Torsion of Ovary
Mehdi Parva and Charles J. Dunton
Causes of acute abdominal pain unique to women include pelvic inflammatory disease, ectopic pregnancy, endometrioma, rupture or hemorrhage of a corpus luteum cyst, and torsion of adnexal structures (1).
Although uncommon, adnexal torsion is not rare and comprises approximately 3% of surgical emergencies in women (2). Diagnosis of this condition is challenging. Prompt diagnosis may allow for preservation of the adnexal structures and fertility.ETIOLOGY
Torsion of the adnexa is caused by rotation of the ovary or the adnexa about the ovarian pedicle, resulting in arterial, venous, or lymphatic obstruction (Fig. 23.1). Initially, the venous and lymphatic obstruction without arterial obstruction produces edema and enlargement of the ovary. If arterial obstruction occurs, the organs may become necrotic and gangrenous. This in turn may lead to peritonitis and intestinal obstruction. In some cases, the twisted adnexa may be absorbed, leading to unilateral absence of the adnexa. Torsion of the fallopian tube alone is rare and has been associated with hydrosalpinx, neoplasms of the tube, and previous tubal ligation (2-5) (Fig. 23.2). Torsion of the adnexa is increased in ovarian hyperstimulation syndrome (OHSS) caused by menotropin therapy for infertility (6-8).
Pregnancy has been associated with an increased risk of adnexal torsion (9,10). If an adnexal mass is associated with a pregnancy, a recent review found that the most frequent complication was torsion (11). This may be due to the repositioning of the ovaries by the enlarging uterus. Torsion is most likely in the first trimester (10,12).
Torsion of the adnexa may involve the ovary, the fallopian tube, or both structures together. In most cases, an ovarian neoplasm is involved (9). Nonetheless, in up to 18% of cases, the torsion may involve normal tubes and ovaries.
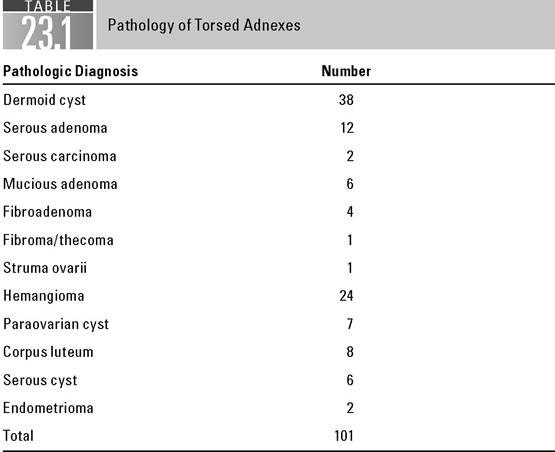
In keeping with the age of the patient population, the neoplasms are usually benign (Table 23.1). The most common neoplasm is the dermoid cyst. Paraovarian cysts have the highest relative risk of torsion (9,13).It is unusual for malignant neoplasm to present with symptoms of torsion. A review of 10 years’ experience at the Women’s Hospital, Los Angeles County, showed only two cases of malignant neoplasms undergoing torsion. In comparison, the relative risk for a benign neoplasm to undergo torsion was 12.9% (95% CI, 10.2 to 15.9) (14,15). However, if a postmenopausal woman presents with torsion, clinicians should consider the possibility of malignancy. In series with a high percentage of malignancy reported with torsion, most patients were postmenopausal (13,16). Postmenopausal patients also had a delayed diagnosis compared to younger patients (13).
Torsion of a normal ovary may present as a massive ovarian edema. This tumor-like condition presents with significant ovarian enlargement and pathologically shows only edema of a normal ovary (17).
CLINICAL FEATURES
The clinical diagnosis of adnexal torsion is often difficult. It occurs mainly in young women and less frequently in children and postmenopausal females. Pain,

FIGURE 23.1 Torsion of infundibulopelvic ligament.

FIGURE 23.2 Torsion of the adnexa.
Source. With permission from Lomano JM, Trelford JD, Ullery JC. Torsion of the uterine adnexa causing an acute abdomen. Obstet Gynecol. 1970;Vol.no. 35, issue.no. 2.
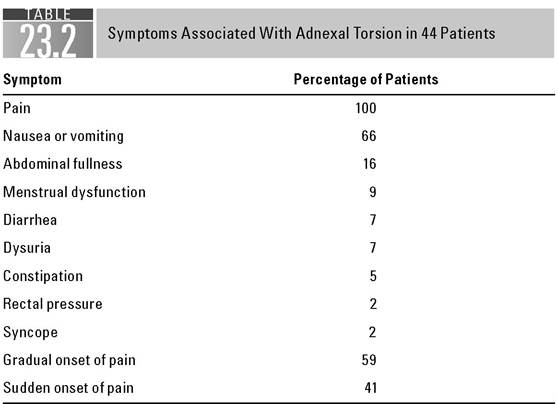
low-grade temperature, moderate leukocytosis, and nausea and vomiting (70%) are present in most cases. The pain associated with torsion may be unilateral or bilateral (25%) and either intermittent or constant.
The pain may be acute, in onset, and may be associated with a vigorous activity or a change in position. The pain may be out of proportion to other findings. Later in the course, if necrosis occurs, high fever and marked leukocytosis may be seen (17-20) (Table 23.2). Symptoms may be present for a number of days prior to the patient seeking medical attention, and physician delay prior to surgical treatment is not uncommon. Reviews showed that the median onset of pain was 1 day, but the range was 0 to 210 days, with a median of 7 to 8 days (18).Abdominal examination may show initial rigidity, spasm, tenderness, and unilateral pain on deep palpation. On pelvic examination, unilateral adnexal tenderness and a palpable mass are usually present. The torsion is more likely to involve the right adnexal (3:2), perhaps because of the proximity of the sigmoid colon to the left adnexa, resulting in less space in which the torsion can occur (21). Half of the patients may have radiation to the back, flank, or groin. One third of patients may exhibit only mild abdominal tenderness and some have no pelvic tenderness (18).
In Bouguizane et al. (22), a review of 135 cases of adnexal torsion, only 57.8% of patients were diagnosed accurately at the first clinical examination. Incorrect preoperative diagnoses in patients subsequently having torsion include adnexal mass, appendicitis, myoma, ectopic pregnancy, abscess, and ruptured viscus (23). Torsion must be considered in the differential diagnosis of abdominal pain, especially when a palpable pelvic mass is present.
If no palpable mass is present, ultrasonography may prove helpful in the diagnosis (17,24). Ultrasonography has been shown to demonstrate a mass in all patients
Source. With permission from Lomano JM, Trelford JD, Ullery JC. Torsion of the uterine adnexa causing an acute abdomen. Obstet Gynecol. 1970;Vol.no. 35, issue.no.
2.with torsion. However, the ultrasonic appearance of the masses was nonspecific (17). The use of Doppler flow examination has recently been shown to be helpful in the diagnosis and management of ovarian torsion. Doppler ultrasound is able to identify the twisted vascular pedicle in the majority of cases (24,25). If normal arterial and venous flow can be demonstrated, untwisting of the pedicle is possible. If no blood flow is seen, this is generally associated with necrotic adnexa (17). However, more recent studies of Doppler ultrasound have shown that normal flow does not exclude the diagnosis of ovarian torsion (17,26). In fact, in one case report, up to 60% of confirmed ovarian torsions had normal flow (27). Approximately 20% of patients with an adnexal torsion will have a concomitant intrauterine pregnancy. Ultrasound can demonstrate the location of the pregnancy and aid in differentiation of torsion with intrauterine pregnancy from an ectopic gestation.
Magnetic resonance imaging (MRI) and computed tomography (CT) scanning have been described in a small number of patients. CT and MRI findings are generally nonspecific unless edema or hemorrhagic findings are present. MRI findings of large areas of high signal intensity on both T1- and T2-weighted images are associated with passive congestion of the torsed mass. The common CT and MRI features of adnexal torsion include thickening of the twisted fallopian tube, smooth thickening of the wall of the cystic ovarian mass, ascites, and uterine deviation to the side of torsion (28-30).
DIFFERENTIAL DIAGNOSIS
The diagnosis of torsion of the adnexa must be considered in women with abdominal pain. The differential diagnoses include ectopic pregnancy, appendicitis, pelvic inflammatory disease, adnexal mass without torsion, endometrioma, degeneration of a myoma, renal calculi, urinary tract infection, and ruptured functional cyst (1,19).
Ectopic pregnancy without an acute abdomen is diagnosed by serial β-human chorionic gonadotropin (β-hCG) testing along with appropriate use of ultrasound when the quantitative β-hCG level reaches the discriminatory zone.
Although intrauterine pregnancy is associated with torsion of the adnexa, ultrasound and β-hCG testing should be used to differentiate an intrauterine pregnancy with torsion from an ectopic gestation. In the event of an unstable patient, emergency laparotomy is indicated with either diagnosis (Chapter 3).In appendicitis, the symptoms of midline abdominal pain with migration to the right lower quadrant and negative pelvic findings other than tenderness on rectal examination differentiate this entity from torsion. In addition, the nausea and vomiting seen in torsion generally occur rapidly after the onset of pain, rather than gradually, as in acute appendicitis.
Pelvic inflammatory disease is usually characterized by bilateral pain and tenderness. Temperature elevation and leukocytosis may be more marked. Pertinent history—such as episodes of pelvic infl ammatory disease, intrauterine device use, and multiple or new sexual partners—points to pelvic inflammatory disease.
Patients who have an adnexal mass without torsion generally present without pain. Those who have a ruptured functional cyst may present at the midpoint of the menstrual cycle (Mittelschmerz) or just prior to the next expected period. Symptoms of nausea and vomiting are less frequent. In cases where there is no hemorrhage, symptoms are less severe than those seen with adnexal torsion and resolve over 48 hours.
Renal calculi usually present with flank pain and hematuria. There is also lack of a palpable pelvic mass. Degeneration of a myoma, especially if pedunculated, may require laparoscopy to confirm the diagnosis. A history of chronic pelvic pain will usually accompany endometriosis. Fever, acute pain, and increased leukocyte count are not seen with endometriomas unless there is a rupture. In cases of rupture, an acute abdomen may be seen necessitating operative intervention.
In all cases of acute pain, an empty bladder is necessary to ensure that urinary retention is not the cause of the pain.
It will also allow for a more complete and accurate pelvic examination.A high index of suspicion for torsion in cases of abdominal pain with a palpable or ultrasonically detected pelvic mass is necessary. Combined with l aparoscopy in equivocal cases, early diagnosis and prompt treatment of this condition are possible.
Serum concentrations of interleukin-6 have been reported to be elevated in ovarian torsion in 75% of cases (six of eight) (31). Ovarian torsion has also been reported along with cases of inguinal hernia (32).
TREATMENT
Treatment for adnexal torsion is surgical and depends on the condition of the ovary at the time of surgery. In most series, treatment has consisted of removal of the affected adnexa because of fear of embolism from thrombosed ovarian veins or necrosis of the ovary and the tube. In these cases, it is wise to expose the ureter to determine its location prior to ligating the ovarian blood supply, as the tenting of the peritoneum by the torsion may cause the ureter to be in or adjacent to the twisted pedicle.
Laparoscopic management of ovarian torsion has become the standard of care. If the ovary is not necrotic and fertility is important, it may be untwisted and stabilized by suturing it to the posterior wall of the uterus or by shortening the ovarian ligament. Observation is important to determine viability. Long-term follow-up has demonstrated that normal ovarian function is present in the great majority of cases. Follow-up ultrasounds have demonstrated normal follicular function in 95% of cases. Two important facto rs that may influence a successful conservative management of adnexal torsion are the surgeon’s experience and the time interval from the beginning of abdominal pain (36 hours) to definitive treatment (33-38). Since torsion is usually associated with neoplasms of the ovary, the ovary should be carefully inspected and cystectomy carried out if necessary. If there is suspicion of a malignancy, unilateral adnexectomy should be performed. Appropriate surgical staging should be carried out if a frozen section shows malignancy (2).
Laparoscopic oophoropexy has been described to prevent recurrent ovarian torsion. This may be performed if the surgeon feels that the risk of recurrent torsion is high based on physical findings or if it represents the remaining ovary in premenopausal women (36).
Ovarian torsion has been described in postmenopausal women on tamoxifen therapy (39).
SPECIAL CONSIDERATIONS
Torsion of the ovary is associated with OHSS caused by the hMG (Pergonal) use for ovulation induction. This syndrome is characterized by high estrogen secretion, enlargement of the ovaries, abdominal discomfort, and nausea and vomiting. In severe cases, clinical manifestations may include ascites, pleural effusions, electrolyte imbalance, oliguria, and shock. Torsion of the ovary was present in 7.4% of cases of OHSS in one series. It was more common (16%) in patients who were pregnant and had OHSS (40). A review of assisted reproductive technologies demonstrated nine cases of ovarian torsion in 10,583 cycles. However, 3 of 104 patients with OHSS demonstrated torsion. All cases were treated conservatively (41). Recent reports of treatment of these patients by the untwisting of the ovarian pedicle even when the ovary appears necrotic have demonstrated no complications. Normal subsequent ovarian function has been demonstrated by ultrasound in these patients. Continuation of pregnancy without problems was also demonstrated. Although the number of patients treated in this manner is still small, this option should be considered for these patients, in whom fertility is such an important issue. This method of treatment may not be applicable to patients who do not have OHSS (38,40).
The diagnosis of ovarian torsion must be considered in children presenting with abdominal pain. In children, the adnexal torsion may present as an abdominal mass. The diagnosis in children is especially important. Kokoska et al. (42) reported on 51 children with ovarian torsion. At their institution, all 51 underwent salpingo-oophorectomy. Earlier diagnosis may allow for conservative treatment (36). This entity has been reported in the infant as well (43).
CONCLUSIONS
Torsion of the adnexal structures must be considered in women of all ages presenting with abdominal pain. The incidence is highest in the reproductive-age group. A palpable or an ultrasonically detected pelvic mass along with pain should alert the clinician to consider this diagnosis. Because of the difficulty of clinical diagnosis, the more frequent use of laparoscopy may lead to early treatment and preservation of fertility.
References
1. SilenW. Cope’s Early Diagnosis of the Acute Abdomen. 21st Ed. New York, NY: Oxford Press; 2005:208.
2. Oelsner G, Shashar D. Adnexal torsion. Clin Obstet Gynecol. 2006;49(3):459-463.
3. Orazi C, Inserra A, Lucchetti M, et al. Isolated tubal torsion: a rare cause of pelvic pain at menarche. Sonographic and MR findings. Pediatr Radiol. 2006;36(12):1316-1318.
4. Antoniou N, Varras M, Akrivis C, et al. Isolated torsion of the fallopian tube: a case report and review of the literature. ClinExp Obstet Gynecol. 2004;31(3):235-238.
5. Krissi H, ShalevJ, Bar-Hava I, et al. Fallopian tube torsion: laparoscopic evaluation and treatment of a rare gynecological entity. JAm BoardFam Pract. 2001;14(4):274-277.
6. Gorkemli H, Camus M, Clasen K. Adnexal torsion after gonadotrophin ovulation induction for IVF or ICSI and its conservative treatment. Arch Gynecol Obstet. 2002;267(1):4-6.
7. Robson S, Kerin JF. Acute adnexal torsion before oocyte retrieval in an in vitro fertilization cycle. Fertil Steril. 2000;73(3):650-651.
8. Zhu W, Li X, Chen X, et al. Conservative management of adnexal torsion via trans- vaginal ultrasound guided ovarian cyst aspiration in patients with ovarian hyperstimulation. Fertil Steril. 2008;89(1):229, e1-3.
9. McWilliams GD, Hill MJ, Dietrich CS III. Gynecologic emergencies. Surg Clin North Am. 2008;88(2):265-283, vi.
10. Whitecar MP, Turner S, Higby MK. Adnexal masses in pregnancy: a review of 130 cases undergoing surgical management. Am J Obstet Gynecol. 1999;181(1):19-24.
11. Kumari I, Kaur S, Mohan H, et al. Adnexal masses in pregnancy: a 5-year review. Aust N Z J Obstet Gynaecol. 2006;46(1):52-54.
12. Chittacharoen A, Wangpusayavisut A, O-Prasertsawat P. Adnexal masses in pregnancy. JMedAssoc Thai. 2005;88(Suppl. 2):S37-S40.
13. Eitan R, Galoyan N, Zuckerman B, et al. The risk of malignancy in post-menopausal women presenting with adnexal torsion. Gynecol Oncol. 2007;106(1):211-214.
14. Sommerville M, Grimes D, Koonings P, et al. Ovarian neoplasms and the risk of adnexal torsion. Am J Obstet Gynecol. 1991;164(2):577-578.
15. Koonings PP, Grimes DA. Adnexal torsion in postmenopausal women. Obstet Gynecol. 1989;73(1):11-12.
16. Lee RA, Welch JS. Torsion of the uterine adnexa. Am J Obstet Gynecol. 1967;97(7): 974-977.
17. Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics. 2008;28(5):1355-1368.
18. Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerg Med. 2001;38(2):156-159.
19. Marx J. R osen’s Emergency Medicine: Concepts and Clinical Practice. 6th Ed. St. Louis, MO: Mosby; 2006.
20. Lomano JM, Trelford JD, Ullery JC. Torsion of the uterine adnexa causing an acute abdomen. Obstet Gynecol. 1970;35(2):221-225.
21. Weitzman VN, DiLuigi AJ, Maier DB, et al. Prevention of recurrent adnexal torsion. Fertil Steril. 2008; 90(5):2018el-3.
22. Bouguizane S, Bibi H, Farhat Y, et al. Adnexal torsion: a report of 135 cases. J Gynecol Obstet Biol Reprod (Paris). 2003;32(6):535-540.
23. Hiller N, Appelbaum L, Simanovsky N, et al. CT features of adnexal torsion. AJR Am J Roentgenol. 2007;189(1):124-129.
24. Moore C, Meyers AB, Capotasto J, et al. Prevalence of abnormal CT findings in patients with proven ovarian torsion and a proposed triage schema. Emerg Radiol. 2009;16(2):115-120.
25. Chang YJ, Yan DC, Kong MS, et al. Adnexal torsion in children. Pediatr Emerg Care. 2008;24(8):534-537.
26. Albayram F, Hamper UM. Ovarian and adnexal torsion: spectrum of sonographic findings with pathologic correlation. J Ultrasound Med. 2001;20(10):1083-1089.
27. Pena JE, Ufberg D, Cooney N, et al. Usefulness of Doppler sonography in the diagnosis of ovarian torsion. Fertil Steril. 2000;73(5):1047-1050.
28. Kimura I, Togashi K, Kawakami S, et al. Ovarian torsion: CT and MR imaging appearances. Radiology. 1994;190(2):337-341.
29. Singh A, Danrad R, Hahn PF, et al. MR imaging of the acute abdomen and pelvis: acute appendicitis and beyond. Radiographics. 2007;27(5):1419-1431.
30. Minutoli F, Blandino A, Gaeta M, et al. Twisted ovarian fibroma with high signal intensity on T1-weighted MR image: a new sign of torsion of ovarian tumors? Eur Radiol. 2001;11(7):1151-1154.
31. Cohen SB, Wattiez A, Stockheim D, et al. The accuracy of serum interleukin-6 and tumour necrosis factor as markers for ovarian torsion. Hum Reprod. 2001;16(10): 2195-2197.
32. Merriman TE, Auldist AW. Ovarian torsion in inguinal hernias. Pediatr Surg Int. 2000;16(5-6):383-385.
33. Oelsner G, Bider D, Goldenberg M, et al. Long-term follow-up of the twisted ischemic adnexa managed by detorsion. Fertil Steril. 1993;60(6):976-979.
34. Dane B, Dane C, Kiray M, et al. Sonographic findings in adnexal torsion: a report of 34 cases. Arch GynecolObstet. 2008.
35. Rody A, Jackisch C, Klockenbusch W, et al. The conservative management of adnexal torsion—a case-report and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2002;101(1):83-86.
36. Rousseau V, Massicot R, Darwish A, et al. Emergency management and conservative surgery of ovarian torsion in children: a report of 40 cases. JPediatrAdolesc Gynecol. 2008;21(4):201-206.
37. Aziz D, Davis V, Allen L, et al. Ovarian torsion in children: is oophorectomy necessary? JPediatr Surg. 2004;39(5):750-753.
38. Eckler K, Laufer MR, Perlman SE. Conservative management of bilateral asynchronous adnexal torsion with necrosis in a prepubescent girl. J Pediatr Surg. 2000;35(8):1248-1251.
39. Barbieri RL, Ferracci AL, Droesch JN, et al. Ovarian torsion in a premenopausal woman treated with tamoxifen for breast cancer. Fertil Steril. 1993;59(2):459-460.
40. Delvigne A, Rozenberg S. Review of clinical course and treatment of ovarian hyperstimulation syndrome (OHSS). Hum Reprod Update. 2003;9(1):77-96.
41. Mashiach S, Bider D, Moran O, et al. Adnexal torsion of hyperstimulated ovaries in pregnancies after gonadotropin therapy. Fertil Steril. 1990;53(1):76-80.
42. Kokoska ER, Keller MS, Weber TR. Acute ovarian torsion in children. Am J Surg. 2000;180(6):462-465.
43. Fitzhugh VA, Shaikh JR, Heller DS. Adnexal torsion leading to death of an infant. J Pediatr Adolesc Gynecol. 2008;21(5):295-297.
More on the topic Torsion of Ovary:
- Torsion of Ovary
- Benrubi Guy I. (ed.). Handbook of Obstetric and Gynecologic Emergencies. 4th edition. — Lippincott Williams & Wilkins,2010. — 424 p., 2010
- CONTENTS
- Imaging in Gynecologic Emergencies
- INDEX
- Pelvic Mass
- Chapter 13 Benign and urogynaecology
- 48 Ovarian Cancer
- Chapter 50 Ovarian and Adnexal Disease
- 29 Ectopic Pregnancy