Aetiology/microbiology
PID has classically been associated with the STIs Neisseria gonorrhoeae and C. trachomatis. Studies in the 1980s and 1990s detected chlamydia and/or gonorrhoea from over 50% of cases (1517) and in up to 77% of tubo-ovarian abscesses at laparoscopy (18).
More recent literature suggests the proportion of PID cases attributable to N. gonorrhoeae or C. trachomatis is declining. Price et al. using multiparameter evidence synthesis estimated that in England in 2002, 35% of PID cases in women aged 16-24 years were due to chlamydia, compared to only 20% of women aged 16-44 years (19). In 2011, in patients diagnosed with PID in an emergency department in North America, Burnett et al. found only 4.4% with gonorrhoea, 10% with chlamydia, and 2.6% of individuals with both organisms (11). This left 83% of cases with no identified organism. This would fit with the overall decrease in prevalence of gonorrhoea in some populations, and also the increase in chlamydia screening. Furthermore, as care has shifted to the outpatient setting, invasive tests are less frequently performed with a possible concomitant reduction in rates of organism identification.Identifying which other organisms are implicated in the pathogenesis of PID is problematic. Firstly it must be considered whether the upper female genital tract is normally sterile. There is some evidence that some microorganisms may be present in healthy, asymptomatic individuals. Even when identified, the role these organisms may play in the disease process is not understood.
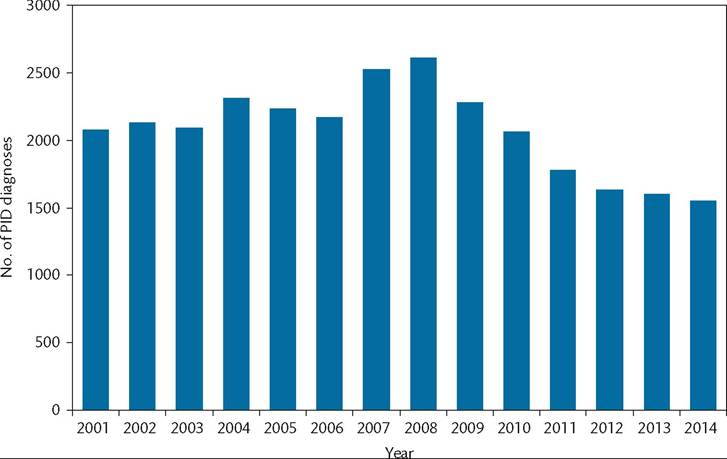
Figure 43.2 PID caused by C. trachomatis diagnosed in England 2001-2014.
Source data from https://www.gov.uk/government/statistics/sexually-transmitted-infections-stis-annual-data-tables.
Acute PID is now considered a polymicrobial infection with involvement of a wide variety of microorganisms, many of which are not routinely tested for in clinical practice.
This may explain why a large proportion of clinical PID cases have unidentified microbiological aetiology. Included among these are genital tract mycoplasmas (particularly M. genitalium) and anaerobic/aerobic bacteria which comprise the endogenous vaginal flora (e.g. black-pigmented Gram-negative anaerobic rods, Gardnerella vaginalis, Escherichia coli, Haemophilus influenzae, and aerobic streptococci). Using newer identification techniques, Hebb et al. obtained fallopian tube samples at laparoscopy from Kenyan women with salpingitis, as well as control subjects having tubal ligation (4). Using a broad range 16s rDNA polymerase chain reaction they identified novel, possibly uncultivatable bacteria from fallopian tube specimens in the women with salpingitis. These were sometimes the sole or predominant phylotype. In addition to N. gonorrhoeae and C. trachomatis, implicated microorganisms included Leptotrichia spp., Atopobium vaginae, Prevotella spp., Peptostreptococci spp., and Streptococcus pyogenes.The exact role of anaerobic bacteria and BV in the pathogenesis of PID remains unclear. Lactobacilli are important in the host defence against STIs, and BV has been shown to increase the risk of incident gonorrhoea and chlamydial infection (20). BV has also been noted to be frequently present in women with PID (up to 70%). But whether BV-associated bacteria independently cause PID, whether they facilitate the ascension of N. gonorrhoeae or C. trachomatis infection, or whether they are simply innocent bystanders following infection with other pathogens are yet to be determined. There are data, however, which suggest anaerobes are capable of causing local tissue damage at the level of the fallopian tube when present (21). The proportion of women with PID who have anaerobes isolated at laparoscopy ranges from 13% to 78% (20). The wide differences are thought to be related to diverse patient populations, different definitions of PID, varying degrees of disease severity, and different microbiological techniques.
Several studies have investigated the role of BV in endometritis or clinically suspected PID. The only prospective study showed no increase in the risk of developing incident PID in women with BV over a 3-year period (22). This study used standard Gram-stained slides and microscopy for the BV diagnosis. However, 1 year later the same authors concluded that women with a heavy growth of BV- associated microorganisms and a new sexual partner appeared to be at particularly high risk of PID (adjusted rate ratio 8.77; 95% confidence interval (CI) 1.11-69.2) (23). Several other studies have also found an association with the presence of anaerobic Gram-negative rods, independent of chlamydia or gonorrhoea infection (24, 25). The differences in these findings have been explained by variable definitions of BV. Although BV as determined by Gram stain is relatively reliable, it does not capture all the microbiological components of the BV ecosystem, in particular anaerobic Gram-negative rods. So when BV was identified by microbial culture, a combination of BV- related microorganisms was shown to significantly increase the risk of acquiring PID (23). There is substantial evidence that anaerobic infection is associated with more severe disease, in particular the formation of tubo-ovarian abscesses (26).
M. genitalium was first identified in the early 1980s in men with non-gonococcal urethritis. The organism was extremely difficult to isolate from clinical specimens, prompting the development of nucleic acid amplification tests (NAATs) which have improved the understanding of pathogenesis and the association with disease processes. M. genitalium has been shown to be sexually transmittable in partner studies which demonstrate concurrent infection with concordant strain types (27). Infection with M. genitalium is as common as C. trachomatis among high-risk women and women with clinical PID, with rates ranging from 2.1% to 16% (28, 29). Studies have increasingly shown an association with cervicitis, PID, and infertility.
An independent association was shown in women with histologically confirmed endometritis who were significantly more likely to have M. genitalium detected than women without endometritis (16% vs2%; P = 0.02) (30). Similarly, in the PID Evaluation and Clinical Health (PEACH) study women testing positive for M. genitalium were more than twice as likely to have histologically confirmed endometritis compared to women without infection (29). More recently, a meta-analysis looking at M. genitalium infection and female reproductive tract disease showed this organism is associated with a significantly increased risk of PID, with a pooled odds ratio (OR) of 2.14 (95% CI 1.31-3.49) (31). Women also had an increased risk of cervicitis (OR 1.66; 95% CI 1.35-2.04), preterm birth (OR 1.89; 95% CI 1.25-2.85), and miscarriage (OR 1.82; 95% CI 1.10-3.03). A significant association between M. genitalium and PID has implications for current testing algorithms and recommended therapies which specify the use of antibiotics with poor efficacy against this organism.
More on the topic Aetiology/microbiology:
- Aetiology/microbiology
- Fallopian tube
- Arulkumaran S., Ledger W., Denny L., Doumouchtsis S. (eds.). Oxford Textbook of Obstetrics and Gynaecology. Oxford University Press,2020. — 928 p., 2020
- 5 Appendices
- CHAPTER 41 HARMFUL ALGAL BLOOMS INCLUDING Cyanobacterial toxicosis
- AVIAN CHOLERA
- CHAPTER 38 ASPERGILLOSIS