Emergency Evaluation and Treatment of the Sexual Assault Victim
James L. Jones
Sexual assault or rape is a common violent crime in the United States. According to the National Crime Victimization Survey, there were 260,940 rapes and sexual assaults in the United States in 2006 (1).
Accurate statistics are difficult to obtain because sexual assault is a common crime and not often reported to authorities. The Rape, Abuse and Incest National Network statistics for 2001 show that 38.6% of rape was not reported to the police (2). Most rape victims who know their assailant are less likely to report the crime when the perpetrator is an acquaintance. These factors make sexual assault the most underreported crime in the United States.
Since the 1970s, rape crisis centers have been developed in urban areas of the United States to deal with the particular problems of the sexual assault victims. Rape crisis centers often provide training for physicians and nurses in performing sexual assault examinations. These centers also provide continuity of care and counseling that is difficult to obtain in many other settings. The multidisciplinary approach used by many centers underscores the importance of the psychological aspects of sexual assault. In addition to meeting the acute medical needs of the patient, the medical staff is responsible for advocating for the immediate and long-term emotional needs of the victim as well.
Many physicians are uncomfortable performing sexual assault examinations. Sexual assault examinations are performed by nurse examiners in many states (3,4). The most important considerations in determining who should perform a sexual assault examination are experience and interest, as well as local statutes related to medical care. The forensic aspects of the examination require strict attention to detail and experience in performing sexual assault examinations. The psychological aspects of sexual assault demand that the examiner be compassionate, patient, and understanding.
A list of the responsibilities of the examiner in caring for a victim, as described by Kobernick et al. (5), follows:1. Prompt treatment of physical injuries
2. Collection of legal evidence
3. Careful physical examination
4. Documentation of pertinent history
5. Prevention of pregnancy
6. Prevention of sexually transmitted disease
7. Psychological support and arrangement for follow-up counseling
The physician or examiner should be familiar with all these aspects of care of sexual assault victims.
Five to ten percent of adult sexual assault victims are men. It is important to realize that male victims deserve the same respect and treatment considerations as female victims.
TRIAGE
Upon arrival at the emergency department, the victim should not wait in a public area but should be quickly and discreetly escorted to a private examination area. An assessment of the extent of the victim’s injuries should be made on admission. Critically injured victims should be treated without delay in an urgent care area. The forensic examination should be performed only after the victim is stabilized. If the victim has to be taken to the operating room, specimens can often be safely collected during an operative procedure. Fortunately, sexual assault victims are not usually severely injured. An unpublished review of 100 consecutive assaults reported to the Sexual Assault Recovery Center at Shands Hospital, Jacksonville, Florida, found that only two patients required hospitalization for injuries sustained during an assault. One patient was bleeding heavily from a labial laceration and required an examination under anesthesia; the other was a victim of a severe beating. A study by Hicks of rape victims presenting to a Miami emergency room also found that <1% of all victims require hospitalization (6).
The victim should be instructed not to wash, use the toilet, eat, or drink until the examination is completed. If friends or family members are present, they may remain with the victim if she wishes.
If the victim is alone, a nurse or rape crisis counselor should stay with her. The victim should not be left alone.Loss of control is an important psychological factor in rape; it is important to help the victim reestablish control over her surroundings. It is important that the victim be reassured as to her safety. The examiner should carefully explain the procedures that will be performed. At the Sexual Assault Recovery Center at Shands Hospital, the victim is given a folder containing information about each step of the examination. A list of tests that have been ordered is included along with the expected completion date. The victim should be informed that she may refuse any part of the examination. Consents for the examination and the release of the information to the police should be reviewed carefully and signed. Whether the victim intends to report the crime should be immaterial; she is still entitled to medical care.
FORENSIC MEDICINE
Many physicians find the medicolegal aspects of sexual assault intimidating. The examining physician must be familiar with the specific guidelines issued by the prosecuting attorney for sexual assault examination (7). Prepackaged rape kits are also available that should fulfill a particular state’s guidelines for collecting evidence. Common medical practices, such as using the newer rapid DNA probe technologies for detection of Neisseria gonorrhoeae and Chlamydia trachomatis, may not be admissible in some courts and cannot replace a traditional culture in making a diagnosis. As newer technologies are introduced, state guidelines change, and the hospital’s protocol should be updated.
The most important aspect of a forensic examination is adequate and careful documentation. Notes must be legible. Physicians may be called to testify years after the assault, and they must be able to rely solely on notes taken during the examination. It is equally important that physicians not make remarks that may be misinterpreted at a later date or in court.
This can be avoided if physicians realize that their role is not to determine whether the victim has been raped but to determine whether the examination is consistent with sexual assault. Physicians should avoid conclusive statements that are not supported by facts or their experience. Remarks concerning the victim’s behavior should not be entered into the record unless they are purely descriptive. Coping mechanisms produce a wide spectrum of responses to rape, thus physicians may encounter behavior that seems incongruent with a history of assault. Therefore, statements such as the victim’s behavior is inconsistent with sexual assault are inappropriate. The patient’s affect can be described instead.Physicians should also understand the concept of “chain of custody.” Courts will not consider evidence admissible if a direct line of custody cannot be established between the examiner and the court. As the evidence is gathered, it is placed into separate envelopes, sealed, and initialed. All specimens must be clearly labeled with the victim’s name, the date, the examiner’s name, and the source of the specimen. Clothing is placed in paper bags. Glass slides should be placed in carriers with rigid sides. The bags, envelopes, and carriers should be sealed with plastic tape and the examiner’s initials written across the tape or the seal. This should be done in such a fashion that if the container were opened, the tampering would be obvious. The evidence should then be placed in a large paper bag or envelope and sealed. The evidence is then either handed directly to a police officer or placed in a locked cabinet. A receipt should be obtained for the evidence when it is transferred to the police. Breaking the chain of custody, by faulty handling or record keeping, may make the entire examination inadmissible in court.
OBTAINING A MEDICAL HISTORY
The purpose of obtaining a history in a sexual assault case is to record as soon as possible the events that have occurred and to guide the physician during the examination.
If the patient is an adult and a good historian, the physician may eliminate some parts of the exam and tests, such as obtaining rectal or oral cultures when only vaginal penetration has occurred. In the absence of an adequate history, the physician should perform an encompassing physical examination. If the physician records remarks made directly by the victim, these should be placed in quotations; otherwise, the remarks are assumed to be paraphrased.The history should include the following:
1. Medical and surgical history: This should include allergies and medications.
2. Gynecologic history: The examiner should emphasize last coitus, menstrual history, current method of contraception, history of sexually transmitted disease, history of pelvic inflammatory disease, tampon use, and douching practices.
3. Obstetric history: Methods of delivery, gravidity, and parity.
4. Location, date, and time of assault.
5. Description of assault: The victim should be asked to describe the assault in her own words. The examiner should ask the victim to include the number of assailants, whether force was used, the presence of weapons, and what type of assault occurred. If the patient does not volunteer enough information, it is appropriate to ask, for example, “Did he put his penis in your vagina?”
PHYSICAL EXAMINATION OF THE ADULT
It is particularly important to inform the patient again of exactly what the examination involves and to reassure her that the examination will not be painful. The examiner should collect as much of the victim’s clothing as feasible, particularly the panties. The victim should remove the clothing herself, preferably over a clean paper or cloth sheet to catch any debris. If it is necessary to cut the victim’s clothing to remove it, torn or stained areas should be left intact.
The victim should then be carefully examined, paying close attention to lacerations, bruises, and foreign material (Fig. 26.1). Any foreign material should be carefully removed, placed in an envelope, and identified as to the location of origin.
Bruises, bite marks, and lacerations should be carefully described and diagrammed. Lacerations should be inspected carefully, particularly if a sharp object was used in the assault, to rule out a deep, penetrating injury. Photographs may be helpful if they effectively demonstrate an injury but should be taken by a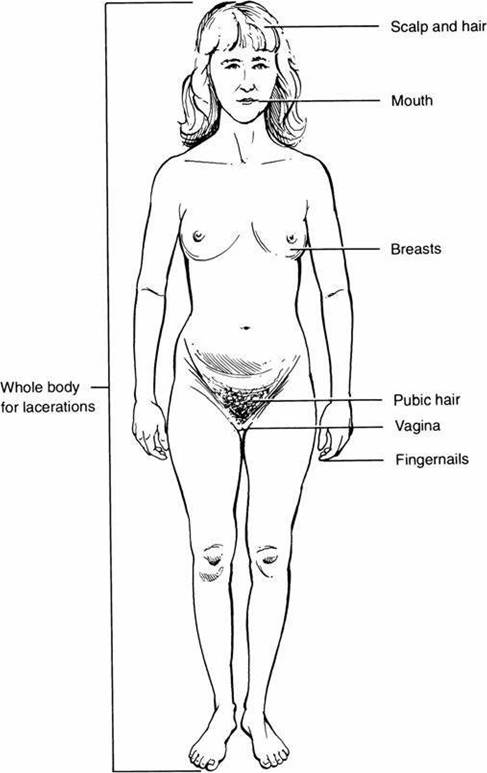
FIGURE 26.1 Examination of the sexual assault victim.
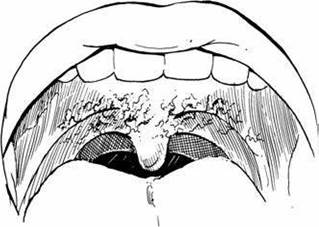
FIGURE 26.2 Fellatio syndrome: ecchymoses of the palate.
police or a medical photographer. Photographs can actually harm a case if they do not add significant graphic detail. The photograph should be labeled with an indelible marker or by other permanent means of identification.
A tongue blade or a moist, cotton-tipped applicator should be used to collect any suspicious stains or deposits on the skin. Since semen fluoresces a bright yellow-green, deposits can often be identified with a Woods light. The head hair should be combed with a new comb over a paper towel, carefully collecting foreign material. Loose pubic hair should be collected in a similar fashion.
The oral cavity should be carefully examined with a tongue blade. Victims will often bite themselves during a sexual assault, producing small abrasions in the buccal mucosa. Fellatio may also cause small submucosal hemorrhages, which are usually seen at the junction of the hard and the soft palates (Fig. 26.2) (8). If there is a history of fellatio, the oral cavity, especially the areas between the gum and the lips, should be swabbed with a cotton-tipped applicator and glass slides should be prepared. When obtaining specimens for determination of the presence of sperm, two slides should be made. One goes directly to the forensic laboratory; the other is used immediately as a wet mount. The specimens should be made with several swabs. After the slides are prepared, the swabs are allowed to air-dry before placing them in an envelope. The presence of sperm as noted by the examiner should be recorded in the chart, and a separate notation should be made as to whether the sperm are motile. Pharyngeal cultures should be taken for N. gonorrhoeae. A saliva specimen is obtained from the victim for blood antigen determination. A small square of filter paper is placed in the victim’s mouth, and the victim is encouraged to saturate it with saliva. It is important that no one handles the filter paper except the victim. If there is a history of fellatio, the victim should rinse her mouth out with water and wait 5 minutes before preparing the specimen.
The fingernails should be inspected for foreign material under the nails. If any foreign material is present, including dirt, it should be collected over a paper towel with a blunt wooden probe. Scrapings from each hand should be submitted separately.
The victim is then asked to lie on the examination table in the dorsal lithotomy position, so that a pelvic examination can be performed. The labia, posterior fourchette, and vestibule are carefully inspected under adequate lighting. Bruises, lacerations, and tender areas are carefully explored, diagrammed, and photographed, if necessary. Wood’s light should again be employed to highlight semen deposits. In younger victims, the posterior fourchette is very susceptible to injury, which appears as fine lacerations. In cases of chronic sexual abuse, the examiner should look for scarring in the posterior fourchette and the posterior vestibule.

FIGURE 26.3 Laceration of hymenal ring and posterior fourchette.
Physical findings suggestive of vaginal penetration are present in approximately 50% of sexual assault victims, but only 2% show clinical evidence of significant genital trauma (9). Injuries are typically minor and appear as small abrasions and lacerations. The examiner should describe any visible lesions and diagram their locations. The most commonly injured sites are the posterior aspect of the introitus, the hymen, labia minora, and the posterior fourchette (Fig. 26.3) (8). In a study of 311 rape victims by Slaughter et al. (10), 76% of the victims had an average of 3.1 sites of injury. Victims with nongenital injury are more likely to have genital trauma. In the absence of gross laceration, two techniques can be employed to highlight microlacerations: colposcopy and toluidine blue staining. The colposcope is a medium-powered binocular microscope with an internal light source that is commonly used to visualize the cervix (9). In a study of 18 volunteers examined within 6 hours after coitus, Norvell et al. (11) showed that microlacerations of the introitus and the vagina could be identified in 61%. Toluidine blue staining can also be used in the absence of gross lesions to highlight microlacerations (12). The stain should be applied directly to the perineum and then carefully wiped off using lubrication jelly on a gauze. Toluidine blue is a nuclear stain, so normal keratinized skin will not stain. Microlacerations show up as finely stained blue lines.
The buttocks are then gently separated and the anus is inspected for evidence of small fissures, lacerations, and scarring. Hemoccult should be obtained for evidence of occult rectal bleeding. If there is a history of anal penetration, the physician should look for evidence of rectal bleeding. Unexplained rectal bleeding should alert the physician to the possibility of bowel perforation. Proctoscopy or flexible sigmoidoscopy is then indicated.
Anal swabs should be taken and glass slides prepared. Sperm may be recovered from the rectum, but the yield is usually significantly lower than that from the vagina or the cervix (13).
A speculum moistened with warm water (do not use lubricant) can then be gently inserted in the vagina. The cervix is visualized for any evidence of trauma. Microlacerations on the cervix resulting from sexual trauma can be visualized with the aid of the colposcope (9). A specimen should be taken from the external os, and two glass slides should be prepared. Samples are also taken from the vaginal pool. Whether the sperm are motile should be noted. Sperm may remain motile in the vaginal pool for 12 hours. Sperm survival in the cervical os is considerably longer; motile sperm can be recovered from the cervix for up to 7 days (14). Cultures for gonorrhea and Chlamydia should be taken. As noted earlier, most courts will not accept direct antigen tests for determination of gonorrhea. At Shands Hospital in Jacksonville, Florida, the sensitivity and the specificity of the BD Probe Tec (15) assay are 100% and 100% for both N. gonorrhoeae and C. trachomatis.
Two vaginal swabs are obtained for antigen determination. Blood group antigens are secreted into body fluids by approximately 80% of the population (16). Although it cannot identify a specific assailant, this technique is useful to exclude or include someone from a list of suspects.
Vaginal swabs are also obtained for analysis of the prostatic antigen, p30, and acid phosphatase. Finding these seminal factors can establish penile penetration in the absence of sperm.
Additional swabs, usually six to eight, also can be obtained from the vaginal pool for DNA profiling. DNA profiling depends on the diversity of repetitive regions of DNA, variable number tandem repeat (VNTR) for forensic analysis. These regions are targeted with specific primers, amplified using PCR and separated with either capillary or gel electrophoresis. First described in 1985, there are a number of analytical techniques including short tandem repeat (STR), Y-STR, and mitochondrial DNA testing in common use. STR is primarily used for forensic analysis. In the United States, the FBI has designated 13 STR loci for analysis and maintains the CODIS, Combined DNA Index System, database. Unlike fingerprint analysis, DNA profiling cannot identify a specific individual. It can, however, indicate the probability that an individual is involved to greater than one in a trillion.
The vaginal walls are then inspected for lacerations. This is most easily accomplished while slowly withdrawing the speculum. In very young or postmenopausal patients, who have poorly estrogenized vaginal mucosa, lacerations of the vaginal sidewalls are more common. Laceration of the cul-de-sac or the posterior vaginal fornix can also be seen, particularly if a foreign object is inserted into the vagina. Injury from insertion of a foreign object can also cause perforation of the cul-de-sac and bowel injury. Ifa penetrating injury is suspected, a laparotomy should be performed to rule out injury to the bowel.
EXAMINATION OF THE CHILD
A discussion of sexual abuse in children must begin with the physician’s legal requirement for reporting of cases. In all states, a physician having a reason to suspect child sexual abuse must report to a designated agency. Agencies that receive reports vary in different states and localities, and it is essential that the physician learns these requirements before performing any examination. The services of a multidisciplinary assessment team, if available, can be of great assistance in evaluating the child and the total family situation.
Examinations for alleged sexual abuse in children usually do not result from allegations of acute rape (17). More commonly, the allegation is of incest, fondling, molestation, or exploitation. This being the case, serious questions must be raised as to whether an emergent examination is required or whether the child should be referred to a team for a total evaluation. In the unusual case where there may be forensic collection considerations, the protocol for obtaining specimens should be similar to that used in adult patients. The expected yield from collection of evidence in child victims, however, is quite different in children than in adults. In the study done at Children’s Hospital of Philadelphia, Christian et al. (18) found that forensic evidence, when present, was found on clothes or bedclothes, not on the prepubertal child. Chronic or recurrent sexual abuse in children is usually manifested by subtle physical signs and is likely to be accompanied by behavioral or developmental signs or symptoms. For this reason, the child sexual assault examination must be carried out in the context of a total pediatric health assessment and by an examiner skilled in assessing for the specific manifestations of child sexual abuse (19). After a history has been taken by the examiner or by a trained interviewer, the examiner should decide the extent of the examinations necessary, decide the cultures and specimens to be collected, and incorporate an explanation for the child, who should know that the examination is not painful or more intrusive than necessary. The examiner should be understanding and patient but should not play games with the child to gain cooperation. This is a common ploy of abusers.
Children should never be examined against their will. If examination is absolutely necessary for medical reasons, the examination should be performed under anesthesia. Genital examinations in children should be carried out in the modified dorsal lithotomy (frog-leg) and/or knee-chest position. Children are often uncomfortable in the knee-chest position, but it may offer visualization up to the cervix without instrumentation. Uncooperative or frightened children often do quite well in their mother’s lap on an examining table (Fig. 26.4). Stirrups may be used in older children but are usually unnecessary and frightening in younger children. The use of a colposcope in the examination offers a light source, magnification, and photographic documentation and greatly simplifies evaluation and documentation (20).
Findings associated with child sexual abuse have been more clearly delineated in recent years. In addition, there is a greatly enhanced understanding of normal anatomic variations based on recent studies (21-27). Most of the physical findings seen with sexual abuse are indicators of genital trauma and must be coupled with the history to raise a serious question of abuse. Some findings or combinations of findings, however, are so compelling as to be reasonably diagnostic of abuse. In our experience with a highly selected referral population, 65% of examinations result in no finding, 30% have findings consistent with sexual abuse, and 5% have findings considered diagnostic of sexual abuse. It is useful to remember that a normal examination is often seen with any kind of allegation. Many times the offender has confessed to specific sexual acts and there is no physical finding. A physical examination alone can never rule out the possibility of sexual abuse (28,29).
The genital examination is best performed by using labial traction, in which the labia majora are grasped between the thumbs and the index fingers and are gently lifted laterally and toward the examiner, or labial separation, where the thumbs of the examiner are placed on the labia majora and mild lateral pressure is applied. The latter is more comfortable, whereas the former usually offers better direct visualization of the edges of the hymen. Digital or speculum examinations are rarely advisable or necessary except in sexually active older children.

FIGURE 26.4 Position of a child on the mother's legs for examination.
Many of the findings associated with genital trauma focus on changes in the hymen. A clear understanding of normal variants is essential. The hymen can normally be circular (annular), semilunar (crescentic, with attachments at about 2 o’clock and 10 o’clock), cribiform, or septate. In unusual circumstances, the hymen may be imperforate, which has medical implications but no implications for sexual abuse. Congenital absence of the hymen has never been reported (30). In the first few months of life, the hymen is still estrogenized from maternal influences and becomes estrogenized again in early puberty. Estrogenization produces an appearance of hypertrophy, redundancy, and white, pearl-like mucosa. It often is more difficult to assess for scars with these changes.
Findings statistically diagnostic of penetrating trauma or sexual abuse are
■ Fresh lacerations of the anus or posterior fourchette
■ Acute laceration or healed complete transection of the hymen
■ Bruising of the hymen
■ Absence of a part of the hymen
■ Scars on the anus, posterior fourchette, penis, or scrotum
■ Pregnancy (31-34).
Documentation issues are even more important in children than in adults, as the time between the examination and the possible testimony is even longer. Photographs are the method of choice for accurate documentation of findings, but detailed diagrams of body findings and specific genital findings may suffice. Laboratory
support may be very useful in supporting the diagnosis of child sexual abuse. Cultures for N. gonorrhoeae should routinely be done in all postpubertal cases where genital contact by the abuser is possible. Cultures in prepubertal children are indicated only if there are signs of infection. Since positive cultures from sites other than the primary contact are common, cultures should be obtained from vaginal, rectal, and oropharyngeal sites. A positive result from culture makes sexual contact a certainty if the patient is not a newborn. Cultures for C. trachomatis and herpes, types 1 and 2, may be indicated under certain clinical conditions. The presence of genital warts on gross inspection or Trichomonas vaginalis in wet preparations is usually considered a strong indicator of sexual abuse in children. However, condylomata can be acquired either through autoinoculation or perinatal transmission (35). Human immunodeficiency virus (HIV) antibody testing and serologic testing for syphilis are not routinely done unless more specific indicators are present (19,36).
TREATMENT OF SEXUAL ASSAULT VICTIMS
Most physical injuries sustained during rape or sexual assaults are minor. Minor cuts, abrasions, and bruises on the external genitalia will respond to cold compresses and sitz baths. Vaginal sidewall lacerations often do not require repair unless they are deep. Deep lacerations are best repaired under anesthesia, where the extent of the lesion can be more fully appreciated. As noted earlier, penetrating injuries to the cul-de-sac also require examination under anesthesia and possible exploratory laparotomy. Patients assaulted with foreign objects should also receive tetanus prophylaxis.
Prevention of Sexually Transmitted Disease
The risks of acquiring a sexually transmitted disease from a single act of sexual assault are difficult to determine. The risks depend on the prevalence of the disease in the local community and on the nature of the assault. Infections detected within 24 hours of the assault most likely represent a preexisting condition (37). In a small study of 109 sexual assault victims who returned for follow-up, Jenny et al. (38) found that the risks of acquiring N. gonorrhoeae and C. trachomatis from a single act of sexual assault were 4% and 2%, respectively. The baseline prevalence of these infections in assault victims is higher: 6% for N. gonorrhea and 10% for Chlamydia. The prevalence of syphilis in rape victims has been reported in several studies to be <3% (38). The risk of acquiring HIV from a single act of unprotected vaginal intercourse has been estimated as between 0.1% and 0.2%. The risk of transmission of HIV from penile-anal penetration is somewhat higher, between 0.1% and 3.0% (36).
Sexual assault may result in an increased risk of the transmission of HIV since transmission of the virus is facilitated if the normal barriers that intact vaginal and vulvar mucosa provide are broken down.
Many sexual assault centers provide prophylactic antibiotics at the time of the sexual assault examination. Although the risk of acquiring a sexually transmitted disease from a single assault is low, treatment at the time of the initial examination is safe and effective and avoids treatment failure due to poor follow-up. Lack of adequate follow-up is a significant challenge in treating sexual assault victims. At Shands Hospital, Jacksonville, Florida, only 20% of victims return for follow-up counseling or testing. In the study by Jenny et al. (38), cited previously, follow-up was accomplished in only 53%.
The treatment should cover the most common pathogens, gonorrhea, Chlamydia, and incubating syphilis. The Centers for Disease Control (CDC) recommendations for treatment of common sexually transmitted diseases are outlined in Table 26.1 (36). Selection of prophylaxis should also be determined by

CDC 2006 GuidelinesforTreatmentofSexuaIIyTransmitted Diseases
| Disease | Treatment |
| Chlamydia Recommended regimens | Azithromycin, 1 g orally in a single dose, OR Doxycycline, 100 mg twice a day for 7 d |
| Alternative regimens | Erythromycin base, 500 mg orally four times a day for 7 days, OR Erythromycin ethylsuccinate, 800mg orally four times a day for 7 d |
| Gonococcal infections Recommended regimens | Cefixime, 400mg orally in a single dose, OR Ceftriaxone, 125mg IM in a single dose, OR |
| Alternative regimens | Spectinomycin,2g IM in a single dose, OR Ceftizoxime, 500mg IM, OR Cefotaxime, 500mg IM, OR Cefotetan, 1 g IM |
| Syphilis Recommended regimen | Benzathine penicillin G, 2.4 million units IM once |
| Alternative regimens | Doxycycline, 100 mg Orallytwice a day for 2 weeks, OR Tetracycline, 500 mg orally four times a day for 2 weeks |
| Trichomoniasis Recommended regimen Alternative regimen | Metronidazole, 2g orally in a single dose Metronidazole, 500 mg twice a day for 7 d |
Note,. CDC, Centers for Disease Control; IM intramuscularly.
Source'. Ref. 36.
local sensitivity studies. It should be noted that the CDC no longer recommends the use of Auroquinolones for the treatment of gonorrhea due to antibiotic resistance (39).
Antibiotics that can be given as a single dose are preferred. The risk that young children will acquire N. gonorrhoeae or Chlamydia from sexual assault is low. Prophylaxis is not recommended unless the assailant is known to be infected, and treatment with antibiotics is withheld until diagnostic tests are completed. Treatment of N. gonorrhoeae and C. trachomatis in children is adjusted to body weight (36).
Postexposure Prophylaxis for Sexually Transmitted Viruses
The management of patients exposed to HIV, human papillomavirus (HPV), herpes simplex virus, and hepatitis continues to evolve. Postexposure prophylaxis (PEP) for health care workers exposed to hepatitis and HIV has become standard practice. It has been estimated that the use of zidovudine has led to an 81% reduction in the transmission of HIV to health care workers after a needle stick (40). PEP is unavailable for HPV and not routinely offered for herpes simplex.
Prophylactic treatment of sexual assault victims for HIV is more controversial. The medications are expensive and funding issues may present obstacles to treatment. Complicating the decision process is the low follow-up rate of rape victims. PEP for HIV is effective but there are significant possible side effects, some so severe as to lead to discontinuance of the medications. Serial laboratory studies such as liver function tests and complete blood counts should be obtained. Close follow-up with psychological support is essential but may be difficult to obtain. Patients requesting such prophylaxis must be carefully counseled prior to initiating treatment.
While the risk of acquiring HIV after a sexual assault is low, approximately 5 per 10,000 exposures, sexual assault victims should be offered prophylaxis for HIV (41).
Such guidelines are based on the familiar Public Health Service guidelines for management of health care workers exposed to HIV (42). When there is a significant risk of exposure to HIV, a course of highly active antiretroviral therapy, HAART, should be initiated as soon as possible. These medications must be initiated within 72 hours of the assault, otherwise, HAART is not recommended. The CDC recommends a 4-week regimen of two drugs, such as zidovudine and lamivudine, for most HIV exposures (42). At this time, there are insufficient clinical data to suggest a specific antiviral regime. A protease inhibitor such as indinavir is added if the exposure involves an increased risk of transmission of the virus or if resistance to one of the drugs used for PEP is suspected. Oral, rectal, or vaginal penetration by the assailant’s penis should be considered a high-risk exposure. The CDC recommendations for management of patients after a sexual exposure are listed in Table 26.2.
Unfortunately, there are no clear-cut guidelines for health care workers regarding counseling of sexual assault victims. It is important to remember that clinical data support only the use of zidovudine. Additional drugs were added based on the experience gathered in treating HIV-infected patients. As this field of medicine is rapidly evolving, patients should be referred to physicians who are expert in the use of these medications and the management of HIV.
If the assailant was known, attempts should be made to determine if he is a carrier of hepatitis B. If the victim requests, she should be offered prophylaxis with hepatitis B immunoglobulin. Prophylactic treatment for hepatitis B is usually not offered to rape victims unless the assailant is a known carrier or the victim requests it.
TABLE

Basic and Expanded PEP Regimens
Basic regimen
4 weeks of both zidovudine, 600 mg PO every day in divided doses (i.e., 300 mg b.i.d.), and lamivudine, 150 mg PO b.i.d.
High-risk exposure
Basic regimen plus either
• Indinavir, 800 mg PO q 8 hr
OR
• Nelfinavir, 750 mg PO t.i.d.
OR
• Abacavir, 300 mg b.i.d.
OR
• Efavirenz, 600 mg daily at bedtime
It is important that these medications be started immediately.
Note: PO, by mouth; b.i.d., twice daily; t.i.d., three times per day.
Source: Ref. 36.
It is also important that the victim understands that sexually transmitted viruses are chronic infections. HPV-related cervical dysplasia may surface years after an exposure, and it is important that the victim understands that yearly Pap smears are essential. Follow-up testing for HIV and hepatitis B may also be indicated.
Prevention of Pregnancy
The risk of pregnancy after an unprotected act of intercourse ranges from 0% to 26%, depending on the timing of the victim’s cycle. If the victim is at risk for pregnancy and the examination occurs within 72 hours of the assault, postcoital (emergency) hormonal birth control should be offered.
While a number of hormonal preparations have been used to prevent pregnancy, a progestin-only formulation, Plan B, is widely used and approved by the US Food and Drug Administration for emergency contraception (43). This method is somewhat more effective than a regime based on the Yuzpe method and is associated with less nausea. However, the original method of Yuzpe is very effective and widely available (44). This technique uses high-dose ethinyl estradiol and norgestrel/levonorgestrel to prevent pregnancy. A commercially available product, Preven, is marketed as an emergency contraceptive based on the Yuzpe technique. The principal mechanism of action is to prevent fertilization. A study of the effectiveness of the Yuzpe method of emergency contraception estimates that the technique reduces the risk of pregnancy by 75.4% (45). One hundred micrograms of ethinyl estradiol and either 1.0 mg of norgestrel or 0.5 mg of levonorgestrel is given orally within 72 hours of the assault; this is repeated 12 hours later. Any combination of birth control pills that provides the equivalent amount of ethinyl estradiol and norgestrel may be used. The pregnancy rate with this regime is approximately 1.6% (43). The ACOG Practice Bulletin on Emergency Contraception (December 2005) outlines 21 separate regimens which may be used for emergency contraception in addition to Plan B (46). The most common side effect of these regimens is nausea and vomiting, which may be treated with antiemetics.
Insertion of a copper-bearing intrauterine device (IUD) within 5 days of conception is also an effective means of preventing implantation (46). In patients in whom hormonal therapy is counterindicated, the copper IUD is a reasonable option. As there are no studies regarding the efficacy of progesterone secreting IUDs in such settings, these devices should not be used.
It should be remembered that postcoital hormonal or IUD birth control is considered by some to be a form of abortion. The mechanism of action of these techniques should be carefully explained to the victim so she can make an informed decision. In addition, a sensitive pregnancy test should be obtained before any treatment is initiated.
Psychological Support and Counseling
The most significant medical problem that the rape victim presents with is a psychological one. Rape trauma syndrome was initially described by Burgess and Holmstrom in 1974 (47). The syndrome is composed of two phases, an acute phase and a long-term reorganization phase.
The response to sexual assault seen in the acute phase is described as either controlled or expressive. Expressive behaviors, demonstrated by 75% of victims, include anger, grief, and anxiety. Twenty-five percent of victims respond in a controlled fashion and internalize their emotions. Such controlled behavior has led some examiners to conclude that the victim has not been assaulted because her behavior is different from what is expected.
Somatization is a common feature of the acute phase. Victims may complain of a wide variety of somatic manifestations of the sexual assault, including sleep disturbances, muscle tension, headaches, and gastrointestinal problems. The acute phase typically lasts from 3 to 6 months (48).
The long-term reorganization phase may last for years. The clinical signs include depression, sexual dysfunction, substance abuse, and low self-esteem (48). Felitti (49) found a significant increase in morbid obesity in victims of child abuse. Chronic pelvic pain is also strongly associated with a history of sexual abuse. When dealing with patients who present with complaints of depression, sexual dysfunction, or chronic pain, one should rule out sexual abuse as an underlying factor. Physicians commonly treat sexual assault victims, but they are not always aware of it.
CONCLUSION
Sexual assault is a major social and medical problem in the United States. Treatment of sexual assault victims presents a unique challenge to the physician. The examination should only be performed by professionals who have both the technical skills to perform and interpret the physical examination and the compassion and understanding to deliver medical care to victims.
Acknowledgement: The author is indebted to Dr Jay M. Whitworth (deceased) who was an invaluable resource in the writing of this chapter.
References
1. Bureau of Justice Statistics. Criminal Victimization, 2006. Washington, DC: U.S. Department ofJustice; 2008.
2. The Rape, Abuse and Incest National Network. Available at: www.rainn.org.
3. Antognoli-Toland P. Comprehensive program for examination of sexual assault victims by nurses: a hospital-based project in Texas. JEmerg Nurs. 1985;11(3):132.
4. Houmes BV, Fagan MM, Quintana NM. Establishing a Sexual Assault Nurse Examiner (SANE) program in the emergency department. JEmergMed. 2003;25(1):111-121.
5. Kobernick ME, Seiferts S, Sanders AB, et al. Emergency department management of the sexual assault victim. JEmerg Med. 1985;2:205.
6. Hicks DJ. Rape: sexual assault. Am J Obstet Gynecol. 1980;137(8):931.
7. Office of the Attorney General. ProtocolforSexualAssaultExaminations. FL: Office of the Attorney General; 2002.
8. Geist RF. Sexually related trauma. EmergMed Clin North Am. 1988;6(3):439.
9. Slaughter L, Brown C. Cervical findings in rape victims. J Obstet Gynecol. 1991; 164(2):528.
10. Slaughter L, Brown CR., Crowley S, et al. Patterns of genital injury in female sexual assault victims. Am J Obstet Gynecol. 1997;176:609-616.
11. Norvell MK, Benrubi GI, Thompson RJ. Investigation of microtrauma after sexual intercourse. J Reprod Med. 1984;29(4):269-271.
12. Lauber AA, Souma ML. Use of toluidine blue for documentation of traumatic intercourse. Obstet Gynecol. 1982;60(5):644.
13. Tucker S. Claire E, Ledray LE, et al. Sexual assault evidence collection. Wis Med J. 1990;89(7):407.
14. Soules MR, Pollard AA, Brown KM, et al. The forensic laboratory evaluation of evidence in alleged rape. Am J Obstet Gynecol. 1978;130(2):142.
15. BD Probe Tec. Sparks, MD: Becton, Dickinson & Co.
16. Cabaniss ML, Scott SE, Copeland L. Gathering evidence for rape cases. Contemp Obstet Gynecol. 1985;25(3):160.
17 American Academy of Pediatrics, Committee on adolescence: rape and the adolescent. Pediatrics. 1988;81:595.
18. Christian C, Lavele J, DeJong A, Loiselle J, Brenner L, Joffe M. Forensic evidence findings in prepubertal victims of sexual assault. Pediatrics. 2000;106(1):100-104.
19. American Academy of Pediatrics, Committee on Child Abuse and Neglect. Guidelines for the evaluation of sexual abuse of children. Pediatrics. 1999;103:186-191.
20. McCann J. The use of culposcope in childhood sexual abuse examinations. Pediatr Clin North Am. 1990;37(4):863.
21. Heger AH, Ticson L, Guerra L, et al. Appearance of the genitalia in girls selected for non-abuse: review of hymenal morphology and non-specific findings. J Pediatr Adolesc Gynecol. 2002;15:27-35.
22. Heger A, Emans SJ, Muram D, eds. Evaluation of the Sexually Abused Child. A Medical Textbook and Photographic Atlas. 2nd Ed. New York, NY: Oxford University Press; 2000.
23. Berenson A, Heger A, Andrews S. Appearance of the hymen in newborns. Pediatrics. 1991;87:458-465.
24. McCann J, Wells R, Simon M, Voris J. Genital findings in prepubertal girls selected for non-abuse: a descriptive study. Pediatrics. 1990;86:428-439.
25. Berenson AB, Heger AH, Hayes JM, et al. Appearance of the hymen in prepubertal girls. Pediatrics. 1992;89:387-394.
26. Berenson AB, Grady JJ. A longitudinal study of hymenal development from 3 to 9 years of age. J Pediatr. 2002;140:600-607.
27. Berenson AB, Chacko MR, Wiemann CM, Mishaw CO, Friedrich WN, Grady JJ. A case-control study of anatomic changes resulting from sexual abuse. Am J Obstet Gynecol. 2000;182:820-834.
28. Muram D. Child sexual abuse: relationship between sexual acts and genital findings. Child Abuse Negl. 1989;13:211.
29. DeJong A, Rose M. Legal proof of child sexual abuse in the absence of physical evidence. Pediatrics. 1991;88(3):506.
30. Jenny C, Kuhns ML, Arakawa F, et al. Hymens in female infants. Pediatrics. 1987; 80(3):399.
31. McCann J, Voris J, Simon M. Genital injuries resulting from sexual abuse, a longitudinal study. Pediatrics. 1992;89:307-317.
32. McCann J, Voris J. Perianal injuries resulting from sexual abuse: a longitudinal study. Pediatrics. 1993;91:390-397.
33. Heppenstall-Heger A, McConnell G, Ticson L, et al. Healing patterns in anogenital injuries: a longitudinal study of injuries associated with sexual abuse, accidental injuries, or genital surgery in the preadolescent child. Pediatrics. 2003;112: 829-837.
34. Heger A, Ticson L, Velasquez O, Bernier R. Children referred for possible sexual abuse: medical findings in 2384 children. Child Abuse Negl. 2002;26:645-659.
35. Wynne JM, Hobbs CJ. Anogenital warts in prepubertal children; sexual abuse or not? Int J Std AIDS. 1993;4(5):271-279.
36. Update to CDC's Sexually Transmitted Diseases Treatment Guidelines, 2006: Fluoroquinolones No Longer Recommended for Treatment of Gonococcal Infections. MMWRMorbMortal WklyRep. 2007;56(14):332-336.
37. Schwarcz SK, Whittington WL. Sexual assault and sexually transmitted diseases: detection and management in adults and children. Rev Infect Dis. 1990;12(Suppl. 6): S680-S690.
38. Jenny C, Hooten TM, Bowers A, et al. Sexually transmitted diseases in victims of rape. N Engl JMed. 1990;322(11):713.
39. Mastro TD, deVincenzi I. Probabilities of sexual HIV-1 transmission. AIDS. 1996; 10(Suppl A):S75-S82.
40. Management of possible sexual, injecting-drug-use, or other non-occupational exposure to HIV, including considerations related to antiretroviral therapy. MMWR Morb Mortal Wkly Rep. 1998;47(RR-17):1-137.
41. Antiretroviral Postexposure Prophylaxis After Sexual, Injection-Drug Use, or Other Nonoccupational Exposure to HIV in the United States. MMWR Morb Mortal Wkly Rep. 2005;54(RR02):1-20.
42. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWRMorbidMortal WklyRep. 2001;50(RR11):1-42.
43. Grimes D. Progestin-only emergency contraception. Contracept Rep. 1999;10(5): 8-10.
44. Yuzpe A, Smith P, Rademakeer A. A multi-center clinical investigation employing ethinyl estradiol combined with dl norgestrel as a postcoital contraceptive agent. Fertil Steril. 1982;37(509):580.
45. Trussel J, Rodriiguex G, Ellertson C. New estimates of the effectiveness of the Yuzpe regime for emergency contraception. Contraception. 1998;57(6):363-369.
46. ACOG. Emergency Contraception. ACOG Practice Bulletin #69, Washington, DC: American College of Obstetricians and Gynecologists; 2005.
47. Burgess AW, Holmstrom LL. Rape trauma syndrome. Am J Psychiatry. 1974; 131(9):981.
48. Gise LH, Paddison P. Rape, sexual abuse, and its victims. Psychiatr Clin North Am. 1988;11(4):629.
49. Felitti VJ. Long term medical consequences of incest, rape and molestation. South MedJ. 1991;84(3):329.