Disorders with increased incidence during pregnancy
Vascular disease
Ischaemic stroke
The incidence of cerebral ischaemia associated with pregnancy is about 25-34:100,000 deliveries, peaking in the third trimester and puerperium.
Its aetiology can be subdivided into thrombotic, embolic (arterio-arterial or cardiac), and haemodynamic. Generally, atherosclerosis is the most common source of cerebral ischaemia. However, rare causes of stroke (e.g. arterial dissection and vasculitis) tend to be more prevalent in a young population. A recent study identified maternal smoking as an independent risk factor for perinatal arterial ischaemic stroke (73). Furthermore, pregnancy predisposes to ischaemia secondary to hypercoagulability (such as cerebral venous thrombosis). Some strokes occur due to conditions exclusively seen in the pregnant (i.e. eclampsia, peripartum cardiomyopathy, and amniotic fluid embolism). Other predisposing conditions include the commonly recognized cerebrovascular risk factors, particularly arterial hypertension (74).Signs and symptoms of cerebral ischaemia depend on the site of the lesion. Common signs of supratentorial infarction include hemiparesis, aphasia, hemianopsia, and hemineglect. Dizziness, ataxia, diplopia, dysarthria, and central facial palsy may herald brainstem/cerebellar ischaemia. An altered level of consciousness—particularly if associated with other brainstem symptoms or bilateral Babinski signs—should prompt immediate investigations for basilar thrombosis.
Diagnosis of ischaemic cerebral infarction is based on radiographic findings. MRI is the method of choice as it does not involve ionizing radiation, is more sensitive for small infarctions and ischaemia in the posterior fossa, and may contribute to determining the exact onset and aetiology of the stroke (e.g. by showing multiple foci in embolic infarction). The time-of-flight technique permits magnetic resonance angiography without the use of contrast agent.
If CT is the only imaging technique available, radiation dose-r eduction methods and proper shielding protection ought to be used (75). Ultrasonography provides additional haemodynamic and structural information of the intra- and extracranial vessels.All patients diagnosed with acute cerebral ischaemia should be monitored on a specialized stroke unit. Further aetiological workup includes a transthoracic echocardiogram, which may be combined with a bubble study to evaluate for a right-to-left shunt (e.g. patent foramen ovale). A transoesophageal echocardiogram may be considered, particularly if conditions requiring specific treatment—such as infective endocarditis or intracardiac thrombi—are suspected. A 24-hour electrocardiogram recording should be performed to exclude relevant cardiac arrhythmias such as atrial fibrillations.
Laboratory tests include a thrombophilia workup. The genetic panels are not influenced by pregnancy. However, the other parameters (e.g. antiphospholipid antibodies) are frequently falsely positive and may have to be postponed until several weeks postpartum (74).
After screening for contraindications, intravenous recombinant tissue plasminogen activator (rtPA; 0.9 mg/kg, maximum dose 90 mg) may be used in patients presenting within a time frame of up to 4.5 hours after onset of symptoms (and in select patients with salvageable tissue as determined by cerebral imaging). In patients with mild
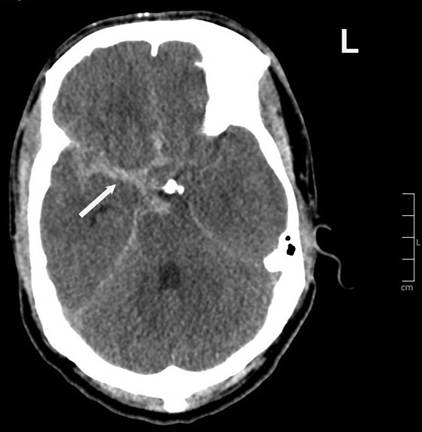
Figure 24.1 Subarachnoid haemorrhage (SAH, arrow) of Hunt and Hess grade III due to rupture of an aneurysm arising from the right middle cerebral artery bifurcation. Courtesy of Dept. of Neuroradiology, Kepler University Hospital, Linz, Austria.
deficits, risks of thrombolytic treatment have to be weighed against anticipated impairments (76). There are no randomized trials on the use of rtPA in pregnancy and experience is limited to case reports (77), but rtPA is not known to be teratogenic and it is too large a molecule to cross the placenta (78).
The decision pro or contra thrombolysis has to be made after individualized appraisal of the case. The indication for endovascular intervention (intra-arterial thrombolysis or mechanical thrombectomy) is subject to interdisciplinary discussion between the stroke specialist and an interventional neuroradiologist (79).Recurrence rates of cerebral ischaemia during subsequent pregnancies depend on the aetiology of the stroke but generally seem to be low (80). For pregnant women with high-risk conditions that would require anticoagulation outside of pregnancy—such as mechanical heart valves—the use of unfractionated heparin or low- molecular-weight heparin (LMWH) is recommended (81). LMWH compares more favourably regarding the risk of obstetric bleeding complications, osteoporosis, and heparin-induced thrombocytopenia (82). Doses should be normalized for body weight changes, and anti- Xa activity ought to be monitored (83). LMWH may be discontinued 24 hours or more before a planned delivery (81). Vitamin K antagonists are better avoided due to the risk of embryopathy and fetal bleeding. Data on direct oral anticoagulants regarding their safety during pregnancy are hitherto insufficient; these agents should therefore not be used in the pregnant (84).
In situations in which antiplatelet therapy would be recommended outside of pregnancy, low-dose aspirin (50-150 mg/day) can safely be used after the first trimester (81, 85). There is no clear consensus on the use of aspirin in the first trimester: a meta-analysis found no evidence of an overall increase of congenital malformations, but showed a possible association with an increased risk of gastroschisis (65). Given the paucity of data concerning the risk-benefit ratio of secondary prevention of non-cardioembolic stroke during the first trimester, the American Heart Association/American Stroke Association guidelines consider low-dose aspirin, unfractionated heparin/ LMWH, or no treatment acceptable treatment options (81).
There are no adequate data on other antiplatelet agents (clopidogrel, dipyridamole) regarding their safety in pregnancy.Cerebral haemorrhage
Haemorrhagic stroke includes intracerebral parenchymal and subarachnoid haemorrhage (Figure 24.1). At 4-6 per 100,000 deliveries, the incidence of haemorrhagic stroke seems to be higher in the pregnant or postpartum population than in age-matched, nonpregnant women (relative risk of 2.5/28.5 during pregnancy/post- partum period) (86).
The major causes of intracranial haemorrhage in pregnancy are ruptured aneurysms, arteriovenous malformations (Figure 24.2), and (pre-)eclampsia. Other risk factors include advanced maternal
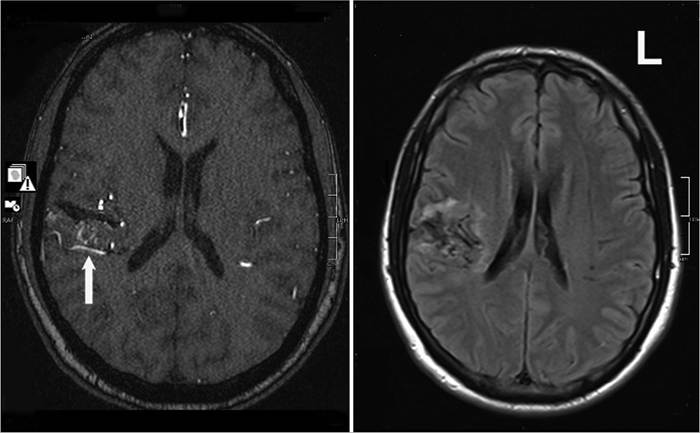
Figure 24.2 Right temporoinsular arteriovenous malformation (AVM). Time-of-flight magnetic resonance angiography (left) shows the AVM, which is fed by temporal branches of the middle cerebral artery and drains via a prominent cortical vein (arrow). Fluid attenuation inversion recovery (FLAIR) imaging (right) shows mild residual oedema and haemosiderin deposits suggesting prior haemorrhage of the AVM. Courtesy of Dept. of Neuroradiology, Kepler University Hospital, Linz, Austria
age, African American race, hypertension, coagulopathy, and tobacco abuse (87, 88).
Signs and symptoms comprise focal neurological deficits corresponding to the site of the lesion, altered state of consciousness, headache (which is typically sudden and severe in subarachnoid haemorrhage), nausea and vomiting, and signs of meningeal irritation such as nuchal rigidity.
Neuroimaging is the most important diagnostic procedure in suspected haemorrhagic stroke. During pregnancy, MRI is preferred over CT. As both methods may yield a small rate of false-negative results, lumbar puncture ought to be considered in patients in whom there is a high suspicion of subarachnoid haemorrhage (89). If further therapeutic planning requires a cerebral angiogram, proper shielding protection of the fetus should be applied (90).
Treatment of intracerebral haemorrhage comprises supportive care (cardiovascular and neurological monitoring, correction of coagulopathies, treatment of intracranial hypertension), symptomatic measures (e.g. treatment of headache, nausea, and epileptic seizures), and possibly elimination of the source of the bleeding. The latter should be subject to careful risk-benefit evaluation in the individual patient (90, 91). The risk of intracranial aneurysm rupture peaks in the third trimester. This situation is associated with a high maternal and fetal mortality, which increases further in the case of a rebleed (no current figures available; in an older study maternal/fetal mortality due to recurrent subarachnoid haemorrhage amounted to 63%∕27%, respectively (92)). Thus, symptomatic aneurysms should be controlled by endovascular or surgical means (90).
Data concerning the risk of bleeding from a previously asymptomatic arteriovenous malformation during pregnancy are inconclusive. However, early intervention should be considered once an arteriovenous malformation has ruptured (90, 93).
If the vascular pathology has been treated, the woman may undergo vaginal delivery. Controversy continues whether or not to recommend caesarean section in patients with untreated aneurysms and arteriovenous malformations (94, 95).
Venous sinus thrombosis
Cerebral venous thrombosis (CVT) (Figure 24.3) affects the dural sinuses and/or cerebral veins. It represents approximately 0.5-1% of all strokes, affecting 5 people/million/year (96, 97). The incidence of CVT in pregnancy increases to about 8-12:100,000 deliveries, accounting for approximately one-third of pregnancy-associated strokes (98, 99). Peak incidence is in the third trimester and postpartum.
CVT can be subclassified into septic and aseptic thrombosis. The former is caused by local inflammation such as sinusitis, otitis, facial and dental infections, and dental infections. The latter is associated with hypercoagulable states.
These include inherited abnormalities of coagulation and acquired conditions, among them pregnancy and puerperium.Signs and symptoms result from either one of two mechanisms: increased intracranial pressure due to impaired venous drainage and focal brain injury secondary to venous infarctions and/or haemorrhage (100). Headache is the most common presentation, reported by 90% of patients with CVT (101). In approximately 25% of patients it is the only presenting symptom (96). Other signs include visual disturbances, focal neurological deficits (most commonly hemiparesis (102)), and epileptic seizures. Bilateral brain involvement is a
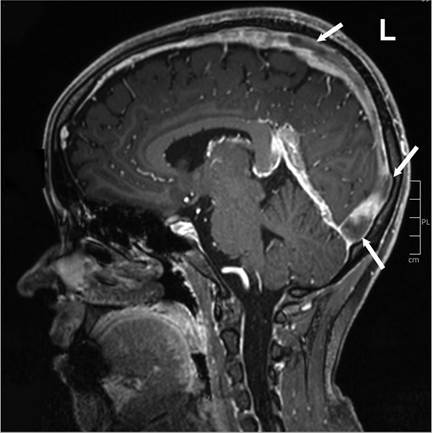
Figure 24.3 Cerebral venous thrombosis (CVT). Contrast-enhanced T1-imaging shows extensive CVT of the superior sagittal sinus (arrows). Courtesy of Dept. of Neuroradiology, Kepler University Hospital, Linz, Austria
distinguishing feature of CVT: reduced consciousness, for example, may be due to bilateral thalamic injury secondary to impairment of the deep venous drainage system (96).
All patients with suspected CVT should be screened for predisposing factors such as hypercoagulable states, infections or inflammatory processes. D-dimer assays have a high negative predictive value (99.6%) (103). However, with a strong clinical suspicion of CVT, a normal level should not preclude further diagnostic evaluation. In pregnant women, D-dimer levels are frequently elevated, particularly in the third trimester. Therefore, the specificity and positive predictive value of elevated D-dimer levels decrease during pregnancy.
MRI with magnetic resonance venography is considered the gold standard in diagnosing CVT (104). The time-of-flight technique permits magnetic resonance venography without the use of contrast agent. Despite the theoretical risks for the fetus, pregnant patients can undergo MRI at any stage of pregnancy if justified after careful risk-benefit considerations (105).
Patients with CVT should be monitored on a stroke unit for early diagnosis and management of complications such as seizures, hydrocephalus, cerebral haemorrhage, and intracranial hypertension. In septic CVT, the infectious focus needs to be eradicated. Once the diagnosis of CVT is made, anticoagulation (unfractionated heparin adjusted to achieve an activated partial thromboplastin time twice the pretreatment value or body-weight adapted LMWH) should be started to prevent thrombus growth. This also applies to patients presenting with secondary intracerebral haemorrhage (106). Preliminary data suggest that LMWH may be more effective than unfractionated heparin (107). In individual cases, endovascular interventions may be considered if there is clinical deterioration due to incomplete sinus recanalization. However, no controlled studies exist to support this approach (96).
Anticoagulation should be continued for 3-6 months in patients with provoked CVT and for 6-12 months in unprovoked CVT. For women with pregnancy-associated CVT, the American Heart AssociationZAmerican Stroke Association recommend LMWH treatment throughout the remaining pregnancy and LMWH or vitamin K antagonists for at least 6 weeks postpartum, aiming at a total minimum duration of therapy of 6 months. In patients with recurrent CVT or high-risk thrombophilia, indefinite anticoagulation may be considered (96).
In the largest study available on the prognosis of CVT, the outcome was favourable (modified Rankin Scale 0-2) in 86.6% of patients (101). Pregnancy-related CVT is associated with a low risk of recurrence (101, 108), but prophylaxis with LMWH may be considered during subsequent pregnancies (96).
Reversible cerebral vasoconstriction syndrome and posterior reversible encephalopathy syndrome
Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by hyperacute severe headaches and segmental dynamic vasoconstriction (109). Different trigger factors have been identified, particularly the use of vasoactive drugs and the postpartum state (110). The typical onset of RCVS is at 1-3 weeks postpartum. It may be associated with (pre-)eclampsia (111).
The hallmark symptom of RCVS is a thunderclap headache defined as severe, with throbbing cephalalgia reaching peak intensity within 60 seconds of onset. It is the sole symptom in about 70% of patients and typically shows a waxing and waning course (110). Other variably associated symptoms include nausea, vomiting, photo- and phonophobia, seizures, and focal neurological deficits. The latter are usually transient but may persist if an ischaemic stroke ensues.
Diagnosis of RCVS rests on visualization of the typical ‘string-of- beads' appearance of one or more intracranial vessels caused by segmental narrowing and dilatation. The vasoconstriction is dynamic and early angiographies may be normal (112).
Differential diagnoses comprise aneurysmal subarachnoid haemorrhage, primary angiitis of the central nervous system, sinus venous thrombosis, pituitary apoplexy, cervical artery dissection, and other primary and secondary headache syndromes. Brain scans in RCVS patients are usually normal but may show sequelae of vascular dysregulation such as cerebral infarction, and intracerebral, subarachnoid, or subdural haemorrhage. Vasoconstriction may be monitored by transcranial ultrasonography. Lumbar puncture should be performed to exclude aneurysmal subarachnoid haemorrhage (109).
Management of the RCVS patient is based on symptomatic treatment and elimination of precipitating factors. Vasodilating medication (nimodipine/verapamil, magnesium sulphate) have been used to relieve vasoconstriction. However, use of these agents is mostly based on anecdotal data and a positive effect on the evolution of the disease has not been convincingly demonstrated so far (109). The same is true for intra-arterial administration of vasodilators and balloon angioplasty (110).
RCVS is usually self-limiting. However, if associated with the postpartum period, it seems to carry a higher risk of permanent deficits or death: only 50% of patients went on to full recovery in one small study (111).
Posterior reversible encephalopathy syndrome (PRES) is characterized by a heterogeneity of neurological symptoms associated with (sub-)cortical vasogenic oedema. PRES (Figure 24.4) has been related to endothelial dysfunction caused by abrupt blood pressure changes or cytokine effects (113). It may be precipitated by a variety
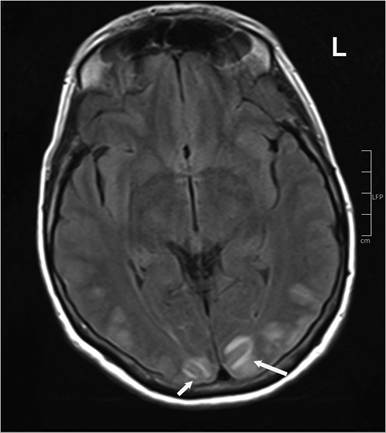
Figure 24.4 Posterior reversible encephalopathy syndrome (PRES). Fluid attenuation inversion recovery (FLAIR) sequences demonstrate confluent temporoparietal signal alterations (arrows) compatible with (sub-)cortical vasogenic oedema. Courtesy of Dept. of Neuroradiology, Kepler University Hospital, Linz, Austria
of factors, such as hypertension, autoimmune disorders, immunosuppression, and (pre-)eclampsia.
PRES is characterized by a (sub-)acute onset of encephalopathic changes, seizures, and visual disturbances. These symptoms are typically accompanied by a dull headache. Focal findings occur in 5-15% of patients (113). PRES is frequently associated with RCVS (109).
Diagnosis is based on the clinical findings and MRI. T2-weighted sequences reveal subcortical—and sometimes cortical—vasogenic oedema, which is usually bilateral, asymmetric, and located in the parieto-occipital regions. However, other cerebral regions may be involved (114).
Management of PRES is symptomatic (e.g. antiepileptic) and by treatment of the causative factor (e.g. hypertension). Its prognosis is usually favourable (113).
Peripheral nervous system disorders
Peripheral nerve compression syndromes
Carpal tunnel syndrome is one of the most frequent peripheral nerve compression syndromes in pregnancy, with a peak incidence in the third trimester. Its occurrence has been associated with increased fluid retention in pregnant women (115). Carpal tunnel syndrome is diagnosed clinically by demonstrating compromised median nerve function. The diagnosis is supported by nerve conduction studies. Patients may benefit from wearing a wrist splint at night. Corticosteroid injections or surgery to release the flexor retinaculum are rarely indicated during pregnancy due to the favourable prognosis of pregnancy-related carpal tunnel syndrome. Symptoms tend to resolve during the weeks and months after delivery, but may recur in subsequent pregnancies (116).
Postpartum compression neuropathies tend to affect the femoral, lateral femoral, cutaneous, and obturator nerves. They are associated with variables related to the fetus (e.g. macrosomia) or to the process of delivery (e.g. prolonged lithotomy position and compression by leg stirrups). The prognosis for recovery is excellent (117). If there is already a history of peripheral nerve compression syndromes or evidence of multiple nerves involved, hereditary neuropathy with liability to pressure palsies should be excluded, a rare genetic neuropathy with a good prognosis (118).
Lumbago and lumbosacral radiculopathies
Lumbago is frequently encountered in pregnant women and is mostly due to local mechanical factors. Disc bulges or prolapses seem to be no more frequent in pregnant than in non-pregnant women (119).
Symptoms of nerve root compression include radiating pain, loss of sensibility, muscular paresis, and bladder/bowel dysfunction. The most commonly affected levels are at L4/L5 and L5/S1.
Physical examination should evaluate for focal neurological deficits. Imaging studies will not be required in the majority of patients but lumbar MRI should be performed in the presence of severe or progressive neurological deficits or when a serious underlying condition is suspected (120).
Conservative management will suffice in most patients. If an analgesic is needed, acetaminophen has one of the best safety profiles in pregnancy (121). Indications for disc surgery during pregnancy are incapacitating pain, severe or progressive neurological deficits, and bladder or bowel dysfunction (122).
Cranial nerve syndromes: Bell's palsy
Bell’s palsy denotes idiopathic peripheral paralysis of the facial nerve. Its incidence seems to be increased during pregnancy (although data are not entirely conclusive), particularly in the third trimester and the postpartum period (123).
The diagnosis is based upon the clinical findings. Electrodiagnostic studies can provide prognostic information. MRI or lumbar puncture may be warranted to exclude symptomatic paralysis, particularly in areas endemic for Lyme disease.
Treatment of idiopathic Bell’s palsy is steroid based (e.g. prednisone 60-80 mg/day for 1 week). Use during the first trimester of pregnancy may be associated with an increased incidence of cleft palate (123, 124). Careful eye care should be performed in the case of incomplete lid closure.
Restless legs syndrome
Restless legs syndrome (RLS) is characterized by an unpleasant sensation in the legs relieved by movement. Symptoms are worse at rest and in the evening/during the night. Its prevalence during pregnancy is approximately two to three times higher than in nonpregnant females (highest in the third trimester and in multiparous women).
Primary and secondary RLS are distinguished. The latter may be due to iron-deficiency, peripheral neuropathy, or renal disease. Endocrine and metabolic changes have been attributed to pregnancy-related RLS (125).
RLS is a clinical diagnosis based upon the criteria proposed by the International RLS Study Group (126). Secondary RLS should be excluded by appropriate laboratory investigations.
Mild forms of RLS may be treated non-pharmacologically (127). Drugs known to aggravate RLS (e.g. neuroleptics) should be withdrawn. Iron supplementation is to be used in iron-deficient patients. In refractory RLS, low-dose carbidopa-levodopa or clonazepam have been recommended (128). There is little data on fetal safety for alternative agents (dopamine agonists, opioids, benzodiazepines, anticonvulsants).
Symptoms of RLS disappear or markedly improve within days after delivery in the majority of women (125). However, patients with pregnancy-related RLS are at an increased risk of developing chronic RLS in the future (129).