Menorrhagia and Abnormal Vaginal Bleeding
Deborah S. Lyon
Most gynecology textbooks begin a discussion of abnormal vaginal bleeding by first carefully outlining the endocrinology of normal bleeding and then detailing various pathologic conditions that can lead to menorrhagia.
In addition, most texts clearly distinguish pregnancy-related bleeding from other vaginal bleeding problems and (depending on whether it is an obstetric or a gynecologic text) concentrate on only one of those categories.For the emergency department (ED) physician, however, the proper focus is the patient and the chief complaint. This is one of many processes in which the initial focus should be stabilization and appropriate categorization (i.e., obstetric, gynecologic, or gastrointestinal) with later emphasis on more precise diagnosis and pathology-specific therapy.
INITIAL EVALUATION AND STABILIZATION
Vaginal bleeding is a common ED complaint and may represent anything from a catastrophic, life-threatening hemorrhage to a normal menstrual period in an anxious patient. An algorithm for patient assessment is presented in Fig. 21.1. To begin an assessment of the severity of the bleeding, the most helpful starting point is the patient’s vital signs. Of particular importance is the pulse rate, because many young patients demonstrate a hyperdynamic pulse well before blood pressure is affected. Some patients can tolerate remarkable anemia with relatively unchanged vital signs, but this generally occurs when bleeding is of a chronic nature. Acute bleeding episodes of hemodynamic consequence manifest themselves in vital signs before blood counts, and these should be the foundation of the initial assessment. If the vital signs point to an acute and profound process, the patient should be managed as a trauma patient, with large-bore intravenous lines, fluid resuscitation, and rapid transfusion.
The patient’s history is extremely important.
Even though patients tend to exaggerate blood loss, semiquantitative evaluations such as pad counts and days of bleeding can be helpful in determining whether a vaginal bleeding episode is of clinical consequence. Of special concern is a patient whose stated history suggests less blood loss than her vital signs or her complete blood count (CBC) does; these patients may have a known problem, such as uterine leiomyomata, with a second hidden problem, such as gastrointestinal bleeding. Alternatively, the patient with an impressive history but normal vital signs may, in fact, be well compensated, and the CBC may be a better diagnostic tool.While collecting the vaginal bleeding history, particularly if the report does not seem to accurately reflect the clinical picture, information that might elucidate other sources of bleeding should be sought. This might include gastrointestinal symptoms, hematuria, a history of liver disease or chronic illness, and a family history of blood dyscrasia.
EXAMINATION OF A PATIENT WITH VAGINAL BLEEDING
Many women are reluctant to be examined when they are actively bleeding, although in the case of an ED visit, this is less often a problem. Nonetheless, it is helpful to explain to the patient what you hope to accomplish by performing a
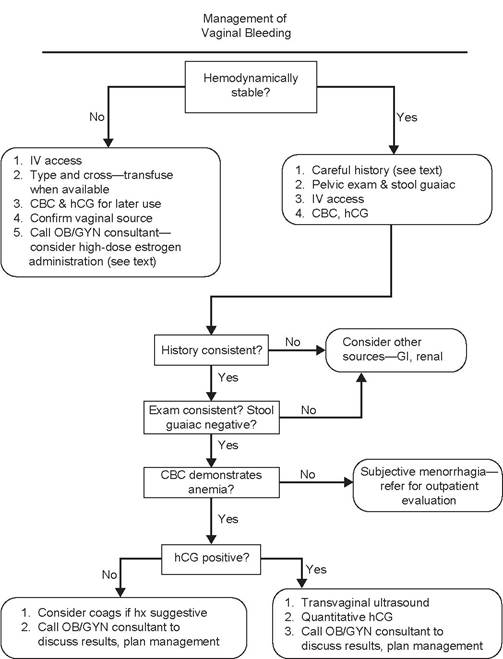
FIGURE 21.1 Menorrhagia and abnormal vaginal bleeding.
pelvic examination. This includes confirming the source ofthe bleeding, evaluating for areas of active bleeding, inspecting for anatomic abnormalities such as cervical lesions or large leiomyomata uteri, and evaluating for abdominal tenderness. In addition, a Hemoccult test should always be performed on a stool sample obtained with a fresh glove to avoid possible cross-contamination from the vagina.
Conventional medical practice places the performance of an examination before obtaining laboratory tests. It is helpful, however, to know the results of a urine pregnancy test before examining the patient, because it may focus the physical examination on a more narrow, differential diagnosis.
A detailed examination is important. Abdominal tenderness should be noted. Even in the absence of pregnancy or trauma, intra-abdominal bleeding is possible (as in the case of a ruptured corpus luteum cyst or diverticulum). Active bleeding should be recorded, as should a quantification of the amount of blood in the vault. Point sources of bleeding should be sought. The cervix should be carefully inspected for lesions as well as possible extruding products of conception. A bimanual pelvic examination should make a faithful attempt to identify the uterine size, recognizing that operator inexperience and patient body habitus may limit the utility of this step. Examiners who are not comfortable with the convention of sizing in comparison to weeks of pregnancy may use fruit (orange, grapefruit, honeydew, and watermelon) or sports equipment (golf ball, tennis ball, baseball, and basketball) to describe findings. Adnexal masses should be sought; although if ectopic pregnancy is on the differential diagnosis list, a vigorous adnexal examination is discouraged. Finally, a thorough rectal examination should be performed, with attention to palpable lesions, as well as Hemoccult testing.
ANCILLARY TESTING TO EVALUATE VAGINAL BLEEDING
Two laboratory tests are critical in the evaluation and management of vaginal bleeding: a CBC and a qualitative human chorionic gonadotropin (hCG) measurement. A quantitative hCG test is not necessary to establish the diagnosis of pregnancy, because most commercial qualitative kits are sensitive to 25IU. Most ectopic pregnancies do not become symptomatic until the hCG level reaches four-digit numbers, so a negative qualitative hCG makes ectopic pregnancy unlikely. Little diagnostic refinement and much delay result from conducting a quantitative test. There is a place for the quantitative test but not in the initial evaluation.
The CBC is useful in differentiating patients who are hemodynamically compromised from those who are well but concerned.
Experienced gynecologists may be surprised when, in the course of an outpatient evaluation of vaginal bleeding, they encounter a hemoglobin of 5 or 6. These numbers occur in patients whose menorrhagia is long-standing and who are relatively well compensated but, nevertheless, require prompt therapy. By the same token, it is common for a woman to be seen in the ED with menorrhagia as her chief complaint, yet her hemoglobin is 12 or 13. In the event of an impressively acute history and an examination compatible with profound acute loss, this hemoglobin may be thought of as spurious, because blood loss takes time to be reflected in the blood count. If the history and examination are less impressive, however, the patient may be assumed to be stable. It is important in this setting to validate the patient’s concern, which may be legitimate in light of her past experience, while still providing her the reassurance she needs to pursue a more problem-specific outpatient evaluation.The hCG serves a much more direct purpose. As mentioned earlier, many texts consider vaginal bleeding exclusively within the context of a positive or a negative hCG. A positive hCG demands a relatively immediate diagnosis, because therapy may be immediately necessary and will be tailored to the diagnosis.
If the hCG is positive for pregnancy, the likelihood is that either the pregnancy is intrauterine and threatening to abort or it is ectopically located. Physical examination may make this distinction, because incomplete spontaneous abortions often are seen with an open os and with tissue extruding. If physical examination is unrevealing, the next step in the workup is to identify the gestational age with reasonable assurance. This can sometimes be accomplished if the patient can confidently establish the date of her last menstrual period; often, laboratory testing is required. It is in this setting that a quantitative hCG is useful. Although not an accurate measure of gestational age per se, this test provides information regarding the quantity of hormone being produced, which is an indirect measure of fetal age as well as viability.
The primary value of this test in the acute setting is in the context of the discriminatory zone. This is a level above which a pregnancy, if intrauterine, can confidently be expected to be of such mass and development that it will be apparent on ultrasound. For most institutions with transvaginal ultrasound capability, this number ranges from 1,500 to 2,500IU (see Chapter 3). If the facility has only transabdominal ultrasound capability, the range jumps to approximately 6,500 IU, and many ectopic pregnancies will have already ruptured by that level. Thus, the ability to detect ectopic pregnancies early and to manage them optimally is dependent on the presence of both quantitative hCG and transvaginal ultrasound capability.A full bladder is not required for a transvaginal probe scan. This is helpful, because many patients find it difficult to fill their bladders sufficiently to form a good acoustic window for a first-trimester scan. However, when necessary, the bladder can be filled by administering intravenous fluids or placing a transurethral catheter that fills it retrograde.
Having emphasized the importance of technology in discriminating between intrauterine and extrauterine pregnancies, it should be repeated that this distinction can often be made on clinical grounds alone. Thus, the physical examination should always precede the ordering of a quantitative hCG or transvaginal probe ultrasound.
MANAGEMENT OF VAGINAL BLEEDING WITH A POSITIVE PREGNANCY TEST
Pregnancies with a quantitative hCG below the discriminatory zone must be evaluated strictly on clinical criteria. Certainly, an acute abdomen or a hemodynamically significant bleed must be addressed. On the other hand, a less significant bleed may be managed by observation and repeat quantitative hCG testing in 48 to 72 hours. This follow-up is best done by on obstetric care provider, and transfer of care may be arranged by telephone from the ED. It is important from a liability perspective that the ED provider documents explaining the differential diagnosis to the patient, along with the importance of keeping follow-up evaluation appointments.
If the patient is stable, management of ectopic pregnancy may be conservative (methotrexate): otherwise, management should be surgical. Management of a spontaneous abortion may include dilation and curettage versus expectant management with close follow-up (Chapters 3 and 8).Management of vaginal bleeding with a negative
PREGNANCY TEST
If the pregnancy test is negative, follow-up is determined by the patient’s clinical condition. In terms of additional testing, a coagulation profile may be considered if the patient has a history or stigmata of liver disease, has a family history of blood dyscrasia, or is an adolescent just beginning menstruation (a time when many bleeding disorders are diagnosed). It is probably not cost effective in other settings. A patient with profound hemodynamic changes, a very low hemoglobin, or brisk bleeding is best managed by admission, whereas a less acute blood loss may easily be managed by prompt outpatient evaluation.
Acute bleeding in the nonpregnant patient is managed by liberal use of intravenous fluid replacement and blood products. Products other than packed red cells should be reserved for use in accordance with institutional protocols rather than by a preset formula. Appropriate indications for replacement of platelets or cryoprecipitate might be a diagnosed dyscrasia, need for immediate surgery, or ongoing bleeding not responding to other medical management (listed below).
There have been many proposed interventions to stop uterine bleeding in the nonpregnant patient. The most common of these is high-dose estrogen, either intravenously or orally (1-3). Estrogen increases coagulation factors V and IX, increases platelet aggregation, and decreases capillary permeability. In addition, estrogen promotes rapid growth of the endometrium, thereby stabilizing bleeding at denuded surfaces. Older literature emphasized the use of intravenous preparations of up to 25 mg every 6 hours. More recent review shows lower and oral doses to be equally efficacious, and intravenous administration is largely limited to patients not tolerating oral intake or for whom oral estrogens induce profound nausea. Even though the possibility of an underlying estrogen-sensitive neoplasia is of concern, achieving hemodynamic stability takes priority. Once bleeding has been stopped, endometrial biopsy can be performed if indicated.
Oral estrogen use is less standardized than intravenous, and many regimens exist for its use. At our institution, we prescribe a 35-μg pill and instruct the patient to take four pills per day for 4 days, three pills per day for 3 days, two pills per day for 2 days, and then finish the remaining pack at one pill per day. The patient must be specifically instructed to discard the placebo pills in the first pack of pills. This tapered dose is intended to allow endometrial and hemodynamic restoration before estrogen withdrawal leads to another bleeding episode. It is highly effective in treating the acute bleeding episode. It is then up to the gynecologic provider to begin evaluation of the source of the bleeding and its optimal control.
Massive bleeding generally occurs in the setting of a cervical or endometrial malignancy, a prolapsing or necrosing fibroid, or a recent intervention such as curettage of an infected uterus. In any case, when the several hours necessary to achieve control through use of estrogen does not appear to be a viable option, four emergent options are available. The first is packing, either of the vagina, if bleeding is primarily cervical, or of the uterine cavity, if bleeding is coming from the uterus. Packing should be done with the goal of putting pressure on every bleeding point, so attention should be given to completely reaching all crevices with the packing material. This may be either ordinary laparotomy sponges or balloons such as a Foley catheter or ablation balloon. Various hemostatic agents have been used in association with the packing. One report from Jamaica described soaking the packing with formaldehyde (4), although at our institution we have used Monsel solution. This is readily available wherever colposcopy is performed and does not have the exposure risks associated with formaldehyde.
The second option is emergent endometrial ablation. This requires an anatomically intact cervical canal, so it cannot be used in cases of bulky tumor or prolapsing fibroid. Ablation can be done fairly quickly and has become quite routine as a management option for more indolent bleeding problems, but a case report has been published showing efficacy in the emergency setting (5), and there is some evidence of durable benefit even in cases of natural or iatrogenic (overanticoagulation) coagulopathies(6).
The third option, transported from more routine menorrhagia management into emergent management, is uterine artery embolization. This is not available at many institutions, and even where interventional radiology capabilities are present, the radiologist must be willing to respond emergently. This limits the utility of embolization. When used, however, it can be extremely successful and may also be employed even in the face of common dyscrasias such as disseminated intravascular coagulopathy and von Willebrand’s disease. Response is quite rapid, and in experienced hands, the complication rate is relatively low. In the one retrospective series of embolizations, fertility appeared to be spared despite occlusion of both uterine arteries (7), although pregnancy is not recommended due to case reports of growth restriction and other vasculopathy-related complications of pregnancies subsequent to uterine artery embolization (8).
Finally, emergent hysterectomy may be required. Packing will usually provide enough time to call in appropriate surgical support and transport the patient to the operating theater. Except in the immediate postpartum period, the requirement for a truly emergent hysterectomy is relatively uncommon.
In summary, management of vaginal bleeding is as follows:
Assess vital signs
Take a thorough history
Perform a rapid qualitative hCG test
Perform a thorough physical examination with stool guaiac
Obtain a CBC and, if indicated, coagulation studies
If indicated, order a quantitative hCG and transvaginal ultrasound
Control bleeding, if necessary, via fluid resuscitation, transfusion, surgical intervention (dilation and curettage for incomplete abortion and laparoscopy or laparotomy for intra-abdominal hemorrhage), mechanical tamponade, and pharmaceutical management.
LONG-TERM MANAGEMENT GOALS IN MENORRHAGIA
Control of heavy vaginal bleeding is readily achieved in the acute setting by use of the aforementioned steps. In the patient who is not pregnant and who does not have a vaginal or cervical laceration (the true menorrhagia patient), bleeding tends to recur unless long-term management goals are established. Although these are frequently undertaken in the gynecologist’s office, the possible outcomes and goals are of interest to the ED physician for two reasons. First, it is important to know what potential options the patient may have, so that she may be appropriately counseled. There should be no need for the frustrated patient in the gynecologist’s office saying, “But the emergency doctor told me I needed a hysterectomy,” when the gynecologist has simply prescribed an increase in the patient’s thyroid medication dose. Second, there may be a relatively high rate of return to the ED in some populations, particularly in urban indigent care centers (9). Thus, the ED physician becomes de facto part of the patient’s continuity care team. Understanding the therapeutic plan provides considerable assistance in dealing with recidivism.
Management of menorrhagia depends on its source. There are four common areas of possible dysfunction leading to menorrhagia (Table 21.1). Thinking in terms of these compartments allows an orderly workup and management of the patient’s bleeding.
CytologicZArchitectural Bleeding
Bleeding of cytologic/architectural origin includes cervical and uterine cancers, as well as endometritis, leiomyomata, and polyps. Diagnostic evaluation mandated for all menorrhagia patients starts with a Papanicolaou smear and endometrial biopsy. If there are any suspicious lesions on the cervix, they should be biopsied as part of the initial evaluation. Cervical cytology is designed as a screening tool and carries a relatively high false-negative rate (10), so it should not replace visual inspection and biopsy of abnormal-appearing areas. Large leiomyomata should be appreciable on bimanual examination, but significant menorrhagia may result from relatively small fibroids if they are submucous. Thus, a sonohysterogram may be helpful. This involves cannulating the cervix and injecting sterile saline into the uterine cavity while performing ultrasound. An acoustic window is developed by the sterile saline, which clearly demonstrates intracavitary lesions. These may then be managed via hysteroscopic resection versus hysterectomy, depending on the size of the lesion and the childbearing wishes of the patient. Uterine artery embolization has become a well-accepted alternative

Causes of Menorrhagia
ArchitecturalZCytologic
Cervical cancer
Endometrial cancer/hyperplasia
Endometritis
Leiomyomata
Polyp
Cervical tr auma
Endocrine
Polycystic ovarian syndrome
Excessive exogenous estrogen use
Excessive endogenous estrogen production or storage (ovarian tumor and obesity)
Hypothyroidism
Hyperthyroidism
Hyperprolactinemia
Hypothalamic—major changes in weight or exercise status, perimenopause
Systemic
Hemophilia
von Willebrand's disease
Thrombocytopenia (idiopathic or autoimmune)
Leukemia
Pancytopenia (immunosuppression, chemotherapy, and bone marrow suppression) Anticoagulation (iatrogenic)
Idiopathic Menorrhagia
to surgery in many instances and is an ideal option for patients with increased surgical risks. Its primary drawback, as noted above, is the requirement for a skilled interventional radiologist, which may not be possible in all areas. Malignancies must be staged, and management may include surgery or radiation.
Endocrine Bleeding
Bleeding of endocrine origin includes polycystic ovarian syndrome and hypo- thalamic/pituitary disorders. Menorrhagia is typically associated with estrogen excess, whereas estrogen deficiency may cause amenorrhea or irregular spotting. This explains why many patients on depot medroxyprogesterone for contraception spot irregularly (progestins stabilize estrogen exposure and, at high doses, may be considered relatively antiestrogenic). Hypothalamic/pitu- itary disorders most often fall into the hypoestrogenic category, so that anorectics, athletes, and patients with prolactinomas rarely have menorrhagia. Polycystic ovarian syndrome, on the other hand, is a relatively hyperestro- genic state. These patients often have very irregular periods and may only bleed once or twice a year, but those periods may be of profound hemodynamic consequence. Although the chain of endocrine events behind this syndrome is complex, the critical issue in this context is the loss of cyclic hormonal surges and suppressions in the face of normal or supranormal amounts of estrogen. The regular withdrawal bleeding that should be induced by an appropriate pattern of hormone secretion is lost, but estrogen continues to stimulate endometrial cell proliferation. Thus, a very thick endometrium is developed, which eventually outgrows its blood supply, causing sloughing and menorrhagia.
Endocrine bleeding is often a diagnosis of exclusion, presumed to be the source of menorrhagia when no architectural/cytologic abnormality is identified. Two blood tests are important, however, to make specific diagnoses. These are prolactin and thyroid-stimulating hormone levels. Hypothyroidism and hyperthyroidism can cause menorrhagia by influencing the feedback loop to the hypothalamus, driving follicle-stimulating hormone and luteinizing hormone levels up. Prolactin may be artifactually elevated in this case, so thyroid disease should always be sought and treated before evaluation for a prolactinoma. Hyperprolactinemia in the absence of thyroid disease is fairly common in women of reproductive age and is often treatable by simple means, so testing for it should not be overlooked.
Virtually all sources of endocrine bleeding problems are managed similarly in the patient not desiring immediate pregnancy. The use of oral contraceptives suppresses and eliminates the need for regular signals from the hypothalamic- pituitary-ovarian axis and provides regular hormonal stimulation and withdrawal, so that an orderly bleeding pattern can be developed. Most patients with exclusively endocrine-mediated bleeding problems are able to establish a normal bleeding pattern on an oral contraceptive regimen without the need for surgical intervention, and it is currently a standard of care in the gynecologic community to attempt medical management of bleeding before undertaking surgical management. Medical management may also be attempted if the patient has fibroids, because it is not uncommon for a patient to have both architectural and endocrine abnormalities. Upon correction of the endocrine abnormalities, the architectural distortion may become clinically irrelevant (11).
An exception to the rule of oral contraceptive use is in the case of the patient with high prolactin levels (12). These patients may have pituitary macroadenomas, and further imaging is indicated to rule out extrinsic compression of the sella turcica or optic chiasm. A more specific treatment such as bromocriptine may be indicated instead of or in addition to oral contraceptives in these patients. A second category of patients who should not receive oral contraceptives is those for whom they are relatively contraindicated (13). This includes patients with a history of prior deep venous thrombosis, severe hepatic disease, or cerebrovascular accident, as well as obese women, hypertensives, and smokers older than 35 years (because estrogen, age, and each of these are multiplicative risk factors for thrombogenesis). For these patients, menorrhagia can be effectively controlled with depot medroxyprogesterone, but there is a high likelihood of persistent spotting. Long-term use of high-dose progestins has also been associated with early onset of osteopenia, so the benefits of medical therapy must be weighed against its risks. Recent evidence supports use of local progestin therapy in the form of the levonorgestrel-releasing intrauterine system (Mirena®) for excellent long-term control of abnormal uterine bleeding with minimal side effects and a high degree of patient satisfaction (14,15).
SYSTEMIC CAUSES OF BLEEDING
The third category of menorrhagia sources is systemic. The most obvious are the bleeding dyscrasias. Congenital bleeding disorders may be diagnosed in a young teenager who is seen for a life-threatening hemorrhage from her first period. Many of these patients are proven to have von Willebrand’s disease (relatively common) or a variant of hemophilia (extremely uncommon). It is rare to diagnose congenital coagulopathies in older patients, but secondary coagulopathies from liver disease or bone marrow suppression should not be overlooked if the patient’s history is suggestive. Appropriate diagnosis depends on a high index of suspicion, because clotting function testing is not recommended routinely. A special subset of this category is the iatrogenic menorrhagia caused by anticoagulation therapy. It is not unusual for a patient on warfarin therapy to have very heavy bleeding, particularly if she becomes overanticoagulated. The best management for this type of bleeding is to hold one or more doses of warfarin and adjust the desired therapeutic window downward. It is rare for coagulopathies to require surgical intervention. The primary mechanism of hemostasis in menstruation is mechanical (constriction of the myometrial muscle) rather than hematologic. Menstrual bleeding in these patients is often a nuisance but not of profound hemodynamic consequence. This is particularly important to remember, because these patients are obviously suboptimal operative candidates as well.
IDIOPATHIC MENORRHAGIA
The fourth category of menorrhagia is idiopathic. This is a diagnosis of exclusion made when architectural abnormalities are ruled out and the patient fails to resume a normal bleeding pattern when exposed to three or more cycles of oral contraceptive management. These patients may have very high endogenous levels of estrogen or simply endometrial receptors that are exquisitely sensitive to estrogen. This is an uncommon category, and most patients who complain of persistent menorrhagia after exclusion of the aforementioned diagnoses are found to have a normal hemoglobin. Thus, it is the perception of the patient that her menstruation is excessive, but objectively, she is maintaining adequate hematopoiesis. These patients can be demanding; nevertheless, a policy of nonintervention is in the physician’s best interest, because any untoward outcome from therapy is likely to be weighed against the therapeutic benefit of the therapy. The ED physician should keep in mind that repetitive somatic complaints, particularly gynecologic ones, have been associated with a history of or current domestic violence in some studies (16-18). Sensitively offered questions on this topic may allow appropriate diagnosis and referral.
If the objective findings support the patient’s claim of menorrhagia, she may be offered endometrial ablation versus hysterectomy. Endometrial ablation may also be appropriate for the patient with endocrine problems discussed earlier but should be undertaken with caution in that category, because ablation does not destroy all the endometrial glands, and the continued hyperestrogenic state may increase the patient’s risk of subsequent endometrial carcinoma. Ablation should only be undertaken in women who have no further childbearing desires, and its long-term success rate (measured as no further need for intervention) is approximately 60% to 85%, with typical short-term satisfaction rates in the range of 90% to 95% (19). Levonorgestrel-releasing intrauterine systems may be a highly satisfactory choice in the setting of iatrogenic menorrhagia as well (14,15).
SUMMARY
In summary, menorrhagia may be due to any of several causes, which should be sought and treated specifically. Even though removal of the endometrium via hysterectomy ultimately solves all cases of uterine bleeding, this treatment is imprecise at best and carries a significant risk of iatrogenic morbidity. With a little patience and a small armamentarium of tests, the physician can confidently establish a diagnosis and undertake specific treatment. Surgical management should be reserved for the patient who will clearly not respond well to more conservative management. This includes the patient with significant anatomic distortion or high-grade cytologic derangements, the patient who has failed medical management, and the patient whose compliance with medical management is poor enough that she is repetitively exposed to major hemodynamic insults.
References
1. DeVore GR, Odell O, Kase N. Use of intravenous Premarin in the treatment of dysfunctional uterine bleeding: a double-blind randomized control study. Obstet Gynecol. 1982;59:285-291.
2. Bayer SR, DeCherney AH. Clinical manifestations and treatment of dysfunctional uterine bleeding. JAMA. 1993;269:1823-1828.
3. Chuong CJ, Brenner PF. Management of abnormal uterine bleeding. Am J Obstet Gynecol. 1996;175:787-792.
4. Fletcher H, Wharfe G, Mitchell S, Simon T. Treatment of intractable vaginal bleeding with formaldehyde soaked packs. JObstet Gynecol. 2002;22(5): 570.
5. Nichols CM, Gill EJ. Thermal balloon endometrial ablation for management of acute uterine hemorrhage. Obstet Gynecol. 2002;100:1092-1094.
6. El-Nashar SA, Hopkins MR, Feitoza SS, et.al. Global endometrial ablation for menorrhagia in women with bleeding disorders. Obstet Gynecol. 2007;109:1381-1387.
7. Ornan D, White R, Pollak J, Tal M. Pelvic embolization for intractable postpartum hemorrhage: long-term follow-up and implications for fertility. Obstet Gynecol. 2003; 102:904.
8. Usadi RS, Marshburn PB. The impact of uterine artery embolization on fertility and pregnancy outcome. Curr Opin Obstet Gynecol. 2007;19(3):279-283.
9. Lyon DS, Ballard L, Jones JL. A retrospective review of inpatients with menometror- rhagia: etiologies, treatments, and outcomes. SouthMedJ. 2000;93(6):571-574.
10. DiSaia PJ, Creasman WT, eds. Clinical Gynecologic Oncology. 5th Ed. St. Louis, MO: Mosby; 1997.
11. ACOG Practice Bulletin No. 96. Alternatives to hysterectomy in the management of leiomyomas. August 2008.
12. SperoffL, Glass RH, Kase NG, eds. Clinical Gynecologic Endocrinology and Infertility. 5th Ed. Philadelphia, PA: Williams & Wilkins; 1994.
13. ACOG Practice Bulletin No. 73. Use of hormonal contraception in women with coexisting medical conditions. June 2006.
14. Rauramo I, Elo I, Istre O. Long-term treatment of menorrhagia with levonorgestrel intrauterine system versus endometrial resection. Obstet Gynecol. 2004;104: 1314-1321.
15. Busfield RA, Farquhar CM, Sowter MC, et.al. A randomised trial comparing the levonorgestrel intrauterine system and thermal balloon ablation for heavy menstrual bleeding. BJOG. 2006;113:257-263.
16. Fillingim RB, Wilkinson CS, Powell T. Self-reported abuse history and pain complaints among young adults. Clin J Pain. 1999;15(2):85-91.
17. Jamieson DJ, Steege JF. The association of sexual abuse with pelvic pain complaints in a primary care population. Am J Obstet Gynecol. 1997;177(6):1408-1412.
18. Reiter RC, Shakerin LR, Gainbone JC, et al. Correlation between sexual abuse and somatization in women with somatic and nonsomatic chronic pelvic pain. Am J Obstet Gynecol. 1991;165(1):104-109.
19. Feitoza SS, Gebhart JB, Gostout BS, Wilson TO, Cliby WA. Efficacy of thermal balloon ablation in patients with abnormal uterine bleeding. Am J Obstet Gynecol. 2003; 189:453.
More on the topic Menorrhagia and Abnormal Vaginal Bleeding:
- Menorrhagia and Abnormal Vaginal Bleeding
- CONTENTS
- 40 Abnormal Uterine Bleeding
- Abnormal uterine ∖bleeding
- Endometrial polyps
- Benrubi Guy I. (ed.). Handbook of Obstetric and Gynecologic Emergencies. 4th edition. — Lippincott Williams & Wilkins,2010. — 424 p., 2010
- Pathogenesis
- REFERENCES
- Chapter 15 Common gynaecological procedures and surgery
- 37 Uterine Leiomyomas