Gynecologic Traumas
Tracey Maurer
Gynecologic trauma can result from a variety of situations. Included in this discussion are sexually related trauma, trauma associated with women’s sports or leisure activities, and trauma that occurs from pelvic fractures.
SEXUALLY RELATED TRAUMA
A substantial body of literature addresses trauma from rape, as well as trauma occurring during consensual coitus (1-10). The major forms of sexually related trauma dealt with in the literature result from unexpected trauma occurring between consenting adults. Even though sexual abuse and its related trauma may be seen in emergency departments (EDs), abused women without lifethreatening injuries or hemorrhage are generally evaluated in a well-controlled setting established for rape victims (1-3) (Chapter 26). Nevertheless, the gynecologic injuries that can occur during consensual and forced coitus are similar.
Women who are seen for emergency evaluation associated with sexually related trauma not only are in pain but also harbor feelings of embarrassment and anguish. In such a setting, compassion is as important as diagnostic acumen.
Trauma resulting from oral-genital sex can present in many ways. One finding seen in the oral cavity is referred to as fellatio syndrome. Erythema, petechia, purpura, and ecchymoses of the soft palate are seen (4). These are due to hemorrhage, possibly from repetitive negative pressure in the oral cavity, combined with the action of the tensor and levator veli palatini muscles, or solely from thrusting against the highly vascular soft palate (4). The lesions are painless, nonulcerative, and nonblanching (4). A history of fellatio can deter an extensive diagnostic workup, but a differential diagnosis includes paroxysmal coughing, sneezing, vomiting, infection, tumors, blood dyscrasias, and capillary fragility (4). Cunnilingus syndrome results from oral-genital sex in which the tongue is used on the partner’s genital areas (4).
The findings are pain of the ventral surfaces of the tongue and throat with abrasions and ulcerations of the lingual frenulum (4). Chronic irritation can result in a traumatic fibroma on the frenulum (4).Two possible, but rare, occurrences can be seen in the female recipient of oral-genital sex. One is a pneumoperitoneum. This can result after air is blown into the vagina, traverses the cervical canal and endometrial cavity, and enters the abdomen through the fallopian tubes (4). Cases have been reported in patients with their uterus in situ (4). Posthysterectomy cases have also been encountered, with the supposition that the air entered through a small dehiscence in the vaginal cuff (4,5). These patients generally have lower abdominal pain, upper quadrant pain, or shoulder pain (4). Peritoneal signs tend to be absent, allowing for conservative management (5). The clinical course is benign, with the air being gradually absorbed spontaneously. Cuff defects should be repaired when encountered (4,5).
Air embolism is the second complication seen in the female recipient of oral-genital sex. It is uniformly fatal (4). Death occurs rapidly, and resuscitative measures are usually too late. This complication has been reported in
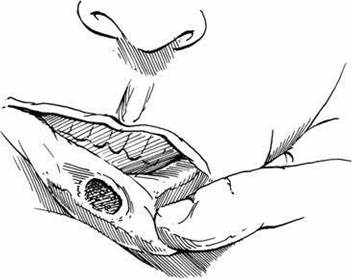
FIGURE 27.1 Chancre behind lip.
seven gravid women, all at >20 weeks of gestation (4). Whether or not oral genital-related air embolism can occur in nonpregnant women is not known.
Another possible, although rarely documented, complication of oralgenital sex is a vulvar hematoma from a human bite. One case report exists in the literature (11). Finally, oral-genital sex can lead to lesions of the oral cavity caused by sexually transmitted diseases. This should be kept in mind by the practitioner, so that information can be elicited from the patient (Fig. 27.1).
Trauma with coitus can range from hymenal tearing during initial intercourse to evisceration with hemorrhage.
Small tears of the hymen are usually associated with minimal discomfort, but occasionally, profuse bleeding that requires repair can occur (4).Vaginal lacerations and ruptures are rare, but when they are seen, it is usually in women of reproductive age who were having consensual intercourse (4,5,9). Metsala and Nieminen (9) found that approximately 88% of vaginal ruptures occurred during penile coital activity, with most of the remaining cases owing to other direct mechanical effects. The exact cause of the rupture often cannot be determined. Many predisposing factors have been suggested (4,7,9). In 1965, Purnell reported several cases of apparently spontaneous rupture of the vaginal vault (9). All of these cases were in postmenopausal women with vaginal atrophy. They occurred with sudden increases in intra-abdominal pressure during lifting, coughing, falling, or defecation. Purnell’s theory was that the sudden intra-abdominal pressure acted through the pouch of Douglas on a weakened posterior fornix to bring about a rupture. Women in both these situations generally had vaginal bleeding as the presenting symptom. Exsanguination has been reported (4,6,7). Sometimes, a history of sharp vaginal pain during intercourse is obtained (6,7). Surrounding structures may also be injured, and evisceration of abdominal contents has been seen (Fig. 27.2) (4,8).
Management starts with controlling the bleeding and treating shock, if present. If the bleeding is heavy, a moist vaginal packing can be placed as a tamponade while the history and physical examination are completed, with particular emphasis on other signs of trauma. When the bleeding has slowed, the vagina can be examined to determine the extent of the laceration. Most lacerations are in the posterior and right lateral fornix (Fig. 27.3) (6,7,9). Often, the examination has to take place in the operating room under general anesthesia for patient comfort. If evisceration has occurred and the penetration is known to be by a penis, finger, or other blunt object, the physician may attempt to replace the

FIGURE 27.2 Evisceration after vaginal laceration.
eviscerated organs, usually bowel, back into the abdomen using moist sponges and with the patient in the Trendelenburg position. If the bowel has passed beyond the introitus, it should be wrapped in moist towels until the patient can be taken to the operating room. Included in the evaluation should be a digital rectal examination to look for a rectal laceration. The bladder can be evaluated by instillation of indigo carmine and then observed for leakage. Cystourethrography may be necessary to look for intra-abdominal leakage (12). A flat plate of the abdomen is necessary to rule out an intraperitoneal foreign body.
Once the evaluation is complete and there are no other injuries besides the vaginal rupture known to be caused by a blunt object, simple vaginal repair with observation and intravenous antibiotics is indicated. Rarely does significant bowel injury occur in this situation (4). If further injury has been documented or evisceration outside the introitus is present, then abdominal repair becomes necessary. If bleeding persists even after closure and applied pressure to a vaginal nonpenetrating laceration, then laparotomy with hypogastric artery ligation is an option (13). A transverse incision has been advocated when an abdominal approach becomes necessary, because it is a stronger incision than those available when operating in a contaminated field. However, if bowel injury is even suspected, a vertical incision is necessary to evaluate the entire bowel fully. Upper abdominal bowel injuries have been reported after a history of blunt
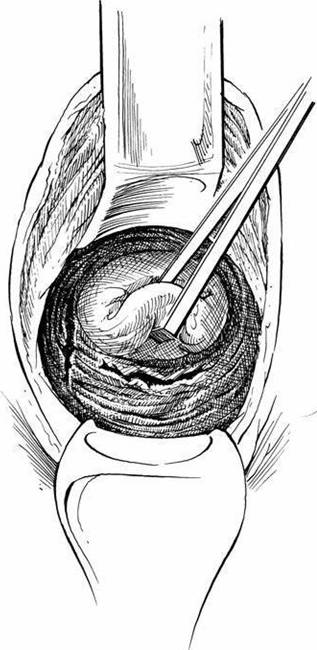
FIGURE 27.3 Laceration
of lateral and posterior vaginal fornices.
vaginal perforations (12). Repair of the vaginal laceration is performed after the abdominal part of the procedure is completed. Closed suction drains should be used routinely (12). Antibiotics are appropriate in all cases after cultures are obtained. Prophylaxis with tetanus toxoid should also be considered.
Complications from penetrating vaginal wounds include pelvic abscesses, vaginal strictures, and vesicovaginal and rectovaginal fistulas (12).Anal intercourse is a practice of the heterosexual as well as the homosexual communities. Various forms of trauma from this practice can present in women as well as men. Proctitis can occur and is generally the result of inflammation caused by trauma, but it may be due to chlamydia or herpes infection. Patients may have rectal bleeding from a rectal mucosal laceration. If a history of anal intercourse is obtained, then evaluation should include an upright abdominal film to rule out pneumoperitoneum and retained foreign body. Proctoscopy is then performed to determine the extent of the lesion. Most patients require no treatment, although transanal repair is occasionally necessary. Stool softeners and sitz baths are recommended. If disruption of the anal sphincter occurs from this form of sexual activity, repair should be done in the operating room. Occasionally, a patient is seen at the ED reporting loss of a sexual aid used in anal-rectal stimulation. Most foreign objects can be removed in the ED with appropriate instruments. Occasionally, general anesthesia is necessary to promote relaxation and patient comfort (10). If a vacuum has been created, passage of a Foley catheter around the object can break the seal (Fig. 27.4). The inflated bulb of the Foley can then help provide traction downward (4). If the object is beyond reach, the patient may be observed for 24 hours. The object will generally descend into the rectum within that time. Sigmoidoscopy should be performed after removal to rule out significant lacerations. If none are found and there are no signs of peritonitis, the patient can be discharged with close follow-up. Rectosigmoid colon perforations are rare but can be caused by foreign body manipulation. Peritonitis is generally the result. Attempts should be made to make the diagnosis without the use of barium enemas or Gastrografin enemas, because these enemas increase irritation and can increase bowel content spillage (4).
A diversionary colostomy is necessary at the time of repair to allow the laceration to heal. Generous irrigation and broad-spectrum antimicrobial coverage are indicated. Perforations occurring below the peritoneal reflection do not cause peritonitis, thus possibly delaying their presentation and diagnosis (4). Treatment, however, is the same.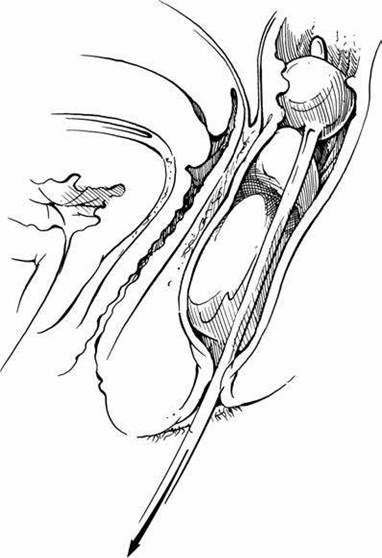
FIGURE 27.4 Foley catheter removal of intrarectal foreign body.
Nonsexually related trauma
Many mechanical causes of vaginal lacerations have been reported, which are not always related to sexual stimulation. Tampons with plastic applicators have been incriminated (14). Patients can have acute bright-red bleeding or a several- week history of bleeding (14). Examination generally shows a linear lesion through the full thickness of the vaginal mucosa. Lesions tend to heal on their own with an extended absence of tampons in the vagina.
Pressurized water entering the vagina can also cause laceration or rupture. Multiple case reports exist involving water skiing, Jet-Skis, and water fountains (13,15-19). The typical fall taken while water skiing is backward with legs abducted. Thus, the speed at impact dictates the amount of pressurized water that enters potential spaces such as the vagina and rectum (20). The pressurized water has been documented to cause significant lacerations with significant blood loss (14,20). Previously published literature led to the conclusion that only the width and relaxation of the parous vagina allowed the forceful entry ofwater. But Perlman et al. (17) reported on a similar injury in a premenarcheal 9-year-old female. The “Jet-Ski douche” is much less common but has also been reported (18,19). The injuries occur when the rider falls backward off the Jet-Ski with legs abducted. The high-pressure water jet from the Jet-Ski is the offender. Both of these types of “water douches” can cause significant lacerations, usually deep in the vagina around the cervix. The blood loss can cause significant anemia. Often, exploration under anesthesia is required to visualize and repair the defect after the patient’s condition has been stabilized. Because of the heavy bleeding, initial management in the field may include perineal pressure packs and antishock trousers. The use of antibiotics in these patients is unclear. There is the potential for infection from vaginal bacteria, as well as the flora from the water. If antibiotics are not used pro- phylactically, then observation for a fever seems prudent. The douche can also cause less visible injuries to the cervix, uterus, and fallopian tubes, such as salpingitis, tubo-ovarian abscesses, and precipitation of a miscarriage (16).
Laparoscopy or laparotomy should be considered when uncertainty as to intraperitoneal injury is present.
More serious gynecologic injuries are seen in automobile accident victims with pelvic fractures. Pelvic fractures in females can be associated with significant intra-abdominal gynecologic injury (21). Intra-abdominal soft tissue injuries are generally caused by tears and lacerations from sharp, bony fragments. Lacerations have been seen in the intestines and genitourinary tract, including the vagina and urethra (21,22). There have been reported cases of laceration to the uterus, tube, and ovary after a pelvic fracture as well as avulsion of the uterus (21,23). Retroperitoneal hematoma may result from such injuries (21). Avulsion of the uterus may result in hysterectomy (23). Infertility and obstetric complications are potential consequences of pelvic fractures as well as vaginal stricture, dyspareunia, osteomyelitis, and pelvic abscess (24). A gentle pelvic examination is warranted in women with pelvic fractures (21). The gentleness is emphasized, because the physician could create an open fracture through the vaginal wall. Delay in identifying lacerations could result in pelvic abscesses and higher rates of mortality. Once an abscess occurs, multiple operations are often necessary before complete cure is achieved (24). Future complications after the apparent resolution of abscesses include urethrovaginal fistula, vesicovaginal fistula, and rectovaginal fistula (24). Sudden bladder rupture has been reported as a result of osteomyelitis (24).
Mechanisms by which pelvic fractures cause vaginal lacerations are multiple. Most obvious is penetration of a bone fragment through the vaginal wall (24). Diastasis of the symphysis pubis tends to result from straddle injuries (24). The lateral tearing force of this injury lacerates deep pelvic soft tissues and sometimes extends to the vaginal wall. Bilateral ischiopubic rami fractures result in the anterior pelvic ring being freed from the weight-bearing portions of the pelvis. This can cause an avulsion of the vaginal vault or urethra (22). Finally, crushing injuries are capable of producing vaginal wall lacerations. Foreign bodies such as tampons and contraceptive devices can increase the chances of a vaginal laceration (24). Urethral and bladder neck injuries occur in about 6% of females with a pelvic fracture (25-32). These patients present with either blood at the introitus or gross hematuria. The physician should have a high suspicion of urethral or bladder neck injury in any female patient presenting with this combination of findings.
Niemi and Norton (24) recommend repair of vaginal lacerations as early as possible. A severely comminuted open pelvic fracture with associated rectal injuries and fecal contamination requires a diverting colostomy to allow the best chance of healing (24). Urethral avulsions have been reported to heal after primary end-to-end reanastomosis (22). Intravenous antibiotics are always indicated with an open fracture.
In one study of 102 major pelvic fractures, the mortality rate was 16%. The researchers suggested that the most significant determinant of mortality was the life-threatening injuries, along with the hemorrhage from lacerated pelvic vessels. Promptly recognizing and treating injuries to the bowel or bladder are also impor tant (24).
Rarely, one finds gynecologic injury after blunt abdominal trauma unassociated with pelvic fracture. Stone et al. (25), in their study of 220 patients with blunt abdominal trauma, found that the most frequent gynecologic injury was a ruptured and bleeding corpus luteum. The ovarian laceration can be simply oversewn, thus preserving the ovary. Also, vaginal evisceration following a simple slip and fall has been reported (31). This particular case occurred in a patient with long-standing procidentia and hypoestrogenemia even without a history of surgery. Wide-spectrum antibiotics should be used and preservation of the bowel in a moist saline wrap should be done while awaiting arrival in the OR. A vaginal approach to repair is reasonable as long as there are no signs of intra-abdominal injury or bowel incarceration.
Vulvar injuries and hematomas are another major area of gynecologic trauma. Injuries to the vulva and perineum of young girls are fairly common. Often, these injuries consist of slight tears that heal on their own. However, more severe cases, including urinary retention from vulvar injury following straddling the bar on a boy’s bike or other toy, have been reported (26). Even a small mucosal tear of the vulva or vestibule can cause intense pain or burning on urination so that the child inhibits voiding. This cause should be considered in young girls with urinary retention. They often will not volunteer information about the injury, so the diagnosis may not be made unless there is a high level of suspicion. Applying lidocaine gel to the tear with each urge to void, as well as voiding in a tub of warm water, is helpful and may prevent the need for catheterization.
Vulvar hematomas from trauma are seen in both young girls and women (Fig. 27.5). Naumann et al. reported two cases of vulvar hematoma that occurred while riding a “mechanical bull,” although such injury can result from any blunt trauma (27-29). Both women experienced abrupt pain and bleeding. One woman had a small hematoma merely treated with ice packs as an outpatient. The second woman had a large vulvar hematoma, producing urethral obstruction that required a Foley catheter for 7 days. She initially had a significant decrease in her hematocrit, which stabilized after 24 hours of conservative management with ice packs and observation. The ice pack is the primary treatment, with surgical evacuation reserved for rapidly enlarging hematomas or drainage of large hematomas following clot lysis (27-29). It is important to make the correct diagnosis,

FIGURE 27.5 Vulvarhematoma.
because evacuation in the first 24 hours could decompress the bleeding vessel, resulting in further blood loss. However, as discussed earlier, an infected vulvar hematoma must be incised, drained, and debrided as soon as possible. The bleeding site in this case must be localized quickly and ligated.
The final topic is iatrogenic gynecologic trauma. One reported case is of bilateral vaginal tears causing the loss of approximately 1,000 mL of blood from a routine speculum examination in a patient with vaginismus (30). No gross vaginal abnormality was apparent. The patient had to be taken to the operating room for repair and was transfused with 2 units of blood.
SUMMARY
Genital trauma in women can have multiple etiologies. Accurate information obtained from a cooperative patient is imperative to guarantee proper management. Compassion and nonjudgmental manner are therefore all-important in ensuring that the appropriate management is rendered.
References
1. Claytor RN, Bath KL, Shubin CI. Evaluating child sexual abuse, observations regarding ano-genital injury. Clin Pediatr. 1989;28:9.
2. Suram D. Child sexual abuse: relationship between sexual acts and genital findings. Child Abuse Negl. 1989;13:211.
3. Slaughter L, Brown CRY. Cervical findings in rape victims. Am J Obstet Gynecol. 1991;154:528.
4. Elam AL, Ray VG. Sexually related trauma: a review. Ann Emerg Med. 1986;15:576.
5. Christiansen WC, Danzl DF, McGee HJ. Pneumoperitoneum following vaginal insufflation and coitus. Ann Emerg Med. 1980;9:480.
6. Smith NC, Van Coeverden De Groot HA, Gunston DK. Coital injuries of the vagina in nonvirginal patients. S Afr MedJ. 1983;64:746.
7. Parakevaides EC. Severe post-coital puerperal vaginal tear. Br J Gun Pract. 1990;44:777.
8. Cullins V, AnastiJ, Huggins GR. Vaginal evisceration with pneumoperitoneum, a case report. J ReprodMed. 1989;34:426.
9. Metsala P, Nieminen U. Traumatic lesions of the vagina. Acta Obstet Gynecol Scand. 1986;47:482.
10. Cummings PH, Cummings SP. Foreign object-induced sexual trauma. JEmerg Nurs. 1981;7:24.
11. Mathelier AC. Vulvar hematoma secondary to a human bite: a case report. J Reprod Med. 1987;32:618.
12. Grindlinger GA, Vester SR. Transvaginal injury of the duodenum, diaphragm and lung.JTraama. 1987;27:575.
13. Druzin ML, Gottesfeld SA. Management of serious vaginal injury: a case report. J ReprodMed. 1986;31:151.
14. Gray MJ, Norton P, Treadwell K. Tampon-induced injuries. Obstet Gynecol. 1981;58:667.
15. Gray HR. A risk of waterskiing for women: a letter to the editor. West J Med. 1982;136:169.
16. Kizer KW. Medical hazards of the water skiing douche, a case report. Ann Emerg Med. 1980;9:268.
17. Perlman S, Hertweck SP, Wolfe, WM. Water-ski douche injury in a premenarcheal female, a case report. MD Consult.1995;96:783.
18. Ramos JP, Cari-ison D, Phillips DL. Unusual vaginal laceration due to high-pressure water jet, a case report. WestJMed. 1998;169:171.
19. Haefner IlK, Andersen HF,Johnson MP. Vaginal laceration following a jet ski accident. Obstet Gynecol. 1991;78:986.
20. Kalaichandran S. Vaginal laceration: a little-known hazard for women water skiers: a letter to the editor. Can J Surg. 1991;34:107.
21. Doman AN, Hoekstra DV. Pelvic fracture associated with severe intra-abdominal gynecologic injury. J Trauma. 1988;28:118.
22. Netto NR, Ikari O, Zuppo VP. Traumatic rupture of the female urethra, case reports. Urology. 1983;22:601.
23. Smith RJ. Avulsion of the nongravid uterus due to pelvic fracture, a case report. South MedJ. 1989;82:70.
24. Niemi TA, Norton LW. Vaginal injuries in patient with pelvic fractures. J Trauma. 1985;25:547.
25. Stone NN, Ances IG, Brotman S. Gynecologic injury in the non-gravid female during blunt abdominal trauma. J Trauma. 1984;24:6226.
26. Manaker JS. Gynecologic trauma, non-obstetrical vulvar, urethral, and vaginal injuries. JKans Med Soc. 1980;81:329.
27. Naumann RO, Droegmueller W. Unusual etiology of vulvar hematomas, a communications in brief. Am J Obstet Gynecol. 1982;142:357.
28. Shesser R, Shulinan D, Smith J. A nonpuerperal traumatic vulvar hematoma, a case report. J Reprod Med. 1987;32:618.
29. Vermesh M, Deppe G, Zbella E. Non-puerperal traumatic vulvar hematoma, a case report. J Gynaecol Obstet. 1984;22:217.
30. Rafla N. Vaginismus and vaginal tears, a case report. Am J Obstet Gynecol. 1988;158:1043.
31. Bozkurt N, Korucuoglu U, Bakirci Y, Yilmaz U, Sakrak O, Guner H. Vaginal eviseratio after trauma unrelated to previous pelvic surgery. Arch Gynecol Obstet. 2009 Apr; 279(4):595-597.
32. Black PC, Miller EA, Porter JR, Wessells H. Urethral and bladder neck injury associated with pelvic fracture in 25 female patients. J Urol. 2006;175(6):2140-2144.