Epidemiology
Accurate measures of PID incidence are difficult to obtain due to the asymptomatic and non-specific nature of many cases. To further complicate matters, symptomatic patients present to a variety of services including primary care, gynaecology, and sexual health clinics.
This makes precise case-finding challenging and almost certainly leads to widespread under-reporting.Examination of general practice-b ased morbidity surveys in England and Wales in 1991-1992, revealed a diagnosis of PID was made in women aged 16- 46 at 1.7% of attendances (6). Over the past decade rates have fallen by over 50%. Using data from the Clinical Practice Research Datalink, rates of definite or probable PID in 15- 44-year-old women attending general practice decreased in England by 9% per year (from approximately 400:100,000 to 180:100,000) between 2000 and 2011. The reduction was seen in all age groups but was most marked in women aged 15-24 years (Figure 43.1) (7).
In the United States there were 1.2 million medical visits for PID in 2000. Here too, the number of annual visits to physicians for PID among women aged 15-44 years has decreased by 39.8% (from 123,000 visits in 2004 to 88,000 visits in 2013) (8). In Canada between 1992 and 2009, PID hospitalizations decreased by 80% and physicians billing for cases of PID decreased by 70% (9). Similar data have been reported from other countries including Sweden, Australia, and Denmark (10).
During this time, all these countries have witnessed an increase in chlamydia diagnoses, partly due to changing sexual behaviour, but also due to increased detection rates through widespread screening.
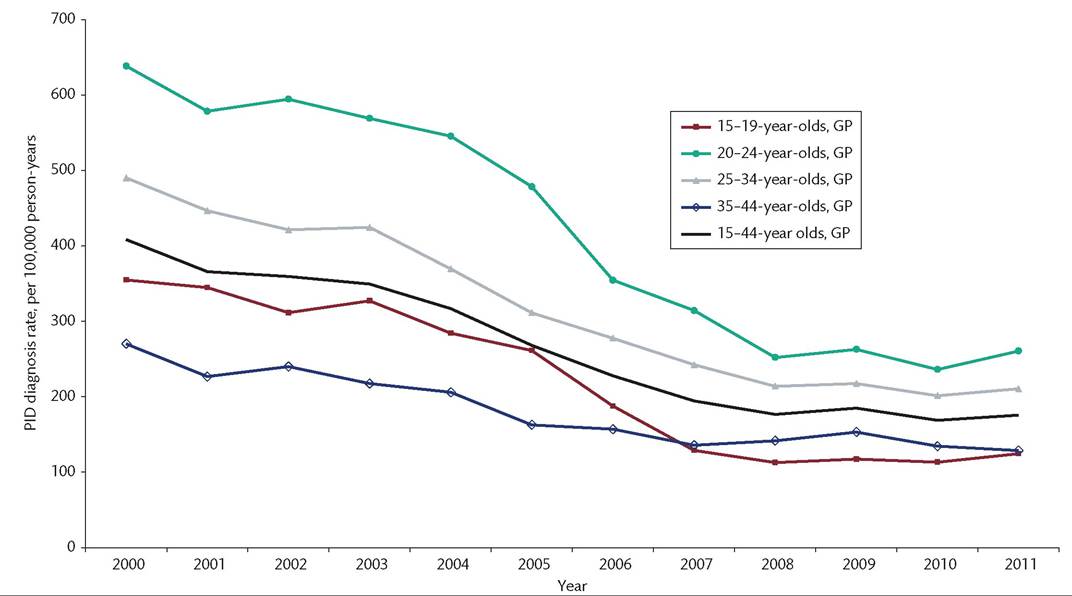
Figure 43.1 PID diagnosis rate by Public Health England centre recorded in general practice (GP) settings from 2000 to 2011.
Source data from Public Health England.
Rates of pelvic inflammatory disease (PID) in England (2000-2013). HPR 2015;9:22.By decreasing prevalent infection and diagnosing chlamydia at an earlier stage, the risk of progression from simple cervical infection to PID is reduced. Data from randomized controlled trials of chlamydia screening to prevent PID have provided evidence that screening and treatment is a useful intervention, although these studies are not without limitations, and the magnitude of their contribution remains unclear. Certainly the number of cases of PID caused by Chlamydia trachomatis seen in many countries has fallen, with chlamydia detected in as few as 10% of cases (11). If chlamydia- associated PID continues to fall, the impact chlamydia screening programmes will have on PID incidence in future may need reevaluating (Figure 43.2).
The estimated medical costs of treating PID range from $700 to $8480 per episode for outpatient and inpatient care respectively (12). Indirect costs relating to sequelae are far higher, and the estimated annual healthcare cost for PID and its complications in the United States is over $2 billion (13).
Risk factors for PID are the same as risks for acquiring STIs. These include unprotected sexual intercourse with multiple sexual partners, young age at onset of sexual activity, previous chlamydia or gonorrhoea infection, low socioeconomic status, lower educational attainment, and a history of PID. Vaginal douching had been previously linked to PID in retrospective studies; however, a prospective study in 2005 showed no causal link. The authors suggested that previous associations had been driven by the symptoms of a genital infection prompting douching, rather than douching causing PID (14).