Imaging in Gynecologic Emergencies
Marcia E. Murakami and Joseph G. Cernigliaro
Ultrasound is the most useful imaging modality in the evaluation of gynecologic emergencies. Moreover, ultrasound does not pose the risk of ionizing radiation, which is a consideration when examining the potentially pregnant patient.
Transvaginal imaging, in particular, permits exquisitely detailed examination of the uterus and ovaries, so that a specific diagnosis can often be made with great confidence. Plain radiographs are rarely useful as the initial screening study. Computed tomography (CT), in selected cases, can provide more global information for extensive disease, especially when the pathologic process extends out of the pelvis.Although some authors think that transvaginal scanning (TVS) alone is sufficient for defining pelvic pathology (1,2), it is our view that transabdominal scanning (TAS) should be performed first. For patients who are suspected of having an emergent gynecologic problem, the sonographer quickly scans the upper abdomen to exclude free intraperitoneal fluid, which is highly suspicious for hemoperitoneum in this patient population. Scanning through the urinary bladder affords a wide field of view and a survey of the entire pelvis. Although the diagnosis often can be made using TAS alone (Fig. 28.1), TVS almost always follows to better characterize the transabdominal findings (Fig. 28.2). The trans- vaginal examination is therefore directed and performed with the confidence that pathology is not outside the limited field of view of the transvaginal probe. Other authors suggest that TVS may be performed first, with addition of TAS as needed (3-5).
THE PREGNANT PATIENT
The development of an accurate and rapid pregnancy test has narrowed the differential diagnosis of otherwise nonspecific clinical findings. Still, the list of diagnostic possibilities in the early stages of pregnancy remains long and includes intrauterine pregnancy (IUP), ectopic pregnancy, embryonic or fetal demise with missed or incomplete abortion, completed abortion, and molar pregnancy.
Ultrasound can make a specific diagnosis in a number of cases or at least aid in the clinical management of the patient. Establishing the presence of a normal IUP essentially excludes an ectopic pregnancy. Evaluation of the gestational sac and its contents can often confirm embryonic demise. Often, correlation of the ultrasound findings with the clinical history may strongly suggest incomplete or completed abortion.Normal Early IUP
At the time of implantation, between day 20 and day 23 (menstrual age), the conceptus is only about 0.1 mm in diameter (6), much too small to be detected by transabdominal or transvaginal probes. Focal echogenic thickening of the endometrium can be visualized at the implantation site between 25 and 29 days. The earliest that a sac may be seen within the uterus is at 3.5 weeks, as a tiny anechoic fluid collection within the thickened decidua, termed the
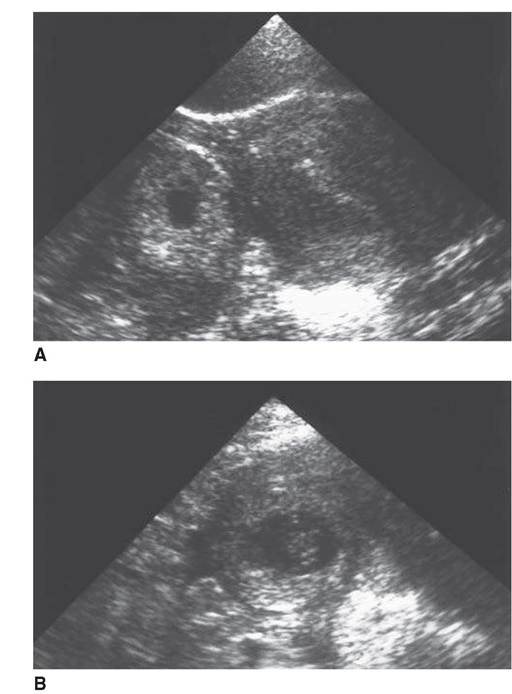
FIGURE 28.1 Value of transabdominal technique. A: Transverse scan through the fundus of the uterus shows echogenic ring in the right adnexal region. Uterus empty. B: High-resolution image of the right adnexa shows embryonic pole. Cardiac activity was observed, diagnostic of a living pregnancy. TVS, even with knowledge of the transabdominal findings, could not visualize the ectopic pregnancy.
intradecidual sign (Fig. 28.3) (7). More commonly, an early gestational sac is reliably detected at approximately 4.5 weeks’ menstrual age by TVS and at 5 weeks’ menstrual age by TAS (8). Correlation with serum human chorionic gonadotropin (hCG) levels is extremely helpful. Sac detection discriminatory levels of 1,800IU/L (Second International Standard [2nd IS]) or approximately 3,600 IU/L (International Reference Preparation [IRP]) TAS (9-11) and 1,000IU∕L (2nd IS) or about 2,000IU∕L (IRP) TVS (10,11) have been established. (The 2nd IS is approximately half the IRP value.) At these levels or higher, a definite intrauterine gestational sac should be visualized.
Below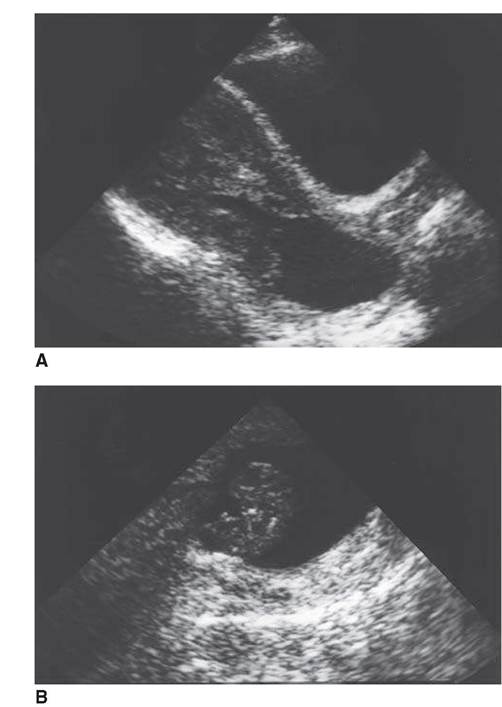
FIGURE 28.2 Value of transvaginal technique. A: Large, irregular fluid collection expands the cervix and the lower endometrial cavity. B: Transvaginal imaging detected an embryo without cardiac activity within the fluid collection, indicating embryonic demise and abortion in progress.
these levels, a normal intrauterine gestation may be too small to detect. If the hCG level is disproportionately low relative to the gestational sac size, an abnormal pregnancy should be suspected (9). In general, the intrauterine findings of an early pregnancy are visualized on TVS approximately 1 week earlier than on TAS (12).
The double decidual sac sign (13) may be the earliest confirmatory sign of an IUP on TAS or TVS (Fig. 28.4) (14,15). Although a definite double decidual sac sign is not identified in all normal IUPs, when this sign is clearly present, it is a very useful indicator of IUP (16). It is based on the visualization of the chorionic cavity
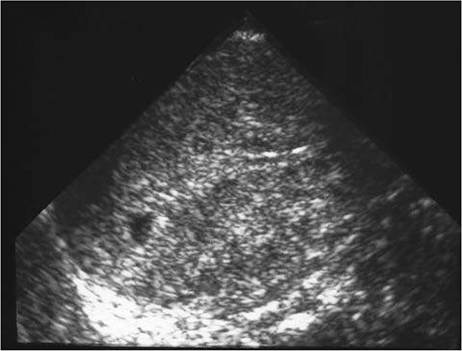
FIGURE 28.3 Intradecidual sign. The very small eccentric fluid collection within the decidua represents a very early (<4-week) IUP.

FIGURE 28.4 Double decidual sac sign. Decidua capsularis and chorion (arrowheads) and decidua parietalis (arrows) form the two arcs of the double decidual sac in a 5.2-week gestation. The yolk sac is clearly visible.
surrounded by two layers of echoes, the inner echogenic ring representing the decidua capsularis and chorion and the outer echogenic ring, the decidua parietalis. The combination of the gestational sac plus the decidual layers forms a much larger complex than the chorionic cavity itself and may be more readily identified at an earlier stage.
Normally, the yolk sac is the first structure seen within the gestational sac (Fig.
28.5). It should always be visualized with a mean sac diameter (MSD) of 20-mm TAS (17) and 8-mm TVS (18). (The MSD is calculated by dividing the sum of the three orthogonal dimensions of the fluid sac by three.) Whereas the double decidual sac sign is not absolutely specific for an intrauterine gestation, the presence of a yolk sac is definitive (14). Between 5 and 10 menstrual weeks, a yolk sac should never exceed 5.6 mm in diameter (19). As early as 5.5 weeks, a second sac may be seen adjacent to the yolk sac. This second sac represents the amnion, and this, together with the yolk sac, forms the double bleb sign (20). The embryonic disc lies between the two sacs. The amnion continues to grow and eventually fills the chorionic cavity by weeks 14 to 16. Normally, the amnion may be seen as a separate membrane until this time (Fig. 28.6).Once a yolk sac is visualized within the gestational sac, a search should be made for an embryo immediately adjacent to the yolk sac (Fig. 28.7). Transabdomi- nally, pulsation of the embryonic heart may be identified at real time, establishing a
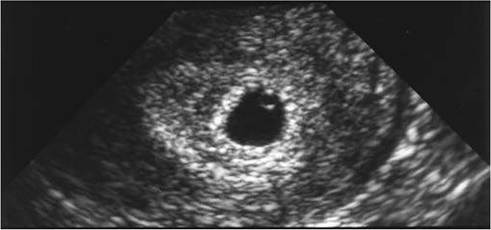
FIGURE 28.5 Yolk sac. Perfectly spherical, thin-walled yolk sac is noted in the periphery of the gestational sac. The 10-mm MSD corresponds to a 5-week gestation. Note the double decidual sac sign.

FIGURE 28.6 Yolk sac and amnion. The delicate amniotic sac envelops an 8-week embryo. The amnion has not yet fused with the chorion. Note the yolk sac adjacent to the embryo.

FIGURE 28.7 Embryo. Gestation of 5.5 weeks (13-mm MSD) with yolk sac and adjacent embryo. Cardiac activity was present.

FIGURE 28.8 Subchorionic hemorrhage.
A 9.5-week living IUP in a patient who was first seen with acute vaginal bleeding. Hemorrhage is more echogenic than the fluid within the gestational sac.live pregnancy, even though a distinct embryo is not visible (21). An embryo should always be visualized with an MSD of 25-mm TAS (9) and 16-mm TVS (10). An embryo is consistently detected transabdominally once it has reached a crown-rump length ≥5mm. Cardiac activity is often visible transvaginally in embryos with a crownrump length of 2 to 4mm (about 6 weeks). However, TVS can identify normal embryos without cardiac activity when they are <5 mm (22). The absence of cardiac activity in these small embryos should not be construed as embryonic demise.
Subchorionic hemorrhage is a common finding late in the first trimester and may be associated with vaginal bleeding. The hemorrhage causes elevation of the chorionic membrane, appearing acutely as a fluid collection more echogenic than amniotic fluid (Fig. 28.8), becoming more hypoechoic in 1 to 2 weeks. The significance of these hematomas is somewhat controversial. Some researchers believe that the prognosis depends on the volume of the hemorrhage, with a better prognosis associated with the smaller hematomas. Others suggest that the vast majority of pregnancies with subchorionic hemorrhage detected before 20 menstrual weeks end in a normal term delivery (23).
Corpus luteum cysts are commonly detected in the first trimester. The cysts may be simple or hemorrhagic (Fig. 28.9). They are usually 3 to 6 cm in size but may be as large as 10 cm. These cysts usually resolve spontaneously by 16 weeks.
Abnormal Early IUP
Ultrasound has proved to be extremely helpful in the evaluation of the failed pregnancy. With TVS, a single examination is often conclusive in establishing embryonic demise. A large gestation sac (MSD, >25-mm TAS [9] or >16-mm TVS [10] without an embryo; MSD, >20-mm TAS [9] or >8-mm TVS [10] without a yolk sac) is diagnostic of an anembryonic gestation or blighted ovum (Fig.
28.10). Distorted gestational sac shape is also highly specific for abnormal pregnancy, although it is a somewhat subjective feature and is relatively insensitive. Suggestive but less specific findings include a thin (<2 mm), weakly echogenic or irregular choriodecidual reaction, absent double decidual sac sign, and low position of the sac within the endometrial cavity (9).The yolk sac itself should not measure >5.6 mm in diameter between 5 and 10 weeks or ≤2 mm between 8 and 12 weeks (19). If a normal embryo cannot be identified adjacent to an abnormally large yolk sac, the diagnosis of blighted ovum or anembryonic pregnancy is made (Fig. 28.11). Conversely, it is also abnormal if a yolk sac is not visualized in the presence of an embryo demonstrated by TVS (8). This is associated with embryonic demise either at the time of the scan or on follow-up examination. Calcification of the yolk sac is also seen with embryonic demise (Fig. 28.12) (24). Just as a gestational sac too large for its contents is abnormal, a gestational sac too small also carries a poor prognosis (Fig. 28.13). Despite the presence of cardiac activity within embryos between 6

FIGURE 28.9 Hemorrhagic corpus luteum cyst. Transvaginal image shows a 4-cm complex mass arising from the ovary compatible with a hemorrhagic cyst. Note adjacent uterus and small amount of simple free fluid.

FIGURE 28.10 Blighted ovum: empty gestational sac. No embryo is visualized and decidual reaction is weak.
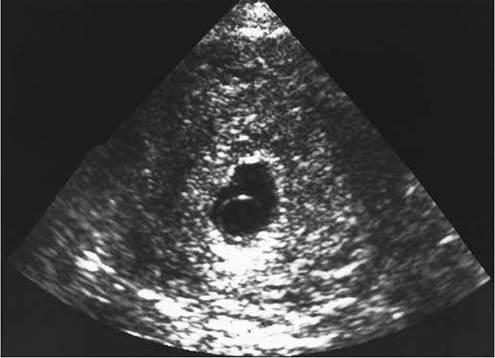
FIGURE 28.11 Blighted ovum: abnormally large yolk sac. A 9-mm yolk sac occupies about one half the volume of the gestational sac. No embryonic pole could be detected.
and 9 weeks, those with a gestational sac size too small for the crown-rump length almost always end in miscarriage (25). Therefore, management of these pregnancies should be cautious.
Cardiac activity establishes embryonic life. In a high-quality TAS, once an embryo is visualized, cardiac activity should always be present (Fig. 28.14). Transvaginally, however, a normal embryo <5 mm in crown-rump length may or
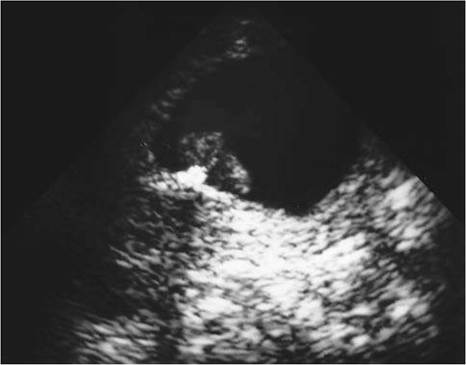
FIGURE 28.12 Embryonic demise: calcification of the yolk sac. Densely echogenic structure with shadowing is presumed to be calcified yolk sac immediately adjacent to the embryo. No cardiac activity was visualized.

FIGURE 28.13 Embryonic demise: missed abortion. An 8.2-week embryo is too large for the gestational sac size, which corresponds to a 6.7-week gestation. Cardiac activity was not present.
may not exhibit cardiac activity, and follow-up sonography may be of benefit to establish normal development (22).
Embryonic bradycardia is also a sign of impending fetal demise. The normal embryonic heart rate at 5 to 6 menstrual weeks is approximately 100 bpm. At 8 to 9 menstrual weeks, the rate is approximately 140 bpm. It has been demonstrated
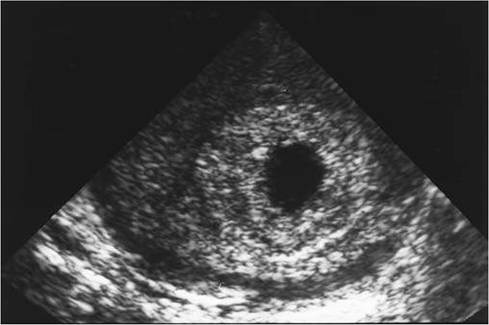
FIGURE 28.14 Incomplete abortion. Intrauterine fluid and markedly thickened endometrium. No yolk sac or embryo is detected.
that embryos between 5 and 8 weeks of menstrual age with heart rates of <85 bpm end in fetal loss (26).
Retained products of conception from an incomplete abortion are quite variable in appearance and are often difficult to differentiate from a pseudoges- tational sac or decidual cast of an ectopic pregnancy. The endometrium may appear abnormally thick (>5 mm), with fluid and debris within the uterine cavity (Fig. 28.14). If the endometrial stripe is thin (<2 mm), there is little likelihood of retained products (27).
At times, an abortion in progress can be observed at real-time ultrasound. The uterine contents move lower in the uterus toward the cervix with active contraction of the uterus, and the cervical canal may be fluid filled and dilated (Fig. 28.2). A completed abortion is often identical in ultrasound appearance to a normal empty uterus. In the presence of a positive pregnancy test, the differential diagnosis must include very early IUP and nonvisualized ectopic pregnancy.
Early trophoblastic disease is usually indistinguishable from an incomplete abortion, demonstrating abnormal echogenicity within the uterine cavity. Hydropic villae may not develop vesicles until 12 weeks or more, making detection by even TVS difficult until that time (28).
Ectopic Pregnancy
The sine qua non for diagnosis of an ectopic pregnancy is the demonstration of an extrauterine embryo with cardiac activity (Fig. 28.15). TVS has increased the detection of live extrauterine embryos compared with TAS (29,30). Practically speaking, the presence of a normal intrauterine gestation excludes ectopic pregnancy. The likelihood of coexistent intrauterine and ectopic pregnancy, also known as heterotopic pregnancy, is variably estimated as 1 in 30,000 to 1 in 7,000 (16).
Apseudogestational sac or decidual cast must be differentiated from a very early IUP (13). The pseudogestational sac represents an intrauterine fluid collection surrounded by a single decidual layer rather than the concentric arcs of the

FIGURE 28.15 Ectopic pregnancy. An 8-week living ectopic pregnancy in the cul-de-sac. Note the empty uterus and free fluid. Cardiac activity was present.
double decidual sac sign (Fig. 28.16). It may be impossible to distinguish a decidual cast from a spontaneous incomplete abortion (Fig. 28.17).
If an IUP is not identified in the patient who is suspected of having an ectopic pregnancy, the adnexal regions should be carefully examined. An adnexal mass is highly suspicious for ectopic pregnancy in this setting. The appearance of the mass is variable but is usually complex (Fig. 28.18). An ectopic tubal ring may be seen separate from the ovaries, a finding strongly associated with an unruptured tubal pregnancy (Fig. 28.19) (31,32). The ring is an echogenic structure created by the trophoblast of the ectopic pregnancy. If this ring is carefully examined, a yolk sac or embryo may be identified within it. Increased flow surrounding a tubal pregnancy on color Doppler or ring of fire is a nonspecific finding as a corpus luteum cyst may also have this appearance. This sign is probably most helpful when an ectopic pregnancy is not visualized but suspected and color Doppler is used as an adjunct to gray scale imaging to detect the extrauter- ine pregnancy separate from the ovary (33).
A search for free fluid should be made in the cul-de-sac, over the fundus of the uterus (34), in both paracolic gutters, in the hepatorenal space, and about the spleen (Fig. 28.20). The fluid of hemoperitoneum is often echogenic. The presence of even relatively small amounts of echogenic fluid should alert the examiner to the strong possibility of an ectopic pregnancy, despite the absence of other abnormal findings (35). Small amounts of free, simple, nonechogenic fluid can be normal and do not necessarily indicate hemoperitoneum.
Interstitial or cornual pregnancies are suggested by the eccentric location of the gestational sac within the fundal region of the uterine cavity (Fig. 28.21). The myometrium surrounding the sac may be thin or incomplete, with the gestational sac within 5mm of the uterine serosa (31,36). The interstitial line sign, a thin echogenic line from the endometrial canal to the cornual sac, is a more sensitive and specific finding (37). A high degree of clinical suspicion should be maintained because these pregnancies tend to rupture later than other tubal gestations, often with massive intraperitoneal hemorrhage.
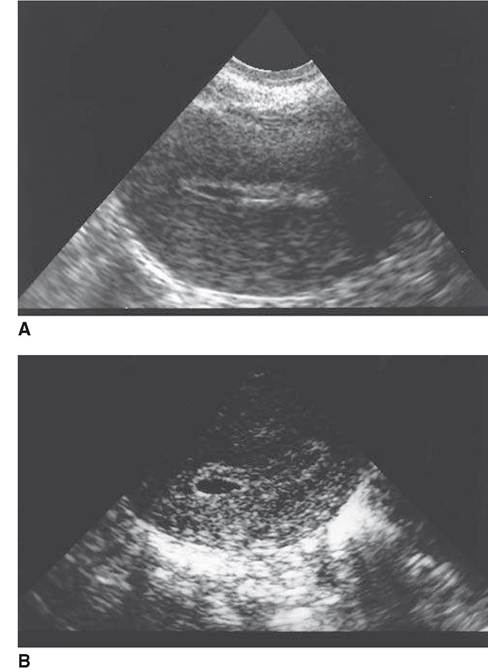
FIGURE 28.16 Pseudogestational sac versus early IUP. A: Small fluid collection within the uterus surrounded by a single echogenic layer in a patient with proven ectopic pregnancy. B: For comparison, a <5-week IUP with the double decidual sac sign.
Cervical pregnancies are extremely rare but must be distinguished from an abortion in progress. The gestational sac of a cervical implantation is expected to be round or oval, fixed in the cervical canal and may contain a yolk sac or embryo; a mobile, collapsed or crenated sac would suggest spontaneously aborting products of conception (38).
PELVIC INFLAMMATORY DISEASE
Pelvic inflammatory disease (PID) is a multimicrobial ascending infection of the female upper genital tract and adjacent pelvic spaces. Prompt recognition and treatment are needed to decrease long-term sequelae of chronic pain and inflammation, infertility secondary to adhesions, and increased risk of future ectopic pregnancy as a result of tubal scarring.
Once the diagnosis of PID is suspected, ultrasound is the study of choice in the emergent setting. The combination of TAS and TVS is able to detect and evaluate the complications of PID. The ultrasound findings of PID will vary based on the degree, duration, and distribution of the disease. In mild cases, the ultrasound may be normal.
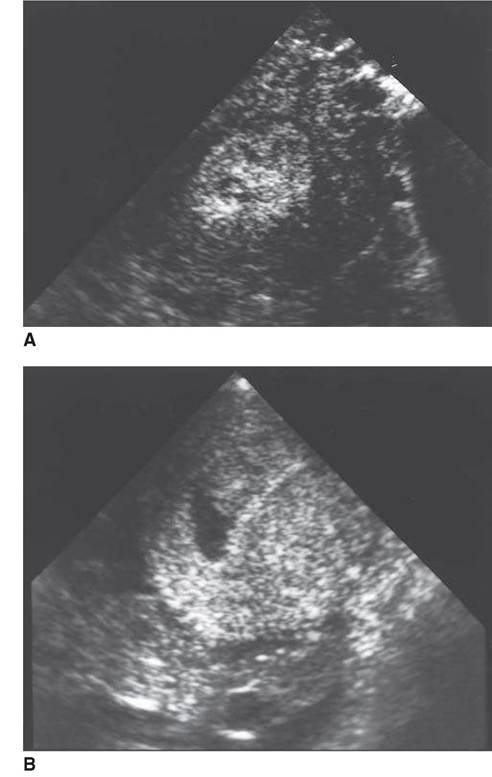
FIGURE 28.17 Decidual cast of ectopic pregnancy versus spontaneous incomplete abortion. Four different patients. A, B: Decidual cast of ectopic pregnancy. (continued)
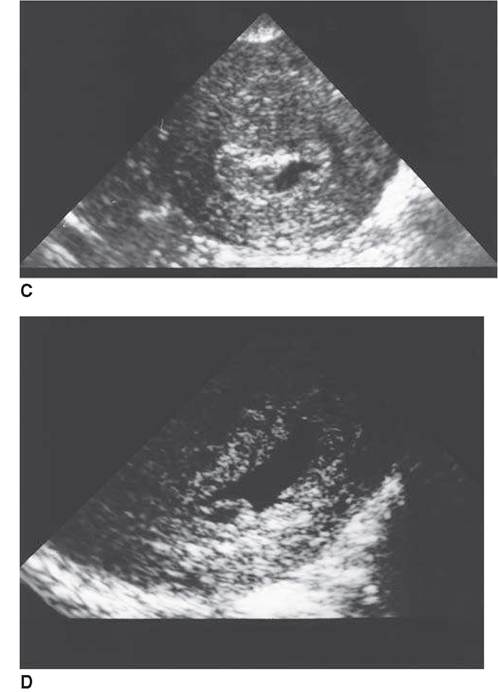
FIGURE 28.17 (Continued) C, D: Incomplete abortion. The nonspecificity of the intrauterine findings is quite evident.
Endometritis
Cases of endometritis are more common after iatrogenic intervention (e.g., cesarean section and dilatation and curettage). Ultrasound findings include endometrial thickening of >12mm, increased or decreased echotexture of the endometrium with poor definition of its interface with the myometrium, fluid in the endometrial canal, and a poorly defined uterine margin resulting from pelvic exudate or adhesions (39).
Salpingitis and Tubo-ovarian Abscess
It is uncommon to identify thin, tortuous, normal-sized fallopian tubes. Tubes can be seen when they are filled with or surrounded by fluid. In acute PID, the tubes can be filled with purulent material or blood (pyosalpinx [Fig. 28.22] or

FIGURE 28.18 Ectopic pregnancy: nonspecific adnexal mass. Transverse image shows a large, complex, predominantly solid mass in the left adnexa. The uterus contains a small amount of fluid. Left ectopic pregnancy was found at surgery.
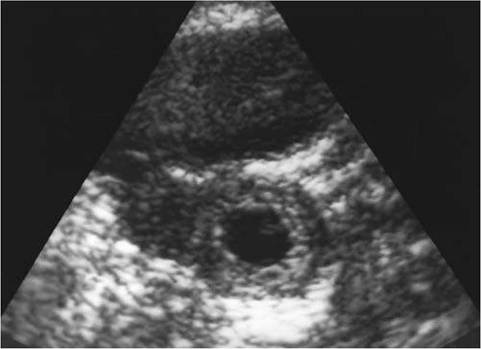
FIGURE 28.19 Tubal ring of ectopic pregnancy. Transvaginal image shows an echogenic ring <2 cm in diameter found to be a tubal pregnancy at surgery.
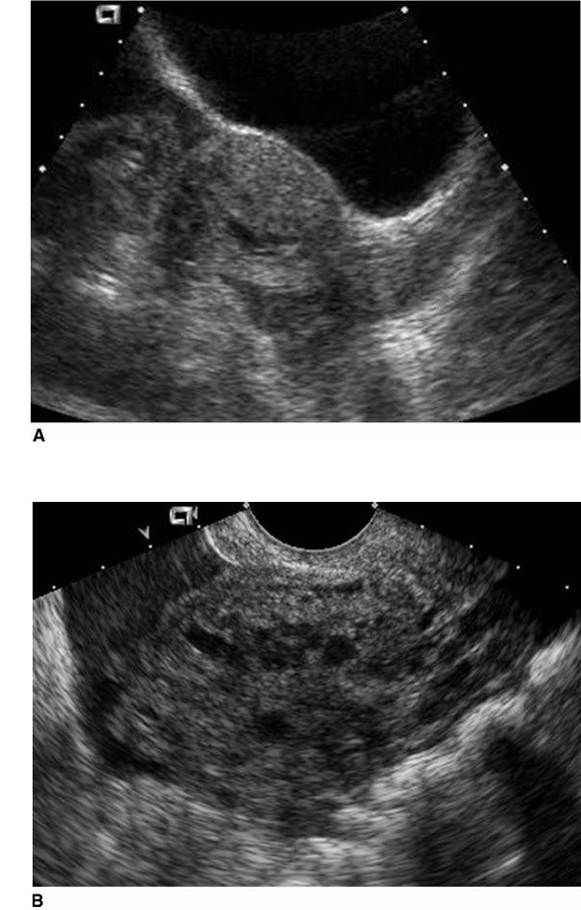
FIGURE 28.20 Hemoperitoneum. A: Sagittal scan shows echogenic fluid in the cul-de-sac and between the uterine fundus and the bladder. B: Echogenic fluid adjacent to adnexal mass in patient with proven ectopic pregnancy. (continued)
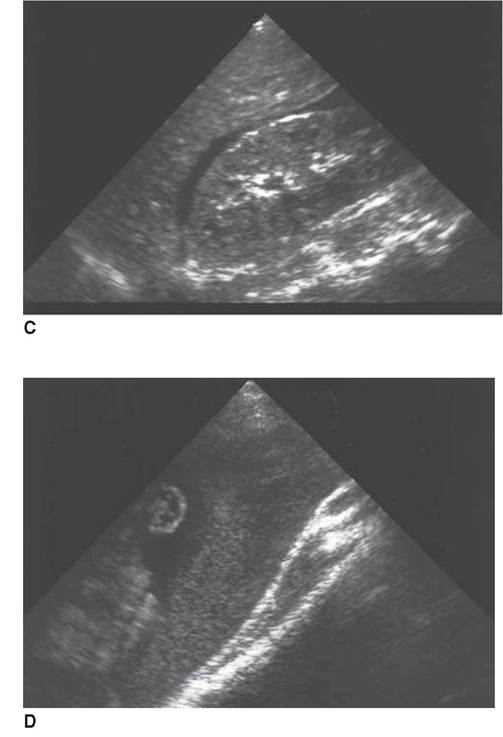
FIGURE 28.20 (Continued) C: Free fluid between the liver and the right kidney in Morison's pouch. D: Image of right iliac fossa shows bowel loops floating in echogenic fluid.
hematosalpinx). On ultrasound, one can recognize the enlarged tube as a serpiginous dilated continuous tubular structure with diffuse internal echoes, which sometimes layer. The process is often bilateral. On occasion, nodular excrescences representing salpingeal fold remnants can be seen (40). After treatment, and with time and proteolysis, the pyosalpinx/hematosalpinx can completely resolve or convert to a hydrosalpinx (Fig. 28.23), which is a dilated, water-filled tube. On ultrasound, this appears as a dilated anechoic tube with a well-defined wall. Color Doppler and real-time observation help to differentiate dilated tubes from dilated pelvic veins or peristalsing bowel.
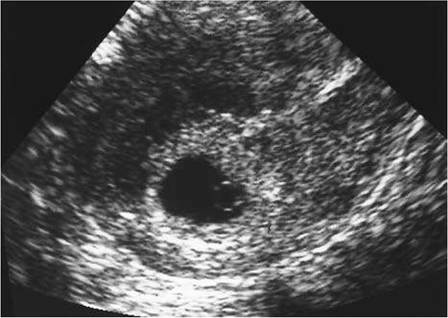
FIGURE 28.21 Interstitial ectopic pregnancy. A highly echogenic ring surrounding the gestational sac eccentrically located in the periphery of the fundal portion of the uterus. Myometrium extends incompletely about the ring and the endometrial echo points directly to the ring (interstitial line sign). Note the yolk sac within the gestational sac. (Courtesy of Maribel U. Lockwood)
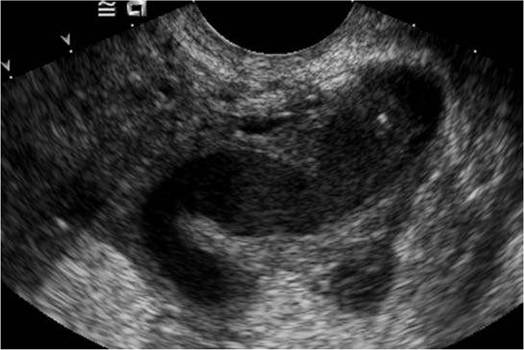
FIGURE 28.22 Pyosalpinx. Tubular adnexal structure containing low-level echoes immediately adjacent to the ovary.
Although the ovaries are relatively resistant to infection, oophoritis and tubo-ovarian abscesses (TOAs) do occur. Oophoritis is characterized on ultrasound as enlarged globular and multicystic ovaries. Leakage of purulent material results in pelvic inflammation and adhesions. Eventually, if the process is untreated or inadequately treated, the dilated tubes and enlarged cystic
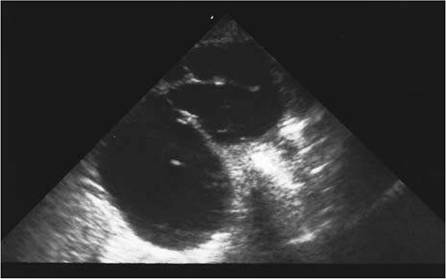
FIGURE 28.23. Hydrosalpinx. Anechoic tubular and tortuous structure in the adnexal region. Good through transmission of sound is indicative of its fluid content.

FIGURE 28.24 Tubo -ovarian abscess. Complex adnexal mass with solid and cystic components. The cystic components contain internal echoes consistent with pus. (Courtesy of Maribel U. Lockwood)
ovaries become a large indistinguishable mass known as a TOA (Fig. 28.24). These masses can have a variable ultrasound appearance ranging from nearly solid to unilocular or multilocular cystic lesions with or without thick walls or fluid-fluid levels. An echogenic focus with “dirty” posterior acoustical shadowing in the TOA represents gas. A TOA cannot be differentiated from a pelvic abscess of nongynecologic origin. Without clinical history, ovarian neoplasm, ectopic pregnancy, and endometriomas can also be confused with a TOA.
CT, although rarely used in initial evaluation, may be useful if there is a concern about an abscess of another source or a TOA poorly responsive to antibiotic therapy. These abscesses may require percutaneous or surgical drainage.
OVARIAN TORSION
Torsion of the ovary is seen most commonly in young women and girls with ovarian cysts, tumors, and other masses (41), but it may also be seen in patients with normal ovaries (42,43). Sonographic findings are nonspecific, but usually, an adnexal mass, either complex or predominantly cystic, can be demonstrated (Fig. 28.25). If the ovary is identified, it is enlarged and may have multiple
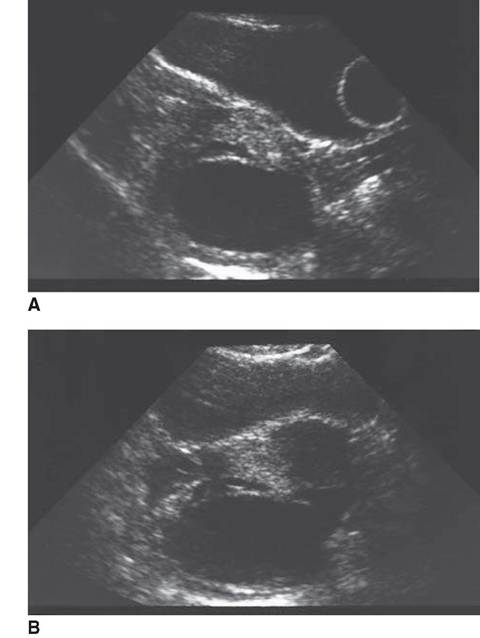
FIGURE 28.25 Ovarian torsion in a 15-year-old female. A: Longitudinal transabdominal scan. B: Transverse transabdominal scans. Complex, predominantly cystic mass within the cul-de-sac and slightly to the right. Note balloon of Foley catheter within the urinary bladder. At surgery, a 6-cm blue necrotic mass compatible with torsion was found in the cul-de-sac originating from the left adnexa.
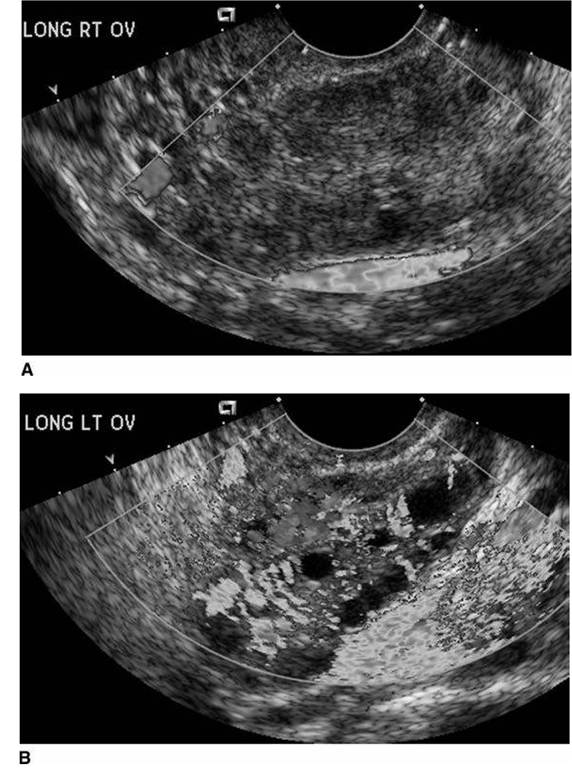
FIGURE 28.26 Right ovarian torsion. A: Color Doppler shows no flow within the right ovary. B: Compare color flow in normal left ovary. (Courtesy of Douglas L. Brown)
id="Picutre 138" class="lazyload" data-src="/files/uch_group75/uch_pgroup318/uch_uch7372/image/image137.jpg">
FIGURE 28.27 Whirlpool sign of ovarian torsion. A: Adnexal mass. (continued)
prominent peripheral follicles, presumably from transudation of fluid from vascular congestion (44). Color Doppler may be useful if no flow is detected within the torsed ovary (Fig. 28.26) or if the whirlpool sign, a swirl of vessels in the adnexal region, is present (Fig. 28.27) (45). However, vascular flow, both arterial and venous, can be detected in ovarian torsion due to the dual arterial blood supply to the ovary. This must be kept in mind when considering this diagnosis (46).

FIGURE 28.27 (Continued) B: Color Doppler reveals swirling configuration of blood vessels in the mass. At surgery, ovarian pedicle was twisted 10 to 12 times.
RUPTURED OVARIAN CYST
A patient with a ruptured cyst may have extreme pain, clinically similar to torsion. The collapsed cyst may or may not be visualized on ultrasound examination. Hemoperitoneum, identical in appearance to that from a ruptured ectopic pregnancy, can be present (47).
REFERENCES
1. Dashefsky SM, Lyons EA, Levi CS, Lindsay DJ. Suspected ectopic pregnancy: endovaginal and transvesical. Radiology. 1988;169:181-184.
2. Tessler FN, Schiller VL, Perrella RR, Sutherland ML, Grant EG. Transabdominal versus endovaginal pelvic sonography: prospective study. Radiology. 1989;170:553-556.
3. Mendelson EB, Bohm-Velez M, Joseph N, Neiman HL. Gynecologic imaging: comparison of transabdominal and transvaginal sonography. Radiology. 1988;166:321-324.
4. Lande IM, Hill MC, Cosco FE, Kator NN. Adnexal cul-de-sac abnormalities: transvaginal sonography. Radiology. 1988;166:325-332.
5. Coleman BG, Arger PH, Grumback K, et al. Transvaginal and transabdominal sonography: prospective comparison. Radiology. 1988;168:639-643.
6. Moore KL. The beginning of development: the first week. In: Moore KL, ed. The Developing Human: Clinically Oriented Embryology. 4th Ed. Philadelphia, PA: WB Saunders; 1988:13-37.
7. Yeh H-C, GoodmanJD, Carr L, et al. Intradecidual sign: a ultrasound criterion of early intrauterine pregnancy. Radiology. 1986;161:463-467.
8. Levi CS, Lyons EA. The first trimester. In: Rumack CM, Wilson SR, Charboneau JW, eds. Diagnostic Ultrasound. St. Louis, MO: Elsevier Mosby; 2005:1076-1077.
9. Nyberg DA, Filly RA, Filho DLD, Laing FC, Mahony BS. Abnormal pregnancy: early diagnosis by US and serum chorionic gonadotropin levels. Radiology. 1986;158:393-396.
10. Nyberg DA, Mack LA, Laing FC, Jeffrey RB. Early pregnancy complications: endovaginal sonographic findings correlated with human chorionic gonadotropin levels. Radiology. 1988;167:619-622.
11. Levine D. Ectopic pregnancy. In: Callen PW, ed. Ultrasonography in Obstetrics and Gynecology. 5th Ed. Philadelphia, PA: Saunders Elsevier; 2008:1022-1024.
12. Bree RL, Edwards M, Bohm-Velez M, Beyler S, Robert J, Mendelson EB. Transvaginal sonography in the evaluation of normal early pregnancy: correlation with HCG level. Am J Roentgenol. 1989;153:75-79.
13. Nyberg DA, Laing FC, Filly RA, et al. Ultrasonographic differentiation of the gestational sac of early intrauterine pregnancy from the pseudogestational sac of ectopic pregnancy. Radiology. 1983;146:755-759.
14. Nyberg DA, Mack LA, Harvey D, Wang K. Value of the yolk sac in evaluating early pregnancies. J Ultrasound Med. 1988;7:129-135.
15. Jain KA, Hamper UM, Sanders RC. Comparison of transvaginal and transabdominal sonography in the detection of early pregnancy and its complications. Am J Roentgenol. 1988;151:1139-1143.
16. Filly RA. Ectopic pregnancy: the role of sonography. Radiology. 1987;162:661-668.
17. Nyberg DA, Laing FC, Filly RA. Threatened abortion: sonographic distinction of normal and abnormal gestation sacs. Radiology. 1986;158:397-400.
18. Levi CS, Lyons EA, Lindsay DJ. Early diagnosis of nonviable pregnancy with endovaginal US. Radiology. 1988;167:383-385.
19. Levi CS, Lyons EA, Lindsay DJ. Ultrasound in the first trimester of pregnancy. Radiol Clin North Am. 1990;28:19-38.
20. Yeh H-C, Rabinowitz JG. Amniotic sac development: ultrasound features of early pregnancy—the double bleb sign. Radiology. 1988;166:97-103.
21. Chadkin AV, McAlpin J. Detection of fetal cardiac activity between 41 and 43 days of gestation. J UltrasoundMed. 1984;3(11):499-503.
22. Levi CS, Lyons EA, Zheng XH, Lindsay DJ, Holt SC. Endovaginal US: demonstration of cardiac activity in embryos of less than 5.0 mm in crown-rump length. Radiology. 1990;176:71-74.
23. Laing FC, Frates MC, Benson CB. Ultrasound evaluation during the first trimester of pregnancy. In: Callen PW, ed. Ultrasonography in Obstetrics and Gynecology. 5th Ed. Philadelphia, PA: Saunders Elsevier; 2008:205-206.
24. Laing FC, Frates MC, Benson CB. Ultrasound evaluation during the first trimester of pregnancy. In: Callen PW, ed. Ultrasonography in Obstetrics and Gynecology. 5th Ed. Philadelphia, PA: Saunders Elsevier; 2008:208-209.
25. Bromley B, Harlow BL, Laboda LA, Benacerraf BR. Small sac size in the first trimester: a predictor of poor fetal outcome. Radiology. 1991;178:375-377.
26. Laboda LA, Estroff JA, Benacerraf BR. First trimester bradycardia: a sign of impending fetal loss. J Ultrasound Med. 1989;8:561-563.
27. Kurtz AB, Shlansky-Goldbert RD, Choi HY, Needleman L, Wapner RJ, Boldberg BB. Detection of retained products of conception following spontaneous abortion in the first trimester. J Ultrasound Med. 1991;10:387-395.
28. Woodward RM, Filly RA, Callen PW. First trimester molar pregnancy: non-specific ultrasonographic appearance. Obstet Gynecol. 1988;55:315.
29. Pennell RG, Baltarowich OH, Kurtz AB, et al. Complicated first-trimester pregnancies: evaluation with endovaginal US versus transabdominal technique. Radiology. 1987;165:79-83.
30. Thorsen MK, Lawson TL, Aiman EJ, et al. Diagnosis of ectopic pregnancy: endovaginal vs transabdominal sonography. Am J Roentgenol. 1990;155:307-310.
31. Fleischer AC, Pennell RG, McKee MS, et al. Ectopic pregnancy: features at transvagi- nal sonography. Radiology. 1990;174:375-378.
32. Cacciatore B. Can the status of tubal pregnancy be predicted with transvaginal sonography? A prospective comparison of sonographic, surgical, and serum HCG findings. Radiology. 1990;177:481-484.
33. Levine D. Ectopic pregnancy. Radiology. 2007;245(2):385-397.
34. Nyberg DA, Laing FC, Jeffrey RN. Sonographic detection of subtle pelvic fluid collections. Am J Roentgenol. 1984;143:261-263.
35. Nyberg DA, Hughes MP, Mack LA, Wang KY. Extrauterine findings of ectopic pregnancy at transvaginal US: importance of echogenic fluid. Radiology. 1991;178: 823-826.
36. Jafri SZH, Loginsky SJ, BouffardJA, Selis JE. Sonographic detection of interstitial pregnancy. JClin Ultrasound. 1987;15:253-257.
37. Ackerman TE, Levis CS, Dashefsky SM, et al. Interstitial line: sonographic finding in interstitial (cornual) ectopic pregnancy. Radiology. 1993;189:83-87.
38. Paspulati RM, Turgut AT, Bhatt S, Ergun E, Dogra V. Ultrasound assessment of premenopausal bleeding. Ultrasound Clin. 2008; 345-368.
39. Bowie JD. Ultrasound of gynecological pelvic masses: the indefinite uterus and other patterns associated with diagnostic errors. J Clin Ultrasound. 1977;5:323.
40. Abbitt HP. Ultrasound: A Pattern Approach. New York, NY: McGraw-Hill; 1995: 379-387.
41. Helvie MA, Silver TM. Ovarian torsion: sonographic evaluation. J Clin Ultrasound. 1989;17:327-332.
42. Han BK, Babcock DS. Ultrasonography of torsion of normal uterine adnexa. J Ultrasound Med. 1983;2:321-323.
43. Graif M, Itzchak Y. Sonographic evaluation of ovarian torsion in childhood and adolescence. Am J Roentgenol. 1988;150:647-649.
44. Graif M, Shalve J, Strauss S, Engelberg S, Mashiach S, Itzchak Y. Torsion of the ovary: sonographic features. Am J Roentgenol. 1984;143:1331-1334.
45. Vijayaraghavan SB. Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med. 2004;23:1643-1649.
46. Stein MW, Ricci ZJ, Novak L, Roberts JH, Koenigsberg M. Sonographic comparison of the tubal ring of ectopic pregnancy with the corpus luteum. J Ultrasound Med. 2004;23:57-62.
47. Salem S, Wilson SR. Gyneclogic ultrasound. In: Rumack CM, Wilson SR, Charboneau JW, eds. Diagnostic Ultrasound. St. Louis, MO: Elsevier Mosby; 2005:557-558.
Urogynecologic Emergencies
Bela I. Kudish and Cheryl B. Iglesia
While urologic emergencies related to gynecology are relatively rare and most are not life threatening, their management should be done in a logical and timely fashion.
URINARY TRACT INJURY FOLLOWING PELVIC SURGERY
Lower urinary tract injuries (bladder and ureter) accompany <2% of hysterectomies, with bladder injuries outnumbering ureteral injuries five to one (1). Ureteral injuries can result from devascularization, crushing, ligation, or transection and, most commonly, occur at the time of abdominal or laparoscopic hysterectomy (2). Although ureteral injury is a rare occurrence, many injuries are not recognized at the time of initial surgery and present as delayed complications with infection, hydronephrosis, urinoma with subsequent ileus, ureterovaginal fistulas, or silent kidney death. In cases of unilateral ureteral obstruction, patients may present with abdominal and flank pain, fever, and leukocytosis. An ultrasound or intravenous pyelogram showing a dilated renal collecting system will suggest the diagnosis, while cystoscopy with retrograde dye studies will confirm it. If the ureter has been transected, the patient can present with abdominal distention, nausea, vomiting, ileus, or clear vaginal discharge suggestive of a ureterovaginal fistula. Cystoscopy with retrograde ureteral stent placement, ureteroscopy, or percutaneous nephrostomy with antegrade stent placement aided by a fluoroscopic dye study will help localize the site of transection (3). Computed tomography with intravenous contrast material is helpful in assessing an intra-abdominal or retroperitoneal process that may be involved in extrinsic ureteral obstruction or compression. After localization of the ureteral leak or site of obstruction, placement of a percutaneous nephrostomy drainage or transvesical ureteral stenting allows for nonoperative diversion and salvage of the remaining renal function. Complete transections of the ureter require definitive repair (uretero- neocystostomy or bladder reimplantation of the ureter, ureteroureterostomy or end- to-end anastomosis, and bladder mobilization and extension). The choice of method is based on the location of the injured ureteral segment.
In cases when a urinary tract fistula is suspected, the emergency room (ER) provider can utilize the “tampon test” to aid in the diagnosis. This test can also help differentiate between a ureterovaginal and a vesicovaginal fistula. The bladder is filled with 250mL of indigo carmine-dyed water or saline, and the vagina is inspected for leakage. If no leakage is visualized but the suspicion of a fistula remains high, a tampon can be pla ced into the vagina, and the patient is then instructed to ambulate for a minimum of 15 to 30 minutes. Observation of the blue dye on the tampon suggests vesicovaginal fistula which can be confirmed with cystoscopy. The presence of nondyed urine in the vagina suggests ureterovaginal fistula. The appearance of a ureterovaginal fistula is usually preceded by a pyelitis, including history of fever spikes and unilateral costovertebral angle tenderness. Intravenous pyelogram and ureteroscopy are diagnostic.
Only physicians with expertise should repair complex ureterovaginal or ure- terovesicovaginal fistulas. Vesicovaginal fistulas are amenable to transvaginal repair, while ureterovesicovaginal fistulas require transabdominal or endoscopic surgery with ureteral reimplantation and omental graft superimposition (4). The role of the ER physician is to recognize the possible symptoms of ureteral injury in a patient who has undergone pelvic surgery which may include abdominal distention with ileus and urine ascites; fever, chills, and flank pain; oliguria, pyuria, or hematuria; pyelonephritis or a urinary tract infection not responding to appropriate antibiotics; and a ureterovaginal fistula with continuous vaginal discharge. Treatment for an underlying infection as well as appropriate and prompt urologic consultation is necessary to avoid further loss of kidney function.
URINARY RETENTION FOLLOWING UROGYNECOLOGIC PROCEDURES
While many pelvic surgeries can lead to acute or subacute urinary retention, urogynecologic procedures, in particular anti-incontinence operations, have the highest incidence of this complication. Patients with urinary retention typically present to the ER with complaints of incomplete bladder emptying, poor urinary stream, dribbling or lower abdominal pain, and bladder distention. These symptoms usually occur in the first few days after the surgery, even though the patient may have documented normal voiding trials and post-void residual volumes. The ER provider must recognize this condition and should attempt to decompress the bladder with a transurethral catheter. An expeditious bladder decompression is necessary to prevent over-distention injury to the bladder. Urinalysis and cultures should be obtained when indicated. In rare instances, such as in the case of an overcorrected repair, a transurethral catheter cannot be passed, and the urologic service should be consulted for cystourethroscopic evaluation and possible suprapubic catheter placement. Transurethral catheters should be placed with caution especially with those who have undergone primary urethral surgery. Medications such as ^-agonists and anticholinergics can aggravate urinary retention and should be discontinued when possible. In cases of mechanical obstruction, further surgical intervention to include urethrolysis or revision of a suburethral sling may be indicated. Patients with incomplete bladder emptying following urogynecologic surgery should be taught intermittent self-catheterization to avoid complications such as recurrent urinary tract infections and upper urinary tract damage.
URETHRAL CARUNCLES AND PROLAPSE
Urethral caruncles, small polyps of urethral mucosa protruding through the meatus, are seen almost exclusively in postmenopausal females, whereas urethral prolapse, defined as an eversion of the urethral mucosa through the external meatus, can be found in both postmenopausal women as well as young girls. The two urethral pathologies may be difficult to distinguish from one another. They commonly present with irritative voiding symptoms. Furthermore, it is not uncommon for urethral prolapse to present with vaginal bleeding. Classically, urethral prolapse is described as a fleshy erythematous mass of tissue surrounding the meatus. It occurs in the setting of vaginal atrophy and may be related to repeated straining, trauma, the placement of periurethral bulking agents, or, rarely, urethral tumors (5). Urethral caruncles, in contrast, are focal and not circumferential. The primary treatment for both is topical estrogen cream. The ER provider must ensure that the patient is not obstructed, in which case a transurethral catheter needs to be placed. If the urethral mucosa appears ischemic due to strangulation or thrombosis is noted, then resection of exposed urethral mucosa may be indicated and urologic consultation is recommended.
BOWEL EVISCERATION FOLLOWING VAGINAL SURGERY
Vaginal evisceration is a rare but serious condition. It has been reported to occur following trauma from intercourse, obstetrical tears, foreign bodies, and vaginal surgery. Most commonly, evisceration will occur following hysterectomy in patients with prolapse, enteroceles, urogenital atrophy, and history of radiation therapy (6). Other predisposing factors include a vaginal cuff left open at the time of hysterectomy and cuff cellulitis or hematoma (7). The distal ileum is most commonly involved in vaginal evisceration (8).
When the patient presents with vaginal evisceration in the ER, the bowel should be wrapped in sterile gauze soaked in saline, and an immediate surgical consultation should be made. Prompt and appropriate surgical intervention is necessary to prevent mortality, which can occur in 6% to 10% of cases due to septicemia and thromboembolism. In general, emergent laparotomy with inspection of the bowel and resection of any compromised areas with reanastomosis is recommended (9). Resection of necrotic tissue at the vaginal cuff and closure of the cuff with interrupted absorbable sutures should be followed by copious irrigation and placement of an appropriate suction drain. Nasogastric drainage may be required for treatment of a prolonged ileus associated with the small bowel resection (10).
FOURNIER'S GANGRENE
Although rare, Fournier’s gangrene is one of the most capricious and deadly urogynecologic emergencies seen in the ER. Fournier’s gangrene is an aggressive form of necrotizing fasciitis of the perineum that, even if aggressively treated, can result in death in 22% to 40% of cases (11). It can present subacutely and with nonspecific symptoms before progressing to its fulminant form associated with extensive tissue destruction and systemic toxicity. The diagnosing physician therefore requires a high index of suspicion.
Fournier’s gangrene is a mixed infection caused by both aerobic and anaerobic bacteria and occurs most commonly after surgical procedures, after vaginal delivery, or associated with primary perirectal infections. This disease can complicate minor vaginal surgical procedures, such as tension-free vaginal tape placement, or newer larger reconstructive vaginal surgeries utilizing mesh (12,13). Patients with diabetes and peripheral vascular disease are at increased risk. The predominant isolates found in patients with necrotizing fasciitis are Staphylococcus aureus, Escherichia coli, group A strepococcus, Peptostreptococcus species, Bacteroides fragilis, and Clostridium species (14).
This infectious process starts in the perineal area or within the vagina with penetration of the gastrointestinal or urethral mucosa by enteric organisms. It is a deep-seated infection of the subcutaneous tissue that results in the destruction of fascia and fat but may spare the skin. These infections begin abruptly, usually with pain over the affected site. In many patients, this initial presentation is overlooked because in postoperative or postpartum patients these symptoms are part of the normal convalescence. Diabetics may present late owing to absence of pain secondary to peripheral neuropathy. Erythema may be present diffusely or locally, but in some patients, excruciating pain in the absence of any cutaneous findings is the only clue of infection. Within 24 to 48 hours, erythema may develop or darken and turn to a reddish-purple color, frequently with associated blisters and bullae. Once the bulla stage is reached, there is already extensive deep soft-tissue destruction, and such patients usually exhibit fever and systemic toxicity including malaise, myalgias, diarrhea, anorexia, and possibly septic shock (15).
The diagnosis is often difficult to appreciate in the early stages. Pain is usually out of proportion to physical findings, and laboratory findings are nonspecific. Blood tests may demonstrate leukocytosis with marked left shift and elevations in serum creatinine or creatinine kinase (16). Imaging studies such as soft-tissue x-rays, computed tomography scans, and magnetic resonance imaging are most helpful but may only show soft-tissue swelling and cannot distinguish necrotizing fasciitis from cellulitis or inflammation (17). Gram stain or cultures via punch biopsies at the site are also ineffective in clarifying the diagnosis rapidly, and therefore, aggressive surgical exploration should proceed immediately once the diagnosis is suspected. Any delay increases mortality. The ER personnel should begin broad-spectrum intravenous antibiotic coverage empirically and aggressively treat any evidence of shock with fluid resuscitation. A surgical team should be organized quickly including general surgery, urology, and gynecolog y to manage these patients appropriately.
INCARCERATED UTEROVAGINAL PROLAPSE
Stage III or IV uterovaginal prolapse is visible prolapse that protrudes outside the hymenal ring. The term “procidentia” refers to stage IV uterovaginal prolapse or prolapse of the uterus and the cervix with a completely inverted vagina. In rare instances, the prolapse may become impossible to reduce back into the vagina. Women presenting with irreducible or incarcerated prolapse to an office or ER are often older and might have neglected routine gynecologic visits. Additionally, an examining physician may find ulcers or areas of erosion of the exposed vaginal mucosa or cervix. Biopsies of any suspicious ulcerations should be performed to rule out any underlying malignancy.
When evaluating a patient with a prolapse that is difficult to reduce, a full history and an examination should be performed to determine the cause for incar- ceration—a large palpable bladder stone, fibroid uterus, pelvic mass, or cul-de-sac abscess. The bladder should be emptied initially with a straight catheter which will allow for evacuation of any elevated residual bladder volumes which are frequently found in patients with incomplete bladder emptying because of urethral kinking from the prolapse. Once the bladder has been emptied and no mass has been palpated in the cul-de-sac through a transrectal examination, the prolapse can be gently squeezed to try to decrease the tissue edema. Alternatively, the uterus can be wrapped in bandages soaked in hypertonic saline, and gentle but steady pressure can be applied on the prolapse with the patient in the lithotomy or Trendelenburg position. Knee-chest positioning has also been recommended to reduce intra-abdominal pressure (18). Once reduced, the vagina will need to be packed until an adequately sized pessary is available for placement.
The donut, Gehrung, Gellhorn, ring-with-support, cube, or Inflato-ball type of pessary is typically used for procidentia. A patient with a widened genital hiatus may be unable to retain the pessary and will therefore need either definitive surgical correction or a pessary with concomitant perineoplasty to reduce the size of the hiatus. Alternatively, local anesthesia can be used to place bilateral labial stitches to hold the pessary in place until surgery. Definitive surgical correction, a partial or complete colpectomy or vaginal hysterectomy with subsequent colpocleisis or reconstructive surgery, should be delayed until the tissues have healed and the surrounding infection and edema have resolved. Bladder calculi if found will need to be treated via cystoscopy or cystotomy.
Emergency requiring ICU admission for stabilization and reduction of prolapse to allow for appropriate urine flow may result from acute renal failure secondary to bilateral ureteral obstruction in rare cases of procidentia (19). This obstruction is secondary to distal kinking of the ureters. Unless there is preceding chronic renal disease, these patients generally recover once the obstruction has been alleviated.
THE NEGLECTED PESSARY
Women using pessaries should have adequately estrogenized vaginas and ideally should remove the pessary nightly. For patients who lack the necessary manual dexterity, a caregiver can remove and clean the pessary two to three times per week, or a health care provider can remove and clean the pessary and inspect the vagina every 8 to 12 weeks. Patients with neglected pessaries will present to the ER with foul-smelling vaginal discharge or vaginal bleeding and, in rare cases, urosepsis (20). The neglected pessary can lead to superficial and full-thickness vaginal erosions from pressure necrosis. These can progress to form vesicovaginal or rectovaginal fistulas. The ER provider must remove the pessary and closely inspect the vagina for evidence of erosion or fistulae. If no lesions are found, the vagina can be cleaned and treated with Trimosan® or other antibacterial creams. The pessary can be replaced once the infection has resolved. Any necrotic tissue should be deb- rided. Superficial erosions can be treated effectively with topical estrogen cream which should be applied topically for several weeks. If a vesicovaginal fistula is suspected, an indwelling Foley catheter should be placed until surgical correction can be performed. Patients with suspected rectovaginal fistula should also be referred urgently to the appropriate surgical service.
FECAL IMPACTION
Fecal impaction is one of the most common urogynecologic presentations to the ER and is defined as the inability to pass a hard collection of stool. The risk factors include a history of constipation with decreased colonic motility, poor eating habits, severe rectocele leading to trapping of stool in the rectal vault, and patient immobility. The pathophysiology involves a combination of these factors, which result in stasis of stool and reabsorption of water, leading to hardening of the stool. This is aggravated by continuous colonic motility, which packs the stool in the rectum. Because of the decreased sensation, the rectoanal reflex becomes dysfunctional, leading to an inability to coordinate defecation. The result is a large bolus of hard stool in the rectal vault, leading to obstruction (21).
The patients are generally elderly, institutionalized, and poor historians but often present acutely with symptoms of obstipation including nausea, vomiting, severe abdominal or rectal pain, paradoxical diarrhea, and fecal incontinence. With severe posterior compartment distension, the urinary tract may also be affected and patients may present with chronic urinary tract infections or irritative voiding. A patient history including bowel habits, systemic disease (i.e., diabetes, multiple sclerosis, hypercalcemia, hypothyroidism), dyschezia, or a history of fecal evacuation disorders should be obtained. The need for the patient to use perineal splinting, digital disimpaction, or unusual positions during defecation suggests pelvic outlet dysfunction. If a sensation of rectal fullness predominates, this could indicate rectal prolapse, internal intussusception, or rectocele (22). Physical examination may reveal a distended abdomen and large hard stool in the vault. Occasionally, impaction may be proximal to the reach of a digital examination. If diagnosis is apparent on history and physical examination, and there is no suspicion of an acute intra-abdominal process, and electrolyte abnormalities have been ruled out, these patients can be treated in the ER. Otherwise, a more extensive workup including radiographic evaluation is warranted.
Acute treatment for fecal impaction generally involves digital disimpaction. Using lidocaine gel for local anesthesia, one or, ideally, two fingers are gradually inserted into the rectum and the stool is extracted. This technique may be aided using transvaginal pressure with the opposite hand. Stool may be softened using glycerin suppositories or mineral oil transrectally. Other options include saline and Fleet enemas. If these are ineffective, a rectal tube or Foley catheter can be carefully passed beyond the presenting fecal bolus, and normal saline solution can be injected promixal to the obstruction. Alternatively, oral treatments including magnesium citrate, oral Fleet’s, polyethylene glycol, and other nonabsorbable sugars such as lactulose and sorbitol can be used. These agents should be used with caution, in particular, oral Fleet’s, which has been reported to cause severe electrolyte disturbances and even death in some patients. Stimulant laxatives such as docusate salts are not as effective for fecal impaction and should not be used in combination with mineral oil on a chronic basis because of the damage this can cause to the myenteric plexus (23).
If fecal impaction can be resolved in the ER, these patients and their caregivers need to be given instruction on prevention. A high-fiber diet with fluids is needed to bulk up stool. The patient should be on a bowel regimen to promote bowel movements at a minimum of every 3 to 4 days. These patients will require close follow-up by their primary care providers, and if fecal impaction persists, further evaluation should be undertaken.
References
1. Ibeanu OA, Chesson RR, Echols KT, Nieves M, Busangu F, Nolan TE. Urinary tract injury during hysterectomy based on universal cystoscopy. Obstet Gynecol. 2009; 223(1):6-10.
2. Jelovsek JE, Chiung C, Chen G, Roberts SL, Paraiso MF, Falcone T. Incidence of lower urinary tract injury at the time of total laparoscopic hysterectomy. JSLS. 2007;11(4): 422-427.
3. Liatsikos EN, Karnabatidis D, Katsanos K, et al. Ureteral injuries during gynecologic surgery: treatment with a minimally invasive approach. JEndourol 2006;20(12):1062-1067.
4. Blaivas JG, Heritz DM, Romanzi LJ. Early versus late repair of vesico-vaginal fistulas: vaginal and abdominal approaches. J Urol. 1995;153:1112.
5. Harris RL, Cundiff GW, Coates KW, et al. Urethral prolapse after collagen injection. Am J Obstet Gynecol. 1998;178(3):614-615.
6. Ramirez PT, Klemer DP. Vaginal evisceration after hysterectomy: a literature review. Obstet Gynecol Surv. 2002;57(7):462-467.
7. Cardosi RJ, Hoffman MS, Spellacy WN. Vaginal evisceration after hysterectomy in premenopausal women. Obstet Gynecol. 1999;94:859.
8. Kambouris AA, Drukker BH, Barron J. Vaginal evisceration. Arch Surg. 1981;116: 949-951.
9. Kowalski LD, Seski JC, Timmins PF, et al. Vaginal evisceration: presentation and management in postmenopausal women. JAm CollSurg. 1996;183(3):225-229.
10. Nichols DH. Evisceration one year after vaginal hysterectomy without colporrhaphy. In: Nichols DH, DeLancey JOL, eds. Clinical Problems, Injuries and Complications of Gynecologic and Obstetric Surgery. 3rd Ed. Baltimore, MD: Williams & Wilkins; 1995: 179-181.
11. Lauks SS. Fournier’s gangrene. Surg Clin North Am. 1994;74:1339-1352.
12. Riedler I, Primus G, Trummer H, et al. Fournier’s gangrene after tension-free vaginal tape procedure. Int UrogynecolJ. 2004;15:145-146.
13. Diwadkar GB, Barber MD, Feiner B, Maher C, Jelovsek JE. Complication and reoperation rates after apical vaginal prolapse surgical repair: a systematic review. Obstet Gynecol. 2009;113(2):367-373.
14. Brook I, Frazier EH. Clinical and microbiological features of necrotizing fascitis. J Clin Microbiol. 1995;33:2382-2391.
15. Stevens DL. Necrotizing infections of the skin and fascia. UpToDate Version 12.1.
16. Simonart T, Simonart JM, Derdelinckx I, et al. Value of standard laboratory tests for the early recognition of group A beta-hemolytic streptococcal necrotizing fasciitis. Clin Infect Dis. 2001;32:E9.
17. Schmid MR, Kossmann T, Duewell S. Differentiation of necrotizing fascitis and cellulites using MR imaging. Am J Roentgenol. 1998;170:615.
18. Delancey JOL. Uterovaginal prolapse that is difficult or impossible to reduce. In: Nichols DH, DeLancey JOL, eds. Clinical Problems, Injuries and Complications of Gynecologic and Obstetric Surgery. 3rd Ed. Baltimore, MD: Williams & Wilkins; 1995: 147-151.
19. Sudhakar AS, Reddi VG, Shei M, et al. Bilateral hydroureter and hydronephrosis causing renal failure due to a procidentia uteri: a case report. Int Surg. 2001;86(3): 173-175.
20. Roberge RJ, McClandish MM, Dorfsman ML. Urosepsis associated with vaginal pessary use. Ann Emerg Med. 1999;33:581-583.
21. Wald A. Approach to patient with constipation. In Yamada T, Alpers D, Kaplowitz N, et al., eds. Textbook of Gastroenterology. 4th Ed. Philadelphia, PA: Lipincott Williams & Wilkins; 2003.
22. Prather CM, Ortiz-Camacho CP. Evaluation and treatment of constipation and fecal impaction in adults. Mayo Clin Proc. 1998;73:881-887.
23. Sloan S. Medical management of constipation In: Brubaker LT, Sclarides S, eds. The Female Pelvic Floor: Disorders of Function and Support. Philadelphia, PA: F. A. Davis; 1996.
More on the topic Imaging in Gynecologic Emergencies:
- Imaging in Gynecologic Emergencies
- Benrubi Guy I. (ed.). Handbook of Obstetric and Gynecologic Emergencies. 4th edition. — Lippincott Williams & Wilkins,2010. — 424 p., 2010
- CONTENTS
- Role of Imaging Modalities in Obstetric Emergencies
- INDEX
- Pelvic Mass
- Postoperative Complications and Postoperative Emergencies
- Oncologic Emergencies
- Chapter 34 Gynecologic Procedures
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020