Pathogenesis
The natural course of C. trachomatis infection and ability of individuals to naturally clear infection is incompletely understood. Studies have shown that approximately half of asymptomatic infections are cleared spontaneously at 1 year after initial chlamydia testing.
However, most chlamydia natural history studies lack data on when the infection was initially acquired, or whether subsequent detection is persistent or new (32). There is also a lack of consensus regarding the risk of PID following untreated cervical chlamydia infection. However, a recent synthesis of the data from screening trials suggests 14.9% of women will go on to develop symptomatic PID (Figure 43.3), and 17.1% of infections if both symptomatic and asymptomatic PID is considered (19). This proportion may be significantly increased by the iatrogenic introduction of organisms into the upper genital tract by procedures involving transcervical instrumentation such as insertion of intrauterine contraceptive devices, hysterosalpingography, hysteroscopy, in vitro fertilization, and termination of pregnancy.The mechanism by which microorganisms ascend spontaneously along the mucosal surfaces from the vagina and cervix to the upper genital tract is unknown. Disruption of the physical mucous barrier, which under normal circumstances would protect the upper genital tract, may be influenced by both microbial and physiological hormonal changes during the menstrual cycle. Both chlamydia and gonorrhoea are known to possess proteolytic enzymes which degrade cervical mucous and associated antimicrobial peptides (33). Physiologically, the cervical mucous barrier will not be as effective during menstruation when the mucous plug is expelled. Similarly, it is likely there is a higher risk of infection at mid cycle, when oestrogen levels are high and progesterone levels relatively low, leading to physiological thinning of the cervical mucous.
Endometrial detection of gonorrhoea and chlamydia is more frequent in the proliferative phase of the menstrual cycle. Additionally, at this stage uterine contractions switch from principally ‘fundo-cervical’ to ‘cervico-fundal’, favouring transport of sperm, and pathogens, towards the upper genital tract (34).There is also likely to be an immunological component linked to both virulence of the organism and host factors such as human leucocyte antigen class. While some women clear C. trachomatis infection without tissue damage, in others, chlamydia induces a chronic low- grade inflammation. There is almost certainly a role for chlamydia virulence proteins (surface-exposed polymorphic membrane proteins or Pmp) which have been shown to stimulate proinflammatory cytokines and induce different antibody responses with variable effects on the degree of inflammation. In one study, women with a genetic predisposition to a higher expression of PmpA antibody had increased inflammatory markers and decreased pregnancy rates and live births (35).
In gonococcal disease, antibody binding to structural components of the gonococcal surface (lipooligosaccharide and peptidoglycan) activates complement and initiates the prostaglandin cascade in the fallopian tubes. It is important to consider that the diameter of the fallopian tubes varies considerably, but is particularly narrow ((2).
Clinical features when present include:
• recent onset of bilateral lower abdominal pain, often described as constant, dull, aching, or cramping
• deep dyspareunia—particularly of recent onset
• abnormal vaginal bleeding—particularly intermenstrual bleeding, postcoital bleeding, or menorrhagia, secondary to associated cervicitis and endometritis
• mucopurulent vaginal discharge—as a result of associated cervicitis
• cervical motion, uterine, and/or adnexal tenderness on bimanual vaginal examination.
The presence of one or more of the following additional criteria will improve the specificity of the minimum criteria:
• Temperature higher than 38.3°C
• Abnormal cervical mucopurulent discharge or cervical friability
• Presence of abundant numbers of white blood cells on saline microscopy of vaginal fluid
• Elevated erythrocyte sedimentation rate; elevated C-reactive protein (41)
• Laboratory documentation of cervical infection with N.
gonorrhoeae, C. trachomatis, or M. genitalium.
Figure 43.5 Hysterosalpingogram demonstrating left salpingitis isthmica nodosa and right hydrosalpinx.
Reproduced with permission from Mr Peter Greenhouse, Bristol Sexual Health Centre.
The absence of endocervical or vaginal pus cells has a good negative predictive value (95%) for a diagnosis of PID but their presence is non-specific (poor positive predictive value of 17%) (42).
Fever of greater than 38°C can occur, but systemic manifestations are not a prominent feature in patients with mild to moderate PID. Infection and inflammation may spread from the pelvis to the liver capsule via the right paracolic gutter. This is thought to affect 4-14% of women and presents with right upper quadrant pain secondary to perihepatitis (Fitz-Hugh-Curtis syndrome). Subsequent adhesions may form between the liver capsule and the diaphragm, classically described as ‘violin string’ adhesions (Figure 43.6).
The presence and severity of PID symptoms varies by microbiological aetiology. Women with gonococcal PID are more likely to
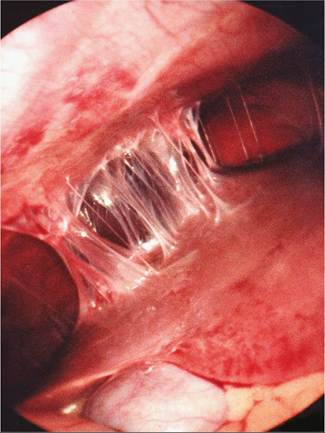
Figure 43.6 Laparoscopic appearance of the Fitz-High-Curtis syndrome showing 'violin string' adhesions between liver capsule and subdiaphragmatic peritoneum with a normal gallbladder.
Reproduced with permission from Mr Peter Greenhouse, Bristol Sexual Health Centre.
have raised systemic inflammatory markers including erythrocyte sedimentation rate and white blood cell count than those with PID caused by chlamydia or mycoplasma. Women with gonococcal PID are also more likely to present with fever, mucopurulent cervicitis, and adnexal tenderness with a higher pelvic pain score (39, 43-46). This may explain why in the PEACH study women with PID associated with N. gonorrhoeae presented to care almost 1 week earlier than women with C. trachomatis or M. genitalium (47). Women with gonococcal PID are also more likely to remember the episode. Miettinen et al. reported that half of the infertile women with positive gonococcal serology recalled a prior episode of PID, compared to only one-quarter of those with positive chlamydia or mycoplasma serology (38). As rates of N. gonorrhoea infection have continued to fall in many countries, atypical, milder clinical manifestations have become more common (2, 40, 48).