Management of Twin Anaemia- Polycythaemia Sequence
Liesbeth Lewi and Enrico Lopriore
The Facts
Twin anaemia polycythaemia sequence (TAPS) is a unique complication of monochorionic multiple pregnancies characterised by a severe difference in haemoglobin levels with an anaemic donor and a polycythaemic recipient.
It is caused by a chronic transfusion of red blood cells across minuscule (1 mm or less) placental vascular anastomoses.1,2Before birth, we can detect TAPS by an elevated middle cerebral artery peak systolic velocity (MCA-PSV) at or above 1.5 multiples of the median (MoM) in the donor in combination with a decreased MCA-PSV at or below 0.8 MoM in the receptor. Also, an inter-twin discordance between MCA-PSV values of 1 MoM or more indicates the presence of TAPS. After birth, we make the diagnosis of TAPS if the haemoglobin difference is at least 8 g/dL. To indicate a chronic transfusion imbalance, the donor must show signs of increased erythropoiesis with an elevated reticulocyte count. In contrast, the recipient must demonstrate a suppressed erythropoiesis with a decreased reticulocyte count, resulting in a donor: recipient reticulocyte count ratio of 1.7 or more.3 Alternatively, the presence of only minuscule anastomoses proves the transfusion imbalance must have occurred over a long time.1,2
On ultrasound scan, additional signs commonly point towards the presence of TAPS. Typically, there is a striking discrepancy in the echogenicity and thickness between the two placental parts. As such, the donor share is usually white and thick whereas the recipient’s part is dark and thin (Figure 14.1A). The anaemic donor often has cardiomegaly whereas the polycythaemic recipient typically has a ‘starry sky’ aspect of the liver (Figure 14.1B).4
Twin anaemia polycythaemia sequence can occur in a previously uncomplicated pregnancy or after fetoscopic laser surgery for twin-twin transfusion syndrome (TTTS) if small anastomoses remain open.1,2 Spontaneous TAPS is rare and its incidence is probably only around 3% in monochorionic-diamniotic twin pregnancies.5 Similarly, the incidence of post-laser TAPS is also 3% if the Solomon technique is used.6 In monoamniotic pairs, TAPS is extremely rare as usually these twins have proximate cord insertions with large anastomoses.
If a transfusion imbalance occurs in a monoamniotic pregnancy, it is usually an acute and substantial transfusion leading to unexpected and usually double demise before any amniotic fluid or haemoglobin discordances appear.In contrast to TTTS, which is typically diagnosed between 16 and 26 weeks of gestation, spontaneous TAPS can occur at any time during pregnancy from as early as the first trimester to late into the third trimester.2,7 Post-laser TAPS usually occurs one to four weeks after the surgery. Twin anaemia polycythaemia sequence is classified according to severity into five stages (Table 14.1).8 Although TAPS has a more benign course than TTTS,
| Table 14.1 | Antenataltwin anaemia polycythaemia sequence staging8 |
| Staging | Findings on prenatal ultrasound examination |
| Stage 1 | MCA-PSV donor > 1.5 MoM and MCA-PSV receptor < 1.0 MoM with no other signs of compromise |
| Stage 2 | MCA-PSV donor > 1.7 MoM and MCA-PSV receptor < 0.8 MoM with no other signs of compromise |
| Stage 3 Stage 4 Stage 5 | Cardiac compromise of the donor with critically abnormal Doppler Hydrops of donor Fetal demise of donor or receptor with TAPS |
TAPS = twin anaemia-polycythaemia sequence; MCA-PSV= middle cerebral artery - peak Systolicvelocity; MoM = multiple of the median
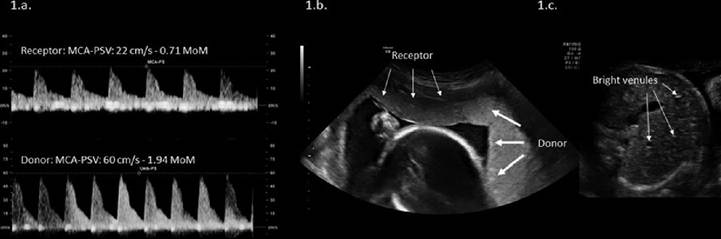
Figure 14.1 Ultrasound images of a spontaneous TAPS at 24 weeks of gestation. (a) The receptor has decreased MCA-PSV. The donor twin's MCA-PSV is increased. (b) The receptors' placentalpart is dark and thin (thin arrows) whereas the donor's part is white and thickened (thick arrows).
(c) The receptor also has a 'starry sky' aspect of the liver due to bright venules (arrows). Both have normalamniotic fluid. This patient underwent a fetoscopic laser coagulation of five tiny anastomoses followed by a Solomon line combined with an intrauterine transfusion of the donor for a haemoglobin of 4 g/dL. She delivered two healthy boys at 34 weeks of gestationalage.TAPS may lead to fetal and neonatal demise. As such, fetal loss occurs in about 10-15% whereas the neonatal mortality rate is around 5-10%.9,10
Severe anaemia may also lead to growth restriction, hydrops and cerebral haemorrhage. Likewise, hyperviscosity in the receptor may cause cerebral insults or vascular occlusion with limb necrosis and amputations. Babies with TAPS are born early, around 32 weeks, and hematologic complications are common in the neonatal period with the need for transfusion and exchange transfusion in the donor and receptor, respectively.9,10 Because of these increased risks and because antenatal treatment is available, we should screen all mono- chorionic twin pregnancies with a fortnightly (biweekly) scan not only for TTTS, but also for TAPS by measuring the MCA-PSV in both twins from 20 weeks onwards, in pregnancies with selective growth restriction, after fetoscopic laser surgery for TTTS or whenever there is a sonographic suspicion of TAPS.11,12
Twin anaemia polycythaemia sequence is characterised by a haemoglobin difference. In TAPS, the amniotic fluid may differ between the twins, but the deepest vertical pocket is
more than 2 cm in the donor and less than 8 cm in the recipient. If the amniotic fluid discordance complies with the TTTS criteria, we classify and treat the pregnancy as TTTS. The hallmark of TTTS is a discrepancy in amniotic fluid and generally, both twins have similar haemoglobin levels. Nevertheless, a minority of TTTS pregnancies (about 10-15%), are accompanied by TAPS with a polycythaemic recipient and an anaemic donor.13 In TAPS, as in TTTS, the donor is commonly smaller than the recipient because the transfusion imbalance affects the growth in monochorionic pregnancies.
If growth is concordant, then the recipient usually has the smaller placental share and the more marginal cord insertion. Twin anaemia polycythaemia sequence must be excluded in growth-discordant monochorionic pairs as management will differ.Twin anaemia polycythaemia sequence is a chronic inter-twin transfusion imbalance and must be differentiated from an acute inter-twin transfusion. An acute transfusion may happen during pregnancy, generally leading to the demise of both twins, or during labour. Acute inter-twin transfusion requires a low-resistance artery-to-artery anastomosis that permits rapid exsanguination of one twin into the other twin. Before birth, a large artery-to- artery anastomosis, proximate cord insertions, a similar echogenicity of the placental territories or a type 3 selective growth restriction decrease the likelihood of TAPS. After birth, colour injection of the placenta with the demonstration of a large artery-to-artery anastomosis confirms an acute inter-twin transfusion. Also, if the maternal side of the placenta has a similar colour, this indicates an acute rather than a chronic transfusion imbalance because TAPS placentas characteristically have a clear colour difference between the two placental territories (Figure 14.2).14 Other reasons for an elevated MCA-PSV or an inter-twin MCA-PSV discordance of 1 MoM or more must be excluded too. As such, in selective growth restriction, the smaller twin commonly has a higher MCA-PSV than the appropriately growing twin in the context of brain sparing.
The Issues
Twin anaemia polycythaemia sequence was described for the first time only ten years ago, first as a complication after fetoscopic laser surgery for TTTS1 and second as a transfusion imbalance in previously uncomplicated twin pregnancies.2 Because of its recent discovery and rarity, many uncertainties remain about its pathophysiology, natural history, diagnostic criteria and management.
We do not know why a transfusion imbalance sometimes presents as a discrepancy in amniotic fluid, like in TTTS, and at other times as a haemoglobin difference, like in TAPS.
It seems the number and type of anastomoses are similar in TTTS and TAPS placentas, but their size differs. Compared to uncomplicated monochorionic placentas, TTTS and TAPS placentas have fewer anastomoses, and typically the artery-to-artery anastomosis is missing. An artery-to-artery anastomosis allows flow in both directions and compensates for any imbalances in inter-twin transfusion. In contrast, in TTTS and TAPS, usually, only artery- to-vein connections are present, which allow flow in one direction only and may cause an inter-twin transfusion imbalance. In contrast to TTTS, the anastomoses in TAPS are significantly smaller (less than 1 mm) and require colour injection to make them visible to the naked eye. This also explains why TAPS may occur after laser surgery for TTTS if we only coagulate the visible anastomoses. By coagulating the large anastomoses, TTTS will disappear, but TAPS may become apparent several weeks later if tiny anastomoses are missed.15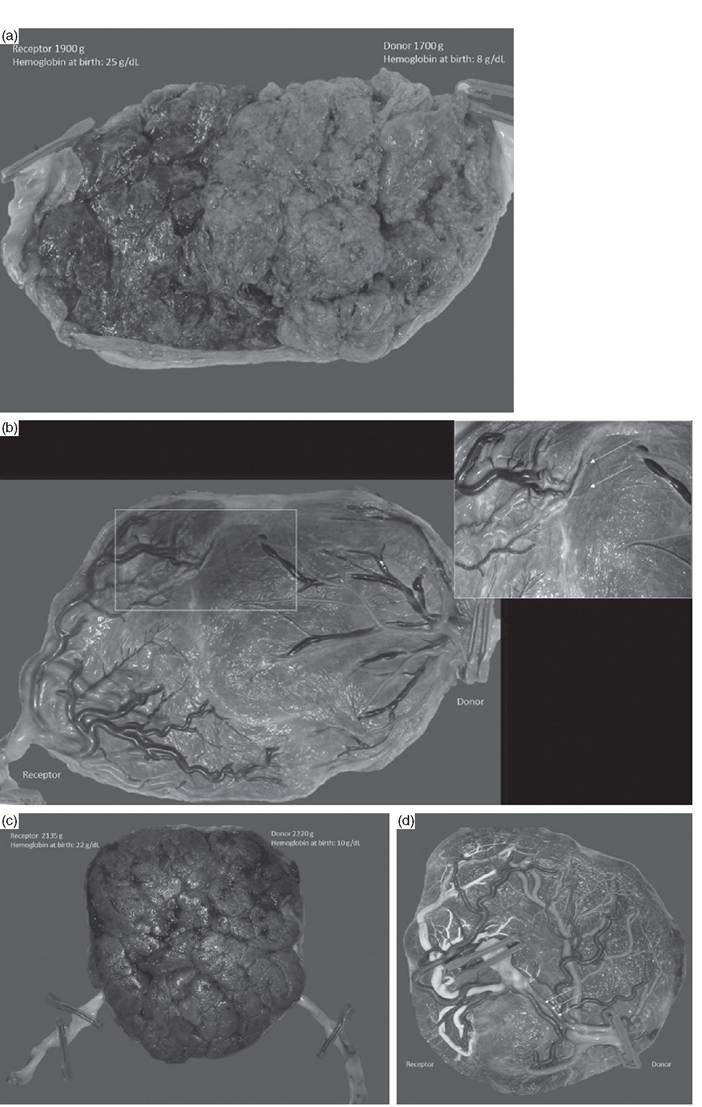
Figure 14.2 (a) Image of the maternalsidefrom a monochorionic placenta of a SpontaneousTAPSdiagnosed at 30 weeks of gestation. This patient received one intrauterine transfusion at 31 weeks and was delivered electively at 32
The larger the anastomoses, the larger the placental part shared by the twins. In TTTS, the twins have a larger shared part than in TAPS, where the twins are connected by minuscule vessels. The size of this shared placental part probably determines if an imbalance results in TTTS rather than TAPS. Although both TTTS and TAPS are due to imbalanced blood flow, the large shared territory in TTTS allows the recipient to recruit fluid into its vascular compartment, which masks its polycythaemia but leads to polyuria and polyhydramnios. On the other hand, the large shared territory allows the donor to contract its vascular compartment and mask the anaemia, which leads to oliguria and oligohydramnios.
When we coagulate all visible anastomoses, we eliminate the shared part, but when tiny communications are left, a chronic net transfer of blood will occur for which the twins can no longer compensate (Figure 14.3).15The natural history of TAPS is also not well documented. The data currently available are from tertiary referral centres and the outcomes may be biased as it is likely that more severe TAPS cases are included.9,10 As such, it is uncertain what proportion of mild TAPS cases, diagnosed in the first or early second trimester, resolve spontaneously without any intervention.7 Also, data on long-term neurodevelopment are limited and based on small cohorts from tertiary referral centres only. These studies suggest a similar risk of severe neurological impairment of 9% after spontaneous and post-laser TAPS. However, in spontaneous TAPS, the donor had a four times higher risk of impairment than the recipient. Also, one in eight donors had bilateral hearing loss.10 Although these numbers underscore the need to organise neurodevelopmental follow-up for these infants, because of possible selection bias of tertiary referral cases, the real impairment rate is likely somewhat lower.
The antenatal criteria to define TAPS have changed repeatedly. As such, for the recipient, a cut-off of 1.0 rather than 0.8 MoM has been proposed. The discordance between the MCA-PSV values may be more accurate than the individual MCA-PSV values of donor and recipient, but it is uncertain whether we best use a discordance of 1 MoM, as is currently recommended, or 0.5 MoM. Another limitation with the current antenatal definition is that it does not distinguish between an acute or chronic inter-twin transfusion imbalance and that an elevated MCA-PSV in the context of brain sparing may lead to a wrong TAPS diagnosis. Additional criteria, such as a difference in placental echogenicity, cardiomegaly in the donor or starry sky liver in the recipient, may improve diagnostic accuracy.
Also, we do not have data from controlled studies on the best management of TAPS. The results from a small observational study comparing fetoscopic laser surgery with intrauterine transfusion did not show a difference in survival and severe neonatal morbidity. However, laser surgery prolonged the interval between diagnosis and birth and decreased the risk of respiratory distress syndrome.9 At present, we decide management for each case individually based on the gestational age, the severity of the disease, the feasibility to perform an intervention and the preference of the patient. We discuss the four different management options next.
Caption for Figure 14.2 (cont.)
weeks. There is a striking colour difference between the two parts. Also, the larger receptor had the smaller part of the placenta, indicating that TAPS influences fetalgrowth. (b) Image of the fetalside after colour injection. There were tiny artery-to-vein anastomoses (arrows). (c) Image of the maternalside from a monochorionic placenta of an acute peri-partum inter-twin transfusion. The babies were born vaginally at 34 weeks. There is no colour difference between the placentalshares. (d) Placentalinjection showed a large artery-to-artery anastomoses (arrow), confirming an acute intra-partum transfusion as the cause of the haemoglobin difference. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
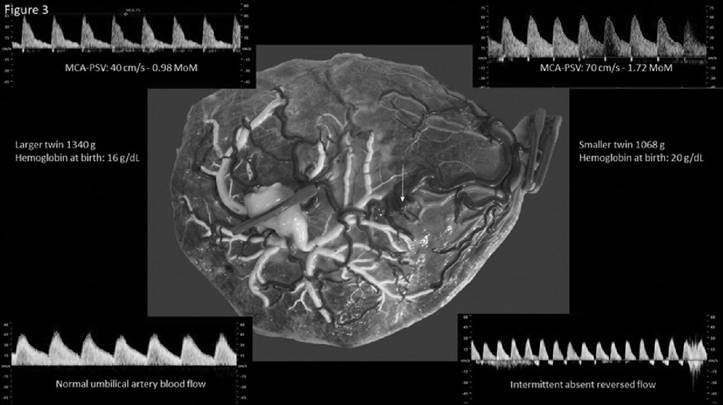
Figure 14.3 Monochorionic twin pair with type 3 selective growth restriction at 30 weeks of gestationalage. Because of brain sparing, the MCA-PSV was increased in the smaller twin and normal in the larger twin. The typical intermittent absent or reversed end-diastolic flow pattern in the Umbilicalartery of the smaller twin indicates the presence of a large artery-to-artery anastomosis, which precludes the diagnosis of TAPS. The placenta showed the typical features of a type 3 growth restriction with a large artery-to-artery anastomosis (arrows) and little individual territory for the smaller twin with the marginalinsertion. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
The Management Options
As mentioned previously, the proposed management (Figure 14.4) is not validated by controlled studies. For each case, a dedicated plan must be developed that weighs the risks and benefits, taking into account the characteristics of each case.8
Expectant Management
Expectant management is currently preferred for stage 1 TAPS.8 Usually, we review the patient within one week to confirm the diagnosis and assess the evolution. Also, we manage stage 2 before 18 weeks and after 28 weeks expectantly. In the early second trimester, the natural history is not well documented, and TAPS may disappear spontaneously when the minuscule TAPS vessels close spontaneously with rapid placental growth.7 Moreover, fetoscopic laser surgery or intrauterine transfusion carries higher loss rates when performed at these early gestational ages. After 28 weeks, the aim is to gain a week or two to attain the 30- to 32-week limit when the risks of severe neonatal morbidity decrease. Fetoscopic laser surgery is usually no longer performed for TAPS after 28 weeks, and intrauterine transfusions should be well timed and limited in number, as each transfusion of the anaemic donor will increase the polycythaemia of the receptor. Therefore, after 28 weeks, we first administer a course of steroids for lung maturation and follow these pregnancies twice a week to timely detect any signs of cardiac decompensation in the donor twin.

Figure 14.4 Images of a monochorionic pair with IIlS and coexistent TAPS at 28 weeks. The deepest vertical pocket was 11 cm in the receptor and 1.3 cm in the donor. At 28 weeks, we coagulated a visible artery-to-vein anastomosis and three tiny, unspecified anastomoses. We could not draw a Solomon line on the placenta because of intra-amniotic bleeding. After the surgery, TTTS disappeared but TAPS persisted. At 29 weeks, we gave an intrauterine transfusion to the donor for a haemoglobin of 6 g/dL and a partial exchange transfusion of the recipient for a haemoglobin of 21 g/dL. She was delivered electively at 32 weeks. The placenta showed minuscule, residualartery-to-vein anastomoses from the donor (2 clamps) to the receptor (1 clamp). (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
Fetoscopic Laser Coagulation of the Vascular Anastomoses
Fetoscopic laser coagulation of the anastomoses cures TTTS and is currently the preferred treatment modality for mid-trimester TTTS. The shared circulation is also the underlying cause of TAPS, and therefore fetoscopic laser surgery may be the best treatment for TAPS in the second trimester. However, controlled studies are not yet available and the intervention is more challenging in TAPS for several reasons. First, there is no poly-oligohydramnios in TAPS. In the absence of a stuck donor, the septum floats freely between the twins and the anastomoses may be behind the inter-twin septum, which then necessitates a septostomy to occlude all anastomoses. Additionally, in the absence of polyhydramnios, the amniotic fluid is more turbid, which hampers visibility, and if the placenta is anterior, there may be no placenta-free access to insert a trocar. Second, the placental territory of the donor is thickened and folded, which does not help to visualise the tiny anastomoses (Figure 14.5). Finally, a second surgery for post-laser TAPS is especially challenging as anastomoses were missed under the best surgical conditions. The first intervention may have caused membrane separation or blood-stained amniotic fluid, hampering a re-intervention.
Amnioinfusion of 1 to 2 litres warmed saline almost certainly improve the operative conditions. Most experts would draw a Solomon line between the vascular territories of both twins from one edge of the placenta to the other, which is usually sufficient to occlude all anastomoses, except when velamentous vessels skip the coagulation line to communicate across the membranes to the other placental territory. At present, laser coagulation is usually offered for stage 2 or above between 18 and 28 weeks, when we anticipate that complete separation is technically feasible.8
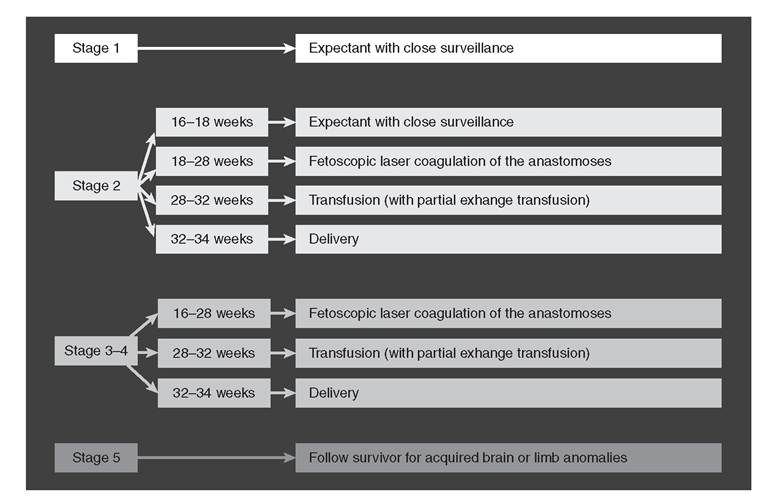
Figure 14.5 Flowchart for the proposed management according to stage and GA at presentation. These recommendations are only indicative, and obviously technicallimitations, Ginicalcharacteristics and patient preference need to be taken into account too. As such, before 28 weeks, an intrauterine transfusion with partial exchange transfusion may be the best option if fetoscopic laser surgery is not feasible.
Intrauterine Transfusion, Exchange Transfusion
Intrauterine transfusion of the donor with/without a partial exchange transfusion of the receptor does not cure the disease and is only a temporary solution to gain time to deliver the babies or to perform a fetal intervention. As such, intrauterine transfusion-exchange transfusion is the preferred treatment between 28 and 32 weeks for stage 3. A cordocentesis also confirms the TAPS diagnosis, and in experienced hands, it is a safe procedure. For severe TAPS in the early second trimester, an intra-peritoneal transfusion may be a safer alternative because an intravascular transfusion is technically challenging and associated with greater risks. Although each transfusion of the donor worsens the polycythaemia of the receptor, it is uncertain if a simultaneous partial exchange transfusion is of benefit. Here, the blood of the receptor is progressively replaced by saline to reduce the hyperviscosity.4 Usually, we start with partial exchange transfusions to the recipient, when we give a second or third intrauterine transfusion to the donor.
Selective Reduction
In the absence of an anomaly, the place of a selective reduction for TAPS is not well established. Like fetoscopic laser coagulation of the anastomoses, a selective reduction will undoubtedly arrest the inter-twin transfusion imbalance. However, especially the anaemic donor is at risk of dying, and theoretically, because of the minuscule anastomoses, the risk of acute exsanguination with subsequent demise or brain damage in the recipient should be
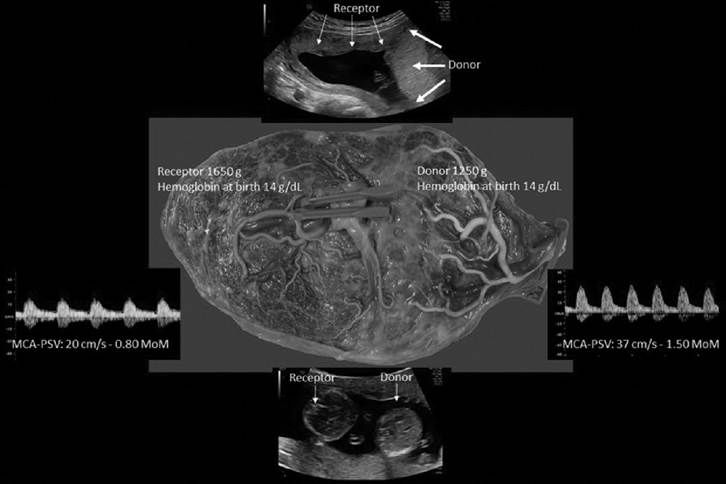
Figure 14.6 Ultrasound image of twin anemia-polycythemia at 15 weeks. The donor had the thick white part of the placenta, whereas the receptor had the thin, dark part. The receptor had a starry sky aspect of the liver. The pregnancy was managed expectantly. The MCA-PSV discordance improved spontaneously, and by 20 weeks, the MCA-PSVwasconcordant. Shedelivered at 31 weeks after spontaneous rupture of the membranes. The placenta did not show any anastomoses, as if we had performed a laser coagulation of allthe anastomoses. (A black and white version of this figure willappear in some formats. For the colour version, please refer to the plate section.)
small. Therefore, if the donor is hydropic in the early second trimester, expectant management may avoid the iatrogenic risks of a probably unnecessary selective reduction.
Elective Birth
At 32 weeks, we usually deliver for stage 3 TAPS or above.14 For the milder TAPS cases, the time of birth depends on the rate of progression and clinical characteristics, but after 34 to 35 weeks, there seems no benefit of delaying birth. Since the risk of an acute intra-partum transfusion is low, we allow a vaginal birth for cases with stage 1 or 2, especially if patients already had a vaginal birth and fetal well-being is acceptable.
Key Points
• Twin anaemia-polycythaemia sequence is characterised by a severe inter-twin haemoglobin discordance.
• Twin anaemia-polycythaemia sequence is caused by a chronic transfer of blood through minuscule anastomoses.
• Twin anaemia-polycythaemia sequence is diagnosed before birth by a discrepancy in MCA-PSV.
• Usually, additional ultrasound features are present, such as a discordance in placental echogenicity.
• Spontaneous TAPS is rare and occurs in about 3% of previously uncomplicated monochorionic twin pairs.
• Post-laser TAPS may occur after fetoscopic laser surgery for TTTS if small anastomoses are missed.
• Twin anaemia-polycythaemia sequence may lead to fetal and neonatal demise and longterm impairment.
• Fetoscopic laser coagulation of the minuscule anastomoses or intrauterine transfusion with partial exchange transfusion may improve the outcome and prolong the pregnancy.
• We should screen monochorionic twin pregnancies for the occurrence of TAPS by measuring the MCA-PSV in both twins.
References
1. Lewi L, Jani J, Cannie M et al. Intertwin anastomoses in monochorionic placentas after fetoscopic laser coagulation for twin-to-twin transfusion syndrome: is there more than meets the eye? Am J Obstet Gynecol 2006;194(3):790-5.
2. Lopriore E, Middeldorp JM, Oepkes D, Kanhai HH, Walther FJ, Vandenbussche FP. Twin anemia-polycythemia sequence in two monochorionic twin pairs without oligopolyhydramnios sequence. Placenta 2007;28 (1):47-51.
3. Khalil A, Gordijn S, Ganzevoort W et al. Consensus diagnostic criteria and monitoring of twin anemia polycythemia sequence: a Delphi procedure. Ultrasound Obstet Gynecol 2019.
4. Tollenaar LSA, Lopriore E, Middeldorp JM et al. Prevalence of placental dichotomy, fetal cardiomegaly and starry-sky liver in twin anemia polycythemia sequence. Ultrasound Obstet Gynecol 2019.
5. Couck I, Ponnet S, Deprest J, Devlieger R, De Catte L, Lewi L. Outcome of selective intrauterine growth restriction in monochorionic twin pregnancies at 16, 20 or 30 weeks according to the new consensus definition. Ultrasound Obstet Gynecol 2020.
6. Slaghekke F, Lopriore E, Lewi L et al. Fetoscopic laser coagulation of the vascular equator versus selective coagulation for twin-to-twin transfusion syndrome: an open-label randomised controlled trial.
Lancet 2014;383(9935):2144-51.
7. Couck I, Valenzuela I, Russo F, Lewi L. Spontaneous regression of twin anemiapolycythemia sequence presenting in the first trimester. Ultrasound Obstet Gynecol 2019.
8. Tollenaar LS, Slaghekke F, Middeldorp JM et al. Twin anemia polycythemia sequence:
current views on pathogenesis, diagnostic criteria, perinatal management, and outcome. Twin Res Hum Genet 2016; 19 (3):222-33.
9. Slaghekke F, Favre R, Peeters SH et al. Laser surgery as a management option for twin anemia-polycythemia sequence. Ultrasound Obstet Gynecol 2014;44 (3):304-10.
10. Tollenaar LSA, Lopriore E, Slaghekke F et al. High risk of long-term neurodevelopmental impairment in donor twins with spontaneous twin anemiapolycythemia sequence. Ultrasound Obstet Gynecol 2020;55(1):39-46.
11. Khalil A, Rodgers M, Baschat A et al. ISUOG practice guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol 2016;47(2):247-63.
12. NICE guideline [NG137]: twin and triplet pregnancy 2019. Available from www.nice.org.uk/guidance/ng137
13. Donepudi R, Papanna R, Snowise S, Johnson A, Bebbington M, Moise KJ, Jr. Does anemia-polycythemia complicating twintwin transfusion syndrome affect outcome after fetoscopic laser surgery? Ultrasound Obstet Gynecol 2016;47(3):340-4.
14. Tollenaar LSA, Zhao DP, Middeldorp JM, Oepkes D, Slaghekke F, Lopriore E. Can color difference on the maternal side of the placenta distinguish between acute peripartum twin-twin transfusion syndrome and twin anemiapolycythemia sequence? Placenta 2017;57:189-93.
15. Couck I, Lewi L. The placenta in twin-to- twin transfusion syndrome and twin anemia polycythemia sequence. Twin Res Hum Genet 2016;19(3):184-90.