating decreased rates of preterm birth and larger neonatal birthweights in women achieving the set thresholds, but the impact of this weight gain on maternal outcomes is unknown.7 Monitoring for excessive weight gain is equally important to optimise pregnancy outcomes and long-term maternal health.
Physical activity in pregnancy plays an important role in avoiding excessive weight gain. Authorities acknowledge the benefits of physical activity and encourage aerobic and strength-conditioning exercises for women with uncomplicated pregnancies. However, they go on to list multiple gestation at risk of premature labour as an absolute contraindication to aerobic exercise during pregnancy without quantifying this level of risk for the clinician. If improving cardiopulmonary reserve is a benefit of physical activity and patients with multifetal gestations are subject to complications rooted in failure to compensate to haemodynamic demands, reason would suggest that women with multifetal pregnancies may derive additional benefits from exercise. With this in mind, reinforcing the recommendation of 150 minutes per week of moderateintensity aerobic activity equivalent to brisk walking in women with multifetal pregnancies seems warranted. The ability of physical activity to improve obstetric outcomes in women with multifetal gestation is unknown, but early encouragement of physical activity is a low-risk intervention with the potential short- and long-term benefits to a woman's health.
Third-Trimester Clinical Conundrums
After this initial anticipatory guidance, the majority of antenatal care for women with multifetal gestations is dedicated to the prevention and early detection of complications arising in the late second and third trimester such as spontaneous preterm birth, fetal growth restriction or pre-eclampsia (Table 18.2). Many guidelines support screening, diagnosis and management for pregnancy complications in a similar way as singleton pregnancies. However, close attention to the rationale and evidence informing these recommendations in singletons and how they may (or may not) be applicable to multife- tal pregnancies is warranted. For example, gestational diabetes mellitus (GDM) can be considered another placentally mediated adaptation or complication of multifetal pregnancies associated with the aforementioned increased metabolic demand. The rationale for universal screening for GDM is derived from randomised controlled trial and metaanalysis data demonstrating a reduction in rates of shoulder dystocia, macrosomia and pre-eclampsia with treatment. Though macrosomia and shoulder dystocia seem less relevant for multifetal pregnancies, the pooled relative risk reduction for pre-eclampsia is estimated at 0.66 (95% CI 0.48-0.90), highlighting the importance of glycaemic control for maternal indications.
Given the baseline complexity of multifetal pregnancies and the higher prevalence of adverse outcomes, management of comorbidities may often occur in the inpatient setting to which underscores the importance of prevention of venous thromboembolism (VTE). A key principle of VTE prophylaxis is encouraging physical activity. There is no evidence to support bed rest in the management of obstetric conditions with the most robust data supporting its lack of efficacy or even potential harm. Activity restriction may offer the benefit of lowering blood pressure in cases of pre-eclampsia, but ambulation should still be encouraged in this population to both reduce the risk of VTE and prevent deconditioning.9 In addition to activity, contemporary guidelines support the use of pharmacologic VTE prophylaxis in patients hospitalised for at least 72 hours who are not at high risk for bleeding or imminent childbirth.10 The main drawback for pharmacologic prophylaxis is the possibility that recent medication administration may be a contraindication to neuraxial analgesia. Guidelines recommend waiting 4-6 hours since the last prophylactic dose of unfractionated heparin and 12 hours since the last dose of prophylactic low-molecular-weight heparin before proceeding with neuraxial analgesia. Balancing the need for VTE prophylaxis in this high-risk population with a similarly elevated risk of imminent delivery suggests that a pharmacologic approach centred on unfractionated heparin seems reasonable. From a practical standpoint, if a patient is too unstable to wait the 4 hours between unfractionated heparin administration and neuraxial analgesia for delivery, then it is possible her clinical condition may also be unstable enough to warrant general anaesthesia at delivery.
Management Options
Balancing Maternal Risks with Neonatal Outcomes
Despite the best efforts at prevention, complications of multifetal pregnancy are inevitable and when they arise, general recommendations are to manage them as you would a singleton pregnancy. Developing guidelines specific to twin or higher-order multiple pregnancies would be challenging if not impossible both due to the tremendous effort required and the paucity of evidence supporting management strategies specific to this population.8 Managing multifetal pregnancies in a similar approach to singleton
Table 18.2 Contributing factors and proposed management strategies for common causes of severe maternal morbidity in Imultifetalpregnancies
| Type of Morbidity | Contributing Factors | Management Strategies |
| Haemorrhage | Uterine atony | Active management of 3rd-stage early uterotonic administration Delivery in operating room Dedicated anaesthesia support |
| Abnormalities of placentation | High index of suspicion Early surgical intervention Experienced surgeon available | |
| Exaggerated anaemia | Consideration of IV iron Ensure availability of blood | |
| Caesarean delivery | Encourage vaginal birth Prepare for breech extraction | |
| Hypertensive Disorders | Increased placental mass | Universal low-dose aspirin Multifetal reduction counselling |
| Maternal cardiovascular health | Support single embryo transfer Encourage physical activity | |
| Atypical presentations common | Low index of suspicion Close clinical follow-up | |
| Preterm presentations common | Closely monitor maternal status Balance with fetal outcomes | |
| Cardiopulmonary Events | Extreme haemodynamic demand | Screening echocardiography Consider in delivery timing |
| Antepartum deconditioning | Encourage physical activity Consider physical therapy | |
| Complications of transfusion | Cross-matched blood available Earlier surgical intervention | |
| Activity restriction | Explicitly prohibit bed rest and encourage physical activity | |
| More inpatient hospitalisations | Pharmacologic prophylaxis Support inpatient activity | |
| Complex clinical presentation | Low threshold for diagnostics Consider empiric anticoagulation |
pregnancies makes practical sense but fails to account for the unique considerations affecting both maternal and neonatal outcomes (Figure 18.2).
Consider a case of pre-eclampsia. Expectant management of pre-eclampsia with severe features is advocated prior to 34 weeks in appropriately selected populations to improve neonatal outcomes without increasing maternal risk. The benefit of prolonging pregnancy for two or more neonates must be balanced with the higher risk of adverse maternal outcomes and limited ability to compensate haemodynamically to the demands of pregnancy. Patients with multifetal pregnancies are more likely to present with atypical features of the disease demanding more frequent laboratory surveillance and a lower threshold to explore seemingly unrelated subjective complaints. Though ambulatory monitoring of preeclampsia can be considered in the absence of severe features, the need for increased maternal and fetal surveillance in twins relative to singletons makes inpatient management an appealing option. Keeping anticipated maternal outcomes and the resources and personnel available to address these at a given centre is of paramount importance and somewhat independent of neonatal needs.11 With the complexities of balancing maternal risk with neonatal outcomes in mind, patients with maternal or obstetric comorbidities may benefit from the presence of a clinician with experience caring for complicated multifetal pregnancies.
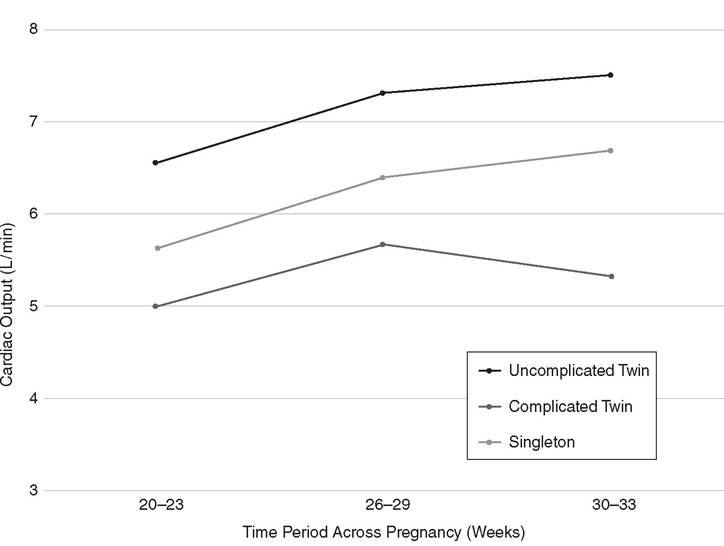
Figure 18.2 Balancing maternaland fetaloutcomes when considering delivery timing in complicated multifetal gestations
Ensuring a Safe and Successful Vaginal Birth
Whether spontaneous or indicated, delivery timing is only one consideration in the conversation on maternal outcomes for multifetal pregnancy. For twin pregnancies in particular, the decision to attempt a trial of labour in hopes of vaginal birth or to pursue an elective caesarean delivery is an evolving clinical question. Despite a wealth of research focusing on the interaction between neonatal outcomes and mode of delivery, few studies have explored this question for maternal morbidity and mode of delivery.
The publication of a landmark randomised controlled trial - the Twin Birth Study - supported the neonatal safety of attempted twin vaginal birth when the presenting fetus is cephalic.12 Their composite maternal outcome including death and serious maternal morbidity was 7.3% in the planned caesarean delivery group and 8.5% in the planned vaginal birth group (odds ratio 0.86, 95% CI 0.65-1.13). Current guidelines aimed at preventing primary caesarean delivery encourage an attempted vaginal delivery for twins when the presenting fetus is cephalic.
These recommendations rely on the data of Barrett and colleagues and apply the known short and long-term morbidity associated with caesarean delivery from the singleton population. Using French data, Madar and colleagues attributed 20.6% (95% CI 12.9-28.2) of SMM to caesarean delivery, highlighting attempted vaginal delivery as a maternal risk reduction strategy. But observational data from the United States show a higher odds of haemorrhage for women attempting vaginal delivery compared to those electing for caesarean delivery. The need for operative vaginal or caesarean delivery of one or both twins during the course of labour may account for some of the conflicting findings in the literature. The increased rates of operative vaginal and intra-partum caesarean delivery in twin pregnancies coupled with variable provider experience in twin vaginal birth and breech extraction highlight that an attempted vaginal birth carries unique considerations in this population.
Guidelines encouraging attempted vaginal birth for twins fail to elaborate on the accompanying anticipatory counselling and proactive intra-partum management requisite to optimise patient outcomes and satisfaction. The concept of breech extraction, the safety data supporting its use and how this differs from a singleton breech vaginal delivery should be discussed. The possibility of intra-partum presentation change from cephalic to non- cephalic presentation as well as the potential role of internal podalic version and breech extraction to expedite delivery of the unengaged cephalic second twin would suggest all patients - even those with cephalic second twins at the onset of labour - be prepared for this possibility. External cephalic version of the non-vertex second twin increases the odds of caesarean delivery of the second twin compared to breech extraction, suggesting its practice should be limited if not abandoned. Ideally, all providers performing twin vaginal deliveries should have a baseline comfort with breech extraction to optimise maternal outcomes. Whether or not a patient with a cephalic second twin should be encouraged to elect caesarean delivery if a provider with this skill set is unavailable is unclear. Clinicians should prioritise shared decision-making, taking into account patient preference, obstetric history and future fertility goals when counselling patients about mode of delivery for twins.
Mitigating Maternal Risk at Delivery
Regardless of mode of delivery, the third stage is a time of increased risk for twins and higher-order multiples. Though uterine atony is most classically associated with multifetal pregnancy, abnormalities of placentation such as placenta praevia and placenta accreta spectrum are more prevalent in this population. As with many obstetric comorbidities, the management of post-partum haemorrhage independent of aetiology parallels that of singleton pregnancy. But the high risk of post-partum haemorrhage and peri-partum hysterectomy in multifetal pregnancies coupled with concerns about increased downstream morbidity warrants a proactive approach predating the patient's arrival on labour and delivery.14
Optimising maternal status in anticipation of delivery is a key component of antenatal care. Early workup and aggressive management of the anaemia of pregnancy, including the use of intravenous iron, is central. Patients with underlying cardiovascular risk factors, including increasing maternal age, chronic hypertension, pre-eclampsia, pre-gestational diabetes or maternal cardiovascular disease, may benefit from transthoracic echocardiography in the third trimester to assess ventricular systolic and diastolic function.3,4 The diagnosis of overt systolic failure in the absence of cardiopulmonary complaints is unlikely, but impaired ventricular relaxation may limit the patient's ability to tolerate large volume transfusion, putting the patient at risk of transfusion-associated circulatory overload (Table 18.3). Concerns for limited haemodynamic reserve may impact clinical decision-making for the provider tasked with managing a haemorrhage, prompting earlier decision to proceed with uterine artery embolisation or definitive surgical management with hysterectomy.
Being prepared for a potential haemorrhage is important for any delivery, but even more so for those involving multifetal pregnancies.14 Active management of the third stage, early medical management with uterotonics and tranexamic acid and availability of blood products are the mainstays of avoiding haemorrhage-associated SMM in this population. National guidelines support delivery of term twin gestations in basic care centres - some of which may have limited blood bank availability or surgical support.11 For patients with multifetal gestation with other haemorrhage risk factors or compounding maternal comorbidities, consideration should be given to the appropriate delivery setting to ensure the patient has the adequate resources and personnel available to address her anticipated intrapartum needs. For some centres, this may involve ensuring additional blood products or anaesthesia care providers are available. For others, this may prompt discussion of transfer of care to optimise maternal outcomes. Regardless of the exact circumstances, a proactive
Table 18.3 Distinguishing transfusion-associated acute lung injury (TRALI) from transfusion-associated circulatory overload (TACO) in haemorrhage-associated pulmonary oedema
| Feature | TRALI | TACO |
| Oedema Pathophysiology | Exudate | Transudate |
| Blood Component | Typically plasma or platelets | Any |
| Blood Pressure | Hypotension | Hypertension |
| Temperature | Elevated | Normal |
| White Blood Cell Count | Leukopenia | Unchanged |
| BNP | Low | Elevated |
| Echocardiogram | Normal ejection fraction | Decreased ejection fraction |
| Diuretics | Worsen | Improve |
| Fluid Response | Improve | Worsen |
approach incorporating maternal comorbidities to prepare for anticipated needs will optimise maternal outcomes at the time of delivery.
Optimising Post-partum Maternal Care
Delivery certainly poses a high-risk time for mothers of multifetal gestations, but the psychosocial complexities of parenting multiples highlights the post-partum period as a vulnerable time.15 Rates of depression and anxiety are higher in parents of multiples with preterm infants requiring admission to the neonatal intensive care unit, conferring additional risk. This coupled with the challenges of breastfeeding, the financial impact and social considerations make the need for increased post-partum support self-evident (Figure 18.3). This need is perhaps even greater for parents suffering from a loss of one or more fetuses during their pregnancy. Close-interval follow-up at the two-week post-partum mark either via phone or in person offers an opportunity for early detection and intervention for post-partum mood disorders. The need for reliable contraception should be emphasised at the six-week visit and throughout post-partum care independent of comor- bid diagnoses of infertility or subfertility.
Patients with prolonged hospitalisations or traumatic birth experiences may benefit from a dedicated visit 3-6 months post partum to review the circumstances of delivery and screen for evidence of childbirth-associated post-traumatic stress disorder. This may be particularly important for patients transferred to referral centres for delivery who may have an otherwise limited ability to access information about the circumstances of their deliveries as a part of post-partum care. This extended post-partum follow-up also affords providers the opportunity to discuss the impact of pregnancy-associated complications on not only future pregnancies, but also on long-term health. Regardless of the approach to post-partum care, dedicated attention to the maternal psychosocial state is an essential component of optimising maternal outcomes in multifetal pregnancies.
Prioritising maternal outcomes in multifetal pregnancies isn't easy. The healthcare system, available scientific evidence and even the patient often focus on the fetal
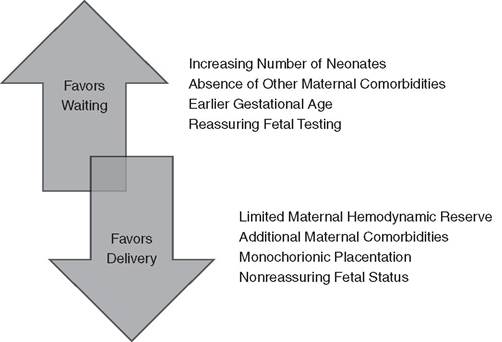
Figure 18.3 Algorithm for Clinicaldecision about delivery timing
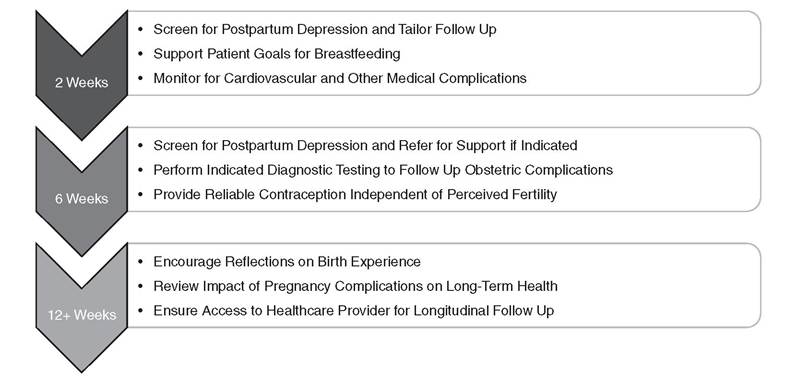
Figure 18.4 Outline for postpartum follow-up
component of this high-risk state. The obstetric care provider may be the first and sometimes only line of defence against adverse maternal outcomes. A uniform approach to management followed by tailored risk-appropriate care as clinical complexities arise is paramount. As decreasing severe maternal morbidity and mortality climbs towards the top of the public health agenda, one must hope that studies and guidelines dedicated to minimising the maternal complications of multifetal pregnancies will follow. Until that time, the obstetric care provider must be the champion for maternal health in multifetal pregnancies.
Key Points
• An increase in placental mass, exaggerated physiologic needs and complexities in clinical management contribute to higher rates of maternal morbidity in multiple pregnancies.
• Hallmark haemodynamic changes of multiple pregnancy include an increased CO with exaggerated plasma volume expansion.
• Failure to meet these physiologic demands contribute to the pathophysiology of obstetric and fetal processes such as growth restriction and pre-eclampsia.
• Administration of low-dose aspirin and attention to optimising nutrition are key tenets of risk reduction in the first trimester.
• Instruct patients to avoid bed rest and engage in physical activity to minimise risk of venous thromboembolism and maximise cardiopulmonary fitness.
• Balancing maternal risk and fetal benefit in multiple pregnancy should incorporate a model of shared decision-making between the patient and her provider.
• Encourage attempted vaginal delivery in patients with a cephalic presenting first twin and ensure support is available to facilitate a safe and successful vaginal birth of
the second, independent of presentation.
• Actively manage the third stage of labour, keeping in mind the comparatively limited cardiopulmonary reserve to manage large volume transfusion.
• Ensure dedicated post-partum follow-up acknowledging the psychosocial impact of multiple pregnancy - particularly those with a complex antenatal course.
• Refer patients with comorbidities complicating multiple pregnancy to hospitals with the resources and personnel to address maternal, not just neonatal needs.
References
1. CommitteeonPracticeBulletins - Obstetrics, Society for Maternal-Fetal Medicine. ACOG Practice Bulletin No. 169: Multifetal gestations: twin, triplet and higher-order multifetal pregnancies. Obstet Gynecol 2016 Oct;128(4):e131-e146.
2. Santana DS, Cecatti JG, Surita FG et al. Twin pregnancy and severe maternal outcomes: the World Health Organization multi-country survey on maternal and newborn health. Obstet Gynecol 2016;127(4):631-41.
3. Ghi T, Kuleva M, Youssef A et al. Maternal cardiac function in complicated twin pregnancy: a longitudinal study. Ultrasound Obstet Gynecol 2011;38:581-5.
4. Ghi T, Esposti D, Montaguti E et al. Maternal cardiac evaluation during uncomplicated twin pregnancy with emphasis on the diastolic function. Am J Obstet Gynecol 2015;213(3):375.e1-e8.
5. Korb D, Schmitz T, Seco A et al. Risk factors and high-risk subgroups of severe acute maternal morbidity in twin pregnancy: A population-based study. PLoS One 2020;15 (2):e0229612.
6. Roberge S, Bujold E, Nicolaides KH. Aspirin for the prevention of preterm and term preeclampsia: systematic review and metaanalysis. Am J Obstet Gynecol 2018;218(3):287-93.
7. Fox NS, Rebarber A, Roman AS, Klauser CK, Peress D, Saltzman DH. Weight gain in twin pregnancies and adverse outcomes: examining the 2009 IOM guidelines. Obstet Gynecol 20105116(1):100-6.
8. SMFM Research Committee, Grantz KL, Kawakita T et al. SMFM special statement: state of the science on multifetal gestations:
unique considerations and importance. Am J Obstet Gynecol 2019 Aug;221(2):B2-B12.
9. Crowther CA, Han S. Hospitalisation and bed rest for multiple pregnancy. Cochrane Database Syst Rev 2010 (7). Art. No.: CD000110. https://doi.org/10.1002/146518 58.CD000110.pub2
10. D'Alton ME, Friedman Am, Smiley RM et al. National Partnership for Maternal Safety: consensus bundle on venous thromboembolism. Obstet Gynecol 2016;128(4):688-98.
11. American Association of Birth Centers; Association of Women's Health, Obstetric and Neonatal Nurses; American College of Obstetricians and Gynecologists et al. Obstetric Care Consensus #9: Levels of Maternal Care. Am J Obstet Gynecol 2019;221(6):B19-B30.
12. Hutton EK, Hanna ME, Ross S et al. Maternal outcomes at 3 months after planned caesarean section versus planned vaginal birth for twin pregnancies in the Twin Birth Study: a randomized controlled trial. BJOG 2015;122(12):1653-62.
13. Easter SR, Robinson JN, Lieberman E, Carusi D. Association of intended route of delivery and maternal morbidity in twin pregnancy. Obstet Gynecol 2017; 129 (2):305-10.
14. Main EK, Goffman D, Scavone BM et al. National Partnership for Maternal Safety: consensus bundle on obstetric hemorrhage. Obstet Gynecol 2015 Jul;126(1):155-62.
15. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 736: optimizing postpartum care. Obstet Gynecol 2018;131(5):e140-e150.