29 Ectopic Pregnancy
Virginia Mensah
Melissa Yates
An ectopic pregnancy (EP) occurs when a fertilized ovum implants outside of the uterine cavity.
EPIDEMIOLOGY OF ECTOPIC PREGNANCY
• Two percent of all first-trimester pregnancies and 6% of all pregnancy-related deaths
• EP is the leading cause of death in the first trimester.
• At least one third of pregnancies that occur after tubal sterilization procedures are EPs.
• Women who use an intrauterine device (IUD) have an overall decreased risk of both intrauterine and extrauterine pregnancies. However, when pregnancy does occur, risk of EP is higher than in women not using an IUD.
• In assisted reproductive technology (ART), the incidence of EP is approximately 3% to 5%. These pregnancies tend to be recognized at an earlier stage due to close monitoring in these patients.
• Ninety-seven percent of ectopic pregnancies are implanted within the fallopian tube, although implantation can occur within the abdomen, cervix, ovary, or uterine cornua. Other rare locations for implantation include previous hysterotomy scars and the rudimentary horn of a uterus. EPs also occur following hysterectomy.
• Risk factors for EP include pelvic inflammatory disease, previous tubal surgery, infertility, current or previous use of an IUD, two or more pregnancy termination procedures, diethylstilbestrol exposure, age >40 years, smoking, greater than three previous spontaneous abortions, and assisted reproduction.
• Risk factors for recurrent EP include previous EP (even if previous EP was treated by salpingectomy), previous spontaneous miscarriage (with likelihood increasing with each miscarriage), and a history of pelvic surgery. No significant increase exists in women with a history of pelvic infections when these patients are compared to those with a primary presentation of EP.
• Etiology of EPs is often multifactorial, and an estimated 40% to 50% of EPs have an unknown etiology.
DIAGNOSIS OF ECTOPIC PREGNANCY
Clinical Presentation
• The Classic triad (present in less than 50% of patients) is amenorrhea followed by abnormal vaginal bleeding and abdominal or pelvic pain.
• Pain is present in 95% of patients with rupturing EP. It is usually located in the lower quadrants but can be anywhere within the abdomen. Cervical motion tenderness (CMT) is present in 75% of patients with ruptured EP.
• Vaginal spotting is present in 60% to 80% of patients and is usually scant, dark brown bleeding, either intermittent or continuous.
• EP may present as a surgical emergency, and timely diagnosis is essential (Fig. 29-1).
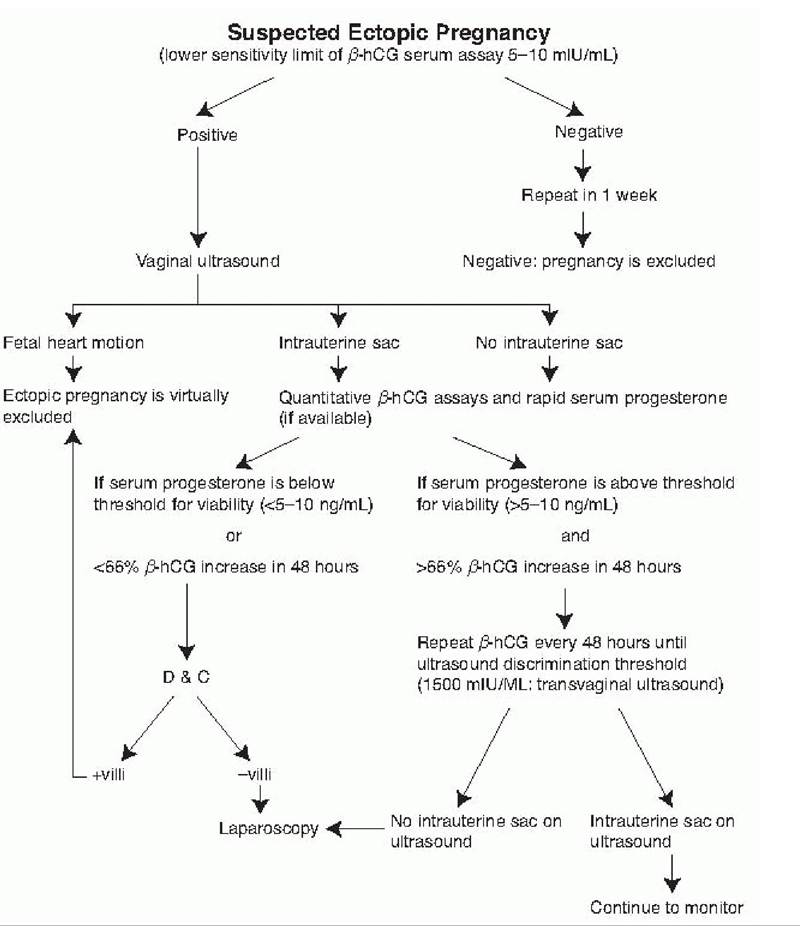
Figure 29-1. Evaluation of the stable patient with suspected EP. Hormonal parameters can vary depending on the assay technique and reference standard used. The discriminatory threshold for sonographic detection of an intrauterine gestational sac is established by each institution. (Reused with permission from Damario MA, Rock JA. Ectopic pregnancy. In Rock JA, Jones HW III, eds. TeLindeS Operative Gynecology, 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:516.)
Differential Diagnosis
• Salpingitis presents with similar signs and symptoms as EP, but negative pregnancy test results, and an elevated white blood cell (WBC) and temperature.
• Threatened abortion: In this condition, bleeding is usually heavier, pain is localized to the lower mid abdomen, and CMT is generally absent.
P.381
• Appendicitis: Persistent right lower quadrant pain, with fever and gastrointestinal (GI) symptoms, suggests appendicitis. CMT, if present, is usually less severe than with EP. Pregnancy test results are negative, and amenorrhea or abnormal vaginal bleeding is usually absent.
• Ovarian torsion: Pain is initially intermittent and later becomes constant as vascular supply is compromised. Findings may include an elevated WBC and a palpable adnexal mass, but pregnancy test
results are negative.
• Other conditions in the differential should include normal intrauterine pregnancy, heterotopic pregnancy (especially in the case of ART), ruptured ovarian cyst, bleeding corpus luteum, endometriosis, diverticulitis, and dysfunctional uterine bleeding. Gastroenteritis, urinary tract infection, or renal calculus early in pregnancy may also mimic an EP.
Physical Examination
• Ruptured unstable EP is a surgical emergency. If unstable, patients may have signs of hypovolemic shock, including tachycardia, hypotension, and confusion. Abdominal exam may reveal peritonitis, including guarding, rigidity, or rebound tenderness. Up to 15% of women complain of shoulder pain, secondary to diaphragmatic irritation from hemoperitoneum.
• Hemodynamically stable EP: Tenderness in patients with EP may be generalized (45%), located bilaterally in the lower quadrants (25%), or located unilaterally in a lower quadrant (30%). Rebound tenderness may or may not be present. CMT, resulting from peritoneal irritation, is usually present but is not specific for EP. A palpable adnexal mass or mass in the cul-de-sac is reported in approximately 40% of cases; absence of a palpable mass does not rule out EP.
Laboratory Evaluation
• If EP is diagnosed before rupture, a laboratory diagnosis may be made and conservative treatment offered.
Quantitative Gonadotropin Levels
• Quantitative beta-human chorionic gonadotropin (β-hCG): The titer climbs in a linear fashion from 2 to 4 weeks after ovulation in normal pregnancy, frequently doubling every 48 to 72 hours until it reaches 10,000 mIU/mL.
• Minimum rise in β-hCG for a viable intrauterine pregnancy (IUP) is typically 53% in 48 hours. Thus, β-hCG that increases less than 50% in 48 hours is almost always associated with an abnormal pregnancy. Serial serum hCG values that increase or decrease more slowly than expected when compared to viable IUPs or spontaneous abortions, respectively, are suggestive of EP; however, the entire clinical picture must be considered.
• Levels of β-hCG are more likely to plateau (is suggested by visualization of both an ectopic and an IUP or the presence of echogenic fluid in the cul-de-sac in the presence of an IUP. Surgery (e.g., salpingostomy or salpingectomy) is the standard treatment of heterotopic pregnancy with a tubal component because the IUP is a contraindication to medical therapy.
• Sensitivity of TVUS in the diagnosis of EP ranges from 70% to 90%. Despite relative accuracy in detection of EPs, there remain some cases where results of TVUS are inconclusive regarding location of pregnancy in the setting of a positive pregnancy test. These are deemed pregnancy of unknown location (PUL). An EP is eventually diagnosed in 7% to 20% of women with PUL. It is important to note that PUL is a classification scheme and not a final diagnosis.
• PUL is a term provided by a classification scheme which was designed to “improve objective comparison of research outcomes in the diagnosis of EP and to reduce clinical heterogeneity.” Using this scheme, there are five classifications depending on sonographic findings: definite EP, probable EP, PUL, probable IUP, and definite IUP.
• For women with PUL, final outcome is classified as visualized EP, visualized IUP, spontaneously resolved PUL, and persisting PUL. In the category of persisting
P.383 PUL, further final outcomes are classified as nonvisualized EP, treated persistent PUL, resolved persistent
PUL, or histologic IUP.
• Radiologic signs of EP include an empty uterus, cystic or solid adnexal masses, dilated and thick-walled fallopian tubes, free echogenic fluid in pelvis, hematosalpinx, extrauterine gestational sac that contains a yolk sac (with or without an embryo), and increased blood flow to the adnexa which contains the EP (using Doppler technology).
• Pseudosac: Ten percent of ectopic pregnancies have a pseudosac in the uterus that lacks the “double decidual” sign of an IUP. A pseudosac tends to be oval in shape with irregular margins in contrast to the smooth margins of an IUP.
It also tends to appear centrally in the intrauterine cavity.• An EP greater than 2 cm in size can be visualized with TVUS.
• Adnexal cardiac activity may be seen when the β-hCG titer is greater than 15,000 mIU/mL.
Diagnosis by Pathology: Dilation and Curettage
• When β-hCG concentration is above 1,500 to 2,000 mIU/mL and TVUS fails to confirm an IUP, dilation and curettage (D&C) should be considered to distinguish between an abnormal IUP and an EP.
• In a recent study of patients with a β-hCG level above 2,000 mIU/mL and no visible IUP on ultrasound, 45.7% had an EP as compared with 54.3% who had a spontaneous abortion. Of the patients with a β-hCG level below 2,000 mIU/mL with similar findings, 68.8% had an EP, whereas 31.2% had a spontaneous abortion.
• Women with abnormally rising or plateauing β-hCG 4 cm on TVUS
Embryonic cardiac activity on TVUS
Patient declines blood transfusion
Patient is unable to follow-up
High initial hCG (>5,000)
MTX, methotrexate; IUP, intrauterine pregnancy; TVUS, transvaginal ultrasound; hCG, human chorionic gonadotropin.
aAdapted from American College of Obstetricians and Gynecologists. Medical management of ectopic pregnancy. ACOG practice bulletin no. 94. Obstet Gynecol 2008;111:1479-1485.
bFrom Practice Committee of the American Society for Reproductive Medicine. Medical treatment of ectopic pregnancy. Fertil Steril 2006;86(5)(suppl 1):S96-S102.
• MTX dosing regimens
• Single-dose versus multidose treatment: Treatment protocols that involve single or multiple injections of MTX have been developed (Table 29-3). Benefits of a single dose include decreased cost, better side effect profile, improved patient compliance, and no need for leucovorin rescue treatment. The benefit of the multidose regimen is a lower failure rate. A systematic review reported a failure
P.386 rate of 14.3% or higher with single-dose MTX when pretreatment β-hCG levels are higher than 5,000 mIU/mL, compared with a 3.7% failure rate for hCG levels less than 5,000 mIU/mL.
If hCG levels are higher than 5,000 mIU/mL, the twodose regimen may be appropriate while avoiding the need for leucovorin rescue and improving patient compliance.TABLE 29-3 Methotrexate Treatment Protocols for Ectopic Pregnancy
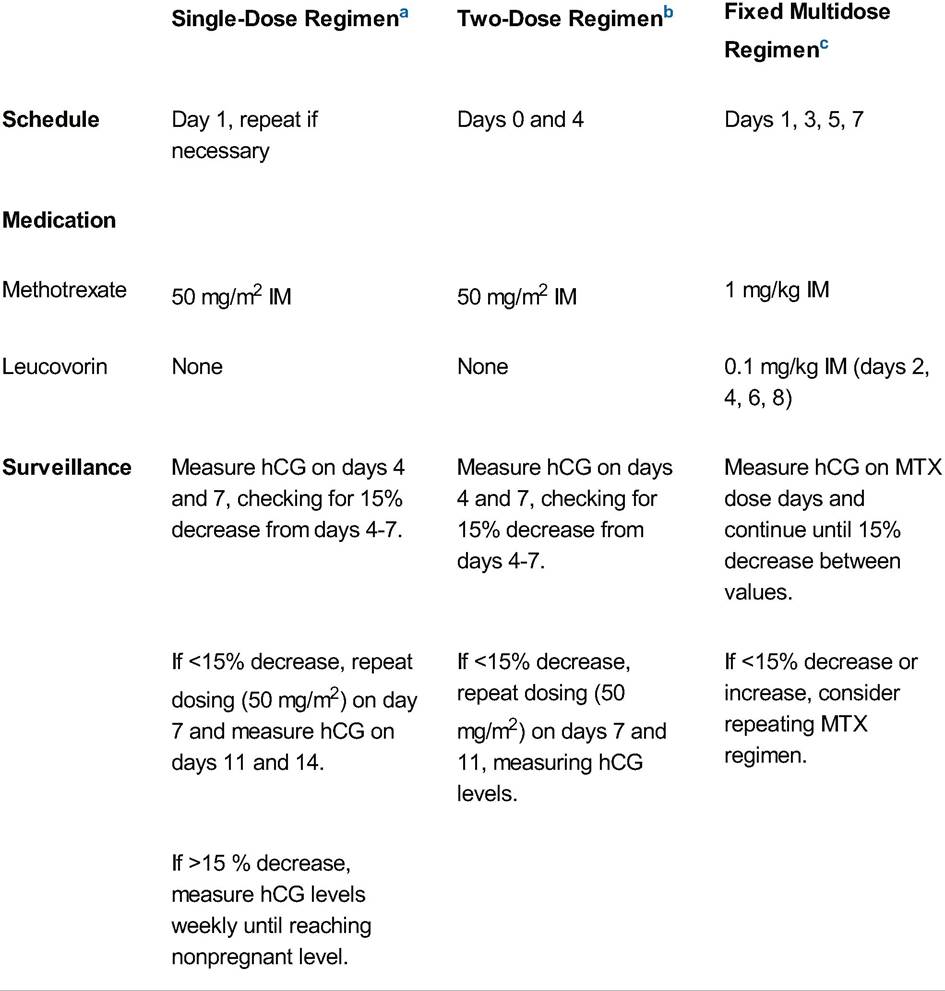
IM, intramuscular; hCG, human chorionic gonadotropin; MTX, methotrexate.
aFrom Stovall TG, Ling FW. Single-dose methotrexate: an expanded clinical trial. Am J Obstet Gynecol 1993;168:1759-1762.
bFrom Barnhart K, Hummel AC, Sammel MD, et al. Use of “2-dose” regimen to treat ectopic pregnancy. Fertil Steril 2007;87:250.
cFrom Rodi IA, Sauer MV, Gorril MJ, et al. The medical treatment of unruptured ectopic pregnancy with methotrexate and citrovorum rescue: preliminary experience. Fertil Steril 1986;46:811-813. Adapted from American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 94: medical management of ectopic pregnancy. Obstet Gynecol 2008;111:1479-1485.
• The overall success rate for MTX is 89%. The success rate of single-dose treatment is reported to be 88.1% versus 92.7% for the multidose regimen (p =.035).
P.387
• Patients with previous EPs are four times more likely to fail MTX treatment.
• Special indications for MTX treatment include known EP in difficult locations, such as cervical, ovarian, or cornual pregnancies in which the risk of surgical management outweighs the risk of attempted medical management.
• Treatment monitoring: Concentration of β-hCG often rises after the initial MTX injection. The level of β-hCG should drop by at least 15% from day 4 to day 7 following administration. TVUS is not an appropriate modality for determining treatment failure. Enlargement of the ectopic mass and/or free fluid in the pelvis are common findings after MTX injection and may prompt unnecessary interventions.
• Treatment failure is generally defined as a need for subsequent surgical intervention, although some studies use the term to describe the failure of a single MTX injection to lower β-hCG concentration by at least 15%.
Surgical Management
• Surgical management is the appropriate course of treatment in hemodynamically unstable patients or patients who have failed MTX therapy. Surgical management is also indicated in patients who have had a previous ectopic in the same fallopian tube.
• The surgical techniques should be tailored to the specific findings and situation, and they include salpingostomy, salpingectomy, partial salpingectomy, segmental resection, cornual resection, and possible hysterectomy for interstitial pregnancy.
• Salpingostomy is the preferred treatment for women who desire future fertility and have a compromised contralateral fallopian tube. A linear incision is made on the antimesenteric border over the pregnancy, which usually extrudes from the incision and is removed. Bleeding points are cauterized with laser or needlepoint cautery, and the incision is left to heal by secondary intention. EPs located in the ampulla are ideal candidates.
• Salpingectomy involves the removal of the entire tube on the affected side. Consideration must be given to tubal damage at the time of surgery, especially in the case of a second EP in the same tube. Candidates for salpingectomy include women who have failed salpingostomy, completed childbearing, and patients with uncontrolled bleeding.
• EP after tubal ligation is most often located in the fimbriated end of the tube. In this case, both fimbriae should be surgically removed and the proximal segments of the tube cauterized to prevent recurrent EP.
Laparoscopy
• Minimally invasive laparoscopy is the preferred surgical approach in the hemodynamically stable patient. It usually provides a definitive diagnosis, although early EPs are missed 4% to 8% of the time. Not all patients are ideal candidates (e.g., patients with large body habitus or previous abdominal surgeries). Surgical approaches include linear salpingostomy and salpingectomy.
• Contraindications to laparoscopy may include pelvic adhesions, hemoperitoneum, pregnancy >4 cm, and hemodynamic instability.
• Linear salpingostomy requires postoperative MTX in 15% of cases, often due to presence of persistent trophoblastic tissue. Serial β-hCG levels must be followed weekly.
• Tubal rupture is not an absolute indication for salpingectomy, especially if the rupture site is linear and small. The rupture site can be used to evacuate the pregnancy and preserve the tube.
• Salpingectomy is indicated when the tube continues to bleed after linear salpingostomy, when an EP occurs in a tube with previous damage, or when an EP occurs
P.388 in a tube with a previously identified hydrosalpinx in a patient who is currently undergoing IVF.
• Copious irrigation of the pelvis is indicated to prevent adhesions and trophoblastic implants.
Laparotomy
• Laparotomy is indicated for a patient with obvious hemorrhage and hemodynamic compromise. After hemostasis is obtained, the treatment of choice is complete or partial salpingectomy. With a ruptured interstitial or cornual pregnancy, cornual resection may be required. Laparotomy is also indicated when adhesive disease precludes adequate visualization through the laparoscope.
Complications of Surgical Management
• Persistent trophoblastic tissue and persistent EP are considered surgical failures. Levels of β-hCG should be followed weekly after salpingostomy, until nonpregnant levels are reached. Surgically managed EPs can be given a dose of MTX for eradication of persistent trophoblastic tissue if β-hCG levels are found to plateau, in lieu of reoperation.
FOLLOW-UP AND PROGNOSIS
• After one EP, approximately 60% of patients conceive spontaneously.
• The recurrence risk ranges from 10% to 27%, which is 5 to 10 times greater than the risk for EP in the general population. The risk of recurrence increases in patients who have had two or more EPs. Only one out of three will conceive, and 20% to 57% of these will have EPs.
• Subsequent tubal patency rates are similar (80% to 85%) for patients treated medically or with salpingostomy.
• Patients with badly damaged fallopian tubes and those whose tubes have been removed can conceive through IVF.
• Patients should be advised to use reliable contraceptive methods until initial inflammation resolves (6 to 12 weeks). Contraception will avoid confusion between rising β-hCG levels from a new pregnancy and those from a persistent EP if conception occurs in the immediate postoperative period.
• Patients should undergo extensive counseling regarding their risk for recurrent EP and the necessity for early medical attention for subsequent pregnancies. The latter includes serial determinations of β-hCG levels until an early ultrasound examination can document an IUP or EP.
• Postoperative RhoGAM must be given to an Rh-negative woman to prevent Rh alloimmunization in a future pregnancy.
SUGGESTED READINGS
Barnhart KT. Ectopic pregnancy. N Engl J Med 2009;361:379-387.
Barnhart KT, Gosman G, Ashby R, et al. The medical management of EP: a meta-analysis comparing “single-dose” and “multidose” regimens. Obstet Gynecol 2003;101:778-784.
Barnhart KT, Van Mello NM, Bourne T, et al. Pregnancy of unknown location: a consensus statement of nomenclature, definitions, and outcome. Fertil Steril 2011 ;95(3):857-866.
Bouyer J, Coste J, Shojaei T, et al. Risk factors for EP: a comprehensive analysis based on a large casecontrol, population-based study in France. Am J Epidemiol 2003;157:185-194.
P.389
Gerton GL, Fan XJ, Barnhart K, et al. Presumed diagnosis of EP. Obstet Gynecol 2002;100: 505-510.
Lipscomb GH, McCord ML, Stovall TG, et al. Predictors of success of methotrexate treatment in women with tubal ectopic pregnancies. N Engl J Med 1999;341:1974-1978.
Lipscomb GH, Stovall TG, Ling FW. Nonsurgical treatment of EP. N Engl J Med2000;343:1325-1329.
Marion LL, Meeks GR. Ectopic pregnancy: history, incidence, epidemiology and risk factors. Clin Obstet Gynecol 2012;55(2):376-386.
Van Mello NM, Femke M, Ankum WM, et al. Ectopic pregnancy: how the diagnostic and therapeutic management has changed. Fertil Steril 2012;98(5):1066-1073.