Pelvic Mass
Karl H.S. Smith
A pelvic mass in a female must always be considered in the context of other parameters. Is the woman symptomatic with abdominal pain and swelling, or has her mass been detected incidentally by an imaging study performed for another reason? What is her age, menstrual and pregnancy history? What has she been using for contraception? Has she had previous pelvic infection or surgery? Has she had any recent pain with sexual intercourse or change in urinary or bowel habits? The answer to each of these questions may have a bearing on determining the ultimate cause of a pelvic mass and lead a clinician through a logical and efficient process of evaluation.
ASYMPTOMATIC PELVIC MASSES
In the 21st century in the United States, the plethora of imaging studies has made the incidental finding of a pelvic mass common. Abdominal and pelvic computerized tomograms (CT scans), sonograms, magnetic resonance imaging (MRI), and positron emission test (PET) scans are being performed with much more frequency than in the past. In 2006, it was estimated that over 60 million CT scans were performed in the United States (1). Sometimes these procedures are performed for nonspecific abdominal complaints or to evaluate urologic, intestinal, or orthopedic problems. Sometimes these tests are performed to further evaluate a known problem such as cancer. There is an increase in the performance of these imaging studies in asymptomatic women as part of a general executive health screening (2). Small asymptomatic cystic ovarian masses assessed on vaginal ultrasound to be <5 cm diameter without septae or nodularity within (simple cysts) may be followed with repeat vaginal sonography in several months time (3). Generally, asymptomatic masses that do not grow are considered benign. In reproductive age women not using hormonal contraception, a functional ovarian cyst (including hemorrhagic corpora lutea and dominant follicles) would be a common finding.
Such cystic masses can sometimes be associated with uterine changes indicating an early pregnancy. In such cases, a pregnancy test is indicated. An adnexal mass imaged in a reproductive age woman with a positive pregnancy test and absence of an intrauterine gestational sac could be the first evidence of an early ectopic pregnancy. Management of ectopic pregnancy is covered in Chapter 3 of this book.For the premenarchal female, an asymptomatic pelvic mass could represent a congenital anomaly involving the upper genital tract, urinary tract, vagina, or colon and rectum. Prior to the availability of sophisticated imaging studies such as sonography and CT scans, a pelvic kidney was commonly misdiagnosed as an ovarian mass. Although the finding of an asymptomatic pelvic mass in a premenarchal girl is not a medical emergency, further evaluation is appropriate. Some of the more common premenarchal conditions that could present as a pelvic mass in an infant or adolescent are as follows: hematocolpos from an imperforate hymen, uterine anomalies, ovarian germ cell or stromal neoplasia, and rarely, endometriomas or abscesses (4,5). Other information obtained by history and general physical examination will be helpful in determining an appropriate differential diagnosis. For example, the presence of precocious puberty with premature breast and pubic hair development or premature menarche may lead to the discovery of an ovarian stromal neoplasm. It is always prudent to consider simple problems such as urinary retention with a full bladder or constipation with a dilated colon or rectum as the cause of a so- called “asymptomatic pelvic mass” in a female child. Further elucidation is beyond the scope of this chapter. The reader is referred to well-documented previous works (6-8).
In reproductive-age women with an intact uterus, the most common asymptomatic pelvic mass after a functional ovarian cyst or early pregnancy is uterine leiomyoma. This occurs in 20% to 30% of women over 30 years of age (9) and is found in up to 75% of hysterectomy specimen (10).
Leiomyoma is often discovered on routine screening pelvic examinations. Women with leiomyoma may have unrecognized symptoms of heavy menstrual periods and pelvic fullness with urinary frequency and/or constipation. The presence of uterine leiomyoma does not represent a medical emergency unless it is causing severe symptoms such as pain or uterine bleeding significant enough to cause acute anemia with decreased intravascular volume. A very large or rapidly growing leiomyoma may cause ureteral obstruction or hydronephrosis. The development of uterine leiomyosarcoma is a feared sequela of uterine leiomyoma. Fortunately, this is a rare condition that occurs in <1% of women with suspected leiomyoma (11). Occasionally, a pelvic mass that is thought to represent a leiomyoma is later determined to be an ovarian mass. If normal ovaries cannot be clearly identified in a women with a pelvic mass suspected to represent leiomyoma, additional studies including combined abdominal/vaginal ultrasound or MR of the pelvis should be considered.The most feared pelvic mass is ovarian cancer. This is an insidious condition with a peak incidence among women in their mid 50s. Like uterine leiomyoma, women with ovarian cancer may experience abdominal fullness, swelling, or early satiety. As women go through menopause and stop menstruating, uterine leiomyoma tend to get smaller, but ovarian masses may continue to grow. Fortunately, most ovarian neoplasms are benign with cystic teratomas being the most common (12). Like leiomyoma, benign ovarian tumors may reach great size, distorting the abdominal contour while causing little in the way of symptoms.
Ovarian masses that are detected during routine prenatal sonograms are particularly challenging. Ovarian masses are detected in approximately 6% of pregnancies during routine obstetrical sonography (13,14). Most of these resolve representing physiologic cysts of pregnancy. Those that persist may cause the same complications seen in nonpregnant women (e.g., torsion, rupture, or hemorrhage), but these events are uncommon.
Approximately 2% of ovarian masses detected during pregnancy will prove to be malignant and most of these are stage 1 (15). In the past, persistent adnexal masses in pregnancy were managed surgically in the second trimester between 14 and 20 weeks’ gestation. Masses detected later were managed by elective cesarean delivery at term followed by surgical management of the ovarian mass. Within the past decade, there has been a trend toward a more conservative management with careful sonographic monitoring allowing vaginal delivery and then management of the mass weeks to months after delivery (15-18).As previously noted, ovarian cancer is the most dreaded cancer of the female reproductive tract because of its insidious and lethal nature. In 2008, it was estimated that 21,650 women in the United States would develop this cancer and 15,520 would die (19). With serous ovarian cancer, the most common type of malignant ovarian epithelial cancer, the ovarian neoplasia may grow as an ovarian mass, spread by direct extension to the peritoneal cavity or other structures in the abdomen and pelvis or development of ascites causing subtle symptoms of bloating and indigestion. These symptoms can be misinterpreted as a primary gastrointestinal (GI) problem. It is not uncommon for a woman to present with ovarian cancer claiming to have no “gynecologic symptoms,” yet she has seen an internist or gastroenterologist for intestinal “problems.” It is not uncommon to have a woman undergo an upper and a lower GI imaging or endoscopy prior to having a pelvic examination or a pelvic sonogram. According to Goffet al. (20), early symptoms associated with the subsequent diagnosis of ovarian cancer consisted of pelvic or abdominal pain, urinary urgency or frequency, increased abdominal size or bloating, and difficulty eating or feeling full.
Common causes of asymptomatic nonovarian pelvic masses in premenopausal women are abnormalities of the fallopian tubes such as hydrosalpinx and paraovarian cysts.
These conditions can often be diagnosed by transvaginal ultrasound, and in most cases, expectant management is appropriate. Other less common conditions of the ovary that can present as an asymptomatic pelvic mass are polycystic ovaries, hyperstimulated ovaries, and, occasionally, an ovarian abscess. These conditions will usually be associated with other suggestive findings in the history and the physical examination leading the clinician to make an appropriate diagnosis. Unfortunately, a final diagnosis sometimes cannot be made without surgery such as a diagnostic laparoscopy.SYMPTOMATIC PELVIC MASS
While asymptomatic pelvic masses are concerning, they rarely present as a medical emergency. Symptomatic pelvic masses are of greater concern because they may represent a serious or even life-threatening situation. One of the most common symptomatic conditions in a reproductive age female is abdominal pain due to ovulation or a ruptured corpus luteum. Rupture of a cyst, though painful, is usually self-limiting and not life threatening. The diagnosis is usually one of the exclusions, and in cases of severe, unrelenting pain, confirmation may require surgical intervention by laparoscopy.
The most serious symptomatic condition in a reproductive age female is an ectopic pregnancy. Despite advances in imaging technology in the 21st century, ectopic pregnancies are still misdiagnosed resulting in serious and sometimes fatal consequences. The importance of obtaining a pregnancy test in a reproductive age women with abdominal pain and menstrual irregularity cannot be over emphasized (see Chapter 3).
After ectopic pregnancy, the most serious symptomatic pelvic mass is a tuboovarian abscess. This usually occurs in a setting of pelvic inflammatory disease as discussed in Chapter 19 of this book. These masses will usually resolve with medical management but will occasionally require surgical intervention.
The next most serious symptomatic pelvic mass is the torsed adnexa.
Adnexal torsion has been found to account for about 3% of surgical emergencies in women (21). Adnexal enlargement on sonography in the presence of abdominal pain and a negative pregnancy test should point to ovarian torsion in the differential diagnosis. These findings indicate the need to consider surgical intervention by laparoscopy or laparotomy (see Chapter 23).The differential diagnosis of a pelvic mass with abdominal pain must also include endometrioma, appendicitis, and colonic diverticulitis. Endometriosis may be associated with a history of progressive dysmenorrhea leading to the presenting episode. Sonographic features of the ovary are also distinctive with the hemorrhagic ovarian cyst and endometrioma showing a ground-glass appearance and sometimes a fluid and solid interface within the ovarian mass where blood has clotted and layered. An ovarian abscess may have nonspecific solid and cystic sonographic features that could be confused with an ovarian malignancy. A pelvic infection often occurs after a menstrual period and may be associated with cervical motion tenderness, fever, and elevated white blood count (WBC). These same findings may be present in a woman with a diverticular abscess. In this case, a history of progressively worsening constipation may be significant and may lead to the diagnosis. Often, a sonogram will not be sufficient to establish a diagnosis, and additional imaging studies such as a CT scan with oral, intravenous (IV), and rectal contrast may need to be considered. If pain persists and the WBC rises, surgical evaluation by laparoscopy may need to be considered.
A uterine disorder is the most common cause of a symptomatic midline pelvic mass. After pregnancy, symptomatic uterine leiomyoma are most common. Rapidly growing or cystically degenerated leiomyoma is a common cause of midline mass with pain. Adenomyosis often occurs in the presence of uterine leiomyoma leading to heavy menstrual bleeding and pelvic pain. The timing of the pain is critical. If the uterus is infected due to pelvic inflammatory disease or endomyometritis, the picture may be confusing. Imaging studies such as pelvic sonograms and CT scans become critical. In this setting, endometrial biopsy may also help determine if an infection is present. WBC will usually be elevated in the presence of infection. Uterine cancer (endometrial or myometrial) or cervical cancer may rarely present as a painful midline pelvic mass. This will usually occur in a perimenopausal woman and be associated with abnormal bleeding. Pelvic examination and pelvic sonography are useful in establishing a diagnosis of uterine cancer; however, a final diagnosis cannot be established without histological evaluation of tissue from the endometrium or the cervix.
In women who have undergone a hysterectomy, the diagnosis of a midline symptomatic pelvic mass can be more challenging. Recent history of surgery such as a hysterectomy should lead to a differential that might include a hematoma or an abscess. With a more remote history of hysterectomy (over 6 months), the differential could include an ovarian or tubal mass in the cul-de-sac, endometrioma, inclusion cyst of the vaginal cuff, or malignancy of the bladder, colon, or rectum. Once again, simple problems such as cystitis with urinary retention and chronic constipation with fecal impaction must be considered. These conditions can usually be established by taking a careful history.
Rarely, symptomatic pelvic masses include metastatic disease to the ovary from cancers of the breast, colon, stomach, small intestine, kidneys, or lymphoma. The ovarian mass may be the first sign of cancer. Cancers metastatic to the ovary tend to be bilateral and solid; however, cystic lesions have been reported (22). A history of breast, GI, renal, or hematologic malignancy should raise suspicion of a metastatic process.
UNUSUAL SITUATIONS PRESENTING AS A PELVIC MASS
The most common causes of pelvic mass have been described. To complete a discussion of the differential diagnosis of a pelvic mass, other diagnoses must be considered. These include neoplasic masses caused by retroperitoneal sarcomas, lymphomas, and retroperitoneal cysts. Pelvic inclusion cysts, which are not neoplastic, can occur in women who have undergone multiple intra-abdominal and/ or pelvic surgeries. Radiated bowel can become agglutinated, forming a mass that is hard to distinguish from a neoplastic process on examination. Also, fluid- filled spaces may occur between loops of intestine simulating a cystic mass. Past history of pelvic surgery with lymph node dissection and a pelvic sidewall cyst could indicate the presence of a lymphocyst. Careful review of imaging studies will usually allow for a correct diagnosis. However, sometimes the correct diagnosis cannot be made until surgery. As noted previously, in the presence of abdominal pain, fever, and elevated WBC, it is sometimes hard to distinguish a
Differential Diagnosis of Pelvic Masses
| Gynecologic | Nongynecologic |
| Uterus—benign | Distended bladder |
| Pregnancy | Feces (impaction) |
| Leiomyoma | Pelvic kidney |
| Congenital anomalies | Urachal cyst |
| Urinoma | |
| Uterus—malignant | Diverticular abscess |
| Cervical carcinoma Endometrial carcinoma | Appendiceal abscess |
| Sarcoma | Lymphoma Lymphocyst |
| Ovary—benign | Anterior sacral teratoma |
| Cystadenoma | Retroperitoneal fibrosis |
| Follicle cyst | Metastatic cancer |
| Sclerocystic ovary | GI tumor |
| Corpus luteum cyst | Abdominal wall hematoma |
| Endometriotic cyst | Abdominal wall radiation fibrosis |
| Germinal inclusion cyst | |
| Theca-lutein cyst | |
| Benign cystic teratoma (dermoid) | |
| Ovarian hyperstimulation | |
| syndrome (OHSS) | |
| Ovary—malignant | |
| Epithelia carcinoma | |
| Germ cell tumor | |
| Gonadal stromal tumor | |
| Metastatic cancer to ovary | |
| Fallopian tube | |
| Ectopic pregnancy | |
| Hydrosalpinx | |
| Paratubal cyst | |
| Carcinoma |
right-sided ovarian abscess from a diverticular abscess or a left-side mass from a diverticular abscess. Other causes of pelvic cysts are listed in Table 22.1.
METHODS OF EVALUATING A MASS
As mentioned earlier, asymptomatic masses are often detected by CT or MRI performed for another reason. For example, a pelvic or abdominal CT or MRI may be ordered to evaluate back pain and a pelvic mass will be discovered. Unfortunately, if only a pelvic CT or MRI is ordered, lower lung fields, diaphragm, liver, stomach, spleen, pancreas, omentum, much of the intestinal tract, and kidneys with upper ureters may not be visible. Sometimes, with very large masses, only the lower aspect of the mass will be seen. These are all sites that may be impacted by a primary ovarian cancer. An abdominal CT or MRI on the other hand often stops at the level ofvertebral body L5 or S1 and misses important pelvic structures such as the uterus, bladder, rectosigmoid colon, and bony pelvis. If a complete survey of the abdomen and the pelvis is to be conducted, imaging of both the abdomen and the pelvis should be ordered when evaluating nonspecific symptoms. For general surveillance of the abdominal and pelvic organs, a CT scan is a better study than an MRI because imaging with the MRI occurs at a slower speed and results in more intestinal or respiratory motion and artifact. The MRI is better for evaluating bony structures. When ordering a CT, it is also prudent to use both oral and IV contrasts. This will allow intestinal and urologic structures to be more easily distinguished from vascular structures and muscles. IV contrast should generally be avoided in patients with a serum creatinine of 1.5 mg/dL to prevent contrast induced nephropathy.
If a mass is detected on pelvic examination and requires further characterization, a pelvic and abdominal sonogram may be more useful than a CT. The sonogram will allow for better characterization of the internal features of an ovarian mass such as septations or papillary features. As previously noted, ovarian masses that are simple (i.e., those containing no internal echoes such as septations, papillary features, or fluid layering) and 5 cm in diameter or less are rarely neoplasic (3). For large pelvic masses, sonographic evaluation of the kidneys and ureters can exclude hydronephrosis or hydroureter. An abdominal ultrasound will also allow ascites or free peritoneal blood to be identified. This is the strategy of the focused assessment with sonography for trauma (FAST scan) used by emergency department physicians and general surgeons in evaluating someone with pelvic trauma (23). Finding free fluid in the pelvis or abdomen following trauma warrants an emergency paracentesis. It is always prudent in the evaluation of a woman of menstrual age to consider a pregnancy condition as a source of hemoperitoneum, emphasizing the importance of performing a screening urine pregnancy test in this situation.
Management of patients with a mass
Asymptomatic masses may usually be managed in an orderly fashion by referring the patient to a gynecologic surgeon and preparing for surgery. However, in a symptomatic patient, some urgency will ensue (Fig. 22.1). In patients with worrisome vital signs such as tachycardia and hypotension, IV hydration should be initiated and blood should be made ready in the blood bank (type and crossmatch). Basic laboratory tests should include a complete blood count (CBC) and basic metabolic profile (BMP) that includes serum electrolytes, glucose, blood urea nitrogen (BUN), and creatinine. If there is any concern about bleeding or liver disease, a coagulation screen consisting or prothrombin time (PT) and partial thromboplastin time (PTT) should be ordered. As noted previously, a urine pregnancy test is warranted in reproductive age women. The patient should be kept from eating or drinking as this can result in anesthetic complications. Depending on the status of the patient and time constraints, simple x-rays of the chest and the abdomen should be obtained (obstructive series). These tests will allow the gynecologic or general surgical consultant to rapidly take a patient to surgery if indicated. Air under the diaphragm suggests a perforated viscous and intestinal obstruction indicating the need for nasogastric tube placement. Both findings warrant consideration for more urgent surgical intervention.
In situations where the need for surgery is not emergent, additional procedures such as a bowel prep or thoracentesis for a pleural effusion might be considered. For patients with large pelvic masses, there is a possibility of respiratory compromise. In the presence of pleural effusion or marked abdominal distension due to ascites or a very large abdominal mass, arterial blood gases should be considered. Finally, attention should be directed to managing comorbid conditions such as diabetes, hypertension, or chronic obstructive pulmonary disease.
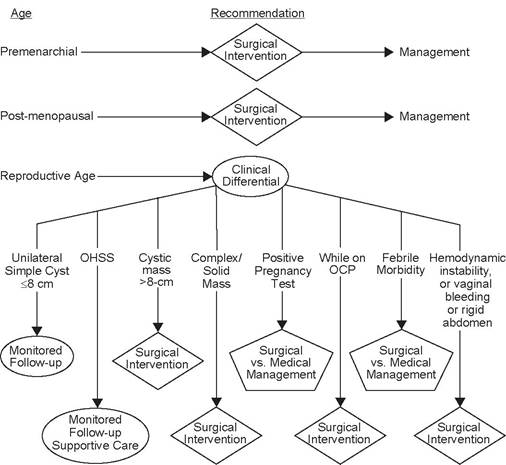
FIGURE 22.1 Algorithm for symptomatic ovarian mass.
The gynecologic or general surgeon who decides to take a patient to surgery must determine the timing (emergent or urgent) and the best approach to surgery (laparoscopic versus open) and then the best type of incision. These decisions should be discussed with the patient. It is important for the surgeon to ask the patient about her future desires for fertility and to determine any limits on surgery. For example, a woman <40 years of age may wish to preserve her uterus for future fertility if possible. This issue becomes critical in situations where both ovaries are involved in a process such as infection, endometriosis, or cancer. Some patient would want the uterus removed if both ovaries were removed, while others would want the uterus preserved. Bilateral ovarian masses have a greater incidence of malignancy (24). Patients should be informed that sometimes the best solution to a particular situation cannot be determined prior to surgery. It should be determined if a patient desires conservative surgery even at the risk of requiring additional surgery in the future. Finally, it is important for the surgeon to explain that unforeseen circumstances may occur that necessitate surgery to the intestinal or urinary tract. This is especially important if there is a possibility that bowel resection or colostomy is necessary.
SUMMARY
The diagnosis and management of a pelvic mass require taking a careful history of recent and past events, a thorough physical examination including a pelvic examination, and a selection of appropriate laboratory tests and imaging studies. The differential diagnosis should be discussed with the patient and her support system (family and/or friends) to determine the best course of treatment based on the most likely diagnosis, severity of symptoms, and desire for future fertility. Once a treatment plan is established, the plan should be implemented with efficiency and safety while maintaining communication with the patient and her family.
References
1. Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. NEnglJMed. 2007;357:2277-2284.
2. Beinfeld MT, Wittenberg E, Gazelle GS. Cost-effectiveness of whole-body CT screening. Radiology. 2005;234:415-422.
3. Van Nagell JR, Depriest PD, Ueland FR, et al. Ovarian cancer screening with annual transvaginal sonography. Cancer. 2007;109:1887-1896.
4. Emans DP. Office evaluation of the child and adolescent. In: Emans SJH, Goldstein DP, eds. Pediatric & Adolescent Gynecology. 3rd Ed. Boston, Toronto, London: Little, Brown and Company; 1990.
5. Muram D. Developmental abnormalities. In: Copeland LJ, ed. Textbook of Gynecology. Philadelphia, PA: W.B. Saunders; 2000.
6. Emans SJH, Goldstein DP, eds. Ovarian masses. In: Pediatric & Adolescent Gynecology. 3rd Ed. Boston, Toronto, London: Little, Brown and Company; 1990.
7. Sanfiliippo JS. Pediatric and adolescent gynecology. In: Copeland LJ, ed. Textbook of Gynecology. Philadelphia, PA: W.B. Saunders; 2000.
8. BekiesiAska-Figatowska M, Jurkiewicz E, Iwanowska B, et al. Magnetic resonance imaging as a diagnostic tool in case of ovarian masses in girls and young women. Med SciMonit. 2007;13(Suppl. 1):116-120.
9. Zaloudek C, Hendrickson M. Mesenchymal tumors of the uterus. In: Kurman RJ, ed. Blausteins Pathology of the Female Genital Tract. 5th Ed. New York, NY: SpringerVerlag; 2002.
10. Cramer SF, Patel A. The frequency of uterine leiomyomas. Am J Clin Pathol. 1990; 94(4):435-438.
11. Parker WH, Fu YS, Bereek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol. 1994;83:414-417.
12. Koonings PP, Campbell K, Mishell DR Jr, Grimes DA. Relative frequency of primary ovarian neoplasms: a 10-year review. Obstet Gynecol. 1989;74(6):921-926.
13. Bernhard LM, Klebba PK, Gray DL, et al. Predictors of persistence of adnexal masses in pregnancy. Obstet Gynecol. 1999;93:585-589.
14. Condous G, Khalid A, Okaro E, et al. Should we be examining the ovaries in pregnancy? Prevalence and natural history of adnexal pathology detected at first-trimester sonography. Ultrasound Obstet Gynecol. 2004;24:62-66.
15. Leiserowitz GS, Xing G, Cress R, et al. Adnexal masses in pregnancy: how often are they malignant? Gynecol Oncol. 2006 May;101(2):315-321.
16. Schmeler KM, Mayo-Smith WW, Peipert JF, et al. Adnexal masses in pregnancy: surgery compared with observation. Obstet Gynecol. 2005;105:1098-1103.
17. Zanetta G, Mariani E, Lissoni A, et al. A prospective study of the role of ultrasound in the management of adnexal masses in pregnancy. BJOG. 2003;110(6):578-583.
18. Giuntoli RL, Vang RS, Bristow RE. Evaluation and management of adnexal masses during pregnancy. Clin Obstet Gynecol. 2006;49(3):492-505.
19. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer JClin. 2008;58;71-96.
20. GoffBA, Mandel LS, Drescher CW, et al. Development of an ovarian cancer symptom index: possibilities for earlier detection. Cancer. 2007 109(2):221-227.
21. Hibbard LT. Adnexal torsion. Am J Obstet Gynecol. 1985;152:456.
22. Young RH, Scully RE. Metastatic tumors of the ovary. In: Kurman RJ, ed. Blausteins Pathology of the Female Genital Tract. 5th Ed. New York, NY: Springer-Verlag; 2002.
23. Von Kuenssberg Jehle D, Stiller G, Wagner D. Sensitivity in detecting free intraperitoneal fluid with the pelvic views of the FAST exam. Am J Emerg Med. 2003;21(6): 476-478.
24. Koonings PP, Grimes DA, Campbell K, Sommerville M. Bilateral ovarian neoplasms and the risk of malignancy. Am J Obstet Gynecol. 1990;162(1):167-169.