Effect of obesity in childhood and adolescence
There is increasing evidence to associate maternal prepregnancy obesity with an increased risk of obesity and cardiometabolic risk factors in the offspring (25). Prepregnancy maternal obesity is associated with a higher likelihood of obesity in children at the age of 3 years (26).
It also confers a higher BMI and increased risk of diabetes in offspring during adolescence and adulthood (26, 27). This association is independent of genetic and environmental factors shared by mother and child (28). Maternal obesity is also associated with a risk of developmental delay and autism spectrum disorder in early childhood (29).There is also emerging evidence that excessive pregnancy weight gain as defined by the American Institute of Medicine is associated in offspring with obesity and an adverse cardiometabolic profile (25, 30, 31). The latter measures included raised C-reactive protein, systolic blood pressure, and lower high-density lipoprotein level. The critical period is suggested to be excessive weight gain in early pregnancy. These adverse metabolic profiles together with an increased risk of obstructive sleep apnoea in obese adolescents are associated with an increased cardiovascular risk in adults (32).
The onset of puberty has lowered over the past 150 years from approximately 14 years of age to 11.5-12 years old in girls in the United Kingdom (33, 34). The factors influencing menarche are well characterized including genetic, hormonal, psychological, and socioeconomic factors. However, this drop in age in girls has also coincided with the rise in obesity seen in the Western world. Since body fat is closely related to pulsatile release of gonadotrophin-releasing hormone and therefore the onset of puberty, a link cannot be excluded.
In young boys, puberty may be delayed with obesity and although the reason is not currently clear as to why, it may be related to feedback inhibition of androgens by a rise in aromatized oestrogen levels by adipocytes (32).
Obesity is also associated with an increased risk of developing asthma. Other problems may be exacerbated in adolescence for obese children such as psychological depression, anxiety, body image disorder, and negative self-esteem, particularly in girls. Increasing BMI is also associated with ovulatory dysfunction, menstrual irregularity, and, later in life, increased time to conception (35).
Obesity is a common feature of polycystic ovarian syndrome (PCOS), but only 20% of obese women have PCOS. This disorder affects 5-10% of women and is commonly diagnosed with two of the following three parameters: hyperandrogenism, chronic anovulation, and polycystic ovaries on ultrasonography. The disorder is closely linked to insulin resistance, type 2 diabetes, infertility, endometrial cancer, and possibly an increased risk of cardiovascular disease. A comparison between normal healthy and PCOS adolescents showed an increased risk of hirsutism, total testosterone, and hyperinsulinaemia in the latter but not dyslipidaemia when adjusted for BMI or waist/waist to hip ratio (36). depot medroxyprogesterone acetate (DMPA) is small (they may affect pharmacokinetics of contraceptives, particularly steroid-based contraceptives. Oral contraceptives are associated with changes in lipid, fibrinogen, and glucose metabolism. Some effects are enhanced further in smokers (40). The effect of hormonal contraceptives in obese patients is largely unknown due to the exclusion of this population in studies, which is of concern since obesity itself causes metabolic changes to increase cardiovascular risks. A recent study has shown that very obese women (BMI >35 kg/m2) using the combined oral contraceptive pill are at an increased risk of venous thromboembolic disease in comparison to non-obese women (41). Obesity is a known independent risk factor for thromboembolic disease and this needs to be considered when prescribing hormonal contraceptives.
Another challenge is the actual ability to perform the necessary examination for the introduction of the contraceptive.
For example, inserting of intrauterine devices or laparoscopic sterilization may be technically difficult particularly in the morbidly obese (42). In the United States, procedure-based methods (tubal ligation, implants, and intrauterine devices) have been shown to be favoured by women with increasing BMI with 50.5% of obese women but only 36.2% of normal weight women using these methods (35).Weight gain is one of the commonest reasons for discontinuation of hormonal contraceptives. However, studies in women using the combined oral contraceptive pill have shown little evidence that this is true (38). Evidence of weight gain identified in patients using Obesity in pregnancy is associated with poor pregnancy outcomes including miscarriage, gestational diabetes, pre-eclampsia, thromboembolism, prolonged labour, and postpartum haemorrhage (45). Fetal complications such as congenital anomalies, shoulder dystocia, stillbirth, and neonatal death are also increased in maternal obesity (46). The problems are not confined to the pathophysiological pathways but also technical difficulties. There is a higher risk of instrumental delivery and caesarean section in obese pregnant women (47, 48).
One-fifth of women from Scotland and one-third of American women entering pregnancy are obese (49, 50). The consequences of obesity in pregnancy extend beyond the immediate gestation as previously discussed. The maternal intrauterine environment impacts the fetal development and the lifetime health of the offspring. Therefore, effective screening policies in early pregnancy should be in place not only to identify high-risk pregnancies but also to put focused care in place (51).
Obesity and miscarriage
Overweight (BMI >25 kg∕m2) and obese women are at significantly increased risk of miscarriage regardless of the mode of conception (48, 52, 53). Furthermore, they have a threefold increased risk of recurrent miscarriage (54, 55). These studies have shown obesity to be an independent risk factor for miscarriage and the single most modifiable risk factor in high-income countries (56).
Lashen et al. (54) have reported an odds ratio (OR) of 1.2 (95% confidence interval (CI) 1.01-1.46) for miscarriage and an OR of 3.5 (CI 1.0312.01) for recurrent miscarriage in obese women with a BMI greater than 30. The higher incidence of spontaneous pregnancy loss is directly linked to a rise in insulin levels. It has been proposed that treatment with insulin-sensitizing agents such as metformin may reduce miscarriage rates. A meta-analysis identified an increased risk of miscarriage after ovulation induction and even oocyte donation suggesting a generally adverse milieu for the fertilized egg in the obese woman (53).Fetal abnormality risk
Once conception has occurred, there is a two- to threefold increased risk of birth defects associated with maternal preconception obesity including neural tube defects, cardiac anomalies (septal, tetralogy of Fallot, transposition of the great arteries), and diaphragmatic hernia (57). This increased risk is directly proportional to increasing maternal weight. The risk of gastroschisis is, however, reduced in obese mothers. A worrying consequence of obesity is the reduced sensitivity of ultrasonography as a screening test for fetal anomalies. It has been estimated that approximately 15% of normally visible structures will be suboptimally seen in women with a BMI above the 90th centile. The anatomical structures commonly less well seen with increasing BMI include the fetal heart, spine, kidneys, diaphragm, and umbilical cord (58). It has been recommended that obese mothers have increased folic acid (5 mg) periconceptually and antenatally, again highlighting the necessity of preconception care for such women (59).
Metabolic syndrome of pregnancy
Obesity is associated with a broad range of complications including diabetes, cardiovascular disease, dyslipidaemia, and hypertension, labelled as metabolic syndrome of pregnancy. Maternal obesity is related to metabolic complications, including the pregnancy-specific conditions of pre-eclampsia and gestational diabetes.
Pregnancy- related endocrine changes favour lipogenesis and fat accumulation (60). All women increase maternal fat stores irrespective of prepregnancy adiposity to meet the fetoplacental and maternal demands of late gestation and lactation; the main increase is towards the end of the second trimester. In normal-weight women, the majority of fat is accumulated centrally in the subcutaneous compartment of the trunk and upper thighs. In later stages of pregnancy, there is an increase in both the thickness of pre-peritoneal fat (visceral) and the ratio of pre-peritoneal to subcutaneous fat as measured by ultrasonography. This pattern of fat deposition is relevant to increasing insulin resistance as accumulation of hepatic fat has been shown to be an important mediator of insulin resistance during pregnancy in the rat model (61). Visceral adiposity is more closely related to adverse metabolic outcomes, including insulin resistance, hyperinsulinaemia, dyslipidaemia, hypertension, and the metabolic syndrome. As obese women have more saturated subcutaneous fat stores, they tend to accumulate more centrally than lean women, an observation which may reflect their higher insulin resistance (60). Central obesity appears to be correlated more strongly with adverse metabolic outcomes in pregnancy including gestational diabetes mellitus (GDM), gestational hypertension, and pre-eclampsia (62).Impaired glucose tolerance and gestational diabetes mellitus screening
The International Diabetes Federation estimates that one in six live births is to women with some form of hyperglycaemia in pregnancy. While 16% of these cases may be due to diabetes in pregnancy (either pre- existing diabetes (type 1or type 2) which antedates pregnancy or is first identified in the index pregnancy), the majority (84%) is due to GDM (6). GDM is defined by the WHO as carbohydrate intolerance resulting in hyperglycaemia first recognized in pregnancy (63). A meta-analysis of 20 studies showed that the unadjusted ORs for the development of GDM were 2.14 (95% CI 1.82-2.53), 3.56 (3.054.21), and 8.56 (5.07-16.04) in overweight, obese, and severely obese women respectively compared with normal-weight pregnant women (47).
However, in women who do not reach diabetes diagnostic criteria, there is mounting evidence that increasing BMI causes higher glucose levels, which in pregnancy are associated with adverse outcomes (49).
In 1954, Pedersen hypothesized that in diabetic mothers, high glucose levels were transferable to the fetus. In order to prevent hyperglycaemia, the fetus produces increased levels of insulin, which results in increased fetal growth (64). Later studies have shown that glucose levels need not reach diagnostic levels for diabetes in order to have similar outcomes. A study of over 1100 non-diabetic pregnant women given an oral glucose tolerance test showed that with resultant increasing glucose levels there was an increasing risk of large-for-gestational-age fetuses, preterm birth with a twofold increase in caesarean section, and clinical chorioamnionitis (64). In the latter case, with high glucose levels, chorioamnionitis was associated with a 12-fold increased risk of very preterm delivery. Later studies have corroborated the link between increasing prepregnancy BMI and neonatal adiposity (66). Fetal macrosomia is associated with an increased risk of caesarean section, birth trauma (vaginal tears, shoulder dystocia, and asphyxia), as well as transient hypoglycaemia (67).
Women who have developed gestational diabetes are at an added risk of then developing type 2 diabetes in later life. This is compounded by associated factors: high BMI, ethnicity, and a family history of type 2 diabetes as well as gestational glycaemic status (68). The gestational age of onset of GDM is linked to an increased risk of hypertensive disorders in pregnancy and preterm delivery, each of which are also associated with a raised BMI.
There remains controversy about the best way of screening women for GDM during pregnancy: should it be risk based? Or one-step screening or two-step screening (69)? In 2015, the European Board and College of Obstetrics and Gynaecology published its position statement on GDM screening in Europe (70). Later in the year, the International Federation of Gynecology and Obstetrics (FIGO) responded to this global challenge and published a report, entitled ‘FIGO Initiative on Gestational Diabetes Mellitus: A pragmatic guide for diagnosis, management and care' (5). This report has advocated one-step GDM screening for all women during pregnancy and has made recommendations for the GDM screening adaptations in different resource settings.
Hypertensive disorders during pregnancy
There is a large body of evidence highlighting the increased risk of hypertension and pre-eclampsia/eclampsia when obese (71-73). Both prepregnancy BMI and adulthood weight gain is associated with an increasing risk of pre-eclampsia. An American prospective study of 1644 pregnant women identified an increased risk of preeclampsia with weight gain in adulthood from the age of 18 years (71). This translated as a 4% increased risk of pre-eclampsia for every 1 kg of adult weight gain after adjusting for maternal age, ethnicity/ race, parity, educational attainment, and weight at age 18 (71).
A large United Kingdom study analysing over a quarter of a million singleton pregnancies (74) showed that the risk of adverse
Table 7.2 Adverse outcomes in pregnant women who are overweight or obese
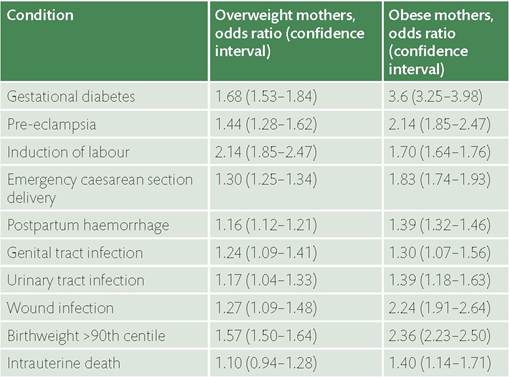
Source data from Sebire NJ, Jolly M, Harris JP1 Wadsworth J, Joffe M, Beard RW, Regan L, Robinson S. Maternal obesity and pregnancy outcome: a study of 287 213 pregnancies in London. International Journal of Obesity & Related Metabolic Disorders 2001;25(8):1175.
outcomes during pregnancy was not confined to the obese but also to the overweight group (BMI 25-30) (Table 7.2). Overweight pregnant women have an increased risk of conditions such as GDM and pre-eclampsia. During the intrapartum and postpartum periods, they are also at increased risk of delivery by emergency caesarean section, postpartum haemorrhage, and infection.
Obesity and risk of preterm rupture of membranes
There is mounting evidence that maternal obesity is associated with preterm rupture of membranes (PPROM) and induced preterm delivery (75, 76). In a systematic meta-analysis of over 1 million singleton births, there was evidence of an increased risk of spontaneous preterm birth in both overweight and obese women. An earlier study of over 250,000 singleton births in the United Kingdom did not find an increased risk of preterm delivery (events (61%). Although overall maternal mortality in the United Kingdom has fallen, the most recent report covering
2011-2013 follows the same trend in that maternal mortality in obese women was 30% and 22% in overweight women. Obesity is independently associated with having higher odds of dying due to specific pregnancy-related complications. Of concern is that an earlier report indicated that in some deaths procedure- related difficulties in obese patients may have contributed to their death such as inappropriately sized sphygmomanometer cuffs for the measurement of blood pressure or logistical issues (e.g. transport of the obese pregnant woman) (89, 90).
There should be clearly defined standards of care for the management of obese pregnant women throughout the course of their pregnancy, including advise as regards pre-conceptual weight loss, antenatal screening strategy, GDM screening, care during labour and postnatally. Each unit should be encouraged to collect data to quality assure their performance (69, 91, 92).