13 Endocrine Disorders of Pregnancy
Clark T. Johnson
Lorraine A. Milio
DIABETES MELLITUS
Diabetes mellitus (DM) is the most common medical complication of pregnancy in the United States, affecting nearly 7% of all pregnancies.
As the incidence of type 2 DM increases nationwide, cases of gestational diabetes mellitus (GDM) have grown also. In 90% of diabetic pregnancies, the cause is GDM.• Diabetes in pregnancy is categorized as pregestational diabetes (diagnosed prior to pregnancy) or GDM (diagnosed during pregnancy). Pregestational diabetes is further classified as type 1 or type 2 (Table 13-1). One half percent to 1% of pregnancies are complicated by pregestational DM.
• Carbohydrate metabolism changes during pregnancy to provide adequate nutrition for both the mother and the fetus.
• In the fasting state, maternal serum glucose is lower in pregnancy than in the nonpregnant state (55 to 65 mg/dL), whereas free fatty acid, triglyceride, and plasma ketone concentrations are increased. A state of relative maternal starvation exists in pregnancy, during which glucose is spared for fetal consumption and alternate fuels are used by the mother.
• GDM is similar to type 2 DM, in which increased pancreatic secretion cannot overcome decreased insulin sensitivity of maternal target tissues. Increased metabolism in pregnancy also increases insulin clearance. These changes are due to the effects of estrogen, progesterone, cortisol, prolactin, and human placental lactogen. The net result is hyperglycemia.
Diagnosis and Screening
• Diagnosis of type 1 and 2 DM before pregnancy is by standard criteria: two abnormal fasting glucose levels ≥126 mg/dL or a random glucose level of ≥200 mg/dL (Table 13-2). Classic symptoms are polydipsia, polyuria, and polyphagia. Clinical signs include weight loss, hyperglycemia, persistent glucosuria, and ketoacidosis.
• Universal screening for GDM is standard in the United States, whether by patient history, clinical risk factors, or laboratory testing. Testing is typically performed at 24 to 28 weeks, but if strong risk factors such as obesity, family history, or a personal history of GDM are present, blood glucose screening may be performed at the first prenatal visit. Not all patients require screening via blood glucose testing (Table 13-3).
• Screening for GDM has undergone much scrutiny in recent years as a result of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study in which progressive hyperglycemia was linked to adverse perinatal outcomes. For many years, a two-step screening/diagnostic protocol has been widely used. In this screening, a 50-g oral glucose challenge is consumed, followed by serum glucose measurement at
P.177
1 hour. No fasting or dietary preparation is required. A serum glucose ≥140 mg/dL identifies 80% of GDM, whereas decreasing the cutoff to ≥130 mg/dL identifies over 90% of GDM but with more “false positives.” A serum glucose ≥200 mg/dL diagnoses GDM without additional testing.
• If the screening test is positive, then a diagnostic 3-hour glucose tolerance test (GTT) should be performed with 100-g oral glucose after at least 8 hours of fasting (Table 13-4). With abnormal fasting or any other two
abnormal values, the diagnosis of DM is confirmed. In patients at high risk for GDM with a normal GTT, a follow-up GTT can be performed at 32 to 34 weeks to identify late-onset diabetes.
P.178
• Based on the HAPO study, the International Association of Diabetes and Pregnancy Study group, in 2010, recommended that a universal 75-g, 2-hour GTT be used in a single-step screening/diagnosis of GDM. In this schemata, the diagnosis of GDM would be made when any single threshold value was reached or exceeded (fasting value = 92 mg/dL, 1-hour value = 180 mg/dL, and 2-hour value = 153 mg/dL).
• This protocol was endorsed by the American Diabetes Association.
However, there has been concern that using this criterion for diagnosis of GDM would result in 17% to 18% of pregnancies diagnosed with GDM and would improvedP.179 perinatal outcomes justify the increased burden of managing such a surge in diagnosed patients. In 2013, a National Institute of Child Health and Human Development consensus panel concluded that there was not enough evidence to date to warrant recommendation of this protocol for universal diagnosis of GDM.
• Classification of GDM depends on the management required to control blood glucose levels. Type A1 achieves euglycemia by dietary changes alone. Type A2 requires additional (i.e., medical) therapy.
| TABLE 13-1 Comparison of Type 1 and Type 2 Diabetes Mellitus | |
| Type 1 | Type 2 |
| Pathophysiology is absolute insulin deficiency. | Pathophysiology is tissue resistance to insulin. |
| Patients are at risk for severe hypoglycemia and DKA. | Patients may develop hyperosmolar nonketotic coma (HONK). DKA is rare. |
| DKA can be encountered at relatively low blood sugars (500mg/dL). | |
| Increased risk for chronic microvascular disease at an early age | Lower incidence of microvascular disease during reproductive age range |
| DKA, diabetic ketoacidosis. | |
TABLE 13-2 Diabetic Screening in the Nonpregnant Patient
1. A1C ≥6.5%. The test should be performed in a laboratory using a method that is NGSP certified and standardized to the DCCT assay.a
OR
FPG ≥126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 hr.a
OR
3. Two-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an OGTT. The test should be performed as described by the World Health Organization using a glucose load containing the equivalent of 75-g anhydrous glucose dissolved in water.a
OR
4.
In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥200 mg/dL (11.1 mmol/L).aDiagnoses based on 1,2, or 3 should undergo repeat testing to confirm findings. NGSP, National Glycohemoglobin Standardization Program; DCCT, Diabetes Control and Complications Trial; FPG, fasting plasma glucose; OGTT, oral glucose tolerance test.
From American Diabetes Association. Standards of medical care in diabetes 2011. Diabetes Care 2011;34(suppl 1):S11-S61.
TABLE 13-3 Gestational Diabetes Risk Assessment
Low risk
Age younger than 25 years
Not a member of an ethnic group with increased risk for type 2 DM (Hispanic, African, Native American, South or East Asian, or Pacific Islander ancestry)
BMI of diabetic mothers, vaginal delivery carries a 2% to 5% risk of brachial plexus injury.
• Twenty-five percent to 40% of infants of diabetic mothers develop neonatal hypoglycemia. The serum glucose nadirs at about 24 hours of life. Poor maternal glycemic control during late pregnancy and at delivery increases the risk. The pathogenesis is in utero stimulation of the fetal pancreas by maternal hyperglycemia leading to fetal islet cell hypertrophy and beta cell hyperplasia. When the maternal glucose source is eliminated, the continued overproduction of insulin leads to newborn hypoglycemia with cyanosis, convulsions, tremor, apathy, diaphoresis, and a weak or high-pitched cry, if untreated. Severe or prolonged hypoglycemia is associated with neurologic sequelae and death. Standard of care includes testing neonatal blood glucose value within 1 hour of birth. Treatment should be instituted when the infant's blood glucose drops below 40 mg/dL.
• Neonatal hypocalcemia and hypomagnesemia are common in infants of diabetic mothers and correlate with the degree of glycemic control.
• Thirty-three percent of infants born to diabetic mothers have polycythemia (hematocrit higher than 65%). Chronic intrauterine hypoxia increases erythropoietin production, resulting in vigorous hematopoiesis.
Alternatively, elevated glucose may lead to early increased red blood cell destruction, followed by increased erythrocyte production.• Neonatal hyperbilirubinemia and neonatal jaundice occur more commonly in infants of diabetic mothers than in infants of nondiabetic patients of comparable gestational age because poor glycemic control delays fetal liver maturation.
• Neonatal respiratory distress syndrome (RDS) may occur more frequently in diabetic pregnancies as a result of delayed fetal lung maturation. Fetal hyperinsulinemia
P.181 may suppress production and secretion of surfactant required for normal lung function at birth.
• The risk of fetal cardiac septal hypertrophy and hypertrophic cardiomyopathy is increased in diabetic pregnancies (up to 10% have hypertrophic changes). There is a strong correlation between cardiomyopathy and poor maternal glycemic control. As an isolated finding, cardiac septal hypertrophy is a benign neonatal condition. However, it increases the risk of morbidity and mortality in neonates with sepsis or congenital structural heart disease.
Maternal Complications of Diabetes Mellitus
• Maternal complications are increased with diabetes.
• Diabetic ketoacidosis (DKA) is a potentially life-threatening metabolic emergency for both mother and fetus. In pregnant patients, DKA can occur at lower blood glucose levels (i.e., infection is detected prior to 20 weeks' gestation. Creatinine clearance 90% (see Chapter 16).
• Diabetic retinopathy is the most common vascular manifestation of diabetes and a principal cause of adultonset blindness in the United States. Proliferative retinopathy is believed to be a consequence of persistent hyperglycemia and is directly related to the duration of disease. Pregnancy does not change the long-term prognosis, but an ophthalmologic evaluation is recommended in preconception counseling or at the time of the pregnancy diagnosis. Progressive disease may be treated with laser treatment during pregnancy.
• The incidence of chronic hypertension is increased in patients with pregestational DM, especially those with nephropathy (see Chapter 14).
• Preeclampsia is two to four times more common in pregestational diabetics. The risk is increased with longer duration of disease, nephropathy or retinopathy, and chronic
P.184 hypertension. Up to a third of women with long-standing diabetes (>20 years) will develop preeclampsia. Even in GDM, the risk of preeclampsia is 13% to 18%. The threshold for preeclampsia workup in these women should be very low (see Chapter 14).
• Preterm labor and delivery may be three to four times higher in patients with DM. Worsening maternal medical status, poor glycemic control, noncompliance with diabetic management, and nonreassuring fetal status result in many iatrogenic preterm deliveries.
• Corticosteroids should be administered as indicated when there is an increased risk for preterm delivery before 34 weeks. Additional insulin or oral agents may be required for 5 to 7 days after steroid administration.
• Diabetics also have increased maternal risk for adverse obstetric outcomes including third- and fourth-degree perineal lacerations and wound infection. Additionally, they are at increased risk for intrauterine fetal demise, particularly after 40 weeks' gestation.
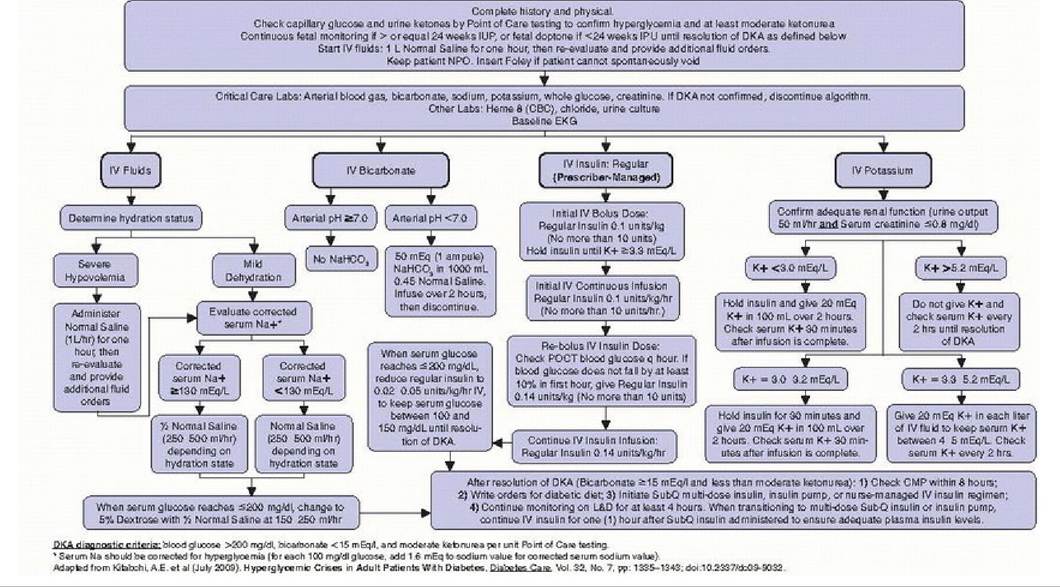
Figure 13-1. Prescriber guidelines for management of obstetric patient with diabetic ketoacidosis.
Management of Diabetes in Pregnancy
• Ideally, diabetic women desiring pregnancy should seek preconception consultation and maintain euglycemia before conception. The initial prenatal visit should include a detailed history and physical examination, an ophthalmologic examination, an ECG (for women older than age 30 years, smokers, or hypertensives), and 24-hour urine collection for protein and creatinine clearance. Echocardiography and cardiology consultation should be obtained for known or suspected cardiovascular disease. HbA1C is helpful in evaluating recent (8 to 12 weeks) glycemic control and in assessing risk for fetal malformations. HbA1C ≥9.5% carries >20% risk of major fetal malformation. Strict glucose control (i.e., HbA1C ≤6%) during organogenesis dramatically reduces embryopathy to nondiabetic levels. Early nutrition consult and counseling may be beneficial.
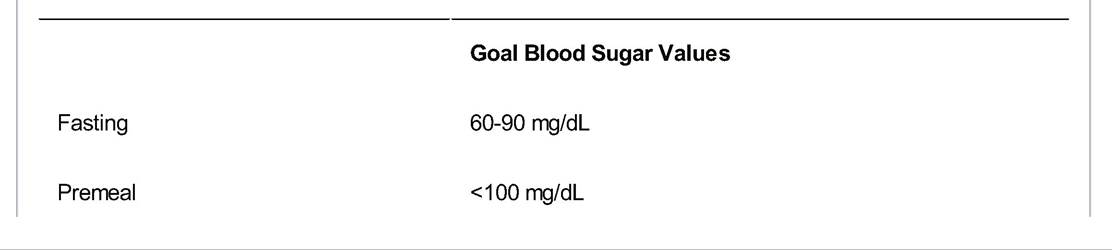
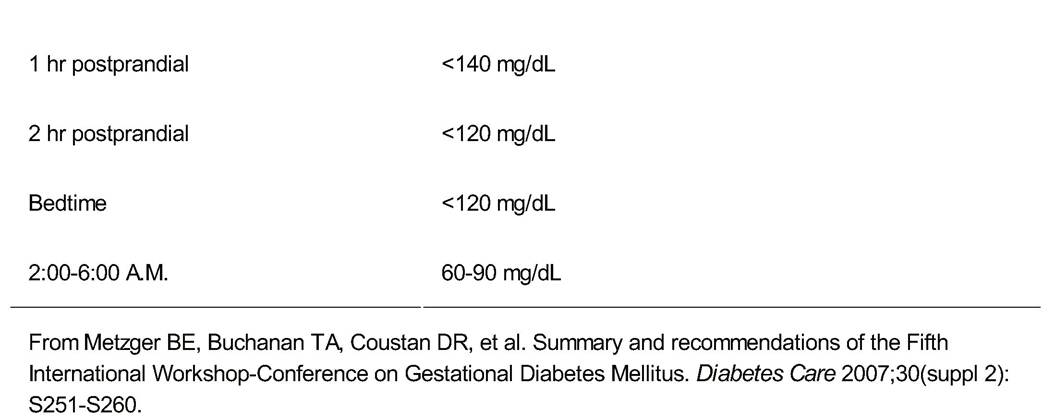
• Blood glucose goals in pregnancy are given in Table 13-5.
• Patients should start or continue intensive glucose monitoring early in pregnancy using a home glucometer. They should record fasting and 1-hour (or 2-hour) postprandial blood sugar levels for each meal.
• Postprandial glycemic control correlates most strongly with risk for neonatal hypoglycemia, macrosomia, fetal death, and neonatal complications. Home monitoring records are reviewed every 1 to 2 weeks and therapy is optimized.
TABLE 13-5 Goals for Glycemic Control in Pregnancy
P.185
Gestational Diabetes Mellitus Management
• Management for GDM initially consists of diet and exercise. If good glucose control is not achieved, oral hypoglycemic agents or insulin are then prescribed.
• Women with newly diagnosed GDM are started on a carbohydrate-controlled diet with three meals and three snacks daily.
• Moderate exercise can improve glycemic control in GDM. Patients are encouraged to maintain a consistent level of activity throughout pregnancy provided there are no contraindications (e.g., preterm labor).
• Oral hypoglycemic agents are acceptable in GDM management when dietary efforts fail to achieve euglycemia. One agent frequently used in pregnancy, glyburide, works by increasing tissue insulin sensitivity and has minimal placental transfer. The starting dose is usually 2.5 mg orally (PO) at bedtime or 2.5 mg PO twice daily, titrated to a maximum dose of 20 mg daily. Glyburide side effects include hypoglycemia, nausea, heartburn, and allergic skin reactions. Metformin is also safe and effective. Four percent to 20% of patients will need additional therapy with insulin, particularly if fasting blood sugars are high.
• Insulin therapy can improve glycemic control for GDM. Different types of insulin are combined to maintain euglycemia throughout the day and night (Fig. 13-2).
• Neutral protamine Hagedorn (NPH) insulin is an intermediate-acting insulin given in the morning and at night, with peak activity at 5 to 12 hours.
• Rapid-acting insulin (e.g., Humalog or NovoLog) is administered with meals because its onset is 5 to 15 minutes and peak activity occurs at 2 to 4 hours.
• Fetal monitoring is not required for GDM-A1 diabetics. They are not at increased risk for fetal demise before 40 weeks' gestation. Women with GDM-A2 require antenatal testing similar to that recommended for pregestational DM (twice weekly nonstress tests or biophysical profile from 32 to 34 weeks until delivery). Delivery by 40 weeks' gestation is recommended due to increased risk of intrauterine demise after that time.
Pregestational Diabetes Mellitus Management
• Management of pregestational DM
• The recommended diet for pregnant diabetic women is 1,800 to 2,400 kcal daily, made up of 20% protein,
60% carbohydrates, and 20% fat. Carbohydrate
P.186 counting, with 180 to 210 g of daily carbohydrates, is becoming more common and replacing caloric guidelines. Three meals and three snacks are recommended for all diabetics in pregnancy. Nutrition consult should be part of preconception or early pregnancy planning.
• Patients are usually continued on their normal prepregnancy insulin regimen while initial blood sugar monitoring is performed. Monitoring and goals are the same for GDM and pregestational DM (see Table 135).
î The American Diabetes Association recommends insulin for pregnant women with DM and for women with DM considering pregnancy. Patients taking oral hypoglycemic agents (except glyburide or metformin) or a 70/30 (NPH/regular) mixed insulin regimen are switched to NPH and a rapid-acting insulin analog. Patients with type 1 DM usually require 50% to 100% increased insulin doses in the second half of pregnancy. Type 2 DM insulin dosing is frequently more than doubled in pregnancy.
î Insulin pumps provide a continuous subcutaneous infusion of insulin. Pump dosing must be managed carefully because the risk of severe hypoglycemia causing seizures and death is increased in pregnancy. Patients must be carefully selected; however, diabetic control may be improved in the correct patient population.
• Fetal assessment and monitoring for pregestational diabetes varies according to gestational age.
• First trimester: Obtain an early dating sonogram to confirm gestational age and document fetal viability.
• Second trimester: Offer maternal serum alpha-fetoprotein screening for neural tube defects (either alone or as part of aneuploidy screening if desired by the patient; see Chapter 12). Ultrasonography at 18 to 20 weeks is recommended for complete anatomy evaluation. Fetal echocardiography is also recommended at 19 to 22 weeks for pregestational diabetics.
• Third trimester: Twice-weekly antenatal testing should be initiated for all diabetic pregnancies starting at 32 to 34 weeks' gestation. Patients with comorbidities or very poor glycemic control may start assessment as early as 28 weeks. Serial ultrasonographic exams for fetal growth should be considered at 28 to 30 weeks and again at 34 to 36 weeks. Monthly fetal growth ultrasounds with umbilical artery Doppler velocimetry may be required to assess for IUGR in patients with microvascular disease (see Chapter 6).
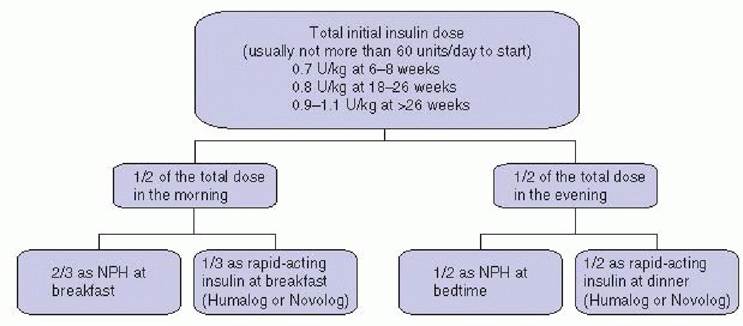
Figure 13-2. Calculation and dose distribution for initial insulin management in pregnancy. (Adapted from Gabbe
SG. Management of diabetes mellitus complicating pregnancy. Obstet Gynecol 2003;102[4]:857.)
Labor and Delivery in Diabetic Pregnancies
• Timing of delivery in an insulin-requiring diabetic patient should consider maternal glycemic control, maternal comorbidities, estimated fetal weight, antenatal testing, and amniotic fluid volume. In many patients with well- controlled DM, labor may be induced safely at 39 to 40 weeks.
• Glucose control during labor and delivery should maintain euglycemia to improve neonatal outcomes. Continuous IV insulin and glucose infusions may be needed to optimize glycemic control. With elective induction, the patient receives her usual insulin the night prior to admission but holds her morning dose. On admission, IV fluids are started along with serial glucose monitoring (every 1 to 2 hours). The infusion fluids are adjusted to maintain blood glucose levels between 70 and 110 mg/dL (Table 13-6). Short-acting insulin boluses may be required in addition to the IV drip.
• Route of delivery is determined by usual obstetric indications. If fetal macrosomia >4,500 g is suspected, cesarean section is considered to avoid the risk of a shoulder dystocia. Otherwise, induction of labor is warranted.
P.187
TABLE 13-6 Low-Dose Continuous Insulin Infusion for Labor and Delivery
| Blood Glucose (mg/dL) | Insulin Dosage (U/hr)a | Fluids (125 mL/hr) |
| 220 | 2.5b,c | Normal saline |
aType 1 diabetic patients need baseline insulin when blood glucose is >60 mg/dL; 0.5 U/hr is reasonable to start.
bIncrease as needed.
cBoluses of insulin may be required in addition to an increase in the insulin drip. D5NS, 5% dextrose in normal saline.
Adapted from Rosenberg V, Eglinton GS, Rauch ER, et al. Intrapartum glycemic control in women with insulin requiring diabetes: a randomized clinical trial of rotating fluids versus insulin drip. Am J Obstet Gynecol 2006;195(5):1095-1099.
Postpartum Care for Diabetics
Postpartum management of diabetic mothers depends on the severity and type of DM.
• For GDM, no immediate postpartum testing is required. Most gestational DM diagnosed in the third trimester resolves rapidly after delivery. Glucose tolerance testing is strongly recommended for these patients at their postpartum visit, with a 2-hour fasting GTT, because some women with GDM will persist as type 2 diabetics after delivery (Table 13-7). GDM will recur in 30% to 50% of subsequent pregnancies. Because women with a history of GDM have a sevenfold increased risk of developing type 2 diabetes, they should be advised postpartum on weight control, a healthy diet, exercise, and yearly evaluation for diabetes.
P.188
• For pregestational diabetics, blood sugar can be monitored with nonpregnant regimen. The insulin dose is typically one half of the dose at the end of pregnancy, and oral hyperglycemics are significantly decreased. Blood sugar testing every 4 to 6 hours for 24 hours after cesarean section, with sliding scale insulin dosing, may be helpful until the patient can resume her normal routine. Keeping blood sugar Function Test Results in Pregnancy Compared with Hyperthyroid and Hypothyroid Conditions
| Test | Normal Pregnancy | Hyperthyroidism | Hypothyroidism |
| Thyroid-stimulating hormone (TSH) | No change | Decreased | Increased |
| Thyroxine-binding globulin (TBG) | Increased | No change | No change |
| Total T4 (T4) | Increased | Increased | Decreased |
| Free T4 (fT4) or free T4 index (FTI) | No change | Increased | Decreased |
| Total triiodothyronine (T3) | Increased | Increased or no change | Decreased or no change |
| Free T3 (fT3) | No change | Increased or no change | Decreased or no change |
| T3 resin uptake (T3RU) | Decreased | Increased | Decreased |
| Iodine uptake | Increased | Increased or no change | Decreased or no change |
Adapted from American College of Obstetricians and Gynecologists. ACOG practice bulletin. Clinica l management guidelines for obstetrician-gynecologists. Number 37, August 2002. (Replaces practice bulletin number 32, November 2001). Thyroid disease in pregnancy. Obstet Gynecol 2002;100:387-396;
Rashid M, Rashid MH. Obstetric management of thyroid disease. Obstet Gynecol Surv 2007;62(10):680-688.
TABLE 13-9 Indications for Thyroid Function Testing in Pregnancy
Patient on thyroid therapy
Large goiter or thyroid nodularity
History of hyperthyroidism or hypothyroidism
History of neck irradiation
Previous infant born with thyroid dysfunction
Type 1 diabetes mellitus
Family history of autoimmune thyroid disease
Fetal demise in utero
Adapted from Mestman JH. Thyroid diseases in pregnancy other than Graves' disease and postpartum thyroid dysfunction. Endocrinologist 1999;9:294-307.
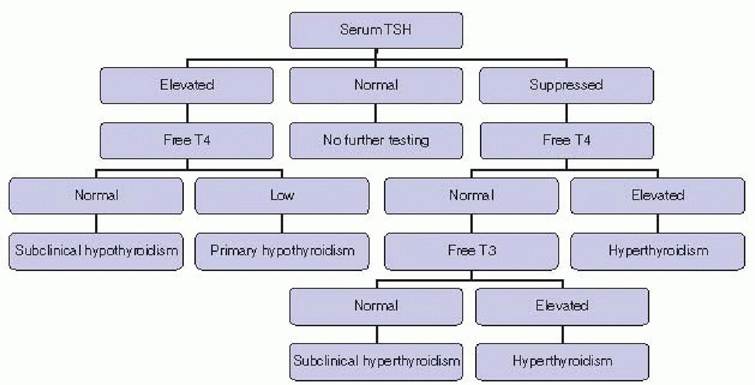
Figure 13-3. Thyroid testing algorithm. (Adapted from Mestman JH. Thyroid and parathyroid diseases in pregnancy. In Gabbe SM, Niebyl JR, Simpson JL, et al, eds Obstetrics: Normal and Problem Pregnancies. Philadelphia, PA: Churchill Livingstone, 2007:1011-1037.)
TABLE 13-10 Indications for Thyroid-stimulating Hormone Receptor Antibody Testing in Pregnancy
Graves disease (TSI)
Fetal or neonatal hyperthyroidism in previous pregnancy
Euthyroid, postablation, in the presence of
Fetal tachycardia
IUGR
Incidental fetal goiter on ultrasound
Incidental fetal goiter on ultrasound (TRAb)
Infant born with congenital hypothyroidism (TRAb)
TSI, TSH receptor-stimulating immunoglobulin; IUGR, intrauterine growth retardation; TRAb, TSH receptor-blocking antibodies.
Adapted from Mestman JH. Hyperthyroidism in pregnancy. Best Pract Res Clin Endocrinol Metab 2004;18(2):267-288.
Hyperthyroid Conditions
• Specific hyperthyroid conditions include Graves disease, hyperemesis gravidarum, gestational trophoblastic disease, struma ovarii, toxic adenoma, toxic multinodular goiter, subacute thyroiditis, TSH-producing pituitary tumor, metastatic follicular cell carcinoma, and painless lymphocytic thyroiditis. Thyrotoxicosis occurs in up to 1 in 500 pregnancies and increases risk for complications such as preeclampsia, thyroid storm, congestive heart failure, IUGR, preterm delivery, and stillbirth.
• Clinical signs of thyrotoxicosis include tachycardia, exophthalmos, thyromegaly, onycholysis, heat intolerance, pretibial myxedema, menstrual irregularities, and weight loss. Table 13-10 lists diagnostic test results for normal and hyperthyroid pregnancy.
• Graves disease is the primary cause of thyrotoxicosis in pregnancy, accounting for 90% to 95% of cases. It is an autoimmune disease in which thyroid-stimulating antibodies (TSAs) or thyroid-blocking antibodies (TRAb) bind to the thyroid TSH receptors and activate or antagonize thyroid growth and function, respectively. The antibodies can also cross the placenta and affect the fetus. Up to 5% of affected fetuses can develop neonatal Graves disease, which is unrelated to maternal thyroid function. Infants of women who have been treated previously with radioactive iodine or surgery may be at higher risk for neonatal complications because the mothers are not maintained on suppressive medications.
• Hyperemesis gravidarum with high hCG levels in early pregnancy can produce biochemical hyperthyroidism with low TSH and elevated fT4 (due to the active subunit of hCG mimicking TSH) that typically resolves by the mid second trimester. Hyperemesis is rarely associated with clinically important hyperthyroidism, and routine thyroid testing is not recommended in the absence of other findings.
Hyperthyroid Management
• Medical management is with propylthiouracil (PTU) or methimazole. Both cross the placenta and can potentially cause fetal hypothyroidism and goiter.
P.191 Maintaining high normal range thyroid hormone levels with a minimum drug dosage is the goal.
• PTU blocks iodide organification in the thyroid and reduces the peripheral conversion of T4 to T3. It is traditionally preferred to methimazole, although placental transfer of the two drugs is nearly equivalent. Both drugs have synthesis and conversion.
î Saturated potassium iodide solution two to five drops every 8 hours blocks thyroid hormone release.
î Dexamethasone 2 mg IV or intramuscular every 6 hours for 24 hours decreases hormone release and peripheral conversion.
î Propranolol is given as mentioned earlier for tachycardia.
î Phenobarbital 30 to 60 mg every 6 to 8 hours can relieve extreme restlessness.
Hypothyroid Conditions
• Hypothyroidism in pregnancy is uncommon because untreated hypothyroidism is associated with infertility. Common causes include Hashimoto thyroiditis, subacute thyroiditis, prior radioablative treatment, and iodine deficiency.
• Type 1 diabetes is associated with 5% incidence of hypothyroidism during pregnancy and has up to a 25% incidence of postpartum thyroid dysfunction.
• Complications of hypothyroidism in pregnancy include preeclampsia, abruptio placentae, anemia, and postpartum hemorrhage. Fetal complications include IUGR,
P.192 congenital cretinism (growth failure and neuropsychological deficits), and stillbirth. Infants of optimally treated hypothyroid mothers usually have no evidence of thyroid dysfunction.
• The most common etiology of hypothyroidism in the United States is Hashimoto chronic autoimmune thyroiditis, resulting from thyroid antimicrosomal and antithyroglobulin antibodies. Worldwide, the most common cause of hypothyroidism is iodine deficiency.
• Presentation may be asymptomatic or include disproportionate weight gain, lethargy, weakness, constipation, carpal tunnel syndrome, cold sensitivity, hair loss, dry skin, and, eventually, myxedema. Table 13-10 lists test results for hypothyroid pregnancy.
• T reatment is initiated if thyroid function testing is consistent with hypothyroidism, regardless of symptoms. Thyroxine replacement is based on the patient's clinical history and laboratory test values and adjusted until TSH remains normal and stable.
• The starting dose for levothyroxine is 50 to 100 μg daily. It may be several weeks before the full effect is obtained. TSH can be checked every 4 to 6 weeks initially. The dose may need to be increased in pregnancy. Stable patients can be tested every trimester.
Nodular Thyroid
• Nodular thyroid disease should be evaluated when detected during pregnancy. Thyroid cancer occurs in 1 in
1,000 pregnancies, and up to 40% of nodules will be malignant. Ultrasonography, fine-needle aspiration, or tissue biopsy can be performed in pregnancy. Surgical excision is the definitive treatment and should not be postponed because of pregnancy, whereas radiation treatment is deferred until after delivery.
PARATHYROID DISORDERS
Parathyroid disorders and calcium dysregulation are uncommon in pregnancy. Calcium requirements do increase during pregnancy, however, so 1,000 to 1,300 mg calcium and 200 IU vitamin D supplementation are recommended. Fetal calcium uptake, increased plasma volume, renal loss from increased glomerular filtration rate (GFR), and hypoalbuminemia lead to lower total maternal serum calcium levels, but ionized calcium remains fairly constant.
• Serum calcium levels are regulated by several hormones:
• Parathyroid hormone (PTH) increases calcium mobilization from bone, calcium recovery in the kidney, and calcium absorption in the intestine (indirectly via activation of vitamin D). PTH increases throughout pregnancy until term, possibly to counteract the inhibitory effects of estrogen on bone.
• Parathyroid hormone—related peptide (PTHrP) is produced by the placenta and fetal parathyroid to activate active placental calcium transport and, like PTH, mobilize maternal calcium stores.
• Calcitonin is produced in the parafollicular cells of the thyroid and acts to decrease serum calcium levels.
Hyperparathyroidism
• Hyperparathyroidism produces hypercalcemia. Clinical manifestations include hyperemesis, weakness, constipation, polyuria, polydipsia, nephrolithiasis, mental status changes, arrhythmias, and occasionally pancreatitis. Obstetric and fetal complications include preeclampsia, stillbirth, premature delivery, neonatal tetany, and
P.193 neonatal death. Poor control of maternal hyperparathyroidism is associated with significant neonatal morbidity and mortality.
• The differential diagnosis of hypercalcemia includes thyrotoxicosis, hypervitaminosis A and D, familial hypocalciuric hypercalcemia, granulomatous disease, and malignancy.
• Laboratory findings include elevated free serum calcium and decreased phosphorus levels. Disproportionately high PTH relative to serum calcium may also be found. ECG abnormalities, including arrhythmias, may be present. Ultrasonography is recommended for localization. If radiation exposure is necessary to identify local disease, it should be kept to a minimum.
• Surgical treatment (e.g., excision) of a parathyroid adenoma is considered in any patient with symptomatic hyperparathyroidism following medical stabilization. Hypercalcemic crisis is corrected with IV hydration, furosemide, electrolyte correction, and calcitonin. Oral phosphates can be used as treatment for mild cases or in preparation for surgery.
Hypoparathyroidism
• Hypoparathyroidism is rare and usually occurs iatrogenically after neck surgery. It is the most common cause of hypocalcemia. Patients exhibit cramps, paresthesias, bone pain, hyperacute deep tendon reflexes, tetany, prolonged QT interval, arrhythmias, and laryngospasm. Trousseau sign (carpopedal spasm after blood pressure cuff inflation above systolic pressure for several minutes) or Chvostek sign (upper lip twitching after tapping of the facial nerve) may be present. Fetal skeletal demineralization, subperiosteal resorption, osteitis fibrosa cystica, growth restriction, and neonatal hyperparathyroidism can develop.
• The differential diagnosis of hypocalcemia includes prior parathyroidectomy or thyroid surgery, prior radioactive iodine or radiation treatment, vitamin D deficiency, hypomagnesemia or hypermagnesemia, autoimmune disorders (e.g., Addison disease, chronic lymphocytic thyroiditis), eating disorders, renal failure, DiGeorge syndrome, and pseudohypoparathyroidism (i.e., PTH resistance).
• Laboratory evaluation shows low serum calcium, low PTH, and elevated serum phosphate levels. 1,25- Dihydroxy vitamin D levels are decreased, and ECG changes include prolongation of the QT interval.
• Treatment is with vitamin D (50,000 to 150,000 IU/day) and calcium (1,000 to 1,500 mg/day) supplementation and low-phosphate diet. Doses may need to be increased during pregnancy and reduced postpartum. Maternal repletion with calcium gluconate during labor and delivery may prevent neonatal tetany. Acute symptomatic hypocalcemia is treated with IV calcium gluconate infusion.
PITUITARY DISORDERS
Pituitary disorders are not common in pregnancy; pituitary dysfunction is commonly associated with anovulatory infertility.
• Pituitary hormone release is under hypothalamic control. The anterior pituitary (adenohypophysis) releases adrenocorticotropin (ACTH), TSH, prolactin, GH, follicle-stimulating hormone (FSH), luteinizing hormone (LH), and endorphins. The posterior pituitary (neurohypophysis) contains the nerve terminals projecting from the hypothalamus that release oxytocin and antidiuretic hormone (ADH; also called arginine vasopressin [AVP]).
• During normal pregnancy, the pituitary gland may more than double in size. Lactotroph growth in response to
estrogen leads to increased serum prolactin levels,
P.194 whereas ACTH release increases in response to placental corticotropin-releasing hormone (CRH). LH and FSH secretion are decreased in pregnancy. Pituitary GH and TSH decrease as placental GH and hCG rise, respectively. ADH secretion may be increased in pregnancy, but placental vasopressinase increases degradation, leading to a lowered plasma osmolality setpoint (i.e., 5 to 8 mOsm/kg decrease).
• The differential diagnosis of pituitary dysfunction includes tumor, infarction, autoimmune/inflammatory disease, infection, infiltrative processes, head trauma, sporadic or familial genetic mutations, prior surgery or radiotherapy, hypothalamic lesions, and empty sella syndrome.
Prolactinoma
• Prolactinoma is the most common pituitary tumor of reproductive age women. Elevated prolactin can cause amenorrhea, anovulation, infertility, and galactorrhea. With increasing size and mass effect, prolactinoma can cause headaches, visual changes, and diabetes insipidus.
• Pituitary adenomas are classified as microadenomas, which are ≤10 mm in size and rarely (10 mm in diameter, during pregnancy. Up to one third of previously untreated macroadenomas, however, may become symptomatic during pregnancy.
• Initial diagnosis is by history, physical exam, and computed tomography (CT) or magnetic resonance imaging (MRI) of the head. Serum prolactin may not be useful during pregnancy due to normal pregnancy-induced elevations. Patients with microadenomas can be monitored for symptoms at each prenatal visit, with visual field testing and MRI if visual symptoms develop. Patients with macroadenomas should have baseline visual field testing early in pregnancy and referral for endocrinology and ophthalmology consults can be considered.
• T reatment of symptomatic prolactinoma is with dopamine agonists, which mimic the prolactin-inhibiting factor activity of hypothalamic dopamine. Bromocriptine (drug of choice; 2.5 to 5 mg daily) or cabergoline (0.5 to 3 mg weekly) can shrink the adenoma and decrease serum prolactin levels. Patients taking these medications should stop them during pregnancy unless they have a symptomatic or large tumor. Transsphenoidal surgical resection of the macroadenoma is indicated for macroadenomas or high prolactin levels that are not controlled with medication. Radiotherapy can also be used to treat persistent disease. Radiologic evaluation and serum prolactin testing should be followed after treatment.
Acromegaly
• Acromegaly is caused by a GH-secreting pituitary adenoma. Symptoms include coarsened facial features, prominent chin, large feet, spade-like hands, irregular menses, headaches, visual changes, hyperhidrosis, arthralgias, and carpal tunnel syndrome. Usually, these women are infertile, with hyperprolactinemia and anovulation. In the rare patient with acromegaly who becomes pregnant, there are no deleterious or teratogenic effects for the fetus. Carbohydrate intolerance, hypertension, and cardiac abnormalities may complicate pregnancy, however. Laboratory testing shows elevated serum insulin-like growth factor 1 (IGF-1) levels and nonsuppressed GH during glucose tolerance testing (100-g glucose load normally suppresses GH release). Diagnosis during pregnancy is complicated by placental GH secretion. Head CT or MRI can localize the tumor. Treatment is with surgical excision; radioablation; or medical treatment with bromocriptine, somatostatin analogues (e.g., octreotide or lanreotide), or the newer GH receptor antagonist pegvisomant.
P.195
Diabetes Insipidus
• Diabetes insipidus (DI) results from abnormal water homeostasis. Central DI results from decreased
ADH/vasopressin release due to pituitary tumor, metastases, granuloma, infection, trauma, or global pituitary failure. Nephrogenic DI due to renal resistance to ADH hormone is rare and primarily found in males.
Psychogenic DI is due to massive free water consumption. Subclinical DI may be identified during pregnancy when ADH/vasopressin metabolism is increased. Viral hepatitis, preeclampsia, HELLP syndrome, and acute fatty liver of pregnancy (AFLP) can also exacerbate or promote DI. Polyuria (>3 L/day) and polydipsia are the clinical hallmarks of DI.
• Diagnosis is by the water deprivation test, showing low urine osmolality and high plasma osmolality with fluid restriction. L-Deamino-I-D-arginine vasopressin (DDAVP) injection corrects central DI and can be helpful in confirming the diagnosis. Head CT or MRI may be used to identify pituitary lesions.
• T reatment is with synthetic ADH/vasopressin (i.e., DDAVP) at 10 to 25 pg/day intranasally. Higher doses may be required during pregnancy.
Other Pituitary Disorders
• Sheehan syndrome results from pituitary necrosis following massive blood loss. Clinical findings include tachycardia, postural hypotension, hypoglycemia, galactorrhea, anorexia, nausea, lethargy, weakness, weight loss, decreased pigmentation, periorbital edema, normocytic anemia, and DI. Approximately 4% of patients with obstetric hemorrhage may have mild pituitary dysfunction, but frank Sheehan syndrome can present up to 20 years later. Diagnosis requires laboratory testing for stimulated pituitary hormone secretion (i.e., after injecting hypothalamic-releasing hormones). Random blood hormone levels are not useful.
• Lymphocytic hypophysitis is caused by autoimmune lymphocyte and plasma cell infiltration with destruction of the pituitary gland, similar to Sheehan syndrome. Pituitary dysfunction can vary widely, and mass effect may cause headache with visual changes. Head CT or MRI may be helpful in diagnosis. Surgery is reserved for severe symptoms from mass effect.
ADRENAL DISORDERS
Adrenal disorders are not pregnancy induced but do persist during pregnancy, causing significant morbidity without prompt diagnosis. The adrenal gland is profoundly affected by pregnancy and its physiologic changes. CRH is secreted by the placenta, stimulating ACTH release from the pituitary that increases cortisol production in maternal adrenal glands. Cortisol clearance is also decreased, leading to more than twofold increase in total and free serum cortisol levels by the third trimester. Aldosterone production is stimulated by elevated renin/angiotensin II levels in pregnancy; renin activity peaks by the second trimester. Androgen levels are increased five- to eightfold, whereas dehydroepiandrosterone sulfate (DHEA-S) is decreased in pregnancy.
Cushing Syndrome
• Cushing syndrome results from long-term exposure to glucocorticoids, either from exogenous steroid use (as in treatment of lupus erythematosus, sarcoidosis, or severe asthma) or from increased endogenous hormone production (from excessive pituitary ACTH production, adrenal hyperplasia, or adrenal neoplasia). Adrenal hyperplasia is the most common cause of Cushing syndrome in pregnancy (up to 50%), with a relative decrease in other etiologies.
P.196
• Signs and symptoms include moon facies, buffalo hump, truncal obesity, striae, fatigue, weakness, hirsutism, easy bruising, nephrolithiasis, mental status changes, and hypertension.
• Diagnosis is by laboratory testing, showing increased plasma cortisol levels or increased 24-hour urine free cortisol. It can be difficult to identify mild cases due to the normal pregnancy-induced changes in cortisol levels. The dexamethasone suppression test can be used to differentiate a pituitary cause (i.e., Cushing syndrome) from adrenal or exogenous sources of the increased cortisol. Head or abdominal CT or MRI is recommended to localize tumors in the pituitary or adrenal gland.
• T reatment of Cushing syndrome entails medical management of blood pressure and subsequent surgical excision of pituitary or adrenal adenoma. Medical management of the pregnant patient until delivery is usually preferred, although maternal morbidity may be higher with adrenal adenomas, prompting earlier surgical treatment. Metyrapone has been used to block cortisol secretion with adrenal hyperplasia, although it crosses the placenta, may affect fetal adrenal function, and has been associated with preeclampsia. Ketoconazole has been associated with IUGR and may have potential antiandrogen activity; mifepristone is contraindicated in pregnancy.
• Prognosis is improved with early detection and close management, although these patients are at increased risk for maternal complications including hypertension, DM, preeclampsia, cardiac problems, and death. There is increased risk for perinatal complications including IUGR, preterm delivery (up to 50%), stillbirth, and neonatal death.
Hyperaldosteronism
• Hyperaldosteronism can result from adrenal aldosteronoma or carcinoma (about 75%) and bilateral adrenal hyperplasia (about 25%). Symptoms include hypertension, hypokalemia, and weakness. Laboratory testing shows increased serum or urine aldosterone and low plasma renin levels. MRI can be used to identify and localize an adrenal tumor. Definitive treatment is tumor resection, which can be performed laparoscopically in the second trimester. Medical management is potassium supplementation and treatment of hypertension. Calcium channel blockers or beta-blockers are preferred agents for blood pressure control, with spironolactone contraindicated in pregnancy.
Pheochromocytoma
• Pheochromocytoma is a rare catecholamine-secreting tumor of chromaffin cells. Ninety percent arise in the adrenal medulla and 10% in sympathetic ganglia. Ten percent of tumors are bilateral. Ten percent are malignant. It is associated with medullary thyroid cancer and hyperparathyroidism in multiple endocrine neoplasia (MEN) type 2 syndromes.
• When diagnosed during pregnancy, pheochromocytoma increases maternal mortality to approximately 10%. Fetal mortality increases to nearly 50%, even though the catecholamines do not cross the placenta or directly affect the fetus. IUGR is common, but there is no increased neonatal mortality after delivery. When the diagnosis is not made before delivery, postpartum maternal mortality increases to about 50%.
• Signs and symptoms of pheochromocytoma include paroxysmal or sustained hypertension, headaches, anxiety, chest pain, visual changes, palpitations, diaphoresis, nausea and vomiting, pallor or flushing, abdominal pain, and seizures. The differential diagnosis should include preeclampsia and other hypertensive diseases.
• Diagnosis is by laboratory testing showing elevated catecholamines, metanephrines, and vanillylmandelic acid in a 24-hour urine specimen. Methyldopa should be discontinued before this test, as it will give a false-positive result. Abdominal CT or MRI can be used for localizing the tumor in pregnancy; myocardial perfusion scan can identify extra-adrenal sites.
P.197
• Definitive treatment is adrenalectomy, although timing of surgical intervention is controversial: generally, it is recommended either gestation in a patient known to be previously normotensive. Trophoblastic disease or multiple gestation can present with preeclampsia before 20 weeks' gestation.
• Mild preeclampsia is defined by the following criteria:
î BP ≥ 140/90 mm Hg confirmed on two measures at least 6 hours but not more than 7 days apart, and
P.199 î Proteinuria ≥300 mg on a 24-hour urine collection or two random urine dipstick results of at least 30 mg/dL (“1+”). Spot urine protein: Creatinine ratios are used by some investigators instead of 24-hour urine collection and show good predictive value in the lower and higher ranges.
î Preeclamptic patients often have wide variation in urine protein values over time, possibly from renal vasospasm. Discrepancies between the random urine dipstick and 24-hour urine collection measurements have been well described. The 24-hour urine collection, therefore, remains the preferred measure for diagnosing preeclampsia.
• Severe preeclampsia is classified by the following criteria:
î BP during bed rest of ≥ 160 mm Hg systolic or ≥110 mm Hg diastolic; or
î Proteinuria ≥5 g on a 24-hour urine collection even if BP is in the mild range. Persistent urine dipstick ≥3+ also qualifies; or
î Signs, symptoms, or lab values of severe preeclampsia with any elevated BP.
• Symptoms of preeclampsia may include the following: cerebral or visual disturbances (e.g., persistent headache, blurred vision, scotomata, and blindness from retinal detachment); epigastric, right upper quadrant, or constant low abdominal pain from liver dysfunction or from abruptio placentae; nausea and vomiting; dyspnea from pulmonary edema; decreased urine output, hematuria, or rapid weight gain >5 pounds in 1 week; and absent or decreased fetal movement.
• Physical findings of preeclampsia may include the following:
î Elevated BP measured in the sitting or semireclined position with the arm positioned roughly at heart level
î Nondependent or generalized edema
î Pulmonary edema, with rales or crackles on lung examination
î Epigastric or right upper quadrant tenderness without a known cause, likely secondary to hepatic edema
î Uterine tenderness or tetany secondary to placental abruption
î Oliguria with 24-hour urine output 70 IU/L)
î Thrombocytopenia with platelet count of 100,000/L or less
î Prolonged prothrombin and partial thromboplastin times that may be due to primary coagulopathy, hepatic synthesis dysfunction, or abruptio placentae leading to disseminated intravascular coagulation
î Decreased fibrinogen, increased fibrin degradation products, or both, as a result of coagulopathy or abruptio placentae
• Fetal findings of preeclampsia may include intrauterine growth restriction (IUGR), oligohydramnios, and other signs of uteroplacental insufficiency.
P.200
• Preeclampsia superimposed on chronic hypertension occurs in patients with preexisting high BP.
Differentiating chronic hypertension with superimposed preeclampsia from a gestational exacerbation of chronic hypertension can be difficult, especially if there is baseline proteinuria. In general, diagnosis requires a significant change from baseline proteinuria and worsening hypertension or the development of symptoms.
• HELLP syndrome is a variant of preeclampsia defined by the following criteria:
î Hemolysis identified by burr cells and schistocytes on an abnormal peripheral smear, an elevated serum bilirubin (>1.2 mg/dL) or LDH level (>600 IU/L), or a low serum haptoglobin
î Thrombocytopenia with platelets ≤100,000∕pL is the most consistent finding in HELLP syndrome.
î Elevated liver function tests (i.e., transaminases) greater than two times the upper limit of normal
î Note that hypertension may be absent (12% to 18% of cases), mild (15% to 50%), or severe (50%). Proteinuria may be absent as well (13%).
• Eclampsia is seizure or unexplained coma in a patient with preeclampsia. Eclampsia can present without hypertension (16%) or proteinuria (14%).
CHRONIC HYPERTENSION
Chronic hypertension carries increased risk for superimposed preeclampsia, preterm delivery, abruptio placentae, and IUGR. See Chapter 1 for general classification and treatment of hypertension.
• The differential diagnosis of chronic hypertension in pregnancy includes the following:
• Essential hypertension, which accounts for 90% of hypertension outside of pregnancy
• Kidney disease, adrenal disorders (e.g., primary aldosteronism, congenital adrenal hyperplasia, Cushing syndrome, pheochromocytoma), hyperthyroidism, newonset collagen vascular disease, systemic lupus erythematosus, aortic coarctation, chronic obstructive sleep apnea, and cocaine use
• Worsening chronic hypertension is difficult to distinguish from superimposed preeclampsia. If seizures, thrombocytopenia, pulmonary edema, unexplained hemolysis, or elevation in liver enzyme levels develop, superimposed preeclampsia should be diagnosed. Monitoring trends in BP and urine protein may also be helpful.
î A 24-hour urine calcium measurement may be useful. Urine calcium with preeclampsia is lower than in patients with hypertension alone.
î A value T reatment for chronic hypertension or persistently elevated BPs can include the following during pregnancy:
î Labetalol—an α1 and nonselective β-adrenergic antagonist that can be used as monotherapy or combined with hydralazine or a diuretic. The initial dose is 100 mg twice daily and may be increased in increments of 100 mg twice daily every 2 to 3 days to a maximum of 2,400 mg daily. It is contraindicated in patients with greater than first-degree heart block. Chronic beta-blocker use in pregnancy has a mild association with IUGR.
î Nifedipine—a calcium channel blocker used commonly in pregnancy that allows convenient daily dosing with the sustained release formulation. A multicenter prospective study of first-trimester drug exposure to calcium antagonists found no increased teratogenicity. The initial dose of nifedipine is 30 mg daily. The dose can be increased to 60 mg daily if adequate response is not seen in 7 days. The maximum daily dose is 90 mg. There is a theoretical risk of neuromuscular blockade when magnesium and nifedipine are administered together, although this was not supported in retrospective studies.
î Methyldopa (Aldomet)—a centrally acting sympathetic outflow inhibitor that decreases systemic vascular resistance and is safe in pregnancy. Side effects include hepatic damage; therefore, liver function tests should be monitored at least once per trimester. Starting dose is 250 mg orally three times daily with a maximum dose of 3 g/day. The dose may be adjusted at increased in intervals of not less than every 2 days.
î Hydralazine—a direct peripheral vasodilator that can be combined with methyldopa or a beta-blocker. It can cause a lupus-like syndrome but usually only at doses higher than 200 mg/day for an extended time. The starting oral dose is 10 mg four times a day and may be increased to a maximum of 200 mg/day.
î Thiazide diuretics—inhibit renal sodium and chloride reabsorption. A large meta-analysis found no adverse outcomes in pregnancy; however, decreased plasma volume from diuresis carries a theoretic risk of placental insufficiency,
P.202 which deters its use as a first-line agent. The initial dose of hydrochlorothiazide (HCTZ) is 12.5 to 25 mg daily, titrated every 2 to 3 weeks to a maximum daily dose of 50 mg daily. Diuretics are not recommended in the setting of preeclampsia, uteroplacental insufficiency, or IUGR. Serum uric acid increases with thiazide diuretics, limiting diagnostic options for preeclampsia.
î Angiotensin-converting enzyme (ACE) inhibitors—inhibit angiotensin I conversion to the vasoconstrictor angiotensin II. ACE inhibitors are contraindicated in pregnancy due to the risk of fetal death in the second and third trimesters and neonatal renal failure and pulmonary failure. There is also an unconfirmed report of first-trimester teratogenicity. Angiotensin antagonists are also contraindicated due to their similar effects on the angiotensin-renal system.
• Severe range BPs: Elevated sustained BPs ≥160 systolic or ≥ 105 to 110 diastolic warrant immediate therapy with intravenous (IV) antihypertensives, including labetalol or hydralazine for the prevention of acute morbidity from hypertensive urgency. See discussion later under “Preeclampsia” and antihypertensive therapy.
• Delivery: Timing of delivery should be tailored to the individual patient. In general, those who do not require antihypertensive medications should be delivered at 38 0/7 to 39 6/7 weeks. Those controlled with antihypertensive medication should be delivered at 37 0/7 to 39 6/7 weeks, and those with difficult to control hypertension at 36 0/7 to 37 6/7 weeks.
GESTATIONAL HYPERTENSION
Gestational hypertension is the most common etiology of hypertension in pregnancy, affecting 6% to 7% of nulliparous and 2% to 4% of parous women. The incidence increases with a history of preeclampsia and in multiple gestations. Earlier diagnosis of gestational hypertension increases the risk of preeclampsia; up to 50% of those with hypertension before 30 weeks will progress to preeclampsia.
• Prognosis and management depend on timing and severity.
• Mild gestational hypertension after 37 weeks has a similar outcome to normotensive patients but an increased rate of labor induction and cesarean section.
î If 37 weeks (full term), deliver if the cervix is favorable; otherwise, close followup may be permitted with delivery achieved between 37 0/7 and 38 6/7 weeks.
• Severe gestational hypertension, especially in early pregnancy, increases fetal and maternal morbidity even more than mild preeclampsia. Risks include placental abruption, preterm delivery, and small-for- gestational-age infants.
î When BP is 160/110 or greater, antihypertensive therapy is indicated, as mentioned earlier. The goal is to maintain uteroplacental perfusion but gently reduce systolic and diastolic BP to the mild hypertensive range.
î If the response to medical therapy is inadequate, the patient must be admitted to the antepartum service for close monitoring.
PREECLAMPSIA
Preeclampsia occurs in 2% to 7% of healthy nulliparous women and 1 % to 5% of parous women. The incidence is higher in twin pregnancies (14%) and for women with a history of preeclampsia (18%). It is the third leading cause of maternal
P.203 mortality, responsible for over 17% of maternal deaths, and a major cause of neonatal morbidity and mortality.
• Risk factors for preeclampsia include:
• Nulliparity
• Multiple gestation
• Obesity
• Chronic hypertension (15% to 50% of cases)
• Systemic lupus erythematosus
• Thrombophilia
• Pregestational diabetes (10% to 36% of cases)
• Kidney disease
• History of preeclampsia or eclampsia
• Poor outcome in a previous pregnancy
• Family history of preeclampsia, eclampsia, or cardiovascular disease
• Molar pregnancy
• Conception via assisted reproductive technologies
• Abnormal uterine Doppler studies at 18 and 24 weeks
• The pathophysiology of preeclampsia requires the presence of trophoblastic tissue but not necessarily a fetus (e.g., molar pregnancy). Proposed mechanisms include impaired trophoblastic differentiation and invasion, immunologic response to pregnancy, and placental or endothelial abnormalities. The temporal sequence and relative importance of these alterations are under investigation.
• The best preventive measures for preeclampsia are early evaluation, risk reduction, and optimizing maternal health. Women with preeclampsia in the second trimester have a recurrence rate as high as 65%. In patients at high risk for development of preeclampsia (history of early onset or severe growth restriction), low-dose aspirin therapy has been shown to reduce the risk of preeclampsia, perinatal mortality, preterm birth, and small-for-gestational-age infants. Supplementation with fish oil, calcium, or vitamins C and E and early antihypertensive therapy are ineffective.
• Diagnosis of preeclampsia is by symptoms and signs, including elevated BP and abnormal laboratory findings (described earlier).
• Definitive management for gestational hypertension, preeclampsia, and eclampsia is delivery.
• In general, mild preeclampsia (see definitions earlier) at term is treated by delivery.
î Optimal treatment prior to 37 weeks is usually expectant management. The benefits of bed rest, antihypertensive medications, and hospitalization are not clearly established. There are no large, randomized trials on the management of mild preeclampsia.
î Close maternal and fetal observation is essential, but there is no standard protocol for testing or frequency.
î Fetal monitoring can include growth ultrasound and amniotic fluid assessment every 3 to 4 weeks, umbilical artery Doppler velocimetry, and once or twice weekly NST or BPP.
î Maternal monitoring can include weekly or semiweekly BP check and evaluation and periodic lab testing such as 24-hour urine protein, serum creatinine, platelet count, and serum transaminases to detect progression to severe preeclampsia.
î A gestational age of >34 weeks with progressive labor, uncontrolled hypertension, abnormal fetal testing, or growth restriction should prompt delivery.
P.204
The first priority in treating severe preeclampsia is to assess and stabilize the mother.
î At ≥34 weeks, delivery is indicated, although immediate cesarean section is not usually warranted.
î Patients in labor, or with a favorable cervix, can deliver vaginally. Careful monitoring, at least hourly assessments, and strict intake/output recordings should be maintained.
î Between 24 and 34 weeks, expectant management is acceptable if BP is adequately controlled with antihypertensive agents, fetal testing is reassuring, and there is no evidence of IUGR.
î Magnesium sulfate and IV antihypertensives may be given initially while betamethasone is administered for fetal lung maturity.
î Fluid status should be monitored.
î CBC, platelets, and liver function tests should be checked daily.
î Fetal surveillance with NST or BPP should be performed at least weekly and patients should be instructed regarding maternal assessment of fetal movement.
î Delivery is indicated by the following: IUGR, nonreassuring fetal tracing, eclampsia, neurologic deficits, pulmonary edema, right upper quadrant/epigastric pain, oliguria 1.5, disseminated intravascular coagulation, HELLP, placental abruption, or uncontrolled severe BP.
î At 24 weeks’ gestation and earlier, expectant management is associated with high maternal morbidity and limited perinatal benefit.
î Expectant management of severe preeclampsia with IUGR has been associated with increased risk of fetal death (rate of perinatal death is 5.4%).
• Seizure prophylaxis during labor and for 24 hours postpartum is recommended for patients with preeclampsia. Some patients with severe persistent preeclampsia need seizure prophylaxis for longer periods before and after delivery.
î Magnesium sulfate (MgSO4) is the agent of choice for eclamptic seizure prophylaxis. MgSO4 has been shown to decrease the risk of eclampsia by more than 50%.
î For prophylaxis, we administer a loading dose of 4 g MgSO4 IV over 15 to 20 minutes.
î Maintenance dose is 2 g/hr IV (dose should be titrated down if the patient has poor urine output, poor kidney function, or an elevated serum creatinine).
î If there is no IV access, the loading dose is 5 g MgSO4 (50% solution) administered intramuscularly in each buttock (10 g total), with a maintenance dose of 5 g in alternating buttocks every 4 hours.
î The therapeutic serum magnesium level for seizure prophylaxis depends on the laboratory. In general, the therapeutic range is 4 to 6 mEq/L. However, it is our practice to follow magnesium levels only for those patients in whom we are unusually concerned for developing supratherapeutic levels. For such patients, check serum magnesium level 4 hours after the loading dose, then every 6 hours as needed or if symptoms suggest magnesium toxicity.
î Diuresis is a useful criterion for early cessation of seizure prophylaxis. Urine output equal to or exceeding 100 mL/hr for 2 hours suggests resolving preeclampsia with no or rare complications.
î Patients are monitored hourly for signs and symptoms of magnesium toxicity:
• Loss of patellar reflexes at 8 to 10 mEq/L
• Respiratory depression or arrest at 12 mEq/L
P.205
• Mental status changes at > 12 mEq/L followed by ECG changes and arrhythmias
• If magnesium toxicity develops, check the patient's vital signs, stop magnesium and check plasma levels, administer 1 g calcium gluconate IV over 3 minutes, and consider diuretics (e.g., furosemide, mannitol).
î Phenytoin (Dilantin) is a secondary agent for eclamptic seizure prophylaxis. Magnesium was clearly superior in a large randomized clinical trial and is preferred. It may, however, be contraindicated as in patients with myasthenia gravis.
î The loading dose is maternal weight based. For 70 kg, load with 1,500 mg phenytoin.
î The first 750 mg of the loading dose should be given at 25 mg/min and the rest at 12.5 mg/min. If the patient maintains normal cardiac rhythm and has no history of heart disease, ECG monitoring is not necessary at this infusion rate.
î Check the serum phenytoin level at 30 to 60 minutes after infusion.
î A therapeutic level is > 12 pg/mL; recheck level in 12 hours.
î If the level is Systemic lupus erythematosus flare
• Antiphospholipid antibody syndrome
• Cholecystitis
• Fulminant hepatitis (of any cause)
• Acute pancreatitis
• Disseminated herpes zoster
• Management is the same as for severe preeclampsia. Platelet transfusion may be required immediately prior to delivery depending on severity of thrombocytopenia. Short-term expectant management in order to allow for administration of betamethasone for fetal lung maturity may be possible in a very select group of patients with HELLP prior to 34 weeks; however, there are no data suggesting improved perinatal outcomes with this approach.
ECLAMPSIA
Eclampsia should be the presumed diagnosis in obstetric patients with seizures and/or coma without a known history of epilepsy. The incidence of eclampsia is between 1 in 2,000 and 1 in 3,500 pregnancies in developed countries. Eclampsia occurs in about 1% of patients with preeclampsia. Virtually all eclampsia is preceded by preeclampsia.
• The pathophysiology of eclamptic seizures is unknown but may occur when mean arterial pressure exceeds the capacity of cerebral autoregulation, leading to cerebral edema and increased intracranial pressure.
• Eclampsia can occur antepartum, peripartum, or postpartum and has been reported as late as 3 to 4 weeks postpartum. Patients may have associated hypertension and proteinuria; a small percentage has neither.
P.207
• Management of eclampsia is an obstetric emergency that requires immediate treatment, including:
• Appropriate management of ABCs (airway, breathing, and circulation) with measures taken to avoid aspiration
• Seizure control with 4 to 6 g MgSO4 IV bolus. If the patient has a seizure during or after the loading dose, an additional 2 g IV bolus of MgSO4 can be given.
• T reatment of seizures refractory to MgSO4 with IV phenytoin or a benzodiazepine (e.g., lorazepam)
• T reatment of status epilepticus with lorazepam 0.1 mg/kg IV at a rate ≥2 mg/min. Patients with status epilepticus may require intubation to correct hypoxia and acidosis and to maintain a secure airway.
• Prevention of maternal injury with padded bedrails and appropriate positioning
• Control of severe hypertension (see medications mentioned earlier)
• Delivery after maternal stabilization
î During acute eclamptic episodes, fetal bradycardia is common. It usually resolves in 3 to 5 minutes. Allowing the fetus to recover in utero from the maternal seizure, hypoxia, and hypercarbia before delivery is optimal. However, if fetal bradycardia persists beyond 10 minutes, abruptio placentae should be suspected.
î Emergency cesarean section should always be anticipated in case of rapid maternal or fetal deterioration.
• Outcomes depend on the severity of disease. Perinatal mortality in the United States ranges from 5.6% to
11.8%, mainly due to extreme prematurity, placental abruption, and IUGR. The maternal mortality rate is from in Pregnancy
• Signs and symptoms of cardiac disease overlap common symptoms and findings in pregnancy including fatigue, shortness of breath, orthopnea, palpitations, edema, systolic flow murmur, and a third heart sound.
• Evaluation of cardiac disease includes a thorough history and physical examination. Noninvasive testing includes an electrocardiogram (ECG), chest radiograph, and an echocardiogram. The ECG may reveal a leftward shift of the electrical axis, especially during the third trimester when the diaphragm is pushed upward by the uterus. Ventricular extrasystoles are a common finding. Routine chest radiographs are used to assess cardiomegaly and pulmonary vascular prominence. Echocardiographic evaluation of ventricular function and structural anomalies is invaluable for diagnosis of cardiac disease in pregnancy. Many changes including mild valvular regurgitation and chamber enlargement are normal findings on echocardiogram during pregnancy.
Management of Patients with Known Cardiac Disease
• Before conception: Whenever possible, women with preexisting cardiac lesions should receive preconception counseling regarding maternal and fetal risks during pregnancy and long-term maternal morbidity and mortality. The New York Heart Association (NYHA) functional class (T able 15-1) is used as a predictor of outcome. Women with NYHA class III and IV face a mortality rate of 7% and morbidity over 30%. These women should be strongly cautioned against pregnancy. A risk index using four risk factors has been shown to accurately predict a woman's chance of having adverse cardiac or neonatal complications: (a) a prior cardiac event, (b) cyanosis or poor functional class, (c) left heart obstruction, and (d) systemic ventricular dysfunction. With two or more risk factors, the chance of cardiac event approaches 75%.
P.210
• After conception: Pregnant patients with significant history require cardiac assessment as early as possible. If the pregnancy poses a serious threat to maternal health, the patient should be counseled about the option of pregnancy termination. Patients need close monitoring and follow-up by both a perinatologist and cardiologist, with attention to signs or symptoms of worsening congestive heart failure (CHF) throughout the pregnancy. Each visit should include the following: (a) cardiac examination and cardiac review of systems; (b) documentation of weight, blood pressure, and pulse; and (c) evaluation of peripheral edema.
• During pregnancy: The most common cardiac complications of pregnancy include arrhythmia and CHF. If symptoms worsen, hospitalization, bed rest, diuresis, or correction of an underlying arrhythmia may be required. Sometimes, surgical correction during pregnancy becomes necessary. When possible, procedures should be performed during the early second trimester to avoid the period of fetal organogenesis and before more significant hemodynamic changes of pregnancy occur. Pregnancy is also a time of hypercoagulability, and anticoagulation should be started if appropriately indicated.
TABLE 15-1 New York Heart Association (NYHA) Functional Classification
NYHA Symptoms
Class
I No symptoms and no limitation in ordinary physical activity such as shortness of breath when walking or climbing stairs.
II Mild symptoms (mild shortness of breath and/or angina) and slight limitation during ordinary activity.
III Marked limitation in activity due to symptoms, even during less-than-ordinary activity such as walking short distances (20-100 m). Comfortable only at rest.
IV Severe limitations. Experiences symptoms even while at rest. Mostly bedbound.
Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 8th ed. Boston, MA Little Brown, 1979.
Antibiotic Prophylaxis for Endocarditis
• American College of Obstetricians and Gynecologists (ACOG) has endorsed the 2007 American Heart Association (AHA) guidelines for prevention of infective endocarditis (IE) which represent a marked change from prior AHA guidelines. Antibiotic prophylaxis is no longer recommended, as IE is more likely to result from frequent random bacteremia with daily activities than from bacteremia caused by specific dental, gastrointestinal (GI), or genitourinary (GU) procedures. Prophylaxis is now based on the risk of adverse outcome with the procedure, and it is not recommended for GU procedures, except in high-risk patients with GU infections, to prevent wound infection and sepsis. Antibiotic prophylaxis for IE is not recommended for vaginal delivery or hysterectomy (see Chapter 27).
Specific Cardiac Conditions
Cardiomyopathy
• Cardiomyopathy can be genetic, idiopathic, or caused by myocarditis or toxins and manifests during pregnancy with signs and symptoms of CHF. These include chest pain, dyspnea, paroxysmal nocturnal dyspnea, and cough. Echocardiography demonstrates chamber enlargement and reduced ventricular function. The heart becomes uniformly dilated, filling pressures increase, and cardiac output decreases. Eventually, heart failure develops and is often refractory to treatment. The 5-year survival rate is approximately 50%; therefore, careful preconception counseling is important, even if the patient is asymptomatic.
• Hypertrophic cardiomyopathy with or without left ventricular outflow tract obstruction is an autosomal dominant disorder with a variable phenotype and incidence of 0.1% to 0.5% in pregnancy. Most women with hypertrophic cardiomyopathy do well in pregnancy, and complications are uncommon with prior prepregnancy risk stratification via NYHA functional class and multidisciplinary specialist management. Risk is increased in patients that are symptomatic or if there is significant left ventricular outflow obstruction. The potential exists for poor tolerance of the circulatory overload of pregnancy. Major complications include pulmonary edema secondary to diastolic dysfunction, dysrhythmias secondary to myofibrillar disarray, functional class decline, obstetric complications, and poor fetal outcomes. During pregnancy, beta-blockers should be continued and the judicious use of diuretics may be required to treat symptoms of dyspnea.
P.211
• Peripartum cardiomyopathy is an idiopathic dilated cardiomyopathy that typically develops in the last month of pregnancy or within 5 months of delivery and is characterized by left ventricular systolic dysfunction with ejection fraction (EF) postpartum, including detection and management of possible autotransfusion-induced pulmonary edema.
Valvular Disease
• Mitral valve prolapse (MVP) is the most common congenital heart defect in women. It rarely has implications for maternal or fetal outcomes. It is the most common cause of mitral regurgitation (MR) in women.
• MR is usually well tolerated during pregnancy. The fall in systemic vasoresistance improves cardiac output in pregnancy. Medical management includes diuretics in the rare event of pulmonary congestion or vasodilators for systemic HTN. Acute, severe worsening of MR can result from ruptured chordae and must be repaired surgically. Women with severe MR before pregnancy should undergo operative repair before conception. Patients with advanced disease may require central monitoring during labor.
• Aortic regurgitation (AR): AR may be encountered in women with rheumatic heart disease, a congenitally bicuspid or deformed aortic valve, IE, or connective tissue disease. AR is generally well tolerated during pregnancy. Medical management includes diuretics and vasodilators. Ideally, women with severe AR should undergo operative repair before conception; as in MR, surgery during pregnancy should be considered only for control of refractory NYHA functional class III or IV symptoms.
• Aortic stenosis (AS): The most common etiology of AS in pregnant women is a congenitally bicuspid valve. Mild AS with normal left ventricular function is usually well tolerated during pregnancy. Asymptomatic severe stenosis can be managed conservatively with bed rest, oxygen, and beta-blockade. Moderate to severe AS markedly increases the medical risk of pregnancy; patients are advised to delay conception until correction is performed. Symptoms, such as dyspnea, angina pectoris, or syncope, usually become apparent late in the second trimester or early
P.212 in the third trimester. Women with bicuspid aortic valves are also at increased risk for aortic dissection and should be followed carefully. Aortic root enlargement >40 mm or an increase in aortic root size during pregnancy are risk factors for dissection. Beta-blockers may be indicated in these patients.
• Severe symptomatic AS can be managed by percutaneous aortic balloon valvuloplasty prior to labor and delivery but not without significant risk to both mother and fetus. If presenting early in pregnancy, termination should be discussed before surgical correction of severe AS (EF 45 mm, or symptomatic ventricular dysfunction with EF Coarctation of the aorta: Severe cases of coarctation of the aorta are usually corrected in infancy. Surgical correction during pregnancy is recommended only if dissection occurs. Some studies suggest that patients with a history of coarctation have increased rates of preeclampsia, gestational HTN, and preterm labor. Coarctation of the aorta is associated with other cardiac lesions such as berry aneurysms. Two percent of infants of mothers with coarctation of the aorta may have other cardiac lesions. Coarctation of the aorta is characterized by a fixed cardiac output. Therefore, the patient's heart cannot increase its rate to meet the increased cardiac demands of pregnancy, and extreme care must be taken to prevent hypotension, as with AS.
• Septal defects: Young women with uncomplicated secundum-type ASD or isolated VSD usually tolerate pregnancy well. ASD is the most common congenital heart lesion in adults. ASDs are usually very well tolerated unless they are associated with pulmonary HTN. Complications, such as atrial arrhythmias, pulmonary HTN, and heart failure, usually do not arise until the fifth decade of
P.214 life and are therefore uncommon in pregnancy. VSDs usually close spontaneously or are closed surgically if the lesion is large. For this reason, significant VSDs are rarely seen in pregnancy. Rarely, uncorrected lesions lead to significant left-toright shunts with pulmonary HTN, right ventricular failure, arrhythmias, and reversal of the shunt. The incidence of VSD in the offspring of affected parents is 4%; however, small VSDs are often difficult to detect antenatally.
• Patent ductus arteriosus (PDA): PDA is not associated with additional maternal risk for cardiac complications if the shunt is small to moderate and if pulmonary artery pressures are normal. Moderate to large PDA may be associated with increased volume, left heart failure, and pulmonary HTN or other pulmonary abnormalities. Therefore, pregnancy is not recommended for patients with large PDA and associated complications.
• Eisenmenger syndrome occurs when an initial left-to-right shunt results in pulmonary arterial obliteration and pulmonary HTN, eventually leading to a right-to-left shunt. This serious condition carries a maternal mortality rate of 50% and a fetal mortality rate of more than 50% if cyanosis is present. In addition, 30% of fetuses exhibit intrauterine growth restriction. Because of increased maternal mortality, pregnancy is generally contraindicated, and termination of the pregnancy should be discussed. If the pregnancy is continued, special precautions must be taken during the peripartum period. Women with Eisenmenger syndrome tolerate hypotension poorly. The patient should be monitored with a Swan-Ganz catheter, and care should be taken to avoid hypovolemia. Postpartum death most often occurs within 1 week after delivery; however, delayed deaths up to 4 to 6 weeks after delivery have been reported.
• Marfan syndrome is an autosomal dominant disorder of the fibrillin gene characterized by connective tissue fragility. Cardiovascular manifestations include aortic root dilation and dissection, MVP, and aneurysms. Genetic counseling is recommended. According to the 2010 American College of Cardiology (ACC)ZAHAZAmerican Association of Thoracic Surgeons guidelines, patients with a dilated aortic root >40 mm are considered high-risk. If cardiovascular involvement is minor and the aortic root diameter is smaller than 40 mm, the risk in pregnancy is less than 1 %. If cardiovascular involvement is more extensive or the aortic root is larger than 40 mm, complications during pregnancy and aortic dissection are increased significantly. Patients should be monitored with serial physical exams as well as echocardiography. HTN should be avoided. Beta-blockade is recommended for patients with Marfan syndrome from the second trimester onward, particularly if the aortic root is dilated. Regional anesthesia during labor is considered safe. Women should labor in the left lateral decubitus position with the second stage shortened by operative vaginal delivery. Cesarean section should be reserved for obstetric indications.
• Idiopathic hypertrophic subaortic stenosis is an autosomal dominant disorder that manifests as left ventricular outflow tract obstruction secondary to a hypertrophic interventricular septum. Genetic counseling is advised for affected patients. Patients' conditions improve when left ventricular end-diastolic volume is maximized. Pregnant patients fare quite well initially because of an increase in circulating blood volume. There is less progression of disease in those patients who are asymptomatic before pregnancy. Later in pregnancy, however, decreased systemic vascular resistance and decreased venous return may worsen the obstruction. This may cause left ventricular failure as well as supraventricular arrhythmias
P.215 from left atrial distention. The following labor management points should be kept in mind: (a) Inotropic agents may exacerbate obstruction, (b) medications that decrease systemic vascular resistance should be avoided or limited, (c) cardiac rhythm should be monitored and tachycardia treated promptly, and (d) the patient should undergo labor in the left lateral decubitus position with the second stage of labor shortened by operative vaginal delivery.
• Transposition of the great arteries (TGA) is characterized by correct atrioventricular connections and inappropriate ventriculoarterial connections; the aorta arises anteriorly from the right ventricle, and the pulmonary artery arises posteriorly from the left ventricle. The Senning operation (using atrial and septal tissues) and Mustard operation (using extrinsic material such as pericardium) redirect atrial blood via baffles to deliver oxygenated pulmonary venous blood to the systemic right ventricle and deoxygenated systemic venous blood to the pulmonary left ventricle. Long-term follow-up demonstrates an 80% survival at 28 years with the majority of survivors in NYHA class I. Pregnancy in women after Senning or Mustard repair is associated with arrhythmias (VT, SVT, atrial flutter), heart failure, and NYHA functional class deterioration as well as a high incidence of serious obstetric complications (65%) and offspring mortality (11.7%).
• Congenital atrioventricular block: Although affected patients may need a pacemaker, they usually fare well and do not require special treatment during pregnancy.
Arrhythmias
• Premature atrial and/or ventricular complexes are not associated with adverse maternal or fetal outcomes and do not require antiarrhythmic therapy. Atrial fibrillation and atrial flutter are rare during pregnancy. Rate control can be safely achieved with digoxin or beta-blockers. Electrical cardioversion can be performed safely during any stage of pregnancy. Other arrhythmias should be managed with the assistance of a cardiologist. Nonsustained arrhythmias in the absence of organic cardiac disease are best left untreated or managed with lifestyle and dietary modifications (e.g., decreasing smoking, caffeine, and stress). Serious, life-threatening arrhythmias associated with an aberrant reentrant pathway should be treated before pregnancy by ablation. If medical therapy is necessary during pregnancy, established drugs such as beta-blockers should be used.
Artificial pacing, electrical defibrillation, and cardioversion should have no effect on the fetus.
Ischemic Heart Disease
• Ischemic heart disease is an uncommon but potentially devastating event in pregnancy. Risk factors include HTN, thrombophilia, diabetes, smoking, transfusion, postpartum infection, obesity, and age >35 years. Anterior wall myocardial infarctions (MIs) are most common. Diagnosis and evaluation of acute cardiac events is similar as in nonpregnant patients. Approximately 67% of MI during pregnancy occurs during the third trimester. If it occurs before 24 weeks' gestation, the option of pregnancy termination should be discussed due to the high incidence of maternal mortality. If delivery takes place within 2 weeks of the acute event, the mortality rate reaches 50%; survival is much improved if delivery takes place more than 2 weeks after the acute event.
P.216
• Coronary angioplasty is the preferred reperfusion therapy in cases of ST-elevated MI. Medical therapy for acute MI should be modified in the pregnant patient. Thrombolytic agents increase the risk of maternal hemorrhage to 8% for women who receive thrombolytic therapy shortly after delivery. Low-dose aspirin and nitrates are considered safe. Beta-blockers are safe, although some have been linked to a slight decrease in fetal growth. Short-term heparin administration has not been associated with increased maternal or fetal adverse effects. Angiotensin-converting enzyme (ACE) inhibitors and statins are contraindicated during pregnancy. Hydralazine and nitrates may be used as substitutes for ACE inhibitors.
Cardiovascular Drugs in Pregnancy
• The most commonly used cardiovascular drugs and their potential adverse effects during pregnancy are shown in Table 15-2.
• Anticoagulation: Several conditions require the initiation or maintenance of anticoagulation during pregnancy. Anticoagulation choice depends on patient and physician preferences after consideration of the maternal and fetal risks. The three most common agents considered during pregnancy are warfarin, unfractionated heparin (UFH), and low-molecular-weight heparin (LMWH).
• UFH does not cross the placenta and is safe for the fetus. Its use, however, has been associated with maternal osteoporosis, hemorrhage at the uteroplacental junction, thrombocytopenia (heparin-induced thrombocytopenia [HIT]), thrombosis, and a high incidence (12% to 24%) of thromboembolic events with older generation mechanical valves. High doses of UFH are often required to achieve the desired activated partial thromboplastin time (aPTT) due to the hypercoagulable state associated with pregnancy. Parenteral infusions should be stopped at least 4 hours before cesarean sections. UFH can be reversed with protamine sulfate.
• LMWH, in comparison to UFH, produces a more predictable anticoagulant response, is less likely to cause HIT, is easier to administer and monitor, and has lower risk of osteoporosis and bleeding complications. LMWH does not cross the placenta and is safe for the fetus. Antifactor-Xa levels can be checked 4 hours after the morning dose and the dose adjusted to attain antifactor-Xa levels of 0.7 to 1.2 U/mL. Although data support the use of LMWH for DVT treatment in pregnant women, there are no data to guide its use in pregnant patients with mechanical valve prostheses and several small studies have shown increased rates of serious complications.
• Warfarin, a vitamin K antagonist, freely crosses the placenta and can harm the fetus. The incidence of warfarin embryopathy (abnormalities of fetal bone and cartilage formation) has been estimated at 4% to 10%; the risk is highest when warfarin is administered during the 6th through 12th weeks' gestation.
Clinically important embryopathy may be lower if the warfarin dose is bgcolor=white>Sodium nitroprusside